Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Decreased Serum Osteocalcin is an Independent Risk Factor for Metabolic Dysfunction-Associated Fatty Liver Disease in Type 2 Diabetes
Authors Wang YJ ![]() , Jin CH, Ke JF, Wang JW, Ma YL, Lu JX, Li MF, Li LX
, Jin CH, Ke JF, Wang JW, Ma YL, Lu JX, Li MF, Li LX ![]()
Received 21 September 2022
Accepted for publication 15 November 2022
Published 29 November 2022 Volume 2022:15 Pages 3717—3728
DOI https://doi.org/10.2147/DMSO.S389794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Yu-Jie Wang,1,* Chun-Hua Jin,2,* Jiang-Feng Ke,1 Jun-Wei Wang,1 Yi-Lin Ma,1 Jun-Xi Lu,1 Mei-Fang Li,3 Lian-Xi Li1
1Department of Endocrinology and Metabolism, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai Clinical Center for Diabetes, Shanghai Diabetes Institute, Shanghai Key Laboratory of Diabetes Mellitus, Shanghai Key Clinical Center for Metabolic Disease, Shanghai, People’s Republic of China; 2Department of Endocrinology and Metabolism, Shanghai Songjiang District Central Hospital, Songjiang Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (Preparatory Stage), Shanghai, People’s Republic of China; 3Department of Emergency, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mei-Fang Li, Department of Emergency, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, 600 Yishan Road, Shanghai, 200233, People’s Republic of China, Tel +86 18930170426, Email [email protected] Lian-Xi Li, Department of Endocrinology and Metabolism, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai Clinical Center for Diabetes, Shanghai Diabetes Institute, Shanghai Key Laboratory of Diabetes Mellitus, Shanghai Key Clinical Center for Metabolic Disease, 600 Yishan Road, Shanghai, 200233, People’s Republic of China, Tel +86 21 64369181x58337, Email [email protected]
Purpose: The association between serum osteocalcin (OCN) levels and metabolic dysfunction-associated fatty liver disease (MAFLD) is still controversial. Moreover, few studies have explored their relationship in type 2 diabetes mellitus (T2DM) patients so far. The present study aimed to investigate the association of serum OCN levels with MAFLD in Chinese T2DM patients.
Methods: This cross-sectional, real-world study included 1889 Chinese T2DM inpatients. MAFLD was diagnosed by abdominal ultrasonography. Participants were divided into four groups according to serum OCN quartiles, among which the clinical characteristics were compared. The association of serum OCN levels with the presence of MAFLD was also analyzed in subjects.
Results: After controlling for sex, age, and diabetes duration, the prevalence of MAFLD significantly decreased across the serum OCN quartiles (55.3%, 52.0%, 48.6%, and 42.1% for the first, second, third, and fourth quartiles, respectively, P < 0.001 for trend). A fully adjusted multiple logistic regression analysis showed that serum OCN levels were independently and negatively associated with the presence of MAFLD in T2DM patients (odds ratio, 0.832; 95% confidence interval, 0.719– 0.962; P = 0.013). Furthermore, there were significant decreases in HOMA-IR (P = 0.001 for trend) and C-reactive protein (P < 0.001 for trend) levels across the serum OCN quartiles after controlling for sex, age, and diabetes duration.
Conclusion: Serum OCN levels were independently and negatively associated with the presence of MAFLD in Chinese T2DM patients, partially due to the improvement of insulin resistance and inflammation mediated by OCN. Serum OCN may be used as a biomarker to assess the risk of MAFLD in T2DM patients.
Keywords: diabetes mellitus, type 2, metabolic dysfunction-associated fatty liver disease, osteocalcin, insulin resistance, inflammation
Introduction
Osteocalcin (OCN), regarded as a biomarker of bone formation, has been recently found to contribute to the regulation of insulin sensitivity and energy metabolism in rodents.1 However, two recent research revealed that the deficiency of OCN shows no effect on glucose metabolism in OCN-knockout mouse.2,3 Despite certain differences between murine and human OCN, some studies in humans have pointed out the negative association between serum OCN levels and metabolic diseases such as obesity, type 2 diabetes mellitus (T2DM), and metabolic syndrome.4–8 For example, Liu et al5 demonstrated that lower serum OCN levels were correlated with less favorable metabolic parameters including waist circumference (WC), triglyceride (TG), blood glucose, blood pressure and high-density lipoprotein cholesterol (HDL-C), and a higher risk of metabolic syndrome.
As a metabolic disease, metabolic dysfunction-associated fatty liver disease (MAFLD), formerly named non-alcoholic fatty liver disease (NAFLD), is a new term to describe the liver disease associated with known metabolic dysfunction,9 which has been endorsed by multiple institutions and individuals.10 There have been several studies focusing on the relationship of serum OCN levels with NAFLD in general population, some of which revealed the decreased change of serum OCN levels in NAFLD patients.11–17 However, a few studies reported that the close association between serum OCN and NAFLD was no longer significant after adjustments for metabolic factors.14–16 Therefore, the relationship between serum OCN levels and MAFLD is inconclusive so far.
Currently, it is well established that T2DM patients tend to have a significantly higher risk of MAFLD than general population.18,19 Furthermore, NAFLD and cardiovascular diseases share several metabolic risk factors including T2DM.20 A recent study revealed that NAFLD was associated with an increased risk of cardiovascular diseases, hepatocellular carcinoma, and all-cause mortality in T2DM subjects.21 Additionally, few studies have investigated the correlation between serum OCN levels and MAFLD in T2DM patients, and the findings from different studies are inconsistent. For example, Wang et al22 reported that serum OCN levels were negatively associated with advanced NAFLD status in middle-aged and elderly men and postmenopausal women with T2DM. However, another study in postmenopausal women with either T2DM or impaired glucose regulation presented a contrary result, in which a positive correlation between OCN levels and NAFLD fibrosis score was observed.23
Therefore, the aims of the present study were to explore the clinical characteristics of MAFLD and the association of serum OCN levels with MAFLD in Chinese T2DM patients in a real-world setting.
Methods
Study Design and Population
T2DM patients hospitalized in our department from January 2009 to December 2012 were enrolled consecutively in this study, and information of some patients was obtained from our previous studies.24–26 The exclusion criteria were as follows: incomplete clinical data; without data of serum OCN and abdominal ultrasonography; diseases influencing serum OCN levels such as hyperparathyroidism; and liver injury caused by drugs, viral hepatitis, and other reasons except for drinking. Finally, there were 1889 patients including 1089 men and 800 women in the present study. According to serum OCN quartiles, the patients were divided into four groups.
All studied subjects were interviewed to obtain their diabetes duration (DD), smoking and drinking habits, history of hypertension (HTN), medications including insulin or insulin analogs (IIAs), lipid-lowering drugs (LLDs), metformin, and insulin sensitizers. The definitions of HTN, smoking, and drinking were consistent with our previous studies.27,28
Medical Examinations and Laboratory Tests
Physical examination included height, weight, hip circumference (HC), WC, and blood pressure. The calculation of waist-to-hip ratio (WHR) and body mass index (BMI) was in line with our previous studies.24 Blood pressure was measured with a standard mercury sphygmomanometer. Obesity was defined as a BMI above 25 kg/m2 based on the Asia/Pacific criteria set by the World Health Organization, consistent with our previous study.29
Venous blood samples from the subjects were collected for laboratory testing after an overnight fast and 2 hours after breakfast, respectively. The measured clinical parameters included fasting plasma glucose (FPG), 2-hour postprandial plasma glucose (2h PPG), glycated hemoglobin A1c (HbA1C), fasting insulin (Fins), 2-hour postprandial insulin (2hins), fasting C-peptide (FCP), 2-hour postprandial C-peptide (2h C-P), TG, total cholesterol (TC), HDL-C, low-density lipoprotein cholesterol (LDL-C), lipoprotein(a) (Lp(a)), alanine aminotransferase (ALT), γ-glutamyltransferase (GGT), creatinine (Cr), C-reactive protein (CRP). 24-hour urinary albumin excretion (UAE) and estimated glomerular filtration rate (eGFR) were determined based on our previous method.30 The homeostasis model assessment of insulin resistance (HOMA-IR) and HOMA2-IR were calculated using corresponding formula and computer model, respectively.24,31 Additionally, serum OCN levels were determined with electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany).
Abdominal Ultrasonography
For detection of hepatic steatosis, abdominal ultrasound examination was conducted in each participant, which was in accordance with our previous reports.26,32 Based on our recent study,33 since all participants in the current study had T2DM, subjects with the evidence of liver steatosis on abdominal ultrasonography were diagnosed as MAFLD according to the definition of MAFLD.9
Statistical Analysis
Statistical analyses were performed using SPSS version 15.0 for Windows. Continuous variables were tested for normality through the Kolmogorov–Smirnov test. Data were expressed as mean ± standard deviation for normally distributed variables, and either independent sample t-test or one-way analysis of variance (ANOVA) with the least significant difference (LSD) was applied to compare the differences between different groups. Skewed data were described as medians with interquartile ranges, using nonparametric tests to compare the differences among different groups. For categorical variables, percentages and chi-squared tests were used to describe and analyze data, respectively. The association of serum OCN levels with the presence of MAFLD was assessed through binary logistic regression using four models. Statistical significance was considered when a two-sided P value was 0.05 or below.
Ethics Statement
This real-world, cross-sectional study was approved by the ethics committee of Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (Approval number: 2018-KY-018(K)). Each participant signed the written informed consent form. In addition, the study was in accordance with the Helsinki Declaration.
Results
Clinical Characteristics of the Study Subjects
The study subjects were divided into quartiles based on serum OCN levels with cutoffs of <9.78, 9.78–12.52, 12.53–16.28 and >16.28 mg/L. According to serum OCN quartiles, the comparisons of the clinical characteristics of the study subjects are shown in Table 1. The results showed that there were more females in the higher serum OCN quartile groups after controlling for age, but no significant difference in age was found among the four groups after adjustment for sex. Additionally, after adjusting for sex and age, the participants in the higher serum OCN quartile were more likely to have a lower prevalence of obesity, along with a lower percentage of the subjects with drinking habits, lower WC, WHR, BMI, and a lower rate of the use of IIAs and metformin (all P < 0.05). Interestingly, the prevalence of hypertension in the fourth quartile was significantly lower than in the other three groups (P = 0.015). In addition, as the serum OCN quartile increased, the levels of 2h C-P and HDL-C showed an increased trend, and the levels of FPG, 2h PPG, TG, ALT, γ-GT, Cr, eGFR, CRP, and UAE displayed a decreased trend (all P < 0.05). No differences were observed in DD, smoking habits, the use of LLDs and insulin sensitizers, SBP, DBP, HbA1c, Fins, 2hins, FCP, TC, LDL-C, Lp(a), and SUA.
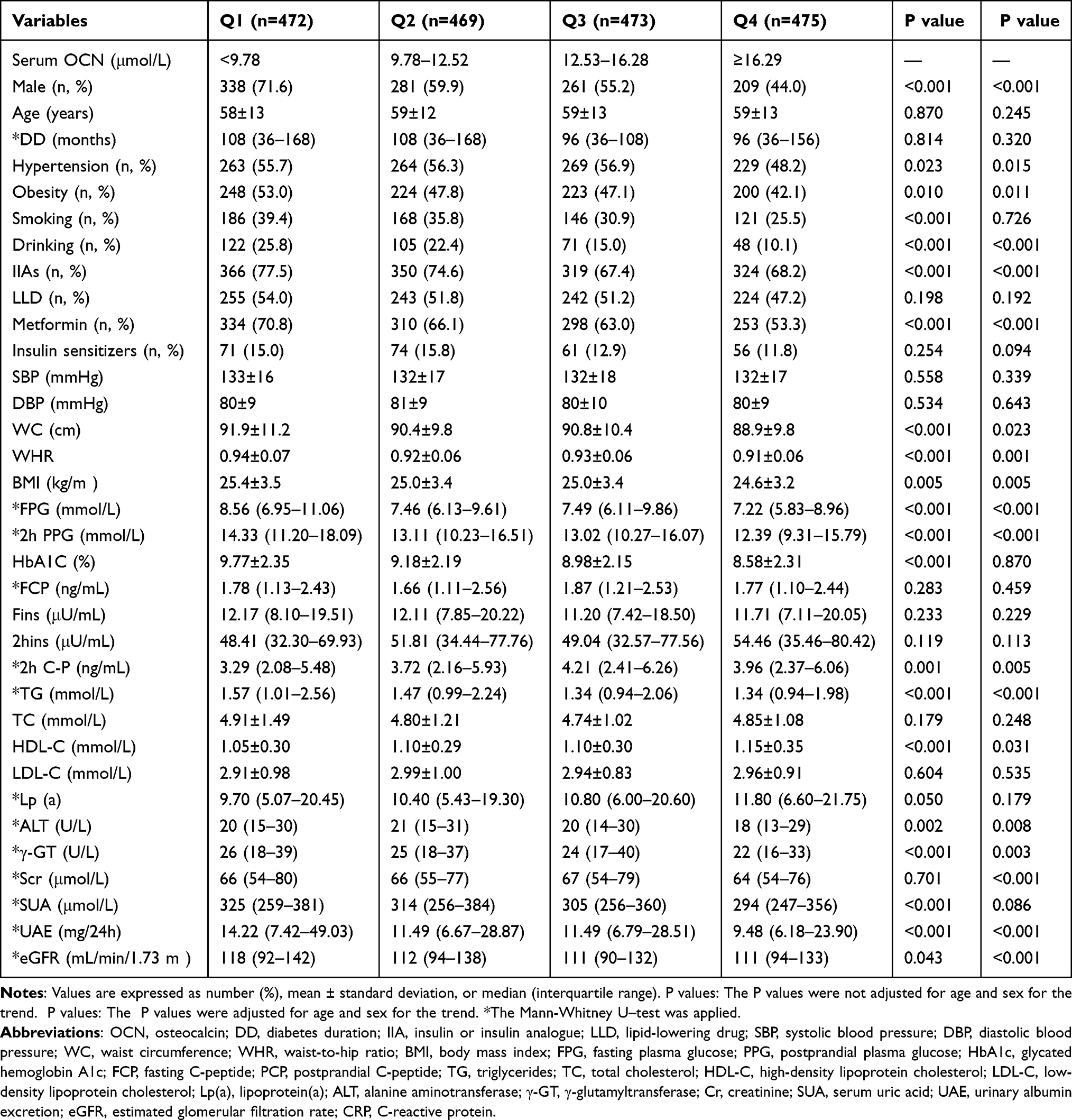 |
Table 1 Characteristics of the Subjects According to Osteocalcin Quartiles |
Comparisons of MAFLD Prevalence and Serum OCN Levels Stratified by Sex, Age, and DD
The comparisons of MAFLD prevalence and serum OCN levels stratified by sex, age, and DD in T2DM patients are presented in Figure 1. The prevalence of MAFLD in all participants was 49.5%, and with 50.9% in women significantly higher than 48.5% in men after adjusting for DD and age (P = 0.003) (Figure 1A). Furthermore, the prevalence of MAFLD markedly decreased with the increase of age (P < 0.001 for trend) and prolongation of DD in T2DM patients (all P < 0.001 for trend) (Figure 1B and C). Additionally, serum OCN levels in women were significantly higher than in men (P = 0.001) (Figure 1D). However, there was no significant difference in serum OCN levels among subjects stratified by age and DD (Figure 1E and F).
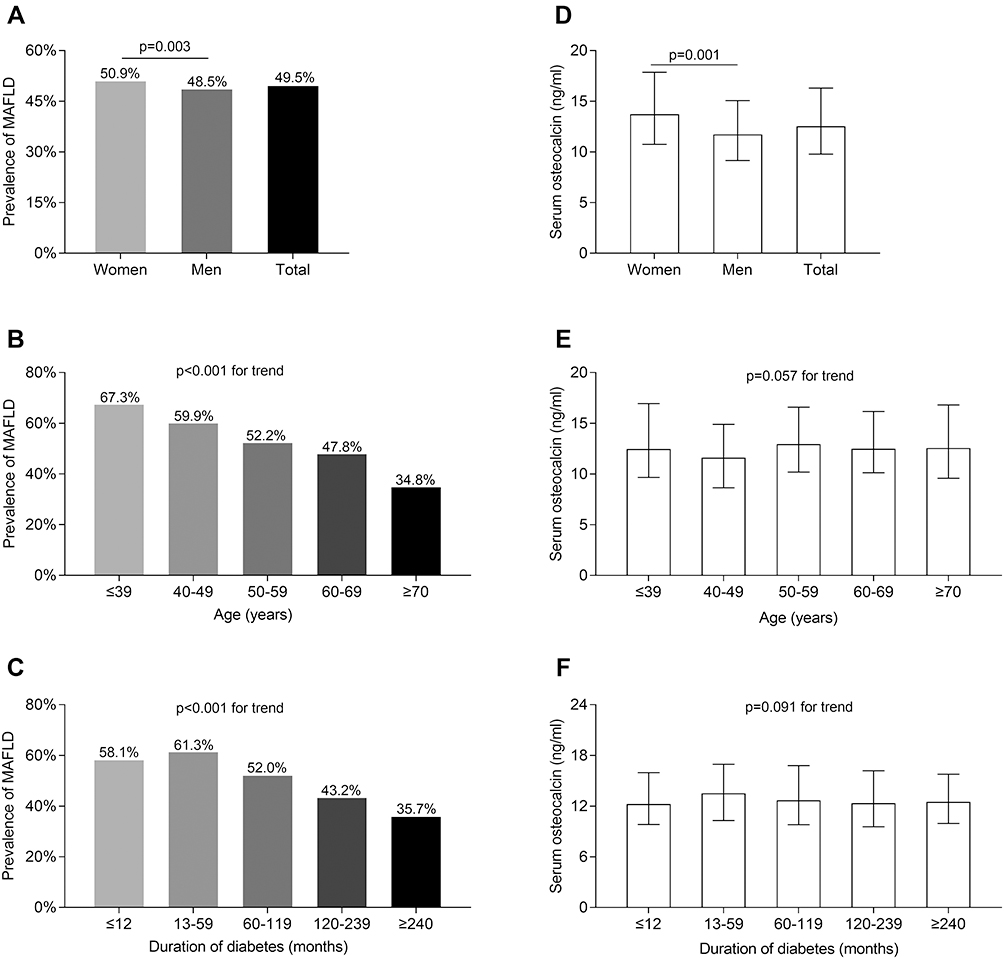 |
Figure 1 Comparisons of MAFLD prevalence and serum OCN levels stratified by sex, age, and DD. (A) Overall prevalence of MAFLD in the subjects and comparison of the MAFLD prevalence between men and women (P = 0.003). (B) Comparison of the MAFLD prevalence among the subjects stratified by age after controlling for sex and diabetes duration (DD) (P < 0.001 for trend). (C) Comparison of the MAFLD prevalence among the subjects stratified by DD after controlling for sex and age (P < 0.001 for trend). (D) Comparison of serum osteocalcin (OCN) levels between men and women (P = 0.001). (E) Comparison of serum OCN levels among the subjects stratified by age after controlling for sex and DD (P = 0.057 for trend). (F) Comparison of serum OCN levels among the subjects stratified by DD after controlling for sex and age (P = 0.091 for trend). |
Comparisons of MAFLD Prevalence
Figure 2 displays the comparisons of MAFLD prevalence among the serum OCN quartiles and the comparison of serum OCN levels between T2DM patients with and without MAFLD. After adjustment for sex, age and DD, the prevalence of MAFLD obviously reduced across the serum OCN quartiles in T2DM patients (55.3%, 52.0%, 48.6%, and 42.1% for the first, second, third, and fourth quartiles, respectively, P < 0.001 for trend) (Figure 2A). Additionally, serum OCN levels in the T2DM patients with MAFLD were significantly lower than in those without MAFLD (P < 0.001) (Figure 2B).
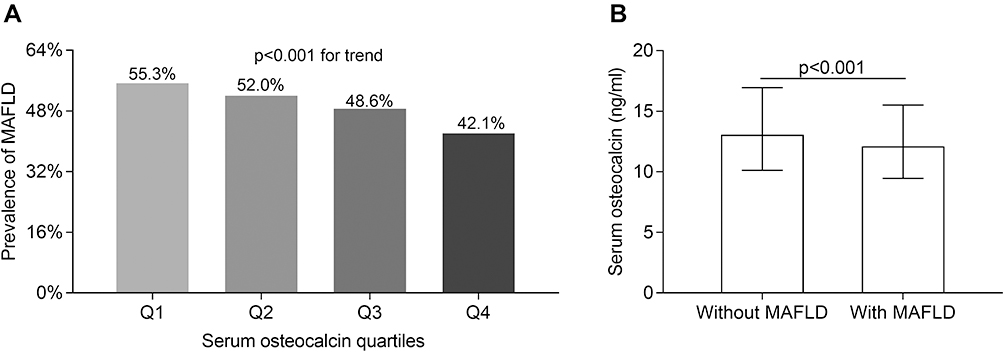 |
Figure 2 Comparisons of metabolic dysfunction-associated fatty liver disease (MAFLD) prevalence. (A) Comparisons of the prevalence of MAFLD across the serum osteocalcin (OCN) quartiles after controlling for sex, age, and diabetes duration (P < 0.001 for trend). (B) Comparisons of serum OCN levels between the type 2 diabetes mellitus patients with and without MAFLD (P < 0.001). |
Comparisons of Liver Enzymes
Figure 3 compares the liver enzymes including ALT and γ-GT among the serum OCN quartiles. As shown in Figure 3A and C, both serum ALT and γ-GT levels in the T2DM subjects with MAFLD were significantly higher than in those without MAFLD (all P < 0.001) (Figure 3A and C). Furthermore, both serum ALT (P = 0.007 for trend) and γ-GT levels (P < 0.001 for trend) were clearly decreased across the serum OCN quartiles in T2DM patients (Figure 3B and D).
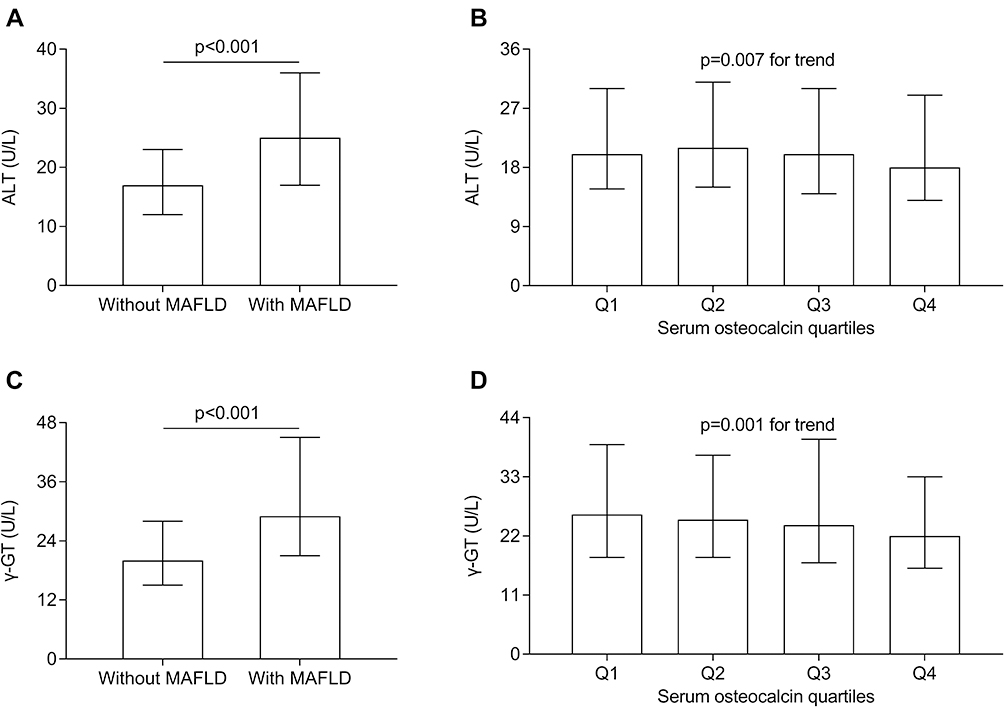 |
Figure 3 Comparisons of liver enzymes. (A) Comparisons of alanine aminotransferase (ALT) between type 2 diabetes mellitus (T2DM) patients with and without metabolic dysfunction-associated fatty liver disease (MAFLD) after controlling for age, sex, and diabetes duration (DD) (P < 0.001). (B) Comparisons of ALT across the serum osteocalcin quartiles after controlling for age, sex, and DD (P = 0.007 for trend). (C) Comparisons of γ-glutamyltransferase (γ-GT) between T2DM patients with and without MAFLD after controlling for age, sex, and DD (P < 0.001). (D) Comparisons of γ-GT across the serum OCN quartiles after controlling for age, sex, and DD (P = 0.001 for trend). |
Comparisons of Insulin Resistance and CRP
The comparisons of insulin resistance (IR) parameters including HOMA-IR and HOMA2-IR and serum CRP levels among the serum OCN quartiles are presented in Figure 4. After controlling for age, sex, and DD, the subjects with MAFLD had obviously increased values of HOMA-IR and HOMA2-IR and serum CRP levels compared with those without MAFLD (all P < 0.001) (Figure 4A, C, and E). Higher serum OCN quartiles were associated with lower IR evaluated by HOMA-IR (P = 0.001 for trend) but not HOMA2-IR (P = 0.068 for trend) (Figure 4B and D). In addition, serum CRP levels were also significantly reduced across the serum OCN quartiles in T2DM patients (P < 0.001 for trend) (Figure 4F).
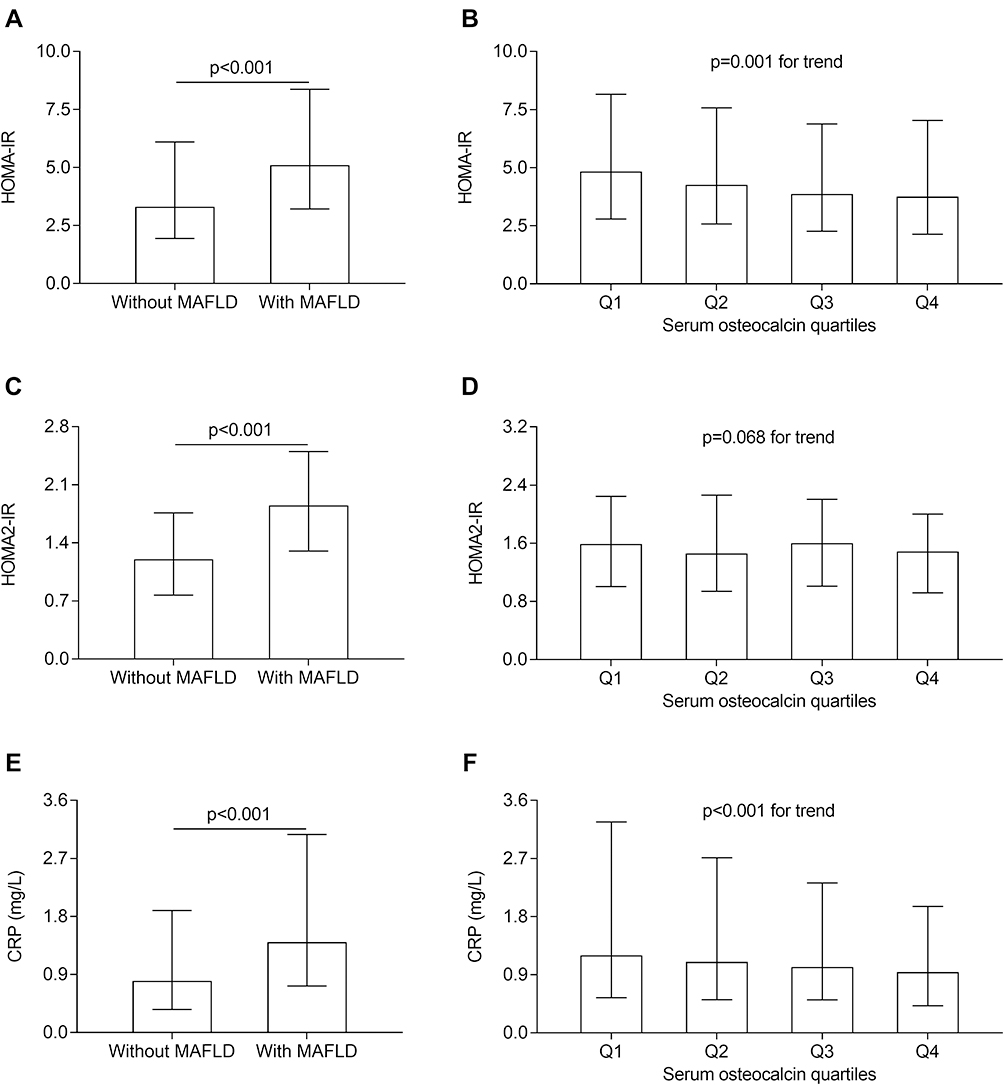 |
Figure 4 Comparisons of insulin resistance parameters and C-reactive protein (CRP). (A) Comparison of homeostasis model assessment of insulin resistance (HOMA-IR) between the type 2 diabetes mellitus (T2DM) patients with and without metabolic dysfunction-associated fatty liver disease (MAFLD) after controlling for age, sex, and diabetes duration (DD) (P < 0.001). (B) Comparisons of HOMA-IR across the serum osteocalcin (OCN) quartiles after controlling for age, sex, and DD (P = 0.001 for trend). (C) Comparison of HOMA2-IR between the T2DM patients with and without MAFLD after controlling for age, sex, and DD (P < 0.001). (D) Comparisons of HOMA2-IR across the serum OCN quartiles after controlling for age, sex, and DD (P = 0.068 for trend). (E) Comparison of serum CRP levels between the T2DM patients with and without MAFLD after controlling for age, sex, and DD (P < 0.001). (F) Comparisons of serum CRP levels across the serum OCN quartiles after controlling for age, sex, and DD (P < 0.001 for trend). |
Association of Serum OCN Levels with MAFLD
Table 2 shows the association between serum OCN levels and the presence of MAFLD in T2DM patients. After adjusting for age, sex, DD, smoking, drinking, HTN and obesity (Model 1), serum OCN levels were independently and negatively correlated with the presence of MAFLD (P < 0.001 for trend). Subsequently, after further adjustment for the use of LLDs, metformin, IIAs and insulin sensitizers (Model 2), and for SBP, DBP, WC, WHR and BMI (Model 3), and for TC, TG, LDL-C, HDL-C, Lp (a), Cr, eGFR, SUA, UAE, CRP, HbA1C, FPG, 2h PPG, Fins, 2-hins,HOMA-IR, FCP, 2h PCP and HOMA2-IR (Model 4), the correlation between serum OCN levels and the presence of MAFLD were still stable in T2DM subjects (P = 0.001, P < 0.001, P = 0.013 for trends in Models 2, 3, and 4, respectively).
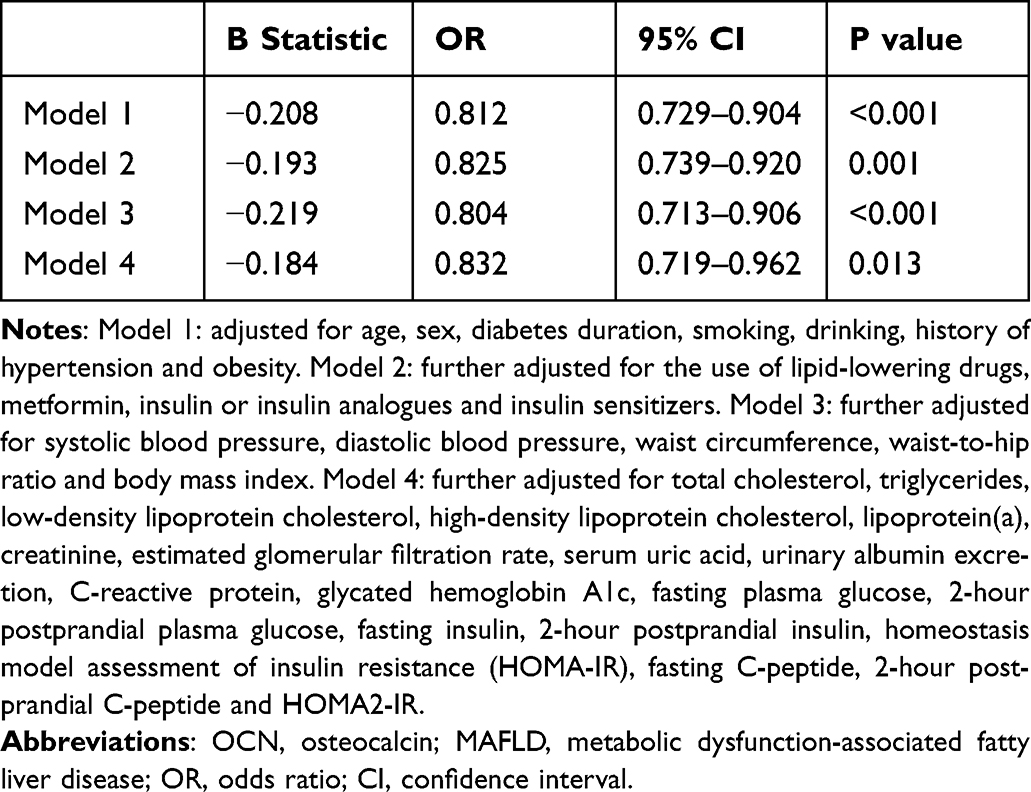 |
Table 2 The Association of Serum Osteocalcin Levels with MAFLD |
Discussion
The new nomenclature “MAFLD” was proposed recently to define the liver disease associated with metabolic dysfunction.9 Compared with the traditional term “NAFLD”, the definition of MAFLD places more emphasis on the pathophysiologic mechanisms of fatty liver, an underlying state of systemic metabolic dysfunction. Additionally, excessive alcohol consumption and other concomitant liver diseases are no longer the exclusion criteria for MAFLD.9 Investigations based on data from the United States demonstrated that MAFLD definition identified a group of patients with a higher risk of advance liver fibrosis, all-cause, cardiovascular-disease-related and other-cause mortality than NAFLD definition.34,35
Although the populations of MAFLD and NAFLD do not overlap completely, the prevalence of MAFLD and NAFLD was relatively consistent.35,36 For example, a study based on the Hong Kong census database showed that MAFLD was diagnosed in 263/1016 (25.9%) subjects, while NAFLD in 261/1016 (25.7%) subjects.36 Likewise, the present study showed that the MAFLD prevalence in T2DM subjects was 49.5%, which was close to the prevalence (52.6%) of NAFLD reported in our previous study.25 Like other studies including our recent studies,24–26,33,37,38 the current study also showed negative correlations of the MAFLD prevalence with age and DD in T2DM patients. One possible explanation for this phenomenon was that early and young T2DM patients had a greater degree of hyperinsulinemia, which led to the uptake of free fatty acids in hepatocytes.39,40
The prevalence of MAFLD in T2DM patients was significantly higher than in general population.18,19 Moreover, the co-existence of MAFLD and T2DM further increases the risk of poor prognosis, engendering severe healthy burden in those patients. For example, a retrospective cohort study found that NAFLD was associated with an increased risk of cardiovascular diseases, hepatocellular carcinoma, and all-cause mortality in T2DM subjects.21 Therefore, it is essential to predict and evaluate the risk of MAFLD to prevent and reduce the harm caused by fatty liver in T2DM patients.
OCN is the most abundant non-collagenous protein produced specifically by osteoblast and plays an important role in bone formation and turnover. Interestingly, several studies, both in vivo and in vitro, have revealed the role of OCN in ameliorating insulin resistance (IR) and regulating energy metabolism.1,41,42 Moreover, correlations between OCN and metabolic diseases such as obesity, type 2 diabetes mellitus (T2DM), and metabolic syndrome were continuously discovered in recent years.4–8 For example, Saleem et al8 demonstrated that serum OCN levels were negatively associated with measures of IR and the presence of metabolic syndrome, but positively associated with serum adiponectin levels.
More importantly, we observed a significantly negative association between serum OCN levels and MAFLD in T2DM in this study. Currently, there have been several studies exploring the relationship of OCN with NAFLD in general population,11–17 most of which supported the view that serum OCN levels were inversely associated with the presence of NAFLD. Luo et al12 presented the negative correlation of serum OCN levels with NAFLD in postmenopausal Chinese women with normal blood glucose levels. Another study in adult males also showed that compared with the subjects in the fourth serum OCN quartile, the risk of NAFLD increased by 2.25-, 2.28-, and 1.83-fold in the subjects in the first, second and third quartile, respectively, which indicated serum OCN levels were inversely related to the presence of NAFLD.13 However, some studies in general population demonstrated that the significant association between serum OCN levels and NAFLD disappeared after adjustment for metabolic parameters such as BMI and HOMA-IR.15,16 We speculated that the discrepancies may be caused by the different clinical characteristics of the study subjects, such as race and concomitant diseases.
However, similar studies focusing on T2DM population have been scarce and controversial so far. A study in a cohort of 4937 subjects by Wang et al22 reported that N-mid fragment of OCN was negatively associated with advanced NAFLD status including nonalcoholic steatohepatitis and significant fibrosis in middle-aged and elderly men and postmenopausal women with T2DM. Nonetheless, another study in postmenopausal women with T2DM and impaired glucose regulation presented a positive correlation of serum OCN levels and NAFLD fibrosis score, a non-invasive test evaluating the severity of hepatic fibrosis caused by NAFLD.23 Consistent with these studies in which negative association was observed between serum OCN and MAFLD,11–13,17 after adjusting for multiple confounding factors, especially parameters of metabolic dysfunction such as HOMA-IR and obesity, serum OCN levels were still independently and negatively correlated with the presence of MAFLD in T2DM patients in the present study. Consequently, our study provided new and confirming evidence for the inverse association of serum OCN levels with MAFLD in a relatively large number of T2DM subjects.
Serum ALT and γ-GT have been used as sensitive biomarkers for the evaluation of hepatocellular injury, which are commonly elevated in MAFLD patients.43,44 In this study, both serum ALT and γ-GT levels showed a downward trend with the increase of serum OCN quartiles. The negative correlations of serum OCN levels with ALT and γ-GT have also been reported by several previous studies.13,45–47 Also, a previous study showed that low levels of serum OCN were associated with liver fibrosis in morbidly obese patients,48 indicating that serum OCN levels might reflect not only the presence but also the severity of MAFLD. In fact, experiments in animal models have provided confirming evidence that OCN treatment alleviates hepatic steatosis by reducing hepatic expression of sterol regulatory element-binding proteins (SREBP-1) and its downstream proteins in wild-type mice fed with Western diet, which play an important role in hepatic lipogenesis and TG accumulation.11 Moreover, Gupte et al demonstrated that OCN reduced expression of proinflammatory and profibrotic genes such as Cd68, Mcp1, Spp1 and Colla2 in liver, and protected against high-fat, high-cholesterol diet-induced NASH in rodents.49
The significant adverse association between serum OCN and MAFLD in T2DM may contribute to IR and systemic chronic low-grade inflammation, which are two crucial mechanisms involved in the pathogenesis of MAFLD.50 IR leads to disorders of glucose and lipid metabolism and the ectopic accumulation of free fatty acid in hepatocytes, which play an important role in the development and progression of MAFLD.51 Another important characteristic of MAFLD was systemic low-grade chronic inflammation, including increased levels of pro-inflammatory cytokines and activation of immune cells, which contributed to the aggravation of IR and hepatocellular injury and fibrosis.50,52 Consistently, several studies have reported negative correlations of serum OCN levels with IR and systemic inflammation.4,8,53 For example, Guo et al4 demonstrated that lower serum OCN levels were associated with higher levels of IR and worse β-cell function in patients with dysglycemia. Furthermore, a cross-sectional study of 246 T2DM patients showed that serum OCN levels were significantly and negatively associated with inflammation indicators such as CRP, ferritin, basophil count and monocyte count.53 Similarly, the current study also showed increased IR and CPR levels in the T2DM subjects with MAFLD and an inverse correlation between serum OCN levels and HOMA-IR and CRP. Given that animal studies have demonstrated OCN can improve insulin sensitivity in metabolic tissues and reduce inflammation in mouse adipose and liver tissues,49,54,55 OCN may have a direct protective effect against MAFLD through ameliorating IR and chronic inflammation. Therefore, the close association of serum OCN levels with MAFLD in T2DM patients may be partially due to the alleviation of IR and inflammation mediated by OCN.
There were limitations to this study. First, this cross-sectional study could not verify the causal relationship between serum OCN and MAFLD. Second, the subjects in the study were hospitalized patients with T2DM in a single-center, which might not fully reflect characteristics of other populations such as community patients with T2DM. Third, variables not included in the analysis might affect the results. However, we controlled for as many clinical factors as possible to minimize the confounding bias. Finally, data on the severity of liver fibrosis in our study such as liver transient elastography or liver biopsy were lacking in the present study. Therefore, large-scale prospective studies are needed to further determine whether serum OCN levels can be used as an independent predictor of MAFLD in diabetic population.
Conclusion
In summary, serum OCN levels were independently and negatively correlated with the presence of MAFLD in Chinese patients with T2DM, which may partially contribute to the alleviation of IR and inflammation mediated by OCN. Serum OCN levels may be used as a potential indicator to assess the risk of MAFLD in T2DM patients, but further prospective studies are needed to obtain more convincing evidence.
Acknowledgments
We thank the support from Shanghai Municipal Key Clinical Specialty, and thank the other investigators, the staff and all the participants of the present study for their invaluable contributions.
This work was supported by grants from the National Key Research and Development Plan (2018YFC1314900, 2018YFC1314905), the National Natural Science Foundation of China (81770813 and 82070866), the Translational Medicine National Key Science and Technology Infrastructure Open Project (TMSK-2021-116), the Exploratory Clinical Research Project of Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (ynts202105), and Shanghai Municipal Key Clinical Specialty.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee NK, Sowa H, Hinoi E, et al. Endocrine regulation of energy metabolism by the skeleton. Cell. 2007;130(3):456–469. doi:10.1016/j.cell.2007.05.047
2. Diegel CR, Hann S, Ayturk UM, et al. An osteocalcin-deficient mouse strain without endocrine abnormalities. PLoS Genet. 2020;16(5):e1008361. doi:10.1371/journal.pgen.1008361
3. Moriishi T, Ozasa R, Ishimoto T, et al. Osteocalcin is necessary for the alignment of apatite crystallites, but not glucose metabolism, testosterone synthesis, or muscle mass. PLoS Genet. 2020;16(5):e1008586. doi:10.1371/journal.pgen.1008586
4. Guo H, Wang C, Jiang B, et al. Association of insulin resistance and β-cell function with bone turnover biomarkers in dysglycemia patients. Front Endocrinol. 2021;12:554604. doi:10.3389/fendo.2021.554604
5. Liu X, Yeap BB, Brock KE, et al. Associations of osteocalcin forms with metabolic syndrome and its individual components in older men: the health in men study. J Clin Endocrinol Metab. 2021;106(9):e3506–e3518. doi:10.1210/clinem/dgab358
6. Razny U, Fedak D, Kiec-Wilk B, et al. Carboxylated and undercarboxylated osteocalcin in metabolic complications of human obesity and prediabetes. Diabetes Metab Res Rev. 2017;33(3):e2862. doi:10.1002/dmrr.2862
7. Zeng H, Ge J, Xu W, et al. Type 2 diabetes is causally associated with reduced serum osteocalcin: a genomewide association and mendelian randomization study. J Bone Miner Res. 2021;36(9):1694–1707. doi:10.1002/jbmr.4330
8. Saleem U, Mosley TH, Kullo IJ. Serum osteocalcin is associated with measures of insulin resistance, adipokine levels, and the presence of metabolic syndrome. Arterioscler Thromb Vasc Biol. 2010;30(7):1474–1478. doi:10.1161/atvbaha.110.204859
9. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209. doi:10.1016/j.jhep.2020.03.039
10. Méndez-Sánchez N, Bugianesi E, Gish RG, et al. Global multi-stakeholder endorsement of the MAFLD definition. Lancet Gastroenterol Hepatol. 2022;7(5):388–390. doi:10.1016/s2468-1253(22)00062-0
11. Xia M, Rong S, Zhu X, et al. Osteocalcin and non-alcoholic fatty liver disease: lessons from two population-based cohorts and animal models. J Bone Miner Res. 2021;36(4):712–728. doi:10.1002/jbmr.4227
12. Luo YQ, Ma XJ, Hao YP, et al. Inverse relationship between serum osteocalcin levels and nonalcoholic fatty liver disease in postmenopausal Chinese women with normal blood glucose levels. Acta Pharmacol Sin. 2015;36(12):1497–1502. doi:10.1038/aps.2015.81
13. Liu JJ, Chen YY, Mo ZN, et al. Relationship between serum osteocalcin levels and non-alcoholic fatty liver disease in adult males, South China. Int J Mol Sci. 2013;14(10):19782–19791. doi:10.3390/ijms141019782
14. Deng H, Dai Y, Lu H, Li SS, Gao L, Zhu DL. Analysis of the correlation between non-alcoholic fatty liver disease and bone metabolism indicators in healthy middle-aged men. Eur Rev Med Pharmacol Sci. 2018;22(5):1457–1462. doi:10.26355/eurrev_201803_14493
15. Dou J, Ma X, Fang Q, et al. Relationship between serum osteocalcin levels and non-alcoholic fatty liver disease in Chinese men. Clin Exp Pharmacol Physiol. 2013;40(4):282–288. doi:10.1111/1440-1681.12063
16. Aller R, Castrillon JL, de Luis DA, et al. Relation of osteocalcin with insulin resistance and histopathological changes of non alcoholic fatty liver disease. Ann Hepatol. 2011;10(1):50–55. doi:10.1016/S1665-2681(19)31587-X
17. Yilmaz Y, Kurt R, Eren F, Imeryuz N. Serum osteocalcin levels in patients with nonalcoholic fatty liver disease: association with ballooning degeneration. Scand J Clin Lab Invest. 2011;71(8):631–636. doi:10.3109/00365513.2011.604427
18. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
19. Wu Y, Zheng Q, Zou B, et al. The epidemiology of NAFLD in Mainland China with analysis by adjusted gross regional domestic product: a meta-analysis. Hepatol Int. 2020;14(2):259–269. doi:10.1007/s12072-020-10023-3
20. Muzurović E, Peng CC, Belanger MJ, Sanoudou D, Mikhailidis DP, Mantzoros CS. Nonalcoholic fatty liver disease and cardiovascular disease: a review of shared cardiometabolic risk factors. Hypertension. 2022;79(7):1319–1326. doi:10.1161/hypertensionaha.122.17982
21. Wild SH, Walker JJ, Morling JR, et al. Cardiovascular disease, cancer, and mortality among people with type 2 diabetes and alcoholic or nonalcoholic fatty liver disease hospital admission. Diabetes Care. 2018;41(2):341–347. doi:10.2337/dc17-1590
22. Wang N, Wang Y, Chen X, et al. Bone turnover markers and probable advanced nonalcoholic fatty liver disease in middle-aged and elderly men and postmenopausal women with type 2 diabetes. Front Endocrinol. 2019;10:926. doi:10.3389/fendo.2019.00926
23. Zhu X, Yan H, Chang X, et al. Association between non-alcoholic fatty liver disease-associated hepatic fibrosis and bone mineral density in postmenopausal women with type 2 diabetes or impaired glucose regulation. BMJ Open Diabetes Res Care. 2020;8(1). doi:10.1136/bmjdrc-2019-000999
24. Zhang ZH, Ke JF, Lu JX, Liu Y, Wang AP, Li LX. Serum retinol-binding protein levels are associated with nonalcoholic fatty liver disease in Chinese patients with type 2 diabetes: a real-world study. Diabetes Metab J. 2021;46(1):129–139. doi:10.4093/dmj.2020.0222
25. Li TT, Wang AP, Lu JX, et al. Prevalence and clinical characteristics of non-alcoholic fatty liver disease in newly diagnosed patients with ketosis-onset diabetes. Diabetes Metab. 2018;44(5):437–443. doi:10.1016/j.diabet.2018.03.002
26. Zhao CC, Wang AP, Li LX, et al. Urine uric acid excretion is associated with nonalcoholic fatty liver disease in patients with type 2 diabetes. J Diabetes Complications. 2016;30(6):1074–1080. doi:10.1016/j.jdiacomp.2016.04.017
27. Li L, Yu H, Zhu J, et al. The combination of carotid and lower extremity ultrasonography increases the detection of atherosclerosis in type 2 diabetes patients. J Diabetes Complications. 2012;26(1):23–28. doi:10.1016/j.jdiacomp.2011.11.006
28. Li LX, Zhao CC, Ren Y, et al. Prevalence and clinical characteristics of carotid atherosclerosis in newly diagnosed patients with ketosis-onset diabetes: a cross-sectional study. Cardiovasc Diabetol. 2013;12:18. doi:10.1186/1475-2840-12-18
29. Li MF, Ren Y, Zhao CC, et al. Prevalence and clinical characteristics of lower limb atherosclerotic lesions in newly diagnosed patients with ketosis-onset diabetes: a cross-sectional study. Diabetol Metab Syndr. 2014;6:71. doi:10.1186/1758-5996-6-71
30. Li LX, Lu JX, Shuai HP, et al. Decreased urine uric acid excretion is associated with diabetic retinopathy but not with lower limb atherosclerosis in hospitalized patients with type 2 diabetes. Atherosclerosis. 2015;242(1):13–18. doi:10.1016/j.atherosclerosis.2015.06.051
31. Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care. 2004;27(6):1487–1495. doi:10.2337/diacare.27.6.1487
32. Hou XH, Zhu YX, Lu HJ, et al. Non-alcoholic fatty liver disease’s prevalence and impact on alanine aminotransferase associated with metabolic syndrome in the Chinese. J Gastroenterol Hepatol. 2011;26(4):722–730. doi:10.1111/j.1440-1746.2010.06509.x
33. Wang JW, Jin CH, Ke JF, et al. Serum iron is closely associated with metabolic dysfunction-associated fatty liver disease in type 2 diabetes: a real-world study. Front Endocrinol. 2022;13:942412. doi:10.3389/fendo.2022.942412
34. Nguyen VH, Le MH, Cheung RC, Nguyen MH. Differential clinical characteristics and mortality outcomes in persons with NAFLD and/or MAFLD. Clin Gastroenterol Hepatol. 2021;19(10):2172–2181.e6. doi:10.1016/j.cgh.2021.05.029
35. Lin S, Huang J, Wang M, et al. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int. 2020;40(9):2082–2089. doi:10.1111/liv.14548
36. Wong VW, Wong GL, Woo J, et al. Impact of the new definition of metabolic associated fatty liver disease on the epidemiology of the disease. Clin Gastroenterol Hepatol. 2021;19(10):2161–2171.e5. doi:10.1016/j.cgh.2020.10.046
37. Han E, Kim MK, Jang BK, Kim HS. Albuminuria is associated with steatosis burden in patients with type 2 diabetes mellitus and nonalcoholic fatty liver disease. Diabetes Metab J. 2021;45(5):698–707. doi:10.4093/dmj.2020.0118
38. Shi R, Lin C, Hong Y, et al. Free triiodothyronine is independently associated with nonalcoholic fatty liver disease in hospitalized type 2 diabetes mellitus patients. Biomed Res Int. 2021;2021:8868339. doi:10.1155/2021/8868339
39. Williamson RM, Price JF, Glancy S, et al. Prevalence of and risk factors for hepatic steatosis and nonalcoholic Fatty liver disease in people with type 2 diabetes: the Edinburgh type 2 diabetes study. Diabetes Care. 2011;34(5):1139–1144. doi:10.2337/dc10-2229
40. Lascar N, Brown J, Pattison H, Barnett AH, Bailey CJ, Bellary S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol. 2018;6(1):69–80. doi:10.1016/s2213-8587(17)30186-9
41. Mukai S, Mizokami A, Otani T, et al. Adipocyte-specific GPRC6A ablation promotes diet-induced obesity by inhibiting lipolysis. J Biol Chem. 2021;296:100274. doi:10.1016/j.jbc.2021.100274
42. Bilotta FL, Arcidiacono B, Messineo S, et al. Insulin and osteocalcin: further evidence for a mutual cross-talk. Endocrine. 2018;59(3):622–632. doi:10.1007/s12020-017-1396-0
43. Newton KP, Lavine JE, Wilson L, et al. Alanine aminotransferase and gamma-glutamyl transpeptidase predict histologic improvement in pediatric nonalcoholic steatohepatitis. Hepatology. 2021;73(3):937–951. doi:10.1002/hep.31317
44. Roberts SK, Majeed A, Glenister K, et al. Prevalence of non-alcoholic fatty liver disease in regional Victoria: a prospective population-based study. Med J Aust. 2021;215(2):77–82. doi:10.5694/mja2.51096
45. Amin S, El Amrousy D, Elrifaey S, Gamal R, Hodeib H. Serum osteocalcin levels in children with nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr. 2018;66(1):117–121. doi:10.1097/mpg.0000000000001768
46. Sinn DH, Gwak GY, Rhee SY, et al. Association between serum osteocalcin levels and non-alcoholic fatty liver disease in women. Digestion. 2015;91(2):150–157. doi:10.1159/000369789
47. El Amrousy D, El-Afify D. Osteocalcin and osteoprotegerin levels and their relationship with adipokines and proinflammatory cytokines in children with nonalcoholic fatty liver disease. Cytokine. 2020;135:155215. doi:10.1016/j.cyto.2020.155215
48. Luger M, Kruschitz R, Kienbacher C, et al. Prevalence of liver fibrosis and its association with non-invasive fibrosis and metabolic markers in morbidly obese patients with vitamin D deficiency. Obes Surg. 2016;26(10):2425–2432. doi:10.1007/s11695-016-2123-2
49. Gupte AA, Sabek OM, Fraga D, et al. Osteocalcin protects against nonalcoholic steatohepatitis in a mouse model of metabolic syndrome. Endocrinology. 2014;155(12):4697–4705. doi:10.1210/en.2014-1430
50. Lim S, Kim JW, Targher G. Links between metabolic syndrome and metabolic dysfunction-associated fatty liver disease. Trends Endocrinol Metab. 2021;32(7):500–514. doi:10.1016/j.tem.2021.04.008
51. Sakurai Y, Kubota N, Yamauchi T, Kadowaki T. Role of insulin resistance in MAFLD. Int J Mol Sci. 2021;22(8):4156. doi:10.3390/ijms22084156
52. Torre P, Motta BM, Sciorio R, Masarone M, Persico M. Inflammation and fibrogenesis in MAFLD: role of the hepatic immune system. Front Med. 2021;8:781567. doi:10.3389/fmed.2021.781567
53. Kanazawa I, Tanaka S, Sugimoto T. The association between osteocalcin and chronic inflammation in patients with type 2 diabetes mellitus. Calcif Tissue Int. 2018;103(6):599–605. doi:10.1007/s00223-018-0460-y
54. Mao H, Li L, Fan Q, et al. Endothelium-specific depletion of LRP1 improves glucose homeostasis through inducing osteocalcin. Nat Commun. 2021;12(1):5296. doi:10.1038/s41467-021-25673-6
55. Guedes JAC, Esteves JV, Morais MR, Zorn TM, Furuya DT. Osteocalcin improves insulin resistance and inflammation in obese mice: participation of white adipose tissue and bone. Bone. 2018;115:68–82. doi:10.1016/j.bone.2017.11.020
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Platelet-Activating Factor Promotes the Development of Non-Alcoholic Fatty Liver Disease
Yin H, Shi A, Wu J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2003-2030
Published Date: 8 July 2022
Prevalence and Pattern of Dyslipidemia and Its Associated Factors Among Patients with Type 2 Diabetes Mellitus in Jordan: A Cross-Sectional Study
Al Quran TM, Bataineh ZA, Al-Mistarehi AH, Zein Alaabdin AM, Allan H, Al Qura'an A, Weshah SM, Alanazi AA, Khader YS
International Journal of General Medicine 2022, 15:7669-7683
Published Date: 4 October 2022
The Association Between Sarcopenia and Diabetes: From Pathophysiology Mechanism to Therapeutic Strategy
Chen H, Huang X, Dong M, Wen S, Zhou L, Yuan X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1541-1554
Published Date: 30 May 2023
Diabetes Distress and Illness Perceptions in Tunisian Type 2 Diabetes Patients
Masmoudi R, Hadj Kacem F, Bouattour M, Guermazi F, Sellami R, Feki I, Mnif M, Masmoudi J, Baati I, Abid M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3547-3556
Published Date: 6 November 2023
The Mechanism of Pyroptosis and Its Application Prospect in Diabetic Wound Healing
Al Mamun A, Shao C, Geng P, Wang S, Xiao J
Journal of Inflammation Research 2024, 17:1481-1501
Published Date: 6 March 2024