Back to Journals » Journal of Pain Research » Volume 19
Deep or Superficial? Autologous Conditioned Serum for Cervical Pain with Degenerative Disc Disease – a Randomized Controlled Trial
Authors Godek P, Paprocka-Borowicz M, Ptaszkowski K ![]()
Received 5 November 2025
Accepted for publication 1 February 2026
Published 13 February 2026 Volume 2026:19 579265
DOI https://doi.org/10.2147/JPR.S579265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Piotr Godek,1 Małgorzata Paprocka-Borowicz,2 Kuba Ptaszkowski3
1Department of Orthopedics, Sutherland Medical Center, Warsaw, Poland; 2Department of Neurological Rehabilitation, Regional Specialist Hospital in Wroclaw, Wrocław, Poland; 3Division of Clinical Physiotherapy and Rehabilitation, Faculty of Physiotherapy, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Piotr Godek, Department of Orthopedics, Sutherland Medical Center, Aleja Stanów Zjednoczonych 32/14, Warsaw, 04-036, Poland, Email [email protected]
Background: Cervical pain of degenerative origin presents a therapeutic challenge due to multiple potential pain generators and the lack of a clear correlation between radiological changes and symptom severity. Autologous conditioned serum (ACS, Orthokine) has demonstrated anti-inflammatory and regenerative effects in musculoskeletal disorders.
Purpose: This study compared the efficacy of ultrasound-guided fascial versus periarticular administration of ACS in patients with cervical disc disease.
Patients and Methods: In this single-center, prospective, randomized trial (ISRCTN38950110), 100 patients of the local population with MRI-confirmed cervical disc degeneration neck pain were allocated to two groups: A (n=50) – fascial infiltration (superficial ACS administration using the hydrodissection technique around the tender points – increased soreness area, which suggest Low Grade Inflammation, LGI) or B (n=50) – periarticular injection (deep administration around cervical facet joints along articular column). Both interventions were performed under ultrasound guidance by the same operator. Pain intensity (Numerical Rating Scale, NRS) and disability (Neck Disability Index, NDI) were assessed at baseline (Initial Assessment, IA) and after 6- (6W), and 12-weeks (12W) post-treatment, while functional test of dynamic proprioception (Dynamic Proprioception Test, DPT) was assessed at baseline (IA) and 12-weeks (12W) post-treatment.
Results: Both groups showed significant improvement over time in NRS and NDI scores (p < 0.001), with no significant between-group differences or time × group interaction. Mean NRS decreased from 4.7 ± 2.2 to 2.1 ± 1.9, and mean NDI from 16.3 ± 7.7 to 8.3 ± 6.1 after 12 weeks. No relevant changes were observed in DPT results.
Conclusion: Fascial and periarticular ACS injections provided comparable pain and disability reduction after 12 weeks, suggesting that fascial infiltration, being less invasive, may serve as an effective therapeutic alternative for neck pain in degenerative disc disease.
Keywords: autologous conditioned serum, orthokine, cervical pain, fascial infiltration, periarticular injection, ultrasound guidance, randomized controlled trial
Introduction
Neck pain is among the most common causes of musculoskeletal dysfunction worldwide. In 2017, the age-standardized global prevalence and incidence rates of neck pain were 3551.1 and 806.6 per 100,000 population, respectively, while data from 2019 indicate that it affects approximately 27 individuals per 1000. The economic burden associated with treatment and work absenteeism due to neck pain in the United States was estimated at USD 134.5 billion in 2016.1
While specific data for degenerative cervical pain prevalence in Poland is limited, general cervical pain is common, with some studies showing high rates (eg, 36% of paramedics experience cervical pain, 18.7% of medical staff have recurrent neck pain) and estimates suggesting degenerative changes affect 12–17% of adults, increasing with age, highlighting a significant burden in Poland, especially in occupational groups like healthcare workers.2
Recognized risk factors for neck pain include female sex, poor posture during computer work, older age, low physical activity, and psychological factors such as elevated anxiety and depressive symptoms—particularly relevant during the first episode of neck pain.3
In the vast majority of cases, neck pain is classified as nonspecific (mechanical) due to the difficulty in identifying a single pain generator. Only about 10% of cases are attributable to specific pathologies such as infection, trauma, neoplastic disease, rheumatoid arthritis, or overt neural compression caused by herniation or degenerative changes.4
In the pathogenesis of nonspecific neck pain, degenerative disc disease (DDD) plays a central role, leading to a cascade of secondary alterations in the uncovertebral (Luschka) joints, facet joints, and vertebral bodies—reflecting an adaptive response to instability and abnormal load vectors.5
Pain patterns specific to facet joint syndrome have been precisely characterized through diagnostic and provocation injections.6 However, a substantial subgroup of patients presents with myofascial-type neck pain, exhibiting features that mimic both radicular and facet-related patterns. This condition may exist independently or overlap with other pain syndromes and is characterized by trigger points or areas of increased tenderness in the surrounding muscles, reduced fascial glide (related to densification), and elevated muscle tone.7,8
One of the most intriguing phenomena in cervical pain research is the lack of direct correlation between the severity of degenerative disc or joint changes observed on imaging and the intensity of pain or disability in axial neck pain. The degree of local inflammation, edema, vascular permeability, and adhesion formation appears to be key to understanding this paradox. Low-grade inflammation (LGI)—a process well recognized in metabolic, neurodegenerative, cardiovascular, and age-related disorders—is associated with the overexpression of proinflammatory cytokines (IL-1, IL-6, IL-8, TNF-α). This cytokine milieu lowers the activation threshold of nociceptors abundantly present within the cervical intervertebral discs, ligamentous and capsular tissues, and myofascial structures.9
Subsequently, this process leads to sensitization not only of the peripheral nerve endings, but also of the spinal cord and dorsal root ganglia, coupled with downregulation or exhaustion of descending opioid pain-inhibitory pathways, ultimately contributing to pain chronification.10
Evidence supporting the involvement of LGI in the development of myofascial trigger points and fascial adhesions generating neck pain comes from clinical experience with manual therapy, dry needling, and acupuncture. Mechanical release, microbleeding, or reflex-induced local cytokine modulation, applied distant from the intervertebral or facet joints, have been shown to alleviate symptoms, despite not directly influencing the structural integrity of the disc or joint itself.11
Given these mechanisms, autologous conditioned serum (ACS, Orthokine) – a biologically active preparation with potent anti-inflammatory properties achieved through competitive blockade of IL-1 receptors may represent a promising therapeutic alternative. Several studies have confirmed its analgesic efficacy in osteoarthritis, tendinopathy, enthesopathy, and even certain neuralgic syndromes.12–14
In spinal disorders, the documented applications of ACS include periarticular, perineural, epidural, and even intradiscal injections.15–18 This raises an important clinical question: could the fascial administration of ACS in the cervical region interrupt the vicious cycle of inflammation, pain, and excessive muscle tension, ultimately leading to symptom resolution within several weeks? To the best of the authors’ knowledge, no study has compared these two routes of ACS administration for the treatment of neck pain.
Fascial deformation due to mechanical overload, injury, or infection can cause pain through two mechanisms. The first is mechanical, through direct irritation of free nerve endings in the distorted network of fibers that make up the fascia and entrapment of small dorsal branches of spinal nerves, which must cross the barrier of the superficial cervical fascia to reach the skin. The second is chemical, where a localized accumulation of inflammatory cytokines (LGI) irritates free nerve endings and, in the long term, leads to sensitization of the dorsal root ganglion and the spinal cord. Changes in neck position due to decreased intervertebral disc height (dehydration) or herniated discs, with limited range of motion due to degenerative changes in the uncovertebral and facet joints, or an antalgic, protective positioning of the neck, may distort the fascial network, which can secondarily result in adhesions and entrapment, and consequently, neck pain. According to the Fascial Distortion Model (FDM), although not universally accepted, fascial adhesions in the form of trigger bands and tangled coils restrict movement, often causing local numbness, tingling, and spasms, very often mimicking the clinical picture of discogenic pain.19
Given the above, ACS administered intrafascially could have a dual analgesic effect: mechanical (elimination of adhesions by hydrodissection) and chemical (interleukin-1 receptor blocking). This prompted the authors to propose this injection method.
An additional reason for introducing this kind of injection is safety considerations for patients taking anticoagulants on a long-term basis. The risk of post-procedure bleeding after superficial fascial injection is significantly reduced.
The intervertebral joints have long been recognized as a source of cervical pain, and Bogduk’s classic work20 confirmed the precise location of the cervical medial branches, whose selective block eliminates pain originating from the facet joints.
Considering the periarticular inflammatory mechanism, it can be assumed that these branches are primarily irritated chemically, as their location lies outside the zone of dominant facet joint proliferation. Although the theory about the primary cause of DDD leading to secondary facet joints proliferative and degenerative changes is still debatable by some authors, the fact of periarticular inflammation remains unchallenged as the potent factor decreasing thresholds of nerve endings in facet capsules as well as elevating baseline discharge rates, hence the most common (and considered as standard) form of ACS administration is directly adjacent to the articular column but not intraarticularly (so practically beneath the deep cervical fascia).21,22
Previous reports indicate that chronic neck pain is often accompanied by impaired sensorimotor function of the upper limb, manifested as slower reaction times, reduced visuomotor coordination, and deficits in joint position sense. These impairments reflect disrupted sensorimotor integration, whereby the brain struggles to process sensory input to control movement effectively.23,24
Therefore, the secondary objective of this study was to introduce a functional test and determine whether the reduction of pain (measured with NRS) and disability (NDI) following ACS treatment would correspond to an improvement in objective upper-limb function, as assessed by our custom-designed Dynamic Proprioception Test (DPT). This test evaluates the error in tracing a given shape, which may be a measure of the disorganization of antagonist muscle tensions (fine tuning) related not only to the compression or swelling of the motor fibers of the spinal nerves, but also to fascial adhesions, which, according to Stecco’s theory, disturb the functioning of the centers of coordination responsible for the correct alignment of antagonist muscle vectors during any movement, especially a precise one.25
To sum up, we know that inflammation is a factor causing pain, we know that ACS has an anti-inflammatory effect, and we also know that DDD harms the intervertebral joints and fascial balance. The purpose of the study was to determine which form of ACS application (superficial and deep) is the most effective in treating pain and improving function, which would be of great value for clinical settings.
Materials and Methods
Study Design and Settings
This was a single-center, prospective, randomized, open-label clinical trial conducted at the Sutherland Medical Center (SMC) in Warsaw, Poland, between March 2023 and November 2023. The study protocol followed the principles of Good Clinical Practice (GCP) and adhered to the CONSORT 2010 guidelines for reporting randomized controlled trials.
All procedures were performed on an outpatient basis by the same experienced physician trained in musculoskeletal ultrasonography. The randomization list was prepared in advance by an independent investigator not involved in patient evaluation or treatment. All study documentation, including the protocol, informed consent forms, and anonymized patient data, is archived at the SMC research site and remains available for monitoring or audit purposes.
Ethical Considerations
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and the Good Clinical Practice (GCP) guidelines to ensure participant safety and data integrity. Ethical approval was obtained from the Bioethics Committee of Wroclaw Medical University (Wroclaw, Poland; approval no. KB-81/2022, issued on February 1, 2023). The study was prospectively registered in the ISRCTN registry under the identifier ISRCTN38950110. The unique study protocol number was SMC2023001 (submitted on February 16, 2023; registered on February 27, 2023; last revised on March 29, 2023). Before enrollment, written informed consent was obtained from all participants after providing full verbal and written explanations of the study objectives, procedures, and potential risks. All participants were covered by comprehensive medical insurance for the duration of the trial.
Study Participants
Patients with MRI-confirmed cervical DDD and neck pain were invited to participate. Inclusion criteria: adults with cervical DDD on MRI, neck pain (axial, mixed, radicular), no neurological deficits, no prior cervical trauma, and no history of systemic or neoplastic disease. Exclusion criteria: age under 18 years, systemic, post-traumatic, or neoplastic conditions, impaired communication, or lack of consent for injection procedures.
Randomization
A total of 100 patients were randomly assigned using a computer-generated list into two equal groups: Group A (n = 50): fascial infiltration – superficial administration of ACS using the hydrodissection technique, and Group B (n = 50): periarticular injection – deep administration of ACS around the cervical facet joints. All procedures were ultrasound-guided and performed by the same experienced operator to minimize variability.
Interventions
Group A: Patients received four ultrasound-guided fascial injections (hydrodissection of superficial fascia) in the cervical region at multiple sites of increased tenderness referred by the patient during palpatory assessment, without any standardization of pressure force. Approximately 0.5 mL of ACS was injected per point using a 0.4 mm (21 G) needle 4 cm long, using the US device Alpinion ECUBE 12 with linear probe 7–12 MHz. Injections were administered along the superficial cervical fascia (every three days by the same operator each time after an updated evaluation of tender points, in the sitting position of the patient (Figure 1).
 |
Figure 1 US-guided fascial injection and area of ACS hydrodissection (encircled). |
Group B: Patients received four ultrasound-guided periarticular injections along the cervical articular column, aiming at the specific level affected by DDD (reference US image was wave-like line of lateral aspect of the articular column while patient was positioned in lateral decubitus), either unilaterally (on the side of dominant pain) or bilaterally, with 4 mL of ACS administered per session beneath the deep cervical fascia using a 0.7–0.8 mm needle (21–22G) and the same US device. The same injection schedule was followed (every three days) (Figure 2).
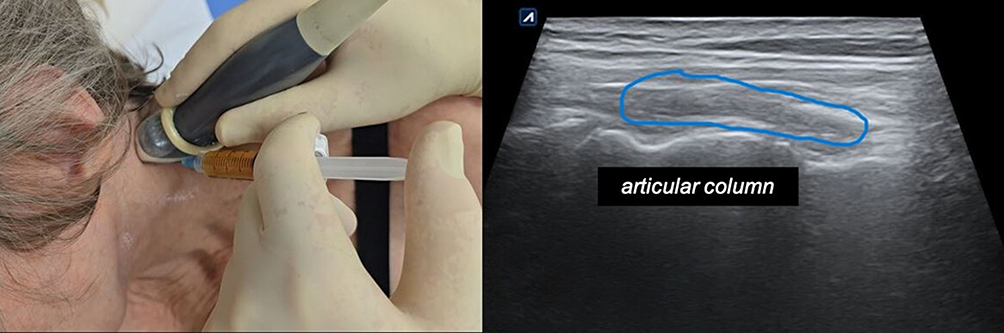 |
Figure 2 US-guided periarticular injection and area of ACS delivery (encircled). |
ACS was prepared using Orthokine EOT II syringes (Orthogen AG, Germany). Ten milliliters of venous blood were incubated in EOT II tubes at 37°C for seven hours, then centrifuged and aliquoted into sterile syringes. The serum was stored at −20°C until use. Every dose was thawed immediately before administration and injected as a whole according to group allocation (superficial or deep). No refreezing of the serum was performed.
Following each injection, patients were observed for 10 minutes at the clinic. Post-procedure recommendations included avoiding strenuous exercise, pausing ongoing rehabilitation, and refraining from heat exposure (eg, sauna, hot baths).
Assessments
Outcome measures included: (i) pain intensity assessed by the Numerical Rating Scale (NRS, 0–10),26 (ii) functional disability assessed by the Neck Disability Index (NDI, 0–50),27, and (iii) dynamic upper-limb proprioception assessed at 12 weeks using the Dynamic Proprioception Test (DPT).28 Pain intensity (NRS) and disability (NDI) were assessed at baseline (Initial Assessment, IA) and after 6 weeks (6W), and 12-weeks (12W) post-treatment, while dynamic proprioception (DPT) was assessed at baseline (IA) and 12-weeks (12W) post-treatment.
In the DPT, participants, seated in a standardized position relative to table height and screen distance, were instructed to trace the outline of a circular shape displayed on a screen of the tablet (Samsung Galaxy Tab X10) of 14″ diameter screen in a continuous, smooth motion. The software, which was designed by Ing. Piotr Murawski in 2016, for a similar purpose, automatically calculated the percentage of relative tracing error, reflecting proprioceptive performance. From among the many numerical data, only the relative error given in percentage was taken into account. The test was validated in another study performed by our clinic (Figure 3).29
 |
Figure 3 Dynamic proprioceptive test – graphics and numerical data. |
Statistical Analysis
Statistical analyses were performed using Python packages (pandas, scipy, statsmodels, pingouin, seaborn, matplotlib). Descriptive statistics were expressed as mean ± standard deviation (M ± SD), median (Me), quartiles (Q1-Q3), and range (Min-Max) for quantitative variables, and as absolute numbers and percentages (n, %) for categorical variables. Normality was assessed using the Shapiro–Wilk test. Between-group comparisons were conducted using Student’s t-test for normally distributed variables and the Mann–Whitney U-test for non-normal distributions. Categorical data were compared using the chi-square test or Fisher’s exact test (when expected cell counts < 5). Primary endpoint analyses were performed using Linear Mixed Models (LMM), including fixed effects for time, group, and time × group interaction, with a random intercept for participants. Linear mixed-effects models were selected as the primary analytical approach due to their suitability for repeated-measures data, allowing for the inclusion of fixed effects for time, treatment group, and their interaction, as well as random subject-level effects to account for within-participant correlations and missing observations. A significance level of p < 0.05 was considered statistically significant.
Results
Participants’ Characteristics
During the recruitment phase, 125 individuals responded to the public announcement posted on the clinic’s website. Of these, 20 did not meet the inclusion criteria, and 5 eligible participants declined to participate. Ultimately, 100 patients were enrolled, and 99 completed the full treatment protocol. One patient in Group B discontinued participation after the third injection due to symptom exacerbation. No other serious adverse events were observed. Mild post-procedure soreness at the injection site, transient pain and tension, or minor subcutaneous bleeding occurred frequently but did not interfere with the continuation of therapy. At the 6-week follow-up (6W), 99 participants were assessed (50 in Group A and 49 in Group B). Between the 6W and 12W assessments, contact was lost with two participants from Group A, whereas all remaining participants from Group B completed the final follow-up. Consequently, data from 97 patients (48 in Group A and 49 in Group B) were included in the final analysis (Figure 4).
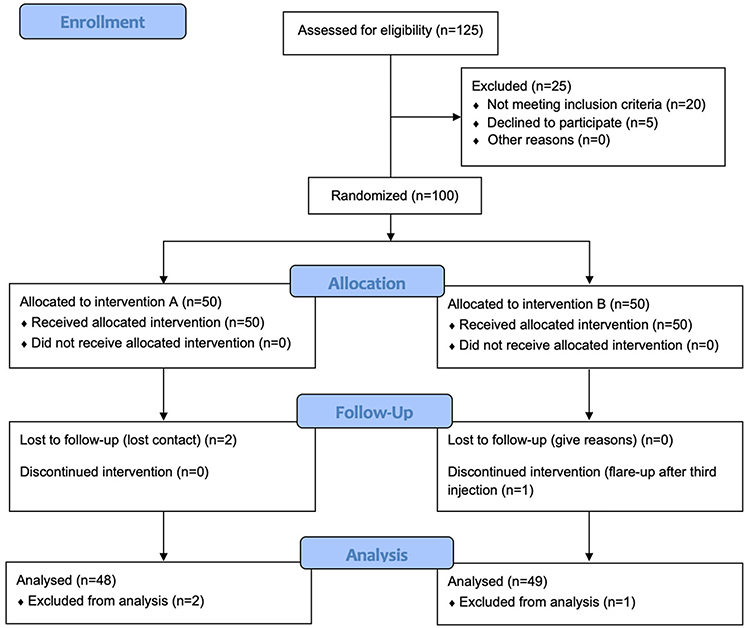 |
Figure 4 Flowchart of the study participants. |
Baseline characteristics of both groups are summarized in Table 1. There were no statistically significant differences between Group A and Group B regarding age, body weight, body mass index (BMI), or duration of symptoms (all p > 0.05).
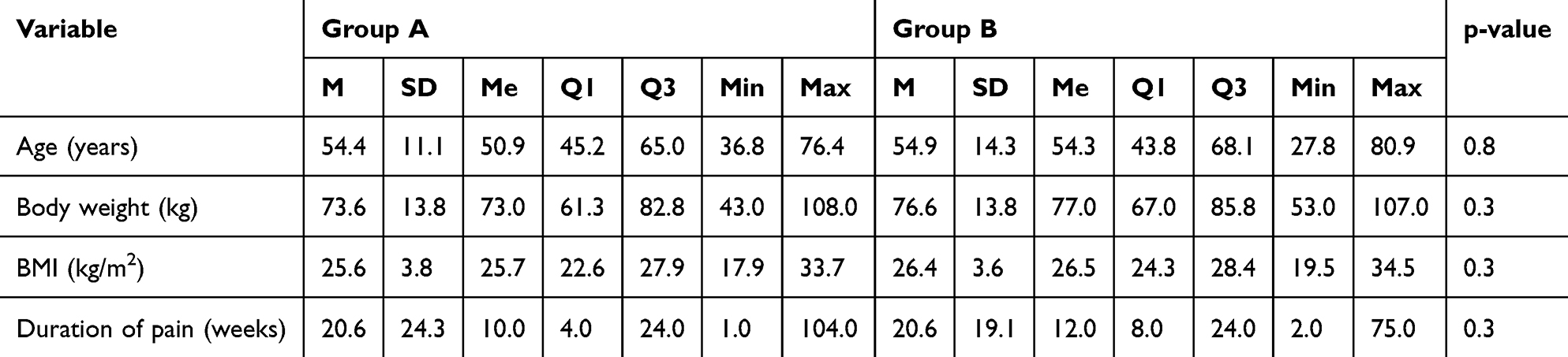 |
Table 1 Baseline Characteristics of Patients in Group A and Group B |
Qualitative Variables
The distribution of qualitative variables is presented in Table 2. The two groups were comparable with respect to sex distribution, type of disc degeneration, presence of comorbidities (diabetes, peripheral vascular disease, depression, trauma history, polyneuropathy), type of herniation, pain, disease phase, and predominant level of degeneration. All comparisons yielded non-significant differences (p > 0.05).
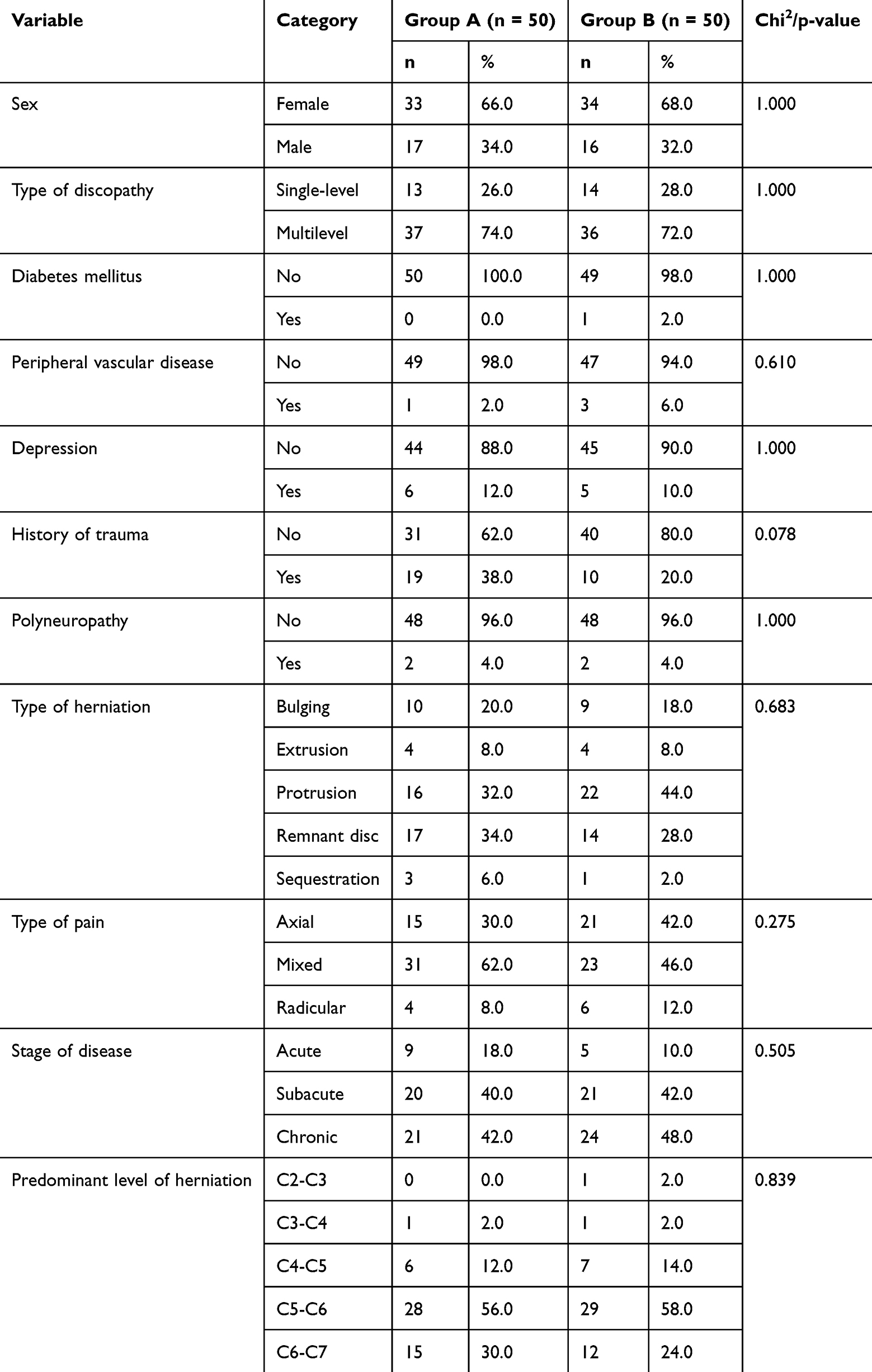 |
Table 2 Distribution of Qualitative Variables in Group A and Group B |
Pain Level
Pain intensity, as measured by the NRS, decreased significantly over time in both groups. In Group A, mean NRS decreased from 4.64 ± 2.34 at baseline to 1.92 ± 1.92 at 12 weeks, while in Group B it decreased from 4.80 ± 2.01 to 2.26 ± 2.00. Similarly, functional disability measured by the NDI improved in both groups. Mean NDI values decreased from 15.48 ± 7.44 to 8.06 ± 5.72 in Group A and from 17.16 ± 8.00 to 8.45 ± 6.43 in Group B. Both treatment methods demonstrated comparable efficacy in reducing pain and improving function over the 12-week observation period (Table 3).
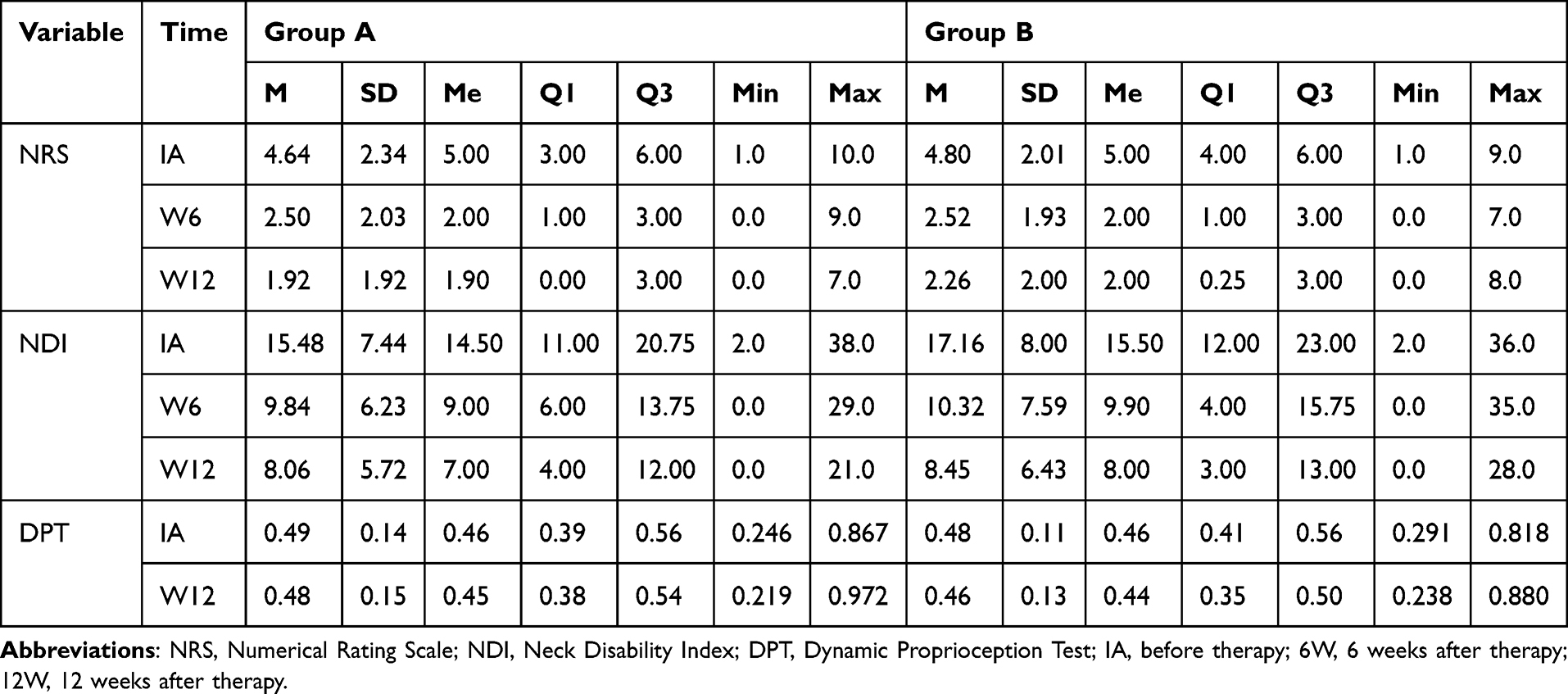 |
Table 3 Summary of Primary and Secondary Endpoint Values in Group A and Group B |
Proprioception Test
Results of the DPT remained relatively stable throughout the observation period, with no significant differences over time or between groups. Mean DPT error values changed minimally, from 0.49 ± 0.14 to 0.48 ± 0.15 in Group A, and from 0.48 ± 0.11 to 0.46 ± 0.13 in Group B (Table 3).
Linear Mixed Models
Results of the linear mixed-model analyses are presented in Table 4. For both primary endpoints (NRS and NDI), a significant main effect of time was observed (p < 0.001), indicating progressive improvement over the study period. However, no significant main effect of group or time × group interaction was detected. For the DPT, no significant effects of time or group were found, suggesting that proprioceptive parameters remained stable throughout the observation period.
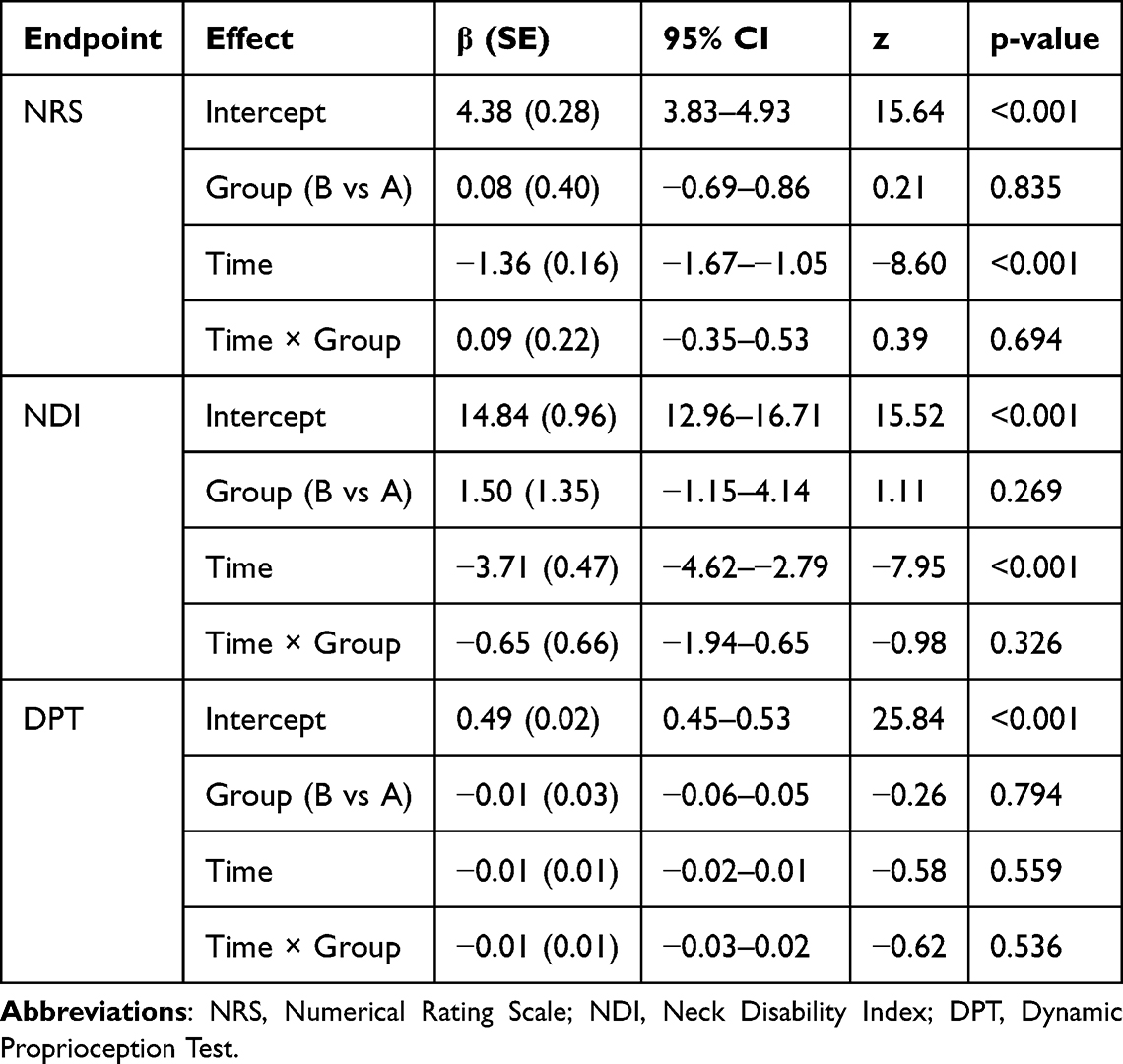 |
Table 4 Results of Linear Mixed-Model (LMM) Analyses for Primary (NRS, NDI) and Secondary (DPT) Outcomes |
In both groups, a significant main effect of time was observed (p < 0.001) (Figure 5), reflecting a gradual reduction in pain intensity across successive assessment points. No significant group effect or time × group interaction was found (p > 0.05), indicating comparable efficacy of the two therapeutic approaches.
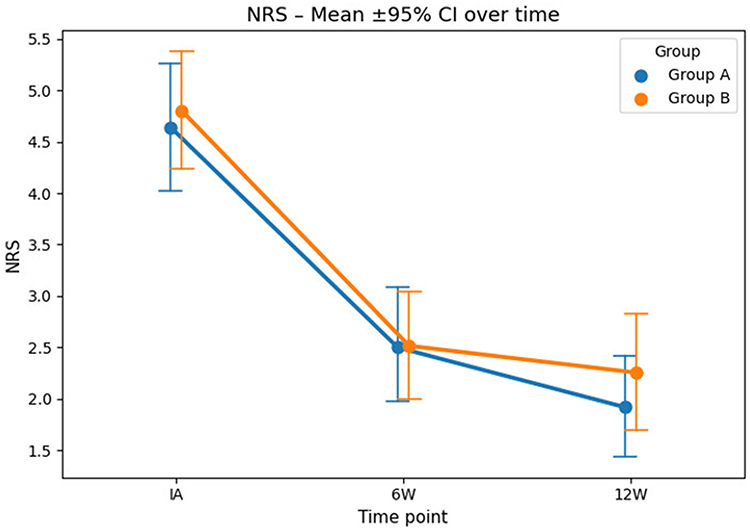 |
Figure 5 Change in pain intensity according to the Numerical Rating Scale (NRS) over the observation period: baseline (IA – before therapy), 6 weeks after therapy (6W), and 12 weeks after therapy (12W) in Group A (fascial infiltration) and Group B (periarticular injection). Error bars represent standard deviations. Both groups demonstrated a significant reduction in pain intensity over time (p < 0.001, time effect; Linear Mixed Model), with no significant differences between groups. Abbreviations: NRS, Numerical Rating Scale; IA, before therapy; 6W, 6 weeks after therapy; 12W, 12 weeks after therapy. |
Similarly, a significant time effect was demonstrated for functional improvement of the cervical spine (p < 0.001) (Figure 6). However, no significant main group effect or time × group interaction was detected (p > 0.05), suggesting equivalent effectiveness of both methods in reducing neck-related disability.
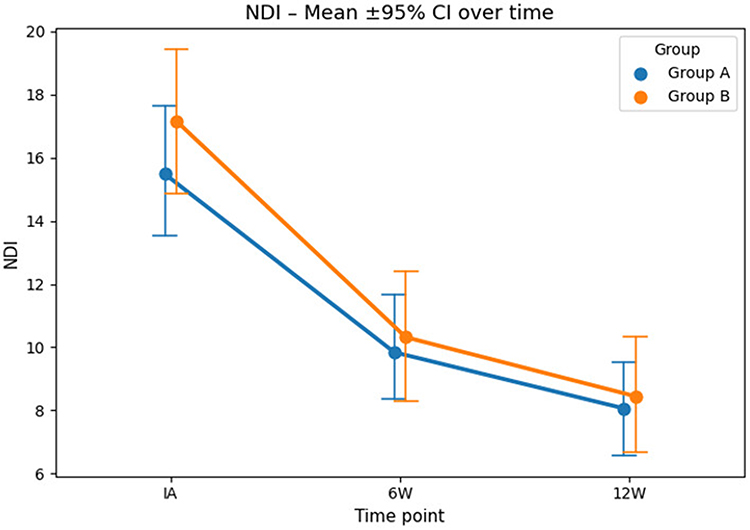 |
Figure 6 Change in the Neck Disability Index (NDI) during the observation period: baseline (IA – before therapy), 6 weeks after therapy (6W), and 12 weeks after therapy (12W) in Group A (fascial infiltration) and Group B (periarticular injection). Error bars represent standard deviations. Both groups demonstrated a significant improvement in functional status over time (p < 0.001, time effect; Linear Mixed Model), with no significant between-group differences. Abbreviations: NDI, Neck Disability Index; IA, before therapy; 6W, 6 weeks after therapy; 12W, 12 weeks after therapy. |
For the Dynamic Proprioception Test (DPT), no significant effects of time, group, or time × group interaction were identified (p > 0.05), indicating that the therapy did not substantially influence dynamic proprioceptive parameters during the observation period (Figure 7).
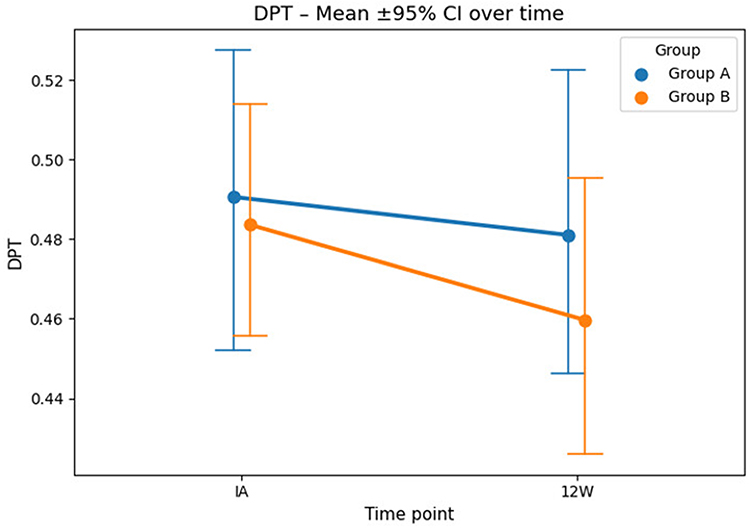 |
Figure 7 Change in the Dynamic Proprioception Test (DPT) values during the observation period: baseline (IA – before therapy) and 12 weeks after therapy (12W) in Group A (fascial infiltration) and Group B (periarticular injection). Error bars represent standard deviations. No significant changes were observed over time or between groups (p > 0.05; Linear Mixed Model), indicating that ACS administration did not significantly affect dynamic proprioceptive performance within the 12-week observation period. Abbreviations: DPT, Dynamic Proprioception Test; IA, before therapy; 6W, 6 weeks after therapy; 12W, 12 weeks after therapy. |
Discussion
There is no universally accepted standard of conservative management for cervical DDD. Treatment options depend on the stage of the condition (acute, subacute, or chronic), the presence of comorbidities, and the availability of specific therapeutic services. Conservative approaches typically include systemic pharmacotherapy, rehabilitation, manual therapy, and local injection techniques aimed at reducing inflammation and edema in structures contributing to neck pain.30
Unlike conservative mechanical interventions such as cervical traction, which primarily aim to temporarily reduce mechanical compression and improve joint spacing, ACS therapy targets the underlying inflammatory and nociceptive processes associated with DDD. While traction may provide short-term symptom relief through biomechanical decompression, it does not directly modulate LGI or biological mediators involved in chronic pain sensitization.31,32 In contrast, fascial ACS administration offers both mechanical effects through hydrodissection and sustained anti-inflammatory biological action, potentially explaining its clinically meaningful and progressive symptom improvement.33,34
Among local anti-edematous interventions, corticosteroid injections, usually combined with local anesthetics and administered periarticularly, perineurally, or epidurally under fluoroscopic or ultrasound guidance, remain the most common approach for acute pain syndromes.35 Unfortunately, corticosteroids are associated with numerous adverse effects, including elevated blood pressure, hyperglycemia, increased intraocular pressure, bone demineralization, and local skin reactions.36
ACS (Orthokine) offers an appealing alternative to corticosteroids in local anti-inflammatory and anti-edematous therapy. Its mechanism of action is based on the competitive blockade of interleukin-1 receptors (IL-1R) by naturally occurring antagonistic proteins (IL-1RA) produced by blood monocytes during several hours of incubation at 37°C in EOT II tubes containing glass beads. This process also promotes the release of beneficial anti-inflammatory cytokines (IL-4, IL-10) and growth factors (HGF, IGF, TGF-β, PDGF, FGF), which synergistically support tissue healing and regeneration, while the production of pro-inflammatory cytokines is not enhanced.13,37–39
Most published studies have evaluated the use of ACS in osteoarthritis, particularly of the knee tendinopathies, and low back pain (LBP).13 Only a few pilot trials have addressed its application in cervical spine disorders, showing comparable efficacy to platelet-rich plasma (PRP) for cervical radiculopathy and superior outcomes to physical or mechanical modalities such as traction or manual therapy, regardless of symptom duration.29
Goni et al40 demonstrated in a pilot study involving 40 patients with cervical radiculopathy (VAS = 7–10) that ACS was more effective than methylprednisolone when administered under fluoroscopic guidance. Although all participants improved and no major adverse events were reported, patients treated with ACS showed a gradual and sustained improvement over six months, whereas those receiving corticosteroids experienced symptom recurrence over time.
To date, no study has directly compared superficial (fascial) versus traditional deep (periarticular, perineural, or epidural) ACS administration. However, evidence from related approaches, such as prolotherapy using PRP or dextrose for post-traumatic instability or DDD – provided the rationale for this investigation. PRP injections, whose composition is most similar to ACS, have been shown to reduce pain and improve function with clinically significant and long-lasting effects (up to two years), while maintaining an excellent safety profile. Another fascially targeted injection method, dry needling, acts through trigger-point stimulation that elicits neuromuscular regulatory mechanisms, reducing excessive muscle tone and myofascial pain.41,42
The choice of fascial infiltration using the hydrodissection technique in the present study was motivated by two main considerations: first, to mechanically separate fascial adhesions (densification points, distortion points) that may entrap tiny nerve endings penetrating fascial mesh. Manual therapists who use fascial manipulation techniques have the same goal, but this is a purely mechanical approach, similar to traction therapies (which also lack specificity). In the case of ACS, the administration of a powerful substance with local anti-inflammatory and pro-regenerative effects plays a crucial role. The hydrodissection technique, especially under US guidance, ensures a much broader distribution of ACS across the injection field than the vertical type of injection used for trigger point infiltration, thereby enhancing diffusion into areas affected by low-grade inflammation (LGI). An additional potential benefit is fascial hydration, which may improve adaptive properties in chronic compartment-like fascial tightness syndromes.28
The observed efficacy of fascial ACS injections in pain reduction supports the hypothesis that nociceptive innervation of the fascia plays a crucial role in spinal cord sensitization and pain chronification. This may also explain the frequent lack of correlation between disc herniation size and pain severity in many patients. Similar mechanisms are suggested by findings in chronic whiplash-associated disorders, where not only joints, muscles, and ligaments but also the entire fascial system sustain microinjury.43
Further support for the concept of fascial pain generation comes from clinical experience with manual therapies, particularly Stecco’s model of fascial manipulation. The mechanical dissipation of densified fascial points during manual treatment can produce substantial and sometimes dramatic symptom relief even in chronic pain syndromes.44 Moreover, ultrasound studies by Stecco et al45 have documented morphological changes in the fascia following such interventions.
While the NRS and NDI measures in this study provided consistent and significant results, the DPT, intended to assess upper-limb functional precision before and after ACS therapy, did not reveal meaningful changes. Several factors may explain this outcome: the absence of a clear correlation between disc herniation characteristics and baseline motor precision, the relatively short follow-up duration, and methodological limitations such as variable participant engagement, fatigue, or unintentional tracing errors (especially with the non-dominant hand).
Strengths and Limitations
The main strength of this study lies in being, to the best of our knowledge, the first randomized clinical trial to evaluate the efficacy of ACS (Orthokine) administered via a fascial approach. The results confirm the clinical effectiveness of this technique and significantly expand the potential indications for its use. Fascial ACS delivery may represent a valuable therapeutic option for patients receiving long-term anticoagulant therapy, in whom deep injections carry an increased risk of bleeding. It may also be preferable for individuals with a heightened level of anxiety regarding periarticular or epidural needle procedures. The concept of fascial injections of biologically active injectables seems to integrate regenerative medicine objectives, fascial pathology, and LGI theory, which can build a bridge between laboratory and clinical settings and innovate the treatment of chronic myofascial pain. In addition, the superficial fascial administration of ACS represents a less invasive therapeutic strategy with potential safety advantages over deep periarticular or paraspinal injections. This approach may be particularly beneficial for patients receiving anticoagulant therapy or those with increased procedural anxiety, thereby expanding the accessibility of biologic treatments for cervical pain. The patient-centered nature of this method enhances its translational relevance for everyday clinical practice.
This study also has several limitations. The sample size was relatively small, and the follow-up period was limited to 12 weeks, which can be too short for the functional improvement measured by the DPT test to be relevant. There is no blinding of the caregiver or participants, so the expectation bias might contribute to outcomes (sham therapy would dramatically strengthen internal validity). The use of a limited number of assessment tools and the open-label design without blinding or a placebo control group (eg, saline injections) represent additional methodological constraints. Moreover, the precision of intrafascial ACS delivery in Group A might have varied among participants due to individual differences in fascial structure and potential sex-related anatomical variability. We are also aware that it would be beneficial in the future to standardize the hydrodissection technique in some way, taking into account the amount of serum administered, the depth of distribution, and above all, specifying the areas affected by adhesions and LGI of the fascia; perhaps the solution would be to use US with the option of elastography.
Finally, during periarticular injections in Group B, the spread of ACS around the facet column could not be fully controlled; it remains unclear what proportion of the injected volume diffused toward the perineural region versus the bony surface beneath the deepest fascial layer. This uncertainty renders the deep injection technique somewhat unpredictable in its exact therapeutic impact on radicular components of cervical pain.
Future Research Directions
Future studies should aim to validate these findings in larger, multicenter randomized trials with extended observation periods to assess the long-term durability of treatment effects and the safety profile of fascial ACS administration. Comparative studies incorporating placebo or active control arms (eg, corticosteroids, PRP, or dextrose prolotherapy) would further clarify its relative efficacy and cost-effectiveness. Advanced imaging and biomechanical analyses, such as ultrasound elastography or MRI-based fascial mapping, could help verify the accuracy of intrafascial delivery and characterize the structural or inflammatory changes induced by ACS. Moreover, incorporating in future trials biochemical assessments of inflammatory cytokines and biomarkers of tissue regeneration could provide valuable insights into anti-inflammatory and regenerative pathways mediated by ACS and provide more individualized, fascial-oriented approaches.
Conclusion
Ultrasound-guided fascial and periarticular administration of ACS both produced meaningful clinical improvement in patients with cervical DDD. The comparable outcomes between these two delivery techniques suggest that fascial infiltration may represent a less invasive yet equally effective therapeutic alternative to deeper periarticular injections. Given its favorable safety profile and procedural simplicity, the fascial approach may be particularly valuable for patients at higher risk of complications from deep injections, such as those on anticoagulant therapy or with heightened anxiety regarding peri-spinal procedures. However, neither therapy showed any significant improvement in hand motor function as measured by the DPT test after 12 weeks of observation.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Ethical Statement
The study was approved by the Bioethics Committee of Wroclaw Medical University, Poland (approval no. KB-81/2022, issued on February 1, 2023).
Acknowledgments
There were no other contributors to the article than the authors as well as there was no writing assistance regarding our paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by the external fundings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kazeminasab S, Nejadghaderi SA, Amiri P, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord. 2022;23(1):26. doi:10.1186/s12891-021-04957-4
2. Bryndal A, Glowinski S, Hebel K, Grochulska J, Grochulska A. The prevalence of neck and back pain among paramedics in Poland. J Clin Med. 2023;12(22):7060. doi:10.3390/jcm12227060
3. Kim R, Wiest C, Clark K, Cook C, Horn M. Identifying risk factors for first-episode neck pain: a systematic review. Musculoskelet Sci Pract. 2018;33:77–15. doi:10.1016/j.msksp.2017.11.007
4. Kim WD, Shin D. Physical factors associated with non-specific neck pain: correlations among pain, disability, posture, endurance, and compensatory movement. Med Sci Monit. 2024;30:e944614. doi:10.12659/MSM.944614
5. Bashkuev M, Reitmaier S, Schmidt H. Relationship between intervertebral disc and facet joint degeneration: a probabilistic finite element model study. J Biomech. 2020;102:109518. doi:10.1016/j.jbiomech.2019.109518
6. Perolat R, Kastler A, Nicot B, et al. Facet joint syndrome: from diagnosis to interventional management. Insights Imaging. 2018;9(5):773–789. doi:10.1007/s13244-018-0638-x
7. Touma J, May T, Isaacson AC. Cervical myofascial pain. In: StatPearls. StatPearls Publishing; 2025.
8. Kondrup F, Gaudreault N, Venne G. The deep fascia and its role in chronic pain and pathological conditions: a review. Clin Anat. 2022;35(5):649–659. doi:10.1002/ca.23882
9. Johnson ZI, Schoepflin ZR, Choi H, Shapiro IM, Risbud MV. Disc in flames: roles of TNF-α and IL-1β in intervertebral disc degeneration. Eur Cell Mater. 2015;30:104–116; discussion 116–117. doi:10.22203/ecm.v030a08
10. Farrell SF, de Zoete RMJ, Cabot PJ, Sterling M. Systemic inflammatory markers in neck pain: a systematic review with meta-analysis. Eur J Pain. 2020;24(9):1666–1686. doi:10.1002/ejp.1630
11. Verzella M, Affede E, Di Pietrantonio L, Cozzolino V, Cicchitti L. Tissutal and fluidic aspects in osteopathic manual therapy: a narrative review. Healthcare. 2022;10(6):1014. doi:10.3390/healthcare10061014
12. Ippolito M, Spurio G, Compagno V, et al. Autologous conditioned serum for chronic pain in patients with osteoarthritis: a feasibility observational study. Br J Pain. 2023;17(1):103–111. doi:10.1177/20494637221134169
13. Raeissadat SA, Rayegani SM, Jafarian N, Heidari M. Autologous conditioned serum applications in the treatment of musculoskeletal diseases: a narrative review. Future Sci OA. 2022;8(2):FSO776. doi:10.2144/fsoa-2021-0088
14. Aghamohammadi D, Sharifi S, Shakouri SK, Eslampour Y, Dolatkhah N. Autologous conditioned serum (Orthokine) injection for treatment of classical trigeminal neuralgia: results of a single-center case series. J Med Case Rep. 2022;16(1):183. doi:10.1186/s13256-022-03393-9
15. Becker C, Heidersdorf S, Drewlo S, de Rodriguez SZ, Krämer J, Willburger RE. Efficacy of epidural perineural injections with autologous conditioned serum for lumbar radicular compression: an investigator-initiated, prospective, double-blind, reference-controlled study. Spine. 2007;32(17):1803–1808. doi:10.1097/BRS.0b013e3181076514
16. Godek P. Use of autologous serum in treatment of lumbar radiculopathy pain. Pilot Study. Ortop Traumatol Rehabil. 2016;18(1):11–20. doi:10.5604/15093492.1198829
17. Godek P, Szczepanowska-Wolowiec B, Golicki D. Comparison of analgesic efficacy between epidural and perineural administration of autologous conditioned serum in the conservative treatment of low back pain due to lumbar degenerative disc disease: a randomized, open-label, controlled clinical trial. Brain Sci. 2023;13(5):749. doi:10.3390/brainsci13050749
18. Rajkovic CJ, Merckling ML, Lee AW, et al. Conservative management of spinal pathology with autologous conditioned serum: a systematic review of the literature. World J Orthop. 2024;15(9):870–881. doi:10.5312/wjo.v15.i9.870
19. Thalhamer C. A fundamental critique of the fascial distortion model and its application in clinical practice. J Bodyw Mov Ther. 2018;22(1):112–117. doi:10.1016/j.jbmt.2017.07.009
20. Bogduk N, MacVicar J. Osteoarthritis of zygapophysial joints as a cause of back pain and neck pain: a scoping review. Pain Med. 2024;25(9):541–552. doi:10.1093/pm/pnae036
21. Lee SH, Son DW, Lee JS, Sung SK, Lee SW, Song GS. Relationship between endplate defects, Modic change, facet joint degeneration, and disc degeneration of cervical spine. Neurospine. 2020;17(2):443–452. doi:10.14245/ns.2040076.038
22. Cavanaugh JM, Lu Y, Chen C, Kallakuri S. Pain generation in lumbar and cervical facet joints. J Bone Joint Surg Am. 2006;88(Suppl 2):63–67. doi:10.2106/JBJS.E.01411
23. Peng B, Yang L, Li Y, Liu T, Liu Y. Cervical proprioception impairment in neck pain-pathophysiology, clinical evaluation, and management: a narrative review. Pain Ther. 2021;10(1):143–164. doi:10.1007/s40122-020-00230-z
24. Cheever KM, Myrer JW, Johnson AW, Fellingham GW. Understanding the complete pathophysiology of chronic mild to moderate neck pain: implications for the inclusion of a comprehensive sensorimotor evaluation. J Back Musculoskelet Rehabil. 2017;30(5):991–997. doi:10.3233/BMR-169535
25. Menon RG, Oswald SF, Raghavan P, Regatte RR, Stecco A. T1ρ-mapping for musculoskeletal pain diagnosis: case series of variation of water bound glycosaminoglycans quantification before and after fascial Manipulation® in subjects with elbow pain. Int J Environ Res Public Health. 2020;17(3):708. doi:10.3390/ijerph17030708
26. Nugent SM, Lovejoy TI, Shull S, Dobscha SK, Morasco BJ. Associations of pain numeric rating scale scores collected during usual care with research administered patient reported pain outcomes. Pain Med. 2021;22(10):2235–2241. doi:10.1093/pm/pnab110
27. Dyrek N, Pulik Ł, Piwowarczyk A, Skała W, Grabowska-Mycko N, Łęgosz P. Cross-cultural adaptation, reliability, and validity of the polish version of the neck outcome score. Clin Pract. 2023;13(6):1352–1359. doi:10.3390/clinpract13060121
28. Godek P, Paprocka-Borowicz M, Ptaszkowski K. Comparative efficacy of ultrasound-guided cervical fascial infiltration versus periarticular administration of autologous conditioned serum (Orthokine) for neck pain: a randomized controlled trial protocol description. Med Sci Monit. 2024;30:e942044. doi:10.12659/MSM.942044
29. Godek P, Murawski P, Ruciński W, Guzek M. Biological, mechanical or physical? Conservative treatment of cervical radiculopathy. Ortop Traumatol Rehabil. 2020;22(6):409–419. doi:10.5604/01.3001.0014.6045
30. Margetis K, Dowling TJ. Cervical degenerative disc disease. In: StatPearls. StatPearls Publishing; 2025.
31. Chacko N, Gross AR, Miller J, et al. Manual therapy with exercise for neck pain. Cochrane Database Syst Rev. 2025;12(12):CD011225. doi:10.1002/14651858.CD011225.pub2
32. Romeo A, Vanti C, Boldrini V, et al. Cervical radiculopathy: effectiveness of adding traction to physical therapy-a systematic review and meta-analysis of randomized controlled trials. Phys Ther. 2018;98(4):231–242. doi:10.1093/physth/pzy001
33. Di Franco M, Bazzichi L, Casale R, Sarzi-Puttini P, Atzeni F. Pain in systemic connective tissue diseases. Best Pract Res Clin Rheumatol. 2015;29(1):53–62. doi:10.1016/j.berh.2015.05.006
34. Langevin HM. Fascia mobility, proprioception, and myofascial pain. Life. 2021;11(7):668. doi:10.3390/life11070668
35. Li BZ, Tang WH, Li Y, Zhou L, Liu MG, Bao SX. Clinical efficacy of epidural injections of local anesthetic alone or combined with steroid for neck pain: a systematic review and meta-analysis. Biomed Res Int. 2022;2022:8952220. doi:10.1155/2022/8952220
36. Yasir M, Goyal A, Sonthalia S. Corticosteroid adverse effects. In: StatPearls. StatPearls Publishing; 2025.
37. Evans CH. Novel biological approaches to the intra-articular treatment of osteoarthritis. BioDrugs. 2005;19(6):355–362. doi:10.2165/00063030-200519060-00003
38. Wehling P, Moser C, Frisbie D, et al. Autologous conditioned serum in the treatment of orthopedic diseases: the orthokine therapy. BioDrugs. 2007;21(5):323–332. doi:10.2165/00063030-200721050-00004
39. Shakouri SK, Dolati S, Santhakumar J, Thakor AS, Yarani R. Autologous conditioned serum for degenerative diseases and prospects. Growth Factors. 2021;39(1–6):59–70. doi:10.1080/08977194.2021.2012467
40. Goni VG, Singh Jhala S, Gopinathan NR, et al. Efficacy of epidural perineural injection of autologous conditioned serum in unilateral cervical radiculopathy: a pilot study. Spine. 2015;40(16):E915–921. doi:10.1097/BRS.0000000000000924
41. Steilen D, Hauser R, Woldin B, Sawyer S. Chronic neck pain: making the connection between capsular ligament laxity and cervical instability. Open Orthop J. 2014;8:326–345. doi:10.2174/1874325001408010326
42. Schol J, Tamagawa S, Volleman TNE, Ishijima M, Sakai D. A comprehensive review of cell transplantation and platelet-rich plasma therapy for the treatment of disc degeneration-related back and neck pain: a systematic evidence-based analysis. JOR Spine. 2024;7(2):e1348. doi:10.1002/jsp2.1348
43. Heneghan NR, Smith R, Rushton A. Thoracic dysfunction in whiplash-associated disorders: a systematic review and meta-analysis protocol. Syst Rev. 2016;5:26. doi:10.1186/s13643-016-0201-0
44. Picelli A, Ledro G, Turrina A, Stecco C, Santilli V, Smania N. Effects of myofascial technique in patients with subacute whiplash associated disorders: a pilot study. Eur J Phys Rehabil Med. 2011;47(4):561–568.
45. Stecco A, Meneghini A, Stern R, Stecco C, Imamura M. Ultrasonography in myofascial neck pain: randomized clinical trial for diagnosis and follow-up. Surg Radiol Anat. 2014;36(3):243–253. doi:10.1007/s00276-013-1185-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.