Back to Journals » International Journal of Women's Health » Volume 18
Cervical Cancer Screening in Transition: Global Challenges and Local Realities
Authors Rakhat A ![]() , Aimagambetova G
, Aimagambetova G ![]()
Received 8 March 2026
Accepted for publication 27 May 2026
Published 2 July 2026 Volume 2026:18 607741
DOI https://doi.org/10.2147/IJWH.S607741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Altynshash Rakhat,1 Gulzhanat Aimagambetova2,3
1School of Medicine, Nazarbayev University, Astana, 010000, Kazakhstan; 2Department of Surgery, School of Medicine, Nazarbayev University, Astana, 010000, Kazakhstan; 3Clinical Academic Department of Women’s Health, CF “University Medical Center”, Astana, 10000, Kazakhstan
Correspondence: Gulzhanat Aimagambetova, Department of Surgery, Nazarbayev University School of Medicine, Kabanbay Batyr 53, Astana, 010000, Kazakhstan, Email [email protected]
Abstract: Cervical cancer remains a major global public health concern that disproportionally affects women in low- and middle-income countries (LMICs), despite being largely preventable through effective primary and secondary prophylaxis. Persistent infection with high-risk human papillomavirus (HPV) is the principal cause of cervical cancer, highlighting the importance of both HPV vaccination and HPV-based screening. This narrative review examines current evidence on the natural history, prevention, and epidemiology of cervical cancer, with particular emphasis on screening practices and emerging innovative methods. It highlights the global patterns in cervical cancer incidence and mortality and provides regional contexts with the specific focus on the evolution of cervical cancer screening techniques, including cytology-based methods, HPV DNA testing, and the increasing role of self-sampling approach. Future perspectives are discussed in relation to the World Health Organization’s cervical cancer elimination strategy.
Keywords:
cervical cancer, HPV, HPV vaccination, cervical cancer screening, Pap test, HPV genotyping, self-sampling, prevention, healthcare access
Introduction
Cervical cancer remains a major public health burden and stands as one of the most common cancers affecting women worldwide and disproportionately impacts low- and middle-income countries (LMICs).1,2 Cervical cancer is widely recognized as one of the most preventable diseases since it has a well-proven and essential causal agent, persistent infection with high-risk human papillomavirus (HPV).1,3,4 The connection between cervical cancer and carcinogenic HPV types establishes that existing prevention methods succeed in discontinuing the disease progression before patients develop invasive cancer.5–7 The natural history of this disease provides two prevention methods: HPV vaccination reduces the risk of oncogenic type infection, while screening, together with early treatment, enables healthcare professionals to find and treat precancerous conditions.8,9 The worldwide distribution of preventive healthcare services remains highly unequal; therefore, women in LMICs continue to experience greater disease burden.3,6
The existing health gaps show that people lack access to essential preventive services, which include HPV vaccination, organized cervical cancer screening procedures, and immediate diagnosis and treatment. Screening effectiveness depends on test performance and delivery systems, and follow-up pathways and population participation; therefore, officials need to conduct discussions about which screening methods to use and how to implement those methods for elimination efforts.10–13The implementation of screening methods through organized population-based programs has demonstrated strong evidence that screening methods like cytology and visual inspection with acetic acid and hrHPV testing can reduce both cervical cancer rates and cancer-related deaths.9,14–16
To prevent cervical cancer and decrease the incidence of the disease, the World Health Organization (WHO) developed the Global Strategy to Accelerate the Elimination of Cervical Cancer.6 The strategy aims for (1) 90% of girls to be fully vaccinated against HPV by age 15, (2) 70% of women to undergo high-performance test screening at least twice during their lifetime (by ages 35 and 45), and (3) 90% of women with cervical disease to receive suitable medical care and treatment.6 However, the progress toward these objectives has not been distributed equally among different groups/countries. Fewer than half of the countries in the world have created systematic screening programs, and global HPV vaccine coverage remains low.17–19 The existing gaps demonstrate that organizations need to develop both effective technologies and implementation methods that will improve their service delivery to different communities.
This narrative review summarizes the most recent research on preventing cervical cancer by focusing on screening methods and ongoing debates, as well as up-to-date solutions, which include HPV self-sampling. The study evaluates worldwide advancements in cervical cancer screening, comparing them to local/regional screening systems to identify potential improvements and existing obstacles, and future development routes needed to achieve the WHO cervical cancer elimination targets.
Materials and Methods
Literature Search
This narrative review used a structured literature search and transparent study-selection, guided by PRISMA guidelines for transparency, and included peer-reviewed articles published in English for the period between January 2016 and February 2026. Major available electronic databases were searched, including PubMed/MEDLINE, Cochrane database, and Google Scholar. In addition, the study examined key international guidelines and policy documents from organizations such as the WHO, the American Society of Clinical Oncology (ASCO), the American Cancer Society (ACS), the National Cancer Institute (NCI), and the European Commission Joint Research Centre (ECJRC). Reference lists of included papers were used to discover additional relevant sources.
The search was performed using the following keywords: “cervical cancer” “human papillomavirus” “HPV” “high-risk HPV” “screening” “HPV testing” “primary HPV screening” “cytology” “Pap test” “visual inspection with acetic acid” “VIA” “HPV genotyping” “self-sampling” “self-collection” “HPV vaccination” “screening guidelines” “screening coverage” “healthcare access”. Medical Subject Headings (MeSH) terms were used wherever available: “Uterine Cervical Neoplasms” (MeSH Unique ID: D002583), “Papillomavirus Infections” (MeSH Unique ID: D030361), “Mass Screening” (MeSH Unique ID: D008403), “Early Detection of Cancer” (MeSH Unique ID: D055088), “Papanicolaou Test” (MeSH Unique ID: D065006), and “Papillomavirus Vaccines” (MeSH Unique ID: D053918).
The search was specified and targeted by using (“Uterine Cervical Neoplasms” OR “cervical cancer”) AND (“Papillomavirus Infections” OR “human papillomavirus” OR HPV OR “high-risk HPV”) AND (“Mass Screening” OR screening OR “HPV testing” OR cytology OR “Pap test” OR VIA OR “HPV genotyping”) AND (“self-sampling” OR “self-collection”) AND (“HPV vaccination” OR “Papillomavirus Vaccines”) (Supplementary Table S1).
Inclusion and Exclusion Criteria
Original studies, previously published reviews, guidelines, and policy documents were identified using the predefined keywords and search combinations and were considered for inclusion in this narrative review. Inclusion criteria were articles published in English between January 2016 and February 2026 (the literature search period) and addressing cervical cancer epidemiology, HPV infection, cervical cancer prevention, screening modalities (cytology, visual inspection with acetic acid, HPV testing, genotyping, self-sampling), vaccination, screening implementation, or issues of access and equity.
Both authors independently searched and screened titles and abstracts to identify relevant studies. Duplicates and irrelevant records were excluded. Full texts of potentially eligible articles were then assessed for inclusion. Due to heterogeneity across studies, findings were synthesized narratively rather than quantitatively.
Overall, 231 studies were included in this review (Figure 1).
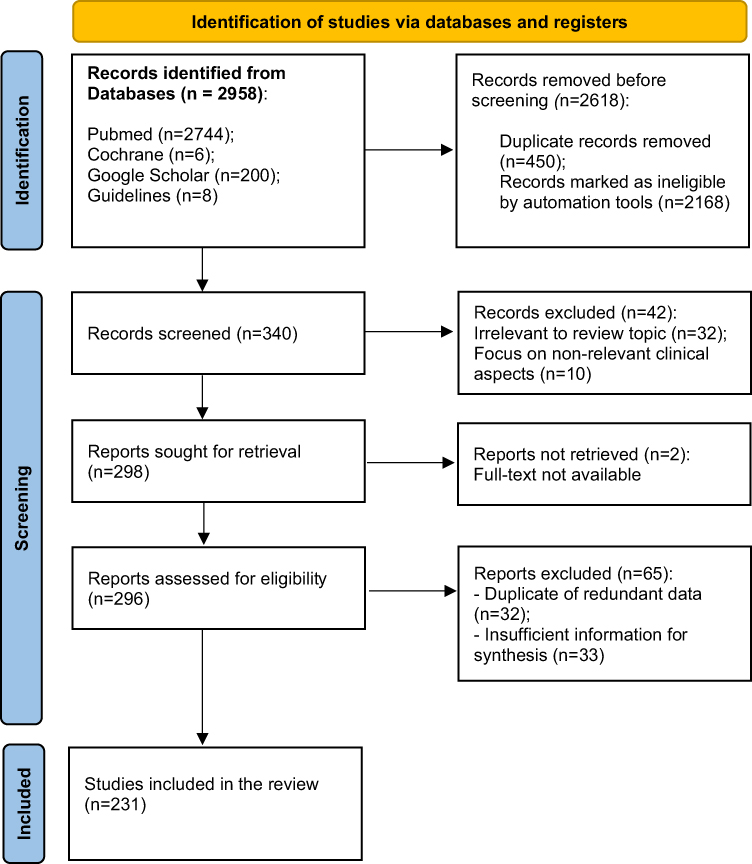 |
Figure 1 Data extraction flowchart. |
Results and Discussion
Definition and Global Epidemiology
Cervical cancer (International Diseases Classification 10th edition code C53) is a malignant tumor originating in the uterine cervix.20 The primary cause is a persistent infection with the high-risk HPV types, particularly HPV-16 and HPV-18, which together account for around 70% of the cases of cervical cancer globally.13,21,22 The squamous epithelial cells of the cervix, which are the most predominant ones, are the main target of the HPV infection.20 The cellular alterations in the cervix are caused by a persistent infection with the high-risk HPV strains, which can lead to the gradual invasion of cancerous cells from precancerous lesions in the uterine cervix.23,24 Besides, cervical cancer can also be triggered by a combination of risk factors like smoking, HIV infection, early sexual debut, contraceptive pill usage, and multiple sexual partners.1,13
Cervical cancer, with large geographical differences in both incidence and mortality, remains a global public health issue of great importance.25,26 The GLOBOCAN estimates indicated that globally, there were around 703,000 new cervical cancer cases and 373,000 deaths caused by the disease in 2025, making it the fourth most common type of cancer among women.27 Of all global cervical cancer cases, about 85% occur in LMICs.27,28 The high incidence of cervical cancer prevailing in LMICs is largely due to limited access to preventive measures, such as HPV vaccination, cervical cancer screening, and adequate, prompt, and targeted treatment.6
The geographical diversity of the rates of cervical cancer continues to be very different with countries within the regions of Eastern, Southern, and Sub-Saharan Africa reported to have the highest age-standardized incidence rate (ASIR) in 2022 with the highest ASIR in Eastern Africa being 40.42 per 100,000 women, and Southern Africa being 34.89 per 100,000 women, with the ASIR in Middle Africa of 31.12 per 100,000 women.29 Eastern Africa also reported an age-standard mortality rate (ASMR) of 28.87 per 100,000 women, the highest rate of cervical cancer mortality among different regions.27,29–31 Countries, including Eswatini, Malawi, and Zambia, have the highest rates of mortality, with Eswatini reporting an ASMR of 64.3 per 100,000 because of the lack of access to preventative services such as the HPV vaccine, other forms of preventative HPV vaccination, or cervical cancer screening, resulting in extreme late-stage diagnosis and poor treatment outcomes.29,32
In contrast, Western Europe and Australia, where healthcare systems have matured to support preventive care programs and services, have significantly lower rates of cervical cancer incidence and mortality than Eastern Africa, where Western Europe’s ASMR rate stands at 2.0 per 100,000 women compared to 28.6 per 100,000 women for Eastern Africa.29,33–36 The large gap illustrates the importance of early detection, vaccination, and screening initiatives in reducing cervical cancer deaths. The differences in the incidence of cervical cancer and its subsequent societal impact necessitate international efforts to implement effective cervical cancer prevention technology, particularly in low-resource countries, to help eliminate the global burden of cervical cancer.37,38
In countries that have high human development indices (HDI), the rate of cervical cancer usually starts increasing around the age of 25, and then it goes up to the maximum level around 40. However, in places where the economy is lowest or just below the middle-class level, the incidence keeps rising until women get to the age of their 50s or 60s.39 Besides this, the geographic distribution of cervical cancer risk differs a lot across the world; for instance, in Eswatini, a woman’s lifetime chance of developing cervical cancer is estimated to be 8.6%, but in Egypt, it’s merely 0.3%.21,40 Such disparities are indicative of differences in health systems and the availability of screening, as well as different levels of HPV infection and concurrent sexually transmitted diseases that may influence the long-term HPV persistence. Cancers of the breast and of the cervix together are responsible for around the same number of deaths among women aged 15 to 44 years, the former being the leading one.39,41 They, thus, severely affect the health of women in lower-middle-income and low-income countries through early mortality.
High-risk HPV strains persistently infecting the cervix are a very significant factor in the occurrence of cervical cancer. Almost all cervical cancer cases worldwide are caused by HPV type 16 or 18, and are supplemented with HPV types 31, 33, 45, 52, and 58, which alone represent 18% of the incidence of cervical cancer.42–44 Globally, it is estimated that 15.3% of women are infected with one or more high-risk HPV strains, indicating that HPV infection is very common.42,43 Also, Hispanic women living in the Caribbean region had the highest prevalence of HPV (50.7%), while women in Southern Asia had the lowest (8.5%).42,43 While younger women are the age group with the highest incidence of HPV infection, women aged over 40 have an increased incidence of HPV infections for an additional surge typically found in resource-poor settings.42–44 Persistent HPV infection, typically defined as detection of the same high-risk HPV type for 12 months or longer, is responsible for most cases of cervical precancer and cervical cancer.45
Projected population growth and aging in LMICs are expected to contribute to an increase of 32% in new cervical cancer cases, as well as an increase of 41% in cervical cancer deaths worldwide by the year 2040.46 However, the incidence and mortality estimates for the global cervical cancer epidemic could be dramatically decreased through vaccination against HPV and screening programs.
Thus, the WHO has established a series of ambitious goals to eliminate cervical cancer as a global health concern by the year 2030, 90–70-90 program.47 If the program initiatives are successfully executed, there is the potential to drastically reduce the occurrence and mortality associated with cervical cancer worldwide.
Etiology: High-Risk Human Papillomavirus
The high-risk HPV infection is responsible for creating the environment in which cervical cancer occurs. The HPV infection DNA is present in more than 95% of cervical carcinomas, indicating that hrHPV is an etiologic precondition for practically all cases of cervical cancer worldwide.29,48–52
HPV vaccines and HPV DNA-based primary cervical cancer screening are the most recent public health strategies employed for the prevention of cervical cancer based upon hrHPV’s role as the causative agent of cervical cancer.51,52 High-risk HPV mainly infects the transformation zone (TZ) of the uterine cervix, which is the area that sees the intersection of viral persistence, neoplastic change, and screening practices, thereby making it the primary location for both virus invasion and precancerous lesions’ development.13,53
The HPV is a small, non-enveloped virus that contains a double-stranded circular DNA of approximately 8 kb.13 The early and late genes are located on the same coding strand of the HPV genome, with six of the early genes (E1-E7) and two late genes (L1 and L2) encoding proteins that regulate the synthesis of HPV proteins during the lytic stage of replication and their preservation through an intermediate period.13,54–57 Additionally, the late gene proteins make up both the major and minor capsids that form the HPV virion.58 Currently, over 200 distinct HPV genotypes exist.13,59 These are classified into different genera and species depending on the types of tissues affected, the degree to which they share sequence-relatedness with each other, and their cancer-causing ability.58,60
From an oncological perspective, most malignancies in the cervix in women are caused by a limited number of mucosotropic alpha-HPV strains. Twelve genotypes at least are classified by the International Agency for Research on Cancer (IARC) as group 1 carcinogens, which include HPV-16, −18, −31, −33, −35, −39, −45, −51, −52, −56, −58, and −59.13,61–64 In a general series of large numbers of cases, approximately 60% of squamous cell carcinomas (SCCs) are attributed solely to HPV-16.65 Also, many adenocarcinomas (ADCs) as well as sections of SCCs can be attributed to both HPV-18 and HPV-45 together.66,67 Collectively, HPV-16 and HPV-18 are estimated to cause around 70–75% of all cervical cancer cases worldwide.23,68,69 Other hrHPV types (31, 33, 52, and 58) provide smaller but regionally variable amounts of causal contributions to the overall numbers of cases.70,71
Cervical Microanatomy and Site of High-Risk HPV Carcinogenesis
Anatomically, the cervix consists of the stratified squamous epithelium of the ectocervix and the columnar glandular epithelium of the endocervix.20 The squamocolumnar junction (SCJ), where these epithelia meet, undergoes squamous metaplasia over the life span, which gives rise to a dynamic transformation zone characterized by the replacement of glandular epithelium with immature metaplastic cells.72–74 Among the progenitor cells in this TZ, especially those with long life span, are those that are highly susceptible to malignant transformation and hrHPV infection.75,76
Precancerous (precursor) lesions, known as cervical intraepithelial neoplasia (CIN), develop in the TZ, which is the most susceptible area.13,72 Due to the vulnerability of the cervical TZ at a younger age, the risk of cervical precancerous lesions and cervical cancer increases if the hrHPV infection is caught at a younger age and persists longer than 24 months.13,72 Early sexual debut and multiple sexual partners are considered risk factors for cervical cancer development.
The revised Bethesda Classification defines CIN I as a low-grade squamous intraepithelial lesion (LSIL), while CIN II and III are classified as high-grade squamous intraepithelial lesions (HSIL).77–80 The cytological numbers in the cervix that are often scratched (micro-abrasions) during intercourse commonly lead to the HPV virus getting into the deeper (basal or parabasal) cells.81–83 The clinician could face different hrHPV-induced clones with diverse lesion grades at the same time, and TZ infections are mostly multifocal. For optimal screening, good access to the TZ is necessary for proper sampling.83 The TZ location slowly moves toward the endocervical canal as a person ages, thus influencing the effectiveness of some screening methods.53
Natural History of High-Risk HPV Infection and Multistage Cervical Carcinogenesis
The occurrence of cervical cancer is directly associated with long-lasting infection with the carcinogenic types of HPV, which indicates that hrHPV is the key factor leading to cervical cancer.13,72,84 The prevalence of HPV infections may be high, but the occurrence of malignant transformation is relatively low, as in most cases the host immune response clears the infection within 12–24 months.13 This means that there will never be a shortage of women who will continue to have multiple concurrent and/or sequential HPV infections cleared from their bodies, but there may be a lot of women who will not be able to control one specific persistent HPV infection that eventually leads to cancer.83–85
The development of cervical cancer is a multistage process that is very clear and takes several years to decades. It starts with a non-infected cervix, progresses through hrHPV type-specific infection, precancerous cervical lesions (CIN 1, CIN2, CIN3), and finally results in invasive carcinoma.72,85,86 The transitions between these states are not constant, and at the beginning, they can even be reversed, while the presence and disappearance of HPV can mean a new infection, a weakened immune system, or revival of a dormant infection.13,72 All these processes are indistinguishable by the current tests.86–89
HPV primarily transmits via sexual activities, encompassing non-penetrative genital contact, meaning that general trends in sexual initiation affect the usual start of cervical cancer development.90 Longitudinal cohort studies consistently demonstrate a notable increase in new HPV infections shortly after sexual debut, confirming HPV as the most common sexually transmitted infection among young women.90–93
The natural progression of HPV infection is characterized more by clearance than by persistence, even though it occurs frequently. In immunocompetent females, more than 70% of hrHPV infections remain undiagnosed within a year, and nearly 90% resolve within two to three years.92–94 Genotypes and age categories exhibit similar clearance trends, emphasizing persistence over acquisition frequency as the main factor affecting cancer risk.93
This biological mechanism clarifies why, despite a high prevalence of HPV, aggressive cervical cancer is relatively rare in women younger than 25.95 Moreover, histologically confirmed CIN2 lesions in young women and girls frequently resolve on their own, showing spontaneous regression rates of nearly 60% within three years, which bolsters conservative treatment strategies for this age group.72,87,95,96
Conversely, a small but clinically relevant high-risk subgroup has been identified as a result of repeated findings of the same hrHPV genotype over the course of multiple screening cycles. Longitudinal studies have shown that persistence of hrHPV, particularly for the hrHPV type HPV-16 and an increased level of viral load (increased amount of virus present), serves as a significant risk factor for progression to CIN2/3 and adenocarcinoma in situ.93,97,98 After five years, there are only a limited number of carcinogenic hrHPV infections that will still be detectable; the majority either did not progress or resolved.93
Molecular Transition from Productive Infection to Transforming Disease
Most HPV infections go through a productive life cycle at the molecular level, which means that virus genomes persist in basal epithelial cells as episomes with a very limited gene expression.13 When the infected cells mature and move to the surface of the epithelium, late viral genes are expressed, new virions are made, and infectious particles are released without the bacteria being integrated into the host genome.73,86 Typically, these kinds of infections are self-limiting and clinically silent.
The development of cervical cancer is associated with persistent hrHPV infection progressing from the early phases to the later stages of viral carcinogenesis, characterized by uncontrolled overexpression of the virus oncogenes E6 and E7.72,84,99 E6 promotes the degradation of the p53 tumor suppressor protein, preventing the induction of DNA damage response and apoptosis by E7 and p53.13,72 E7 binds to the retinoblastoma protein and releases E2F factors, causing unscheduled activation of cell-cycle progression.100,101 The combined effect of these two events disrupts normal cell-cycle regulation, leading to a greater chance of genetic instability and subsequent development of oncogenic changes.
The molecular mechanisms described correlate with the progression of high-grade squamous intraepithelial lesions (HSIL/CIN2-3) and their cellular morphology.13,102 Increased expression of p16INK4a combined with Ki-67 provides an excellent biomarker profile for distinguishing between transforming lesions and transient infections.103–105 Without intervention, many high-grade lesions will develop into invasive carcinoma over a period of years. The type of HPV is a large determining factor in the rate at which a high-grade lesion will progress to an invasive carcinoma, with HPV16 being the largest factor.93
Modifiers of Persistence and Progression
The host and environmental factors impact the risk of hrHPV cervical cancer infection. And these factors are mainly smoking, high parity, long-term use of hormonal contraceptives, and early sexual debut, which each slightly increase the risk of progression.84,106 Immunosuppression is a modulator that becomes particularly important, especially when considering the fact that women with HIV have higher rates of HPV, more frequent infections with multiple types, and quicker progression to CIN3 and invasive cancer.13,72,107
The findings related to biological research are the foundation of strategies for preventing the disease. Young women tend to have higher rates of the spontaneous clearing of the virus from their systems and very low rates of cancer. Therefore, the recommendation is to delay initiating screening in an effort to decrease the likelihood of overdiagnosis and treatment.106 However, in mid to late life, when cancer is often more prevalent, and the presence of hrHPV is an indicator of prolonged infection, HPV-based screening has the ability to accurately assess a woman’s risk for developing cervical cancer. As such, it is a preferred method of identifying women who may be at high risk for significant cancer.84,93
Cervical Cancer Prevention – Primary and Secondary
Cervical cancer prevention is a twofold method of primary and secondary prevention, which is directed to both the avoidance of HPV infection and the early detection and treatment of HPV-related precancerous lesions.108 Taking into account the long-time interval between HPV infection and cancer tumor, the continuity of both strategies is the requirement for effective prevention.6,109,110
Primary Prevention
HPV Vaccination
The HPV vaccination is the primary prevention method and is recognized as a major intervention for cancer prevention that can save lives.109,111 Since the HPV infection is defined as the major cause of cervical cancers, the HPV vaccination is the most effective way to prevent HPV infection and subsequent HPV-related diseases. The global prevalence of HPV among women aged over 30 years is estimated to be about 11.7%, with the highest prevalence in sub-Saharan Africa (24%) and differing national prevalence (2%-42%).7,112,113 The highest infection rates occur among women under 25 years, where the HPV prevalence might come close to 25%, which indicates that the virus is mainly transmitted through sexual intercourse after the beginning of sexual relations.114 Thus, the best time for vaccination is before the start of sexual activity, the main target group being girls aged 9–15 years.7,111
Currently, since 2006, HPV vaccines have been approved globally by the WHO.7,115,116 In a number of regions, especially in Europe, North America, and Australia, the vaccines that are most frequently used are Cervarix (bivalent), Gardasil (quadrivalent), and Gardasil-9 (nonavalent).7,117
The bivalent vaccine (Cervarix, Cecolin) is designed to prevent HPV-16 and −18 infections and has been found to provide some level of protection for HPV types 31 and 45 with good immunogenic response.7,118 The quadrivalent vaccine (Gardasil), in addition to HPV-16 and −18, protects against HPV-6 and −11, which are responsible for genital warts.119 The nonavalent vaccine (Gardasil-9), apart from the types for which the previous vaccines offer protection, the types include in the vaccine are now HPV-31, −33, −45, −52, and −58, and thus almost total protection against cervical precancerous lesions caused by the genotypes covered in the vaccine is ensured.7,120
The WHO, along with the different authorities at regional and national levels, recommends routine HPV vaccination for girls and boys between the ages of 9–15 years, usually administered in one or two doses, and catch-up vaccination for older adolescents and young adults utilizing two- or three-dose regimens.7,116,121,122 Those at higher risk, including HIV-positive individuals and the immunocompromised, are advised to receive two or three doses to make sure enough protection is provided.116
There is evidence that the vaccination against HPV can significantly reduce the incidence of diseases related to HPV, which are represented by the six types of cancer (cervical, anal, oropharyngeal, vulvar, vaginal, and penile) that HPV causes.120,122 Furthermore, large cohort studies demonstrated that HPV vaccination not only prevents the prevalence of serious cervical dysplasia (CIN2+), but also eliminates the risk of genital warts and non-oncogenic HPV strains.123,124 In Sweden, a follow-up study of more than 1.6 million women found an 88% reduction in cervical cancer among those vaccinated before the age of 17.4
Even though the vaccine’s safety and effectiveness have been widely accepted, the global vaccine coverage is still very low. By the year 2023, only about 27% of the world’s adolescent girls had received at least one dose of the HPV vaccine, and even fewer than 15% are fully vaccinated worldwide.125,126 The situation is even worse in the case of boys, with only about 4% of them being fully vaccinated in 2019.120
There are many reasons that contribute to low vaccination rates, like lack of knowledge, high cost, limited availability, and hesitation to take the vaccine, particularly in those regions where there is no gender-neutral vaccination policies.98,127 A major factor in resolving these problems will be the improvement of vaccine access, which is very important in the case of LMICs that are often unable to meet vaccination targets.128 School vaccination programs have been very successful in raising the number of vaccinated people and are evidenced by the case of Malaysia, where 80% of 13-year-old girls were vaccinated in only two years.129 Besides, financial rewards, employing nontraditional areas for delivery (like pharmacies and public health clinics), along with incorporation into the national cancer prevention program, can boost the uptake of vaccines and simultaneously save costs.130,131
In the fight for global fairness and equal vaccination opportunities, the Global Alliance for Vaccines and Immunization (GAVI) plays a vital role in guaranteeing lower vaccine prices and thus better access in the less developed countries.132
Education and Behavioral Interventions
Education campaigns on HPV knowledge and awareness support vaccination programs and protect against vaccine hesitancy related to HPV.109 Research consistently shows that people with lower levels of educational attainment are less likely to be aware of HPV and less likely to be vaccinated.133 There is evidence that integrating HPV education into schools, community initiatives, and mass media campaigns improves knowledge about HPV, perceptions of the disease, and willingness to be vaccinated.134,135
Peer-led education, storytelling techniques, and multimedia initiatives have produced positive outcomes for adolescents.136,137 Participation by medical professionals and local community leaders, including opinion leaders, enhances the success of education programs, especially in underserved communities.3,138
Moreover, the combination of educational and vaccine promotion, along with behavioral interventions, could effectively cut HPV transmission rates. Early onset of sexual activity, having multiple sex partners, or engaging in non-exclusive sexual relations are identified as increased risks for HPV infection, and men who engage in sexual contact with men are significantly more prone to higher HPV infection than their peers.139,140 Barrier methods are not completely effective against HPV transmission; nevertheless, regular condom and dental dam use significantly reduces the risk of infection.141,142 Male circumcision has been associated with both lower HPV rates and faster viral clearance, which has implications for both men and their female partners.143,144
Secondary Prevention: Cervical Screening and Its Modalities
Secondary prevention aims at preventing invasive cervical cancer by the early detection and treatment of precancerous lesions associated with HPV infection.72,109,145 The HPV vaccination program has expanded, but screening tests remain essential for reducing cervical cancer rates, particularly in countries with low- and middle-income, which do not have a national HPV vaccination program and account for most cervical cancer deaths.35,72 Screening programs help healthcare providers to detect precancerous conditions, which allow them to initiate required medical treatment and prevent further invasive cervical cancer development. The transition of screening methods from cytology-based techniques to HPV-based testing occurred due to the low sensitivity of cytological tests and the higher sensitivity of HPV testing.
The Papanicolaou test (Pap test) served as the primary screening technique from the 1950s until HPV testing started to replace it in the mid-2000s.72,146,147 The current methods use three techniques, which include the Pap test for cytology, visual inspection with acetic acid (VIA), and HPV testing methods such as HPV-DNA analysis and genotyping and self-collection (Figure 2). HPV-focused approaches have gained more significance because they are instrumental in detecting high-risk infections.15,72,148 Moreover, recently, the WHO identified self-sampling for HPV testing as a successful method that improves participation rates among groups who fail to obtain proper screening.149
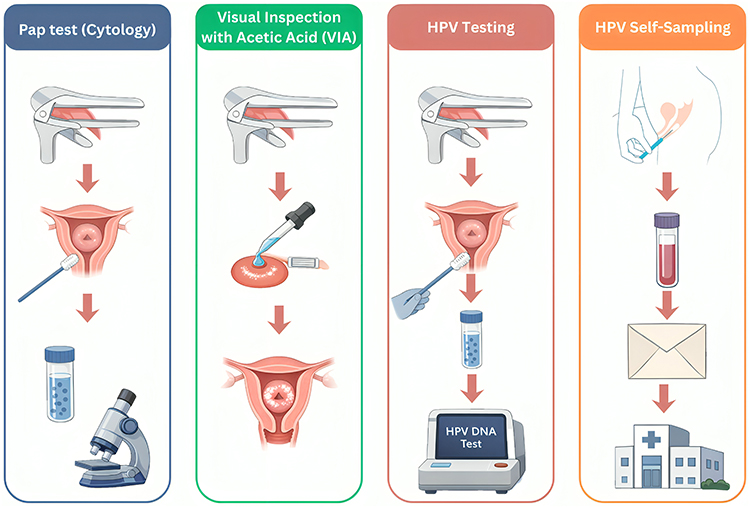 |
Figure 2 Cervical cancer screening modalities. |
Most screening programs target women, and routine HPV screening has no established procedures to screen men, but there exist ongoing discussions about targeted approaches for high-risk groups (eg, men who have sex with men)109,150,151 The regional differences in screening protocols exist because they reflect the health system resources and national health system capabilities, which LMIC countries need for their implementation.109
Global Differences in Cervical Cancer Screening Approaches
Cervical cancer screening strategies and approaches vary greatly across different regions, driven mainly by the healthcare resources, infrastructure, and public health regulations available in each area (Tables 1 and 2). In countries of North America and Australia, HPV testing has become the preferred primary screening method due to its excellent sensitivity (92–98%).152–155 These regions generally propose HPV screening every 5 years or cytology-based screening every 3 years.153–155 The American Cancer Society and the National Cancer Institute recommend starting the screening at 25 years of age, performing HPV testing every five years until 65 years of age.153–155
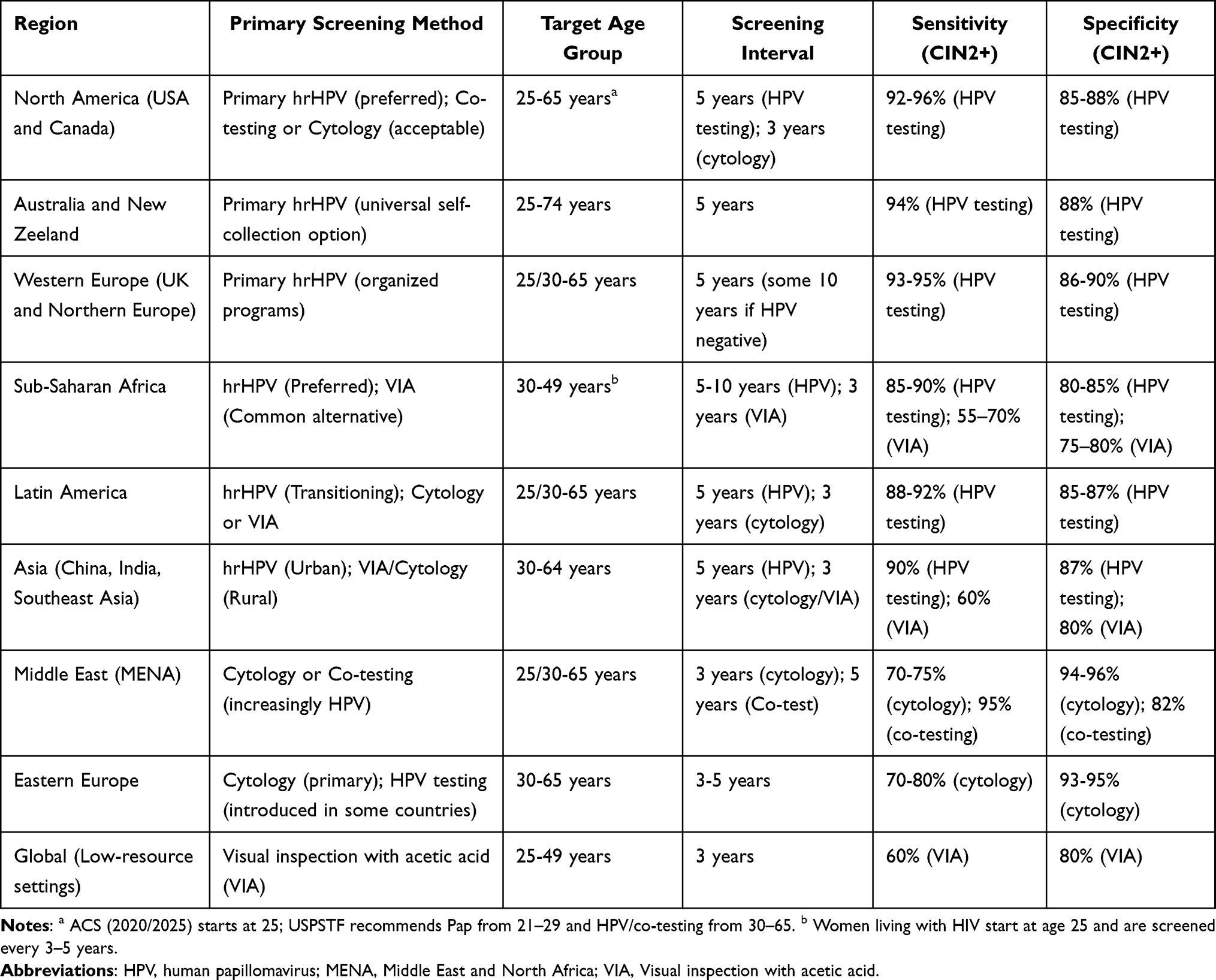 |
Table 1 Global Cervical Cancer Screening Strategies |
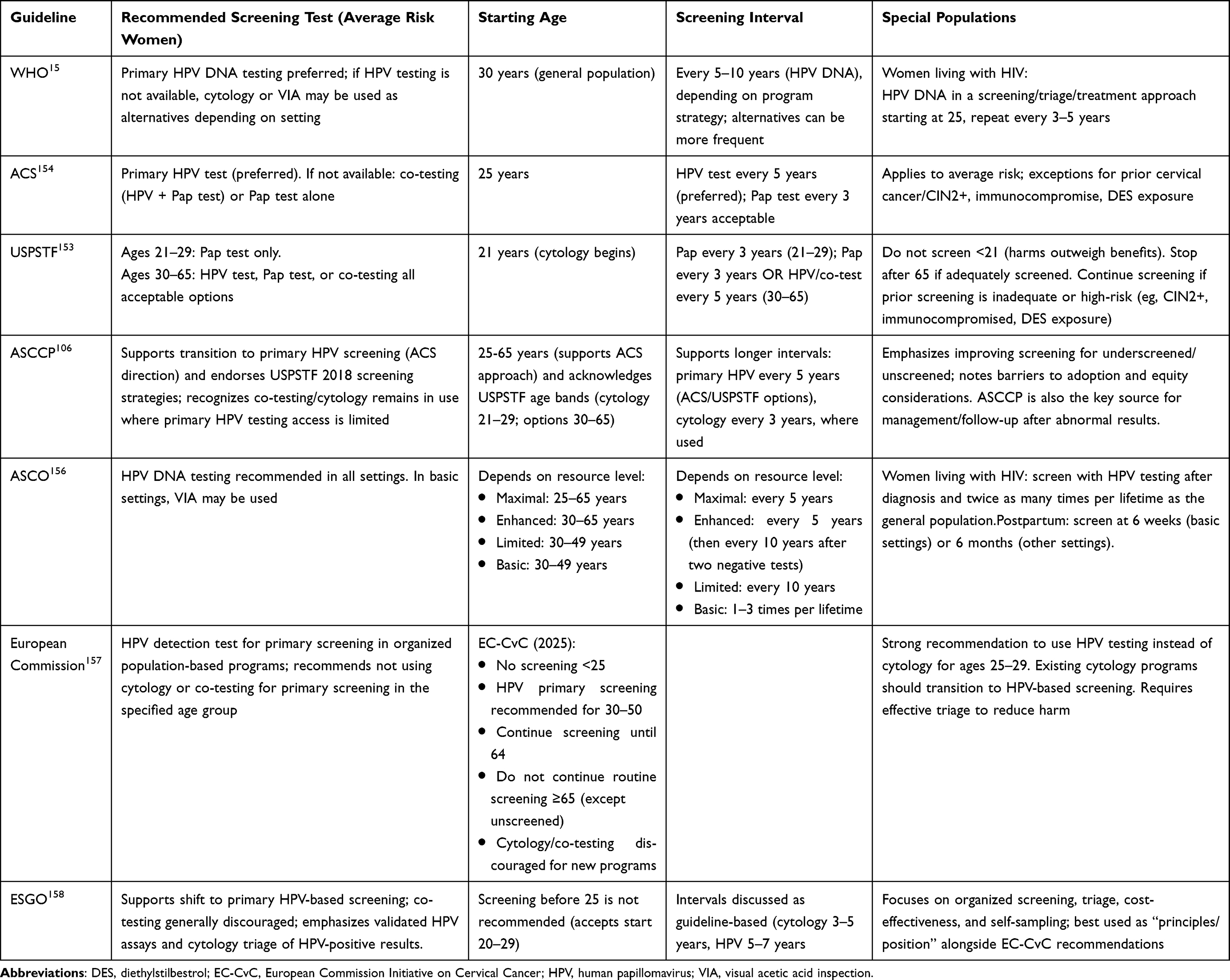 |
Table 2 Summary of Global Cervical Cancer Screening Guidelines |
In contrast, many low-resource areas, such as Sub-Saharan Africa are relying on the less sensitive methods like VIA, which is a low-cost method with moderate performance.159 The WHO states that VIA has a sensitivity of about 60% and a specificity of 79% compared with HPV testing, which achieves 98% sensitivity and 85% specificity.15
The gap mentioned above emphasizes the challenges of using the same screening protocols throughout different regions. Regions with better healthcare facilities usually opt for hrHPV testing-based initiatives, while in Eastern Europe and some parts of Asia, the old practice of mixing cytology with VIA is still going on due to limitations in infrastructure.160–162 Besides, HPV testing has been proven to be effective which also supports its role in triage approaches and therefore its use in these areas, reflecting the growing global consensus on the advantages of HPV-based screening.163
The differences in the cervical cancer screening methods across the globe reflect the need for tailored regional approaches to the prevention of cancer worldwide (Table 2).
International Guideline Recommendations Shaping Cervical Screening Strategies
Global standards show that various countries have developed distinct approaches to screening for cervical cancer (Table 1 and Table 2). The widespread agreement states that primary high-risk HPV testing offers superior sensitivity and longer protection to patients compared to cytology testing, which makes it the preferred screening method used in various medical settings.15,153–155,157
The WHO guideline suggests using HPV DNA testing as the main screening approach that allows for cytology or VIA to be used in cases where molecular testing cannot be performed according to the existing test conditions in multiple LMICs. The WHO recommends that all women begin screening at age 30, but the organization recommends that women with HIV should receive screening before this age.15 The ASCO recommendations provide increased flexibility through its resource-stratified framework, which recommends different age groups and time periods together with triage methods that depend on health system capabilities.156
High-income regions use their guidelines to establish HPV-based screening as their main screening method. The ACS recommends that women begin screening at 25 years old, when they need to undergo primary HPV testing every five years, and should use cytology testing only when they cannot get HPV tests.154 The U.S. Preventive Services Task Force (USPSTF) recommends that women between 21 and 29 years old should use cytology testing, while they allow women aged 30 to 65 to select between HPV testing and cytology or co-testing, with longer intervals recommended for HPV-based testing methods.153 The European Commission and JRC in Europe support HPV testing as the primary screening method for organized population-based programs, while they recommend against establishing new programs that use cytology or co-testing, thus demonstrating a systemic shift toward HPV-based preventive measures.157 The European Society of Gynaecological Oncology (ESGO) expert statement supports these views by recommending a transition to HPV-based screening, which demonstrates the importance of using verified tests and triage procedures and requires screening programs to maintain their quality assurance standards.158
Cytology-Based Screening: Papanicolaou Test and Liquid-Based Cytology
The impact of cytology-based screening, especially the Pap test, has been huge in cervical cancer prevention, and it has been one of the main reasons for the drop in both cancer incidence and mortality rates in countries with sustained implementation.72,96,145,164,165 The process of cervical cytology involves examination of the exfoliated cervical cells collected during pelvic exams with the purpose of detecting morphological changes associated with HPV-induced epithelial transformation.
The first step in analyzing the collected specimens is performing cervical cytopathology, and this can be done along with HPV testing or without it. The Papanicolaou stain is applied, which enhances the details of the nucleus and the cytoplasm that are required for diagnostic evaluation, thereby making it easier to see and identify.166,167 Cytology can be done by either traditional Pap smears or liquid-based cytology (LBC), both of which rely on microscopic evaluation of cellular structure.168 In addition to detecting dysplasia, cytology may also reveal inflammation or the presence of infectious agents and, by chance, may detect other gynecologic conditions, such as cervicitis, endometritis, endometrial hyperplasia, candidiasis, or trichomoniasis.166
Cervical cells in a classic Pap test are applied directly on a glass slide and then immediately fixed for staining. In contrast, liquid-based cytology washes the sampling tool into a vial filled with a preservative solution and afterwards prepares a thin, monolayer slide in the laboratory.169,170 Around the mid-1990s, liquid-based cytology was introduced as obtained through stepping up traditional cytology, focusing on better diagnostic accuracy and improving specimen quality.171 There were various existing commercial LBC platforms by the year 2022, such as ThinPrep, which was FDA-approved in 1996, and SurePath, which was FDA-approved in 1999, and these two are actually the most preferred ones in high-income settings.
Cytology is a very specific method of detecting high-grade cervical lesions (CIN2+), which generally reaches a specificity of more than 95%. However, it still possesses a moderate level of sensitivity. According to meta-analyses and guideline summaries, the sensitivities for traditional cytology are approximately 50–70%.96,166,172 The LBC method, on the other hand, brings about slight improvements in the quality of specimens and a bit higher sensitivity in some studies while maintaining the same specificity. For example, studies that compare cohorts have noticed LBC having CIN2+ sensitivities of approximately 75–77%, in contrast to the 70–75% seen with conventional Pap smears, while specificity for both techniques remain almost at 98–99%.170,173 However, both randomized and observational studies have shown different results and the overall variations in diagnostic accuracy between traditional cytology and LBC are generally very small, particularly with respect to high-grade lesions.174,175
Since a single cytology test can miss quite a few precancerous lesions, cytology-based screening methods have to conduct several rounds of testing at shorter intervals (generally, once every three years) and have very strong recall and follow-up mechanisms for their efficacy to be ensured.176,177 This limitation has been a major factor in the migration to the HPV-based screening, as a series of negative HPV tests leads to a risk that is exponentially lower for the long term than just a negative cytology result.96,178 Furthermore, the precursors of adenocarcinoma that appear in the endocervical canal are more frequently neglected by cytology and colposcopy than squamous precancers, which causes the preventive effect of adenocarcinoma to be smaller than that of squamous cell carcinoma.96,178,179
The LBC method has one of the most significant technical benefits that it can keep the remaining cellular material for further or secondary tests, including HPV high-risk screening, sexually transmitted infections, or cytology repeating without the need for an additional sample collection.170,179 This characteristic has rendered it feasible to have cytology as a part of the current screening techniques. On the downside, LBC is still costlier than the traditional method of cytology, thus it requires a higher capital investment and has a higher operating cost per test, which is a limiting factor for its use in developing countries with less money.102,170
Overall, cytology-based screening, primarily liquid-based cytology, has improved specimen quality and enabled more flexible diagnostic procedures. However, its moderate sensitivity to high-grade lesions has led to a slow re-evaluation of cytology’s part in cervical cancer prevention strategies. In many modern guidelines, cytology is often deployed as a triage test post-positive HPV screening rather than being the primary screening method.96,166
Visual Inspection of the Uterine Cervix
Visual inspection with acetic acid has been used in resource-poor settings due to the fact that it requires minimal laboratory infrastructure and also grants instant clinical response including screening and treating.10,180 VIA generally involves putting about 5% acetic acid on the cervix and, after one minute, roughly judging the transformation zone as VIA-negative (no or very few acetowhite change) or VIA-positive (bright, thick acetowhite lesions bordering the squamocolumnar junction) according to established pictorial guidelines.181 This quickness can reduce the number of patients lost to follow-up in comparison with multi-visit strategies that depend on laboratory processing times and recall systems.182,183
Strong evidence exists indicating that the VIA procedure can be a major primary screening method or, in more instances, a second-line test after HPV-positive results, but its efficacy is largely reliant on concrete situation, the extent and proficiency of training given and the endpoint projected (CIN1+ versus CIN2+/CIN3+).181,184
The VIA method is one of the main techniques currently in use that helps in the processing of HPV-positive women in order to shade the referral loads when the availability of colposcopy is limited or when the biomarkers are not so stable.159,172,182 In the large-scale multi-country ESTAMPA project with HPV-positive women as participants, the VIA method of triaging detected 84.5% of cases with CIN3+ overall (277/328), and the sensitivity reached 85.9% in women younger than 50 years, but it dropped to 78% in older women, while the specificity was the same for those older women.181 The primary outcome of the ESTAMPA study was that VIA triage reduced off-the-referral/treatment flow by putting close to half of the HPV-positive women in the VIA-negative category, but, on the other hand, it still did not detect some cancers, thereby emphasizing the need for escalation protocols in cases of suspected cancers and follow-up after negative VIA results in HPV-positive women.181
The VIA method has a major disadvantage that is its dependence on operators and the inherent variability in the process, which might lead to loss of reproducibility and give rise to false positives and the use of unnecessary treatments in case the training and quality assurance are not done properly.180,181 In the case of ESTAMPA, huge examiner-level variances were measured (CIN3+ sensitivity of about 25%-95% and specificity of roughly 45%-94%) and linked to better performance due to intense training, high number of exams, plus ongoing supervision/feedback.181 The above evidence is in line with the implementation literature that emphasizes the need for professional education, supervision, and structured digital support as key drivers for expanding the reach of VIA techniques.185,186
VIA is the method that is mainly emphasized to determine the eligibility of patients for ablative therapy procedures during screening and treating strategies. The method is the most accurate among the screening methods; however, its accuracy can be limited in older women who may have transformation zones that are either completely or partially visible. Hence, it is mostly recommended that women over 50 be triaged through means other than VIA.6,181 In general, the current guidelines seem to progressively accept the introduction of the HPV test as the primary screening test, while VIA continues to be a reasonable, context-sensitive approach, most legitimized as a second step in HPV-based screening or as a temporary measure where molecular testing and follow-up systems are not yet in place.96,181
HPV-Based Screening and HPV Genotyping (Primary HPV Testing, Co-Testing, Triage)
HPV screening directly determines the presence of high-risk HPV infections, and thus, it is more precise in focusing on the primary cause of cervical cancer than morphology-based cytology.96,187 Numerous randomized trials and meta-analyses show that hrHPV testing is much more sensitive than cytology in detecting CIN2+ and CIN3+, while a negative HPV test implies a very low long-term risk for cervical precancer and cancer.96,184,188,189 These risk parameters warrant prolongation of the screening interval (≥5 years) following HPV-negative results and direct the transition to HPV-based primary screening in worldwide guidelines.6,110,166
The majority of the HPV tests that are currently available use PCR-based amplification of the target DNA to identify the DNA (or rarely, E6/E7 mRNA) of the high-risk HPV types that are responsible for the cancer, usually consisting of the 12 group 1 hrHPV genotypes (HPV-16, −18, −31, −33, −35, −39, −45, −51, −52, −56, −58, −59), while there are also some tests that detect HPV66 and HPV68 as well.190–192 However, there are also tests that target the L1 gene and have very high analytical sensitivity, and the extensive validation studies show that such tests have 90–95% sensitivity for detecting CIN2+ lesions, along with the specificity that is acceptable for the screening populations that are 30 years old and older.193,194
HPV genotyping segregates infections caused by HPV16 and HPV18, which are responsible for nearly 70% of invasive cervical cancers, from those caused by other hrHPV types, thus giving a clinically relevant risk stratification.93,195 Risk-based screening protocols depend on genotype-specific results to determine the next step in dealing with the condition: usually, women who test positive for HPV-16 and/or HPV-18 are sent directly to colposcopy, whereas those positive for other hrHPV types are either re-tested or subjected to further molecular or cytological triage.96,106 Evidence from programmatic data suggests that the use of targeted HPV genotyping can improve clinical management; the main reason being that it can lead to immediate colposcopy or quick treatment for those with the highest short-term risk of progressing to CIN3+, which is a significant advantage for the underrepresented groups that usually do not stick to long-term follow-up.196
Due to the fact that nearly all precancers are associated with HPV, the merging of cytology and HPV testing provides no more than a slight advantage in most primary screening options, but it also complicates the process and demands more resources.96,197 Consequently, cytology is becoming more and more popular as a triage method rather than a first testing method in HPV-centered approaches.96,106
The main benefit of HPV genotyping is that it can be done with self-sampling, which makes it easier for women to have access to the screening, while the accuracy of the diagnosis is not affected. Many studies have been done through meta-analysis, and they suggest that PCR-based HPV detection on self-sampled vaginal specimens has similar sensitivity for CIN2+ detection as clinician-collected cervical specimens (pooled sensitivity ratio ≈ 0.99), with only a minor drop in specificity (2–4%).39 The HPValidate study proved that DNA-based methods (like Evalyn brush or FLOQSwab with Cobas assays) keep strong HPV16/18 genotype identification and get relative sensitivities of 0.90–0.94 for CIN2+.198 Studies on automated systems like Cobas 4800/6800 confirm having sensitivity of ≥93% and specificity of >92% for CIN2+ in women aged ≥30, while self-collected and clinician-collected samples show high agreement in genotype (κ ≈ 0.80–0.92).194,199
HPV genotyping is a very sensitive primary screening method that also provides risk assessment, supports longer screening intervals, and enables reliable self-sampling. These traits make HPV-based screening, augmented by genotype-specific triage, the leading technique in contemporary cervical cancer prevention strategies, particularly in settings that aim to improve coverage without reducing clinical effectiveness.6,96
Self-Sampling in HPV-Based Cervical Cancer Screening
One of the main strategies employed to increase participation in cervical cancer screening among the underserved and hard-to-reach groups is self-sampling for HPV testing.200 This strategy allows women to take their samples in the comfort of their homes and to avoid issues related to the invasiveness and discomfort that are often associated with clinician-collected specimens. The evidence in support of the self-sampling’s effectiveness and acceptability has been extremely convincing, with a vast number of systematic reviews and randomized trials indicating its potential to increase screening rates significantly.39,200
HPV self-sampling is a method that is very effective in identifying the high-risk HPV types. These types are important for recognizing women with a higher chance of developing cervical cancer. Research indicates that the sensitivity of the HPV testing on the self-collected samples is equal to that of the samples collected by the clinician, if validated PCR-based assays are employed.39,200,201 This equal diagnostic performance, together with the simplicity of use, makes self-sampling an appealing option to the conventional screening methods. The most significant thing is that the detection of HPV infection through self-sampling brings forth the scenario for earlier intervention and better outcomes, as the persistent infection with high-risk HPV types is the major predictor of cervical precancer and cancer.201,202
One of the primary advantages of self-sampling is that it leads to an increase in screening participation, particularly among women who have not been attending regular screening services.203 Researchers have established that self-sampling almost doubles the participation in screening of women when compared with the clinician-based sampling method.200 The impact of HPV self‑sampling is most discernible among the under-screened and never-screened women, who are typically very difficult to engage in cervical cancer control.39,204 Self-collection resolutions tackle a number of screening barriers, ie., logistical issues, costs, and fears of losing one’s privacy or being uncomfortable during the medical examination.197
Sending self-sampling kits directly to women’s homes has been proven as a very effective strategy to increase participation, particularly in areas where resources are limited or among populations with restricted access to health care.200,201 By enabling people to do the test themselves and mail the samples for receiving the results, this system not only expands the coverage but also reduces the burden on health care facilities.96
Self-collection has been widely accepted by women, with research consistently indicating high satisfaction rates. The majority of women preferred self-sampling over the sampling done by health professionals, which showed the extra comfort and privacy it brings. Acceptance was seen to be high among different groups, such as women living in both wealthy and poor communities, and also in rural and urban areas.205,206 Most notably, the method has been able to gain good acceptance among women from different classes and cultures, including those who have always been left out of the screenings for cervical cancer.207,208
Studies show that women who had not been attending the screening before were the most likely to accept the self-sampling method, and this is due to the autonomy and comfort it provides. This trend shows the importance of self-sampling as a tool to cover the lack of access to screening, particularly in groups that are in difficulties in getting traditional screening methods.209,210
Self-sampling when used in structured screening programs could lead to increased overall participation in the screenings and consequently more cases detected early. Self-sampling has been recognized by the WHO as a method incorporated into the worldwide campaigns to eradicate cervical cancer, thereby admitting its role in the screening rates and impact of cervical cancer lessening.6 Furthermore, self-sampling can easily become part of the national screening programs, thus being a major player in the realization of the WHO’s 90–70-90 goals in the area of cervical cancer prevention.201
HPV self-sampling also has a drawback in the accuracy of diagnosis that might differ based on the user factors, self-sampling kits used and test/method applied for HPV identification.201,202 Also, while self-sampling increases participation in screenings, follow-ups after positive outcomes are not consistent.
To obtain the full advantages of self-sampling, it is essential to offer proper guidance and educational resources that will help women to carry out the test the right way. The use of clear communication and effective outreach programs will not only raise awareness but also increase the participation level.96 Moreover, supplying pre-paid and pre-addressed envelopes for the return of samples can be a significant factor in minimizing the logistical problems.201
Nevertheless, the method’s limitation still exists in the form of cultural acceptance, and people from different backgrounds need to be properly addressed and given the right information. Women’s viewpoint on self-sampling may be largely affected by cultural and social circumstances, hence, the need to take these factors into account when planning screenings.197,201
Self-sampling is an essential aspect that should be included in a more comprehensive approach consisting of follow-up care for patients who are diagnosed with high-risk HPV. Providing sufficient follow-up care, which may include colposcopy or treatment for the precancerous lesions, is one of the main conditions for the success of the screening programs.211,212
Self-HPV sampling ensures that those at risk of getting cervical cancer receive the advantage of screening on their own, particularly those who are hard to reach by screening programs. Gradually, with the incorporation of self-sampling into the global screening programs, the incidence and mortality associated with cervical cancer will be eradicated.6,200,201
The suggested framework for implementing HPV self-sampling should be tailored according to the specifics of social/cultural environment of country, the health care system, and screening coverage. For instance, in high-income countries with well-established screening programs and laboratory capacities, self-sampling can be implemented as part of population-based cervical cancer screening programs using mailed samples, digital applications, and HPV testing pathways. These measures can enhance participation rates in underserved populations such as rural areas, migrants, and underscreened women.201,203,213 In contrast, in LMICs, self-sampling should be implemented in a community-based manner involving primary health care centers and community outreach programs. Both types of implementation frameworks should ensure that self-sampling is accessible and affordable, culturally sensitive education is provided, linkage-to-care systems for HPV-positive women are developed, and quality assurance measures are in place.203,213 Further practical priorities should include assessment of long-term clinical efficacy, cost-effectiveness, implementation feasibility in various health care systems, acceptability by different target populations, and implementation of digital applications in facilitating screening processes.
Factors Affecting Cervical Cancer Screening Coverage
The cervical cancer screening rates remain very low despite the availability of effective screening methods (Figure 3). Evidence from LMICs shows that screening uptake depends on multiple personal and sociocultural and health-system factors rather than a single determinant.214–216
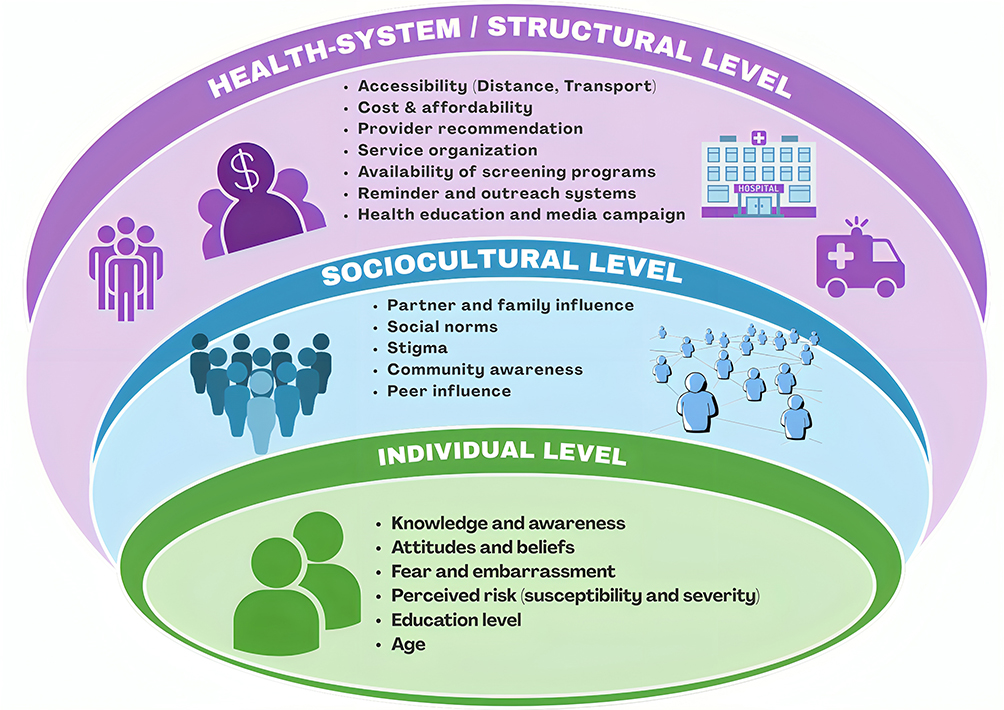 |
Figure 3 Multilevel factors influencing cervical cancer screening uptake. |
Screening participation faces a significant obstacle because people lack basic knowledge about the screening process. Women who do not have symptoms of a medical condition fail to understand the need for screening tests, which work to prevent future health problems.217,218 Across African and Asian settings, limited awareness has consistently been linked to decreased usage of screening services.219 In contrast, higher education is strongly associated with participation. A meta-analysis from Ethiopia proved that women with high knowledge levels had three times greater screening participation rates, and similar patterns have been observed in LMICs following health education and awareness interventions.220,221 Crucially, knowledge by itself might not be adequate to achieve useful results because people need to recognize knowledge as important for their personal lives.218
Screening behavior is influenced by people’s attitudes and their psychological evaluation of the situation. Women who have positive attitudes about early cancer screening benefits and screening effectiveness are more likely to take part in screening programs.222 Also, women who support screening programs display much higher participation rates because positive attitudes toward screening programs lead to multiple times more involvement in screening programs.223 At the same time, fear of experiencing pain, their desire to avoid embarrassment and anxiety about potential results can discourage participation.224 The fear of cancer diagnosis becomes more pronounced in settings that associate cancer with a high likelihood of death.218 The meta-analytic results show that perceived vulnerability, together with severity increase screening participation.220
Sociodemographic factors also influence screening participation. The main focus of screening programs targets women who are between 30 and 49 years because this age group shows higher uptake of screening tests.219,225 The educational level of women acts as a primary indicator because women who have not completed formal schooling show lower participation rates, which results from their limited health literacy and limited access to information.220,221 Urban residents tend to show higher uptake because they have better access to services and greater exposure to information, although the degree of this relationship varies with different situations.217 The sociodemographic patterns show different results in various contexts because the local healthcare system capabilities and outreach strategies determine their distribution.
One important factor is still the accessibility of the health system. The three main obstacles that people face in accessing medical facilities include distance to facilities, transportation issues, and travel duration.218,226 The service organization also has a significant impact. The restricted screening locations, along with the extended wait times and the unpredictable service times, create obstacles that prevent people from participating in the screening.225 Provider recommendation acts as a crucial element because women who receive advice from healthcare professionals demonstrate higher screening participation rates.221 Programs that incorporate a combination of reminder outreach activities and community-based screening methods in screening programs lead to improved program participation because these factors demonstrate the impact of system-wide design.214
Economic constraints add another layer of barriers because screening services depend on their budget subsidies. People face difficulties in participating because of transportation expenses and indirect costs and lost work time.226,227 The existing limitations create greater disadvantages for rural and low-income communities, which leads to increased screening access disparities.218
Social and cultural norms also influence screening behavior. Women make their healthcare decisions based on their partner’s permission in specific situations.228 The anxiety about how people will judge them, together with the stigma of reproductive health check-ups, prevents people from participating in these activities.224 Conversely, peer communications and community discussions can facilitate uptake. Women who participate in community screening discussions tend to increase their screening activities at their local health facilities.213,226–231 Community mobilization campaigns, together with media exposure campaigns, lead to positive results which promote their usage of services.221
Conclusion
Cervical cancer remains a major public health concern globally, with marked differences in incidence and mortality rates between high-income and low- and middle-income countries. Despite the success of HPV vaccination programs and screening initiatives in decreasing disease burden in several countries, poor uptake of cervical cancer screening programs, especially among women in rural and socioeconomically disadvantaged populations, continues to pose a challenge. The introduction of HPV testing as a part of cervical cancer screening, including self-sampling methods, can potentially be a positive step towards making cervical cancer prevention more effective and efficient, thus, its success can be boosted. Evidence from multiple studies has demonstrated that self-sampling has proven to be very effective by improving screening uptake, especially among previously underscreened populations. In countries where the cervical cancer rate is still high, integrating HPV self-sampling into the national screening program could solve the problem of limited access and increase the number of early detections. In the future, the combination of vaccination, HPV-focused screening, and innovative methods such as self-sampling will drastically reduce the number of cervical cancer deaths, thus facilitating global efforts to reach the World Health Organization’s 90–70-90 goal for eradication.
Ethics Statement
Due to the nature of the study (narrative review) no ethical approval is required.
Funding
This research has been funded by the Science Committee of the Ministry of Science and Higher Education of the Republic of Kazakhstan (Grant No. AP26194759, “Cervical Cancer Screening Using Self-sampling Approach: Validation of Human Papillomavirus Self-sampling Kits Among Kazakhstani Women”). Gulzhanat Aimagambetova is the PI of the project.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):e191–26. Erratum in: Lancet Glob Health. 2022 Jan;10(1)e41doi: 10.1016/S2214-109X(21)00554-4. PMID: 31812369; PMCID: PMC7025157. doi:10.1016/S2214-109X(19)30482-6
2. Singh D, Vignat J, Lorenzoni V, et al. Global estimates of incidence and mortality of cervical cancer in 2020: a baseline analysis of the WHO global cervical cancer elimination initiative. Lancet Glob Health. 2023;11(2). doi:10.1016/s2214-109x(22)00501-0
3. UNICEF USA. HPV vaccination campaign protects girls in Nigeria [Internet]. New York: UNICEF USA; Available from: https://www.unicefusa.org/stories/hpv-vaccination-campaign-protects-girls-nigeria.
4. Lei J, Ploner A, Elfstrom M, et al. HPV vaccination and the risk of invasive cervical cancer. N Engl J Med. 2020;383:1340–1348.
5. Small W, Bacon MA, Bajaj A, et al. Cervical cancer: a global health crisis. Cancer. 2017;123(13):2404–2412.
6. World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva: World Health Organization; 2020. Available from: https://www.who.int/publications-detail-redirect/9789240014107.
7. Akhatova A, Azizan A, Atageldiyeva K, et al. Prophylactic Human Papillomavirus Vaccination: from the Origin to the Current State. Vaccines (Basel). 2022;10(11):1912. PMID: 36423008; PMCID: PMC9696339. doi:10.3390/vaccines10111912
8. HPV Vaccination Impact Study Group. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: updated systematic review and meta-analysis. Lancet. 2019;394(10197):497–509. doi:10.1016/S0140-6736(19)30298-3
9. Zampaoglou E, Boureka E, Gounari E, et al. Screening for cervical cancer: a comprehensive review of guidelines. Cancers. 2025;17(13):2072. doi:10.3390/cancers17132072
10. Bouvard V, Wentzensen N, Mackie A, et al. The IARC perspective on cervical cancer screening. N Engl J Med. 2021;385(20):1908–1918. doi:10.1056/nejmsr2030640
11. Wentzensen N, Clarke MA, Perkins RB. Impact of covid-19 on cervical cancer screening: challenges and opportunities to improving resilience and reduce disparities. Prevent Med. 2021;151:106596. doi:10.1016/j.ypmed.2021.106596
12. Das M. Who launches strategy to accelerate elimination of cervical cancer. Lancet Oncol. 2021;22(1):20–21. doi:10.1016/s1470-2045(20)30729-4
13. Chan CK, Aimagambetova G, Ukybassova T, Kongrtay K, Azizan A. Human papillomavirus infection and cervical cancer: epidemiology, screening, and vaccination-review of current perspectives. J Oncol. 2019;2019:3257939. PMID: 31687023; PMCID: PMC6811952. doi:10.1155/2019/3257939
14. Landy R, Pesola F, Castañón A, Sasieni P. Impact of cervical screening on cervical cancer mortality: estimation using stage-specific results from a nested case–Control Study. Br J Cancer. 2016;115(9):1140–1146. doi:10.1038/bjc.2016.290
15. World Health Organization. WHO guideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention [Internet]. 2nd ed. Geneva: World Health Organization; 2021. Table 1, Screening and treatment recommendations and good practice statements for the general population of women and women living with HIV. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572317/.
16. Pankakoski M, Sarkeala T, Anttila A, Heinävaara S. Effectiveness of cervical testing in and outside a screening program—a case-control study. Cancers. 2022;14(21):5193. doi:10.3390/cancers14215193
17. Almonte M, Ilbawi AM, Maza M, et al. From commitments to action: the first global cervical cancer elimination forum. Lancet Reg Health Am. 2024;36:100812. doi:10.1016/j.lana.2024.100812
18. Asangbeh-Kerman SL, Davidović M, Taghavi K, et al. Cervical cancer prevention in countries with the highest HIV prevalence: a review of policies. BMC Public Health. 2022;22(1). doi:10.1186/s12889-022-13827-0
19. eClinicalMedicine. Global strategy to eliminate cervical cancer as a public health problem: are we on track?. eClinicalMedicine. 2023;55:101842. doi:10.1016/j.eclinm.2023.101842
20. National Cancer Institute. What Is Cervical Cancer? Available from: https://www.cancer.gov/types/cervical.
21. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2021;71(3):209–249. doi:10.3322/caac.21660
22. Włoszek E, Krupa K, Skrok E, Budzik MP, Deptała A, Badowska-Kozakiewicz A. HPV and cervical cancer-biology, prevention, and treatment updates. Current Oncol. 2025;32(3):122. doi:10.3390/curroncol32030122
23. Baba SK, Alblooshi SS, Yaqoob R, et al. Human papilloma virus (HPV) mediated cancers: an insightful update. J Transl Med. 2025;23(1). doi:10.1186/s12967-025-06470-x
24. Mohammed MM, Al-Khafaji ZA, Al-Hilli NM. The orchestration of high-risk HPV-induced cervical cancer: a comprehensive review. Med J Babylon. 2025;22(3):621–631. doi:10.4103/mjbl.mjbl_230_24
25. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(1):9–29.
26. Tewari KS. Cervical cancer. N Engl J Med. 2025;392(1):56–71. doi:10.1056/NEJMra2404457
27. WHO. GLOBOCAN. Cancer Tomorrow. Available from: https://gco.iarc.fr/tomorrow/en/dataviz/isotype?types=0&single_unit=5000&populations=900&group_populations=0&multiple_populations=0&years=2025&cancers=23.
28. Arrossi S, Temin S, Garland S, et al. Primary Prevention of Cervical Cancer: American Society of Clinical Oncology Resource-Stratified Guideline. J Glob Oncol. 2017;3(5):611–634. PMID: 29094100; PMCID: PMC5646902. doi:10.1200/JGO.2016.008151
29. Wu J, Jin Q, Zhang Y, et al. Global burden of cervical cancer: current estimates, temporal trend and future projections based on the Globocan 2022. J Natl Cancer Cent. 2025;5(3):322–329. doi:10.1016/j.jncc.2024.11.006
30. Canfell K, Kim JJ, Brisson M, et al. Mortality impact of achieving who cervical cancer elimination targets: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. 2020;395(10224):591–603. doi:10.1016/s0140-6736(20)30157-4
31. Son Y, Hong S, Jang W, et al. Global, regional, and national burden of cervical cancer in 2022 and projections to 2050: a population-based analysis of Globocan. Int J Gynecol Cancer. 2026;36(1):102751. doi:10.1016/j.ijgc.2025.102751
32. Zhou L, Li Y, Wang H, Qin R, Han Z, Li R. Global cervical cancer elimination: quantifying the status, progress, and gaps. BMC Med. 2025;23(1). doi:10.1186/s12916-025-03897-3
33. Hall MT, Simms KT, Lew J-B, et al. The projected timeframe until cervical cancer elimination in Australia: a modelling study. Lancet Public Health. 2019;4(1). doi:10.1016/s2468-2667(18)30183-x
34. Mao Y, Gao Y, He Y, et al. Global burden of cancer in women, 1990–2021: a systematic analysis from the GBD 2021 Study. Front Oncol. 2025;15. doi:10.3389/fonc.2025.1633894
35. International Agency for Research on Cancer. Cervix uteri fact sheet. Global Cancer Observatory. Available from: https://gco.iarc.who.int/media/globocan/factsheets/cancers/23-cervix-uteri-fact-sheet.pdf.
36. WHO. Global cancer burden growing, amidst mounting need for services. Available from: https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing--amidst-mounting-need-for-services#:~:text=Lung%20cancer%20was%20the%20most,persistent%20tobacco%20use%20in%20Asia.
37. Nabi S, Mimba B-R, Akunne O. Eliminating cervical cancer: the impact of screening and human papilloma virus vaccination. Prev Chronic Dis. 2025. doi:10.5888/pcd22.250127
38. Broutet N, Jeronimo J, Kumar S, et al. Implementation research to accelerate scale-up of national screen and treat strategies towards the elimination of cervical cancer. Prevent Med. 2022;155:106906. doi:10.1016/j.ypmed.2021.106906
39. Arbyn M, Smith SB, Temin S, Sultana F, Castle P. Detecting cervical precancer and reaching underscreened women by using HPV testing on self-samples: updated meta-analyses. BMJ. 2018;363:k4823. doi:10.1136/bmj.k4823
40. Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today. Lyon, France: International Agency for Research on Cancer; 2020. Available from: https://gco.iarc.fr/today.
41. Ginsburg O, Bray F, Coleman MP, et al. The global burden of women’s cancers: a grand challenge in global health. Lancet. 2017;389(10071):847–860. doi:10.1016/s0140-6736(16)31392-7
42. Bruni L, Diaz M, Barrionuevo-Rosas L, et al. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. Lancet Glob Health. 2016;4(7):e453–63. Erratum in: Lancet Glob Health. 2017 Jul;5(7)e662doi: 10.1016/S2214-109X(17)30186-9. PMID: 27340003. doi:10.1016/S2214-109X(16)30099-7
43. Bruni L, Albero G, Serrano B, et al. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human papillomavirus and related diseases in the world. Summary report; 2023. Available from: https://www.hpvcentre.net.
44. Wei L-H, Su -Y-Y, Hu Y-M, et al. Age distribution of human papillomavirus infection and neutralizing antibodies in healthy Chinese women aged 18–45 years enrolled in a clinical trial. Clin Microbiol Infect. 2020;26(8):1069–1075. doi:10.1016/j.cmi.2019.12.010
45. Zhao M, Kang P, Zhu L, et al. Global pattern of persistent human papillomavirus infection in female genital tract: an update system review and meta-analysis. iScience. 2024;27(10):110991. doi:10.1016/j.isci.2024.110991
46. Simms KT, Steinberg J, Caruana M, et al. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020–99: a modelling study. Lancet Oncol. 2019;20(3):394–407. doi:10.1016/s1470-2045(18)30836-2
47. Brisson M, Kim JJ, Canfell K, et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. 2020;395(10224):575–590. doi:10.1016/s0140-6736(20)30068-4
48. de Martel C, Plummer M, Vignat J, Franceschi S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int J Cancer. 2017;141(4):664–670. doi:10.1002/ijc.30716
49. Ramakrishnan S, Partricia S, Mathan G. Overview of high-risk HPV’s 16 and 18 infected cervical cancer: pathogenesis to prevention. Biomed Pharmacother. 2015;70:103–110. doi:10.1016/j.biopha.2014.12.041
50. Okunade KS. Human papillomavirus and cervical cancer. J Obstetrics Gynaecol. 2019;40(5):602–608. doi:10.1080/01443615.2019.1634030
51. World Health Organization. Human papilloma virus and cancer [Internet]. Geneva: World Health Organization; 2024. Available from: www.who.int.
52. World Health Organization. Cervical cancer. Geneva: World Health Organization; 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer.
53. Yusuf M. Perspectives on cervical cancer: insights into screening methodology and challenges. Cancer Screen Prevent. 2024;3(1):47–55. doi:10.14218/csp.2023.00041
54. National Center for Biotechnology Information. Human Papillomavirus (HPV) Infection. Available from: https://www.ncbi.nlm.nih.gov/books/NBK321770/
55. Haręża DA, Wilczyński JR, Paradowska E. Human papillomaviruses as infectious agents in gynecological cancers. oncogenic properties of viral proteins. Int J Mol Sci. 2022;23(3):1818. doi:10.3390/ijms23031818
56. Cerqueira C, Schiller JT. Papillomavirus assembly: an overview and perspectives. Virus Res. 2017;231:103–107. doi:10.1016/j.virusres.2016.11.010
57. Kirk A, Graham SV. The human papillomavirus late life cycle and links to keratinocyte differentiation. J med virol. 2024;96(2). doi:10.1002/jmv.29461
58. Pešut E, Đukić A, Lulić L, et al. Human papillomaviruses-associated cancers: an update of current knowledge. Viruses. 2021;13(11):2234. doi:10.3390/v13112234
59. International Human Papillomavirus Reference Center Human Reference Clones – hpvcenter 2022. Available from: https://www.hpvcenter.se/human_reference_clones/.
60. Wang X, Huang X, Zhang Y. Involvement of human papillomaviruses in cervical cancer. Front Microbiol. 2018;9. doi:10.3389/fmicb.2018.02896
61. Salehi S, Rafiei R, Ghadarjani R, Gharaei Nejad K. The prevalence of human papillomavirus genotypes among patients with sexually transmitted HPV in North Iran. Clin Epidemiol Global Health. 2024;28:101693. doi:10.1016/j.cegh.2024.101693
62. Correa RM, Baena A, Valls J, et al. Distribution of human papillomavirus genotypes by severity of cervical lesions in HPV screened positive women from the Estampa Study in Latin America. PLOS ONE. 2022;17(7). doi:10.1371/journal.pone.0272205
63. Nikolic N, Basica B, Strbac M, et al. Prevalence of carcinogenic genotypes of HPV-infected women in a ten-year period (2014–2023) in Vojvodina, Serbia. Medicina. 2024;60(6):922. doi:10.3390/medicina60060922
64. Aimagambetova G, Bapayeva G, Ukybassova T, et al. Risks of cervical cancer recurrence after fertility-sparing surgery and the role of human papillomavirus infection types. J Clin Med. 2024;13(21):6318. PMID: 39518458; PMCID: PMC11547075. doi:10.3390/jcm13216318
65. Sandoval-Clavijo A, Martí-Martí I, Ferrándiz-Pulido C, Verdaguer-Faja J, Jaka A, Toll A. Human papillomavirus-related cutaneous squamous cell carcinoma. Cancers. 2025;17(5):897. doi:10.3390/cancers17050897
66. Zhuang L, Xie X, Wang L, et al. Assessment of high-risk human papillomavirus infection characteristics in cervical squamous cell carcinoma and adenocarcinoma in China. Risk Manag Healthc Policy. 2022;15:2043–2055. doi:10.2147/rmhp.s384342
67. Campos-Parra AD, Pérez-Quintanilla M, Martínez-Gutierrez AD, et al. Molecular differences between squamous cell carcinoma and adenocarcinoma cervical cancer subtypes: potential prognostic biomarkers. Current Oncol. 2022;29(7):4689–4702. doi:10.3390/curroncol29070372
68. Cho EH, Park M-S, Woo H-Y, Park H, Kwon M-J. Evaluation of clinical usefulness of HPV-16 and HPV-18 genotyping for cervical cancer screening. J Gynecol Oncol. 2024;35(6). doi:10.3802/jgo.2024.35.e72
69. Letafati A, Motlaghzadeh S, Ardekani OS, et al. Uncommon high distribution of HPV-16, HPV-54, and HPV-56 in female referred to a laboratory in Karaj, Iran: indications of a paradigm shift in HPV genotypes?. Virol J. 2024;21(1). doi:10.1186/s12985-024-02457-0
70. Volpini LP, Dias JA, de Freitas LB, Silva MC, Miranda AE, Spano LC. Viral load and high prevalence of HR-HPV52 and 58 types in black women from rural communities. BMC Infect Dis. 2021;21(1). doi:10.1186/s12879-021-06042-6
71. Kondlo S, Giyose N, Businge CB, Mbulawa ZZ. Human papillomavirus genotype landscape across cervical cytology grades and impact of HIV among women of Eastern Cape Province, South Africa. Viruses. 2025;18(1):65. doi:10.3390/v18010065
72. Aimagambetova G, et al. Cervical cancer natural history, diagnosis, and treatment: from molecular events to clinical management. In: Rezaei N, editor. Gynecological Cancers: An Interdisciplinary Approach. Interdisciplinary Cancer Research. Vol. 17. Cham: Springer; 2024.
73. Doorbar J, Griffin H. Refining our understanding of cervical neoplasia and its cellular origins. Papillomavirus Res. 2019;7:176–179. doi:10.1016/j.pvr.2019.04.005
74. Prendiville W, Sankaranarayanan R IARC Technical Report, No. 45. Lyon (FR): International Agency for Research on Cancer; 2017.
75. Schichl K, Doorbar J. Regulation and deregulation of viral gene expression during high-risk HPV infection. Viruses. 2025;17(7):937. doi:10.3390/v17070937
76. Aiyenuro A, Griffin H, Schichl K, et al. Role of reserve cells in metaplasia and the development of human papillomavirus–associated high-grade squamous intraepithelial lesions at the cervical transformation zone. Lab Invest. 2025;105(7):104166. doi:10.1016/j.labinv.2025.104166
77. Vallejo-Ruiz V, Gutiérrez-Xicotencatl L, Medina-Contreras O, Lizano M. Molecular aspects of cervical cancer: a pathogenesis update. Front Oncol. 2024;14. doi:10.3389/fonc.2024.1356581
78. Pangarkar MA. The Bethesda System for reporting cervical cytology. Cytojournal. 2022;19:28. doi:10.25259/CMAS_03_07_2021
79. Nayar R, Wilbur DC. The Bethesda system for reporting cervical cytology: a historical perspective. Acta Cytol. 2017;61(4–5):359–372. PMID: 28693017. doi:10.1159/000477556
80. Khieu M, Butler SL. High-Grade Squamous Intraepithelial Lesion of the Cervix. StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
81. Sibeko S, Sanderson M, Moyo S, Botha MH. Role of the epithelium in human papillomavirus and human immunodeficiency virus infections in the female genital tract. Front Reprod Health. 2024;6. doi:10.3389/frph.2024.1408198
82. Kamassa HE, Katawa G, Isawumi A, et al. Understanding the role of oral and vaginal microbiomes in HPV-related cervical, head, and neck cancers: knowledge gaps and feasibility in Sub-Saharan Africa. Front Microbiomes. 2025;4. doi:10.3389/frmbi.2025.1576394
83. Luo H, Du H, Belinson JL, Wu R. Evaluation of alternately combining HPV viral load and 16/18 genotyping in secondary screening algorithms. PLOS ONE. 2019;14(7). doi:10.1371/journal.pone.0220200
84. Schiffman M, Doorbar J, Wentzensen N, et al. Carcinogenic human papillomavirus infection. Nature Reviews Disease Primers. 2016;2(1). doi:10.1038/nrdp.2016.86
85. Espinoza H, Ha KT, Pham TT, Espinoza JL. Genetic predisposition to persistent human papillomavirus-infection and virus-induced cancers. Microorganisms. 2021;9(10):2092. doi:10.3390/microorganisms9102092
86. Ozbun MA, Campos SK. The long and Winding road: human papillomavirus entry and subcellular trafficking. Curr Opin Virol. 2021;50:76–86. doi:10.1016/j.coviro.2021.07.010
87. Gravitt P, Winer R. Natural history of HPV infection across the lifespan: role of viral latency. Viruses. 2017;9(10):267. doi:10.3390/v9100267
88. Lycke KD, Steben M, Garland SM, et al. An updated understanding of the natural history of cervical human papillomavirus infection—clinical implications. Am J Clin Exp Obstet Gynecol. 2025;232(5):453–460. doi:10.1016/j.ajog.2025.02.029
89. Ryser MD, Bravo IG, Campos NG, et al. IPVS consensus statement on the natural history of cervical human papillomavirus infection. J Infect Dis. 2025. doi:10.1093/infdis/jiaf574
90. Malagón T, Louvanto K, Wissing M, et al. Hand-to-genital and genital-to-genital transmission of human papillomaviruses between male and Female Sexual Partners (hitch): a prospective cohort study. Lancet Infect Dis. 2019;19(3):317–326. doi:10.1016/s1473-3099(18)30655-8
91. González JV, Deluca GD, Liotta DJ, et al. Baseline prevalence and type distribution of human papillomavirus in sexually active non-vaccinated adolescent girls from Argentina. Revista Argentina de Microbiología. 2021;53(1):11–19. doi:10.1016/j.ram.2020.06.004
92. Liu H, Duan S, Chu W, Yang R, Wei L, Zhang S. Age-specific prevalence of multiple human papillomavirus infections in a clinical cohort of men: a cross-sectional study in Shenzhen, China. Emerg Microbes Infect. 2026;15(1). doi:10.1080/22221751.2025.2608402
93. Demarco M, Hyun N, Carter-Pokras O, et al. A study of type-specific HPV natural history and implications for contemporary cervical cancer screening programs. EClinicalMedicine. 2020;22:100293. doi:10.1016/j.eclinm.2020.100293
94. Huber J, Mueller A, Sailer M, Regidor P-A. Human papillomavirus persistence or clearance after infection in reproductive age. what is the status? Review of the literature and new data of a vaginal gel containing silicate dioxide, citric acid, and selenite. Women’s Health. 2021;17. doi:10.1177/17455065211020702
95. Fowler JR, Maani EV, Dunton CJ, et al. Cervical cancer. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
96. Perkins RB, Wentzensen N, Guido RS, Schiffman M. Cervical cancer screening. JAMA. 2023;330(6):547. doi:10.1001/jama.2023.13174
97. Wang J. Risk factors for persistent infection of high-risk HPV in patients with cervical intraepithelial neoplasia. Am J Transl Res. 2025;17(4):2992–3000. doi:10.62347/ggvr2248
98. Wang W. The impact of vaccine access difficulties on HPV vaccine intention and uptake among female university students in China. Int J Equity Health. 2025;24(1). doi:10.1186/s12939-024-02370-6
99. Balasubramaniam SD, Balakrishnan V, Oon CE, Kaur G. Key molecular events in cervical cancer development. Medicina. 2019;55(7):384. doi:10.3390/medicina55070384
100. Mittal S, Banks L. Molecular mechanisms underlying human papillomavirus E6 and E7 oncoprotein-induced cell transformation. Mutat Res/Rev Mutat Res. 2017;772:23–35. doi:10.1016/j.mrrev.2016.08.001
101. Wootton LM, Morgan EL. Ubiquitin and ubiquitin-like proteins in HPV-driven carcinogenesis. Oncogene. 2025;44(11):713–723. doi:10.1038/s41388-025-03310-6
102. Gupta R, Yadav R, Sharda A, et al. Comparative evaluation of conventional cytology and a low-cost liquid-based cytology technique, eziprepTM, for cervicovaginal smear reporting: a split sample study. CytoJournal. 2019;16:22. doi:10.4103/cytojournal.cytojournal_11_19
103. Ebisch RM, van der Horst J, Hermsen M, et al. Evaluation of p16/KI-67 dual-stained cytology as triage test for high-risk human papillomavirus-positive women. Mod Pathol. 2017;30(7):1021–1031. doi:10.1038/modpathol.2017.16
104. Harper DM, Paczos T, Ridder R, Huh WK. p16/ki-67 dual stain triage of individuals positive for HPV to detect cervical precancerous lesions. Int J Cancer. 2025;156(12):2257–2264. doi:10.1002/ijc.35353
105. Wentzensen N, Clarke MA, Bremer R, et al. Clinical evaluation of human papillomavirus screening with p16/ki-67 dual stain triage in a large organized cervical cancer screening program. JAMA Intern Med. 2019;179(7):881. doi:10.1001/jamainternmed.2019.0306
106. Perkins RB, Guido RS, Castle PE, et al. 2019 ASCCP Risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24(2):102–131. doi:10.1097/lgt.0000000000000525
107. Gravitt PE, Marks M, Kosek M, et al. Soil-transmitted helminth infections are associated with an increase in human papillomavirus prevalence and a T-helper type 2 cytokine signature in cervical fluids. J Infect Dis. 2015;213(5):723–730. doi:10.1093/infdis/jiv498
108. Descamps P, Dixon S, Bosch Jose FX, et al. Turning the tide—recommendations to increase cervical cancer screening among women who are underscreened. Int J Gynecol Obstet. 2024;166(S1):3–21. doi:10.1002/ijgo.15600
109. Hristamyan MA. Primary and secondary prophylaxis for diseases caused by human papillomavirus infections. J Cancer Prev. 2025;30(3):146–153. doi:10.15430/jcp.25.018
110. World Health Organization (WHO). WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, second Edition: Use of mRNA Tests for Human Papillomavirus (HPV). WHO; 2021.
111. Harper DM, DeMars LR. HPV vaccines – a review of the first decade. Gynecologic Oncol. 2017;146(1):196–204. doi:10.1016/j.ygyno.2017.04.004
112. Lei M, Zhao C, Zhao Y, Li J, Wei L. Immunogenicity, safety and efficacy of human papillomavirus vaccine: data from China. Front Immunol. 2024;14:1112750.
113. Li M, Zhao C, Zhao Y, Li J, Wei L. Immunogenicity, efficacy, and safety of human papillomavirus vaccine: data from China. Front Immunol. 2023;14:1112750. PMID: 36993948; PMCID: PMC10040563. doi:10.3389/fimmu.2023.1112750
114. Bobadilla ML, Villagra V, Ortiz V, Deluca G, de Paula VS. High prevalence and co-infection of high-risk Human Papillomavirus genotypes among unvaccinated young women from Paraguay. PLoS One. 2023;18(4):e0283542. PMID: 37023094; PMCID: PMC10079089. doi:10.1371/journal.pone.0283542
115. Williamson A-L. Recent developments in human papillomavirus (HPV) vaccinology. Viruses. 2023;15(7):1440. doi:10.3390/v15071440
116. World Health Organization. Human papillomavirus vaccines (HPV). Available from: https://www.who.int/teams/immunization-vaccines-andbiologicals/diseases/human-papillomavirus-vaccines-(HPV).
117. Colzani E, Johansen K, Johnson H, Pastore Celentano L. Human papillomavirus vaccination in the European Union/European Economic Area and globally: a moral dilemma. Eurosurveillance. 2021;26(50). doi:10.2807/1560-7917.es.2021.26.50.2001659
118. Amiri S, Rasekh S, Moezzi SM, et al. Prophylactic vaccines against HPV-caused cervical cancer: novel vaccines are still demanded. Infect Agent Cancer. 2025;20(1). doi:10.1186/s13027-025-00643-5
119. National Cancer Institute (NCI). Cervical cancer screening [Internet]. Bethesda (MD): National Cancer Institute; 2025. Available from: https://www.cancer.gov/types/cervical/screening.
120. Falcaro M, Soldan K, Ndlela B, Sasieni P. Effect of the HPV vaccination programme on incidence of cervical cancer and grade 3 cervical intraepithelial neoplasia by socioeconomic deprivation in England: population based observational study. BMJ. 2024;385. doi:10.1136/bmj-2023-077341
121. Dykens JA, Peterson CE, Holt HK, Harper DM. Gender neutral HPV vaccination programs: reconsidering policies to expand cancer prevention globally. Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1067299
122. Rosado C, Fernandes ÂR, Rodrigues AG, Lisboa C. Impact of human papillomavirus vaccination on male disease: a systematic review. Vaccines. 2023;11(6):1083. doi:10.3390/vaccines11061083
123. Drolet M, Bénard E, Pérez N, et al. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: updated systematic review and meta-analysis. Lancet. 2019;394(10197):497–509. doi:10.1016/s0140-6736(19)30298-3
124. Kjaer SK, Dehlendorff C, Belmonte F, Baandrup L. Real-world effectiveness of human papillomavirus vaccination against cervical cancer. J Natl Cancer Inst. 2021;113(10):1329–1335.
125. World Health Organization. Global childhood immunization levels stalled in 2023, leaving many without life-saving protection. Available from: https://www.who.int/news/item/15-07-2024-global-childhoodimmunization-levels-stalled-in-2023-leaving-many-without-lifesaving-protection.
126. Ewongwo A, Sahor AF, Ngwa W, Nwachukwu C. A guide to global access to HPV vaccination to all women in low- and middle-income countries; a minireview of innovation and equity. Front Oncol. 2024;14. doi:10.3389/fonc.2024.1380663
127. Iwami M, Bouaddi O, Razai MS, et al. Drivers of human papillomavirus vaccine uptake in migrant populations and interventions to improve coverage: a systematic review and meta-analysis. Lancet Public Health. 2025;10(8). doi:10.1016/s2468-2667(25)00148-3
128. Gilchrist SA, Nanni A. Lessons learned in shaping vaccine markets in low-income countries: a review of the vaccine market segment supported by the Gavi Alliance. Health Policy Plann. 2012;28(8):838–846. doi:10.1093/heapol/czs123
129. Khalid K, Lee KY, Mukhtar NF, Warijo O. Recommended interventions to improve human papillomavirus vaccination uptake among adolescents: a review of Quality Improvement Methodologies. Vaccines. 2023;11(8):1390. doi:10.3390/vaccines11081390
130. Khiari H, Makni K, Meddeb K, Jaidane O, Hsairi M. Cost-effectiveness of human papillomavirus (HPV) vaccination in Tunisia: a modelling study. BMJ Open. 2024;14(12). doi:10.1136/bmjopen-2024-085462
131. Mavundza EJ, Iwu-Jaja CJ, Wiyeh AB, et al. A systematic review of interventions to improve HPV vaccination coverage. Vaccines. 2021;9(7):687. doi:10.3390/vaccines9070687
132. Nunes C, McKee M, Howard N. The role of Global Health Partnerships in vaccine equity: a scoping review. PLOS Global Public Health. 2024;4(2). doi:10.1371/journal.pgph.0002834
133. Stephens ES, Dema E, McGee-Avila JK, Shiels MS, Kreimer AR, Shing JZ. Human papillomavirus awareness by educational level and by race and ethnicity. JAMA Network Open. 2023;6(11). doi:10.1001/jamanetworkopen.2023.43325
134. Grandahl M, Rosenblad A, Stenhammar C, et al. School-based intervention for the prevention of HPV among adolescents: a cluster randomised controlled study. BMJ Open. 2016;6(1). doi:10.1136/bmjopen-2015-009875
135. Krokidi E, Rao AP, Ambrosino E, Thomas PP. The impact of Health Education Interventions on HPV vaccination uptake, awareness, and acceptance among people under 30 years old in India: a literature review with systematic search. Front Reprod Health. 2023;5. doi:10.3389/frph.2023.1151179
136. Aldawood E, Alzamil L, Dabbagh D, Hafiz TA, Alharbi S, Alfhili MA. The effect of educational intervention on human papillomavirus knowledge among male and female college students in Riyadh. Medicina. 2024;60(8):1276. doi:10.3390/medicina60081276
137. Rafeie L, Vizeshfar F, Nick N. The effect of education based on planned behavior theory on women’s knowledge and attitudes about human papillomavirus. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-69340-4
138. International Papillomavirus Society. International HPV awareness day campaign report 2024 [Internet]; 2025. Available from: https://www.askabouthpv.org/assets/downloads/HPV_Awareness_Day2024_PostCampaign_Report_V13.pdf.
139. Del Pino M, Vorsters A, Joura EA, et al. Risk factors for human papillomavirus infection and disease: a targeted literature summary. J med virol. 2024;96(2). doi:10.1002/jmv.29420
140. Yang D, Zhang J, Cui X, Ma J, Wang C, Piao H. Risk factors associated with human papillomavirus infection, cervical cancer, and precancerous lesions in large-scale population screening. Front Microbiol. 2022;13. doi:10.3389/fmicb.2022.914516
141. Zou K, Huang Y, Li Z. Prevention and treatment of human papillomavirus in men benefits both men and women. Front Cell Infect Microbiol. 2022;12. doi:10.3389/fcimb.2022.1077651
142. Gutierrez D, Tan A, Strome A, Pomeranz MK. Dental dams in dermatology: an underutilized barrier method of protection. Int J Women Dermatol. 2022;8(1). doi:10.1097/jw9.0000000000000008
143. Smith JS, Backes DM, Hudgens MG, et al. Male circumcision reduces penile HPV incidence and persistence: a randomized controlled trial in Kenya. Cancer Epidemiol Biomarkers Prev. 2021;30(6):1139–1148. doi:10.1158/1055-9965.epi-20-1272
144. Shapiro SB, Laurie C, El-Zein M, Franco EL. Association Between Male Circumcision and Human Papillomavirus Infection in Males and Females: A Systematic Review, Meta-Analysis, and Meta-Regression; 2022. doi:10.1101/2022.08.08.22278357
145. Eun TJ, Perkins RB. Screening for cervical cancer. Med Clin North Am. 2020;104(6):1063–1078. doi:10.1016/j.mcna.2020.08.006
146. Bedell SL, Goldstein LS, Goldstein AR, Goldstein AT. Cervical cancer screening: past, present, and future. Sexual Med Rev. 2019;8(1):28–37. doi:10.1016/j.sxmr.2019.09.005
147. Wentzensen N, Arbyn M. HPV-based cervical cancer screening- facts, fiction, and misperceptions. Prevent Med. 2017;98:33–35. doi:10.1016/j.ypmed.2016.12.040
148. Carvalho CF, Teixeira JC, Bragança JF, Derchain S, Zeferino LC, Vale DB. Cervical cancer screening with HPV testing: updates on the recommendation. Revista Brasileira de Ginecologia e Obstetrícia / RBGO Gynecology and Obstetrics. 2022;44(03):264–271. doi:10.1055/s-0041-1739314
149. World Health Organization. Self-care interventions: human papillomavirus (HPV) self-sampling as part of cervical cancer screening and treatment, 2022 update. Available from: https://www.who.int/publications-detail-redirect/WHO-SRH-23.1
150. Mannam G, Miller JW, Johnson JS, et al. HPV and penile cancer: epidemiology, risk factors, and clinical insights. Pathogens. 2024;13(9):809. doi:10.3390/pathogens13090809
151. Ren W, Jin Y, Shi L, et al. The necessity and challenges of human papillomavirus testing for men. Front Cell Infect Microbiol. 2025;15. doi:10.3389/fcimb.2025.1563499
152. Bhatla N, Singhal S. Primary HPV screening for cervical cancer. Best Pract Res Clin Obstet Gynaecol. 2020;65:98–108. doi:10.1016/j.bpobgyn.2020.02.008
153. U.S. Preventive Services Task Force. Cervical cancer: screening [Internet]. Rockville (MD): U.S. Preventive Services Task Force; 2018. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/cervical-cancer-screening.
154. American Cancer Society. Cervical cancer early detection, diagnosis, and staging. Available from: https://www.cancer.org/cancer/types/cervical-cancer/detection-diagnosis-staging/cervical-cancer-screening-guidelines.html.cancer.org|1.800.227.2345.
155. Australian Government Department of Health. National cervical screening program [Internet]. Canberra: Australian Government Department of Health; 2025. Available from: https://www.health.gov.au/our-work/national-cervical-screening-program?language=en.
156. Shastri SS, Temin S, Almonte M, et al. Secondary prevention of cervical cancer: ASCO resource-stratified guideline update. JCO Glob Oncol. 2022;8:e2200217. PMID: 36162041; PMCID: PMC9812449. doi:10.1200/GO.22.00217
157. European Commission, Joint Research Centre and International Agency for Research on Cancer, Taghavi K, Dimitrova N, Basu P, Garcia EM, Janusch R, EC-CvC at a Glance. European Commission Initiative on Cervical Cancer. Publications Office of the European Union, Luxembourg; 2025. Available from: https://data.europa.eu/doi/10.2760/2601357.
158. Kyrgiou M, Arbyn M, Bergeron C, et al. Cervical screening: ESGO-EFC position paper of the European Society of Gynaecologic Oncology (ESGO) and the European Federation of Colposcopy (EFC). Br J Cancer. 2020;123(4):510–517. PMID: 32507855; PMCID: PMC7434873. doi:10.1038/s41416-020-0920-9
159. Kunckler M, Schumacher F, Kenfack B, et al. Cervical cancer screening in a low-resource setting: a pilot study on an hpv-based screen-and-treat approach. Cancer Med. 2017;6(7):1752–1761. doi:10.1002/cam4.1089
160. Davies P, Aluloski I, Aluloski D, et al. HPV vaccination and cervical cancer screening policies and practices in 18 countries, territories and entities across Eastern Europe and Central Asia. Asian Pac J Cancer Prev. 2023;24(5):1781–1788. doi:10.31557/apjcp.2023.24.5.1781
161. Ussai S, Seyidov T, Blanqué Catalina N, Khomasuridze T. Cervical screening systems in Eastern Europe and Central Asia: a comparative policy evaluation. Healthcare. 2025;13(22):2889. doi:10.3390/healthcare13222889
162. Sabeena S, Ravishankar N, Kalpana M. Implementation strategies of cervical cancer screening in South Asia: a systematic review. Int J Gynecol Obstet. 2024;166(2):483–493. doi:10.1002/ijgo.15366
163. Thrall MJ, McCarthy E, Mito JK, Rao J. Triage options for positive high-risk HPV results from HPV-based cervical cancer screening: a review of the potential alternatives to Papanicolaou test cytology. J Am Soc Cytopathol. 2025;14(1):11–22. doi:10.1016/j.jasc.2024.09.003
164. Yang DX, Soulos PR, Davis B, Gross CP, Yu JB. Impact of widespread cervical cancer screening. Am J Clin Oncol. 2018;41(3):289–294. doi:10.1097/coc.0000000000000264
165. Chrysostomou AC, Stylianou DC, Constantinidou A, Kostrikis LG. Cervical cancer screening programs in Europe: the transition towards HPV vaccination and population-based HPV testing. Viruses. 2018;10(12):729. doi:10.3390/v10120729
166. Curry SJ, Krist AH, Owens DK, et al. Screening for cervical cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;320(7):674–686. doi:10.1001/jama.2018.10897
167. Sathawane P, Kamal MM, Deotale PR, Mankar H. Nuances of the Papanicolaou stain. Cytojournal. 2022;19:43. doi:10.25259/cmas_03_18_2021
168. Hashmi AA, Naz S, Ahmed O, et al. Comparison of liquid-based cytology and conventional Papanicolaou smear for cervical cancer screening: an experience from Pakistan. Cureus. 2020. doi:10.7759/cureus.12293
169. Makde MM, Sathawane P. Liquid-based cytology: technical aspects. Cytojournal. 2022;19:41. doi:10.25259/cmas_03_16_2021
170. Patel N, Bavikar R, Buch A, Kulkarni M, Dharwadkar A, Viswanathan V. A comparison of conventional pap smear and liquid-based cytology for cervical cancer screening. Gynecol Minim Invasive Ther. 2023;12(2):77–82. Erratum in: Gynecol Minim Invasive Ther. 2024 Feb;13(1):68. doi: 10.4103/gmit.gmit_21_24. PMID: 37416097; PMCID: PMC10321340. doi:10.4103/gmit.gmit_118_22
171. Ezzat N, Abusinna E. Comparison between conventional pap smear and liquid-based cytology in cervical cancer screening. Egypt J Pathol. 2019;39(2):280. doi:10.4103/egjp.egjp_36_19
172. Smith SK, Nwosu O, Edwards A, et al. Performance of screening tools for cervical neoplasia among women in low- and middle-income countries: a systematic review and meta-analysis. PLOS Global Public Health. 2023;3(2).
173. Pankaj S, Nazneen S, Kumari S, et al. Comparison of conventional Pap smear and liquid-based cytology: a study of cervical cancer screening at a tertiary care center in Bihar. Indian J Cancer. 2018;55(1):80–83. PMID: 30147099. doi:10.4103/ijc.IJC_352_17
174. Nishio H, Iwata T, Nomura H, et al. Liquid-based cytology versus conventional cytology for detection of uterine cervical lesions: a prospective observational study. Jpn J Clin Oncol. 2018;48(6):522–528. doi:10.1093/jjco/hyy050
175. Engh MA, Teutsch B, Schulze Wenning A, Kói T, Hegyi P, Erőss B. Combined liquid-based cytology and conventional smear provides better sensitivity and adequacy rates after endoscopic ultrasound-guided tissue acquisition of abdominal masses: a systematic review and meta-analysis. J Clin Med. 2025;14(18):6685. doi:10.3390/jcm14186685
176. Ramírez AT, Valls J, Baena A, et al. Performance of cervical cytology and HPV testing for primary cervical cancer screening in Latin America: an analysis within the estampa study. Lancet Reg Health Am. 2023;26:100593. doi:10.1016/j.lana.2023.100593
177. Gottschlich A, Gondara L, Smith LW, et al. Human papillomavirus-based screening at extended intervals missed fewer cervical precancers than cytology in the HPV for cervical cancer (HPV focal) trial. Int J Cancer. 2022;151(6):897–905.
178. Castle PE, Kinney WK, Cheung LC, et al. Why does cervical cancer occur in a state-of-the-art screening program?. Gynecologic Oncol. 2017;146(3):546–553. doi:10.1016/j.ygyno.2017.06.003
179. Srisomboon S, Tantipalakorn C, Charoenkwan K, Srisomboon J. Cervical screening results leading to detection of adenocarcinoma in situ of the uterine cervix. Asian Pac J Cancer Prev. 2019;20(2):377–382. doi:10.31557/apjcp.2019.20.2.377
180. Lohiya A, Daniel R, Kumar D, et al. Effectiveness of visual inspection with acetic acid (via) screening on cervical cancer mortality and incidence - A systematic review and meta-analysis. Asian Pac J Cancer Prev. 2022;23(2):399–407. doi:10.31557/apjcp.2022.23.2.399
181. Baena A, Mesher D, Salgado Y, et al. Performance of visual inspection of the cervix with acetic acid (VIA) for triage of HPV screen-positive women: results from the ESTAMPA study. Int J Cancer. 2022;152(8):1581–1592. doi:10.1002/ijc.34384
182. Wang S, Dang L, Liu S, et al. Cervical cancer screening via visual inspection with acetic acid and Lugol iodine for triage of HPV-positive women. JAMA Network Open. 2024;7(3). doi:10.1001/jamanetworkopen.2024.4090
183. Adsul P, Manjunath N, Srinivas V, Arun A, Madhivanan P. Implementing community-based cervical cancer screening programs using visual inspection with acetic acid in India: a systematic review. Cancer Epidemiol. 2017;49:161–174. doi:10.1016/j.canep.2017.06.008
184. Kelly H, Jaafar I, Chung M, et al. Diagnostic accuracy of cervical cancer screening strategies for high-grade cervical intraepithelial neoplasia (cin2+/cin3+) among women living with HIV: a systematic review and meta-analysis. eClinicalMedicine. 2022;53:101645. doi:10.1016/j.eclinm.2022.101645
185. Frund C, Kenfack B, Sormani J, et al. Training, supervision, and Competence Assessment of Cameroonian Health Care Providers using HPV self-sampling, triage by visual inspection, and treatment by thermal ablation in a single visit. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.875177
186. Yeates K, Erwin E, Mtema Z, et al. Smartphone-enhanced training, QA, monitoring, and evaluation of a platform for secondary prevention of cervical cancer: opportunities and challenges to implementation in Tanzania. JCO Global Oncol. 2020;6:1114–1123. doi:10.1200/go.20.00124
187. Ogilvie GS, van Niekerk D, Krajden M, et al. Effect of screening with primary cervical HPV testing vs cytology testing on high-grade cervical intraepithelial neoplasia at 48 months. JAMA. 2018;320(1):43. doi:10.1001/jama.2018.7464
188. Li Z-F, Jia X-H, Feng X, et al. Comparison of primary cytology, primary HPV testing and co-testing as cervical cancer screening for Chinese women: a population-based screening cohort. BMJ Open. 2022;12(10). doi:10.1136/bmjopen-2022-063622
189. Arbyn M, Simon M, de Sanjosé S, et al. Accuracy and effectiveness of HPV mrna testing in cervical cancer screening: a systematic review and meta-analysis. Lancet Oncol. 2022;23(7):950–960. doi:10.1016/s1470-2045(22)00294-7
190. Mousavi A-S, Pouryasin A, Yarandi F, et al. Assessment of cervical cancer molecular-based screening tools; HPV-DNA detection versus E6/E7 mrna testing; first report of a prospective cohort study among Iranian women. Iran J Public Health. 2020. doi:10.18502/ijph.v49i9.4093
191. Maver PJ, Poljak M. Primary HPV-based cervical cancer screening in Europe: implementation status, challenges, and future plans. Clin Microbiol Infect. 2020;26(5):579–583. doi:10.1016/j.cmi.2019.09.006
192. Arbyn M, et al. HPV detection and typing. Hum Papillomavirus E-Lab Man. 2025;1–36.
193. Bellosillo B, Ibáñez R, Roura E, et al. Clinical validation of the VITRO HPV screening assay for its use in primary cervical cancer screening. Cancers. 2024;16(7):1322. doi:10.3390/cancers16071322
194. Sundström K, Lamin H, Dillner J. Validation of the cobas 6800 human papillomavirus test in primary cervical screening. PLOS ONE. 2021;16(2). doi:10.1371/journal.pone.0247291
195. Lagström S, Løvestad AH, Umu SU, et al. HPV16 and HPV18 type-specific APOBEC3 and integration profiles in different diagnostic categories of cervical samples. Tumour Virus Res. 2021;12:200221. doi:10.1016/j.tvr.2021.200221
196. Sawaya GF, Dorismond VG. Avoiding low-value care and patient financial harm in cervical cancer screening. Cancer Prev Res. 2023;16(7):363–364. PMID: 37403658. doi:10.1158/1940-6207.CAPR-23-0173
197. Schiffman M, Kinney WK, Cheung LC, et al. Relative performance of HPV and cytology components of cotesting in cervical screening. J Natl Cancer Inst. 2018;110(5):501–508. doi:10.1093/jnci/djx225
198. Mathews CS, Sargent A, Cuschieri K, et al. HPValidate—human papillomavirus testing with DNA and mrna assays on self-collected samples in cervical screening: comparison of test characteristics on three self-sampling devices. Br J Cancer. 2025;133(5):665–673. doi:10.1038/s41416-025-03102-5
199. Tranberg M, Jensen JS, Bech BH, Andersen B. Urine Collection in cervical cancer screening – analytical comparison of two HPV DNA assays. BMC Infect Dis. 2020;20(1). doi:10.1186/s12879-020-05663-7
200. Di Gennaro G, Licata F, Trovato A, Bianco A. Does self-sampling for human papilloma virus testing have the potential to increase cervical cancer screening? An updated meta-analysis of observational studies and randomized clinical trials. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.1003461
201. Rakhat A, Marat A, Sakhipova G, Sakko Y, Aimagambetova G. Self-sampling modality for cervical cancer screening: overview of the diagnostic approaches and sampling devices. Sci. 2026;8(1):5. doi:10.3390/sci8010005
202. Chao YS, McCormack S. HPV Self-Sampling for Primary Cervical Cancer Screening: A Review of Diagnostic Test Accuracy and Clinical Evidence – An Update. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2019.
203. Mekuria SF, Timmermans S, Borgfeldt C, Jerkeman M, Johansson P, Linde DS. HPV self-sampling versus healthcare provider collection on the effect of cervical cancer screening uptake and costs in LMIC: a systematic review and meta-analysis. Syst Rev. 2023;12(1). doi:10.1186/s13643-023-02252-y
204. Costa S, Verberckmoes B, Castle PE, Arbyn M. Offering HPV self-sampling kits: an updated meta-analysis of the effectiveness of strategies to increase participation in cervical cancer screening. Br J Cancer. 2022;128(5):805–813. doi:10.1038/s41416-022-02094-w
205. Aimagambetova G, Atageldiyeva K, Marat A, et al. Comparison of diagnostic accuracy and acceptability of self-sampling devices for human Papillomavirus detection: a systematic review. Prev Med Rep. 2024;38:102590. PMID: 38283967; PMCID: PMC10821625. doi:10.1016/j.pmedr.2024.102590
206. Abodunrin OR, Akinsolu FT, Ola OM, et al. Acceptability of human papillomavirus self-sampling among women living with HIV in sub-Saharan Africa: a systematic review and meta-analysis. PLOS Global Public Health. 2025;5(5). doi:10.1371/journal.pgph.0004605
207. Brewer N, Bartholomew K, Grant J, et al. Acceptability of human papillomavirus (HPV) self-sampling among never- and under-screened indigenous and other minority women: a randomised three-arm community trial in Aotearoa New Zealand. Lancet Reg Health West Pac. 2021;16:100265. doi:10.1016/j.lanwpc.2021.100265
208. Le Goff J, Le Duc-Banaszuk A-S, Lefeuvre C, et al. Acceptance of self-sampling by women not regularly participating in cervical cancer screening in areas with low medical density: a qualitative study within the French capu4 trial. Cancers. 2024;16(11):2066. doi:10.3390/cancers16112066
209. Wong EL-Y, Cheung AW-L, Wong AY-K, Chan PK-S. Acceptability and feasibility of HPV self-sampling as an alternative primary cervical cancer screening in under-screened population groups: a cross-sectional study. Int J Environ Res Public Health. 2020;17(17):6245. doi:10.3390/ijerph17176245
210. da Pereira S, Nobre L, Ribeiro M, et al. Targeting under-screened women in cervical cancer: combining self-sampling and human papillomavirus testing with a strategic reminder plan. Eur J Public Health. 2025;35(5):984–991. doi:10.1093/eurpub/ckaf122
211. Drysdale H, Marlow LA, Lim A, Sasieni P, Waller J. Self-sampling for cervical screening offered at the point of invitation: a cross-sectional study of preferences in England. J Med Screen. 2022;29(3):194–202. doi:10.1177/09691413221092246
212. Ganguly AP, Pretsch PK, Brewer NT, et al. Streamlined self-collection screening for sexually transmitted infections and human papillomavirus. JAMA Network Open. 2026;9(1). doi:10.1001/jamanetworkopen.2025.51345
213. Serrano B, Ibáñez R, Robles C, Peremiquel-Trillas P, de Sanjosé S, Bruni L. Worldwide use of HPV self-sampling for cervical cancer screening. Prevent Med. 2022;154:106900. doi:10.1016/j.ypmed.2021.106900
214. Yimer NB, Mohammed MA, Solomon K, et al. Cervical cancer screening uptake in Sub-Saharan Africa: a systematic review and meta-analysis. Public Health. 2021;195:105–111. doi:10.1016/j.puhe.2021.04.014
215. Petersen Z, Jaca A, Ginindza TG, et al. Barriers to uptake of cervical cancer screening services in low-and-middle-income countries: a systematic review. BMC Women’s Health. 2022;22(1). doi:10.1186/s12905-022-02043-y
216. Issa T, Babi A, Azizan A, et al. Factors associated with cervical cancer screening behaviour of women attending gynaecological clinics in Kazakhstan: a cross-sectional study. Womens Health. 2021;17:17455065211004135. PMID: 33784210; PMCID: PMC8013635. doi:10.1177/17455065211004135
217. Getachew S, Getachew E, Gizaw M, Ayele W, Addissie A, Kantelhardt EJ. Cervical cancer screening knowledge and barriers among women in Addis Ababa, Ethiopia. PLOS ONE. 2019;14(5). doi:10.1371/journal.pone.0216522
218. Asthana S, Devarapalli P, Labani S, Nagarjuna N, Panchal P. Barriers affecting uptake of cervical cancer screening in low and middle income countries: a systematic review. Indian J Cancer. 2018;55(4):318. doi:10.4103/ijc.ijc_253_18
219. Belay Y, Dheresa M, Sema A, Desalew A, Assefa N. Cervical cancer screening utilization and associated factors among women aged 30 to 49 years in Dire Dawa, Eastern Ethiopia. Cancer Control. 2020;27(1). doi:10.1177/1073274820958701
220. Desta M, Getaneh T, Yeserah B, et al. Cervical cancer screening utilization and predictors among eligible women in Ethiopia: a systematic review and meta-analysis. PLOS ONE. 2021;16(11). doi:10.1371/journal.pone.0259339
221. Musa J, Achenbach CJ, O’Dwyer LC, et al. Effect of cervical cancer education and provider recommendation for screening on screening rates: a systematic review and meta-analysis. PLOS ONE. 2017;12(9). doi:10.1371/journal.pone.0183924
222. Getaneh A, Tegene B, Belachew T. Knowledge, attitude and practices on cervical cancer screening among undergraduate female students in University of Gondar, Northwest Ethiopia: an Institution based Cross Sectional Study. BMC Public Health. 2021;21(1). doi:10.1186/s12889-021-10853-2
223. Yosef T, Birhanu B, Shifera N, Bekele BB, Asefa A. Determinants of cervical cancer screening uptake among reproductive-age women in southwest Ethiopia: a case-control study. Front Oncol. 2024;14. doi:10.3389/fonc.2024.1424810
224. Maree JE, Kampinda-Banda M. Knowledge and practices of cervical cancer and its prevention among malawian women. J Cancer Educ. 2020;35(1):86–92. doi:10.1007/s13187-018-1443-4
225. Wanyenze RK, Bwanika JB, Beyeza-Kashesya J, et al. Uptake and correlates of cervical cancer screening among HIV-infected women attending HIV care in Uganda. Global Health Action. 2017;10(1). doi:10.1080/16549716.2017.1380361
226. Ndejjo R, Mukama T, Musabyimana A, Musoke D. Uptake of cervical cancer screening and associated factors among women in rural Uganda: a cross sectional study. PLOS ONE. 2016;11(2). doi:10.1371/journal.pone.0149696
227. Ampofo AG, Adumatta AD, Owusu E, Awuviry-Newton K. A cross-sectional study of barriers to cervical cancer screening uptake in Ghana: an application of the health belief model. PLOS ONE. 2020;15(4). doi:10.1371/journal.pone.0231459
228. Kangmennaang J, Onyango EO, Luginaah I, Elliott SJ. The next sub saharan African epidemic? A case study of the determinants of cervical cancer knowledge and screening in Kenya. Soc sci med. 2018;197:203–212. doi:10.1016/j.socscimed.2017.12.013
229. Kassie AM, Abate BB, Kassaw MW, Aragie TG, Geleta BA, Shiferaw WS. Impact of knowledge and attitude on the utilization rate of cervical cancer screening tests among Ethiopian women: a systematic review and meta-analysis. PLOS ONE. 2020;15(12). doi:10.1371/journal.pone.0239927
230. Nishimura H, Yeh PT, Oguntade H, Kennedy CE, Narasimhan M. HPV self-sampling for cervical cancer screening: a systematic review of values and preferences. BMJ Glob Health. 2021;6(5):e003743. PMID: 34011537; PMCID: PMC8137189. doi:10.1136/bmjgh-2020-003743
231. Boyard J, Caille A, Brunet-Houdard S, et al. A home-mailed versus general practitioner-delivered vaginal self-sampling kit for cervical cancer screening: a cluster randomized controlled trial with a cost-effectiveness analysis. J Women’s Health. 2022. doi:10.1089/jwh.2021.0597
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
“Barriers and Advantages of Self-Sampling Tests, for HPV Diagnosis: A Qualitative Field Experience Before Implementation in a Rural Community in Ecuador”
Vega-Crespo B, Neira VA, Maldonado - Rengel R, López D, Delgado-López D, Guerra Astudillo G, Verhoeven V
International Journal of Women's Health 2024, 16:947-960
Published Date: 28 May 2024
A Survey of Physicians and Patients in Pakistan Assessing the Improvement of Visualization of the Cervix, Ease of Use, and Patient Comfort Using a Newly Designed Vaginal Speculum: A Pilot Study

Khan S, Waters-Kellar L, Barsh E, Shannon A, Clark S, Ryznar RJ, Trawick A, Payton M, Bouquet J
Medical Devices: Evidence and Research 2025, 18:309-317
Published Date: 11 June 2025
High-Risk HPV Persistence and Clearance Patterns Among Women in Ethiopia: A Longitudinal Study
Teka B, Addissie A, Mihret A, Gizaw M, Shiferaw W, Chanyalew Z, Kaufmann AM, Kantelhardt EJ, Abebe T
International Journal of Women's Health 2025, 17:3799-3810
Published Date: 22 October 2025
Demographic and Screening-to-Diagnosis Cascade Indicators for Risk Stratification in an Organized Cervical Cancer Screening Program: Evidence from 82,141 Women in Yunnan, China
Fan M, Yang F, Zhang D, Dang H, Lai S, Li Y, Chen X, Zhou A, Hai Q, Liu T, Lin J
International Journal of Women's Health 2026, 18:602135
Published Date: 3 June 2026