Back to Journals » Vascular Health and Risk Management » Volume 18
Demographics and Risk Profile of Elderly Middle Eastern Patients with Atrial Fibrillation: The Jordan Atrial Fibrillation (JoFib) Study
Authors Alhaddad Z, Hammoudeh A, Khader Y ![]() , Alhaddad IA
, Alhaddad IA ![]()
Received 3 February 2022
Accepted for publication 6 April 2022
Published 15 April 2022 Volume 2022:18 Pages 289—295
DOI https://doi.org/10.2147/VHRM.S360822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Zayd Alhaddad,1 Ayman Hammoudeh,2 Yousef Khader,3 Imad A Alhaddad4
1Department of Medicine, MedStar Union Memorial Hospital, Baltimore, MD, USA; 2Cardiology Department, Istishari Hospital, Amman, Jordan; 3Department of Public Health, Jordan University of Science and Technology School of Medicine, Irbid, Jordan; 4Cardiovascular Department, Jordan Hospital, Amman, Jordan
Correspondence: Imad A Alhaddad, Cardiovascular Department, Jordan Hospital, Amman, Jordan, Tel +962 795303502, Email [email protected]
Background: Atrial fibrillation (AF) is the most common arrhythmia that is associated with high morbidity and mortality. The prevalence of AF increases with age and the elderly constitute a vulnerable cohort for higher stroke and bleeding complications.
Methods: A total of 2163 adult consecutive patients with AF in 19 hospitals and 11 outpatient clinics in Jordan were enrolled in the Jordan AF study from May 2019 to January 2021. The clinical characteristics, demographics, and risk profiles of the elderly patients (≥ 80 years old) were compared to the younger patients (< 80 years old).
Results: Of 2163 patients, 379 (17.5%) constituted the elderly group. The elderly group had higher prevalence of hypertension (79.9% vs 73.5%, p=0.01), lower prevalence of smoking (5.0% vs 15.2%, p< 0.001) and lower body mass index (28.1 ± 5.5 kg/m2 vs 29.8 ± 6.2 kg/m2, p< 0.001) compared with younger patients. They also had more strokes or systemic emboli (25.6% vs 14.7%, p< 0.001), heart failure (30.3% vs 22.9%, p=0.002), pulmonary hypertension (30.6% vs 24.8%, p=0.02), and chronic kidney disease (13.5% vs 8.3%, p=0.002). The elderly cohort had higher mean CHA2DS2-VASc (5.0 ± 1.5 vs 3.6 ± 1.8, p< 0.001) and HAS-BLED scores (2.2 ± 1.1 vs 1.5 ± 1.1, p< 0.001) compared to younger group. Among 370 elderly with non-valvular AF (NVAF), oral anticoagulant agents (OACs) were prescribed for 278 (84.2%) of eligible high-risk patients. Of the 1402 younger patients with NVAF, OACs were prescribed for 1133 (84.3%) of eligible patients. Direct oral anticoagulant agents (DOACs) were more frequently used in the elderly compared to the young (72.3% vs 62.3%, p< 0.001).
Conclusion: Elderly Middle Eastern AF patients have worse baseline clinical profiles and higher risk scores compared to younger patients. The majority of the elderly were prescribed guideline directed OACs, with higher use of DOACs than the younger cohort.
Clinical Studies Registration: The study is registered on clinicaltrials.gov (unique identifier number NCT03917992).
Keywords: atrial fibrillation, elderly patients, middle eastern patients, risk scores
Introduction
Atrial fibrillation (AF) is the most common arrhythmia that is associated with high morbidity and mortality and an increased risk of stroke and systemic embolization.1,2 The prevalence of AF increases with age and it affects up to 17% of people over the age of 80 years.3 The elderly patients constitute a vulnerable cohort who are not only at a higher risk of complications of AF, but also of complications of treatment such as major bleeding events. Identifying the demographics and risk assessment of such a vulnerable group is important for tailoring therapeutic interventions.
Most clinical and epidemiological studies and registries of AF have been conducted in Western countries where clinical features, guideline adherence, and prognosis in patients with AF may differ significantly compared with those in the Middle East.4–6 Several Middle Eastern studies have shown that the AF population in the region is younger with a higher prevalence of cardiovascular risk factors including obesity, diabetes mellitus, hypertension, and coronary arterial disease.4
Many of the studies in the Middle East incorporate foreign nationals, mainly the working force of South Asians, and were conducted before the wide use of newer oral anticoagulant agents (OACs). Hence, the conclusions of these studies cannot be generalized to embody the native populations of the region.
Prevention of stroke and systemic embolization in patients with AF is mainly achieved by the prescription of OACs, including vitamin K antagonists (VKA) which are approved for valvular AF (VAF), and direct oral anticoagulants (DOACs) that are preferably indicated over VKA for non-valvular AF (NVAF).7 Adoption of recent guideline directed therapies of OAC varies widely from one region to the other and within the same region.
This study aimed to assess the demographics, clinical characteristics, CHA2DS2-VASc and HAS-BLED scores, and utilization of OAC in a cohort of elderly Middle Eastern patients (≥ 80 years old).
Methods
The Jordan AF (JoFIB) registry is a prospective, multicenter observational registry that enrolled consecutive AF patients aged >18 years in 19 hospitals and 11 outpatient clinics across Jordan between May 2019 through January 2021. The methodology was published previously.8 Briefly, data were collected using standardized clinical data form at the time of enrollment, and at one, 6 and 12 months after the initial assessment. Diagnosis of AF was confirmed by a 12-lead electrocardiogram (EKG) rhythm strip lasting >30 seconds, >1 episode of AF on an ambulatory EKG monitor, or a past diagnosis by a treating cardiologist. Baseline data included clinical and demographic profiles, laboratory data, EKG, transthoracic echocardiographic features, and the use of OACs and other pharmacological medications. Standard definitions were used to classify the types of AF, including paroxysmal, persistent, long-standing, and permanent and to calculate the CHA2DS2-VASc9 and HAS-BLED10 scores for each patient. Eligibility for oral anticoagulant agents was analyzed based on the 2019 focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation.11
The patients were stratified into two groups based on age with the elderly group including all patients aged 80 years and older at the time of inclusion and the younger group being patients 79 years and younger. The clinical characteristics, comorbidities, risk scores, and use of different medications were compared between the two groups.
The study was approved by the Institutional Review Board of participating centers and patients signed written informed consent. All treatment decisions were left to the discretion of the treating physician. The study was registered at clinicaltrials.gov (NCT03917992).
Statistical Analysis
Descriptive statistics were performed using means and standard deviation (SD) to describe the continuous variables and percentages to describe the categorical variables. An independent t-test was used to compare means and Chi-square test was used to compare categorical data. A p<0.05 was considered statistically significant.
Results
A total of 2163 patients were included in the study with 379 (17.5%) patients being 80 years or older at the time of enrollment and 1784 (82.5%) patients were the younger than 80 years. The patients’ demographic and clinical data are shown in Table 1. Both age groups did not differ significantly in gender distribution and prevalence rates of diabetes and dyslipidemia. However, the elderly group had more hypertensives but fewer smokers compared to the younger group. Overall, the elderly patients had a more favorable body mass index (BMI) profile with fewer obese patients. The elderly were less likely to have VAF or paroxysmal AF compared to the younger patients. Baseline clinical profile showed that the elderly patients were more likely to have had a stroke or systemic embolization, heart failure, pulmonary hypertension, and chronic kidney disease compared to the younger patients.
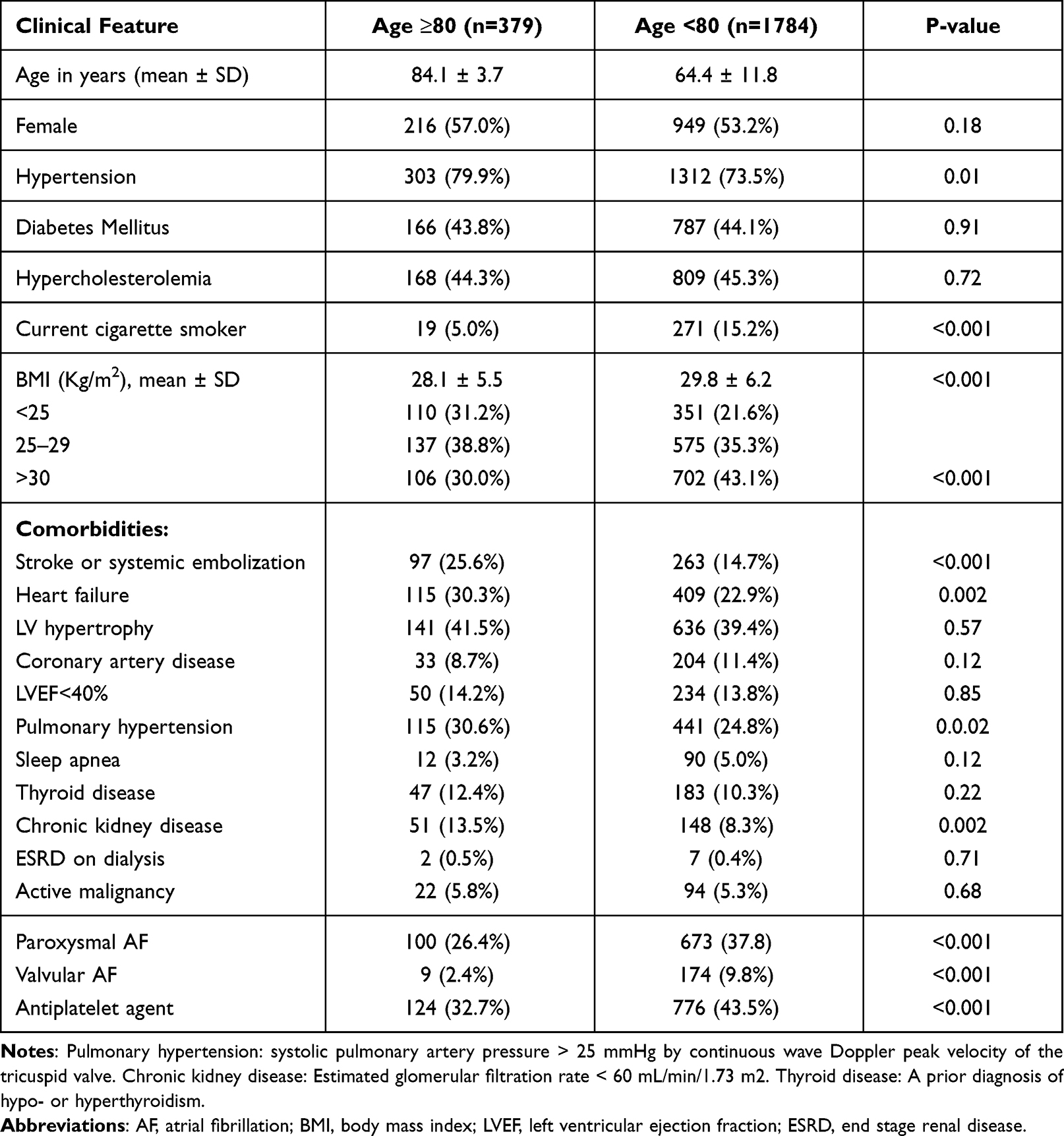 |
Table 1 Demographics and Clinical Characteristics of Middle Eastern Patients with Atrial Fibrillation |
As for AF specific risk scores, the elderly patients were at higher risk of both stroke and systemic embolization and major bleeding events as represented by the CHA2DS2-VASc (5.0 ± 1.5 vs 3.6 ± 1.8, p<0.001) and HAS-BLED scores (2.2 ± 1.1 vs 1.5 ± 1.1, p<0.001) compared to the younger patients. Figure 1 shows the CHA2DS2VASc scores in both groups. Most elderly patients were more likely to have scores > 3 than younger patients (83.6% vs 46.2%, p<0.001). Figure 2 shows the HAS-BLED scores in both groups.
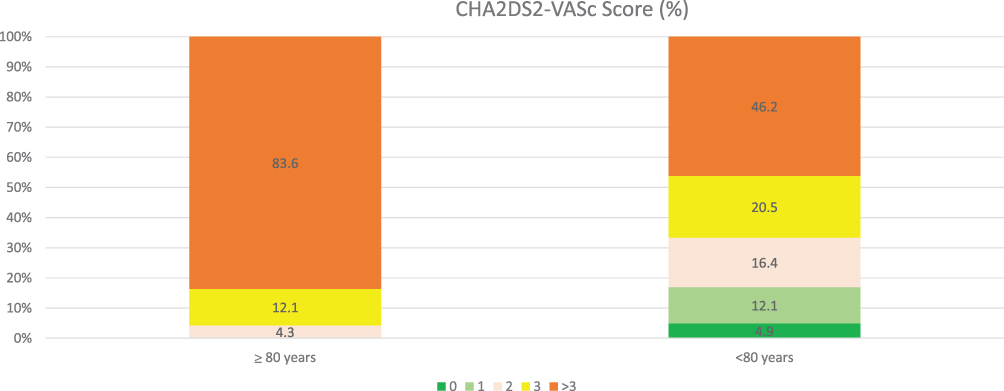 |
Figure 1 CHA2DS2-VASc score in the two age groups of patients with non-valvular atrial fibrillation (NVAF). |
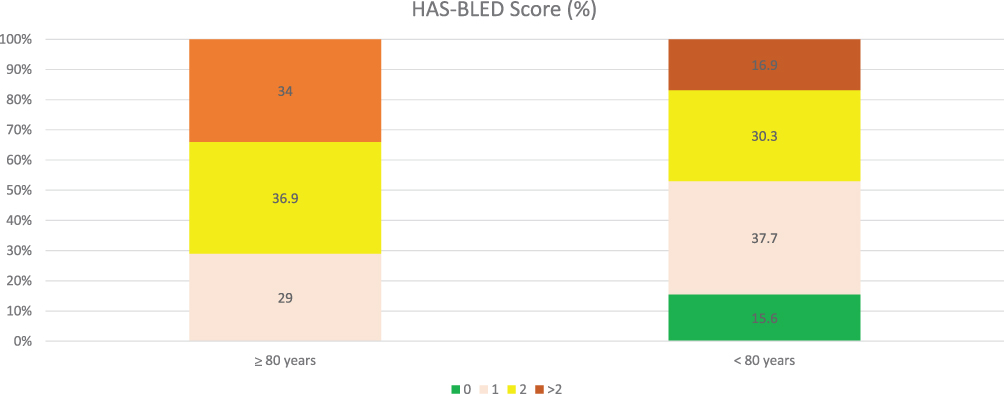 |
Figure 2 The HAS-BLED score in the two age groups of patients with non-valvular atrial fibrillation (NVAF). |
The utilization of OAC in patients with NVAF in both groups is shown in Table 2. Most patients in both groups were eligible for OCA. While there was a similar rate of utilization of OAC in both groups, the elderly patients were more likely to be treated with DOACs compared to younger patients.
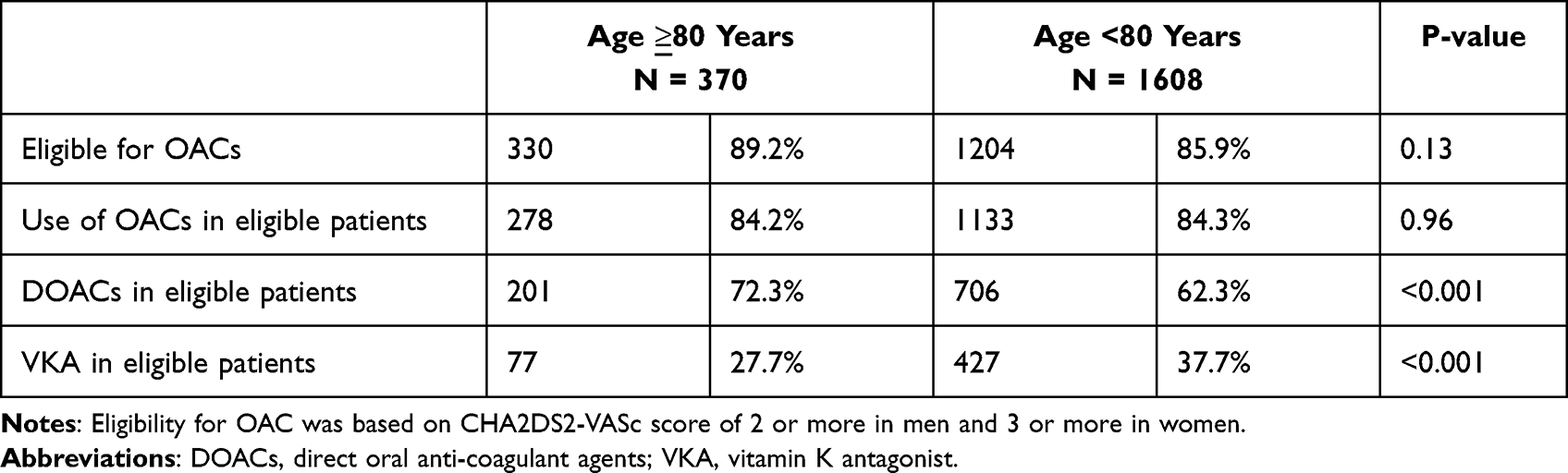 |
Table 2 The Utilization of Oral Anticoagulation in Patients with Non-Valvular Atrial Fibrillation |
Discussion
To our knowledge, this is the first study to provide a better understanding of the clinical and risk profiles of octogenarian and older Middle Eastern AF patients. Almost one in five Middle Eastern patients with AF were ≥ 80 years, a unique and vulnerable population. Unlike other Middle Eastern studies that included heterogeneous patient populations from southeast Asia,12 our study was a homogenous Middle Eastern population with AF, enrolled in ambulatory and in-patient settings in private, public and university sectors in the country. This translated that our study has older patients with more comorbidities such as hypertension and diabetes mellitus.8,12
The overwhelming majority of Middle Eastern AF patients had nonvalvular AF with an especially higher proportion in the elderly cohort, a finding in agreement with studies from other regions in Asia such as Japan and China.13,14 Similar to the findings by other regional studies,15–17 a minority of the enrolled patients had VAF including moderate to severe rheumatic mitral stenosis and mechanical heart valves. Rheumatic heart disease prevalence is decreasing globally,18 usually affects young age groups and decreases life expectancy.19 Similarly, the implantation of mechanical heart valves is decreasing worldwide especially in elderly patients.20 In the natural time course of AF, AF commonly progresses from silent and undiagnosed to paroxysmal AF and subsequently sustained (persistent or permanent) AF.21,22 Thus, younger patients (<80 years old) are more likely to have paroxysmal AF compared to the elderly (≥ 80 years old) as many of the younger patients progress into sustained AF with time and aging.
It is not surprising that the elderly population had higher CHA2DS2-VASc and HAS-BLED scores because age is incorporated in the calculation of both scores. However, higher scores are also related to significant comorbidities including hypertension and heart failure, both of which are more prevalent in the older group. The increased prevalence of stroke and systemic embolization in this population also plays a role in the higher scores and further highlights the need for a more aggressive approach when prescribing OACs.
Contrary to the belief that elderly AF patients are less likely to receive OACs therapy because of the perception of high bleeding risk in this age group, this study shows that OACs were prescribed in a high proportion of the elderly cohort like the younger age group. Moreover, there was a higher adoption of DAOCs in the elderly group compared to the younger cohort. This could be due to the proven superior benefits and major bleeding events risk reduction of this age group compared with VKA.
The present study has few potential limitations. Similar to registries of observational nature, collected data might be subject to potential bias despite reinforcing consecutive recruitment from the outset of the study. The current study was based on patients managed by cardiologist such that these findings may not be generalizable to other specialties. However, involving 30 outpatient clinics and hospitals from private, public and university sectors in the study enhances the generalizability and relevance of the results. Despite potential limitations, the data shown represent a regional perspective to studies that evaluate clinical features, risk assessment and contemporary utilization of OACs in elderly AF patients. Furthermore, the study sets a higher standard for adherence to recent clinical practice guidelines on the utilization of OACs in the vulnerable elderly population and may help further dissemination of such measures to other specialties dealing with AF.
Conclusion
Elderly Middle Eastern AF patients have worse baseline clinical profiles and higher risk scores compared to younger patients. The majority of the elderly were prescribed guideline directed OACs, with higher use of DOACs than the younger cohort. The impact of these observations on the incidence of stroke, systemic embolization and major bleeding events awaits the one-year follow up.
Clinical Implications: The current study provides a better understanding of the clinical and risk profiles of octogenarian and older Middle Eastern AF patients. Despite an elevated bleeding risk, this group has a much higher risk of stroke and systemic embolization and was appropriately treated with guideline directed OACs including DOACs.
Data Sharing Statement
The authors intend to share all pertinent individual deidentified participant data. Data can be shared for 3 years after publication and will be available by contacting the corresponding author directly.
Ethics Statement
The study was approved by the Institutional Review Board of the following participating centers: Amman Surgical Hospital, Arab Medical Center, Essra Hospital, Ibn Haitham Hospital, Islamic Hospital, Istishari Hospital, Jordan Hospital, Khalidi Medical Center, King Abdullah University Hospital, King Hussein Medical Center, Prince Hamza Hospital, Prince Hashem Hospital, Queen Alia Cardiac Center, Salt Medical Center and Specialist Hospital.
All patients signed written informed consent and treatment decisions were left to the discretion of the treating physician.
Acknowledgments
The authors would like to thank the participating physicians who enrolled patients for the study (in alphabetical order): Abdallah Al-Kasasbeh, Abdelrahman Obiedat, Abdullah Bani-Melhim, Abdul Nasser Almohamed, Ahmad Abdelsattar, Ahmad Abu Awwad, Ahmad Sbaih, Ahmad Tamari, Alaa Ababneh, Alanoud Hamada, Alia Khamis, Ali Abu-Romman, Ali Shakhatreh, Amer Asia, Amin Ibdah, Amr Adas, Assem Nammas, Aws Mukhtar, Ayad Al Qudsi, Basil Abdeen, Dalia Rawashdeh, Eid Abu- Eid, Eyadeh Madanat, Eyas Al Mousa, Fahd Al-Karmi, Farah Al-Sayyed, Farah Halaweh, Fatima Al Nadi, Hana Al- Raie, Haneen Shawer, Hani Juha, Hanin Saleh, Hanna Makhamreh, Hazem Abu Asbeh, Hesham Janabi, Hisham Amin, Ibrahim Abbadi, Ibrahim Jarrad, Islam Abu Sedo, Islam Obeidat, Ismail Hamam, Kais Bilbeisi, Lama Khader, Leen Sharqawi, Liza Shaban, Lubaba Qabbaa, Lubna Haikal, Lubaba Qabbaah, Laith Habahbeh, Marwan Nemri, Marwan Al Sultan, Mo’ath Alfawar’a, Mohammad Abdah, Mohammad Afeef, Mohammad Al-Jawabreh, Mohammad Ali Jarrah, Mohammad Hani, Mohammad Kraishan, Mohannad Ababneh, Mohamad Jarrah, Mohammad Jabary, Munir Zaqqa, Mustafa Jammal, Myassar Amr, Nazih Kaderi, Noor Al-Badaineh, Obada Mansour, Odai Khasawneh, Oday Abu Ajameyyeh, Omar Abu Slieh, Omar Obeidat, Omar Salaymeh, Omran Abukhalaf, Osama Oudeh, Qusai Abu Ajameyyeh, Raed Awaisheh, Rami Bataineh, Ramzi Tabbalat, Rashid Abdah, Sa’ad Al-Muhaisen, Saed Al Ghamri, Safa’ Amro, Said Meri, Saleh Ghamdi, Sukaina Rawashdeh, Sara Al-Thunibat, Sara Younis, Sharif Adwan, Sulafa Saffarini, Tamer Salhab, Tawfiq Barqawi, Yahya Badaineh, Yahya Ismail, Yousef Khader, Zaid Dabash, Zeina Abu-Orabi, Zainab Salahat, Zainah Matani, Zakaria Shkoukani, and Zakariya Al-Hasanat.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest for this work.
References
1. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2021;16(2):217–221. doi:10.1177/1747493019897870
2. Lopez-Lopez JA, Sterne JAC, Thom HHZ, et al. Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis. BMJ. 2017;359:j5058. doi:10.1136/bmj.j5058
3. Gómez-Doblas JJ, Muñiz J, Martin JJ, et al. OFRECE study collaborators. Prevalence of atrial fibrillation in Spain. OFRECE study results. Rev Esp Cardiol. 2014;67(4):259–269. doi:10.1016/j.rec.2013.07.014
4. Azar RR, Ragy HI, Kozan O, et al. Antithrombotic treatment pattern in newly diagnosed atrial fibrillation patients and 2-year follow-up results for dabigatran-treated patients in the Africa/Middle-East Region: Phase II results from the GLORIA-AF registry program. Int J Cardiol Heart Vasc. 2021;34:100763. doi:10.1016/j.ijcha.2021.100763
5. Healey JS, Oldgren J, Ezekowitz M, et al. RE-LY Atrial Fibrillation Registry and Cohort Study Investigators. Occurrence of death and stroke in patients in 47 countries 1 year after presenting with atrial fibrillation: a cohort study. Lancet. 2016;388(10050):1161–1169. doi:10.1016/S0140-6736(16)30968-0
6. Ribeiro AL, Otto CM. “Heartbeat: the worldwide burden of atrial fibrillation. Heart. 2018;104:1987–1988. doi:10.1136/heartjnl-2018-314443
7. Bassand JP, Virdone S, Goldhaber SZ, et al. Early Risks of Death, Stroke/Systemic Embolism, and Major Bleeding in Patients With Newly Diagnosed Atrial Fibrillation. Circulation. 2019;139(6):787–798. doi:10.1161/CIRCULATIONAHA.118.035012
8. Hammoudeh AJ, Khader Y, Kadri N, et al. Adherence to the 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline on the Use of Oral Anticoagulant Agents in Middle Eastern Patients with Atrial Fibrillation: the Jordan Atrial Fibrillation (JoFib) Study. Int J Vasc Med. 2021;2021:5515089. doi:10.1155/2021/5515089
9. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263–272. doi:10.1378/chest.09-1584
10. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138(5):1093–1100. doi:10.1378/chest.10-0134
11. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(1):104–132. doi:10.1016/j.jacc.2019.01.011
12. Zubaid M, Rashed WA, Alsheikh-Ali AA, et al. Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) Investigators. Gulf Survey of Atrial Fibrillation Events (Gulf SAFE): design and baseline characteristics of patients with atrial fibrillation in the Arab Middle East. Circ Cardiovasc Qual Outcomes. 2011;4(4):477–482. doi:10.1161/CIRCOUTCOMES.110.959700
13. Hiasa KI, Kaku H, Inoue H, et al. Age-Related Differences in the Clinical Characteristics and Treatment of Elderly Patients With Atrial Fibrillation in Japan - Insight From the ANAFIE (All Nippon AF In Elderly) Registry. Circ J. 2020;84(3):388–396. doi:10.1253/circj.CJ-19-0898
14. Xing L, Lin M, Du Z, et al. Epidemiology of atrial fibrillation in northeast China: a cross-sectional study, 2017-2019. Heart. 2020;106(8):590–595. doi:10.1136/heartjnl-2019-315397
15. Salam AM, AlBinali HA, Al-Mulla AW, Singh R, Al Suwaidi J. Secular trends, treatments, and outcomes of Middle Eastern Arab and South Asian patients hospitalized with atrial fibrillation: insights from a 20-year registry in Qatar (1991-2010). Angiology. 2013;64(7):498–504. doi:10.1177/0003319712460332
16. Lip GYH, Brechin CM, Lane DA. The global burden of atrial fibrillation and stroke: a systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe. Chest. 2012;142(6):1489–1498. doi:10.1378/chest.11-2888
17. El Kadri M, Bazargani N, Farghaly M, et al. Profiling clinical characteristics and treatment patterns among non-valvular atrial fibrillation patients: a real-world analysis in Dubai, United Arab Emirates. Open Med J. 2019;6:33–41. doi:10.2174/1874220301906010033
18. Watkins DA, Johnson CO, Colquhoun SM, et al. Global, Regional, and National Burden of Rheumatic Heart Disease, 1990-2015. N Engl J Med. 2017;377(8):713–722. doi:10.1056/NEJMoa1603693
19. He VY, Condon JR, Ralph AP, et al. Long-Term Outcomes From Acute Rheumatic Fever and Rheumatic Heart Disease: a Data-Linkage and Survival Analysis Approach. Circulation. 2016;134(3):222–232. doi:10.1161/CIRCULATIONAHA.115.020966
20. Manji RA, Ekser B, Menkis AH, Cooper DK. Bioprosthetic heart valves of the future. Xenotransplantation. 2014;21(1):1–10. doi:10.1111/xen.12080
21. Kato T, Yamashita T, Sagara K, Iinuma H, Fu LT. Progressive nature of paroxysmal atrial fibrillation. Observations from a 14-year follow-up study. Circ J. 2004;68:568–572. doi:10.1253/circj.68.568
22. Kerr CR, Humphries KH, Talajic M, et al. Progression to chronic atrial fibrillation after the initial diagnosis of paroxysmal atrial fibrillation: results from the Canadian Registry of Atrial Fibrillation. Am Heart J. 2005;149:489–496. doi:10.1016/j.ahj.2004.09.053
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.