")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Decreased Intracellular to Total Body Water Ratio and Depressive Symptoms in Patients with Maintenance Hemodialysis
Authors Tian M, Qian Z, Long Y, Yu F, Yuan J, Zha Y
Received 14 September 2023
Accepted for publication 11 October 2023
Published 26 October 2023 Volume 2023:16 Pages 4367—4376
DOI https://doi.org/10.2147/PRBM.S436574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Maolu Tian,1– 3 Zuping Qian,4 Yanjun Long,1,2 Fangfang Yu,1 Jing Yuan,1 Yan Zha1,2
1Department of Nephrology, Guizhou Provincial People’s Hospital, Guiyang, Guizhou, People’s Republic of China; 2NHC Key Laboratory of Pulmonary Immunological Disease, Guizhou Provincial People’s Hospital, Guiyang, Guizhou, People’s Republic of China; 3Medical College, Guizhou University, Guiyang, Guizhou, People’s Republic of China; 4Clinical Medical College, Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China
Correspondence: Yan Zha, Department of Nephrology, Guizhou Provincial People’s Hospital, 83 Zhongshan Road, Nanming District, Guiyang, Guizhou, 550002, People’s Republic of China, Email [email protected]
Objective: Depression is a common psychiatric disorder and related to poor outcomes in patients undergoing maintenance hemodialysis (MHD). Previous studies have reported some associations between sarcopenia and depressive symptoms. Recently, intracellular water (ICW) and total body water (TBW) have been found to reflect muscle function and muscle mass. ICW/TBW ratio is a marker of sarcopenia that is simple to assess. However, the relationship between ICW/TBW ratio and depression has not been explored in MHD patients.
Methods: In our cross-sectional and multi-center study, 3300 adult MHD patients were included from June 1, 2021, to August 30, 2021. Depressive symptoms were evaluated using the Beck Depression Inventory-II (BDI-II). TBW and ICW were measured by Body Composition Monitor (BCM). Multivariable logistic regression, stratified analyses, and interactive analyses were conducted to assess the relationship between ICW/TBW ratio and depression.
Results: About 16.5% of the 3300 MHD patients were found to have depressive symptoms. The prevalence of depression increased with decreasing quartiles of ICW/TBW ratios, and decreased ICW/TBW ratio was independently associated with depression after adjusting for potential confounders. Patients in Quartile 1 of ICW/TBW ratios were more likely to have depressive symptoms (odds ratio 1.55, 95% confidence interval 1.07– 2.22; p=0.002) than those in Quartile 4. History of diabetes and education status had interactive roles in the relationship between depression and ICW/TBW ratios (p < 0.05). The association of ICW/TBW ratios and depression existed in patients of both genders and different education levels, but only in non-diabetic patients.
Conclusion: In MHD patients, the decreased ratio of ICW/TBW was independently related to high depression rates.
Keywords: depression, hemodialysis, intracellular water, total body water
Introduction
Psycho-nephrology, which is mainly caused by kidney damages, existed commonly in patients with chronic kidney disease (CKD) and maintenance hemodialysis (MHD).1 Depressive symptoms are serious psychiatric disorders in MHD patients that cause bad patient outcomes. According to a guideline recommended for dialysis patients, the psychological status of patients, especially the presence of depressive symptoms, should be evaluated at least once every 2 years.2 Compared with the general population, patients with every CKD stage have a much higher prevalence of depression,3,4 and the prevalence is estimated between 13.1% and 76.3% for patients on dialysis.5 Different psychometric scales, different diagnostic threshold values, and different populations might explain this wide range of depression rates.
In the CKD population, depressive symptoms were reported to be related to more hospitalization events, faster deterioration of renal function, and worse quality of life.6–11 In 2019, a study from Taiwan found that dialysis patients who were previously diagnosed with depression had higher risks of both severe and fatal infections.12 Many researchers also reported a significant relationship between depressive symptoms and death in patients with ESRD.11,13–16 Due to its adverse outcomes and the difficulty of drug treatment only, depression needs to be carefully observed and its risk factors should be identified. Early detection of patients with high risk of depression and intervention targeting risk factors will help to prevent this mental disease. Early detection of patients at high risk of depression and intervention measures targeting risk factors will help prevent this psychological disorder.
A systematic review showed that sarcopenia is related to depression in the general population.17 Another cross-sectional study also reported a significant association between this psychological disorder and sarcopenia in elderly HD patients.18 Furthermore, a recent report suggested that depression could predict one-year sarcopenia in patients with end-stage renal disease (ESRD), though sarcopenia was defined by a simple scale in this study.19 It is well known that sarcopenia is represented as weakened muscle strength and reduced muscle mass. Intracellular water (ICW), a marker of cell hydration, was reported to reflect muscle mass and function in both elderly individuals and athletes.20–23 A proposed explanation for the relationship between muscle quality and ICW is the cell swelling theory,24,25 which has in vivo evidence suggesting that cellular swelling stimulates anabolism and glycogen synthesis, whereas ICW depletion promotes catabolic effect and protein degradation. In clinical practice, lower ICW was found to be related to increased risk of memory impairment, frailty, and reduced psychomotor skills.20,26,27
In MHD patients, the water balance in their bodies is obviously disordered due to the complete loss of renal function, which is characterized by a significant decrease in ICW and its proportion in total cell water (TBW). Therefore, the study aims to assess if ICW/TBW ratio in an MHD population is associated with depression, independently of other confounding factors.
Methods
Patients
From June 1, 2021, to August 30, 2012, we conducted a cross-sectional and multicenter study in 20 dialysis centers of tertiary hospitals. Adult patients who received HD for at least 3 months were recruited to this investigation. If participants met one or more criteria, they were excluded: (a) patients with any extremity amputation or those with the implanted stent, cardioverter-defibrillator, or pacemaker; (b) patients with neurological and psychiatric disorders diagnosed prior to beginning dialysis therapy and patients with long-term drug abuse; (c) patients with language incompatibility, visual or auditory disability that affected the accuracy of the questionnaire evaluation; (d) patients who received hospitalization because of severe infection, congestive heart failure, gastrointestinal bleeding, and other reasons at the time of evaluation; (e) individuals with malignant tumor; (f) unwillingness to participate. 3300 HD patients were eventually included in this study.
Body Water and Lean Tissue Mass Measurements
ICW, ECW, total body water (TBW), and lean tissue mass (LTM) were measured approximately 30 min before the HD session using Body Composition Monitor (BCM, Fresenius Medical Care, Bad Homburg, Germany), a portable whole-body bioimpedance spectroscopy device. The accuracy of this device in measuring cellular waters has been proven to be satisfactory.28 Patients were placed in a supine position, with their arms parallel to their trunks. Two disposable electrodes were placed on the dorsal surface of the patient’s hand and two on the foot contralateral to the vascular access. TBW, ICW, ECW, and LTM were extracted from the measuring instrument.
Assessment of Depression
Depression was evaluated with the Beck Depression Inventory II (BDI-II), which has been widely verified for depression screening in CKD patients.29–31 BDI-II is a 21-item self-report scale and includes somatic, cognitive, and affective observed items. Each item of BDI-II scores on a scale of 0 to 3 and a total score ranges from 0 to 63 with higher scores suggesting more severe symptoms of depression. According to the literature, BDI-II scores greater than or equal to 11 were used to define depression.32 Those with scores of less than 11 were classified as not having depression. Throughout the study, this depression scale was assessed by professionally trained and same medical staff.
Other Data Collection
This study also included other variables such as sociodemographic and disease characteristics, lifestyle behaviors, and laboratory data. As described in our previous study,33 these variables were acquired from a standardized questionnaire, dialysis run sheets, or electronic medical record system. More than 9 years of schooling education was classified as a high school level. In this study, a history of cardiovascular disease (CVD) was defined as congestive heart failure, arrhythmia, coronary artery disease, and stroke that required hospitalization in the past. Daily urine volume greater than 200mL was considered to have residual renal function.
Statistical Analysis
Categorical data were expressed as numbers and percentages. Continuous data with a skewed distribution were expressed as the medians and interquartile ranges. The differences between non-depressed and depressed groups were compared by the Chi-square tests or Mann–Whitney U-test. We further split patients into four groups of Quartile 1, Quartile 2, Quartile 3, and Quartile 4 according to their ICW/TBW ratios. Chi-square tests or Kruskal–Wallis tests were applied to compare the characteristics of the above 4 groups. Odds ratios (ORs) and 95% confidence intervals (CIs) for the association of ICW/TBW ratios with depressive symptoms were calculated by multivariable logistic regression. In multivariate logistic regression models, covariates included were those whose p value was less than 0.05 in univariate logistic regression analysis. Prior to logistic regression, the collinearity between covariates was also checked. A subgroup analysis was conducted to determine the stability of the original results. The grouping variables of the subgroup analysis included sex (male or female), education level (≤9 or >9 years of schooling education), and the presence of diabetes (yes or no). All analyses were conducted using R software version 4.0.1 and SPSS version 26.0. Statistical significance was determined at p < 0.05.
Results
Comparison of Characteristics Between Non-Depressed and Depressed Groups
In our final analysis, data on 3300 patients were used. Table 1 depicts the clinical and sociodemographic characteristics of all participants, non-depressed, and depressed patients. According to the BDI-II scoring criteria used in this study, 543 (16.5%) participants were judged to have depression. Compared to non-depressed participants, depressed patients had a higher proportion of diabetes, a history of CVD, and females; lower educational level and older age; higher BDI scores; lower diastolic blood pressure (DBP), albumin, and hemoglobin; lower LTM, ICW, TBW, and ICW/TBW ratio. Patients in the depressed group also worked less and needed more dialysis companionship (all p < 0.05). Other variables such as C-reactive protein (CRP), hemodiafiltration (HDF) treatment, hemoperfusion (HP) treatment, residual renal function, dialysis vintage, and body mass index (BMI) were not different in the two groups (p>0.05).
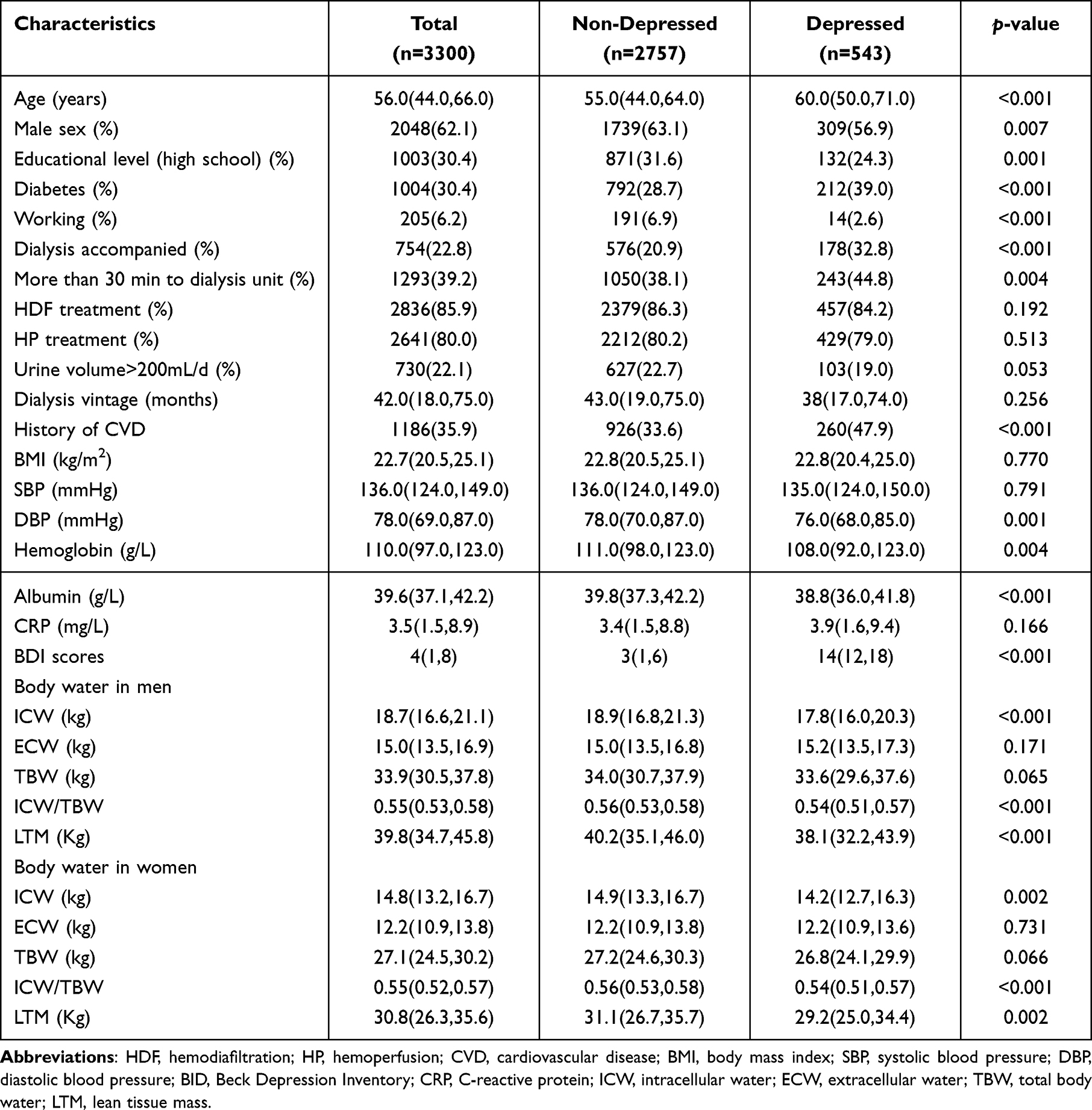 |
Table 1 Characteristics of the Patients in Depressed and Non-Depressed Groups |
Characteristics Comparison of Patients Grouped by ICW/TBW Ratio Quartiles
As shown in Table 2, the prevalence of depression increased with decreasing quartiles of ICW/TBW ratio. The depression rates of patients with Quartile 4, Quartile 3, Quartile 2, and Quartile 1 were, respectively, 11.9%, 12.2%, 16.9%, and 26.4% (p<0.001). Patients in the lower ICW/TBW ratio group had older age, more histories of diabetes and CVD. Statistically decreased trends were also observed in LTM, albumin, hemoglobin, serum creatinine, serum uric acid, and DBP with decreasing quartiles of the ICW/TBW ratio. Other variables such as HDF treatment, HP treatment, residual renal function, dialysis vintage, BMI, and CRP were similar across groups of ICW/TBW ratio quartiles (p>0.05).
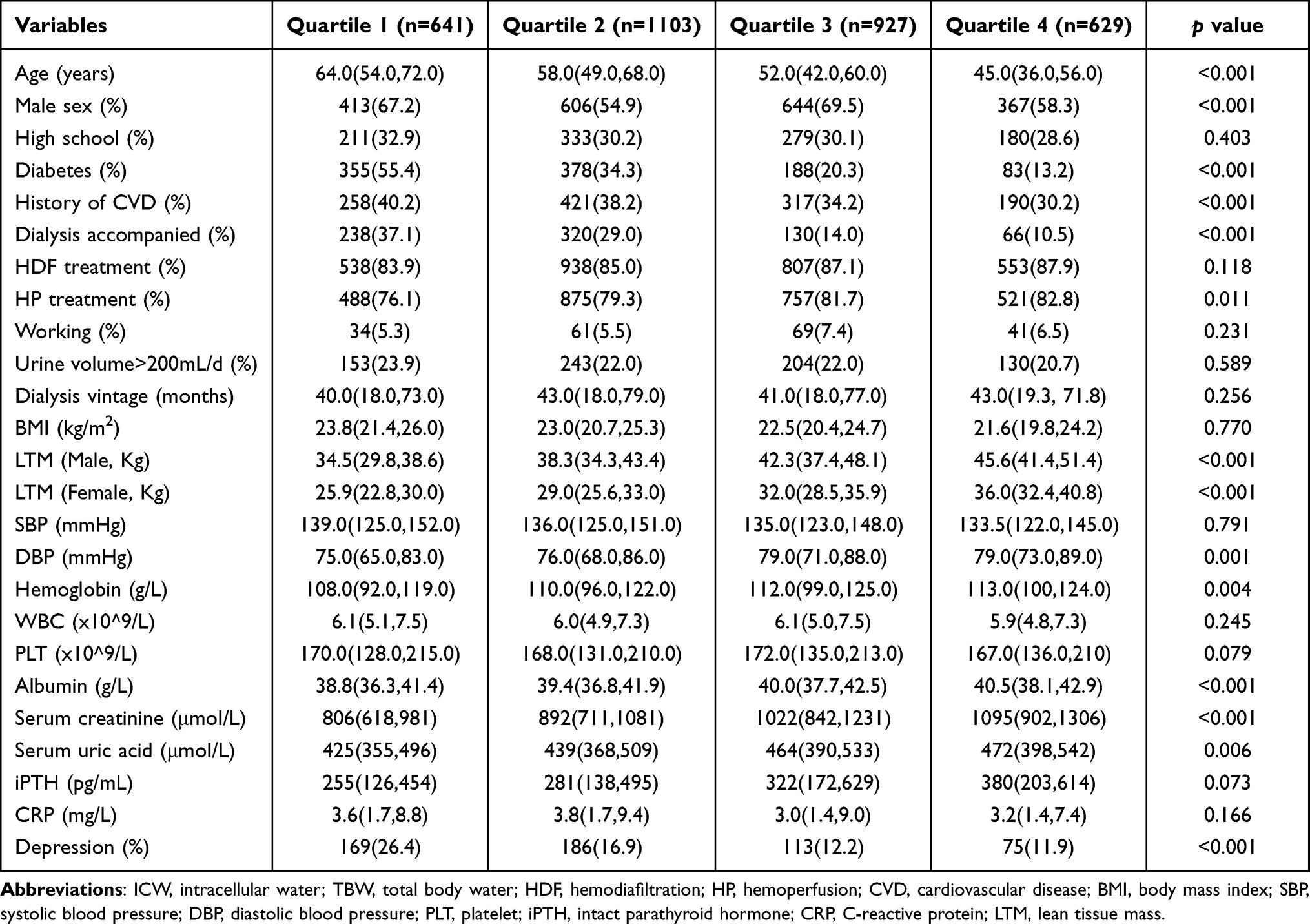 |
Table 2 Characteristics of Study Subjects According to the ICW/TBW Ratio Quartiles |
Association Between ICW/TBW Ratio and Depression
In univariate logistic regression analysis, these parameters including ICW/TBW ratio, age, sex, education, working, the distance from home to the dialysis unit, history of diabetes, history of CVD, diastolic blood pressure, albumin, and hemoglobin were statistically correlated with depression (p<0.05). With the highest quartile as reference, Table 3 shows ORs and 95% CIs in six models for the associations of depression and quartiles of ICW/TBW ratio. The depression risk of patients with Quartile 1 is 1.55 times higher than that of participants with Quartile 4 after adjusting for other above potential confounders. Patients in Quartile 2 and Quartile 3 had similar depression ORs compared with those in Quartile 4 in the fully adjusted model. To estimate whether correlations between ICW/TBW ratio and the depression diagnosed by different cutoff values of BDI scores are different, BDI cutoff scores of ≥13 and ≥15 instead of BDI scores ≥11 were, respectively, used to suggest diagnosis of depression. Though 11.4% and 7.9% instead of 16.5% of participants were diagnosed with depression (n = 375 and 261 respectively), the correlation between ICW/TBW ratio and depression has not materially been changed.
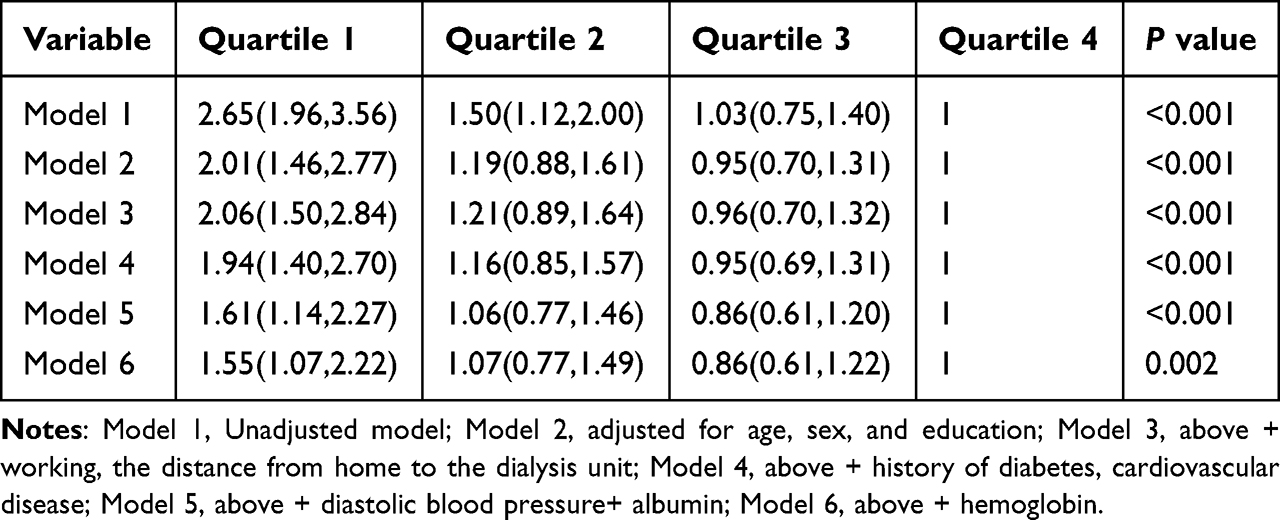 |
Table 3 Multivariate-Adjusted Odds Ratio (OR) and 95% Confidence Intervals (CI) for Depression According to the ICW/TBW Ratio Quartiles |
Subgroup Analyses for the Associations Between Depression and ICW/TBW Ratio
As shown in Figure 1, the stability of associations between depressive symptoms and ICW/TBW ratio was checked by subgroup analyses of multivariable logistic regression (quartile 4 vs quartile 1–3). On the whole, after adjusting for education, sex, age, working, the distance from home to the dialysis unit, history of diabetes, history of CVD, diastolic blood pressure, albumin, and hemoglobin except for the stratified variable, the relationship between depression and ICW/TBW ratio still persisted in four subgroups divided by education status and gender. However, this association only existed in non-diabetic patients but not diabetic patients. Both history of diabetes and education status had interactive roles in the correlation between depression and ICW/TBW ratios (p < 0.05).
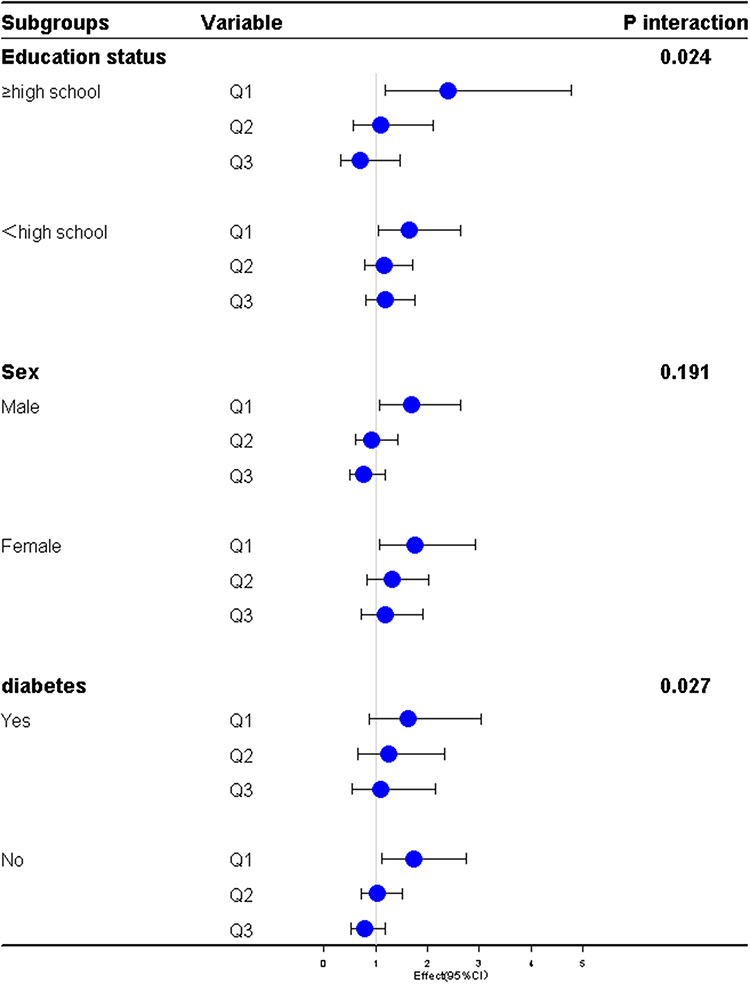 |
Figure 1 Subgroup analyses of the association between intracellular to total body water ratio and depression stratified by sex, diabetes, and education status. Notes: Odds ratios (ORs) were calculated after adjusting for age, sex, education, work, the distance from home to the dialysis unit, history of diabetes, history of cardiovascular disease, diastolic blood pressure, albumin, and hemoglobin if not stratified. |
Discussion
Previous reports have shown that the prevalence of depression diagnosed by the BDI-II questionnaire is mostly over 20% in CKD patients.34–39 However, in our study, the rate of depression was only 16.5%, even with a lower BDI cutoff. The relatively lower prevalence of depression in our MHD patients was similar to that of other two reports.40,41 This lower rate of depression might be mainly caused by two reasons. First one is that patients diagnosed with neurological and psychiatric disorders prior to beginning dialysis therapy and patients with long-term drug abuse were excluded. Second one is that the depression of our participants might have been improved to some extent because they were MHD patients, having obtained disease education in HD centers for a longer time. Consistent with most previous reports, we also found that diabetes, CVD, serum albumin, hemoglobin, gender, and education level were associated with depression, while CRP was not associated with it.38,42–47 In addition, patients with depression had lower pre-dialysis DBP than non-depression patients. Lower DBP was speculated to cause decreased cerebral perfusion and psychiatric disorders.
To our knowledge, this multicenter study is the first to explore the correlation between depression and ICW/TBW ratio in MHD patients. The main finding was that the rates of depression increased with decreasing ICW/TBW ratio. In MHD subjects, the association between ICW/TBW ratio and depression was independent of sex, education, age, work, the distance from home to the dialysis unit, history of diabetes, history of CVD, diastolic blood pressure, albumin, and hemoglobin. Moreover, both history of diabetes and education status and had interactive roles in the relationship between depression and ICW/TBW ratios. The association between ICW/TBW ratios and depression existed in patients of both genders and different education levels, but only in non-diabetic patients. In this study, we included patients who had been on MHD for more than 3 months without obvious edema. However, we also admitted that in addition to the small sample size, the reason why there was no correlation between ICW/TBW ratio and depression in diabetic patients might be the effect of diabetic recessive edema on this outcome compared with non-diabetic patients. To assess the stability of the relationships between ICW/TBW ratio and depression, BDI cutoff scores of ≥13 and ≥15 but not BDI scores ≥11 was used to suggest the diagnosis of depression, respectively. The association between ICW/TBW ratio and depression has not materially been changed.
The coexistence of depression and low ICW/TBW ratios might be ascribed to the fact that they share common risk factors such as older age, CVD, diabetes, low blood perfusion, and malnutrition. However, after multivariable adjustment including common risk factors of both depression and ICW depletion, ICW/TBW ratio is still independently associated with depression, which suggests that there might be some unique pathophysiological mechanism between depression and ICW/TBW ratios in MHD patients. Existing evidence for a relationship between depression and sarcopenia17–19 in patients undergoing MHD might suggest identifying the capacity of ICW/TBW ratios for depressive symptoms in this population.
For the treatment of depression in HD subjects, short daily HD was reported not to improve self-reported depression compared with conventional HD.48 In a meta-analysis, antidepressant use had no advantage or ungradable benefits over placebos.49 Moreover, some adverse reactions such as hypotension, headache, and sexual dysfunction had been reported during the antidepressant therapy.49 Compared with drug therapy, non-pharmacological therapies such as self-management, cognitive-behavioral therapy (CBT), telephone care, psychological intervention, music, problem-solving, and laughter therapies might have better efficacy and safety.5 For patients with depression, exercising may also be a promising therapy.50 In addition, both endurance and resistance training during HD were shown to help alleviate depressive symptoms.51 Early identification of depression and application of non-drug therapy need to be advocated, and multidisciplinary teams to work together to implement appropriate interventions should be required.
Although this study has several strengths such as detailed ascertainment of potential confounders, multicenter representation, subgroup analyses, and a relatively large sample size. The limitations of our analysis should be recognized. Firstly, this observation was based on a cross-sectional design, so we could not deduce the causal relationship between the ICW/TBW ratio and depression. In our follow-up, we will explore whether there is a mutually causal relationship between the two through a cohort study. Secondly, depression was diagnosed by a BDI-II questionnaire rather than a structured clinical interview. However, the gold standards that need judgement from psychological experts, are complex and time-consuming to be used in busy clinical work. The BDI-II scale with a high sensitivity was validated against a gold standard for diagnosing depression and has often been applied to evaluate depression among CKD participants.29–31,52–54 Thirdly, ICW, ECW, and TBW were measured using the BCM. Although tracer dilution is the gold standard for evaluating body water, it is unrealistic to use this method to assess cellular hydration state in both clinical research and daily work. BCM has been highly recognized for evaluating fluid overload and body composition among HD participants.55,56 Fourthly, although we considered some demographic and laboratory confounders in the adjusted models, there might still be some variables such as marital status and monthly income that remain unadjusted.
In conclusion, decreased ICW/TBW ratio was related to high prevalence of depression in MHD patients. Our findings may suggest that the measurement of cellular waters based on bioimpedance spectroscopy might be a simple and valid means for identifying the occurrence of depression in HD patients.
Data Sharing Statement
The datasets analyzed in this study could be obtained from the first author if the request is reasonable.
Informed Consent and Ethics Approval
Informed consent forms were signed by patients or their legal representatives before participation. This study was performed in compliance with the Declaration of Helsinki. The Ethics Review Committee of Guizhou Provincial People’s Hospital approved the protocol, and the approval number was “(Scientific Research) (2019) No. 29”.
Acknowledgment
All the patients who participated in the study are appreciated.
Funding
Guizhou Science and Technology Plan Project (QKH [2020] 2201) and Guizhou High-level innovative Talent Project (QKH [2018] 5636-2).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Levy NB. What is psychonephrology? J Nephrol. 2008;21(Suppl 13):S51–S53.
2. K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45(4 Suppl 3):S1–S153.
3. Sjöberg L, Karlsson B, Atti AR, Skoog I, Fratiglioni L, Wang HX. Prevalence of depression: comparisons of different depression definitions in population-based samples of older adults. J Affect Disord. 2017;221:123–131. doi:10.1016/j.jad.2017.06.011
4. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316(21):2214–2236. doi:10.1001/jama.2016.17324
5. Tian N, Chen N, Li PK. Depression in dialysis. Curr Opin Nephrol Hypertens. 2021;30(6):600–612.
6. Moreira JM, Bouissou Morais Soares CM, Teixeira AL, Simões E, Silva AC, Kummer AM. Anxiety, depression, resilience and quality of life in children and adolescents with pre-dialysis chronic kidney disease. Pediatr Nephrol. 2015;30(12):2153–2162. doi:10.1007/s00467-015-3159-6
7. Lee YJ, Kim MS, Cho S, Kim SR. Association of depression and anxiety with reduced quality of life in patients with predialysis chronic kidney disease. Int J Clin Pract. 2013;67(4):363–368. doi:10.1111/ijcp.12020
8. Kimmel PL, Patel SS. Quality of life in patients with chronic kidney disease: focus on end-stage renal disease treated with hemodialysis. Semin Nephrol. 2006;26(1):68–79. doi:10.1016/j.semnephrol.2005.06.015
9. Bilgic A, Akgul A, Sezer S, Arat Z, Ozdemir FN, Haberal M. Nutritional status and depression, sleep disorder, and quality of life in hemodialysis patients. J Ren Nutr. 2007;17(6):381–388. doi:10.1053/j.jrn.2007.08.008
10. Tsai YC, Chiu YW, Hung CC, et al. Association of symptoms of depression with progression of CKD. Am J Kidney Dis. 2012;60(1):54–61. doi:10.1053/j.ajkd.2012.02.325
11. Lopes AA, Bragg J, Young E, et al.; Dialysis Outcomes and Practice Patterns Study (DOPPS). Depression as a predictor of mortality and hospitalization among hemodialysis patients in the United States and Europe. Kidney Int. 2002;62(1):199–207. doi:10.1046/j.1523-1755.2002.00411.x
12. Wu PH, Lin MY, Huang TH, et al. Depression amongst patients commencing maintenance dialysis is associated with increased risk of death and severe infections: a nationwide cohort study. PLoS One. 2019;14(6):e0218335. doi:10.1371/journal.pone.0218335
13. Riezebos RK, Nauta KJ, Honig A, Dekker FW, Siegert CE. The association of depressive symptoms with survival in a Dutch cohort of patients with end-stage renal disease. Nephrol Dial Transplant. 2010;25(1):231–236. doi:10.1093/ndt/gfp383
14. Lopes AA, Albert JM, Young EW, et al. Screening for depression in hemodialysis patients: associations with diagnosis, treatment, and outcomes in the DOPPS. Kidney Int. 2004;66(5):2047–2053. doi:10.1111/j.1523-1755.2004.00977.x
15. Boulware LE, Liu Y, Fink NE, et al. Temporal relation among depression symptoms, cardiovascular disease events, and mortality in end-stage renal disease: contribution of reverse causality. Clin J Am Soc Nephrol. 2006;1(3):496–504. doi:10.2215/CJN.00030505
16. Farrokhi F, Abedi N, Beyene J, Kurdyak P, Jassal SV. Association between depression and mortality in patients receiving long-term dialysis: a systematic review and meta-analysis. Am J Kidney Dis. 2014;63(4):623–635. doi:10.1053/j.ajkd.2013.08.024
17. Chang KV, Hsu TH, Wu WT, Huang KC, Han DS. Is sarcopenia associated with depression? A systematic review and meta-analysis of observational studies. Age Ageing. 2017;46(5):738–746. doi:10.1093/ageing/afx094
18. Kim JK, Choi SR, Choi MJ, et al. Prevalence of and factors associated with sarcopenia in elderly patients with end-stage renal disease. Clin Nutr. 2014;33(1):64–68. doi:10.1016/j.clnu.2013.04.002
19. Kurita N, Wakita T, Fujimoto S, et al. Hopelessness and depression predict sarcopenia in advanced CKD and dialysis: a multicenter cohort study. J Nutr Health Aging. 2021;25(5):593–599. doi:10.1007/s12603-020-1556-4
20. Serra-Prat M, Lorenzo I, Palomera E, Ramírez S, Yébenes JC. Total body water and intracellular water relationships with muscle strength, frailty and functional performance in an elderly population. J Nutr Health Aging. 2019;23(1):96–101. doi:10.1007/s12603-018-1129-y
21. Silva AM, Matias CN, Santos DA, Rocha PM, Minderico CS, Sardinha LB. Increases in intracellular water explain strength and power improvements over a season. Int J Sports Med. 2014;35(13):1101–1105. doi:10.1055/s-0034-1371839
22. Silva AM, Fields DA, Heymsfield SB, Sardinha LB. Body composition and power changes in elite judo athletes. Int J Sports Med. 2010;31(10):737–741. doi:10.1055/s-0030-1255115
23. Silva AM, Fields DA, Heymsfield SB, Sardinha LB. Relationship between changes in total-body water and fluid distribution with maximal forearm strength in elite judo athletes. J Strength Cond Res. 2011;25(9):2488–2495. doi:10.1519/JSC.0b013e3181fb3dfb
24. Lang F, Busch GL, Ritter M, et al. Functional significance of cell volume regulatory mechanisms. Physiol Rev. 1998;78(1):247–306.
25. Häussinger D, Roth E, Lang F, Gerok W. Cellular hydration state: an important determinant of protein catabolism in health and disease. Lancet. 1993;341(8856):1330–1332. doi:10.1016/0140-6736(93)90828-5
26. Hooper L, Bunn D, Jimoh FO, Fairweather-Tait SJ. Water-loss dehydration and aging. Mech Ageing Dev. 2014;136–137:50–58. doi:10.1016/j.mad.2013.11.009
27. Miller HJ. Dehydration in the Older Adult. J Gerontol Nurs. 2015;41(9):8–13. doi:10.3928/00989134-20150814-02
28. Van Eyck A V, Eerens S, Trouet D, et al. Body composition monitoring in children and adolescents: reproducibility and reference values. Eur J Pediatr. 2021;180(6):1721–1732. doi:10.1007/s00431-021-03936-0
29. Weisbord SD, Fried LF, Unruh ML, et al. Associations of race with depression and symptoms in patients on maintenance haemodialysis. Nephrol Dial Transplant. 2007;22(1):203–208. doi:10.1093/ndt/gfl521
30. Cukor D, Coplan J, Brown C, et al. Depression and anxiety in urban hemodialysis patients. Clin J Am Soc Nephrol. 2007;2(3):484–490. doi:10.2215/CJN.00040107
31. Toups M, Carmody T, Trivedi MH, Rush AJ, Hedayati SS. Performance of depression rating scales in patients with chronic kidney disease: an item response theory-based analysis. Gen Hosp Psychiatry. 2016;42:60–66. doi:10.1016/j.genhosppsych.2016.07.005
32. Hedayati SS, Yalamanchili V, Finkelstein FO. A practical approach to the treatment of depression in patients with chronic kidney disease and end-stage renal disease. Kidney Int. 2012;81(3):247–255. doi:10.1038/ki.2011.358
33. Tian M, Yuan J, He P, Yu F, Long C, Zha Y.Lean-to-fat tissue ratio as a risk factor for cognitive impairment in patients undergoing maintenance hemodialysis. J Psychosom Res.2023;174:111464. doi:10.1016/j.jpsychores.2023.111464
34. Duan D, Yang L, Zhang M, Song X, Ren W. Depression and associated factors in Chinese patients with chronic kidney disease without dialysis: a cross-sectional study. Front Public Health. 2021;9:605651. doi:10.3389/fpubh.2021.605651
35. Haverkamp GLG, Loosman WL, Schouten RW, et al. Longitudinal associations between inflammation and depressive symptoms in chronic dialysis patients. Psychosom Med. 2019;81(1):74–80. doi:10.1097/PSY.0000000000000649
36. Oliveira CM, Costa SP, Costa LC, Pinheiro SM, Lacerda GA, Kubrusly M. Depression in dialysis patients and its association with nutritional markers and quality of life. J Nephrol. 2012;25(6):954–961. doi:10.5301/jn.5000075
37. Saglimbene V, Palmer S, Scardapane M, et al. Depression and all-cause and cardiovascular mortality in patients on haemodialysis: a multinational cohort study. Nephrol Dial Transplant. 2017;32(2):377–384. doi:10.1093/ndt/gfw016
38. Park HC, Lee H, Lee JP, et al. Lower residual renal function is a risk factor for depression and impaired health-related quality of life in Korean peritoneal dialysis patients. J Korean Med Sci. 2012;27(1):64–71. doi:10.3346/jkms.2012.27.1.64
39. van den Beukel TO, Siegert CE, van Dijk S, Ter Wee PM, Dekker FW, Honig A. Comparison of the SF-36 Five-item Mental Health Inventory and Beck Depression Inventory for the screening of depressive symptoms in chronic dialysis patients. Nephrol Dial Transplant. 2012;27(12):4453–4457. doi:10.1093/ndt/gfs341
40. Vučković M, Radić J, Kolak E, Nenadić DB, Begović M, Radić M. Body composition parameters correlate to depression symptom levels in patients treated with hemodialysis and peritoneal dialysis. Int J Environ Res Public Health. 2023;20(3):2285. doi:10.3390/ijerph20032285
41. Gao B, Song X, Hao J, et al. Association between serum uric acid and depression in patients with chronic kidney disease not requiring kidney dialysis: cross-sectional and longitudinal analyses. Med Sci Monit. 2020;26:e925386. doi:10.12659/MSM.925386
42. Brown EA, Johansson L, Farrington K, et al. Broadening Options for Long-term Dialysis in the Elderly (BOLDE): differences in quality of life on peritoneal dialysis compared to haemodialysis for older patients. Nephrol Dial Transplant. 2010;25(11):3755–3763. doi:10.1093/ndt/gfq212
43. Watnick S, Kirwin P, Mahnensmith R, Concato J. The prevalence and treatment of depression among patients starting dialysis. Am J Kidney Dis. 2003;41(1):105–110. doi:10.1053/ajkd.2003.50029
44. Araujo SM, de Bruin VM, Daher Ede F, Almeida GH, Medeiros CA, de Bruin PF. Risk factors for depressive symptoms in a large population on chronic hemodialysis. Int Urol Nephrol. 2012;44(4):1229–1235. doi:10.1007/s11255-011-0032-9
45. Feng J, Lu X, Li H, Wang S. High neutrophil-to-lymphocyte ratio is a significant predictor of depressive symptoms in maintenance hemodialysis patients: a cross-sectional study. BMC Psychiatry. 2022;22(1):313. doi:10.1186/s12888-022-03963-7
46. Gregg LP, Carmody T, Le D, Martins G, Trivedi M, Hedayati SS. A systematic review and meta-analysis of depression and protein-energy wasting in kidney disease. Kidney Int Rep. 2019;5(3):318–330. doi:10.1016/j.ekir.2019.12.009
47. Kalender B, Ozdemir AC, Koroglu G. Association of depression with markers of nutrition and inflammation in chronic kidney disease and end-stage renal disease. Nephron Clin Pract. 2006;102(3–4):c115–c121. doi:10.1159/000089669
48. Rocco MV, Lockridge RS, Beck GJ, et al. Effects of frequent nocturnal home hemodialysis: the Frequent Hemodialysis Network Nocturnal Trial. Kidney Int. 2011;80(10):1080–1091. doi:10.1038/ki.2011.213
49. Palmer SC, Natale P, Ruospo M, et al. Antidepressants for treating depression in adults with end-stage kidney disease treated with dialysis. Cochrane Database Syst Rev. 2016;2016(5):CD004541. doi:10.1002/14651858.CD004541.pub3
50. Mitrou GI, Grigoriou SS, Konstantopoulou E, et al. Exercise training and depression in ESRD: a review. Semin Dial. 2013;26(5):604–613. doi:10.1111/sdi.12112
51. Dziubek W, Kowalska J, Kusztal M, et al. The level of anxiety and depression in dialysis patients undertaking regular physical exercise training--a preliminary study. Kidney Blood Press Res. 2016;41(1):86–98. doi:10.1159/000368548
52. Østhus TB, Dammen T, Sandvik L, Bruun CM, Nordhus IH, Os I. Health-related quality of life and depression in dialysis patients: associations with current smoking. Scand J Urol Nephrol. 2010;44(1):46–55. doi:10.3109/00365590903449324
53. Kimmel PL, Peterson RA, Weihs KL, et al. Multiple measurements of depression predict mortality in a longitudinal study of chronic hemodialysis outpatients. Kidney Int. 2000;57(5):2093–2098. doi:10.1046/j.1523-1755.2000.00059.x
54. Preljevic VT, Østhus TB, Sandvik L, et al. Screening for anxiety and depression in dialysis patients: comparison of the Hospital Anxiety and Depression Scale and the Beck Depression Inventory. J Psychosom Res. 2012;73(2):139–144. doi:10.1016/j.jpsychores.2012.04.015
55. Gracia-Iguacel C, González-Parra E, Mahillo I, Ortiz A. Low intracellular water, overhydration, and mortality in hemodialysis patients. J Clin Med. 2020;9(11):3616. doi:10.3390/jcm9113616
56. Tian M, Zha Y, Qie S, Lin X, Yuan J. Association of body composition and intradialytic hypotension in hemodialysis patients. Blood Purif. 2020;49(3):334–340. doi:10.1159/000504245
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.