Back to Journals » Advances in Medical Education and Practice » Volume 17
Defining Preliminary Core Nontechnical Skills for Anesthesia Crisis Management in Indonesia: An Expert Consensus from a Modified Delphi Study Emphasizing Communication and Situational Awareness
Authors Heriwardito A ![]() , Ramlan AAW
, Ramlan AAW ![]() , Soemantri D
, Soemantri D ![]()
Received 20 March 2026
Accepted for publication 29 June 2026
Published 9 July 2026 Volume 2026:17 610271
DOI https://doi.org/10.2147/AMEP.S610271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Aldy Heriwardito,1 Andi Ade Wijaya Ramlan,1 Diantha Soemantri2
1Department of Anesthesiology and Intensive Care, Dr Cipto Mangunkusumo National General Hospital–Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 2Department of Medical Education, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia
Correspondence: Aldy Heriwardito, Department of Anesthesiology and Intensive Care, Dr Cipto Mangunkusumo National General Hospital–Faculty of Medicine Universitas Indonesia, Jl. Pangeran Diponegoro 71, Jakarta, Indonesia, Tel +6281386211017, Email [email protected]
Purpose: To identify, through expert consensus, a preliminary set of core nontechnical competencies for anesthesia crisis management in Indonesia, with particular emphasis on situational awareness and communication.
Patients and Methods: This exploratory sequential qualitative study was conducted in Indonesia between January and December 2025. Phase one comprised a structured literature review using the Population, Concept, and Context framework across four databases, yielding 17 included studies. Phase two employed a modified Delphi method with a purposively sampled expert panel of 13 professionals, including anesthesiologists, nurse anesthetists, non-anesthesia surgical specialists, and patient-safety and education leaders, drawn from seven institutions across four Indonesian cities. Competencies were rated on a 4-point Likert scale, with responses dichotomised for analysis (ratings of 3 or 4 indicating agreement) and consensus predefined at ≥ 75% agreement. Content validity was evaluated using item- and scale-level content validity indices.
Results: The literature review identified communication and situational awareness as the most consistently operationalized competencies in crisis-oriented instruments. Through two Delphi rounds with a 100% response rate, consensus was reached on 11 final competency items: five in communication and six in situational awareness. First-round agreement averaged 96% (range 82– 100%). All items achieved an item-level content validity index of 1.00, yielding a scale-level content validity index of 1.00.
Conclusion: Situational awareness and communication emerged as the core nontechnical competency domains for anesthesia crisis management in the Indonesian context. These findings constitute a preliminary, expert-consensus framework with content-validity evidence within the panel, providing a theoretically informed foundation for national anesthesia training and assessment; pilot implementation, inter-rater reliability, and construct and criterion-related validity are required next steps before operational deployment.
Keywords: nontechnical skills, anesthesia, Delphi method, communication, situational awareness
Introduction
Crises may arise during anesthetic practice and pose significant threats to patient safety. Compared with many other medical disciplines, anesthesiology plays a central leadership role in ensuring safe perioperative care. Prior to the 1980s, anesthesia-related mortality was estimated to range between 1 in 2,500 and 1 in 5,000 cases. Advances in technology and patient monitoring have markedly reduced this risk, with current estimates suggesting anesthesia-related mortality of approximately 1 in 100,000 cases. Despite these improvements, anesthesia-related adverse events remain common, with minor perioperative incidents reported in 18–22% of cases and severe events occurring in 0.45–1.4%.1,2
Anesthesiology is a complex and dynamic specialty in which crises may occur without warning. During such events, anesthesiologists must rapidly recognize and interpret changes in patient status, manage competing clinical demands, and lead interprofessional teams while maintaining continuous patient care. Crisis conditions often arise from a combination of patient comorbidities, procedural complexity, and equipment-related challenges, all of which may threaten life.3,4
Human error remains a leading contributor to anesthesia-related morbidity and mortality, with early studies demonstrating that it accounts for more than 80% of preventable anesthetic incidents, far exceeding equipment-related failures.4 Further, newer analyses have continued to implicate breakdowns in cognitive processing and team interaction in the majority of preventable perioperative harm.5,6 While technical proficiency and medical knowledge remain central to safe anesthetic care, nontechnical skills, ie. the social and personal-resource skills that complement technical performance, represent a critical and modifiable domain for improving outcomes during crises.5,7
Within the nontechnical skills domain, situational awareness and communication have been frequently identified as two of the competencies most consistently implicated in safe crisis performance. Communication failures and impaired situational awareness are repeatedly identified as the most common contributors to adverse anesthetic events, even among technically proficient practitioners,4,5 and a recent analysis from the Anesthesia Patient Safety Foundation attributed approximately three quarters of preventable patient harm to situational-awareness breakdowns.6 Situational awareness, conceptualized in Endsley’s model as the perception of relevant cues, comprehension of their meaning, and projection of future states, enables clinicians to detect deterioration, integrate multimodal information, and anticipate evolving trajectories under time pressure.8 Effective communication, on the other hand, is the mechanism through which situational awareness is shared across the team, mental models are aligned, and coordinated action is achieved.9 High-reliability-organization theory similarly identifies collective mindfulness, anticipatory thinking, and open communication as the core mechanisms that interrupt error cascades in complex, high-risk systems.10,11
Other nontechnical skills described in established frameworks, including leadership, decision-making, teamwork, task management, and adaptability, remain important to anesthesia crisis performance.7,12–16 However, these competencies are functionally dependent on accurate situational awareness and effective communication: leadership cannot direct action without a shared understanding of the evolving clinical situation, and time-critical decisions cannot be made without the perceptual and interpretive foundations that situational awareness provides.9 For this reason, the present study focuses on situational awareness and communication as foundational competencies on which other nontechnical skills depend. The aim is not to dismiss the other domains, but to start with a core set that can be grounded in the local context.
In Indonesia, anesthesiology training standards are defined by national regulations, which include competencies such as communication, leadership, decision-making, and teamwork.17,18 However, other key nontechnical skills, particularly situational awareness and task management, are not explicitly emphasized. Moreover, despite growing recognition of the importance of nontechnical skills in crisis management, there remains limited consensus on how these competencies should be defined and prioritized within the national training and practice context. This lack of conceptual clarity hinders efforts to integrate nontechnical competencies systematically into education, assessment, and clinical performance improvement.
Much of the existing research on nontechnical skills, including widely used frameworks such as the Anesthetists’ Non-Technical Skills (ANTS) system, was developed in different cultural and healthcare contexts.7,16,19 ANTS provides a validated behavioral marker framework, but it was developed in settings characterized by explicit assertiveness norms and relatively low power distance, and its multidomain structure (leadership, teamwork, task management, situational awareness) presupposes resources for faculty development, standardized rater training, and structured simulation infrastructure that are not uniformly available across institutions.20–22 These conditions differ markedly from the Indonesian operating-room environment, where communication norms are more hierarchical and indirect23–25 and interprofessional power distance remains a documented influence on team interaction and patient safety,26 which may limit the direct transferability of ANTS behavioral markers without cultural adaptation.27
At the behavioral level, these cultural conditions affect the specific actions on which crisis management depends. High power distance and indirect communication norms have been associated with reduced frequency of speaking up to authority,23,25,28 inconsistent use of closed-loop confirmation when receiving orders from senior clinicians, delayed escalation of clinical concerns, ambiguous role clarification during rapidly evolving events, and reluctance to seek help when uncertain; each of which has been linked to preventable adverse outcomes in operating-room teams.28,29 These behaviors, rather than the broader cultural patterns themselves, are the practical targets for any locally grounded competency framework.
Two issues therefore frame the present work. First, mature international frameworks for anesthesia nontechnical skills are well validated within their settings of origin,7,16,19 but their direct application to the Indonesian context is constrained by differences in communication norms, training infrastructure, and team hierarchy. Second, no localized, expert-consensus framework currently exists for anesthesia crisis management in Indonesian clinical practice. Addressing this gap requires a method capable of integrating dispersed expert knowledge under conditions of limited comparative empirical evidence; the modified Delphi technique is well established for this purpose and has been used widely in medical-education competency development.30,31
Accordingly, this study aims to identify a preliminary set of core nontechnical competencies for anesthesia crisis management in Indonesia, with particular emphasis on situational awareness and communication, and to evaluate their content validity through expert consensus. Examining these competencies within a specific cultural and healthcare context may also contribute to broader discussions on the adaptability of established nontechnical skills frameworks across diverse health systems.
Material and Methods
Study Design
This study used an exploratory sequential qualitative design to develop a nontechnical skills assessment instrument for crisis management in anesthesia, which consists of two sequential phases: (1) a structured literature review and (2) expert consensus on core competencies using a modified Delphi method. The study was conducted between January and December 2025.
Phase 1: Structured Literature Review
A structured literature review was conducted to generate an initial pool of nontechnical skill competencies relevant to anesthesia crisis management, which served as input for subsequent expert appraisal in the Delphi process rather than as a comprehensive synthesis of the field. PRISMA-compliant systematic-review procedures, including dual independent screening and formal risk-of-bias assessment, were therefore not applied.
The eligibility criteria were defined using the PCC framework (Population, Concept, and Context).32 Studies were included if the population comprised anesthesiologists, anesthesia trainees, or other anesthesia-related professionals, including nurse anesthetists. The concept of interest was the assessment of nontechnical skills and the context was restricted within anesthesia-related clinical environments, including the operating room, intensive care unit, and emergency care settings, as well as high-fidelity simulation settings designed to replicate clinical crises. Studies were excluded if they were focused on technical skills only or did not report an original instrument intended to assess nontechnical skills in crisis management contexts. No restrictions on publication date or language were applied.
The literature search was conducted in February 2025 through four electronic databases (PubMed, Scopus, Cochrane Library, and Google Scholar). Keywords derived from the terms “anesthesia”, “nontechnical skills”, “situational awareness”, “communication”, “crisis management”, “behavior”, “education”, and “assessment” were used. Search results were optimised through the use of Boolean operators. The detailed search strategy is presented in Supplementary Table S1.
Collected articles were uploaded into the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia), and duplicates were removed.33 Title and abstract screening, full-text review, and data extraction were performed by a single reviewer (AH). Existing nontechnical skills frameworks, behavioral marker systems, and assessment instruments from anesthesia were examined, and extracted competencies were synthesized, merged, and refined to produce an initial draft list of candidate competencies, which served as the input for the Delphi process.
Phase 2: Identification of Core Nontechnical Skill Competencies (Delphi Study)
A modified Delphi technique was used to achieve expert consensus on essential nontechnical skills for anesthesia crisis management. Experts were recruited using purposive sampling, with a minimum panel size of 10 experts.34 Inclusion criteria were: (1) a minimum of 5 years of professional experience; and (2) recognized expertise in anesthesiology and intensive care, perioperative or anesthesia nursing, or medical education. Experts were recruited from academic and clinical institutions and professional organizations. Panelists remained anonymous to one another throughout the Delphi process.
The initial competency list derived from the literature review was distributed to panelists using an electronic survey platform, and panelists received standardized instructions regarding study objectives, rating procedures, and consensus criteria. Each competency was rated on a 4-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree), with optional open-text comments to allow qualitative justification, item refinement, or proposal of new competencies. For analysis, responses were dichotomised into agreement (ratings of 3 or 4) and disagreement (ratings of 1 or 2).35
Consensus was defined a priori as ≥75% agreement.36 Competencies meeting the threshold were retained; those failing to reach consensus were revised based on qualitative feedback and redistributed in subsequent rounds. Items that reached the consensus threshold but received substantive qualitative suggestions were classified as having preliminary consensus and were revised accordingly before being redistributed in subsequent rounds. The number of Delphi rounds was not fixed in advance; instead, iteration continued until predefined consensus criteria were met for all retained competencies. To ensure that the final framework would remain usable in practice, where rater cognitive load and the number of dimensions evaluated simultaneously are recognised constraints on assessment quality,37 the total number of competencies was limited to a maximum of 20 items.
Content validity was evaluated by expert rating of each item on a 4-point relevance scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, 4 = highly relevant). For Item Content Validity Index (I-CVI) calculation, ratings of 3 or 4 were classified as indicating item relevance, in line with standard CVI scoring practice. The I-CVI was calculated for each item as the proportion of panelists rating it 3 or 4; the Scale Content Validity Index (S-CVI/Ave) was calculated as the average of the I-CVI values across all retained items. Items with I-CVI ≥0.79 were accepted; items scoring 0.70–0.79 were revised, and items <0.70 were removed.38,39
Ethical Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was granted by the Ethics Committee of the Faculty of Medicine, University of Indonesia - Cipto Mangunkusumo Hospital (approval number: KET-65/UN2.F1/ETIK/PPM.00.02/2025). Prior to recruitment, each prospective panelist received an individual briefing via in-person meeting or video call, during which the study objectives, procedures, voluntary nature of participation, and confidentiality of individual responses were explained using a standardized presentation. Following this briefing, written informed consent was obtained from all participants prior to their inclusion in the study. Ongoing consent to participate in each subsequent Delphi round was further indicated through voluntary completion and return of the survey instrument.
Results
Structured Literature Review
Based on the search strategy outlined in Supplementary Table S1, a total of 307 studies were identified. After removal of duplicates, 300 studies underwent title and abstract screening. Following screening, 84 studies were assessed in full text, of which 67 were excluded for the reasons detailed in Figure 1. Ultimately, 17 studies were deemed relevant and were used to inform the development of nontechnical skill competency items and the assessment instrument. The summary of relevant nontechnical skills measured is provided in Table 1.
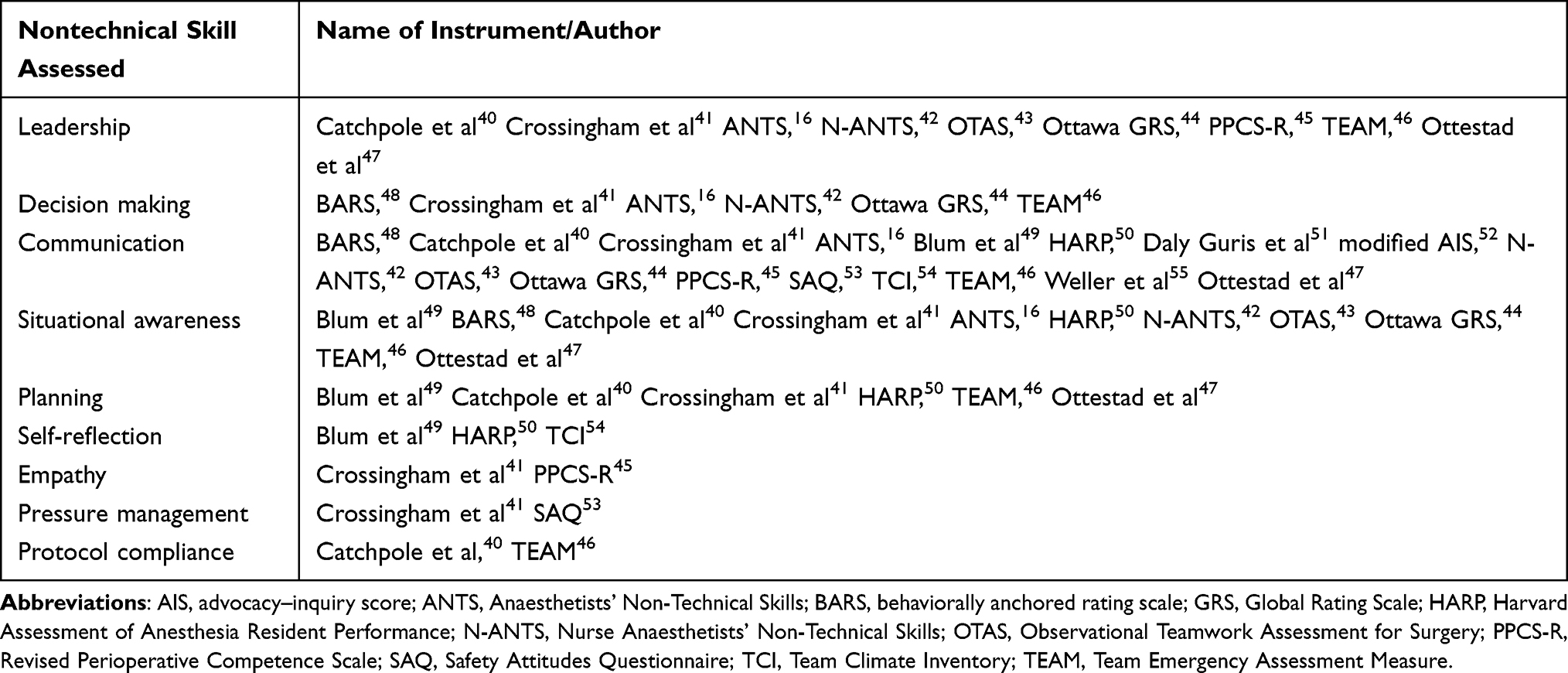 |
Table 1 Summary of Nontechnical Skills Assessed in Previous Studies |
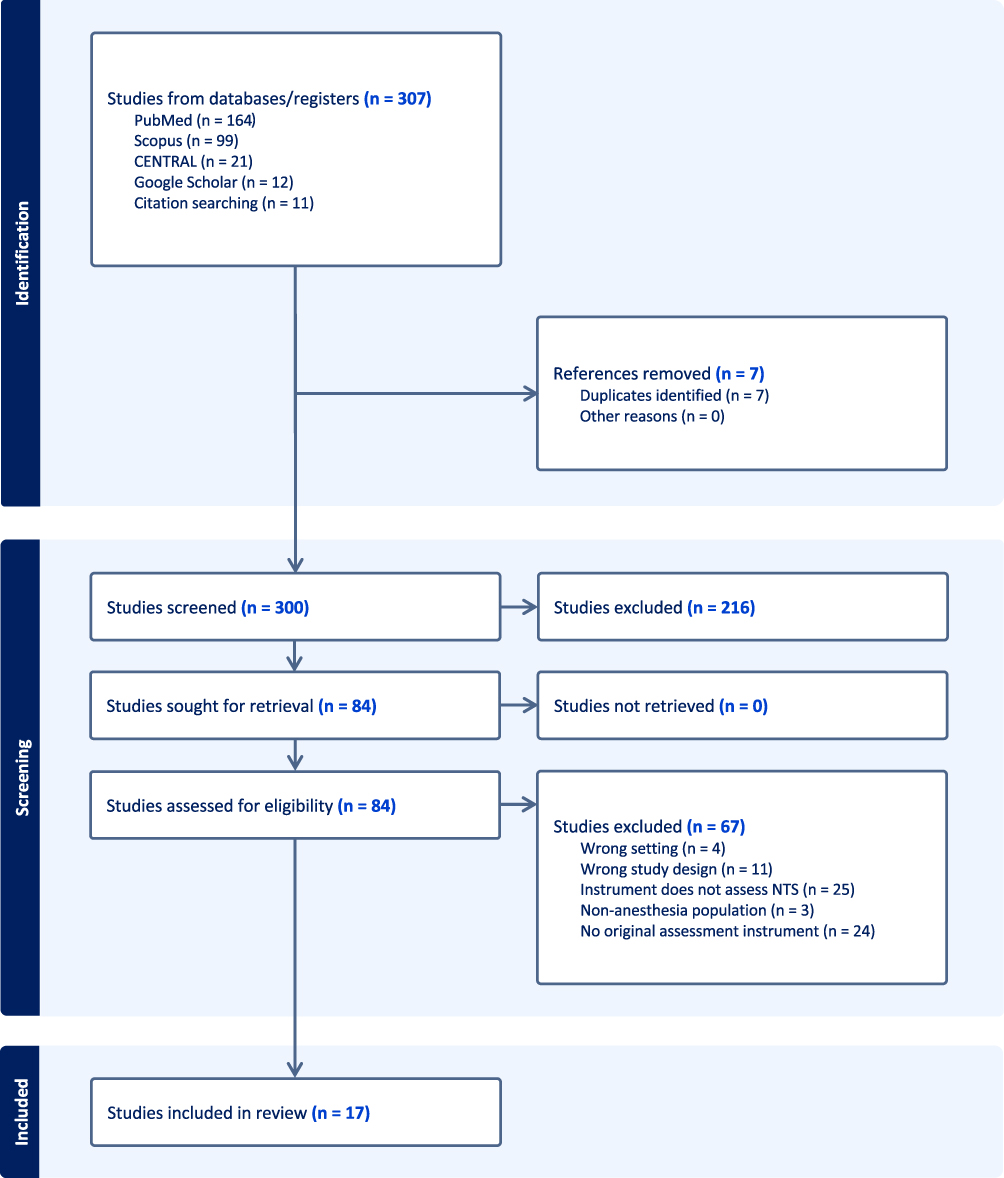 |
Figure 1 Flow diagram of the study identification process for the structured literature review. |
Of the 17 included studies, five instruments, ie. the Behaviorally Anchored Rating Scale (BARS),48 modified advocacy–inquiry score (AIS),52 Ottawa Global Rating Scale (GRS),44 Team Emergency Assessment Measure (TEAM),46 and the nontechnical scorecard by Ottestad et al47 were specifically designed to assess performance in crisis management contexts. The remaining twelve instruments evaluated nontechnical skills in broader, non–crisis-specific clinical settings.16,40–43,45,49–51,53–55
Among the five crisis-specific instruments, the most consistently assessed nontechnical skills were situational awareness, communication, and leadership. Situational awareness was operationalized through behaviours such as continuous patient monitoring, detection of deteriorating conditions, and anticipation of evolving clinical events.44,46,47 Communication was assessed through structured information exchange, use of both verbal and non-verbal methods, closed-loop communication, and assertive speaking up during critical situations.44,46,47,52 Leadership was evaluated through behaviours related to direction-giving, task delegation, and maintenance of team coordination under pressure.44,46,47 Decision-making was also assessed in several instruments, reflecting the time-critical nature of crisis scenarios.48 Notably, planning and teamwork appeared in some crisis-specific tools as supporting domains,46,47 often operationalized as components of situational awareness or leadership rather than as standalone constructs.
Communication
The most frequently reported nontechnical skill domain was communication, which was evaluated by all of the identified studies.40–55 Communication was operationalised using a variety of behavioural, observational, and attitudinal indicators. In the Behaviourally Anchored Rating Scale (BARS), communication was assessed through explicit behavioural descriptors related to speaking up, structured information exchange, and the use of non-verbal communication.48 Similarly, Catchpole et al and the Modified Score System for Advocacy-Inquiry emphasised the importance of speaking up within teams and highlighted the role of structured communication.40,52 In addition, these tools underscored the importance of minimising unnecessary communication during critical tasks.40 Collectively, these items reflect communication being measured primarily through observable, task-focused interactions and patterns of information flow within the team.
Within anesthesia-specific tools such as ANTS and N-ANTS,16,42 communication was defined as a core nontechnical skill encompassing the exchange of information, coordination of activities, and demonstration of authority and clarity when interacting with team members. The Harvard Assessment of Anesthesia Resident Performance (HARP) and the framework proposed by Weller et al similarly emphasised the necessity of clarity and assertiveness in communication.50,55 This concept was further articulated by Daly Guris et al, who defined assertive communication as the ability to convey ideas clearly, directly, and without hesitation.51 Together, these instruments conceptualised communication largely in terms of individual communication style, assertiveness, and effectiveness in interpersonal interactions.
Several instruments assessed communication using items that captured perceptions of communication quality and adaptability. In the Revised Perioperative Competence Scale (PPCS-R), communication was measured through items such as using appropriate communication methods according to situational needs, tailoring communication based on team personalities, and employing language that is appropriate to the clinical context.45
Finally, attitudinal aspects of communication were primarily captured through the Safety Attitudes Questionnaire (SAQ) and the Team Climate Inventory (TCI).53,54 These instruments measured communication indirectly through team members’ perceptions, including whether individual views were listened to, whether information was shared openly, comfort in expressing new ideas, willingness to listen to colleagues’ problems, and the presence or absence of blame within the team. This indicates that, in these tools, communication was assessed at the level of team climate and psychological safety rather than through direct observation of communicative behaviours. A summary of the identified sub-components of communication across the instruments is provided in Table 2.
 |
Table 2 Sub-Components of Communication Identified Across Included Instruments |
Situational Awareness
Situational awareness was also commonly assessed and was reported across multiple instruments, including in both anesthesia-specific tools (eg., ANTS, N-ANTS, HARP) and more general team-based assessment instruments.16,40–44,46,48–50 Across the included studies, situational awareness was operationalised using a combination of behavioural indicators, cognitive processes, and observational markers related to perception, understanding, and anticipation of clinical events.
In the ANTS16 and N-ANTS42 frameworks, situational awareness was assessed through components such as gathering information, recognising and understanding relevant cues, and anticipating future states. Similarly, in several observational tools, including BARS,48 OTAS,43 TEAM,46 and Ottawa GRS,44 situational awareness was reflected in observable behaviours such as tracking relevant information, detecting emerging problems, and adjusting actions in response to situational demands.
Several tools further operationalised situational awareness by providing explicit behavioural examples to differentiate effective and ineffective performance. In particular, Catchpole et al40 described specific markers of good situational awareness, such as ensuring that monitors and infusion pumps are clearly visible, and markers of poor situational awareness, such as failure to maintain visibility of critical equipment. The ANTS framework similarly provided behavioural indicators of poor practice, including not asking relevant questions and becoming distracted from the clinical environment.16 In HARP,50 situational awareness was also reflected in participants’ ability to recognise clinical problems, such as bleeding or hypertension, in a timely manner. Collectively, these instruments assessed situational awareness using concrete behavioural anchors that enabled raters to distinguish between varying levels of performance. A summary of the identified sub-components of situational awareness is provided in Table 3.
 |
Table 3 Sub-Components of Situational Awareness Identified Across Included Instruments |
Other Nontechnical Skills
In addition to communication and situational awareness, several other nontechnical skill domains were assessed across the included studies, although these were reported less consistently and in fewer instruments. These domains included leadership, decision making, planning, self-reflection, empathy, pressure management, and protocol compliance (Table 1).
Leadership was assessed in multiple instruments, including both anesthesia-specific and general team-based tools. Specifically, leadership was reported in studies by Catchpole et al40 and Crossingham et al41 as well as in the ANTS,16 N-ANTS,42 OTAS,43 Ottawa GRS,44 PPCS-R,45 TEAM,46 and the framework proposed by Ottestad et al47 This indicates that leadership was among the more frequently assessed nontechnical skills outside communication and situational awareness. Similarly, decision making was also evaluated in several instruments, including BARS,48 ANTS,16 N-ANTS,42 Ottawa GRS,44 TEAM,46 and the framework described by Crossingham et al.41
Planning was reported in a smaller subset of studies and instruments, including those by Blum et al49 Catchpole et al40 Crossingham et al41 Ottestad et al47 and in HARP50 and TEAM.46 However, it should be noted that some tools include planning as a subset to situational awareness.
Several nontechnical skills were assessed in only a limited number of tools. Self-reflection was reported in Blum et al49 HARP,50 and TCI,54 while empathy was assessed in Crossingham et al41 and PPCS-R. Pressure management was included in only two instruments, namely Crossingham et al41 and SAQ.53 Finally, protocol compliance was assessed in Catchpole et al40 and TEAM.46
Delphi Study
Panel Participation
The expert panel consisted of 13 professionals with diverse backgrounds in anesthesiology, surgery, patient safety, and health professions education. A detailed breakdown of panel composition is presented in Table 4.
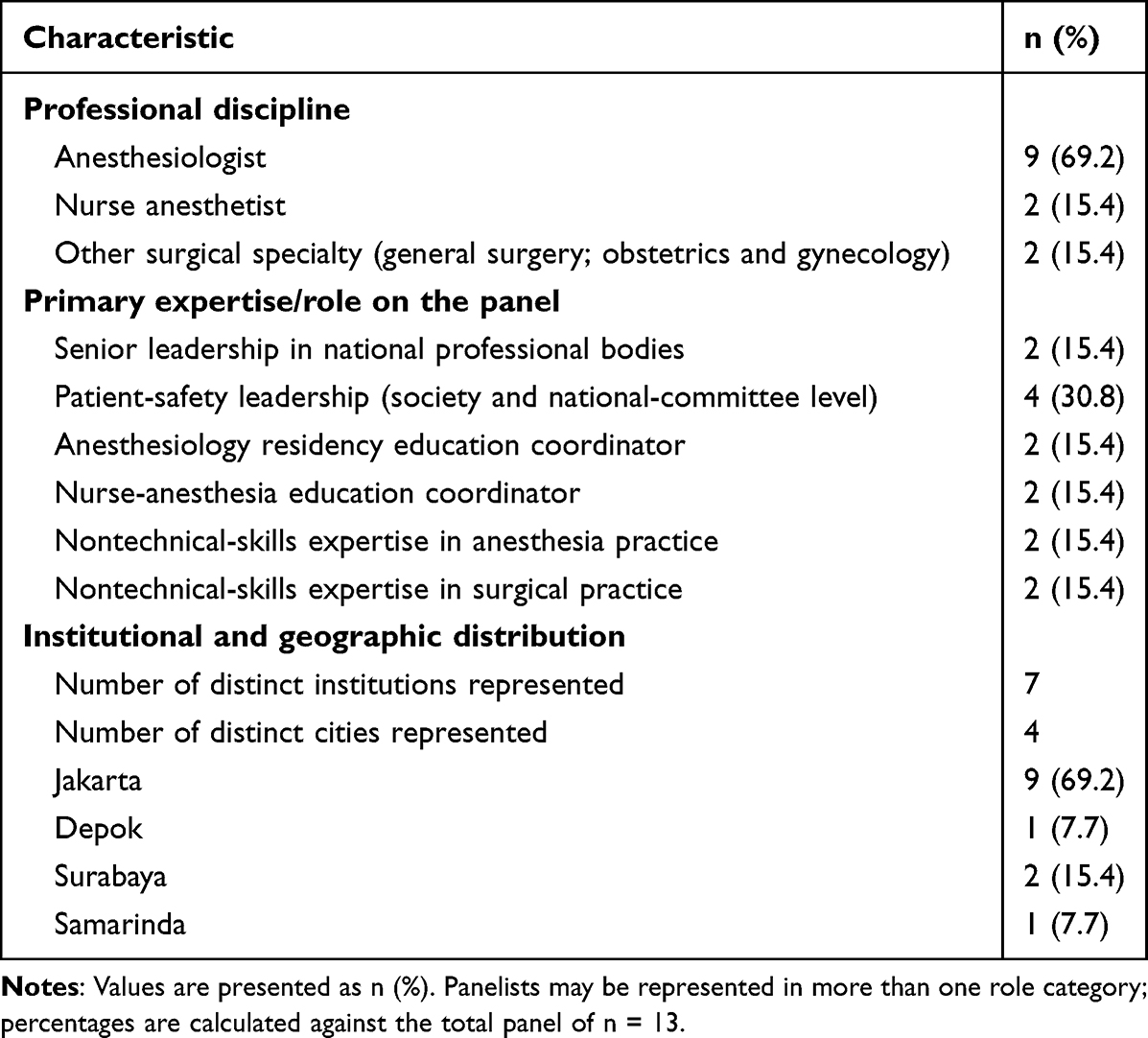 |
Table 4 Characteristics of the Expert Delphi Panel (n = 13) |
Two panelists held senior leadership positions in national-level professional bodies. One was Head of the Division for Competency Development at the Indonesian College of Anesthesiology, and the other was Chair of the National Committee for Patient Safety. Both contributed perspectives shaped by national-level responsibility for anesthesia competency standards and patient safety policy, respectively.
Patient-safety expertise was further represented by three additional anesthesiologists actively involved in patient-safety initiatives within professional societies. Two panelists were practicing anesthesiologists with specific expertise in nontechnical skills, and two others served as coordinators of anesthesiology residency education, contributing perspectives from postgraduate medical training and curriculum development.
Interprofessional and cross-disciplinary perspectives were incorporated through two nurse anesthetists who served as coordinators of nurse-anesthesia education, and through two non-anesthesia surgical specialists, ie. a general surgeon and an obstetrician–gynecologist, both with particular interest and expertise in nontechnical skills in surgical practice.
The panel was drawn from four cities across Indonesia: Jakarta (9 panelists), Surabaya (2 panelists), Depok (1 panelist), and Samarinda (1 panelist). Twelve panelists were based in Java and one in East Kalimantan (Samarinda).
In each Delphi round, one Email containing the questionnaire was distributed to all panel members, followed by up to three reminder emails. This process resulted in a 100% response rate, with no panel members withdrawing from the study.
Item Consensus
The initial questionnaire consisted of 10 items, five regarding “Communication” and five regarding “Situational Awareness”, respectively. The first round resulted in an average agreement of 96%, varying from 82 to 100%. Eight items reached full consensus (≥75% agreement) without substantive qualitative concerns and were retained without modification. Two items received preliminary consensus, ie. meeting the agreement threshold but accompanied by qualitative suggestions for rewording, and were revised accordingly before redistribution. One panelist proposed an additional item pertaining to pre-action preparation, specifically the checking of equipment and ensuring that all team members understand their respective roles (item 2.2), which was deemed conceptually distinct from the existing situational awareness items and was incorporated into Round 2 after review by the research team.
Round 2 consisted of three items: the two revised items from Round 1 and the newly added item. All three reached full consensus in Round 2, with no further items proposed or returned for re-discussion. In total, consensus was reached on 11 items across two rounds (Figure 2), comprising five communication items and six situational awareness items, as presented in Table 5. The full audit trail of item wording, rating distributions, qualitative comments, and revisions across both rounds is presented in Supplementary Table S2.
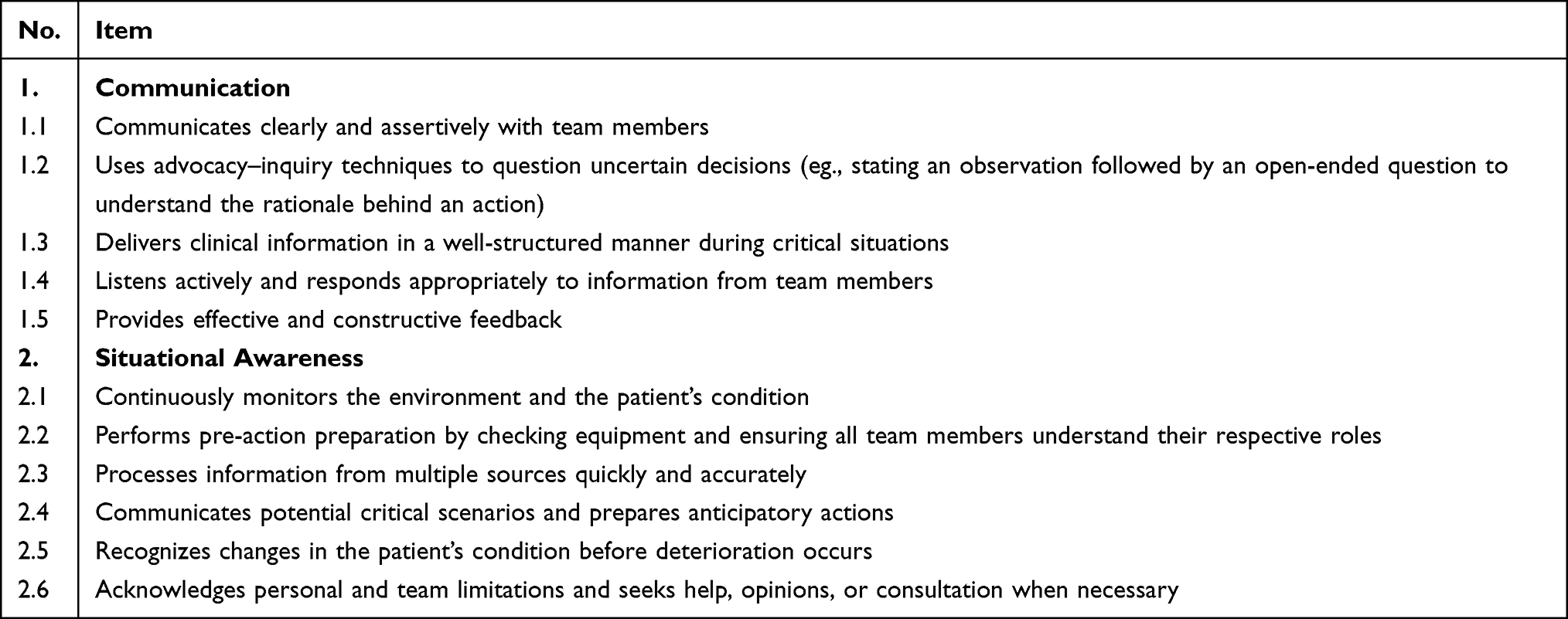 |
Table 5 Core Nontechnical Competencies Identified Through Expert Consensus |
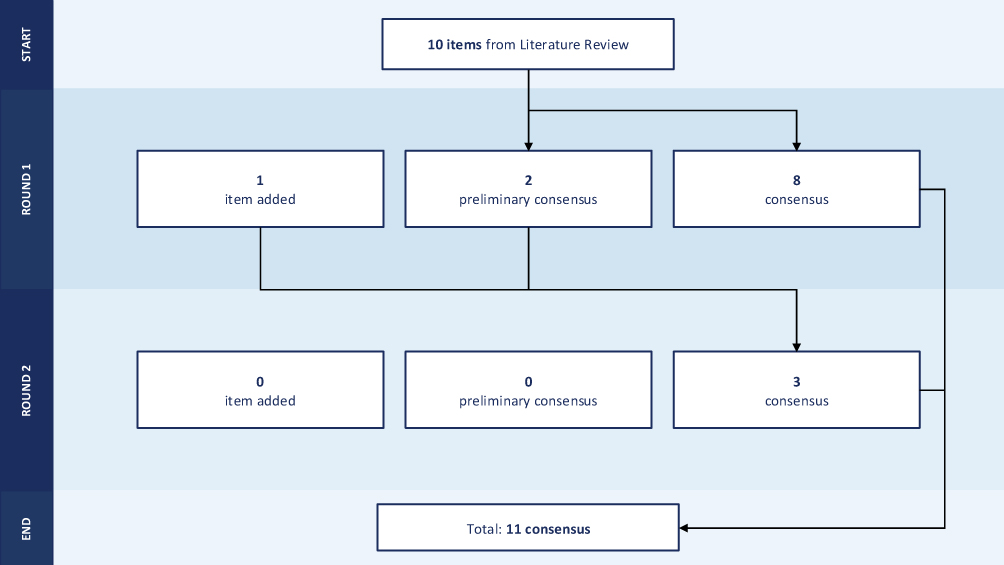 |
Figure 2 Flowchart of the Delphi Study. |
Content Validity
Content validity analysis showed that all items demonstrated excellent item-level content validity. Each item was rated as relevant (score of 3 or 4) by all experts, yielding an Item Content Validity Index (I-CVI) of 1.00 for each item (Supplementary Table S3). The scale-level content validity index (S-CVI/Ave) was also 1.00. Consequently, no items were revised or removed.
Discussion
This study identified, through structured literature review and modified-Delphi expert consensus, a preliminary set of core nontechnical competencies for anesthesia crisis management in Indonesia, with particular emphasis on situational awareness and communication. The literature review demonstrated that, although nontechnical skills are commonly conceptualized within broad multidomain frameworks, situational awareness and communication consistently emerge as the most frequently operationalized competencies in high-acuity and crisis-oriented contexts. These findings were reinforced by expert consensus, in which situational awareness and communication were prioritized as central competencies for safe and effective crisis performance. Further, content validity analysis demonstrated strong agreement across the expert panel, with all items achieving an I-CVI of 1.00 and a scale-level S-CVI/Ave of 1.00. Together, the results highlight the foundational role of these cognitive and interpersonal domains in anesthesia crisis management within the national training and practice context.
Interpretation of Findings
Situational awareness (SA) emerged as a central competency in both the literature review and the Delphi consensus, underscoring its critical role in anesthesia crisis management. Across nontechnical skills frameworks, situational awareness is among the most frequently operationalized domains, particularly in instruments designed for high-acuity or crisis settings.44,46–48 In time-critical clinical environments, clinicians must continuously detect evolving physiological changes, interpret complex and sometimes conflicting data streams, and anticipate potential deterioration.8 These demands likely explain why situational awareness consistently appears as a foundational competency underpinning effective teamwork and decision-making during crises.
The prominence of situational awareness in crisis contexts is theoretically grounded in Endsley’s cognitive model, which conceptualizes SA as comprising three hierarchical levels: perception of relevant environmental cues (Level 1), comprehension of their meaning (Level 2), and projection of future states (Level 3).56 The competencies identified in this study map onto this hierarchical structure: items emphasizing continuous monitoring and pre-action verification correspond to Level 1 (perception); items focusing on pattern recognition and information integration align with Level 2 (comprehension); and items involving anticipatory preparation capture Level 3 (projection). This conceptual alignment is consistent with established nontechnical skills frameworks. Instruments such as ANTS16 and the Situation Awareness Global Assessment Technique (SAGAT)57 similarly distinguish between information gathering, synthesis, and forecasting through detailed behavioral markers, enabling structured training and performance assessment under stress. The convergence between these frameworks and the consensus-derived competencies strengthens the theoretical validity of prioritizing situational awareness and emphasizes the need for educational strategies that deliberately cultivate abilities across all three levels.
Communication emerged as a co-dominant competency in both the literature review and the Delphi consensus, underscoring its essential role in anesthesia crisis management. In high-acuity situations, effective communication facilitates the development of shared situational awareness, supports task coordination, and enables timely decision-making under pressure. Communication failures, such as incomplete information transfer, lack of closed-loop confirmation, and unspoken concerns, have been consistently implicated in preventable adverse events, particularly in time-critical and hierarchically structured environments.58–60 The competencies identified in this study reflect this operational role: items emphasizing clear role delegation, explicit verbalization of clinical concerns, and anticipatory information sharing support coordinated team response during rapidly evolving events, mirroring the behavioral markers operationalized in ANTS and other team-based performance tools.16,46,47,52 The convergence between the consensus findings and existing frameworks reinforces the importance of embedding structured communication training, particularly in simulation-based crisis scenarios,61 into anesthesia education to enhance team coordination and patient safety.
The emphasis on assertive communication and advocacy-inquiry techniques in this study carries particular significance within the Indonesian clinical context. Communication norms in Indonesia have been characterized in the published literature as marked by high power distance and indirect expression, which may discourage speaking up or challenging authority, particularly in hierarchical team structures such as those encountered in the operating room.23,24 Consistent with these established characterizations, the panel’s prioritization of assertive communication and advocacy-inquiry in this study can be interpreted as a deliberate response to the specific behavioral patterns that high power distance is reported to influence, ie. reduced speaking up to authority, inconsistent closed-loop confirmation, delayed escalation of clinical concerns, and reluctance to seek help when uncertain.28
While the literature review identified several other nontechnical skill domains, including leadership, decision-making, teamwork, and task management, the decision to focus on situational awareness and communication was made on the basis of two considerations. First, these two domains were the most consistently operationalized competencies across the 17 included studies, appearing in all five crisis-specific instruments identified. Second, the remaining domains are functionally dependent on accurate situational awareness and effective communication; leadership cannot direct action without a shared understanding of the evolving situation, and decisions cannot be enacted without structured information exchange.5–9 This empirical and theoretical rationale guided the selection of situational awareness and communication as the domains presented to the expert panel for consensus.
Theoretical Implications
Beyond the empirical findings reported above, the prioritization of situational awareness and communication has broader implications for how anesthesia nontechnical skills are conceptualized. These two competencies align closely with established human error and human factors theories in high-risk industries. These models emphasize that adverse events rarely result from isolated technical failures but rather from breakdowns in cognitive processing, team interaction, and system coordination. In particular, failures in perception, comprehension, and projection of evolving situations may initiate error cascades, while ineffective communication compounds these vulnerabilities by preventing the formation of shared mental models among team members.62,63 High-reliability organization (HRO) principles similarly stress the importance of collective mindfulness, anticipatory thinking, and open communication in preventing escalation of minor deviations into major failures.64 Viewed through this lens, situational awareness and communication function as core protective mechanisms that interrupt error propagation and enhance resilience during anesthesia crises; these theoretical alignments, however, represent interpretive context for the present findings rather than empirical claims established by this study.
Translating these competencies into educational practice in the Indonesian context calls for concrete operationalization rather than direct adoption of frameworks developed elsewhere. Several directions can be considered from the established literature on speaking-up and graded-assertiveness training. First, scripted advocacy-inquiry phrasing adapted to local linguistic norms can lower the activation energy for junior team members to raise concerns; for example, an observation followed by an open-ended question preserves respect for hierarchy while explicitly inviting a clinical decision.65 Second, graded-assertiveness tools such as the PACE (Probe, Alert, Challenge, Emergency) or CUSS (Concerned, Uncomfortable, Safety issue, Stop) frameworks provide stepwise scripts that have been shown to durably increase the number and quality of challenges by anesthesia residents in subsequent simulated emergencies.65,66 These can be taught and rehearsed in local language and adapted to address the specific authority gradients encountered in Indonesian operating rooms. Third, structured debriefing after simulation can normalize junior team members questioning senior decisions and create the psychological safety needed for these behaviors to transfer to clinical practice.67 Embedding these specific scripts and tools into anesthesia residency curricula in Indonesia, rather than transplanting Western frameworks unmodified, is likely to enhance both the relevance and the uptake of the competencies identified in this study.
Building on these findings, several educational directions warrant consideration. First, training programs should move beyond implicit exposure to nontechnical skills and instead incorporate explicit instruction on the cognitive components of situational awareness, such as perception, comprehension, and projection, alongside structured communication strategies such as closed-loop communication and anticipatory information sharing. Embedding these competencies within curricula ensures that they are taught as core clinical skills rather than supplementary attributes.68,69
Second, training should be deliberately designed to challenge learners’ situational awareness across all three levels, incorporating dynamic patient trajectories, evolving data, and decision points that require anticipatory reasoning. Scenarios should also assess and reinforce communication behaviours that promote shared mental models and coordinated action under time pressure. Structured debriefing, which has been shown to improve non-technical skills among anesthesia residents,70 may be particularly effective when it explicitly addresses situational awareness breakdowns and communication lapses, thereby enhancing reflective learning and performance improvement.
Third, assessment practices should align with these priorities. Incorporating validated behavioral markers for situational awareness and communication into simulation and workplace-based evaluations may enhance the quality of feedback and promote accountability in professional development. Embedding these competencies systematically across training, simulation, and assessment may contribute to greater resilience and safety in high-risk anesthesia care, though direct evidence linking the present competency set to patient-safety outcomes will require prospective implementation and evaluation studies. More broadly, this framework can serve as the conceptual foundation for developing a dedicated training module and a structured assessment instrument for the Indonesian anesthesia context. Developing both in parallel from the same competency scaffold would help align what is taught with what is measured, and would establish the basis for subsequent psychometric evaluation.
Limitations and Future Directions
Several limitations warrant acknowledgment. First, this study focused on identifying and achieving expert consensus on core competencies rather than conducting full psychometric validation of a measurement instrument. Although the competencies identified demonstrated strong content validity, their translation into an operational assessment tool requires further investigation, including pilot implementation, evaluation of inter-rater reliability, and accumulation of construct and criterion-related validity evidence.71
Second, the perfect content validity indices should be interpreted with caution. In small panels, perfect scores carry a recognised risk of inflation through chance agreement,72,73 and a related concern arises when items are derived from a shared initial source, in this case the structured literature review, since framing and anchoring effects can shape panelists’ independent judgments, a Delphi limitation that heterogeneous panel composition partly mitigates.74,75 Although the panel was deliberately recruited from multiple institutions, four cities, and five distinct professional-role categories to limit this concern, some professional-network overlap inherent to a national specialty community could not be fully eliminated. The indices therefore reflect strong agreement on relevance within the panel rather than independent psychometric validation, and the rapid convergence across two Delphi rounds is best understood as agreement on a well-bounded set of competencies. Establishing broader validity will require external review, larger and more diverse samples, and construct-level psychometric testing.76
Third, the findings reflect the perspectives of experts within the Indonesian clinical context, which was an intentional design feature given the study’s aim of developing locally grounded competencies. Rather than limiting the study’s value, this contextual specificity strengthens the relevance of the identified competencies for national training and assessment purposes. Nevertheless, replication studies in other cultural and healthcare settings would be valuable to determine how these competencies are interpreted and prioritized elsewhere, and to contribute to broader comparative evidence on the contextual sensitivity of nontechnical skills frameworks.
Fourth, although the literature synthesis provided a structured overview of existing nontechnical skills frameworks, it did not fully adhere to the methodological standards of a systematic review, such as dual independent screening and formal risk-of-bias assessment.77 Future research employing more rigorous review methodologies may further strengthen the evidentiary foundation for competency development in anesthesia crisis management.
Conclusion
This study identified, through structured literature synthesis and expert consensus, a preliminary set of contextually grounded core nontechnical competencies for anesthesia crisis management in Indonesia. Situational awareness and communication emerged as central domains, reflecting their foundational role in enabling effective decision-making, coordination, and resilience in high-risk clinical environments. The consensus-derived competencies, including assertive communication and advocacy-inquiry techniques, are consistent with the hierarchical communication norms documented in the published literature as characteristic of Indonesian clinical practice, suggesting that nontechnical skills frameworks may benefit from contextual adaptation to ensure relevance in diverse healthcare settings. By prioritizing these competencies within the national training context, this work provides a theoretically informed foundation for targeted educational, simulation, and assessment strategies. The validity evidence reported here is limited to content validity; pilot implementation, inter-rater reliability, and construct and criterion-related validity evidence remain necessary next steps before the framework can be operationalized as an assessment instrument. The framework is intended to support, rather than directly demonstrate, safer anesthesia practice. Whether its implementation translates into measurable improvements in clinical performance and patient safety would need to be established through subsequent prospective evaluation.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Staender SEA, Mahajan RP. Anesthesia and patient safety: have we reached our limits? Curr Opin Anaesthesiol. 2011;24(3):349–16. doi:10.1097/ACO.0b013e328344d90c
2. Mellin-Olsen J, Staender S, Whitaker DK, Smith AF. The Helsinki Declaration on Patient Safety in Anaesthesiology. Eur J Anaesthesiol. 2010;27(7):592–597. doi:10.1097/EJA.0b013e32833b1adf
3. Burden A. The history of crises and crisis management in anesthesia: prevention, detection, and recovery. Int Anesthesiol Clin. 2020;58(1):2–6. doi:10.1097/AIA.0000000000000258
4. Cooper JB, Newbower RS, Long CD, McPeek B. Preventable anesthesia mishaps: a study of human factors. Anesthesiology. 1978;49(6):399–406. doi:10.1097/00000542-197812000-00004
5. Kelly FE, Frerk C, Bailey CR, et al. Implementing human factors in anaesthesia: guidance for clinicians, departments and hospitals: guidelines from the Difficult Airway Society and the Association of Anaesthetists. Anaesthesia. 2023;78(4):458–478. doi:10.1111/anae.15941
6. Tscholl DW, Hunn CA, Gasciauskaite G. Three quarters of preventable patient harm stems from situation awareness breakdowns: recognizing and addressing the core issue. APSF Newsletter. 2024;39:29–30.
7. Flin R, Patey R, Glavin R, Maran N. Anaesthetists’ non-technical skills. Br J Anaesth. 2010;105(1):38–44. doi:10.1093/bja/aeq134
8. Schulz CM, Endsley MR, Kochs EF, Gelb AW, Wagner KJ. Situation Awareness in Anesthesia: concept and Research. Anesthesiology. 2013;118(3):729–742. doi:10.1097/ALN.0b013e318280a40f
9. Weller JM, Mahajan R, Fahey-Williams K, Webster CS. Teamwork matters: team situation awareness to build high-performing healthcare teams, a narrative review. Br J Anaesth. 2024;132(4):771–778. doi:10.1016/j.bja.2023.12.035
10. Sutcliffe KM. Building Cultures of High Reliability. Anesthesiol Clin. 2023;41(4):707–717. doi:10.1016/j.anclin.2023.03.012
11. Fricke J, Galligan M, Douma C, Souder J, Mull N; Johns Hopkins University Evidence-based Practice Center. Examining the Impact of Implementing High-Reliability Organization Principles on Patient Safety Outcomes. AHRQ. 2025. doi:10.23970/AHRQEPC_MHS4HRO
12. Cook TM, Woodall N, Frerk C. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. Br J Anaesth. 2011;106(5):617–631. doi:10.1093/bja/aer058
13. Wilson RM, Harrison BT, Gibberd RW, Hamilton JD. An analysis of the causes of adverse events from the Quality in Australian Health Care Study. Med J Aust. 1999;170(9):411–415. doi:10.5694/j.1326-5377.1999.tb127814.x
14. de Oliveira GS, Chang R, Fitzgerald PC, et al. The Prevalence of Burnout and Depression and Their Association with Adherence to Safety and Practice Standards: a Survey of United States Anesthesiology Trainees. Anesthesia Analg. 2013;117(1):182–193. doi:10.1213/ANE.0b013e3182917da9
15. Gjeraa K, Jepsen RMHG, Rewers M, Østergaard D, Dieckmann P. Exploring the relationship between anaesthesiologists’ non-technical and technical skills. Acta Anaesthesiol Scand. 2016;60(1):36–47. doi:10.1111/aas.12598
16. Fletcher G, Flin R, McGeorge P, Glavin R, Maran N, Patey R. Anaesthetists’ Non-Technical Skills (ANTS): evaluation of a behavioural marker system. Br J Anaesth. 2003;90(5):580–588. doi:10.1093/bja/aeg112
17. Konsil Kedokteran Indonesia. Peraturan Konsil Kedokteran Indonesia Nomor 37 Tahun 2015 Tentang Standar Pendidikan Dokter Spesialis Anestesiologi Dan Terapi Intensif. Konsil Kedokteran Indonesia; 2015.
18. Konsil Kedokteran Indonesia. Peraturan Konsil Kedokteran Indonesia Nomor 38 Tahun 2015 Tentang Standar Kompetensi Dokter Spesialis Anestesiologi Dan Terapi Intensif. Konsil Kedokteran Indonesia; 2015.
19. Zwaan L, Tjon Soei Len L, Wagner C, van Groeningen D, Kolenbrander M, Krage R. The reliability and usability of the Anesthesiologists’ Non-Technical Skills (ANTS) system in simulation research. Adv Simul. 2016;1:18. doi:10.1186/s41077-016-0013-2
20. Feldman M, Lazzara EH, Vanderbilt AA, DiazGranados D. Rater training to support high-stakes simulation-based assessments. J Contin Educ Health Prof. 2012;32(4):279–286. doi:10.1002/chp.21156
21. Quilici AP, Bicudo AM, Gianotto-Oliveira R, Timerman S, Gutierrez F, Abrão KC. Faculty perceptions of simulation programs in healthcare education. Int J Med Educ. 2015;6:166–171. doi:10.5116/ijme.5641.0dc7
22. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
23. Lee SE, Choi J, Lee H, Sang S, Lee H, Hong HC. Factors Influencing Nurses’ Willingness to Speak Up Regarding Patient Safety in East Asia: a Systematic Review. RMHP. 2021;14:1053–1063. doi:10.2147/RMHP.S297349
24. Claramita M, Susilo AP. Improving communication skills in the Southeast Asian health care context. Perspect Med Educ. 2014;3(6):474–479. doi:10.1007/S40037-014-0121-4
25. Valencia MIB, Ceballos KR. Speaking up in the Operating Room: Escalating Concerns. World Federation of Societies of Anaesthesiologists; 2023. Available from: https://resources.wfsahq.org/wp-content/uploads/atow-490-00.pdf.
26. Rahayu SA, Widianto S, Defi IR, Abdulah R. Does power distance in healthcare teams linked to patient satisfaction? A multilevel study of interprofessional care teams in a referral hospital in Indonesia. BMC Health Serv Res. 2024;24(1):83. doi:10.1186/s12913-023-10534-3
27. Jepsen RMHG, Spanager L, Lyk-Jensen HT, Dieckmann P, Østergaard D. Customisation of an instrument to assess anaesthesiologists’ non-technical skills. Int J Med Educ. 2015;6:17–25. doi:10.5116/ijme.54be.8f08
28. Lee SE, Lee JW. Effects of Hierarchical Unit Culture and Power Distance Orientation on Nurses’ Silence Behavior: the Roles of Perceived Futility and Hospital Management Support for Patient Safety. J Nurs Manage. 2024;2024(1):6564570. doi:10.1155/jonm/6564570
29. Kyynärsalmi A, Hammarén M, Kanste O. Understanding Power Distance in Healthcare: a Scoping Review. Nurs Inq. 2025;32(2):e70022. doi:10.1111/nin.70022
30. Gottlieb M, Caretta-Weyer H, Chan TM, Humphrey-Murto S. Educator’s blueprint: a primer on consensus methods in medical education research. AEM Educ Train. 2023;7(4):e10891. doi:10.1002/aet2.10891
31. Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: how to decide its appropriateness. World J Methodol. 2021;11(4):116–129. doi:10.5662/wjm.v11.i4.116
32. Hosseini MS, Jahanshahlou F, Akbarzadeh MA, Zarei M, Vaez-Gharamaleki Y. Formulating research questions for evidence-based studies. J Med Surg Public Health. 2024;2:100046. doi:10.1016/j.glmedi.2023.100046
33. McKeown S, Mir ZM. Considerations for conducting systematic reviews: evaluating the performance of different methods for de-duplicating references. Syst Rev. 2021;10(1):38. doi:10.1186/s13643-021-01583-y
34. Skulmoski GJ, Hartman FT, Krahn J. The Delphi method for graduate research. J Inform Technol Educ Res. 2007;6(1):1–21.
35. Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
36. Nayahangan LJ, Stefanidis D, Kern DE, Konge L. How to identify and prioritize procedures suitable for simulation-based training: experiences from general needs assessments using a modified Delphi method and a needs assessment formula. Med Teach. 2018;40(7):676–683. doi:10.1080/0142159X.2018.1472756
37. Tavares W, Eva KW. Exploring the impact of mental workload on rater-based assessments. Adv in Health Sci Educ. 2013;18(2):291–303. doi:10.1007/s10459-012-9370-3
38. Rubio DM, Berg-Weger M, Tebb SS, Lee ES, Rauch S. Objectifying content validity: conducting a content validity study in social work research. Social Work Res. 2003;27(2):94–104. doi:10.1093/swr/27.2.94
39. Rutherford-Hemming T. Determining Content Validity and Reporting a Content Validity Index for Simulation Scenarios. Nursing Education Perspectives. 2015;36(6):389–393. doi:10.5480/15-1640
40. Catchpole KR, De Leval MR, Mcewan A, et al. Patient handover from surgery to intensive care: using Formula 1 pit-stop and aviation models to improve safety and quality. Pediatr Anesthesia. 2007;17(5):470–478. doi:10.1111/j.1460-9592.2006.02239.x
41. Crossingham GV, Sice PJA, Roberts MJ, Lam WH, Gale TCE. Development of workplace-based assessments of non-technical skills in anaesthesia. Anaesthesia. 2012;67(2):158–164. doi:10.1111/j.1365-2044.2011.06977.x
42. Lyk-Jensen HT, Dieckmann P, Konge L, Jepsen RMHG, Spanager L, Østergaard D. Using a Structured Assessment Tool to Evaluate Nontechnical Skills of Nurse Anesthetists. AANA J. 2016;84(2):122–127.
43. Hull L, Arora S, Kassab E, Kneebone R, Sevdalis N. Observational Teamwork Assessment for Surgery: content Validation and Tool Refinement. J Am Coll Surge. 2011;212(2):234–243e5. doi:10.1016/j.jamcollsurg.2010.11.001
44. Kim J, Neilipovitz D, Cardinal P, Chiu M, Clinch J. A pilot study using high-fidelity simulation to formally evaluate performance in the resuscitation of critically ill patients: the University of Ottawa Critical Care Medicine, High-Fidelity Simulation, and Crisis Resource Management I Study. Crit Care Med. 2006;34(8):2167–2174. doi:10.1097/01.CCM.0000229877.45125.CC
45. Gillespie BM, Polit DF, Hamlin L, Chaboyer W. Developing a model of competence in the operating theatre: psychometric validation of the Perceived Perioperative Competence Scale-Revised. Int J Nurs Stud. 2012;49(1):90–101. doi:10.1016/j.ijnurstu.2011.08.001
46. Cooper S, Cant R, Porter J, et al. Rating medical emergency teamwork performance: development of the Team Emergency Assessment Measure (TEAM). Resuscitation. 2010;81(4):446–452. doi:10.1016/j.resuscitation.2009.11.027
47. Ottestad E, Boulet JR, Lighthall GK. Evaluating the management of septic shock using patient simulation. Crit Care Med. 2007;35(3):769–775. doi:10.1097/01.CCM.0000256849.75799.20
48. Watkins SC, Roberts DA, Boulet JR, McEvoy MD, Weinger MB. Evaluation of a Simpler Tool to Assess Nontechnical Skills During Simulated Critical Events. Sim Healthcare. 2017;12(2):69–75. doi:10.1097/SIH.0000000000000199
49. Blum RH, Boulet JR, Cooper JB, Muret-Wagstaff SL. Simulation-based Assessment to Identify Critical Gaps in Safe Anesthesia Resident Performance. Anesthesiology. 2014;120(1):129–141. doi:10.1097/ALN.0000000000000055
50. Blum RH, Muret-Wagstaff SL, Boulet JR, et al. Simulation-based Assessment to Reliably Identify Key Resident Performance Attributes. Anesthesiology. 2018;128(4):821–831. doi:10.1097/ALN.0000000000002091
51. Daly Guris RJ, Duarte SS, Miller CR, Schiavi A, Toy S. Training novice anaesthesiology trainees to speak up for patient safety. Br J Anaesth. 2019;122(6):767–775. doi:10.1016/j.bja.2019.01.017
52. Sydor DT, Bould MD, Naik VN, et al. Challenging authority during a life-threatening crisis: the effect of operating theatre hierarchy. Br J Anaesth. 2013;110(3):463–471. doi:10.1093/bja/aes396
53. Sexton JB, Helmreich RL, Neilands TB, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6(1):44. doi:10.1186/1472-6963-6-44
54. Anderson NR, West MA. Measuring climate for work group innovation: development and validation of the team climate inventory. J Organiz Behav. 1998;19(3):235–258. doi:10.1002/(SICI)1099-1379(199805)19:3<235::AID-JOB837>3.0.CO;2-C
55. Weller J, Clin M, Henderson R, Davies E, Henderson K, Frampton C. Building the Evidence on Simulation Validity Comparison of Anesthesiologists’ Communication Patterns. Anesthesiology. 2014;120(1):142.
56. Endsley MR. Toward a Theory of Situation Awareness in Dynamic Systems. Hum Fact. 1995;37(1):32–64. doi:10.1518/001872095779049543
57. Endsley M. Direct Measurement of Situation Awareness: validity and Use of SAGAT. Situation Awareness. 2000.
58. Douglas RN, Stephens LS, Posner KL, et al. Communication failures contributing to patient injury in anaesthesia malpractice claims. Br J Anaesth. 2021;127(3):470–478. doi:10.1016/j.bja.2021.05.030
59. Lingard L, Espin S, Whyte S, et al. Communication failures in the operating room: an observational classification of recurrent types and effects. Qual Saf Health Care. 2004;13(5):330–334. doi:10.1136/qshc.2003.008425
60. Lee H, Merry AF, Woodward-Krohn R, Weller JM. Use and effectiveness of directed, closed-loop communication in the operating theatre: mixed methods analysis of simulated clinical emergencies. Br J Anaesth. 2025;135(5):1279–1285. doi:10.1016/j.bja.2025.05.015
61. Lorello GR, Cook DA, Johnson RL, Brydges R. Simulation-based training in anaesthesiology: a systematic review and meta-analysis. Br J Anaesth. 2014;112(2):231–245. doi:10.1093/bja/aet414
62. Wu Y, Zhang S, Zhang X, Lu Y, Xiong Z. Analysis on coupling dynamic effect of human errors in aviation safety. Accid Anal Prev. 2023;192:107277. doi:10.1016/j.aap.2023.107277
63. Dörner D, Güss CD. Human error in complex problem solving and dynamic decision making: a taxonomy of 24 errors and a theory. Computers Human Behav Rep. 2022;7:100222. doi:10.1016/j.chbr.2022.100222
64. Sanders KB. British government communication during the 2020 COVID-19 pandemic: learning from high reliability organizations. Commun Culture. 2020;5(3):356–377. doi:10.1080/23753234.2020.1824582
65. Sekar H, Dharmasena D, Gunasekara A, Nauta M, Sivashanmugarajan V, Yoong W. Understanding authority gradient: tips for speaking up for patient safety (and how to enhance the listening response). Obstetc Gynaecol. 2022;24(4):272–280. doi:10.1111/tog.12829
66. Friedman Z, Perelman V, McLuckie D, et al. Challenging Authority During an Emergency—the Effect of a Teaching Intervention. Crit Care Med. 2017;45(8):e814–e820. doi:10.1097/CCM.0000000000002450
67. Rudolph JW, Simon R, Raemer DB, Eppich WJ. Debriefing as Formative Assessment: closing Performance Gaps in Medical Education. Acad Emergency Med. 2008;15(11):1010–1016. doi:10.1111/j.1553-2712.2008.00248.x
68. Perez MEC, Perez AR. Evaluating Nontechnical Skills Training in Anesthesia: a Scoping Review of Methodologies and Implementation Challenges for the Past Decade (2015–2025). Philippine J Anesthesiol. 2025;30(1):5–13. doi:10.4103/PJA.PJA_10_25
69. Yee B, Naik VN, Joo HS, et al. Nontechnical Skills in Anesthesia Crisis Management with Repeated Exposure to Simulation-based Education. Anesthesiology. 2005;103(2):241–248. doi:10.1097/00000542-200508000-00006
70. Garden AL, Le Fevre DM, Waddington HL, Weller JM. Debriefing after Simulation-Based Non-Technical Skill Training in Healthcare: a Systematic Review of Effective Practice. Anaesth Intensive Care. 2015;43(3):300–308. doi:10.1177/0310057X1504300303
71. Mokkink LB, Prinsen CAC, Bouter LM, Vet HCWD, Terwee CB. The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) and how to select an outcome measurement instrument. Braz J Phys Ther. 2016;20(2):105–113. doi:10.1590/bjpt-rbf.2014.0143
72. Almanasreh E, Moles R, Chen TF. Evaluation of methods used for estimating content validity. Res Social Administrative Pharm. 2019;15(2):214–221. doi:10.1016/j.sapharm.2018.03.066
73. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Research in Nursing & Health. 2007;30(4):459–467. doi:10.1002/nur.20199
74. Schifano J, Niederberger M. How Delphi studies in the health sciences find consensus: a scoping review. Syst Rev. 2025;14(1):14. doi:10.1186/s13643-024-02738-3
75. Winkler J, Moser R. Biases in future-oriented Delphi studies: a cognitive perspective. Technol Forecasting Social Change. 2016;105:63–76. doi:10.1016/j.techfore.2016.01.021
76. Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: a Primer. Front Public Health. 2018;6:149. doi:10.3389/fpubh.2018.00149
77. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:n71. doi:10.1136/bmj.n71.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.