")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Delivering Bad News: Emotional Perspective and Coping Strategies of Medical Students
Authors Sobczak K , Trzciński M, Kotłowska A , Lenkiewicz J , Lenkiewicz O, Przeniosło J, Plenikowski J
Received 8 June 2023
Accepted for publication 26 July 2023
Published 7 August 2023 Volume 2023:16 Pages 3061—3074
DOI https://doi.org/10.2147/PRBM.S421995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mei-Chun Cheung
Krzysztof Sobczak,1 Marcin Trzciński,2 Agata Kotłowska,2 Julia Lenkiewicz,2 Oliwia Lenkiewicz,2 Julia Przeniosło,2 Jan Plenikowski2
1Department of Sociology of Medicine & Social Pathology, Medical University of Gdansk, Gdansk, Poland; 2Student Scientific Circle of Medical Communication, Medical University of Gdansk, Gdańsk, Poland
Correspondence: Krzysztof Sobczak, Department of Sociology of Medicine & Social Pathology, Medical University of Gdansk, Tuwima, 15 Street, 80-210, Gdansk, Poland, Tel +48 58 349 15 53, Email [email protected]
Purpose: The aim of our study was to analyze students’ emotional experiences and coping mechanisms regarding the situation of delivering bad news (DBN).
Patients and Methods: 291 fifth- and sixth-year students from 14 medical universities took part in our study. Their responses were analyzed from the perspective of their experience – whether the individuals received bad news, delivered bad news themselves, witnessed bad news being delivered, or had no experience at all. We used content analysis (CA) to examine the responses and analyzed classified variables using χ2 tests, logistic regression, and predictive modeling with multiple correspondence analysis (MCA).
Results: Students who had experience as a deliverer were more likely to experience failure and guilt (p=0.005). Predictions of anxiety (59.3%), stress (41.9%), and sadness (33.7%) were the highest in the students with no DBN experience. These students were most likely to make statements suggesting lack of methods and strategies for coping with difficult emotions. Students, who were immersed in DBN experiences, more often expressed the need to talk about their emotions with an experienced doctor, a family member or a friend, and used those conversations as a coping strategy.
Conclusion: The most important aspects that influence the quality of delivering bad news are both communication skills and emotional context. Training regarding DBN should not only contain those two elements, but also consider the development of coping mechanisms.
Keywords: truth disclosure, communication, emotions, medical educations, anxiety
Introduction
Numerous reports have pointed to the relationship between the manner of delivering bad news (DBN) and patients’ behavior. With good communication, the patient experiences less stress and has more trust in the physician and the efficiency of their effort, leading to better compliance.1–3 Patients who negatively evaluate the behavior of their physicians are more likely to decide to discontinue treatment.4 Improperly delivering bad news reduces the acceptance level and increases the risk of depression and Post-Traumatic Stress Disorder (PTSD).5 Undoubtedly, the quality of communication is an element that directly translates into therapeutic results.6
Despite multiple studies indicating that expanding knowledge and skills related to DBN improves communication between medical practitioners and patients, it is not clear what benefits can be derived from various educational methods and techniques.7 Knowledge and experience alone may not be sufficient to deliver bad news properly.8 Joekes points out that deliverers are usually focused on passing on information regardless of the psycho-emotional context. In her view, this is because it is not easy to adjust the information to a patient’s cognitive and emotional abilities. The process is different if the patient is, for example, a child or an adult suffering from mental illness.9 Thus, delivering bad news requires a complex spectrum of abilities, including competencies related to emotional intelligence (EI) and those based on knowledge.
Using the ability model, Mayer, Salovey, and Caruso described EI as the ability to understand emotions, both one’s own and those of others, and to use them in thinking and acting (perception, understanding, managing, and agency).10 In other words, those concerned about the toll of delivering bad news must recognize that the interpersonal sphere is not the only important factor – the intrapersonal sphere plays a vital role too. In fact, Brown et al analyzed the physiological responses of experienced medical practitioners during interactions with a simulated patient and demonstrated that emotions, rather than a lack of experience, were the source of difficulty when delivering bad news.8 While examining the levels of stress in students in fourth and fifth years, Hulsman et al found it to be the highest in situations where bad news delivery was necessary, even when part of a simulation.11
Most medical practitioners experience emotional arousal when delivering bad news, which is a concern because stress has been linked to lower quality clinical reasoning. This is due to the fact that emotions determine the mechanisms of thinking and decision making.12,13 Reacting with anxiety translates into a reluctance to communicate bad news, described by Tesser and Conlee as the Minimizing Unpleasant Message effect (“MUM” effect).14 People who are required to convey unfavorable information are more likely to delay the delivery and reframe the information to alleviate the discomfort for the recipient. Dibble et al observed that an insufficient ability to manage emotions may lead to a worsening of patient care.15 As such, abilities that help one to cope with emotional tension when delivering bad news appear to be of paramount importance.
The Context of a Research
Medical education is not only the process of gaining knowledge and new skills, but also receiving a certain kind of professional socialisation.16 We can assume that medical students’ clinical experience at university will shape their behaviours in their future careers as doctors. According to Díaz-Martínez et al, the same mechanism can be applied to the context of DBN.17 It has been frequently reported that students do not feel sufficiently prepared for DBN.18 It seems this shortcoming may be only partially caused by insufficient communications training.19 Multiple research papers have said that a high proportion of medical students suffer from high stress levels, depression, and burnout. Steiner-Hofbauer et al found out in their study on a group of 589 students that as many as 90% have experienced elevated stress levels, which correlated with the incidence of depression among them.20 Thomspon et al reported that 17% of the research group of 161 medical students suffered from depression and 49% from burnout. As many as 23% claimed that depression is a direct result of the inability to deliver bad news.21 As is universally recognised, elevated stress levels and depression result in decreased empathy levels, which negatively affect one’s cognitive skills as well as their relationships with patients.22,23 This highly significant context is often neglected in the teaching of DBN. Toivonen et al touched upon these issues in their research study on a group of 351 medical students, from which 46% reported the feelings of insecurity and anxiety, 30% sadness, 29% ambivalence, 79% empathy during the process of DBN.24 This emotional context leads us to the need for the incorporation of adaptive coping strategies during the process of medical education at university. By analysing 18 reports on the feelings and behaviours of medical students and resident doctors, we have concluded that the ability to understand one’s own emotional mechanisms is vital to working out effective coping strategies.22 That is why the DBN immersive experience should become an essential part of curricula, as it can lead to introspection and, consequently, help future doctors develop effective coping mechanisms.16,19,24 However, many reports highlight the importance of systemic support for students and resident doctors from more experienced medical staff.25,26 Young doctors would expect from their older peers more support in developing their communication skills and more help with working through the emotional tension they experience when delivering bad news.27
Jones et al noticed that medical students use a combination of strategies focused on problem solving (acceptance, positive thinking, action) and emotionality (they are looking for emotional support from others, leisure activities) in order to cope with difficult experiences.20,28 According to Neufeld et al, passive and avoidant strategies (denial, social isolation, emotional suppression) are a less common coping mechanism that is used more often by older students.29
According to Lazarus and Folkman’s transactional model of stress and coping, managing emotions is a multidimensional process that relies on cognitive and behavioral exertions. The aim of those exertions is to cope with precise expectations (both internal and external) which pose a burden or exceed the available resources.30 The strategy of coping includes two styles: concentration on the task (aimed at problem-solving) and concentration on emotions (eg, perseverating on the unpleasantness of an experience).31 Endler and Parker expanded this model by adding another style, concentration on avoidance (diminishing the importance of the problem by diverting attention away from it).32
Psycho-emotional and behavioral difficulties associated with the acquisition of bad news delivery skills can be observed as early as in undergraduate medical education.11,18,19,33 There is, however, a noticeable dearth of research exploring how or if students’ experience in delivering bad news influences their emotions and their ability to manage them. In our study, we examined students’ statements regarding the emotions they anticipate when delivering bad news. This is a significant outcome given that it is the dread of what is to come that is most likely to delay these important conversations and result in the non-adaptive reactions mentioned above. We wanted to shed light on two questions: what emotional reactions have students experienced when delivering bad news relative to what they anticipate if they themselves have not had experience delivering bad news? And, what are the coping strategies these groups anticipate employing? A better understanding of their difficulties with the delivery of bad news could help improve the quality of educational efforts.
Materials and Methods
Aim and Objectives
The objective of our study was to analyze fifth- and sixth-year medical students’ views on emotions concerning the delivery of bad news (in this case, an unfavorable diagnosis). Further, we wanted to identify the methods they used to reduce the tension and stress caused by this difficult experience. We were interested in what impact respondents’ personal experiences had on their strategies for coping with emotions.
Study Design
A study was conducted using the computer-assisted web interview (CAWI) techniques. Data were collected through a e-questionnaire constructed by the authors, which included a selection of multiple-choice questions and two open-ended questions. The questionnaire collected data on nine independent variables: sex, age, year of schooling, medical university, planned medical specialization, experience interacting with patients outside of obligatory clinical practice and personal experience of delivering bad news in any role. Seven closed questions revolved around the respondent’s subjective sense of preparedness for delivering bad news and related educational preferences. In this context we analyzed the experiences and opinions. We asked the respondents whether they had witnessed the delivery of bad news by the doctor during clinical practice. We tried to establish if they experienced being a deliverer of bad news as medical students. We were interested in how they rated this experience in terms of the level of stress they felt and their self-assessment of performance. We asked the students to evaluate the level of universities’ preparation for teaching how to deliver bad news. We were also interested in determining which model of doctor-patients relationship is most preferred by the students. Closed-ended questions also addressed one’s own concerns and difficulties, as well as educational needs and preferred methods of competence development for situations concerning delivering bad news.18,19 We built those questions using dichotomous and Likert scale. Two last questions of the questionnaire were open-ended and became the subject of the analyzes presented here.
The primary outcome of interest is the results from the two prospective, open-ended questions. The first referred to the emotions students anticipate experiencing when delivering bad news. To enable participants to answer more openly, the question did not relate their experience to a specific context, time, or place. The second explored respondents’ methods of coping with the apprehension and emotions that may come into play when bad news delivery is necessary. We assumed that identifying any illness that requires permanent or long-term treatment or a therapy that provides relief from symptoms can be considered an unfavorable diagnosis. Such an understanding allowed us to include discussion of genetic diseases, untreatable diseases, mental illness, and so-called diseases of civilization.4
Study protocol in the form of flowchart summarizing has been included in the supplements (Supplementary Figure 1). A detailed description of the various stages of the study can be found in the following sections.
Data Collection
The study group was contacted by means of student councils, research circles, medical universities’ bulletins, and social media outlets with a nationwide reach. Students were also informed and invited to participate in the study through the administrative structures of their universities, which were asked to send information about the opportunity to participate through their email distribution lists. A professional e-research service (www.eBadania.pl) was used to reduce missing data points and effectively eliminate “framing” (when a single respondent completes the questionnaire several times) by automatically blocking the Internet Protocol (IP) address of a device from which the questionnaire has already been filled out.
Participant Identification
Study participants were fifth- and sixth-year medical students who were completing their medical course in Polish. A total of 321 responses were collected. Our research involved students from 14 out of 21 medical universities in Poland. A total of 291 questionnaires were included in the analysis; the questionnaires from the other 30 participants were rejected due to the missing responses (n=22) or comments that could not be classified (n=8). All responses to the first question, pertaining to emotional concerns in relation to bad news delivery, were included in the analysis (n=291). Within this group, 39 respondents (13.4%) failed to answer the question that focused on strategies for coping with difficult experiences. The official data published by the Central Statistical Office only includes the total number of medical students and does not present the number of students for each year. Therefore, we were unable to determine the saturation rate or the size of the quota selection for the study group.
Ethical Considerations
The questionnaire was approved by the Independent Bioethics Committee for Research. Prior to filling out the survey, participants were asked to read detailed information on the purpose and nature of the study. Participants informed consent included publication of anonymized responses. Each respondent was asked to provide informed consent to participate. No sensitive data were collected as part of the study and participation was anonymous and non-remunerated.
Data Analysis
To analyze the information acquired from the open-ended questions, we first applied cognitive analysis of content, which assumes that the choice of language is linked to the structures and processes of cognition.34 This model presents language as a method by which “perception” and internal experiences manifest, while also having an influence on how we think.35 Therefore, we sought to illustrate the structure of the students’ experiences and emotions regarding delivering bad news through an analysis of their statements.
Content analysis began by identifying the main categories of meaning so they could be subjected to inductive coding for identification of more refined categories.36,37 We generated 16 categories for the first question and 14 for the second by iteratively reading and naming ideas embedded in respondents’ answers. Examples of coding categories for question are included in the supplements (Supplementary Tables 1 and 2). The categorization was reviewed several times by two independent scorers. Together, they then abstracted and codified key categories of meaning. Once further analysis no longer generated any new meanings and efforts to refine categories no longer led to additional insights, we ended the coding stage. Two members of the research team then independently checked and verified the categorization of answers. Two independent translators rendered the responses into English and excerpts were chosen by consensus. From here we used quantitative analysis to explore the relationship between the categories identified and independent variables that included the type of experience participants expressed having had:
- None – the student had no experience with bad news delivery;
- Recipient – the student had personally received bad news as a patient;
- Observer – the student had observed the process of delivering bad news as part of a clinical training curriculum;
- Deliverer – the student had personally delivered bad news to at least one patient.
Multiple Correspondence Analysis (MCA) was then used to predict anticipations of emotions as a function of category of experience. This technique facilitated prediction estimation for particular experiences as well as the risk for various combinations of experience types (by summing the prediction related to individual types). MCA allowed us to estimate the simple effect and to predict the emotional projections of the respondents in relation to delivering bad news.
Statistical Considerations
Once classified, the variables were subjected to statistical analysis using the software program Statistica version 13.3. Pearson’s χ2 test was used in the analysis of intervariable relationships, with the significance level being set at p<0.05. Rank correlation analysis was performed using Spearman’s test.
The Cohen’s kappa coefficient was used to assess the accuracy of measures of agreement between judges categorizing responses.38 The results of the analyses revealed repetitiveness and stability of categorization (the Kappa coefficient was between 0.677 and 8.880). We repeated the compliance analysis by estimating Kendall’s coefficient of concordance. Kendall’s W for each category ranged between 0.716 and 0.973 for the first question and 0.739 and 0.977 for question two.
Logistic regression and MCA were used to assess the relationship between the type of experience and the response categories. MCA is an exploratory analysis of categorical variables, whereas Principal Component Analysis (PCA) was used for quantitative and ordinal variables.39 Since Root Mean Square Error of Approximation (RMSEA<0.01) and the remaining indicators: Goodness of Fit Index and Confirmatory Fit Index are high (GFI=0.955; CFI=0.977; CMIN=204.858; p=0.002), we can conclude that the model is well-fitted.
The Bonferroni correction was used only to verify the correctness of multiple comparisons. For the MCA model, which applies to the entire construct of variables and not to individual variables, the Bonferroni correction does not apply.
Results
Overall, 291 students’ statements were included in the analyses. The study group featured an over-representation of women, as the percentage of female respondents was 12.7% higher than the percentage of women studying at Polish departments of medicine. Fifth-year students constituted a slight majority within the study group. Exactly 52.6% (n=169) of students were at least 25 years old, whereas the remaining 47.4% (n=152) were 23–24 years of age. Most of the students (40.2%) had no experience interacting with patients other than mandatory clinical classes. However, 44 individuals disclosed that they were employed as medical assistants and 20.6% admitted that they would meet patients as part of their additional activities. These contexts appeared to be significant, as students with greater experience in dealing with patients felt better prepared to deliver unfavorable information. They also had more opportunities to observe doctors and participate in breaking bad news, which seems to be an important part of developing DBN skills.18
Emotional Experiences in the Perspective of Delivering Bad News
In order to assess students’ emotional perspectives, we constructed a prospective open-ended question. The question asked what feelings might accompany the respondents when delivering bad news. As a result of meaning content analyses, we abstracted 16 categories from the responses. We compared the obtained categories with the types of experience (Table 1). Then, using prediction analysis, we determined the probability of the occurrence of emotion experiences for the adopted experience types.
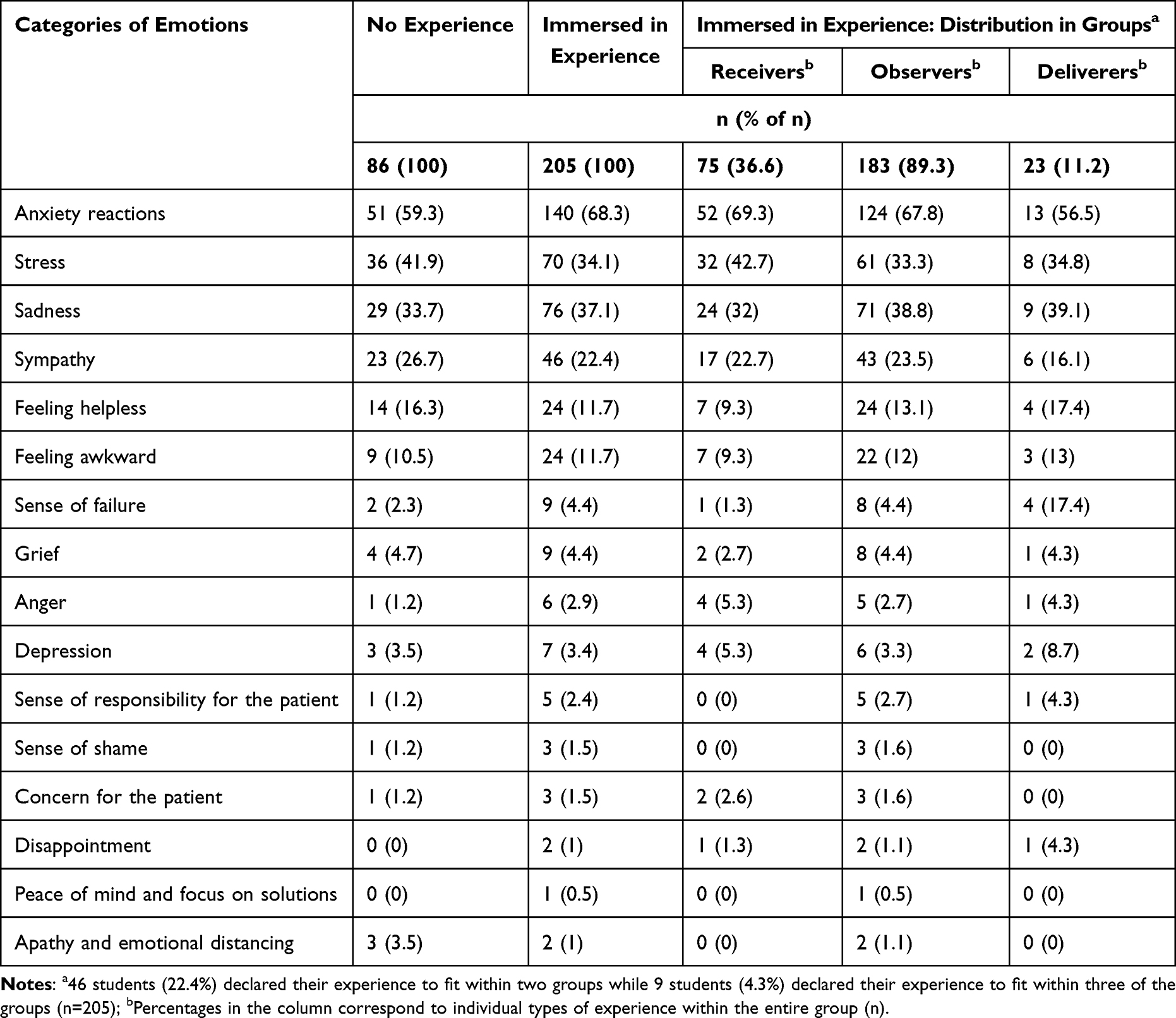 |
Table 1 Distribution of Response Categories as Related to DBN Situations (n=291) |
Content Analysis of the Responses of Students with and without Experience Delivering Bad News
Projections of anxiety and fear of experiencing a high level of stress were the most common. Students with experience (regardless of the type) referred to the anxiety category (63.3%, n=140) more frequently than those who did not have the experience of delivering bad news. (59.3%, n=51). Examples include:
Stress. It’s difficult to predict a patient’s reaction – I’d be afraid of being attacked by the family, of the patient giving up their will to fight, of bringing my work-related problems back home with me. (Student 1 – type of experience: recipient and observer)
Anxiety in relation to the patient’s reaction (aggression/hysteria/tears), a sense of guilt over being the source of suffering or taking away hope. (Student 2 – type of experience: observer)
Fear, a sense of failure, concern, sadness caused by a late diagnosis. (Student 3 – type of experience: deliverer)
Helplessness, a feeling of disorientation, exhaustion (for example, after an outburst of anger from a patient), sadness, a sense of failure. (Student 4 – type of experience: deliverer)
The responses of inexperienced students also included concerns about the emotional response to bad news, but more often focused on their own experiences. For example:
Stress, grief, depression, helplessness, a feeling of a failure. (Student 5 – no experience)
Stress. Confusion. Failure to find the right words. Fear of the patient’s reaction. (Student 6 – no experience)
Anxiety, sadness, fear of not being able to control my own emotions. (Student 7 – no experience)
I’m afraid that I would be too concerned for the patients’ fate and that I would be the one to be comforted by them as I’d cry. (Student 8 – no experience)
While decoding some of those categories, we observed, that statements indicating a caring attitude towards the patient and concern for their emotions, appeared relatively rarely. However, such statements occurred slightly more often in the case of students who experienced DBN. They included comments such as:
Sympathy for the patient. Stress at the patient’s possible reaction to an unfavorable diagnosis and (being unsure of) how to continue with the conversation so that the patient would feel satisfied and at peace. (Student 9 – type of experience: recipient and observer)
I’d be afraid of not being fully understood by the patient, who would then become concerned for their life. I am afraid I would not be able to convince the patient to undergo or change their treatment. (Student 10 – type of experience: observer)
First of all, sadness, probably some fear, the feeling that hope is being taken away from the patient, and worry that the patient might either stay in denial of the news or fall victim to suicidal thoughts they might try to put into practice. (Student 11 – type of experience: observer)
The feeling that I’ve failed to meet patient’s expectations and the trust they put in their doctor, since they put their health and life in (doctors’) hands. I am certainly concerned about the patient’s emotional response, so (I) fear whether I would be able to cope with that response. (Student 12 – type of experience: observer)
Prediction of Emotional Experience Projections as a Function of Experience
We applied a logistic regression model to examine whether the type of experience one had delivering bad news (none, or as a recipient, observer, or deliverer) had a significant impact on the emotions related to DBN. MCA allowed us to predict specific emotional experiences for any combination of types of experience (Table 2). The analysis demonstrated that those who had experience as a deliverer were more likely to experience failure and guilt (B=2.119; p=0.005). For the other categories of analysis, we did not reveal a correlation between the type of experience delivering bad news and emotions.
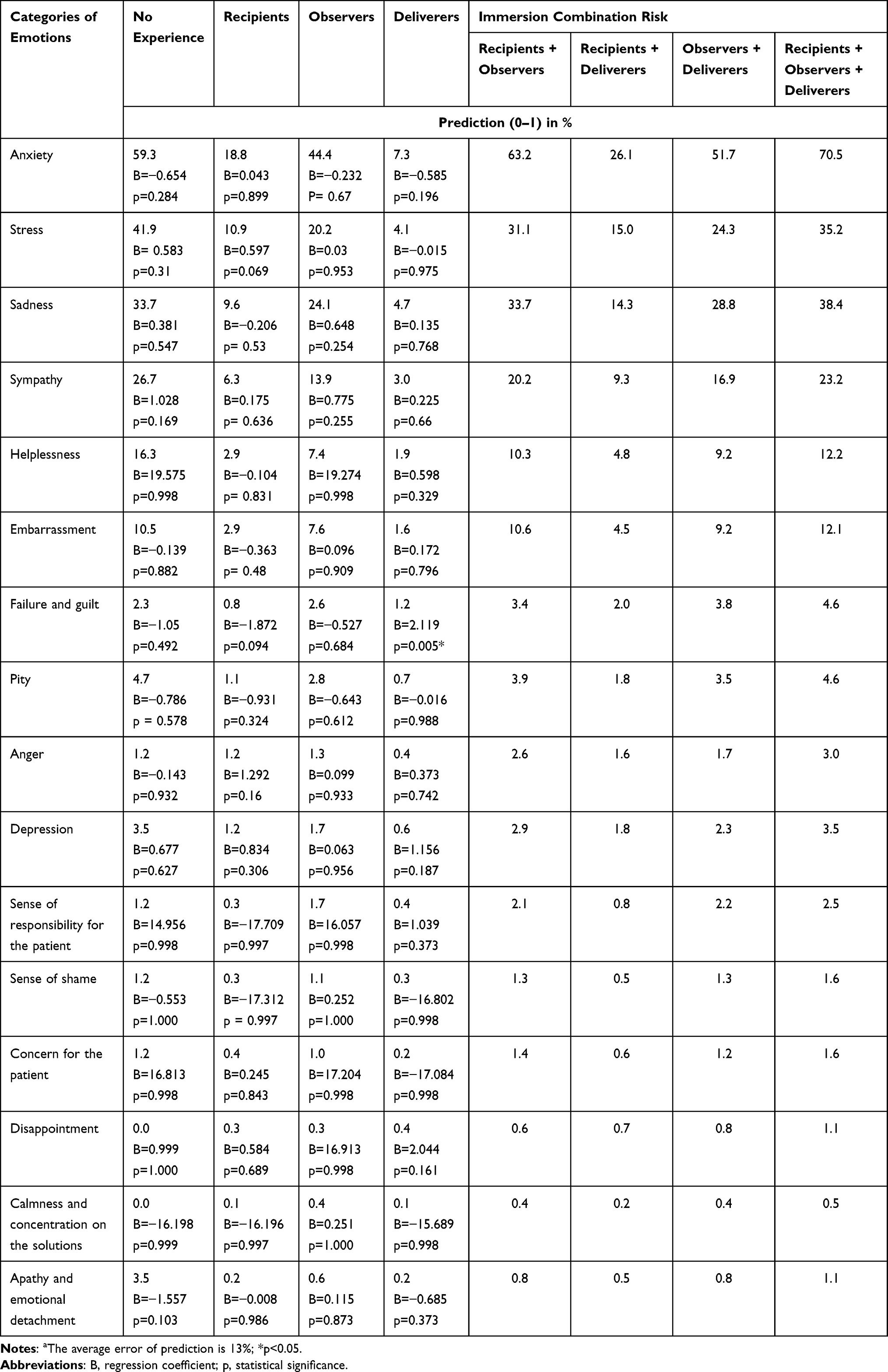 |
Table 2 Prediction of Individual Emotional Reactions Depending on the Immersion Combinations as Determined Using the MCA Modela |
The experience of being an observer had a greater influence on reactions of anxiety, stress, sadness, sympathy, helplessness, and/or embarrassment than for the recipients and deliverers (Table 2).
We summarized the predictions of individual emotions by aggregating them by category, with the highest predictions of anxiety (70.5%) and sadness (38.4%) observed among students with all three types of DBN experience.
The prediction of the risk of occurrence of the analyzed emotions for individual categories of experiences is presented in the chart (Table 2).
Coping Styles in the Context of Delivering Bad News
The second prospective question referred to the individual’s methods of coping with difficult emotions concerning delivering bad news. Similar to the previous question, we performed a content analysis extracting 14 categories. The respondents who did not provide an answer or whose answers could not be assigned to any of the 13 categories were isolated as the 14th category, which was excluded from the analyses. The remaining categories were classified according to the Folkman and Lazarus concept as strategies that focus on tasks, emotions or avoidance (Table 3).30,31 We analyzed the categorized responses by relating them to whether or not the student had experience related to DBN.
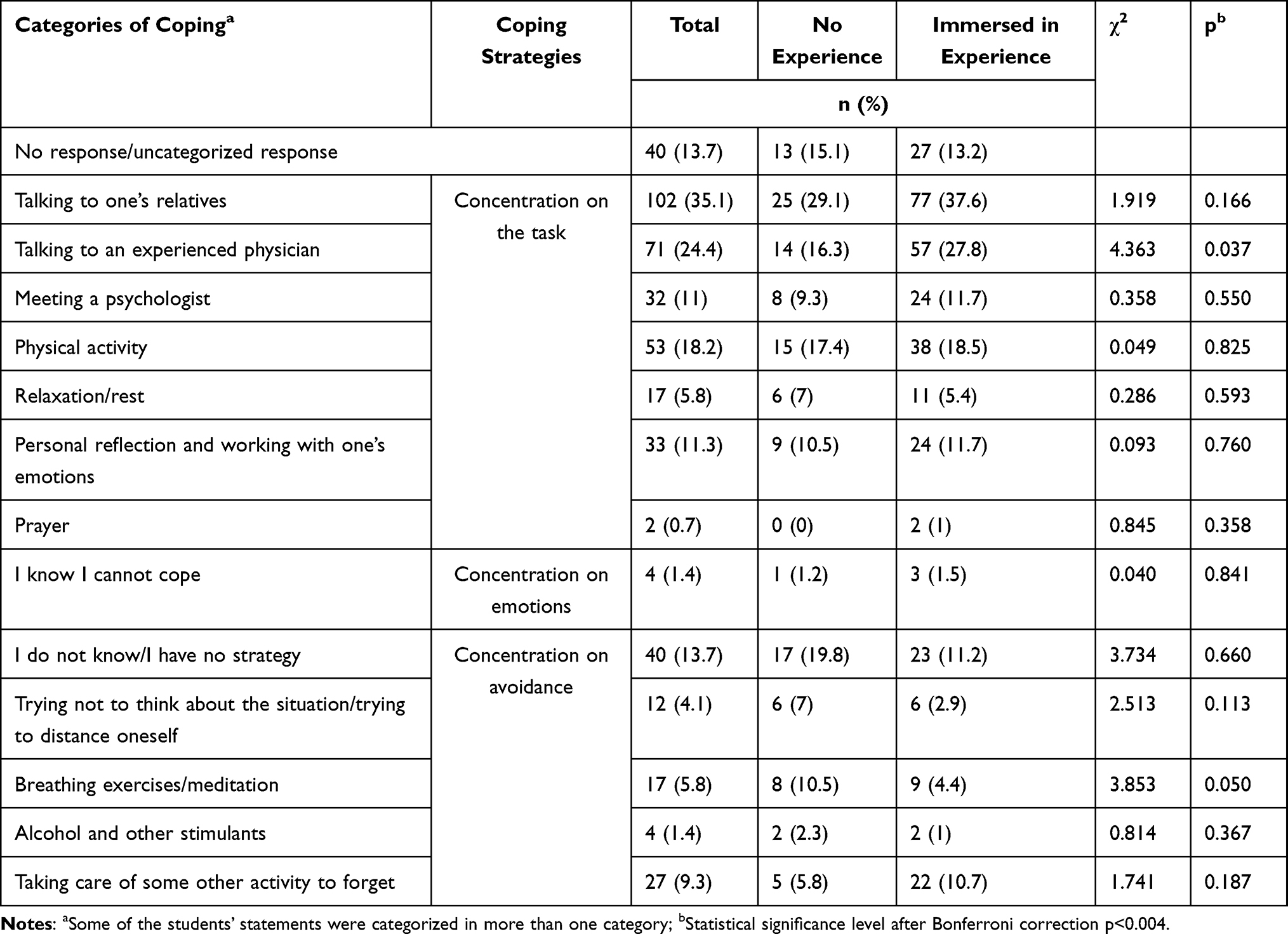 |
Table 3 Analysis of the Distribution of Responses Depending on the Coping Strategy |
Content Analysis of Responses Regarding the Strategy of Coping with Emotions
Students with no DBN experience answered more frequently that they lack strategies and ways to cope with difficult emotions. Among those immersed in DBN experience, responses relating to adaptive strategies (involving the search for support in a direct relationship with relatives and significant others) were more common as compared to responders with no DBN experience. Examples of student answers to the question regarding strategies of coping with emotions included:
I have no specific way of coping; I will struggle with this until the day I manage to forget about it. (Student 13 – no experience)
I’ll take two deep breaths, clench my teeth, and do my job. (Student 14 – no experience)
Cutting off from it - finding a distraction like a TV show, a party, a job. (Student 15 – no experience)
I’m going to try to separate myself from it and leave the unpleasant emotions behind. (Student 16 – no experience)
I will talk about it with my partner, close friends in the field who may have had similar situations, or with a supervisor/senior colleague with whom I feel close enough to be able to ‘talk through’ these emotions, to feel supported that I am not alone. (Student 17 – no experience)
Talking to a more experienced doctor, a psychologist in the department. Discharging emotions through sports. (Student 18 - type of experience: observer)
Chat with other members of the team, exercise, spend time on my own (walking, resting, or a hobby), crying over the situation, giving myself space to go through the experience and name my emotions, keeping a diary. (Student 19 – type of experience: observer and deliverer)
Chatting with someone close to me about my feelings. Thinking the situation through on my own: Did I act the way I would like someone else to act towards me? (Student 20 – type of experience: recipient and observer)
Talking with those closest to me. Evaluating and thinking about the situation on my own, and then understanding where in the conversation I made mistakes and not making them in the future. (Student 21 – type of experience: observer and deliverer)
Analysis of Categories in Relation to Strategies for Coping
Analysis of the distribution of density of the categorized responses demonstrated, that students with experience of communicating bad news utilized adaptive strategies for coping with emotions slightly more often (Table 3). At the same time, a marginally higher number of those students who had no experience of DBN declared utilizing non-adaptive strategies.
Importantly, the correlation analysis did not show any significant relationships between these groups and coping strategies (RS=0.329, p=0.425).
Discussion
The purpose of our project was to analyze participants’ statements regarding the emotional context of DBN and strategies for coping with those difficult experiences. Among the categorized respondents’ statements, we revealed the connection between failure and guilt (p=0.005) as emotions more often experienced by students immersed in situations related to DBN.
Orlander et al showed that, in opinion of 95% of students, having experience as an observer alone was enough to contribute to their development.40 Students with DBN experience as observers and deliverers may have a more balanced set of cognitive and emotional resources at their disposal, which translates into better control and lower stress levels. In their analysis of statements from students who had participated in DBN training courses, Toivonen et al emphasized the crucial importance of challenging experiences, which provide essential material for personal reflection and enable students to construct their own emotional awareness for such situations.24
It is possible that students with no DBN experience are likely to have fewer psychological resources appropriate for this type of situation. Thus, they express their own concern by adopting a defensive attitude and focusing on their own anxieties, concerns, and feelings of helplessness more frequently. They tend to describe their relationships with patients in these situations as being more stressful, since they lack experience using their DBN skills.
The answers related to anxiety and fear of undue stress were mostly provided by those students who had experienced receiving bad news.4 Perhaps the personal history of having received bad news is so persistent and emotional an experience that it is subsequently reflected in the predictions of future behavior, particularly in young people.
Comparing the non-adaptive and adaptive strategies of coping with emotions of students with and without DBN experience, we found no statistically significant differences between these groups. This could be an important result. Strategies for coping with difficult emotions are a component of the skills acquired by students, regardless of their DBN experience. They may stem directly from one’s personal strategies for coping with difficult experiences and they may be linked to personal characteristics and skills. We know that individuals with a high degree of cognitive flexibility are equipped with better mechanisms of adapting to difficult situations and are more likely to use secondary strategies, such as meditation and relaxation.41,42
It seems to us that teaching competences related to DBN based on the idea of immersing students in increasingly difficult educational situations can effectively develop skills as well as more adaptive strategies for dealing with clinically difficult situations. Thus, the risk of reacting with intense anxiety and stress can be avoided. We think that the spiral model of DBN training proposed by Kurtz et al might safely and effectively meet the postulate of education through experience.43 According to this postulate, skills are acquired gradually, starting from elementary education and followed by simulated contact and subsequent actual relationships with patients and their families. The DBN-related skills are strengthened and enhanced in the process. The level of immersion increases with time and skills. This approach gives students the opportunity to identify their own deficits and observe their own difficulties.44,45 This standpoint has been supported by Meitar et al, who observed that student’s competencies in communicating with patients can be improved if the students learn to relate to their own difficulties and receive support in coping with them.46 An awareness of insufficient skills can be seen as the first step towards further development. The conclusion of the research conducted by Jones et al. Was the adoption of the analogical educational mode that is based on personal interaction with the patient, self-reflection, and adherence to role models.28 Trivate et al similarly emphasize the importance and effectiveness of students’ self-reflection, augmented by the support of medical staff as an effective educational strategy.26 Bhandari et al also noted the need to support medical personnel in working through DBN situations.27 Our research confirmed this optics. In our study, the expectation of support from an experienced doctor or psychologist was frequently indicated.
As noted by Toivonen et al, all of these experiences constitute an important element that shapes the future professional identity of students.24 According to Díaz-Martínez et al the quality of the students’ DBN experience affects how they will notify bad news as doctors.17 Therefore, we should not avoid making the students face emotionally difficult situations in the education process. Students should be prepared for such situations and the educational process should be designed in a manner that ensures a safe experience for both students and patients. Numerous guidelines and recommendations have already been developed, in which learning takes the form of practical exercises with group feedback.47,48 Clinical classes, during which students get actual experience as observers or deliverers of bad news, should clearly define the roles of the student and the teacher, also taking into account the information delivered to the patient.47 In the area of clinical education, the key role is that of the teaching physician. It depends on the level of their involvement as well as their communication and teaching skills. The model of education that is currently in effect also plays a key role here. There are certain educational strategies which promote the development of the students’ experience by engaging them in DBN. In our research, only 11.2% of the respondents (n=23) declared that they had such experience. Research conducted by Westmoreland showed that 71% of students had had personal experience with DBN, despite the fact that DBN was not an obligatory part of the curriculum.49 Yale Medical School has implemented an educational strategy based on workshops on delivering bad news or assigning students to care for patients at the end of life.50
Our findings indicate the necessity to enhance one’s abilities in conveying bad news by gradually acquiring experience. The incorporation of training related to emotion management during clinical education may prove to be a viable solution that facilitates the preparation for the delivery of bad news. It appears the acquisition of communication skills, coupled with training in emotion management, can enhance the standard of medical work and medical services provided by doctors. Like Jonas et al we suggest that training related to coping strategies should be implemented as part of medical courses.28
While our study provides some important observations, we realize that it is also burdened by some objective limitations. When assessing the forms of experience, we determined only the nature of experience (recipient, observer, or deliverer). We clearly understand that the differences between such experiences can be as significant as the differences between the personalities of the individuals having the experience. Other important elements include the quantity, duration, and quality of exposure and the emotional reaction of the patient, as they may have a significant impact on the nature of the experience and its cognitive and emotional outcomes. Likewise, the behavior of the physician who delivered the bad news might have influenced the experience of the recipients and observers. When interpreting the results, the prospective nature of the study and the differences in training models for DBN skills should be taken into account. We are aware that caution should be taken when interpreting the results. The study group was not representative. Due to the lack of detailed data on the number of students studying in the fifth and sixth years, it was not possible to calculate the saturation for this study. In the survey, we observed an overrepresentation of students from the Medical University of Gdansk (34.9%). We are also aware that individual medical school have some level of discretion regarding the organization of education. This implies that some of the students did not participate in the courses developing skills for delivering bad news. Furthermore, the size of medical schools affects their clinical base, and therefore the nature of clinical contacts during medical education.
Given the above limitations and results, we believe that future research directions related to the measurement of students’ sense of preparedness to deliver unfavorable information should be continued. Therefore, we are planning further comparative studies in which some groups of students will be subjected to additional educational training related to coping strategies, while others will undergo training implemented as part of their mandatory education. It seems important that this kind of research should also be continued in the long-term analysis, and that the measurement of the self-assessment of these students should also be done in the future, with reference to their experiences as doctors. After all, the psycho-emotional context related to the delivery of bad news may be just as important as communication skills and professional experience.
Conclusion
Personal experience with DBN is a form of education that provides an opportunity for growth by raising awareness of the difficulties encountered. It stimulates the development of empathy and turns the students’ attention to the patient’s perspective. Therefore, we propose to include elements of intrapersonal communication in courses developing the skills involved in delivering bad news. Taking into account, that the training related to the development of adaptive coping strategies seems to be an important competence, it may affect the quality of the DBN process and, consequently, affect medical services provided.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics Approval and Consent to Participate
The proprietary research tool was approved by the Independent Bioethics Committee of the Medical University of Gdansk (decision no. NKBBN/287/2021). All methods were carried out in accordance with relevant guidelines and regulations. All participants gave informed consent to participate in the study.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Zachariae R, Pedersen CG, Jensen AB, Ehrnrooth E, Rossen PB, von der Maase H. Association of perceived physician communication style with patient satisfaction, distress, cancer-related self-efficacy, and perceived control over the disease. Br J Cancer. 2003;88(5):658–665. doi:10.1038/sj.bjc.6600798
2. Golin C, DiMatteo MR, Duan N, Leake B, Gelberg L. Impoverished diabetic patients whose doctors facilitate their participation in medical decision making are more satisfied with their care. J Gen Intern Med. 2002;17(11):857–866. doi:10.1046/j.1525-1497.2002.20120.x
3. Zolnierek KB, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(8):826–834. doi:10.1097/MLR.0b013e31819a5acc
4. Sobczak K, Leoniuk K, Janaszczyk A. Delivering bad news: patient’s perspective and opinions. Patient Prefer Adherence. 2018;12:2397–2404. doi:10.2147/PPA.S183106
5. Johnson J, Panagioti M. Interventions to improve the breaking of bad or difficult news by physicians, medical students, and interns/residents: a systematic review and meta-analysis. Acad Med. 2018;93(9):1400–1412. doi:10.1097/ACM.0000000000002308
6. Narayanan V, Bista B, Koshy C. “BREAKS” protocol for breaking bad news. Indian J Palliat Care. 2010;16(2):61–65. doi:10.4103/0973-1075.68401
7. Dale MacLaine T, Lowe N, Dale J. The use of simulation in medical student education on the topic of breaking bad news: a systematic review. Patient Educ Couns. 2021;104(11):2670–2681. doi:10.1016/j.pec.2021.04.004
8. Brown R, Dunn S, Byrnes K, Morris R, Heinrich P, Shaw J. Doctors’ stress responses and poor communication performance in simulated bad-news consultations. Acad Med. 2009;84(11):1595–1602. doi:10.1097/ACM.0b013e3181baf537
9. Joekes K. Breaking bad news. In: Llewellyn CD, McManus C, Weinman J, Petrie KJ, Newman S, Ayers S, editors. Cambridge Handbook of Psychology, Health and Medicine.
10. Mayer JD, Caruso DR, Salovey P. The ability model of emotional intelligence: principles and updates. Emot Rev. 2016;8(4):290–300. doi:10.1177/1754073916639667
11. Hulsman RL, Pranger S, Koot S, Fabriek M, Karemaker JM, Smets EM. How stressful is doctor-patient communication? Physiological and psychological stress of medical students in simulated history taking and bad-news consultations. Int J Psychophysiol. 2010;77(1):26–34. doi:10.1016/j.ijpsycho.2010.04.001
12. Pottier P, Dejoie T, Hardouin JB, et al. Effect of stress on clinical reasoning during simulated ambulatory consultations. Med Teach. 2013;35(6):472–480. doi:10.3109/0142159X.2013.774336
13. LeBlanc VR, McConnell MM, Monteiro SD. Predictable chaos: a review of the effects of emotions on attention, memory and decision making. Adv Health Sci Educ Theory Pract. 2015;20(1):265–282. doi:10.1007/s10459-014-9516-6
14. Tesser A, Conlee M. Recipient emotionality as a determinant of the transmission of bad news. Proc ACAP. 1973;1973:247–248.
15. Dibble JL, Levine TR. Breaking good and bad news: direction of the MUM effect and senders’ cognitive representations of news valence. Communic Res. 2010;37(5):703–722. doi:10.1177/0093650209356440
16. Janssen AL, Macleod RD, Walker ST. Recognition, reflection, and role models: critical elements in education about care in medicine. Palliat Support Care. 2008;6(4):389–395. doi:10.1017/S1478951508000618
17. Díaz-Martínez LA, Cuesta Armesto MH, Díaz Rojas MJ. Perspectives of Colombian medicine students about their formation on breaking bad news: a cross-sectional study. Educ Méd. 2021;22:305–313. doi:10.1016/j.edumed.2021.05.009
18. Lenkiewicz J, Lenkiewicz O, Trzciński M, et al. Delivering bad news: self-assessment and educational preferences of medical students. Int J Environ Res Public Health. 2022;19:2622. doi:10.3390/ijerph19052622
19. Kotłowska A, Przeniosło J, Sobczak K, et al. Influence of personal experiences of medical students on their assessment of delivering bad news. Int J Environ Res Public Health. 2022;19(19):12040. doi:10.3390/ijerph191912040
20. Steiner-Hofbauer V, Holzinger A. How to cope with the challenges of medical education? Stress, depression, and coping in undergraduate medical students. Acad Psychiatry. 2020;44(4):380–387. doi:10.1007/s40596-020-01193-1
21. Thompson G, McBride RB, Hosford CC, Halaas G. Resilience among medical students: the role of coping style and social support. Teach Learn Med. 2016;28(2):174–182. doi:10.1080/10401334.2016.1146611
22. Neumann M, Edelhauser F, Tauschel D, et al. Empathy decline and its reasons: a systematic review of studies with medical students and residents. Acad Med. 2011;86(8):996–1009. doi:10.1097/ACM.0b013e318221e615
23. Zdun-Ryżewska A, Sobczak K, Rudnik A. Fatigue Pro-social attitude and quality of life as predictors of empathy in medical and social-oriented students. Int J Environ Res Public Health. 2022;19:15853. doi:10.3390/ijerph192315853
24. Toivonen AK, Lindblom-Ylänne S, Louhiala P, Pyörälä E. Medical students’ reflections on emotions concerning breaking bad news. Patient Educ Couns. 2017;100(10):1903–1909. doi:10.1016/j.pec.2017.05.036
25. van der Merwe LJ, Botha A, Joubert G. Resilience and coping strategies of undergraduate medical students at the University of the Free State. S Afr J Psychiatr. 2020;28(26):1471.
26. Trivate T, Dennis AA, Sholl S, Wilkinson T. Learning and coping through reflection: exploring patient death experiences of medical students. BMC Med Educ. 2019;19(1):451. doi:10.1186/s12909-019-1871-9
27. Dosanjh S, Barnes J, Bhandari M. Barriers to breaking bad news among medical and surgical residents. Med Educ. 2001;35(3):197–205. doi:10.1046/j.1365-2923.2001.00766.x
28. Jones FM, Fellows JL, Horne DJ. Coping with cancer: a brief report on stress and coping strategies in medical students dealing with cancer patients. Psychooncology. 2011;20(2):219–223. doi:10.1002/pon.1751
29. Neufeld A, Malin G. How medical students cope with stress: a cross-sectional look at strategies and their sociodemographic antecedents. BMC Med Educ. 2021;21(1):299. doi:10.1186/s12909-021-02734-4
30. Folkman S, Lazarus RS. The relationship between coping and emotion: implications for theory and research. Soc Sci Med. 1988;26(3):309–317. doi:10.1016/0277-9536(88)90395-4
31. Lazarus SR, Folkman S. Stress, Appraisal, and Coping. New York: Springer Publishing Company; 1984.
32. Endler NS, Parker JD. Multidimensional assessment of coping: a critical evaluation. J Pers Soc Psychol. 1990;58(5):844–854. doi:10.1037/0022-3514.58.5.844
33. Cohen L, Baile WF, Henninger E, et al. Physiological and psychological effects of delivering medical news using a simulated physician-patient scenario. J Behav Med. 2003;26(5):459–471. doi:10.1023/A:1025724118504
34. Lakoff G, Johnson M. Metaphors We Live By. Chicago: University of Chicago Press; 1980.
35. Reber AS, Reber ES. Dictionary of Psychology. Warszawa: Scholar; 2005.
36. Taylor SJ, Bogdan R. Introduction to Qualitative Research Methods: A Guidebook and Resource.
37. Pickard AJ. Research Methods in Information. London: Facet; 2007.
38. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22(3):276–282. doi:10.11613/BM.2012.031
39. Topolski M. Algorithm of multidimensional analysis of main features of PCA with blurry observation of facility features detection of carcinoma cells multiple myeloma. In: Burduk R, Kurzynski M, Wozniak M, editors. Progress in Computer Recognition Systems. Wrocław: Springer; 2020:286–294.
40. Orlander JD, Fincke BG, Hermanns D, Johnson GA. Medical residents’ first clearly remembered experiences of giving bad news. J Gen Intern Med. 2002;17(11):825–831. doi:10.1046/j.1525-1497.2002.10915.x
41. Gan Y, Zhang Y, Wang X, Wang S, Shen X. The coping flexibility of neurasthenia and depressive patients. Pers Individ Dif. 2006;40(5):859–871. doi:10.1016/j.paid.2005.09.006
42. Cheng C, Lau HP, Chan MP. Coping flexibility and psychological adjustment to stressful life changes: a meta-analytic review. Psychol Bull. 2014;140(6):1582–1607. doi:10.1037/a0037913
43. Kurtz S, Silverman J, Draper J. Teaching and Learning Communication Skills in Medicine. Oxford, England: Radcliffe Medical Press; 1998.
44. de Moura Villela EF, Bastos LK, de Almeida WS, et al. Effects on medical students of longitudinal small-group learning about breaking bad news. Perm J. 2020;24:19.
45. Kiluk JV, Dessureault S, Quinn G. Teaching medical students how to break bad news with standardized patients. J Cancer Educ. 2012;27(2):277–280. doi:10.1007/s13187-012-0312-9
46. Meitar D, Karnieli-Miller O, Eidelman S. The impact of senior medical students’ personal difficulties on their communication patterns in breaking bad news. Acad Med. 2009;84(11):1582–1594. doi:10.1097/ACM.0b013e3181bb2b94
47. Rosenbaum ME, Ferguson KJ, Lobas JG. Teaching medical students and residents skills for delivering bad news: a review of strategies. Acad Med. 2004;79(2):107–117. doi:10.1097/00001888-200402000-00002
48. Meitar D, Karnieli-Miller O. Twelve tips to manage a breaking bad news process: using S-P-w-ICE-S - A revised version of the SPIKES protocol. Med Teach. 2021;44:1–5.
49. Westmoreland KD, Banda FM, Steenhoff AP, Lowenthal ED, Isaksson E, Fassl BA. A standardized low-cost peer role-playing training intervention improves medical student competency in communicating bad news to patients in Botswana. Palliat Support Care. 2019;17(1):60–65. doi:10.1017/S1478951518000627
50. Ellman MS, Fortin AH. Benefits of teaching medical students how to communicate with patients having serious illness: comparison of two approaches to experiential, skill-based, and self-reflective learning. Yale J Biol Med. 2012;85(2):261–270.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.