Back to Journals » Drug, Healthcare and Patient Safety » Volume 15
Delta-8, a Cannabis-Derived Tetrahydrocannabinol Isomer: Evaluating Case Report Data in the Food and Drug Administration Adverse Event Reporting System (FAERS) Database
Authors Simon TA, Simon JH, Heaning EG, Gomez-Caminero A, Marcu JP
Received 4 November 2022
Accepted for publication 16 January 2023
Published 29 January 2023 Volume 2023:15 Pages 25—38
DOI https://doi.org/10.2147/DHPS.S391857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Siew Siang Chua
Teresa A Simon,1 John H Simon,1 Erin G Heaning,1 Andres Gomez-Caminero,1 Jahan P Marcu1,2
1Physicians Research Center, LLC, Toms River, NJ, USA; 2Marcu Enterprises, Jersey City, NJ, USA
Correspondence: Teresa A Simon, Physicians Research Center, LLC, Toms River, NJ, 08753, USA, Tel +732 818-7900, Fax +732 557-0217, Email [email protected]
Purpose: The aim of this study was to characterize the frequency of adverse effects where delta-8 tetrahydrocannabinol (D8-THC) was identified as a possible suspect drug in the FDA Adverse Event Reporting System (FAERS) database.
Methods: A case-series design was used.
Results: A total of 183 cases listed D8-THC as a suspect drug in FAERS as of June 30, 2021. The most common events included dyspnea, respiratory disorder, and seizure. The reporting odds ratios were consistently and significantly greater than 2, a 2-fold increase from 2019 to 2021, indicating a potential safety signal.
Conclusion: The first report of D8-THC, in the FAERS database, as a suspect drug appears to be in 2011. Overall, there are 183 total cases listing D8-THC as a suspect drug in the FAERS database as of June 30, 2021. Of the 183 cases, most were respiratory in nature.
Keywords: cannabis, hemp-derived, safety, adverse effects, public health, cannabinoid, delta-8 tetrahydrocannabinol, hemp, adverse event
Plain Language Summary
There exists a lack of nationally representative, real-world data on the benefits and risks associated with hemp-derived products. This study aims to address this gap by identifying the unexpected medical problems for consumers of these products. In total, this study identified 183 cases which listed D8-THC as a suspect drug in the FDA Adverse Event Reporting System (FAERS) database. The most common adverse events included dyspnea, respiratory disorders, and seizures. Future work focusing on reliable, comprehensive safety data will promote progress in identifying risk of hemp-derived products and making them safer for consumers.
Introduction
In the United States, you can walk by shops and kiosks that have stacks of delta-8-tetrahydrocannabinol (D8-THC) products on their shelves. This ingredient is an isomer of delta-9-tetrahydrocannabinol (D9-THC) the well-known psychoactive ingredient in cannabis. D8-THC and other D9-THC isomer products have mysteriously flooded the market with confusing label information while resembling commercially available food products. The products are often characterized as hemp-derived products, meaning the main ingredient is artificially derived (aka synthesized or semi-synthesized) from cannabidiol (CBD) that is sourced from hemp. If asked, a shopkeeper may state that D8-THC and D9-THC are reported to have similar pharmacological activities.1 Limited evidence from basic and clinical research suggests that D8-THC can be less potent than D9-THC at creating a cannabis-like high.2 Unfortunately, hemp-derived products containing D8-THC and other isomers may have a greater probability of contamination or adulteration due to the synthetic processing and a lack of regulatory requirements, as compared to medical or adult-use cannabis products from state licensed operators.
Many hemp operators (ie, cultivators, manufacturers, distributors, etc.) in the United States argue that the Agricultural Improvement Act of 2018 (aka the Hemp Farm Bill) created a loophole for THC “rich” compounds to be considered as “hemp products” and not “cannabis” products.3 This seems to have allowed privileges to any entity wishing to create and distribute drugs that they claim are derived from CBD.3 According to legal experts, the intention of the 2018 Hemp Farm Bill was to allow farmers to produce industrial hemp products (ie, textiles, fuel, and largely other non-consumables) and was not intended to allow the sale of products that are laced with psychotropic substances derived from CBD as the reactant.4
In December 2018, congressional approval of the Hemp Farm Bill amended the federal Controlled Substances Act to exclude hemp from the Schedule I definition of marijuana. Hemp is being defined as cannabis plants and products containing less than 0.3% THC in the United States. The statute remains silent on D8-THC and other isomers. The legislation does not explicitly state that certain isomers of THC are still Schedule I or which THC-isomer products exceed the 0.3% THC limit. Under this “0.3.% rule”, hemp edibles can exceed the THC limit imposed for cannabis edibles (eg, 10mg THC maximum in most jurisdictions for cannabis products), as hemp is determined by the percent weight of THC – not a specific amount per dose or unit.5 Basically, you may be able to buy more edible THC at a gas station than you are able to at a licensed cannabis dispensary.
Outside of the hemp industry, federal6,7 agencies maintain that all THC-type compounds (ie, D8-THC) and synthesis thereof remain a Schedule I issue.8 In 2020, the Drug Enforcement Administration (DEA) clarified the status of D8-THC regarding the Farm Bill saying, “all synthetically derived tetrahydrocannabinols (THC) remain Schedule I controlled substances”.1 The DEA specifically lists D8-THC as a Schedule I substance under the category “tetrahydrocannabinols”. Despite this explanation, D8-THC and related isomers made from CBD are sold without oversight, under the guise of the Hemp Farm Bill. This has led to D8-THC and other isomers becoming the highest growth market area for hemp. To clarify, D8-THC can occur in cannabis and hemp plants but only in minuscule quantities from the natural degradation of D9-THC.9,10 The process of manufacturing and marketing D8-THC-containing hemp products is reminiscent of designer drugs (ie, K2, spice, etc.) from the recent past, which seems to borrow legitimacy with false-hearted comparisons to regulated cannabis products and pharmaceutical cannabinoids.9 As a court-qualified synthetic drug expert stated, “we have been here before, synthetic cannabinoids are very different from cannabis”.10,11
An increase in D8-THC use led to a notable increase in cases of intoxication and nonfatal overdose to poison control centers and emergency room visits in the US. This has raised concerns on the safety of products containing or labeled as D8-THC derived from hemp or CBD. On September 14th, 2021, the Food and Drug Administration (FDA) and Centers for Disease Control (CDC) both issued Health Warnings regarding D8-THC.12,13 Presently, efficacy and safety has only been demonstrated for a few pharmaceutically licensed preparations, through traditional FDA drug approval processes, eg, Syndros™, Marinol™, and Epidiolex™. D8-THC products are currently not FDA approved.
The US FDA Adverse Event Reporting System (FAERS) database is currently the only national reporting system that has the capability to monitor the safety of products including products that are not FDA approved. FAERS is a signal detection tool and an increase in specific AEs indicates that there is a potential unidentified risk. A signal observed in FAERS may have large public health significance since only a small fraction of AEs are reported into FAERS.14
We sought to use the only known national database (ie, FAERS) to evaluate cannabis and hemp-derived products, specifically D8-THC. The aim of the study was to identify cases of AEs where D8-THC was identified as a possible suspect drug in the FDA FAERS database.
Methods
Data Source and Collection
The FAERS database structure adheres to the international safety reporting guidance issued by the International Conference on Harmonization, ICH E2B. Adverse events and medication errors are coded using terms in the Medical Dictionary for Regulatory Activities (MedDRA) terminology.15 Reports can be submitted by healthcare professionals and consumers through the “MedWatch” program.16–18 The original FAERS system was started in 1969. In 1997, it underwent a major revision resulting in an increase in reporting.19,20 To date, the FAERS is the largest repository of spontaneously reported AEs in the world with more than 22 million total reports.19,20 The FDA releases these data to the public. Public access allows external researchers to explore these data through pharmacoepidemiologic/pharmacovigilance analyses. It has also evolved to allow broader public health utilization, as Healthcare Professionals (HCP) and consumers can report AEs/side effects from any medication or product.
There are a series of tables available in the FDA FAERS dataset including: case demographics (sex, age, weight), suspect drug, and a list of all suspect drugs; report to the FDA dates, outcomes, reactions (AE), indications for use, reporter (consumer, healthcare provider, not specified) administrative information (DEMO), drug/biologic information (DRUG), a, drug therapy start and end dates (THER). The drugs in the DRUG table are assigned as any of primary suspect, secondary suspect, concomitant, or interacting. The AEs in the REAC (reaction) table are coded using the preferred terms (PTs) in MedDRA. FAERS permits the reporting of random drug names, including trade names and abbreviations. Spelling errors and drug combinations of interest were reviewed by the authors. A case can have multiple events reported, and each event or AE will be listed; therefore, the number of events will be greater than the number of cases.
For simplicity, system organ class (SOC) will be used to represent the “reaction group”/body system. Preferred Term (PT) will represent the “reaction” or AE that was reported. D8-THC will be used to represent all formulations/combinations of D8-THC identified in FAERS.
Descriptive data analyses (total number of cases and percentages) were performed. Subset analyses were performed and evaluated as a case series where we analyzed AEs caused by drugs, not by disease state. Disproportionality analysis was performed using the relative odds ratio (ROR) to detect unexpected (spontaneous) signals. Our approach allows for the detection of increased frequencies of drug-related AEs21 using a case/no case method. “Cases” are defined as a person who reported exposure to a specific drug and who also reported a specific AE, while all other possible pairs are “non-cases”. The calculation for ROR uses a two-by-two contingency table reporting event counts for each specific drug and all other drugs. ROR represents the odds that an outcome will occur given a particular exposure and is a measure of an association between an exposure to a drug, and the odds a specific outcome will occur.22 The Yates Correction is recommended when expected cell frequencies are below 10 or even 5. For these data, none of the expected cells were below 10 and given the large sample size of the FAERS database and the Yates correction was not applied. We did, however, have circumstances where there were 0 cases in the observed. For this, we assigned a 0.5 to the cell per the Cochrane handbook.23 All data processing and statistical analyses were performed using Excel (version 2201).
An ROR signal is defined positive if the lower limit of the 95% confidence interval (CI) is greater than 1.24 The 95% CI gives an indication of the precision of the estimate of the ROR. As with proportional reporting ratios, an ROR value equal to 2 or greater can be used as a threshold; however, the lower bound of the 95% CI is preferred. For this analysis, the odds of reports of the pre-specified event with the product of interest (D8-THC) are 2x (two times) higher than the odds of the event occurring among all other reports in the database (FAERS).
ROR = (a*d)/(c*b)
95% CI = Lower 95% CI = eln(OR) – 1.96√(1/a + 1/b + 1/c + 1/d) and
Upper 95% CI = eln(OR) + 1.96√(1/a + 1/b + 1/c + 1/d)
This reference risk is believed to reflect the baseline risk of the reported event in a person exposed to that product provided there is no specific association between the product and the event of interest. A possible limitation is if the reference risk provides an accurate estimate of the baseline risk of an event for a person receiving a product since the rate is calculated by using a group of medications (products) that include treatments that may be known for the event of interest. It has been theorized that the ROR may have an advantage over the proportional reporting ratio by estimating the relative risk. Both are disproportionality measures and do not allow for risk quantification. These measures and analytical tools assist in the possibility of identifying an indication of the strength of a signal.25
Analyses of the data extracted from the FAERS database included all cases with suspect drug D8-THC. The first data extraction was performed on March 11, 2021, and it included data from 2011 to December 2020. A subsequent data extraction was performed with the last being September 14, 2021 and included data up to June 30, 2021. For this analysis, the specific drug search terms in this evaluation included D8-THC; D8-THC/device/herbals; D8-THC/device/herbals/nicotine; D8-THC/herbals. Prior to data mining, all duplicate reports were deleted according to the FDA’s recommendation by utilizing the most recent case number. There were no duplicates identified. The number of reports remained at 183.
Results
Descriptive Results on D8-THC Cases
Overall Cases of D8-THC in FAERS
The data extraction period covered 2011 to June 30, 2021. The first report of a D8-THC suspect drug was in 2011. Overall, there are 183 total cases listing D8-THC as a suspect drug in the FAERS database as of June 30, 2021. Of the 183 cases, most are respiratory in nature. There are a total of 937 AEs with 322 individual MedDRA PT terms. A case can experience/report more than one AE.
Table 1 presents the cases overall, by seriousness, deaths, non-serious and hospitalizations. Excluding deaths, 109 (60%) were deemed serious of these, 45% resulted in a reported hospitalization. Most cases were in males between 18 and 64 years of age.
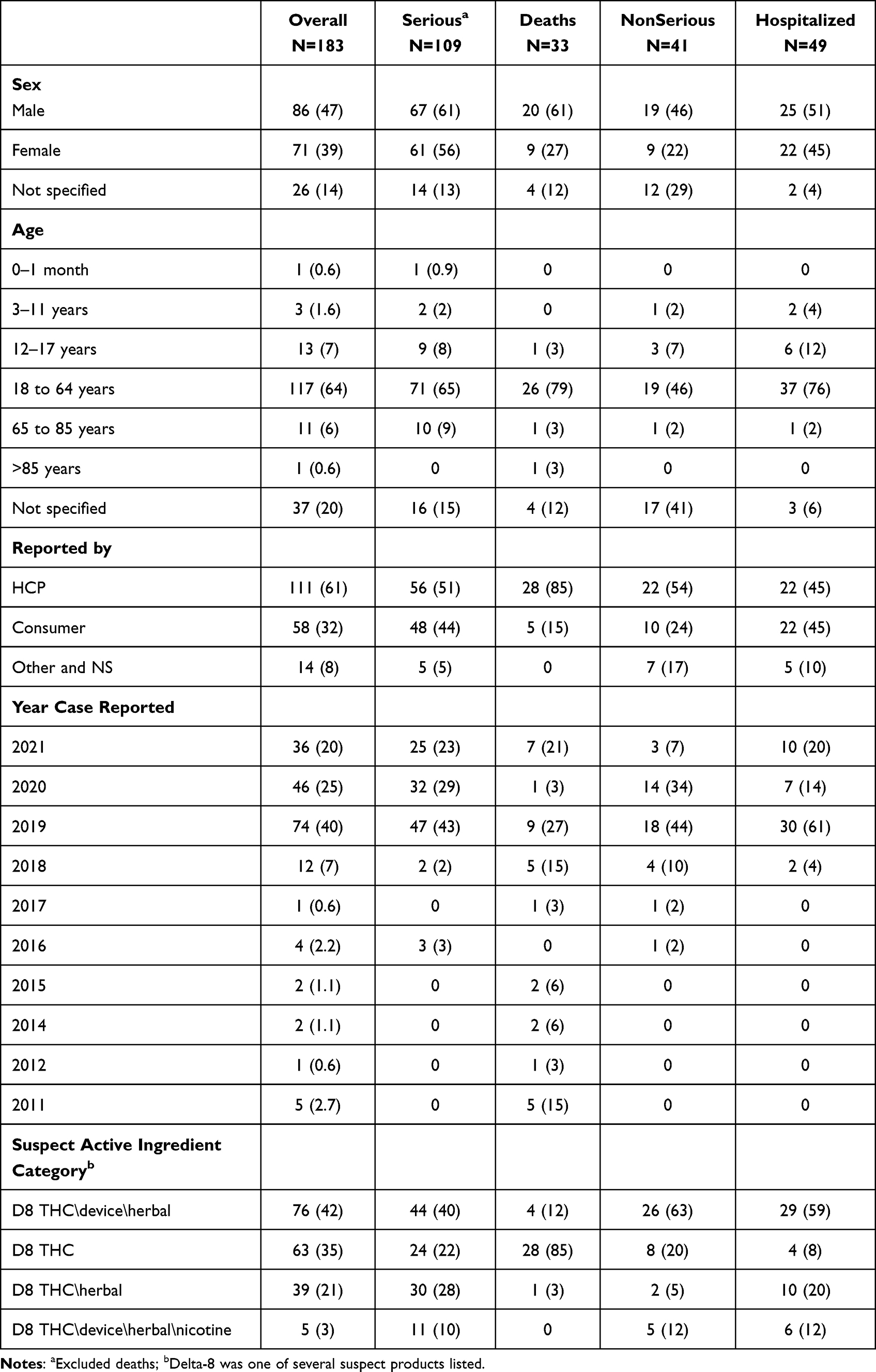 |
Table 1 Number (%) of Overall D8-THC Case Descriptions |
Of the cases that resulted in death (N = 22; 67%), most occurred between 2018 and 2021. Four deaths (21F, 22M, 62M 71M) listed a D8-THC product as the only suspect product. The three male cases reported a respiratory event. Most cases were reported by a healthcare professional (61%). Of the four D8-THC drug classifications in the FAERS database, D8-THC herbal/device (N = 76; 42%) was the most frequently reported suspect drug within the D8-THC classifications. Of the 183 cases, few (N = 15; 8%) were reported between 2011 and 2017. Most 92% (N = 168) have been reported between 2018 and June 2021.
Table 2 presents the D8-THC AEs by System Organ Class (SOC) classification. Primary terms (reactions; AEs) occurring in the respiratory, thoracic and mediastinal disorders SOC were the most frequent (45%). A case can experience more than one event; however, duplicates were removed and only single occurrences within the SOC are reported.
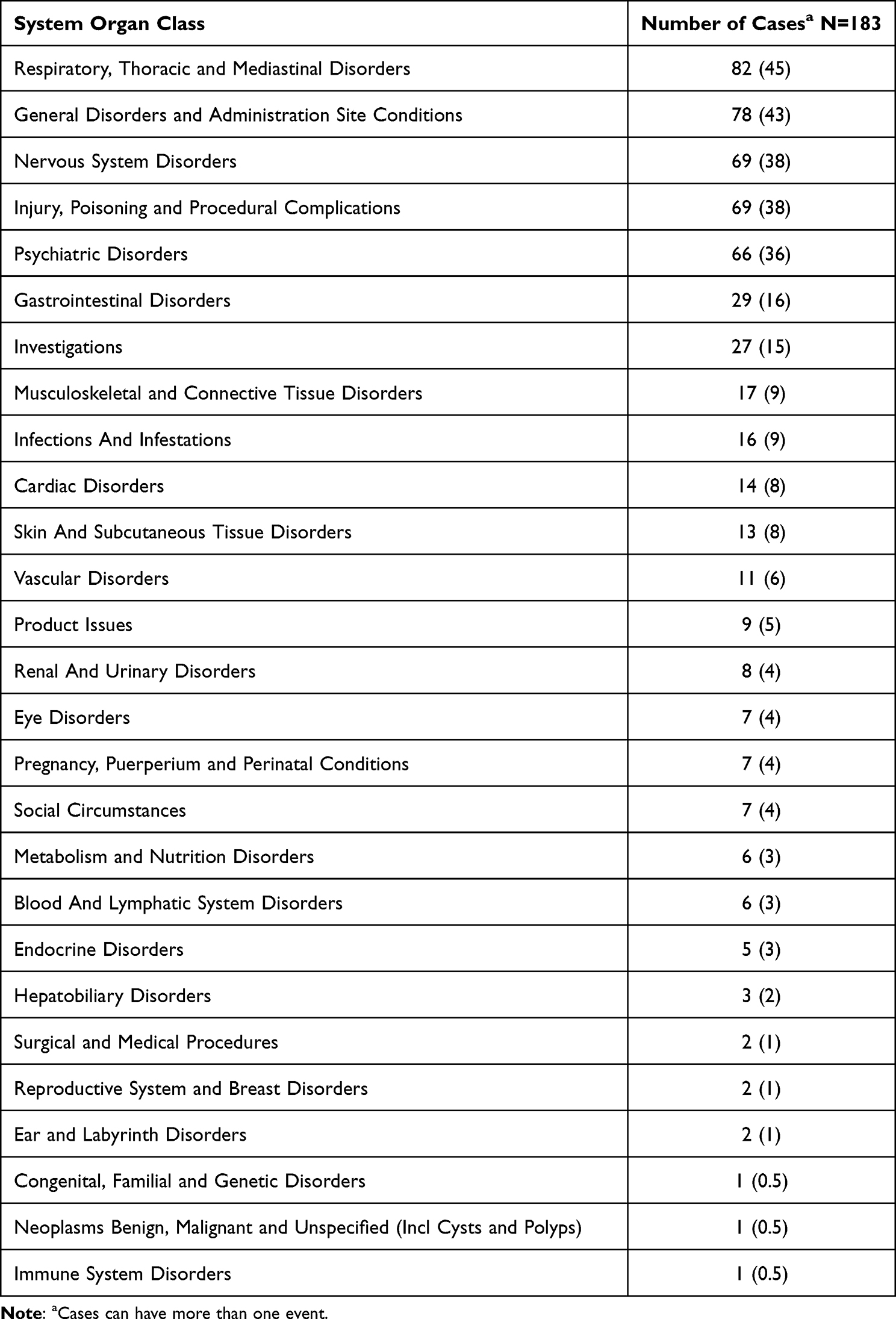 |
Table 2 Number (%) of D8-THC Adverse Events by System Organ Class (Body System) |
Table 3 presents the individual preferred terms “reaction terms” or AEs that occurred in ≥ 4%. The most frequently reported event is dyspnea (18%). As shown in Table 3, several preferred terms are respiratory in nature. Supplementary Table 1 presents the number (%) of overall D8-THC respiratory-like adverse events reported in >3% of cases.
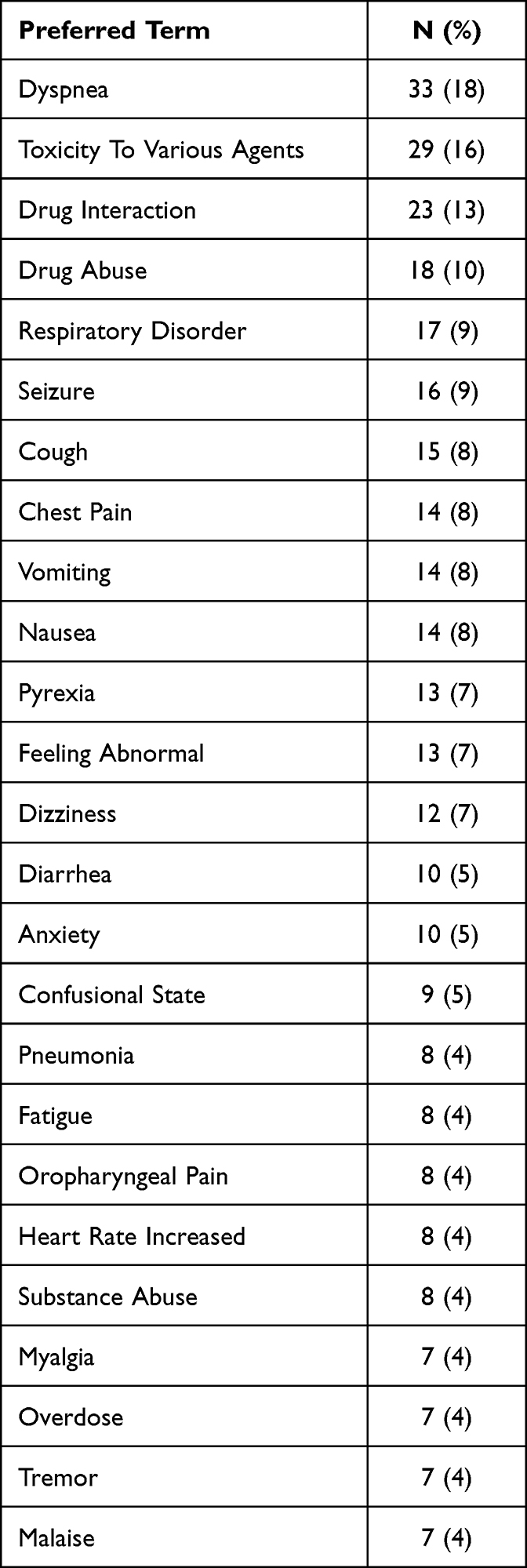 |
Table 3 Number (%) of Most Frequent (>4%) Preferred Term Reported with D8-THC |
All PTs of AEs occurring ≥ 3% are listed in the Supplemental Listing for healthcare professionals to review and understand the scope of the AEs reported.
Post Hemp Farm Bill Cases of D8-THC in FAERS
Given that most (92%) of the D8-THC suspect cases occurred after the 2018 Hemp Farm Bill was passed, we evaluated this subset of data. When limiting the cases to the post Hemp Farm Bill (2018) to June 2021, there are a total of 168 cases with D8-THC listed as a suspect drug. We observed similar trends with most cases (N = 78) having a respiratory-like event. Supplemental Table 2 presents the descriptive characteristics for D8-THC cases post Hemp Farm Bill.
Potential Signal Associated with D8-THC
For this portion of the analysis. The study period was limited to January 2018 to June 2021 inclusive. Overall, a total of 7,748,276 reports were submitted to FAERS. In total, 168 reports listed D8-THC as a possible suspect drug. The descriptive statistics on this subset were not different from the overall population outlined in Table 1. The significant SOC continued to be Respiratory, Thoracic and Mediastinal Disorders and General Disorders and Administration Site Conditions. The most frequent reaction types/AEs continued to be dyspnea, respiratory disorder, and seizure.
Table 4 presents the ROR for reactions of dyspnea, respiratory disorder, and seizure. We also computed the ROR for cases that met the definition of serious. An ROR of 2 or greater indicates a potential safety signal. The ROR lower bound of the 95% CI is greater than 1 also indicates a safety signal. The highest ROR was for seizure followed by dyspnea. The ROR for seizure was 18.9 (95% CI 11,32.4) for all seizures with ROR ranging from 8.7 to 36 depending on the reporting year. Similarly, the ROR for dyspnea was 13 (95% CI 9.0.212) for overall dyspnea with RORs ranging from 2.3 in 2018 to 23 in 2019.
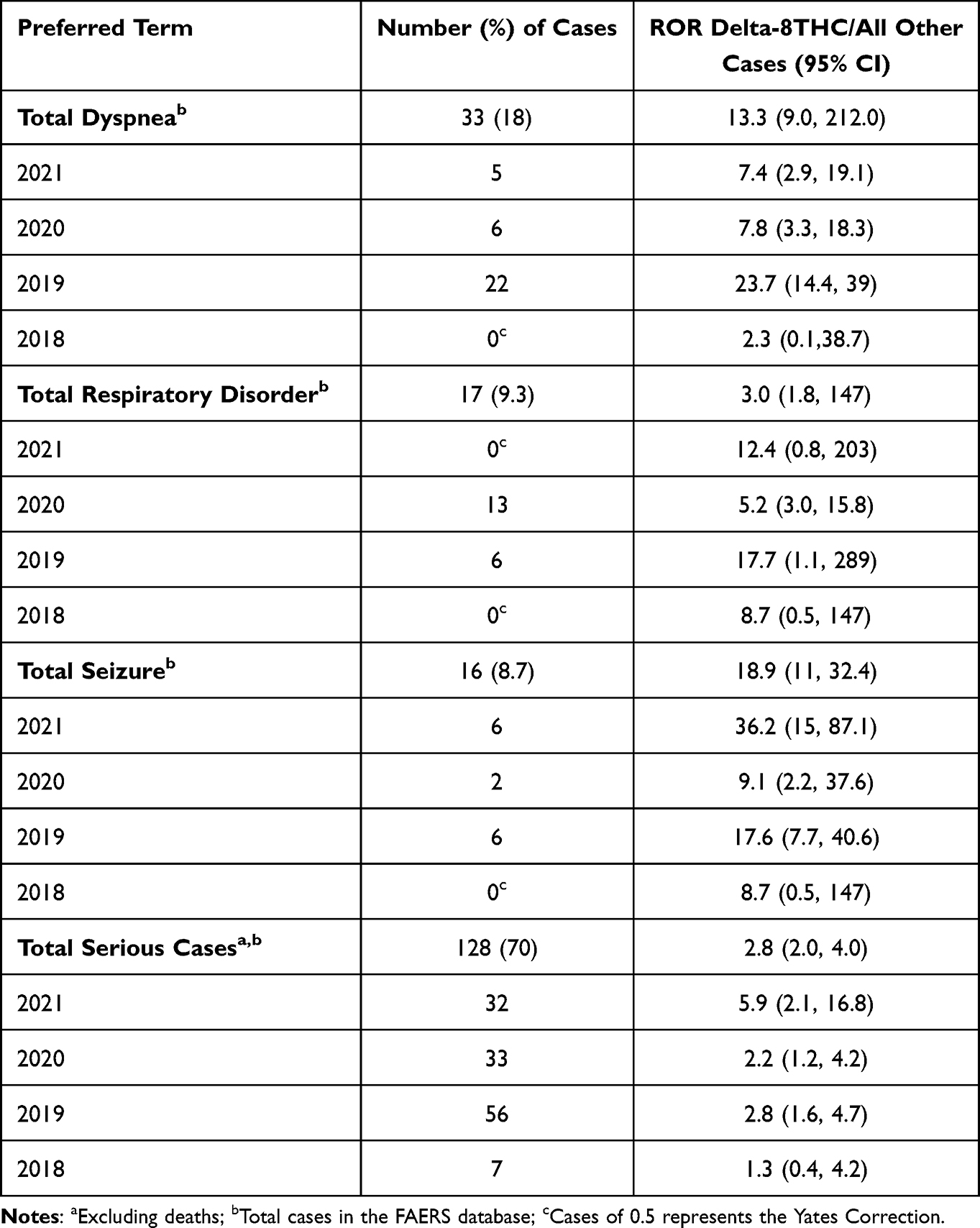 |
Table 4 Relative Odds Ratios (ROR), Signal Strength of Most Frequent AEs Number (%) of D8-THC at the Preferred Term Level in FAERS Database |
Discussion
Main Findings
To our knowledge, this is the first study to analyze AEs related to D8-THC products, reported in a national database (ie, FAERS) in the United States. Overall, the findings demonstrate that the FAERS database captured almost triple the number of cases where D8-THC was listed as a suspect product compared to D9-THC products.26 This has remained consistent as of Jan 3, 2022.
Our data show that, since 2018, the increases of D8-THC AEs occurred in mostly males aged 18 to 65 years in the US when compared to D9-THC products.26 The most frequent events occurred in the respiratory and nervous system organ class (SOC, ie, body systems). When the most common AEs (eg, dyspnea, respiratory disorder, and seizure) with D8-THC were compared to all cases of dyspnea, respiratory disorder, and seizure events reported in the FAERS database, the RORs were consistently and significantly greater than 2 from 2019 to 2021. This represents a doubling indicative of a potential safety signal. The respiratory event profile in the D8-THC cases appears to be unique for products labeled as D8-THC derived from CBD or hemp and not for D9-THC or cannabis. D8-THC products are not approved by the FDA.
D8-THC in Case Reports and Health Advisories
The most urgent and important concern is the possible association of D8-THC labeled products causing respiratory and cardiac issues from public health-related data sources (ie, case reports, poison control centers, AEs databases, etc.). A few case reports highlighting this possible public health issue are described below. The first case report is that of acute encephalopathy in a 2-year-old-female in Kentucky ingesting approximately 15mg/kg of D8-THC gummies.27 The patient was minimally responsive with a noted Glasgow Coma scale (GCS) of three and a heart rate of 136 beats per minute; the patient was intubated using fentanyl and ketamine. Since D8-THC is not included in the typical drug screen, the hospital collaborated with the DEA toxicology division to confirm the presence of D8-THC. Parents estimate that the child ingested about 9 gummies, an estimated total dose of 225 mg of D8-THC. The child was extubated after 10 hours, and GCS returned to a 15, a score generally associated with a mild head injury. The patient was discharged after 24 hours of observation and mental impairment resolved.27
Another case report documented an instance of a potentially life-threatening heart rhythm disorder after exposure to D8-THC, known as a Brugada electrocardiogram pattern (BEP; type III to type I).28 A healthy 31-year-old male in Texas presented with sudden onset of chest pain with associated pallor and dyspnea 20 minutes after ingesting a hemp D8-THC gummy. The chest pain was non-specific and non-exertional, substernal, and not relieved with rest or nitroglycerin. Abnormal EEG and BEP persisted for 16 hours post D8-THC ingestion. The Brugada pattern resolved upon one month of follow-up.28
The Michigan Poison Control Center reported two cases of severe AEs to D8-THC in children who ingested an adult’s hemp D8-THC-infused gummies obtained from a vape shop.29,30 The children experienced deep sedation and slow breathing with increased heart rate that progressed to a slow heart rate and decrease in blood pressure.29,30 The West Virginia Poison Control Center has reported cases of AEs in adults who mistakenly ingested a hemp D8-THC product, presuming it did not contain intoxicants.
Based on the totality of data, (case reports, data from this FAERS analysis and the warnings from the FDA and CDC) D8-THC containing products or exposure to D8-THC seems to be associated with significant risks of experiencing an AE. Many of these AEs seem to resolve; however, there have been some reports about a D8-THC product that was a possible factor associated with a death.26
D8-THC Animal Toxicology Data
D8-THC toxicity has clinical features of hypothermia, bradypnea, rapid weight loss, inactivity, ataxia, muscle tremors, prostration, lethargy, drowsiness, and depressive behavior.31,32 Histopathologic changes from toxic doses of D8-THC were observed in rats but not dogs or monkeys.32 Sagratella and Wada reported similar characteristics in baboons and in rabbits.33,34 In light of modern evidence, it does not appear that the doses administered by these investigators produced the aforementioned D8-THC effects as seen in FAERs.
D8-THC in Population-Based and Clinical Trial Studies
There is limited, if any, meaningful population-based information on modern D8-THC uses in humans. Our results appear to be in direct contrast to a D8-THC consumer survey published by Kruger (2021); participants were provided with CBD and D8-THC products by a manufacturer and no side effects were reported.35 The respondents also perceived D8-THC products to be safer than prescription cannabinoids (ie, Epidiolex™, Marinol™, etc.) and the FDA approved prescription drugs.35 There is a discrepancy between consumer reported perceptions of the “immaculate” safety of D8-THC and the AE data that are available.5,13
Decades ago, three small clinical trials2,6,7 compared the effects of oral doses of D8-THC to D9-THC. Hollister et al (1973) investigated D8-THC (20, 40 mg) and D9-THC (20 mg) in a small sample (n = 6), and intravenous (IV) doses of D8-THC (n = 3) and D9-THC (n = 4).2 Results indicated that oral D8-THC and D9-THC produced a similar profile of typical cannabinoid agonist effects which can include euphoria, dry mouth, red eyes, dizziness, vision that is blurred, relaxation, and small increase in heart rate (7–12 bpm). Symptom onset occurred 30–90 min after administration, with peak effects at 2.5–3.5 h (with some effects still present at 5 h). Results from the IV administration of THC and its isomer were comparable, with dose-dependent increases in tachycardia (9–41 bpm) and faster onset (ie, peak effects at 20–60 min). The authors concluded that D8-THC is slightly less potent than D9-THC.2
Years later, Gong et al evaluated the bronchodilation effect of 4 gel capsule cannabinoids: D8-THC (N = 8), D9-THC (N = 18), cannabinol (CBN) (N = 14) and CBD (N = 10). Effects of BP, heart, respiratory rates, and specific airway were measured.6 D8-THC subjects’ heart rate increased similarly to D9-THC. Level of intoxication was measured using a VAS 0 to 7, with a 7 being the highest high they have ever experienced. Oral D8-THC was rated as a 3 and 2 for 50mg and 75mg, respectively, whereas D9-THC 20mg rated a 4. No change in BP or other side effects were reported. Abrahamov et al evaluated the antiemetic effects of D8-THC without a placebo or comparable drug, in 8 children (10 m to 13yrs) with hematologic cancers.7 D8-THC (18mg/m2) was administered as oil drop on tongue for 6 hours for 24 hours. A total of 480 treatments were administered. None of the children were reported to have vomited while receiving D8-THC treatment. The treatment was well tolerated, and 2 patients were reported to experience irritability and one euphoria.
Babalonis et al summarized the current understanding regarding the comparison of D8-THC to D9-THC.1 The author states that clinically distinguishing D8-THC ingestion from D9-THC ingestion by hospital toxicology laboratories is difficult and does not seem to have changed medical management of cannabinoid-related adverse events.1 Currently, symptomatic, and supportive care without any antidotal therapy is indicated for acute intoxication. An article by Richards et al is consistent with the data found in FAERS, such as respiratory issues and severe sedation are more common in children and after high-dose exposure in adults.36
In the FAERS data, we found that the types of AEs reported in D8-THC cases had a different profile compared to those reported in the D9-THC cases. More respiratory-related AEs were reported with D8-THC than for any other cannabis or hemp product during the observation period used for this analysis.
Strengths and Weaknesses of the Methods
The main limitations of our investigation are related to the FAERS data source. At a national level, the rate of reporting an AE for an FDA approved, marketed product is about 6%. We speculate that the reporting rate could be significantly lower for non-FDA approved cannabis and hemp-derived products in FAERs. Each state cannabis program has a reporting system designated in their regulations (eg, usually local poison control centers). There is no such requirement for hemp programs. Given the overall low rate of reporting AEs and decentralization of safety data collection – simply being able to detect D8-THC safety signals in FAERS is concerning.
Data mining does not provide adequate evidence for causation. In many of the reports, there were multiple medications listed as suspect. However, in greater than 50%, D8-THC was the only suspect product listed. Given that the only data available to healthcare providers are case reports, we believe this paper will generate discussion both between and among healthcare workers and consumers. The public needs to be aware that not every product available to them has been standardized or deemed safe for consumption.
Rothman et al discuss the advantages of a reporting odds ratio over a proportional reporting ratio.22 It is stated that given the weaknesses of a spontaneous reporting database like FAERS, the data can be treated as a case–control study. For this reason, our ‘case series’ approach focuses on the importance of an appropriate choice of controls for the comparison. This is challenging and thereby highlights weaknesses in spontaneous reporting case data. In drug safety assessments and surveillance, these approaches are considered exploratory and for the purposes of identifying signals. A disproportionality ratio greater than 2 for a drug should lead to an investigation of all available data that includes a comprehensive literature review, a review of current and past animal toxicology, pharmacology, case reports and randomized clinical trials. An epidemiologic assessment may include the initiation of a case–control or cohort study to confirm the signal.
It is the body of evidence and strong pharmacovigilance assessments that allow for the complete evaluation of a potential signal. No one method (experimental data, clinical trials, spontaneous notifications, case–control studies, cohort studies and data mining) should be considered definitive when evaluating drug risk. It is the level of evidence that is generally used for evaluating drug efficacy and safety. Safety is and should be monitored for the lifetime of a product. This is true for FDA approved products. The authors believe that a product is obligated to demonstrate that it works (efficacy) and is safe in order to get on the market, however it is the safety data that keeps the product on the market. Therefore, all methods and available data are of interest and considered in an evaluation of an AE signal.
Knowledge and attitudes of consumers and healthcare professionals are important as educational intervention improves the reporting of AEs in FAERs.37–39 Increased publicity for the FAERS database and/or education should be considered to increase consumer and patient reporting.40 Many AEs may go under reported if an individual or healthcare professional does not take the time to submit a report to FAERs. Further, precise exposure to the product in question is generally unknown and limits analysis as these signal detection tools do not imply causation. The strength of FAERS is its ability to generate early signal detection for serious public health issues. Additionally, the analysis of ROR is an accepted and a standard reporting disproportionality measure of association between a product and an AE.
Public Perceptions and Public Health Implications
D8-THC products are procurable in many formulations: cookies, gummies, vaporizer cartridges, hemp flower, tinctures, and other food-like products. Yet, hemp-derived D8-THC products do not follow any standards expected of basic food items found in a grocery store, such as a loaf of bread, dairy products, or a product known to contain allergens. In effect, D8-THC, allegedly derived from hemp, is an unregulated intoxicant that can be purchased by any individual without age restrictions or proper food safety labeling.
It is theorized that the rise of access to this product and other newly obtainable isomer (THC-O acetate; D10-THC, etc.) compounds are attributed to an oversupply of CBD. Oversupply pushed producers to seek alternative products that could be profitable. Synthesizing illicit substances from CBD continues to be profitable and remains federally prohibited without licensure or approval from the DEA or other applicable regulatory bodies. Even if the chemical process was legal, regulated, and standardized, the resulting product in this case, D8-THC, can be intoxicating.41
In closing, D8-THC and other THC-isomer sales have been rising, and the perception of the public is that if a packaged product is in a storefront, then it must be safe or at least deemed safe by an authority (eg, FDA).3,35 It is unclear if D8-THC is directly responsible for the events reported in the FAERS database, or are they due to other adulterants, or due to misleading packaging.26,30,42
Conclusion
Our study was conducted to evaluate case report data on the nature and extent of D8-THC, as reported in the FAERS database. Reports of respiratory and cardiac events were most frequently reported in young males. D8-THC products continue to be sold openly, and the Hemp Farm Bill’s legal loophole is slowly constricting across jurisdictions, as separate laws are enacted to prohibit CBD-derived compounds such as D8-THC.
The lack of access to consistent and comprehensive safety data collection hinders progress in identifying and assessing the risks associated with products labeled to contain cannabinoids and their isomers. There needs to be a scientific and data-driven approach to the policies surrounding the regulation of cannabinoids. There is a lack of nationally representative real-world data on the benefits and risks associated with hemp-derived products. This includes any synthetic, semi-synthetic, and artificially derived products from hemp CBD or THC.
We feel strongly that the adoption of protocols for cannabis and hemp operators to monitor their products on the market could help preserve access as risks could be clearly identified. One method is the appropriate recording of product experiences through AEs reporting tools. Figure 1 is a QR code that links to an adverse event reporting tool. Another method is consumer education, which is needed to ensure that adults are informed of the risks to protect themselves and their children from accidental ingestion and to assume the responsibility to report unwanted effects.
 |
Figure 1 A QR code that links to an adverse event reporting tool. |
Data Sharing Statement
The data extracts from the FAERS database are available from the corresponding author upon reasonable request.
Ethics Approval
The study was conducted in accordance with the 2016 International Society for Pharmacoepidemiology guidelines for good pharmacoepidemiology practices (GPP), and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study used data from FAERS, a public anonymized database. Public use data sets like the FDA adverse event data are prepared with the intent of making them available to the public. IRBs recognize that the analysis of de-identified, publicly available data is not comparable to human subject’s research as defined at 45 CFR 46.102 and that it does not require IRB review; therefore, this project was not submitted to an IRB.
Acknowledgments
The authors thank Shannon Heaning for editorial support and Phil Molloy, MD for reviewing drafts of the manuscript. The authors are thankful to the healthcare providers and consumers who went through the process of reporting the AEs that are in the FAERS database.
Author Contributions
All authors made a significant contribution to the work reported. This includes its conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding source for this study.
Disclosure
TAS, JPM, JHS and EGH have no competing interests; JPM is a paid consultant to the cannabis industry. AG-C is currently employed by Merck. AG-C and JPM are unpaid consultants to PRC. JHS and EGH are paid student interns to Physicians Research Center and Bristol Myers Squibb at the time of analysis. JHS is now an employee of Bristol Myers Squibb. TAS is a paid health outcomes epidemiology consultant to Janssen and Bristol-Myers Squibb.
References
1. Babalonis S, Raup-Konsavage WM, Akpunonu PD, Balla A, Vrana KE. Δ8-THC: legal status, widespread availability, and safety concerns. Cannabis Cannabinoid Res. 2021;6(5):362–365. doi:10.1089/can.2021.0097
2. Hollister LE, Gillespie HK. Delta‐8‐ and delta‐9‐tetrahydrocannabinol; Comparison in man by oral and intravenous administration. Clin Pharmacol Ther. 1973;14(3):353–357. doi:10.1002/cpt1973143353
3. Leas EC. The hemp loophole: a need to clarify the legality of delta-8-THC and other hemp-derived tetrahydrocannabinol compounds. Am J Public Health. 2021;111(11):1927–1931. doi:10.2105/ajph.2021.306499
4. Mead A. Legal and regulatory issues governing cannabis and cannabis-derived products in the United States. Front Plant Sci. 2019;10:697. doi:10.3389/fpls.2019.00697
5. Johnson L. CBD oracle lab study shows some delta-8 products are 7700% over the legal delta-9 THC limit. ORACLE. Available from: https://cbdoracle.com/news/delta-8-thc-products-market-study-consumer-safety-and-legality/#The-labeling-lies.
6. Gong H, Tashkin DP, Simmons MS, Calvarese B, Shapiro BJ. Acute and subacute bronchial effects of oral cannabinoids. Clin Pharmacol Ther. 1984;35(1):26–32. doi:10.1038/clpt.1984.4
7. Abrahamov A, Mechoulam R, Mechoulam R. An efficient new cannabinoid antiemetic in pediatric oncology. Life Sci. 1995;56(23–24):2097–2102. doi:10.1016/0024-3205(95)00194-B
8. Marcu J. The legalization of cannabinoid products and standardizing cannabis-drug development in the United States: a brief report. Dialogues Clin Neurosci. 2020;22(3):289–293. doi:10.31887/dcns.2020.22.3/jmarcu
9. Sheet D fact. What is K2? What is its origin? getsmartaboutdrugs. Available from: https://www.dea.gov/sites/default/files/2020-06/K2-spice-2020.pdf.
10. Kiley B. “Synthetic Marijuana” has nothing to do with actual marijuana; 2015. Available from: https://www.thestranger.com/blogs/2015/09/16/22867088/synthetic-marijuana-has-nothing-to-do-with-actual-marijuana.
11. Goldstein C. “Synthetic pot” it’s not. Bans bring unintended consequences; 2013. Available from: https://www.inquirer.com/philly/columnists/philly420/Synthetic_pot_its_not_Designer_drug_ban_brings_unintended_consequences_.html&outputType=app-web-view.
12. Knopf A. CDC and FDA warn of delta‐8 THC harms. Alcohol Drug Abus Wkly. 2021;33(36):7. doi:10.1002/adaw.33199
13. FDA. 5 things to know about delta-8 tetrahydrocannabinol – delta-8 THC. Available from: https://www.fda.gov/consumers/consumer-updates/5-things-know-about-delta-8-tetrahydrocannabinol-delta-8-thc.
14. Xu R, Wang Q. Large-scale combining signals from both biomedical literature and the FDA Adverse Event Reporting System (FAERS) to improve post-marketing drug safety signal detection. BMC Bioinform. 2014;15(1):17. doi:10.1186/1471-2105-15-17
15. Medical Dictionary for Regulatory Activities (MedDRA) version 24.1. Available from: https://www.meddra.org/index.asp.
16. Rodriguez EM, Staffa JA, Graham DJ. The role of databases in drug postmarketing surveillance. Pharmacoepidem Dr S. 2001;10(5):407–410. doi:10.1002/pds.615
17. FDA. Questions and answers on FDA’s Adverse Event Reporting System (FAERS). Available from: https://www.fda.gov/drugs/surveillance/questions-and-answers-fdas-adverse-event-reporting-system-faers.
18. Wysowski DK, Swartz L. Adverse drug event surveillance and drug withdrawals in the United States, 1969–2002: the importance of reporting suspected reactions. Arch Intern Med. 2005;165(12):1363–1369. doi:10.1001/archinte.165.12.1363
19. Moore TJ, Cohen MR, Furberg CD. serious adverse drug events reported to the food and drug administration, 1998–2005. Arch Intern Med. 2007;167(16):1752–1759. doi:10.1001/archinte.167.16.1752
20. Weiss-Smith S, Deshpande G, Chung S, Gogolak V. The FDA drug safety surveillance program: adverse event reporting trends. Arch Intern Med. 2011;171(6):591–593. doi:10.1001/archinternmed.2011.89
21. Zink RC, Huang Q, Zhang LY, Bao WJ. Statistical and graphical approaches for disproportionality analysis of spontaneously-reported adverse events in pharmacovigilance. Chin J Nat Med. 2013;11(3):314–320. doi:10.1016/s1875-5364(13)60035-7
22. Rothman KJ, Lanes S, Sacks ST. The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidem Dr S. 2004;13(8):519–523. doi:10.1002/pds.1001
23. Green EJPH and S, Green JPH and S, Green S. Cochrane handbook for systematic reviews of interventions V5.1.0 2011; 2011. Available from: https://handbook-5-1.cochrane.org/chapter_16/16_9_2_studies_with_zero_cell_counts.htm.
24. Sakaeda T, Tamon A, Kadoyama K, Okuno Y. Data mining of the public version of the FDA adverse event reporting system. Int J Med Sci. 2013;10(7):796–803. doi:10.7150/ijms.6048
25. Montastruc J, Sommet A, Bagheri H, Lapeyre‐Mestre M. Benefits and strengths of the disproportionality analysis for identification of adverse drug reactions in a pharmacovigilance database. Brit J Clin Pharmaco. 2011;72(6):905–908. doi:10.1111/j.1365-2125.2011.04037.x
26. Simon TA, Gomez A, Marcu J. What Cannabis related data is Reported in the FDA FAERS Database. Cannabis Res Conf. 2021. doi:10.26226/morressier.60dc99f4e537565438d6c0b4
27. Akpunonu P, Baum RA, Reckers A, et al. Sedation and acute encephalopathy in a pediatric patient following ingestion of delta-8-tetrahydrocannabinol gummies. Am J Case Reports. 2021;22:e933488. doi:10.12659/ajcr.933488
28. Jo NY, Chu CC, Ramsey BC. Brugada electrocardiogram pattern induced by recreational delta-8-tetrahydrocannabinol (THC): a case report. Cureus. 2021;13(10):e19058. doi:10.7759/cureus.19058
29. Knopf A. Keep your eye on…The risks of delta-8 THC in CBD and hemp. Brown Univ Child Adolesc Behav Lett. 2021;37(11):2. doi:10.1002/cbl.30583
30. Delta 8 PSA, Michigan poison center. Wayne State University. Available from: https://static1.squarespace.com/static/5f777ef4c9213f4b5800fc9a/t/60832a49de02a46cdbd3a25d/1619208777303/Delta-8+THC+PSA+final.pdf.
31. Yoshimura H, Watanabe K, Oguri K, Fujiwara M, Ueki S. Synthesis and pharmacological activity of a phosphate ester of delta8-tetrahydrocannabinol. J Med Chem. 1978;21(10):1079–1081. doi:10.1021/jm00208a014
32. Thompson GR, Rosenkrantz H, Schaeppi UH, Braude MC. Comparison of acute oral toxicity of cannabinoids in rats, dogs and monkeys. Toxicol Appl Pharm. 1973;25(3):363–372. doi:10.1016/0041-008x(73)90310-4
33. Sagratella S, Pézzola A, Scotti de Carolis A. An EEG investigation on nabilone, a synthetic cannabinoid, in rabbits. Pharmacol Res Commun. 1986;18(7):653–662. doi:10.1016/0031-6989(86)90107-4
34. Wada JA, Osawa T, Corcoran ME. Effects of tetrahydrocannabinols on kindled amygdaloid seizures and photogenic seizures in Senegalese Baboons, Papio papio. Epilepsia. 1975;16(3):439–448. doi:10.1111/j.1528-1157.1975.tb06071.x
35. Kruger DJ, Kruger JS. Consumer Experiences with Delta-8-THC: medical Use, Pharmaceutical Substitution, and Comparisons with Delta-9-THC. Cannabis Cannabinoid Res. 2021. doi:10.1089/can.2021.0124
36. Richards JR, Smith NE, Moulin AK. Unintentional cannabis ingestion in children: a systematic review. J Pediatrics. 2017;190:142–152. doi:10.1016/j.jpeds.2017.07.005
37. Herdeiro MT, Polónia J, Gestal-Otero JJ, Figueiras A. Improving the reporting of adverse drug reactions. Drug Safety. 2008;31(4):335–344. doi:10.2165/00002018-200831040-00007
38. Lopez-Gonzalez E, Herdeiro MT, Figueiras A. Determinants of under-reporting of adverse drug reactions: a systematic review. Drug Saf. 2009;32:19–31. doi:10.2165/00002018-200932010-0000
39. Figueiras A, Herdeiro MT, Polónia J, et al. An educational intervention to improve physician reporting of adverse drug reactions: a cluster-randomized controlled trial. JAMA. 2006;296:1086–1093. doi:10.1001/jama.296.9.1086
40. Du D, Goldsmith J, Aikin KJ, Encinosa WE, Nardinelli C. Despite 2007 law requiring FDA hotline to be included in print drug ads, reporting of adverse events by consumers still low. Health Affair. 2017;31(5):1022–1029. doi:10.1377/hlthaff.2010.1004
41. World Health Organization. WHO Expert Committee on Drug Dependence. 2003:25.
42. Meehan-Atrash J, Rahman I. Novel Δ8-tetrahydrocannabinol vaporizers contain unlabeled adulterants, unintended byproducts of chemical synthesis, and heavy metals. Chem Res Toxicol. 2021. doi:10.1021/acs.chemrestox.1c00388
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Adverse Drug Events Presented in Health Institutions in Monteria, Colombia, 2018–2021
Martínez M, Villa-Dangond HS, López EM, Guzmán C
Journal of Multidisciplinary Healthcare 2023, 16:3887-3895
Published Date: 6 December 2023