Back to Journals » International Journal of Women's Health » Volume 18
Demographic and Screening-to-Diagnosis Cascade Indicators for Risk Stratification in an Organized Cervical Cancer Screening Program: Evidence from 82,141 Women in Yunnan, China
Authors Fan M ![]() , Yang F, Zhang D, Dang H, Lai S, Li Y, Chen X, Zhou A, Hai Q, Liu T, Lin J
, Yang F, Zhang D, Dang H, Lai S, Li Y, Chen X, Zhou A, Hai Q, Liu T, Lin J
Received 1 March 2026
Accepted for publication 1 May 2026
Published 3 June 2026 Volume 2026:18 602135
DOI https://doi.org/10.2147/IJWH.S602135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Mingyao Fan,1,2,* Fuhua Yang,3,* Dongwei Zhang,4,* Haoyuan Dang,1,2 Shunbin Lai,4 Yuxi Li,5 Xiaoai Chen,5 Ailan Zhou,4 Qingshan Hai,1,2 Tao Liu,5 Jiaci Lin6
1School of Basic Medicine, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 2Yunnan Key Laboratory of Integrated Traditional Chinese and Western Medicine for the Prevention and Treatment of Chronic Diseases, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 3School of Information, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 4Yuxi Maternal and Child Health Hospital, Yuxi, Yunnan, People’s Republic of China; 5The First Affiliated Hospital of Yunnan University of Chinese Medicine/Yunnan Provincial Hospital of Traditional Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 6School of Social and Behavioral Sciences, Nanjing University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingshan Hai, School of Basic Medicine, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China, Email [email protected] Jiaci Lin, School of Social and Behavioral Sciences, Nanjing University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: To assess an organized cervical cancer screening-to-diagnosis cascade in Yunnan Province, China, and to examine the associations of demographic factors, HPV genotyping, and cytology results with the detection of cervical precancer and cancer.
Methods: This retrospective analysis included 82,141 women who participated in a government-supported free screening program between January 2023 and July 2025. The primary endpoint was the final integrated diagnosis based on cytology, colposcopy, and histopathology, with histopathology serving as the diagnostic gold standard. Associations between candidate variables and the outcome were assessed using chi-square tests and multivariable logistic regression, and adjusted odds ratios (aORs) with 95% confidence intervals (95% CIs) were reported. Uniform Manifold Approximation and Projection (UMAP) was used for multidimensional visualization of high-risk clustering patterns.
Results: Among the participants, 1678 (2.04%) were classified as positive for cervical cancer or precancerous lesions. In the descriptive analysis, positivity rates showed significant non-linear variation across age groups, with higher proportions in women aged < 25 and ≥ 65 years, and were also higher among women with lower educational attainment and in some ethnic minority groups, including Hani and Dai women. In multivariable analysis, age remained significant overall, although only women aged 35– 44 years had higher adjusted odds than those aged 45– 54 years, while ethnicity was not significant overall except for a higher risk observed among Dai women. HPV positivity showed the strongest association with the outcome, and risk increased markedly across cytology categories from NILM to HSIL. UMAP visualization further showed that high-risk cases formed compact clusters enriched for HPV16/18 positivity and high-grade cytology.
Conclusion: In this organized screening program, HPV status and cytology were strongly associated with the detection of cervical precancer and cancer. Educational level and some demographic factors were also associated with variation in screening outcomes after adjustment, although these associations were more modest than those observed in the descriptive analysis. Demographic indicators such as age and educational level may be useful for identifying underserved groups and informing targeted referral and follow-up strategies within organized screening programmes.
Keywords: cervical cancer screening, HPV genotyping, cytology, risk stratification
Background
Cervical cancer remains one of the most common malignant tumors among women worldwide. In 2022, an estimated 660,000 new cases and 350,000 deaths were reported globally, ranking fourth in both incidence and mortality among female cancers, with the majority of the burden occurring in low- and middle-income countries.1 Human papillomavirus (HPV) is a highly prevalent double-stranded DNA virus transmitted primarily through sexual contact and skin-to-mucosa exposure, and it is recognized as a necessary cause of virtually all cervical cancers.2,3 Although most HPV infections (70–90%) are transient and clear spontaneously within 12–24 months, persistent infection with high-risk HPV (hr-HPV) genotypes can progress to cervical intraepithelial neoplasia (CIN) and, in some cases, invasive cervical cancer.4–7
Cervical cancer is largely preventable because of its well-defined etiology and the long precancerous phase. Extensive evidence has demonstrated that organized screening and HPV vaccination substantially reduce cervical cancer incidence and mortality by enabling the timely detection and treatment of precancerous lesions.8,9 Evaluations by the IARC and the WHO suggest that more than 95% of the global cervical cancer burden is potentially preventable with adequate coverage of high-quality screening and HPV vaccination, and that effective screening alone can reduce cervical cancer mortality by approximately 80% or more.10,11 Nevertheless, in settings with suboptimal HPV vaccination uptake and limited screening coverage, cervical cancer continues to impose a substantial burden among women of reproductive and midlife age.
In China, the overall prevalence of high-risk HPV (hr-HPV) infection among women has been reported to be approximately 17.7%. Globally, HPV-16 and HPV-18 account for about 70% of cervical cancers.12,13 In response, China launched a national free screening program for breast and cervical cancer in rural women in 2009, and, under the Health China Initiative (2019–2030) and the WHO cervical cancer elimination strategy, has progressively established a multi-tiered screening–diagnosis–follow-up system centered on HPV testing, cytology, and colposcopy.14,15 Modeling studies suggest that achieving the WHO “90–70–90” targets—particularly screening 70% of women with a high-performance test by age 35 and again by age 45—could reduce cervical cancer incidence to below the elimination threshold of 4 per 100,000 women-years by the end of this century. In China-focused projections, meeting the 90–70–90 targets could avert approximately 3.5 million cervical cancer cases cumulatively by 2100.16 Recent national data showed that the cervical cancer screening rate among women aged 35–64 years in China reached 51.5% in 2023–2024, while the corresponding rate in rural areas was 48.2%. These findings suggest that overall coverage has approached the 2025 target of 50%, but in some settings it still remains below the 2030 target of 70%.15,17 Encouraging trends—declining or stabilizing cervical cancer incidence and mortality—have been reported in some settings following improvements in screening coverage and the implementation of standardized management pathways.18,19
However, the effectiveness of cervical cancer screening in real-world settings is highly dependent on regional differences in HPV epidemiology, population structure, healthcare access, and follow-up adherence. Yunnan Province, characterized by complex geography, diverse ethnic populations, and marked socioeconomic disparities between urban and rural areas, has been reported to exhibit substantial variation in HPV prevalence, genotype distribution, and cervical cancer risk across different ethnicities and regions.20–22 Screening participation and adherence to follow-up management also vary considerably across localities. Despite the expansion of national screening programs, there remains a lack of large-scale, population-based real-world evidence from such heterogeneous regions to comprehensively evaluate HPV infection patterns, the detection of precancerous lesions and cervical cancer, and the practical performance of screening strategies.
Therefore, this study utilized large-scale real-world data from the 2023–2025 free cervical cancer screening program in a city in Yunnan Province, China, to systematically analyze HPV infection patterns and the detection rates of cervical cancer and precancerous lesions among women of screening age. The objectives were to characterize the current epidemiological profile of HPV infection and cervical cancer–related disease in the region, evaluate the effectiveness of the existing screening strategy under real-world conditions, and provide evidence to support optimization of resource allocation and ongoing cervical cancer elimination efforts in Yunnan Province.
Methods
Participants and Procedures
Data for this study were obtained from maternal and child health institutions across all counties and districts in a city in Yunnan Province, China. The study population consisted of women who participated in a government-supported free cervical cancer screening program between January 1, 2023, and July 15, 2025. Inclusion and exclusion criteria are detailed in Figure 1, which summarizes the participant selection process. Briefly, the initial dataset comprised 99,437 women enrolled in the free cervical cancer screening program in this city. Women were eligible if they were aged 18 years or older, had Yuxi household registration or belonged to the resident population, and had completed at least one cervical cancer screening procedure. Women were excluded if they were menstruating, pregnant, or lactating; had a prior history of cervical cancer or related treatment; or had records with missing key variables or logical inconsistencies. In addition, records without an available final diagnosis, including those classified as not examined, indeterminate, or not available, were excluded. After deduplication, consistency checks, and application of these criteria, 82,141 participants remained and were included in the final analysis (Figure 1). The present study involved a secondary analysis of de-identified data derived from an existing government-supported cervical cancer screening programme database. The dates from 2023 onward refer to the period of routine data generation within the screening programme rather than the initiation of the present research analysis. The study protocol was reviewed and approved by the Ethics Committee of Yunnan Provincial Hospital of Traditional Chinese Medicine (Approval No.: 2024-KY-006-01). Written informed consent had been obtained from participants during the original screening programme. This study was conducted in accordance with the Declaration of Helsinki, and all methods were performed in accordance with relevant guidelines and regulations. Written informed consent was obtained from participants before examination and before the collection of screening-related data.
 |
Figure 1 Flowchart of participant selection. |
Screening Procedures, and Variable Definitions
The original screening data were derived from an organized cervical cancer screening program conducted under a standardized quality-control framework.23 According to the applicable technical standard, this framework covered institutional requirements, personnel qualifications and training, information management, specimen collection and handling, HPV testing procedures, cytology reporting using the Bethesda System, colposcopy referral and examination, histopathologic assessment, and routine quality-control measures across the screening pathway. For the present analysis, core variables, including demographic characteristics, gynecologic clinical findings, HPV testing results, cytology (TBS), colposcopy, and histopathology, were further reviewed for completeness and logical consistency, and duplicate or ineligible records were excluded. The primary analytic outcome was the final diagnosis, determined through an integrated assessment of cytology, colposcopy, and histopathology, with histopathology serving as the diagnostic gold standard.
Among 82,141 participants, records with missing, indeterminate, or “not examined” final diagnoses were excluded. Ultimately, 1678 women (2.04%) were classified as having cervical cancer or precancerous lesions (positive group), and 80,466 were classified as negative (Figure 1). All participants completed HPV testing (100%). The completion rate for cytology was 87.61% (71,997/82,141), 7554 women (9.19%) underwent colposcopy, and 2908 (3.54%) received histopathological examination.
Screening Procedure
Screening followed standard clinical guidelines. Participants first underwent routine gynecologic examination and HPV DNA testing. Liquid-based cytology was then performed and classified according to the Bethesda System (TBS). Individuals with abnormal cytology or suspicious clinical findings underwent colposcopy, and biopsy was performed when high-grade lesions were suspected. Histopathology was considered the definitive diagnostic reference and the primary study endpoint.24–27
Outcome Definition
Participants were categorized into positive and negative groups based on the final integrated diagnosis rather than cytology classification alone. The positive group included LSIL, HSIL/CIN2–3, AIS, microinvasive cervical cancer, and invasive cervical cancer. ASC-US and ASC-H were recorded as abnormal or equivocal cytological findings under the Bethesda System, but they were not treated as positive endpoints unless subsequent integrated diagnostic assessment confirmed cervical precancer or cervical cancer. The negative group included NILM, ASC-US, ASC-H, benign inflammatory conditions, benign structural lesions, and non-cervical malignancies when no cervical precancer or cervical cancer was confirmed.28–30
Demographic Variables
Baseline demographic variables included age, ethnicity, and educational level for descriptive and stratified analyses. Age was grouped as <25, 25–34, 35–44, 45–54, 55–64, and ≥65 years.31 Ethnicity was categorized as Han, Yi, Hani, Dai, Hui, Mongol, Bai, Lahu, and other minorities. Educational level was categorized as illiterate or primary school, junior high school, senior high school / vocational school and college degree or above.32
Screening and Diagnostic Variables
Gynecologic clinical findings were classified as normal, infectious or inflammatory, structural or neoplastic, other abnormal, not examined, or missing.29 HPV genotypes were grouped by oncogenic risk as HPV16/18 positive, positive for other high-risk types without HPV16/18, low-risk or unclassified HPV positive, and HPV negative or not tested (reference).26,33 Cytological results were classified according to TBS as NILM, low-grade abnormalities (ASC-US or LSIL), high-grade abnormalities (ASC-H, HSIL, or SCC), glandular epithelial abnormalities or glandular-origin neoplasia (AGC, AGC-FN, AIS, or cervical adenocarcinoma), and cytology not performed or missing.34–36 Colposcopic findings were categorized as normal, low-grade lesions, high-grade lesions, suspected malignancy, other abnormal findings, and colposcopy not performed, missing, or uninterpretable. Histopathological diagnosis was categorized by the most severe finding as unavailable or non-diagnostic histopathology, negative or benign changes, LSIL/CIN1, HSIL/CIN2–3, AIS, and microinvasive or invasive cervical cancer, including squamous cell carcinoma and adenocarcinoma.37–39
Statistical Analysis
All statistical analyses were performed using R software (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria). After excluding records that did not meet the inclusion criteria or lacked a final diagnosis, a total of 82,141 participants were included in the final analytic sample. Descriptive statistics were first used to summarize demographic characteristics and screening-related variables, with results presented as frequencies and percentages (n, %). Differences in the distribution of categorical variables between the positive and negative groups were assessed using Chi-square tests (χ2-tests), treating missing or unperformed examinations as separate analytical categories. All statistical tests were two-sided, and a significance level of P < 0.05 was applied.
Univariable associations for all categorical candidate variables were first described using crude odds ratios (ORs) with 95% confidence intervals (95% CIs), and these results are presented in Supplementary Figure S1. Multivariable logistic regression was then performed to assess adjusted associations with the final diagnosis. Age, ethnicity, educational level, gynecologic clinical findings, and HPV diagnosis were included in the model to account for potential confounding factors. For each categorical variable, the clinically relevant or most common category was designated as the reference group. Adjusted odds ratios (aORs) with 95% confidence intervals (95% CIs) were estimated for all non-reference levels, and likelihood ratio tests were used to evaluate the overall significance of multi-category variables. Forest plots were used to visualize the adjusted associations.
In addition, to explore the latent structure of multidimensional clinical features within the overall sample and to characterize the distribution patterns of different stratification variables in the feature space, we applied Uniform Manifold Approximation and Projection (UMAP) for nonlinear dimensionality reduction and visualization. Six variables—age, ethnicity, educational level, gynecologic clinical diagnosis, HPV diagnosis, and TBS diagnosis—were used to construct the feature matrix. All categorical variables were transformed into numeric form through one-hot encoding. The UMAP algorithm was implemented in R using the “uwot” package with the following parameter settings: n_neighbors = 30, min_dist = 0.10, and metric = “euclidean”. A two-dimensional embedding (UMAP_1 and UMAP_2) was generated, and UMAP scatterplots were created by coloring the embedded points according to different stratification variables. These visualizations were used to qualitatively assess the overall sample structure and the distributional patterns of different categories within the embedded feature space.
Results
Socio-Demographic Characteristics of the Respondents
Demographic characteristics are shown in Table 1. A total of 82,141 women were included in this study. Overall, the majority of participants were within the 35–54-year age range, with 35–44 years accounting for 30.9% (25,341 cases) and 45–54 years accounting for 41.6% (34,136 cases), which aligns with the primary target age for cervical cancer screening in China. Women aged <25 years and ≥65 years represented 0.6% and 0.4% of the population, respectively.
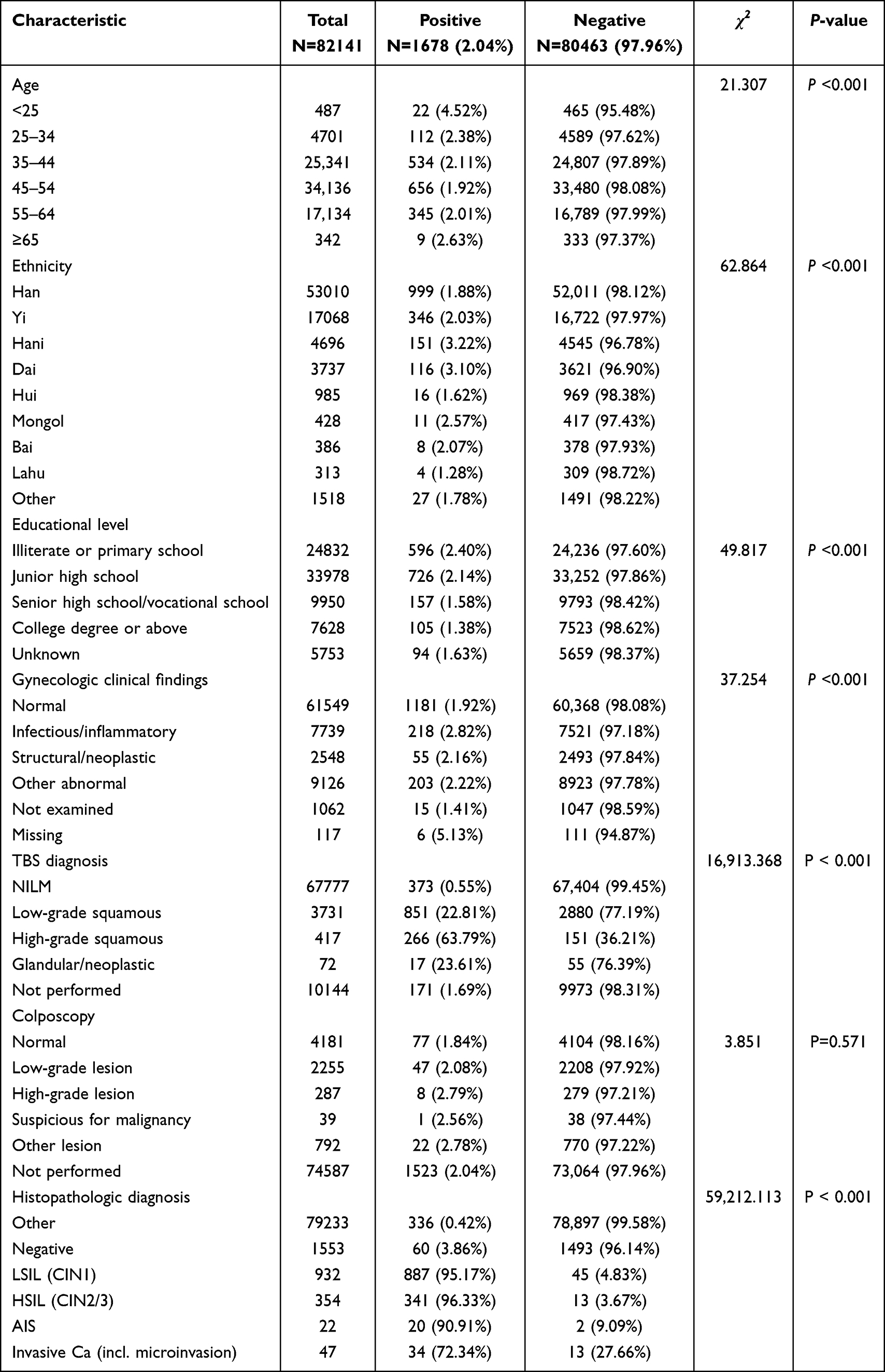 |
Table 1 Distribution of Demographic and Clinical Characteristics Between Positive and Negative Groups (χ2-Tests) |
Regarding ethnic distribution, Han ethnicity constituted the largest group (64.5%, 53,010 cases), followed by Yi (20.8%, 17,068 cases), Hani (5.7%, 4696 cases), and Dai (4.6%, 3737 cases). Other minority groups—including Hui, Mongol, Bai, and Lahu—collectively accounted for 4.4% (3214 cases), reflecting the multi-ethnic composition of Yunnan Province.
In terms of educational attainment, illiterate or primary school level accounted for 30.3% (24,832 cases); junior high school was the most common level, representing 41.4% (33,978 cases); senior high school or vocational school accounted for 12.1% (9950 cases); and college degree or above accounted for 9.3% (7628 cases). Additionally, 7.0% (5753 cases) did not report their educational level.
Bivariate Associations with the Final Diagnosis
As shown in Table 1, bivariate chi-square analyses indicated significant associations between several demographic characteristics and the final diagnosis of cervical cancer or precancerous lesions. The proportion of positive diagnoses differed significantly across age groups, with relatively higher positivity observed among women aged <25 years and those ≥65 years, whereas the 45–54-year group exhibited the lowest positivity rate. Ethnic disparities were also evident, with Hani and Dai women showing notably higher positivity rates compared with Han women, while some minority groups demonstrated comparatively lower rates. Educational attainment likewise showed a clear association with the final diagnosis, displaying a gradient pattern in which the positivity rate decreased progressively with increasing education level.
In terms of routine gynecologic clinical findings, significant differences were observed across clinical diagnostic categories, with women presenting with infectious or inflammatory changes showing a slightly higher positivity rate than those with normal findings. However, colposcopic categories did not differ significantly between the positive and negative groups (χ2=3.851, P=0.571), indicating limited discriminatory value of colposcopy in this screening population.
Key indicators related to cervical cancer screening demonstrated strong associations with the final diagnosis. Women who tested positive for HPV showed substantially higher positivity rates compared with HPV-negative individuals, and a clear risk gradient was observed across HPV genotype categories: the HPV16/18 group had the highest positivity rate, followed by other high-risk types, whereas the lowest rate was found among HPV-negative or untested participants. Cytological findings under the TBS system showed the strongest association with the final diagnosis; positivity increased sharply from NILM to LSIL, HSIL, and glandular abnormalities, reflecting a pronounced cytology-grade gradient. Histopathological diagnoses exhibited a similarly consistent pattern, with higher-grade categories showing markedly higher positivity rates (Table 2).
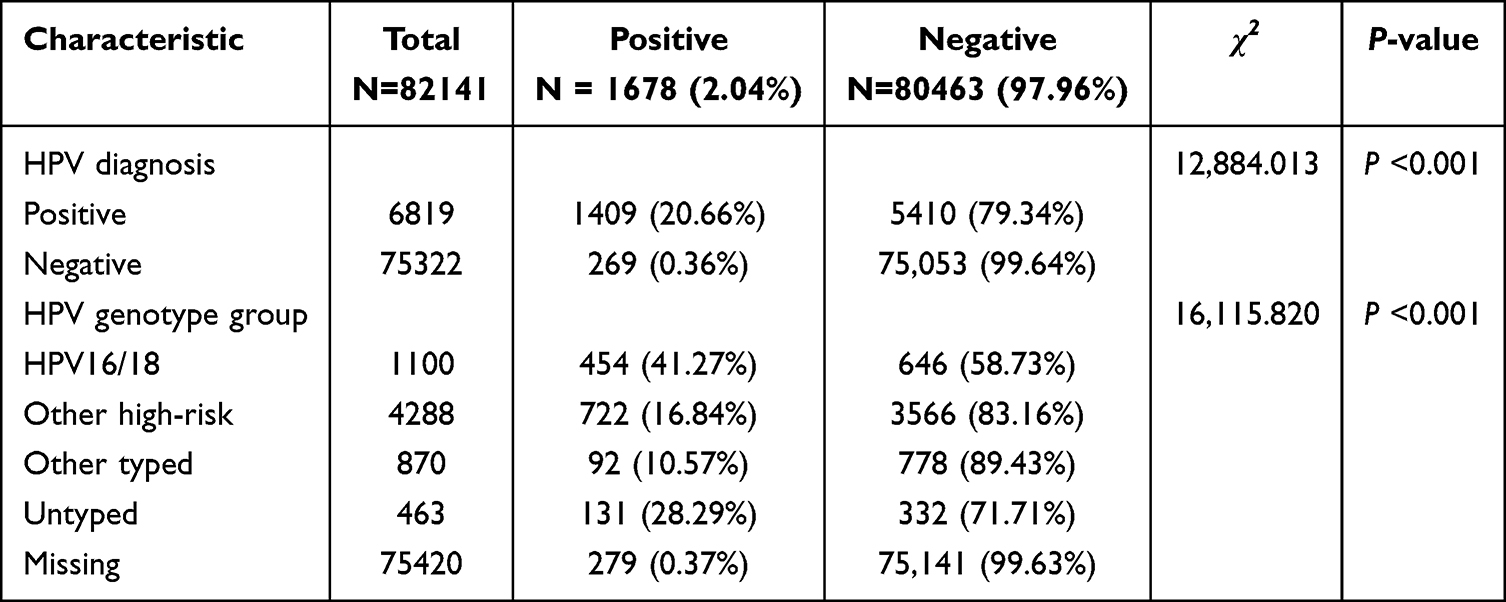 |
Table 2 Distribution of HPV Diagnosis and Genotype Categories and Their Associations with the Final Diagnosis |
Integration of Statistical Risk Profiling and Multidimensional Structural Mapping of Cervical Lesion Indicators
Associations between screening indicators and the final diagnosis were examined using multivariable logistic regression and UMAP visualization (Table 3, Figures 2 and 3). Univariable crude odds ratios are presented in Supplementary Figure S1.
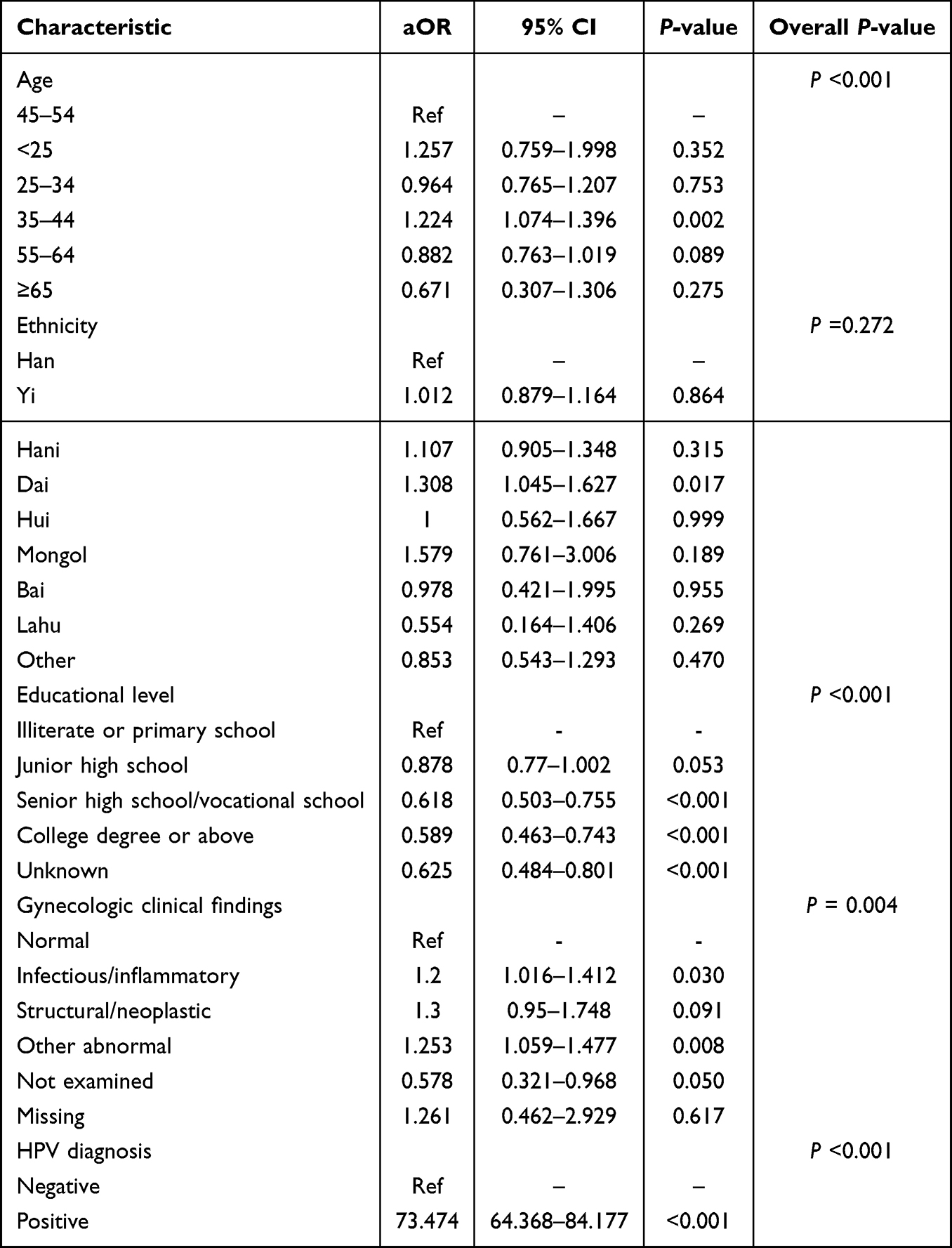 |
Table 3 Multivariable Logistic Regression Analysis of Factors Associated with a Positive Final Diagnosis |
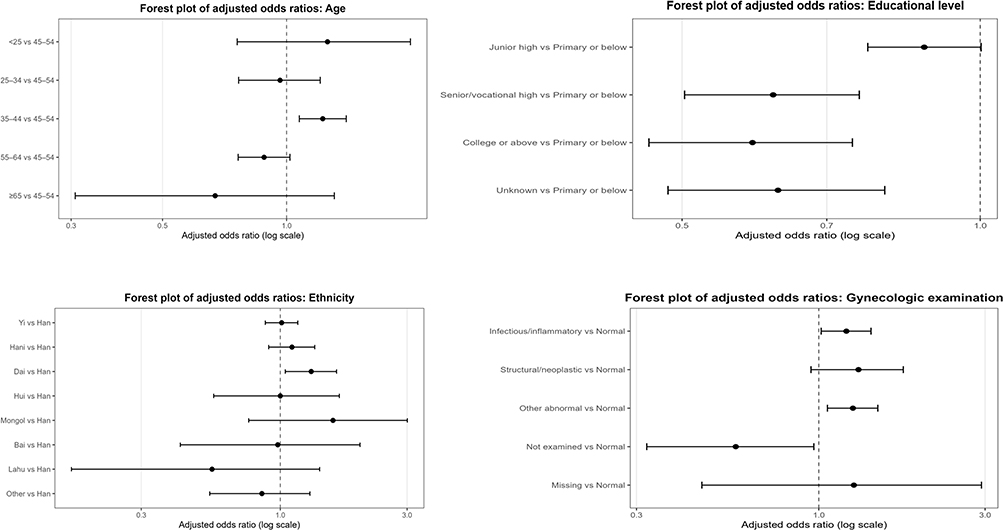 |
Figure 2 Forest plots of aORs for factors associated with a positive final diagnosis. Notes: Adjusted odds ratios (aORs) and 95% confidence intervals (95% CIs) were estimated using multivariable logistic regression. The model included age, ethnicity, educational attainment, gynecologic clinical findings, and HPV diagnosis. |
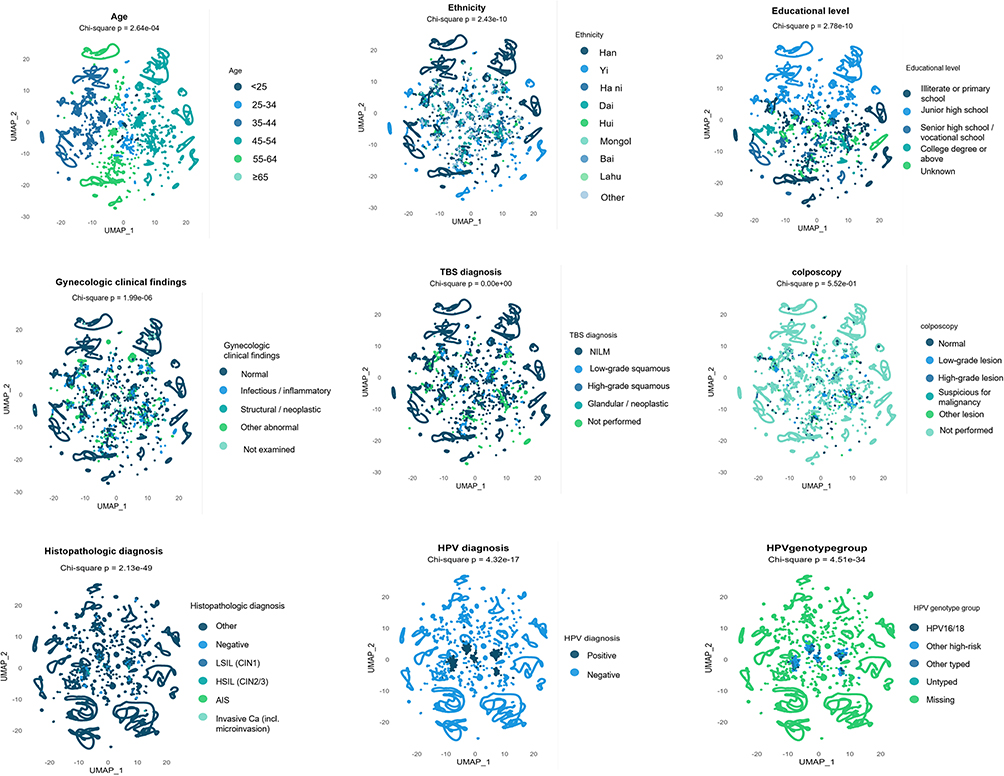 |
Figure 3 UMAP projection of multidimensional clinical features by final diagnostic outcome. Notes: UMAP embeddings were constructed using age, ethnicity, educational attainment, gynecologic clinical findings, cervical cytology (TBS classification), HPV diagnosis, HPV genotype group, and histopathologic diagnosis. Each panel shows the distribution of samples colored according to different variable categories, illustrating the multidimensional organization of clinical features in the study population. Higher-risk categories, including HPV16/18 positivity, high-grade cytologic abnormalities, and CIN2+ histopathologic lesions, tended to cluster in more localized regions, whereas lower-risk categories, such as HPV-negative status, NILM cytology, and negative histopathology, were distributed more centrally or diffusely across the embedding space. |
In the multivariable model, age remained significant overall. With women aged 45–54 years as the reference group, those aged 35–44 years had higher odds of a positive final diagnosis, whereas no significant differences were observed for the other age groups. Educational level also remained significant overall. Compared with women with illiterate or primary school education, those with senior high school/vocational school education and those with a college degree or above had lower odds of positivity. Ethnicity was not significant as an overall variable, although Dai women had higher adjusted odds than Han women. Among gynecologic clinical findings, infectious/inflammatory findings and other abnormal findings were associated with higher odds of a positive final diagnosis, whereas structural/neoplastic findings were not significant after adjustment. HPV diagnosis showed the strongest adjusted association.
The UMAP projection showed partial separation of several clinical features. Women aged 25–54 years were mainly distributed in central regions of the embedding space, whereas younger and older women were more diffusely distributed. Educational level showed a graded pattern, with lower educational categories distributed more broadly and higher educational categories located more centrally. Ethnic categories overlapped substantially, although Dai cases appeared relatively enriched in some regions. Gynecologic clinical findings also showed considerable overlap, with infectious/inflammatory and other abnormal findings displaying modest regional enrichment, whereas colposcopy categories showed little obvious separation.
Among all variables displayed in the UMAP space, TBS diagnosis, histopathologic diagnosis, HPV diagnosis, and HPV genotype group showed the clearest structural differences. NILM and negative histopathology were widely distributed, whereas high-grade cytologic abnormalities and CIN2+ or invasive lesions were concentrated in more localized regions. HPV-negative cases showed a broad central distribution, while HPV-positive cases were more localized.
Discussion
The present study used data from 82,141 women participating in an organized cervical cancer screening programme in a prefecture-level city in Yunnan Province, China, to examine how demographic characteristics and routine screening indicators were associated with the final diagnosis of cervical precancer and cervical cancer. In descriptive analyses, positive and negative groups differed by age, ethnicity, educational level, gynecologic clinical findings, cytology, histopathology, HPV diagnosis, and HPV genotype group, whereas colposcopy categories showed no significant difference. After adjustment, HPV diagnosis showed the strongest association with the final diagnosis, while age, educational level, and gynecologic clinical findings also remained associated with the outcome; ethnicity was not significant as an overall variable. UMAP visualization further supported the clustering of higher-risk cases around HPV-related and high-grade cytological features. Taken together, these findings indicate that established screening indicators, particularly HPV testing and cytology, remain central to the screening-to-diagnosis pathway, while demographic factors may help identify population groups requiring closer follow-up support in a multi-ethnic regional screening setting.
Age showed a non-linear distribution in the descriptive analysis, with the highest positivity observed in women aged <25 years, relatively lower positivity in women aged 25–54 years, and a modest increase again in older age groups. This general pattern is broadly consistent with previous population-based studies reporting non-linear or U-shaped age distributions for HPV-related abnormalities.40–43 Prior evidence suggests that the early peak may reflect recent HPV acquisition after sexual debut and increased susceptibility of the cervical transformation zone in younger women.43–47 Because many newly acquired infections clear spontaneously within 1–2 years, and only a minority persist and progress to high-grade lesions or cancer higher positivity in younger women is more likely to reflect the detection of early abnormalities than a higher burden of invasive cervical cancer.48,49
The decline in positivity among women aged 25–54 years is likely multifactorial. First, HPV infection is typically self-limited, with most newly acquired infections becoming undetectable within approximately 1–2 years (apparent clearance).50,51 Second, new HPV acquisition is closely related to sexual exposure (eg, number of partners and partner change). As individuals enter midlife, incident exposure commonly decreases as partnership patterns become more stable, which further contributes to a reduced prevalent infection burden in the 25–54-year population.52,53 A rebound in positivity in women aged ≥65 years may reflect inadequate prior screening or prolonged under-screening after program exit, allowing persistent infection and/or precancerous lesions to remain undetected and accumulate at older ages. Therefore, screening discontinuation should not be determined by age alone but should consider an adequate negative screening history and risk stratification.54,55 Among women aged ≥55 years, evidence suggests that a negative HPV test provides more durable long-term reassurance than negative cytology alone, supporting HPV-based risk stratification when considering screening exit.56,57
In the multivariable model, age remained significant as an overall variable; however, only women aged 35–44 years had higher odds of a positive final diagnosis than those aged 45–54 years after adjustment, whereas the other age groups did not differ significantly. This suggests that the age-related variation observed in the descriptive analysis may partly reflect differences in HPV status and other screening indicators across age groups, rather than a simple independent effect of age.58 This interpretation is consistent with current risk-based approaches to cervical screening, which rely more directly on current HPV and cytology results and prior screening history than on age alone for risk estimation.59
Ethnicity-stratified analyses showed significant between-group differences in the composition of positive outcomes, with some minority groups, particularly Hani and Dai women, showing relatively higher positivity in the descriptive analysis. However, after adjustment in the multivariable model, ethnicity was not significant as an overall variable, although Dai women still had higher odds of a positive final diagnosis than Han women. This suggests that the ethnic differences observed in the descriptive analysis should not be interpreted simply as evidence of inherent biological susceptibility. Rather, they may reflect imbalances along the real-world screening cascade, including differences in screening entry, completion of triage referral, and follow-up adherence.
Real-world evidence from rural Yunnan suggests that screening coverage remains suboptimal, and that the acceptability of screening approaches is lower among minority populations, individuals with lower educational attainment, and those with limited screening-related knowledge, indicating that attrition may occur early at the screening entry stage and continue through follow-up completion.60–63 In addition, multiple studies and systematic reviews have shown that limited health literacy, shame and fear related to screening, cultural and language barriers, differences in trust in health services, and economic and geographic accessibility (costs, distance, and time opportunity costs) can reduce screening participation and increase loss to follow-up after abnormal results. This, in turn, contributes to under-screening or delays and a greater burden of positivity at the stage of diagnostic confirmation.64–67 Therefore, in multi-ethnic settings such as Yunnan, incorporating ethnicity into routine monitoring may be more useful as a service performance and accessibility indicator to identify underserved groups, pinpoint critical points of attrition, and guide resource prioritization and culturally adapted interventions. Furthermore, prior case–control evidence from Yunnan suggests that ethnicity-related differences often co-exist with socioeconomic factors such as medical payment/insurance patterns, supporting an interpretation based on “accessibility and adherence” considerations.68
In terms of educational attainment, the composition of positive outcomes declined progressively with increasing education, with the lowest positivity observed among individuals with college-level education or above. In the multivariable model, educational level remained significantly associated with a positive final diagnosis overall. Compared with individuals who were illiterate or had only primary school education, those with senior high school/vocational education and those with college-level education or above had significantly lower odds of a positive final diagnosis, whereas the association for junior high school was attenuated and did not reach conventional statistical significance. These results suggest that education-related attributes, including health literacy, risk awareness, and the capacity to navigate and utilize health services, may act as upstream determinants within the screening cascade by shaping proactive and regular participation in screening.69,70 Prior evidence indicates that higher educational attainment is associated with greater uptake of cervical cancer screening and HPV vaccination, whereas lower education is linked to under-screening or prolonged screening intervals, which may increase the likelihood that lesions are detected at subsequent screening visits.71 Population-based surveys further show that knowledge related to HPV, vaccination, and screening increases markedly with education level, implying that individuals with lower educational attainment are more likely to disengage at key points across the “screening, follow-up, and treatment” continuum.67,70,72
From the performance of individual indicators across the screening process, our findings were broadly consistent with previous studies and further suggested that different steps contributed unequally to the identification of positive outcomes.73 Routine gynecological clinical findings may show some association with positivity; however, precancerous lesions and early cervical cancer are often clinically silent, and a “normal” clinical examination does not exclude the risk of CIN2+ or AIS.74 Therefore, clinical findings are more appropriately regarded as supportive information for result interpretation rather than as a core screening modality.10 By contrast, cytological results classified according to the Bethesda System demonstrated a clearer graded relationship with positive outcomes, consistent with their established role in risk stratification and triage management.30,59 High-grade cytological abnormalities are more strongly suggestive of CIN2+/AIS, whereas low-grade abnormalities more often reflect early infection-related changes.75
No significant differences in the rate of positive final diagnoses were observed across colposcopic categories. This finding is not unexpected. Colposcopic interpretation is inherently influenced by examiner experience, lesion visibility, transformation zone type, as well as the number and location of biopsies obtained, and its sensitivity may decline further in postmenopausal women.76–78 At the same time, although colposcopic findings were included as analytical variables in the present study, more detailed information on standardized examination procedures, operator training and interobserver consistency assessment, and quality control measures was not available. Previous studies have shown that colposcopy is not a fully objective or uniformly reproducible examination; its interpretation is subject to interobserver variability, and differences among operators in biopsy number, biopsy site selection, and the use of additional endocervical sampling may further affect the detection of high-grade lesions.79–82 In particular, in older women, CIN2+ may be underestimated if assessment relies solely on colposcopy-directed biopsy results.80 Accordingly, colposcopy is better regarded as a tool for lesion localization and standardized biopsy guidance rather than as an independent predictor of risk. At the stage of diagnostic confirmation, histopathology remains the reference standard for the diagnosis of cervical precancerous lesions and cervical cancer, and in the present study it showed the greatest discriminatory capacity. This is also consistent with the natural history of cervical disease: CIN1 has a relatively high likelihood of spontaneous regression, whereas CIN2/3 and AIS carry a greater risk of persistence or progression.83 Future studies should include operator-level data and standardized colposcopy quality-control indicators to better assess and control for diagnostic variability.
Meanwhile, the strong association between HPV positivity, particularly HPV16/18, and positive outcomes further indicates the important role of HPV testing and genotyping in long-term risk assessment and subsequent triage.84,85 This is also consistent with the current evidence supporting HPV-based primary screening over cytology alone.86 Taken together, our findings suggest that, in cervical cancer screening, HPV testing, especially HPV16/18 genotyping, together with cytology, should serve as the main basis for risk assessment and decisions regarding subsequent evaluation.57,87,88 By contrast, demographic characteristics such as age, ethnicity, and educational attainment may be more useful for identifying differences in screening participation, follow-up adherence, and access to health services, and may therefore help inform subsequent intervention strategies.89
Although this study was based on real-world screening data and therefore captures population heterogeneity and screening practice under routine programme conditions, the findings should be interpreted with appropriate caution. First, all participants were drawn from a single region in Yunnan Province, China, where population structure, healthcare accessibility, and the organization of screening are region-specific; extrapolation to other settings or health systems may therefore be limited. Although multivariable logistic regression was performed to adjust for available covariates, prior screening history, health behaviour, socioeconomic status, and access to follow-up care could not be fully accounted for in the analysis. Second, we used a composite endpoint combining LSIL, HSIL/CIN2–3, AIS and invasive cervical cancer, which facilitates an overall description of abnormal burden but may be influenced by fluctuations in the detection of low-grade lesions. Future work should consider separating outcomes such as CIN2+, CIN3+ or AIS+ that are more closely aligned with intervention thresholds, in order to strengthen the interpretability of findings in terms of progression risk. Third, typical sources of bias in real-world research also apply here: individuals with abnormal results may not complete colposcopy/biopsy or guideline-concordant follow-up, and differences in access to referral, adherence, and sampling quality may lead to underestimation or overestimation of risk.
In conclusion, our results highlight two priorities for screening optimization. First, refined risk stratification based on age-specific HPV genotyping is necessary to balance the risk of over-referral in younger women against the need for rigorous assessment in older populations. Second, program improvements must focus on closing gaps in the diagnostic pathway by standardizing referral systems and providing navigation support for vulnerable groups (minority and low-education populations). These measures will enhance lesion detection, reduce missed diagnoses, and promote health equity across diverse subgroups.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this manuscript, the authors used ChatGPT-4o to optimize theEnglish language. After employing this tool, the authors carefully reviewed and edited the content as necessary and assume full responsibility for the final publication.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Qingshan Hai, upon reasonable request. The data are not publicly available because they contain information derived from a cervical cancer screening programme database and are subject to privacy and ethical restrictions.
Ethics Approval and Consent to Participate
The study design was approved by the Ethics Committee of Yunnan Provincial Hospital of Traditional Chinese Medicine (IRB number: 2024-KY-006-01). This study involved a secondary analysis of de-identified data from an existing cervical cancer screening programme database. Written informed consent had been obtained from participants during the original screening programme. This study was conducted in accordance with the Declaration of Helsinki, and all methods were performed in accordance with the relevant guidelines and regulations.
Acknowledgments
The authors wish to thank all of the participants involved in this study.
Funding
This study was supported by the Yunnan Provincial Science and Technology Plan Program (202401AZ070001-002) and the General Program of the Yunnan Provincial Department of Science and Technology (202101AZ070001-213).
Disclosure
The authors declare that they have no competing financial or personal relationships that could have influenced the work reported in this paper.
References
1. Cervical cancer; n.d. Available from: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer.
2. Lin KY, Lin IF, Wu PF, et al. Recommendations and guidance for human papillomavirus (HPV) vaccination for adults in Taiwan. J Microbiol Immunol Infect. 2025;58:383–16. doi:10.1016/j.jmii.2025.03.009
3. Cervical cancer causes, risk factors, and prevention - NCI; 2022. Available from: https://www.cancer.gov/types/cervical/causes-risk-prevention.
4. Boldeanu L, Assani M-Z, Boldeanu MV, et al. Cervical cancer in the era of HPV: translating molecular mechanisms into preventive public health action. Int J Mol Sci. 2025;26:8463. doi:10.3390/ijms26178463
5. Wu J, Jin Q, Zhang Y. Global burden of cervical cancer: current estimates, temporal trend and future projections based on the GLOBOCAN 2022. J Natl Cancer Center. 2025;5(3):322–329. doi:10.1016/j.jncc.2024.11.006
6. Osmani V, Hörner L, Nkurunziza T, Rank S, Tanaka LF, Klug SJ. Global prevalence of cervical human papillomavirus in women aged 50 years and older with normal cytology: a systematic review and meta-analysis. Lancet Microb. 2025;6. doi:10.1016/j.lanmic.2024.100955
7. Włoszek E, Krupa K, Skrok E, Budzik MP, Deptała A, Badowska-Kozakiewicz A. HPV and cervical cancer—biology, prevention, and treatment updates. Current Oncol. 2025;32:122. doi:10.3390/curroncol32030122
8. Falcaro M, Castañon A, Ndlela B, et al. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. Lancet. 2021;398(10316):2084–2092. doi:10.1016/S0140-6736(21)02178-4
9. Arbyn M, Xu L, Simoens C, Martin-Hirsch PP. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database Syst Rev. 2018;5. doi: 10.1002/14651858.CD009069.pub3
10. IARC, Cervical cancer screening; n.d. Available from: http://publications.iarc.who.int/Book-And-Report-Series/Iarc-Handbooks-Of-Cancer-Prevention/Cervical-Cancer-Screening-2022.
11. Bouvard V, Wentzensen N, Mackie A, et al. The IARC perspective on cervical cancer screening. N Engl J Med. 2021;385(20):1908–1918. doi:10.1056/NEJMsr2030640
12. Guo W, Hu Z, Yan J, et al. Epidemiological study of human papillomavirus infection in 105,679 women in wuhan, China. BMC Infect Dis. 2024;24(1):1111. doi:10.1186/s12879-024-10011-0
13. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries, CA Cancer J Clin. 2024;74:229–263. doi:10.3322/caac.21834
14. Zhang M, Zhong Y, Wang L, et al. Cervical cancer screening coverage — china, 2018–2019. China CDC Wkly. 2022;4:1077–1082. doi:10.46234/ccdcw2022.217
15. Zhao F, Lang J, Qiao Y, Zhu L. How can China achieve WHO’s 2030 targets for eliminating cervical cancer? BMJ. 2024;386:e078641. doi:10.1136/bmj-2023-078641
16. Zou Z, Fairley CK, Ong JJ, et al. Impact of achieving WHO’s 90-70-90 targets on cervical cancer elimination and potential benefits in preventing other HPV-related cancers in China: a modelling study. EClinicalMedicine. 2024;77:102878. doi:10.1016/j.eclinm.2024.102878
17. Zhang M, Wang L, Zhang X, et al. Cervical cancer screening rates among Chinese women — China, 2023–2024. CCDCW. 2025;7(10):321–326. doi:10.46234/ccdcw2025.052
18. Wu S, Jiao J, Yue X, Wang Y. Cervical cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with England and India based on the global burden of disease study 2019. Front Public Health. 2024;12. doi:10.3389/fpubh.2024.1358433
19. Liao Y, Zhu Q, Sun K, et al. Trends in the incidence, mortality and lifetime risks of female breast and cervical cancer - guangdong province, China, 2023. China CDC Wkly. 2025;7:940–946. doi:10.46234/ccdcw2025.157
20. Huang Y, Wei X, Guo Y, et al. Incidence, persistence, and clearance of cervical human papillomavirus infection among gynecological outpatients in kunming, yunnan, China, 2019–2023: a retrospective cohort study. PeerJ. 2025;13:e20215. doi:10.7717/peerj.20215
21. Zhao M, Gao M-Z, Gu R, et al. The risk of cervical cancer in women among han, bai, dai and hani ethnic minorities in yunnan province of China. Int J Womens Health. 2024;16:373–384. doi:10.2147/IJWH.S445471
22. Li Z, Liu F, Cheng S, et al. Prevalence of HPV infection among 28,457 Chinese women in yunnan province, southwest China. Sci Rep. 2016;6(1):21039. doi:10.1038/srep21039
23. Beijing Municipal Administration for Market Regulation. Specification for quality control of cervical cancer screening; n.d.
24. Li M, Wei L, Sui L. Guidelines for cervical cancer screening in China. Gynecol Obstetr Clin Med. 2023;3(4):189–194. doi:10.1016/j.gocm.2023.10.005
25. Zampaoglou E, Boureka E, Gounari E, et al. Screening for cervical cancer: a comprehensive review of guidelines. Cancers. 2025;17:2072. doi:10.3390/cancers17132072
26. Li M, Li J, Li X, et al. Guidelines for cervical cancer screening in China II. Gocm. 2025;5(2):e000205. doi:10.1136/gocm-2025-000205
27. World Health Organization. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention: Use of MRNA Tests for Human Papillomavirus (HPV).
28. World Health Organization. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention: Use of Dual-Stain Cytology to Triage Women After a Positive Test for Human Papillomavirus (HPV). Web annex C. Evidence-to-Decision Framework for Dual-Stain Cytology to Triage Women after a Positive Test for Human Papillomavirus (HPV). World Health Organization; 2024. doi:10.2471/B09020
29. Zhou X, Han T, Guo T, et al. Cervical intraepithelial neoplasia and cervical cancer in Hunan Province, China, 2020–2023. Front Oncol. 2024;14:1480983. doi:10.3389/fonc.2024.1480983
30. Wang T, Zhang H, Liu Y, Zhao C. Updates in cervical cancer screening guidelines, the Bethesda system for reporting cervical cytology, and clinical management recommendations. J Clin Transl Pathol. 2023;3:75–83. doi:10.14218/jctp.2023.00004
31. Li X, Xiang F, Dai J, et al. Prevalence of cervicovaginal human papillomavirus infection and genotype distribution in shanghai, China. Virol J. 2022;19:146. doi:10.1186/s12985-022-01879-y
32. Yu Y-Q, Jiang M-Y, Zhang X, et al. Effectiveness of high-risk human papillomavirus genotyping for cervical cancer screening. A multicentre screening cohort study in rural China. An Sist Sanit Navar. n.d.;47:e1065. doi:10.23938/ASSN.1065
33. Hanley SJB, Fujita H, Aoyama-Kikawa S. Noriaki, for the C. study Group, Evaluation of partial genotyping with HPV16/18 for triage of HPV positive, cytology negative women in the COMPACT study. J Gynecol Oncol. 2021;32(6). doi:10.3802/jgo.2021.32.e86
34. Alrajjal A, Pansare V, Choudhury MSR, Khan MYA, Shidham VB. Squamous intraepithelial lesions (SIL: LSIL, HSIL, ASCUS, ASC-H, LSIL-H) of uterine cervix and Bethesda system. Cytojournal. 2021;18:16. doi:10.25259/Cytojournal_24_2021
35. Pangarkar MA. The Bethesda system for reporting cervical cytology. Cytojournal. 2022;19:28. doi:10.25259/CMAS_03_07_2021
36. Nayar R, Wilbur DC. The Bethesda system for reporting cervical cytology: a historical perspective. Acta Cytol. 2017;61(4–5):359–372. doi:10.1159/000477556
37. Cervical screening programme: histopathology reporting handbook, GOV.UK; n.d. Available from: https://www.gov.uk/government/publications/cervical-screening-histopathology-reporting-handbook/cervical-screening-programme-histopathology-reporting-guidance.
38. Khieu M, Butler SL. High-grade squamous intraepithelial lesion of the cervix. In: StatPearls. Treasure Island (FL):StatPearls Publishing;2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK430728/.
39. Simonella LM, Lewis H, Smith M, Neal H, Bromhead C, Canfell K. Type-specific oncogenic human papillomavirus infection in high grade cervical disease in New Zealand. BMC Infect Dis. 2013;13(1):114. doi:10.1186/1471-2334-13-114
40. Zhu L, Li P, Wang Y, et al. The relationship between human papillomavirus genotype distribution and age and the association with high-grade squamous intraepithelial lesions of the cervix or cervical cancer in jilin province, China. Virol J. 2025;22:380. doi:10.1186/s12985-025-02963-9
41. Chen L, Zhu K, Chen H, et al. Correlation of immediate prevalence of cervical squamous cell precancers and cancers with HPV genotype and age in women with LSIL cytology: a retrospective analysis of 1617 cases. Diagn Cytopathol. 2024;52(1):10–15. doi:10.1002/dc.25229
42. Zhang J, Zha T, Wang X, He W. Prevalence and genotype distribution of HPV infections among women in Chengdu, China. Virol J. 2024;21(1):52. doi:10.1186/s12985-024-02317-x
43. Chen M, Lhamo Y, Chödrön K, Chen L. High-risk human papillomavirus (hr-HPV) prevalence and abnormal cervical cytology in rural high-altitude communities: a population-based cross-sectional study in the southern Tibetan Plateau, China (2023–2024). Virol J. 2025;22(1):279. doi:10.1186/s12985-025-02909-1
44. Smith JS, Melendy A, Rana RK, Pimenta JM. Age-specific prevalence of infection with human papillomavirus in females: a global review. J Adolesc Health off Publ Soc Adolesc Med. 2008;43:S5–S25, S25.e1–41. doi:10.1016/j.jadohealth.2008.07.009
45. Franceschi S, Herrero R, Clifford GM, et al. Variations in the age-specific curves of human papillomavirus prevalence in women worldwide. Int J Cancer. 2006;119(11):2677–2684. doi:10.1002/ijc.22241
46. Houlihan CF, Baisley K, Bravo IG, et al. Rapid acquisition of HPV around the time of sexual debut in adolescent girls in Tanzania. Int J Epidemiol. 2016;45(3):762–773. doi:10.1093/ije/dyv367
47. Aiyenuro A, Griffin H, Schichl K. Role of reserve cells in metaplasia and the development of human papillomavirus–associated high-grade squamous intraepithelial lesions at the cervical transformation zone. Lab Invest. 2025;105(7):104166. doi:10.1016/j.labinv.2025.104166
48. Tessandier N, Elie B, Boué V, et al. Viral and immune dynamics of genital human papillomavirus infections in young women with high temporal resolution. PLoS Biol. 2025;23(1):e3002949. doi:10.1371/journal.pbio.3002949
49. Bruno MT, Pagana A, Giudice CL, Panella MM, Mascellino G, Laganà AS. CIN2 in the era of risk-based management and HPV vaccination: epidemiology, natural history and guidelines. Diagnostics. 2025;15(19):2512. doi:10.3390/diagnostics15192512
50. McGee AE, Hawco S, Bhattacharya S, Hanley SJB, Cruickshank ME. Alternatives to surveillance for persistent human papillomavirus after a positive cervical screen: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2024;302:332–338. doi:10.1016/j.ejogrb.2024.09.019
51. Sierra MS, Carvajal LJ, Dull P. Human papillomavirus type 16 and 18 viral clearance and progression to precancer among women aged 18–25 years enrolled in the Costa Rica HPV prophylactic vaccine trial (CVT). Vaccine. 2025;50:126841. doi:10.1016/j.vaccine.2025.126841
52. Del Pino M, Vorsters A, Joura EA, et al. Risk factors for human papillomavirus infection and disease: a targeted literature summary. J Med Virol. 2024;96(2):e29420. doi:10.1002/jmv.29420
53. Hu J-P, Wang J-L, Li Y, et al. Trends in the molecular epidemiology of human papillomavirus in males from the plateau region of southwest China: an 11-year retrospective analysis (2014–2024). Virol J. 2025;22(1):238. doi:10.1186/s12985-025-02861-0
54. Tranberg M, Petersen LK, Hammer A, et al. Value of a catch-up HPV test in women aged 65 and above: a Danish population-based nonrandomized intervention study. PLoS Med. 2023;20(7):e1004253. doi:10.1371/journal.pmed.1004253
55. Santos N, Kim J, Hsu K, et al. Association between age and race and cervical cancer stage. O G OPEN. 2025;2(6):e138. doi:10.1097/og9.0000000000000138
56. Cervical cancer screening guidelines; n.d. Available from: https://www.cancer.org/cancer/types/cervical-cancer/detection-diagnosis-staging/cervical-cancer-screening-guidelines.html.
57. Wang J, Elfström KM, Dillner J. Human papillomavirus-based cervical screening and long-term cervical cancer risk: a randomised health-care policy trial in Sweden. Lancet Public Health. 2024;9(11):e886–e895. doi:10.1016/S2468-2667(24)00218-4
58. Gage JC, Katki HA, Schiffman M, et al. Age-stratified 5-year risks of cervical precancer among women with enrollment and newly detected HPV infection. Int J Cancer J Int Du Cancer. 2015;136(7):1665–1671. doi:10.1002/ijc.29143
59. Perkins RB, Guido RS, Castle PE, et al. ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24(2):102–131. doi:10.1097/LGT.0000000000000525
60. Duan R, Yang H, Zhai X, et al. Accuracy and acceptability of self-sampling HPV testing in cervical cancer screening: a population-based study in rural yunnan, China. Sci Rep. 2025;15(1):26390. doi:10.1038/s41598-025-09292-5
61. Zhai X, Kong T, Yang X, et al. Clinical performance of triage strategies for HPV-positive women in cervical cancer screening in rural yunnan China. BMC Cancer. 2025;26(1):57. doi:10.1186/s12885-025-15375-3
62. Garcia A, Juarez M, Sacuj N, et al. Loss to follow-up and the care cascade for cervical cancer care in rural Guatemala: a cross-sectional study. JCO Glob Oncol. 2022;8(8):e2100286. doi:10.1200/GO.21.00286
63. Liu Y, Guo J, Zhu G, Zhang B, Feng XL. Changes in rate and socioeconomic inequality of cervical cancer screening in northeastern China from 2013 to 2018. Front Med. 2022;9. doi:10.3389/fmed.2022.913361
64. Farajimakin O. Barriers to cervical cancer screening: a systematic review. Cureus. n.d.;16:e65555. doi:10.7759/cureus.65555
65. Srinath A, van Merode F, Rao SV, Pavlova M. Barriers to cervical cancer and breast cancer screening uptake in low- and middle-income countries: a systematic review. Health Policy Plan. 2023;38(4):509–527. doi:10.1093/heapol/czac104
66. Olthof EMG, Aitken CA, Siebers AG, van Kemenade FJ, de Kok IMCM. The impact of loss to follow-up in the Dutch organised HPV-based cervical cancer screening programme. Int J Cancer. 2024;154(12):2132–2141. doi:10.1002/ijc.34902
67. Martinez-Gutierrez J, Chima S, Boyd L, et al. Failure to follow up abnormal test results associated with cervical cancer in primary and ambulatory care: a systematic review. BMC Cancer. 2023;23(1):653. doi:10.1186/s12885-023-11082-z
68. Zhao M, Gu R, Ding S, et al. Risk factors of cervical cancer among ethnic minorities in yunnan province, China: a case–control study. Eur J Cancer Prev. 2022;31(3):287–292. doi:10.1097/CEJ.0000000000000704
69. Dema E, Osman R, Soldan K, Field N, Sonnenberg P. Are there any sociodemographic factors associated with non-uptake of HPV vaccination of girls in high-income countries with school-based vaccination programmes? A systematic review. J Epidemiol Community Health. 2025;79(5):388–396. doi:10.1136/jech-2024-222488
70. Gao D, Wang X, Juan J, Pei Z, Zhang X. Association between knowledge of cervical cancer prevention and screening behaviors among women aged 20 to 49 years: a cross-sectional study in six provinces, China. BMC Public Health. 2025;25(1):1821. doi:10.1186/s12889-025-22971-2
71. Murfin J, Irvine F, Meechan-Rogers R, Swift A. Education, income and occupation and their influence on the uptake of cervical cancer prevention strategies: a systematic review. J Clin Nurs. 2020;29(3–4):393–415. doi:10.1111/jocn.15094
72. Stephens ES, Dema E, McGee-Avila JK, Shiels MS, Kreimer AR, Shing JZ. Human papillomavirus awareness by educational level and by race and ethnicity. JAMA Network Open. 2023;6(11):e2343325. doi:10.1001/jamanetworkopen.2023.43325
73. I.W.G. on the E. of C.-P. Interventions, Preventive and adverse effects of cervical cancer screening. In: Cervical Cancer Screening. International Agency for Research on Cancer; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK601985/.
74. Reed N, Balega J, Barwick T, et al. British gynaecological cancer society (BGCS) cervical cancer guidelines: recommendations for practice. Eur J Obstet Gynecol Reprod Biol. 2021;256:433–465. doi:10.1016/j.ejogrb.2020.08.020
75. Bruno MT, Cavallaro AG, Sudano MC, et al. Role of endocervical curettage in detecting CIN2 + in postmenopausal women with persistent high-risk HPV and type 3 transformation zone. BMC Cancer. 2025;25(1):1486. doi:10.1186/s12885-025-14868-5
76. Chu Y, Chen Q, Liu R, et al. Analysis of factors affecting the accuracy of colposcopic diagnosis of cervical lesions: a retrospective cohort study. Front Med. 2024;11:1462079. doi:10.3389/fmed.2024.1462079
77. Bertelsen VM, Tranberg M, Petersen LK, Booth B, Bor P. Improving diagnostic of cervical dysplasia among postmenopausal women aged ≥50 years using local vaginal oestrogen treatment prior to colposcopy: study protocol for a multicentre randomised controlled trial (the IDEAL study). BMJ Open. 2024;14(6):e082833. doi:10.1136/bmjopen-2023-082833
78. McGee AE, Alibegashvili T, Elfgren K. European consensus statement on expert colposcopy. Eur J Obstet Gynecol Reprod Biol. 2023;290:27–37. doi:10.1016/j.ejogrb.2023.08.369
79. Schiffman M, Wentzensen N. Issues in optimising and standardising the accuracy and utility of the colposcopic examination in the HPV era. Ecancermedicalscience. 2015;9:530. doi:10.3332/ecancer.2015.530
80. Gustafson LW, Hammer A, Bennetsen MH, et al. Cervical intraepithelial neoplasia in women with transformation zone type 3: cervical biopsy versus large loop excision. BJOG. 2022;129(13):2132–2140. doi:10.1111/1471-0528.17200
81. Petry KU, Nieminen PJ, Leeson SC, Bergeron COMA, Redman CWE. 2017 update of the European federation for colposcopy (EFC) performance standards for the practice of colposcopy. Eur J Obstet Gynecol Reprod Biol. 2018;224:137–141. doi:10.1016/j.ejogrb.2018.03.024
82. Massad LS, Perkins RB, Naresh A, et al. Colposcopy standards: guidelines for endocervical curettage at colposcopy. J Low Genit Tract Dis. 2023;27(1):97–101. doi:10.1097/LGT.0000000000000710
83. Gisca T, Munteanu I-V, Vasilache I-A, et al. A prospective study on the progression, recurrence, and regression of cervical lesions: assessing various screening approaches. J Clin Med. 2024;13(5):1368. doi:10.3390/jcm13051368
84. Massad LS, Clarke MA, Perkins RB, et al. Applying results of extended genotyping to management of positive cervicovaginal human papillomavirus test results: enduring guidelines. J Low Genit Tract Dis. 2025;29(2):134–143. doi:10.1097/LGT.0000000000000865
85. Damgaard RK, Jenkins D, Stoler MH. Human papillomavirus genotypes and risk of persistence and progression in women undergoing active surveillance for cervical intraepithelial neoplasia grade 2. Am J Obstet Gynecol. 2024;230(6):655.e1–655.e10. doi:10.1016/j.ajog.2024.01.029
86. Vahteristo M, Leinonen MK, Sarkeala T, Anttila A, Heinävaara S. Similar effectiveness with primary HPV and cytology screening - long-term follow-up of randomized cervical cancer screening trial. Gynecol Oncol. 2024;180:146–151. doi:10.1016/j.ygyno.2023.11.036
87. Thrall MJ, McCarthy E, Mito JK, Rao J. Triage options for positive high-risk HPV results from HPV-based cervical cancer screening: a review of the potential alternatives to papanicolaou test cytology. J Am Soc Cytopathol. 2025;14(1):11–22. doi:10.1016/j.jasc.2024.09.003
88. Stoler MH, Parvu V, Yanson K, Andrews J, Vaughan L. Risk stratification of HPV-positive results using extended genotyping and cytology: data from the baseline phase of the onclarity trial. Gynecol Oncol. 2023;174:68–75. doi:10.1016/j.ygyno.2023.04.022
89. Spencer JC, Kim JJ, Tiro JA, et al. Racial and ethnic disparities in cervical cancer screening from three U.S. healthcare settings. Am J Prev Med. 2023;65(4):667–677. doi:10.1016/j.amepre.2023.04.016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cervical Cancer Screening in Transition: Global Challenges and Local Realities
Rakhat A, Aimagambetova G
International Journal of Women's Health 2026, 18:607741
Published Date: 2 July 2026