")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Declined Serum Resolvin D1 Levels to Predict Severity and Prognosis of Human Aneurysmal Subarachnoid Hemorrhage: A Prospective Cohort Study
Authors Yu D, Jiang F, Xu W, He P, Chen F, Liu X, Bao X
Received 17 April 2023
Accepted for publication 19 June 2023
Published 27 June 2023 Volume 2023:19 Pages 1463—1476
DOI https://doi.org/10.2147/NDT.S417630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Danfeng Yu, Fengfeng Jiang, Wei Xu, Pingyou He, Feng Chen, Xiaobo Liu, Xiang Bao
Department of Neurosurgery, Jinhua Municipal Central Hospital, Jinhua, 321000, People’s Republic of China
Correspondence: Xiang Bao, Department of Neurosurgery, Jinhua Municipal Central Hospital, Jinhua, 321000, People’s Republic of China, Email [email protected]
Background: Resolvin D1 (RvD1) possesses anti-inflammatory properties and may be neuroprotective. This study was designed to ascertain the potential role of serum RvD1 in the evaluation of aSAH severity and prognosis of human aneurysmal subarachnoid hemorrhage (aSAH).
Methods: In this prospective observational study, serum RvD1 levels were measured in 123 patients with aSAH and in 123 healthy volunteers. Six-month neurological function was assessed using extended Glasgow outcome scale (GOSE). A prognostic prediction model was appraised using a series of evaluative tools, such as a nomogram, receiver operating characteristic (ROC) curve, decision curve, calibration curve, restricted cubic spline, and Hosmer-Lemeshow goodness of fit statistics.
Results: Serum RvD1 levels were markedly lower in patients than in controls (median, 0.54 versus 1.47 ng/mL; P< 0.001). Serum RvD1 levels were independently correlated with Hunt-Hess scores (beta, − 0.154; 95% confidence interval [CI], − 0.198--0.109; VIF, 1.769; P=0.001), modified Fisher scores (beta, − 0.066; 95% CI, − 0.125--0.006; VIF, 1.567; P=0.031) and 6-month GOSE scores (beta, 1.864; 95% CI, 0.759– 2.970; VIF, 1.911; P=0.001) and were independently predictive of a poor prognosis (GOSE scores of 1– 4) (odds ratio, 0.137; 95% CI, 0.023– 0.817; P=0.029). Serum RvD1 levels significantly distinguished the risk of a worse prognosis, with an area under the ROC curve of 0.750 (95% CI, 0.664– 0.824). Using the Youden method, serum RvD1 levels < 0.6 ng/mL was effective in predicting worse prognosis with 84.1% sensitivity and 62.0% specificity. Moreover, the model containing serum RvD1 levels, Hunt-Hess scores and modified Fisher scores was efficient, reliable and beneficial in prognostic prediction using a series of the afore-mentioned evaluative tools.
Conclusion: A decline in serum RvD1 levels following aSAH is closely correlated with illness severity and independently predicts a worse outcome in patients with aSAH, implying that serum RvD1, as a prognostic biomarker of aSAH, may be of clinical value in aSAH.
Keywords: aneurysm, subarachnoid hemorrhage, resolvin D1, prognosis, severity
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH), a very important type of cerebrovascular disease globally, has a high mortality and disability rate among survivors.1 Clinically, two severity indicators, namely, the Hunt-Hess scale and modified Fisher (mFisher) scale, have been frequently applied to distinguish the risk of poor prognosis in patients with aSAH.2 Gradually, the extended Glasgow Outcome Scale (GOSE), as a substitute for the Glasgow Outcome Scale, is predominantly employed to assess the neurological outcomes of aSAH.3 Early brain injury (EBI) is specially mentioned as a pathophysiological process that is closely related to acute brain injury resulting from bleeding accumulation inside the subarachnoid space after aSAH.4 Mechanisms implicated in the molecular reactions underlying EBI include inflammatory reactions, oxidative stress, neuronal necrosis and apoptosis.5 In recent decades, some EBI-relevant biomarkers, such as neurofilament light chain, S100B, CC chemokine ligand 23, nucleotide-binding oligomerization domain-like receptor family pyrin domain-containing 3 and growth-arrest-specific protein 6, have been extensively studied with respect to their prognostic significance in aSAH.6
Resolvin D1 (RvD1) is apparently recognized as one of the lipid mediators and holds relatively potent anti-inflammatory activities.7 It is generated from docosahexaenoic acid (DHA) in phospholipid-rich tissues.8 A significant reduction of RvD1 expressions was proved in rat brain tissues after subarachnoid hemorrhage.9 Functionally, RvD1 displays neuroprotective effects by halting inflammation, attenuating cerebral edema, protecting astrocytic mitochondria, and ameliorating blood-brain barrier permeability in animal models of subarachnoid hemorrhage or traumatic brain injury.9–11 In some inflammatory patients with acute myocardial infarction, bipolar disorder, or irritable bowel syndrome, circulating levels of RvD1 are substantially reduced.12–14 Notably, plasma RvD1 levels were markedly decreased in rats subjected to traumatic brain injury or global cerebral ischemia.15 Interestingly, plasma RvD1 levels are significantly decreased after acute ischemic stroke in humans.16 Taken together, these results suggest that circulating RvD1 may serve as a biomarker of brain injury. To address this hypothesis, we measured serum RvD1 levels in a cohort of patients with aSAH and explored its prognostic role.
Methods
Study Design and Selection of Patients and Controls
In this prospective, observational, cohort, longitudinal, single-center study of aSAH patients who were enrolled at the Jinhua Municipal Central Hospital during a 3-year study period between October 2018 and October 2021, the patients underwent an initial assessment based on the following pre-specified inclusion criteria: (1) A non-traumatic history, (2) A radiologically diagnosed SAH, (3) A first-ever hemorrhagic stroke, (4) An age of adulthood, (5) A radiologically confirmed intracranial aneurysm, (6) Post-ictus hospital admission time within 24 h, and (7) Securing aneurysm using surgical clipping or interventional embolization within 48 h of hospitalization. Subsequently, patients were excluded from the current study if they met one or more of the following exclusion criteria: (1) Some specific states in relation to SAH, such as aneurysmal rerupture, multiple aneurysmal ruptures, and pseudoaneurysm rupture; (2) A history of neurological diseases, such as stroke, moderate-to-severe head trauma, moyamoya disease, intracranial arteriovenous malformations, and intracranial tumors; and (3) Other specific diseases or conditions, such as pregnancies, malignancies, haematological diseases, and severe heart, liver, lung, or kidney dysfunction. Controls were recruited from among healthy volunteers at Jinhua Municipal Central Hospital from October 2020 to October 2021. They did not present with some conventional chronic diseases, such as hyperuricemia, hypertension and diabetes mellitus, as well as there were normal results in some conventional laboratory test, such as blood glucose levels, blood leucocyte count, blood erythrocyte counts and blood potassium levels. This study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of Jinhua Municipal Central Hospital (No. JMCH2017-019) preceding the study. Informed consent was obtained from the patients’ legal representatives and controls.
Data Collection, Follow-Up and Clinical Assessment
The registered parameters included demographic data (age and sex), vascular risk factors (cigarette consumption, alcohol consumption, hypertension, diabetes mellitus, dyslipidemia, and coronary heart disease), medication history (statins, anticoagulants, antiplatelet agents, antihypertensive drugs, hypoglycemic drugs, and insulin), and vital signs (systolic and diastolic arterial blood pressure). The Hunt-Hess and mFisher scales were used as indicators for severity assessment. The parameters pertaining to the aneurysm included location, shape, and size. Neurosurgical clipping or endovascular intervention was performed to secure aneurysms. Acute hydrocephalus and intraventricular bleeding were diagnosed based on the radiological findings. External ventricular drainage was performed, as necessary. Two common complications were recorded: pneumonia and seizures. The follow-up duration after aSAH was six months. The Extended Glasgow Outcome Scale (GOSE) was used to evaluate neurological function, and scores from 1 to 4 indicated a worse prognosis.17
Laboratory Test
Venous blood was drawn from patients with aSAH, and the time from symptom onset to blood collection was recorded. Venous blood samples from controls were acquired during this study. All blood samples were centrifuged, and the separated serum samples were stored at −80°C. Serum samples were prepared. Serum RvD1 levels were measured in duplicate using an enzyme-linked immunosorbent assay kit (catalog number: EIA06548h), following the manufacturer’s instructions (Wuhan Xinqidi Biological Technology Co., Ltd., Wuhan, China). The detection range of RvD1 was from 31.2 to 2000pg/mL, sensitivity was 12pg/mL, the rate of recovery is 70–110%, inter-assay precision coefficient of variation ≤ 12% and intra-assay precision coefficient of variation ≤ 8%. All determinations were completed by the same experienced technician, who was inaccessible to the clinical information, and the mean values of the two measurements were calculated for the final data analyses.
Statistical Analysis
Measurement data, which were summarized as mean ± standard deviation (SD) or median (percentiles 25th −75th) based on the normal distribution test, were compared between the two groups using the t-test or Mann–Whitney U-test, where appropriate. Count data reported as number (percentage) were compared between the two groups using Fisher’s exact test or Pearson’s chi-square test, where appropriate. Serum RvD1 levels were compared between multiple groups using the Kruskal–Wallis test. Bivariate correlations of serum RvD1 levels and postinjury six-month GOSE scores with other variables were analyzed using Spearman correlation coefficient test. In addition, multivariate models, including the binary logistic regression model and multiple linear regression model, were configured to identify independent factors in correlation with serum RvD1 levels and poststroke six-month poor prognosis, as well as in association with 6-month poor outcome. A restricted cubic spline was constructed to verify linear association. A prognostic prediction model integrating independent predictors of six-month poor outcome, was visually displayed using a nomogram. This prediction model was appraised using a series of evaluative tools, such as receiver operating characteristic (ROC) curves, decision curves, calibration curves, and Hosmer-Lemeshow goodness of fit statistics. All statistical tests were performed using SPSS (version 22.0; SPSS Inc., Chicago, IL, USA), R software (version 3.5.1; https://www.r-project.org) and MedCalc 20.1 (MedCalc Software, Mariakerke, Belgium), and a two-sided P-value <0.05 was deemed as statistical significance.
Results
Participant Selection and Characteristics
During the study period, 160 patients with aSAH met the preset inclusion criteria and 37 patients were excluded based on exclusion criteria. Subsequently, 123 patients were included in the statistical analyses (Figure 1). A total of 123 healthy controls were included in this study.
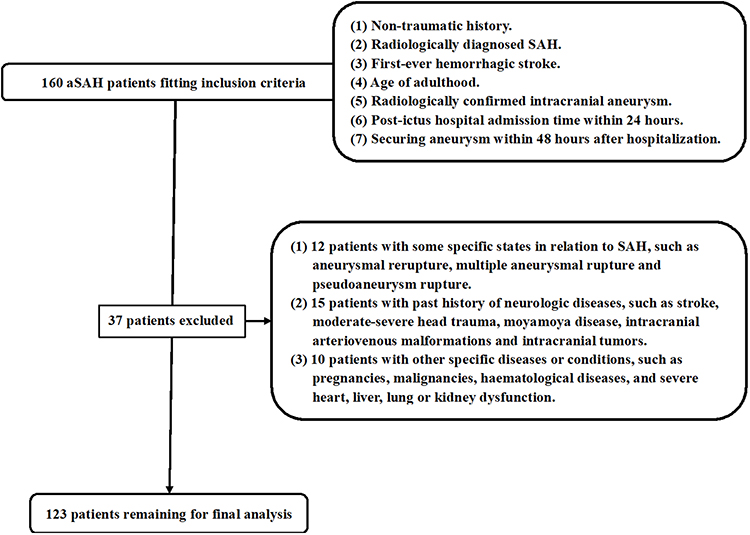 |
Figure 1 Study flowing-diagram to enroll suitable patients with aneurysmal subarachnoid hemorrhage. A total of 160 patients were recruited in accordance with the inclusion criteria; 37 patients met the exclusion criteria and were therefore excluded, leaving 123 patients for clinical investigation. Abbreviation: aSAH, aneurysmal subarachnoid hemorrhage. |
Patients were composed of 60 males and 63 females; their age ranged from 26 to 71 years, with a mean value of 50.2 years (SD,10.7 years); and there were 41 cigarette smokers and 34 alcohol drinkers among them. Controls, among whom 65 were male and 58 were female, were aged from 28 to 77 years (mean, 49.4 years; SD, 10.5 years), and a total of 43 smoked cigarettes and 36 consumed alcohol. Comparatively, the preceding variables did not differ between the two groups (all P>0.05).
Among these patients, 17 had hypertension, 10 had diabetes, 27 had dyslipidemia, and 8 cases suffering from coronary heart disease. Regarding medication history, previous oral administration of statins, anticoagulants, antiplatelet agents, antihypertensive drugs, and hypoglycemic drugs or insulin was observed in 19, 6, 11, 12, and 7 patients, respectively. Systolic and diastolic arterial blood pressure ranged from 73 to 183 mmHg (mean, 129.5 mmHg; SD, 25.5 mmHg) and from 48 to 110 mmHg (mean, 78.4 mmHg; SD, 17.1 mmHg) respectively. As regards aneurysmal radiological parameters, ratio of anterior to posterior circulation, cystic aneurysm to others, and aneurysmal diameter <10 mm to ≥10 mm were 4.13 (99/24), 5.47 (104/19) and 1.24 (68/55) respectively. Aneurysms were treated using surgical clipping and endovascular intervention in 48 and 75 patients, respectively. Seventeen patients had acute hydrocephalus and 20 had intraventricular bleeding. Eventually, 18 underwent external this study. The common complications included pneumonia (n = 17) and epilepsy (n = 11). Patients were admitted into hospital from 1.0 to 24.0 hours (median, 9.5 hours; percentiles 25th–75th, 6.1–14.0 hours) after stroke. And blood-collection was done from 2.0 to 26.0 hours (median, 10.3 hours; lower-upper quartiles, 6.6–15.1 hours).
Serum RvD1 Levels and Its Relation to Stroke Severity
As shown in Figure 2, serum RvD1 levels were markedly lower in the aSAH group than in the control group (P<0.001). Among patients with aSAH, Hunt-Hess scores and mFisher scores ranged from 1 to 5 (median, 3; lower-upper quartiles, 2–4) and from 1 to 4 (median, 2; lower-upper quartiles, 2–3) respectively; and serum RvD1 levels were significantly inversely correlated with Hunt-Hess scores (P<0.001; Figure 3A) and mFisher scores (P<0.001; Figure 3B). In addition to Hunt-Hess and mFisher scores, serum RvD1 levels were also highly correlated with the other two variables listed in Table 1, namely, leakage of bleeding into the intraventricular space (P<0.01) and blood glucose levels (P<0.01). The above-mentioned four significantly correlated variables were forced into the multivariate linear regression model, and it was confirmed that serum RvD1 levels were independently correlated with Hunt-Hess and mFisher scores (both P<0.05; Figure 3C). Furthermore, Hunt-Hess and mFisher scores were considered as two qualitative variables. Among them, Hunt-Hess scores from 1 to 5 were 21, 22, 40, 32, and 8, respectively, and the mFisher scores from 1 to 4 were 20, 46, 45, and 12, respectively. As shown in Figure 3D and E, serum RvD1 levels were substantially reduced in the order of Hunt-Hess scores from 1 to 5 and mFisher scores from 1 to 4 (both P<0.001).
 |
Table 1 Bivariate Correlative Analysis of Serum Resolvin D1 Levels After Aneurysmal Subarachnoid Hemorrhage |
 |
Figure 2 Serum resolvin D1 levels between controls and patients with aneurysmal subarachnoid hemorrhage. Patients exhibited significantly lower serum resolvin D1 levels than controls (P<0.001). Abbreviation: RvD1, resolvin D1. |
 |
Figure 3 Serum resolvin D1 levels in relation to severity of aneurysmal subarachnoid hemorrhage. Serum resolvin D1 levels were significantly inversely correlated with Hunt-Hess scores (P<0.001; (A)), and modified Fisher scores (P<0.001; (B)) using univariate correlative analysis were also independently correlated with them (both P<0.05; (C)) and were significantly decreased in the order of Hunt-Hess scores from 1 to 5 (P<0.001; (D)) and modified Fisher scores from 1 to 4 (P<0.001; (E)). Abbreviations: RvD1, resolvin D1; mFisher, modified Fisher; 95% CI, 95% confidence interval. |
Serum RvD1 Levels and Poststroke 6-Month GOSE Scores
Six months after aSAH, GOSE scores ranged from 1 to 8 (median, 5; percentiles 25th–75th, 3–7); and GOSE scores from 1 to 8 were experienced by 11, 11, 9, 13, 22, 14, 15, and 28 patients, respectively. Figure 4A shows that there was a close, positive correlation between serum RvD1 levels and GOSE scores (P<0.001); and in Figure 4B, serum RvD1 levels were significantly increased in the order of GOSE scores from 1 to 8 (P<0.001). As shown in Table 2, serum RvD1 levels were significantly correlated with Hunt-Hess scores, mFisher scores, intraventricular bleeding, and blood glucose levels (all P<0.05). The preceding significant variables in the univariate analysis were incorporated into the multiple models, and it was shown that serum RvD1 levels, Hunt-Hess scores, and mFisher scores were independently correlated with GOSE scores 6 months after aSAH (all P<0.05; Figure 4C).
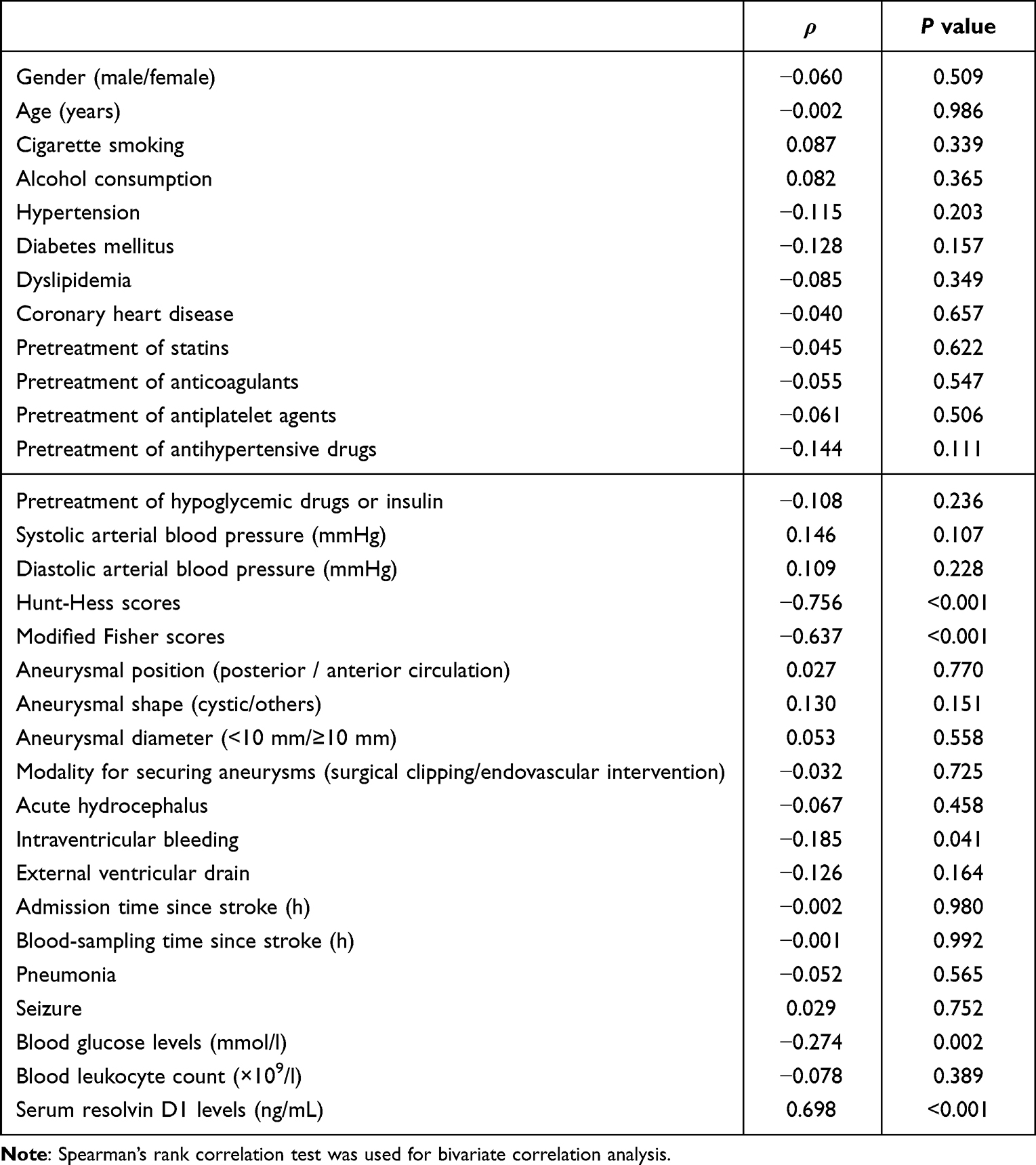 |
Table 2 Bivariate Correlative Analysis of Extended Glasgow Outcome Scale Scores at Six Months After Aneurysmal Subarachnoid Hemorrhage |
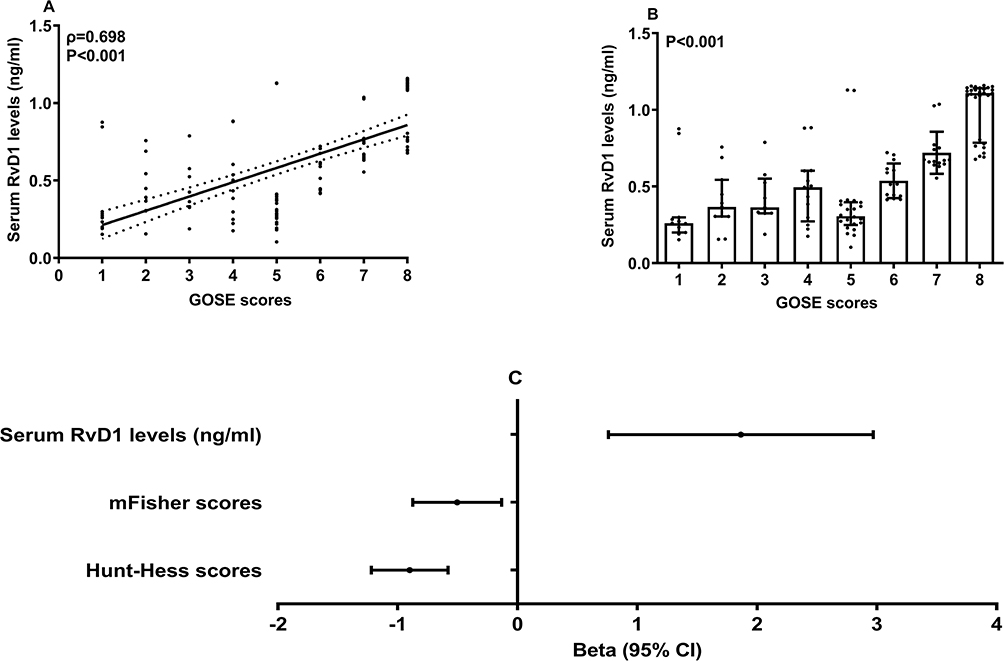 |
Figure 4 Serum resolvin D1 levels in correlation with Extended Glasgow Outcome Scale scores at six months after aneurysmal subarachnoid hemorrhage. Serum resolvin D1 levels were significantly positively correlated with Extended Glasgow Outcome Scale scores six months after stroke (P<0.001; (A)) using univariate correlative analysis, were significantly increased in the order of Extended Glasgow Outcome Scale scores from 1 to 8 (P<0.001; (B)), and were also independently correlated with it (P<0.05; (C)). Abbreviations: RvD1, resolvin D1; mFisher, modified Fisher; 95% CI, 95% confidence interval; GOSE, Extended Glasgow Outcome Scale. |
Serum RvD1 Levels in Relation to Post-Stroke Poor Outcome
Six months after aSAH, 44 patients had poor outcomes (GOSE scores of 1–4). As shown in Figure 5A, patients with poor prognosis had significantly lower serum RvD1 levels than those with good prognosis (P<0.001). As listed in Table 3, in addition to serum RvD1 levels, other variables were Hunt-Hess scores, mFisher scores, and blood glucose levels, which were significantly higher in patients with a poor prognosis than in those with a good prognosis (all P<0.05). As depicted in Figure 5B, serum RvD1 levels, Hunt-Hess scores, and mFisher scores remained independently associated with a 6-month poor prognosis (all P<0.05). Alternatively, using the Hosmer-Lemeshow test, the model was comparatively stable (P=0.692). Figure 6A shows the AUC and optimal cutoff value of serum RvD1 levels for prognostic prediction. As outlined in Figure 6B, serum RvD1 levels had a similar AUC in comparison to Hunt-Hess scores and mFisher scores (both P>0.05); the combination of the preceding three variables had an AUC that significantly exceeded any one of them (all P<0.05). Under a restricted cubic spline, serum RvD1 levels showed a linear relationship with the risk of poor prognosis (P=0.428; Figure 7). As outlined in Figure 8, a nomogram integrating the three prognostic determinants provides a visual description of the prediction model. Calibration curve analysis demonstrated that the model was relatively stable (Figure 9), and decision curve analysis confirmed that the model was of clinical benefit (Figure 10).
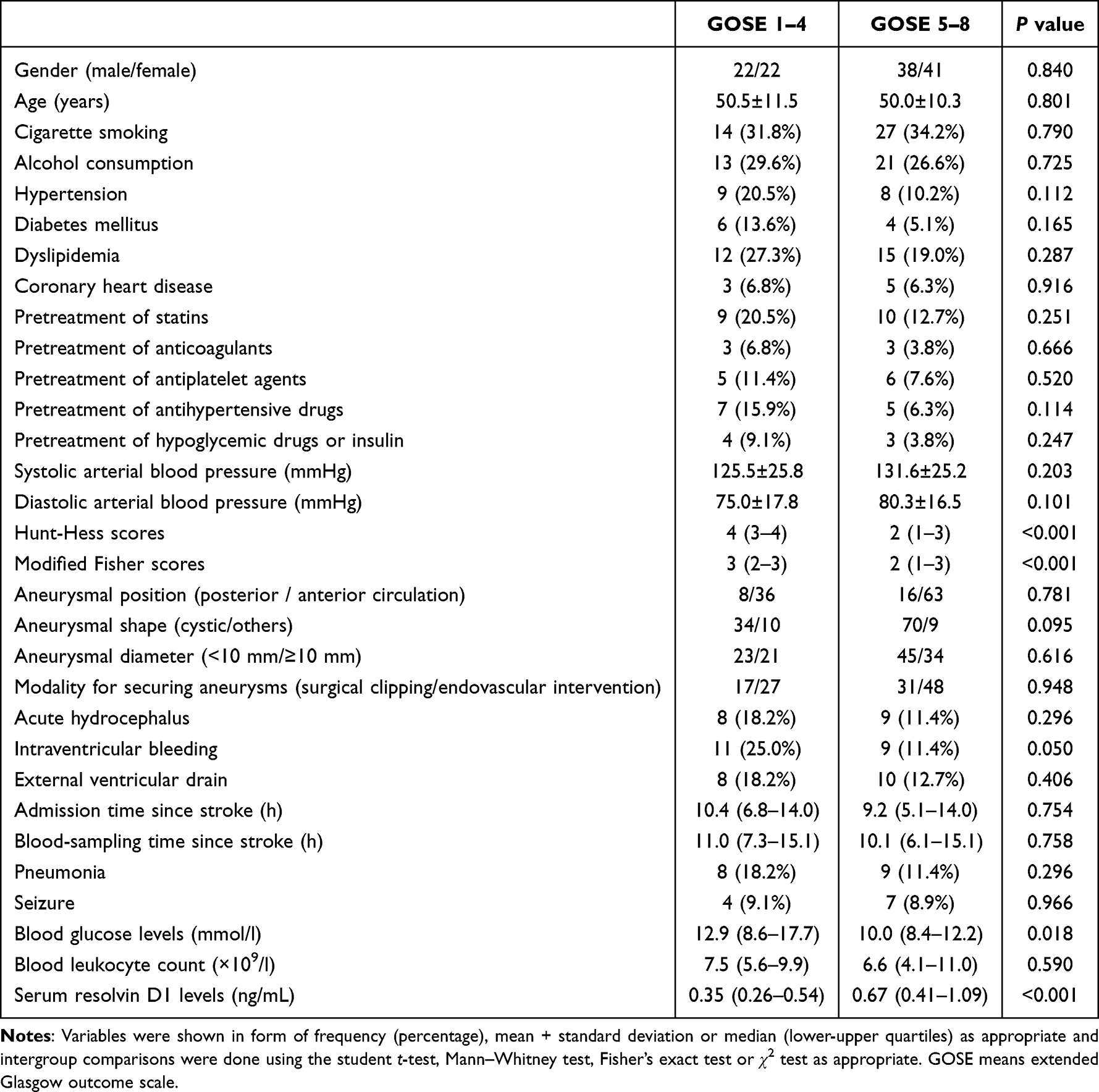 |
Table 3 Factors in Relation to Poor Outcome at Six Months After Aneurysmal Subarachnoid Hemorrhage |
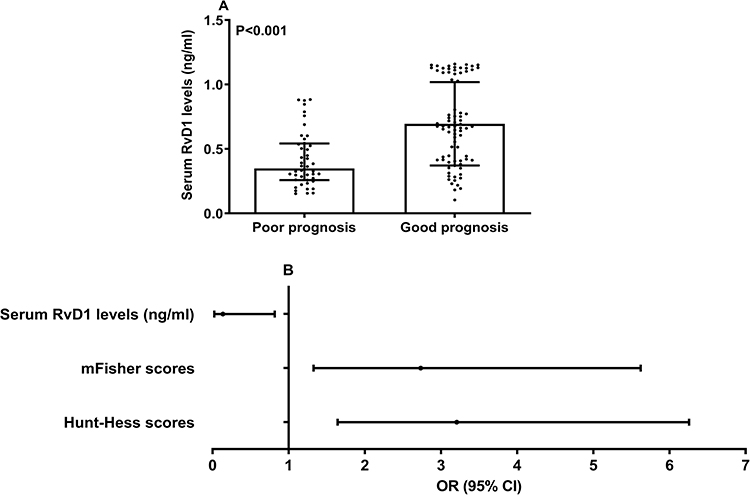 |
Figure 5 Serum resolvin D1 levels in association with poor prognosis at six months after aneurysmal subarachnoid hemorrhage. Serum resolvin D1 levels were significantly lower in patients with poor prognosis than in those with good prognosis at six months after stroke (P<0.001; (A)) using univariate analysis and were also independently associated with post-stroke six-month poor prognosis (P<0.05; (B)). Abbreviations: RvD1, resolvin D1; mFisher, modified Fisher; OR, odds ratio; 95% CI, 95% confidence interval. |
 |
Figure 6 Receiver operating characteristic curve with respect to serum resolvin D1 levels for predicting poor prognosis at 6 months after aneurysmal subarachnoid hemorrhage. Serum resolvin D1 levels significantly predicted six-month poor prognosis after stroke (P<0.001; (A)), and its combination with Hunt-Hess and modified Fisher scores had a significantly stronger prognostic capability than any one of them (all P>0.05; (B)). Abbreviations: RvD1, resolvin D1; mFisher, modified Fisher; AUC, area under the curve; 95% CI, 95% confidence interval. |
 |
Figure 7 Restricted cubic spline assessing linear relationship between serum resolvin D1 levels and risk of poor prognosis at 6 months after aneurysmal subarachnoid hemorrhage. Serum resolvin D1 levels linearly correlated with the risk of poor prognosis (P>0.05). Abbreviations: RvD1, resolvin D1; OR, odds ratio; 95% CI, 95% confidence interval. |
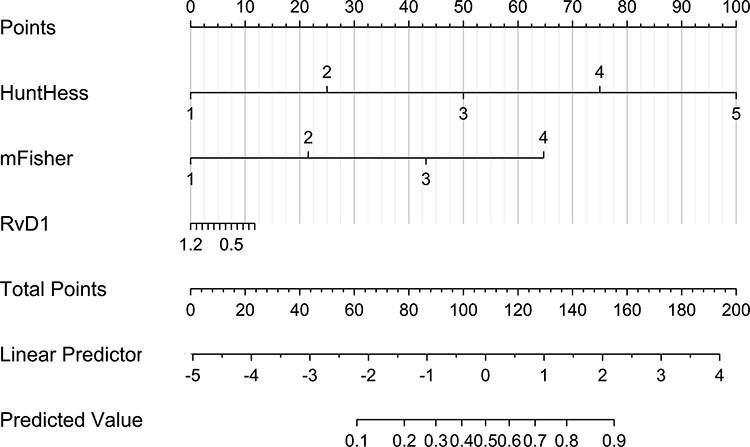 |
Figure 8 Nomogram visually describing prediction model integrating serum resolvin D1 levels Hunt-Hess scores and modified Fisher scores in prognostic prediction after aneurysmal subarachnoid hemorrhage. Nomogram could efficiently predict 6-month poor prognosis following aneurysmal subarachnoid hemorrhage. Abbreviations: RvD1, resolvin D1; mFisher, modified Fisher. |
 |
Figure 9 Calibration curve determining model stability in prognostic prediction among patients with aneurysmal subarachnoid hemorrhage. Prediction model was comparatively stable in prognostication of aneurysmal subarachnoid hemorrhage in humans. |
 |
Figure 10 Decision curve investigating model clinical benefit in prognostic prediction of patients after aneurysmal subarachnoid hemorrhage. The prediction model containing serum resolvin D1 levels, Hunt-Hess scores, and modified Fisher scores showed a relatively high clinical benefit in predicting prognosis among patients with aneurysmal subarachnoid hemorrhage. Abbreviations: RvD1, resolvin D1; mFisher, modified Fisher. |
Discussion
Although serum RvD1 levels were found to be significantly decreased after acute ischemic stroke in humans,16,18 to the best of our knowledge, change in its levels in patients with aSAH remain unclear. This clinical study demonstrated that (1) decreased serum RvD1 levels after human aSAH, in comparison to healthy controls, were independently correlated with Hunt-Hess scores, mFisher scores and post-stroke six-month GOSE scores; (2) serum RvD1 emerged as an independent predictor of six-month poor prognosis (GOSE scores of 1–4) after aSAH; and (3) serum RvD1 levels alone or in combination with Hunt-Hess scores and mFisher scores displayed high prognostic predictive efficiency. In summary, serum RvD1 levels may be correlated with the severity and clinical outcomes of human aSAH.
RvD1 mainly exhibits potent anti-inflammatory and pro-resolving effects, thereby exerting protective effects.7 Specifically, RvD1 efficiently stabilized atherosclerotic plaques in rats with carotid artery balloon injury.19 In an experimental model of cerebral injury, RvD1 was found to significantly decrease neuronal apoptosis.20 In addition, RvD1 attenuates neuronal injury and subsequently improves motor dysfunction in Parkinson’s disease rats.21 Similarly, in rats with subarachnoid hemorrhage, RvD1 markedly depresses brain edema, represses blood-brain barrier disruption, and ultimately improves neurological deficits.9,10 Consistently, RvD1 can dramatically inactivate microglia, thereby improving cognitive impairment in rats with traumatic brain injury.22 RvD1 can be produced from docosahexaenoic acid,8 indicating that RvD1 may be harmless to humans. Additionally, RvD1 may be more effective than docosahexaenoic acid in preventing cadmium chloride-induced memory loss and hippocampal damage in rats.23 Therefore, RvD1 may be considered as a potential drug for the clinical treatment of aSAH.
In rat brain tissues subjected to subarachnoid hemorrhage, RvD1 expression is significantly decreased.9 Moreover, plasma RvD1 levels are substantially lower in rats with traumatic brain injury or global cerebral ischemia than in normal rats.15 Alternatively, RvD1 levels are markedly decreased in patients with acute plaque rupture events compared to those with asymptomatic carotid disease.24 Moreover, plasma RvD1 levels in patients with acute ischemic stroke are significantly lower than those in control individuals.18 Recently, reduced plasma RvD1 levels after acute ischemic stroke have been reversed by endovascular thrombectomy.16 In our study, serum RvD1 levels were significantly decreased after aSAH. Considering its protective effects,7 reduced circulating RvD1 levels may be partially attributed to the depletion of RvD1.
Higher circulating RvD1 levels correspond to better cognitive function in patients with acute ischemic stroke during a 6-month follow-up.25 In the current study, serum RvD1 levels were strongly correlated with the severity of aSAH and substantially associated with six-month poor outcome in patients with aSAH. Moreover, serum RvD1 levels were significantly effective in predicting post-stroke six-month poor prognosis. Intriguingly, serum RvD1 levels combined with Hunt-Hess scores and mFisher scores had significantly higher prognostic predictive ability than any one of them. Such a prediction model integrating serum RvD1 levels, Hunt-Hess scores, and mFisher scores may be relatively stable and clinically beneficial when using a series of evaluative tools such as decision curves, calibration curves, and Hosmer-Lemeshow goodness-of-fit statistics. Overall, serum RvD1 may serve as a potential prognostic marker of aSAH in humans.
Conclusions
Our study found that serum RvD1 levels, which are significantly lower after aSAH and highly correlated with the severity of aSAH, are substantially associated with GOSE scores and poor prognosis 6 months after aSAH. These data strongly support the assumption that serum RvD1 is a promising prognostic biomarker that may be of clinical value for aSAH prognostication and risk stratification.
Abbreviations
aSAH, aneurysmal subarachnoid hemorrhage; AUC, area under the curve; CI, confidence interval; GOSE, extended Glasgow outcome scale; OR, odds ratio; ROC, receiver operating characteristic; RvD1, resolvin D1; EBI, early brain injury.
Acknowledgment
The authors thank all staff for technical support and are grateful to all participants for providing blood samples.
Disclosure
The authors report no conflicts of interest concerning the materials or methods used in this study, or the findings specified in this article.
References
1. Rouanet C, Silva GS. Aneurysmal subarachnoid hemorrhage: current concepts and updates. Arq Neuropsiquiatr. 2019;77(11):806–814. doi:10.1590/0004-282X20190112
2. Osgood ML. Aneurysmal subarachnoid hemorrhage: review of the pathophysiology and management strategies. Curr Neurol Neurosci Rep. 2021;21(9):50. doi:10.1007/s11910-021-01136-9
3. Jiang F, Chen Z, Hu J, Liu Q. Serum soluble scavenger receptor A levels are associated with delayed cerebral ischemia and poor clinical outcome after aneurysmal subarachnoid hemorrhage: a prospective observational study. Neuropsychiatr Dis Treat. 2022;18:2529–2541. doi:10.2147/NDT.S387487
4. Zhao Y, Luo Y, Liu Y, Lenahan C, Wu Q, Chen S. The role of autophagy and apoptosis in early brain injury after subarachnoid hemorrhage: an updated review. Mol Biol Rep. 2022;49(11):10775–10782. doi:10.1007/s11033-022-07756-9
5. Daou BJ, Koduri S, Thompson BG, Chaudhary N, Pandey AS. Clinical and experimental aspects of aneurysmal subarachnoid hemorrhage. CNS Neurosci Ther. 2019;25(10):1096–1112. doi:10.1111/cns.13222
6. Neifert SN, Chapman EK, Martini ML, et al. Aneurysmal subarachnoid hemorrhage: the last decade. Transl Stroke Res. 2021;12(3):428–446. doi:10.1007/s12975-020-00867-0
7. Roohbakhsh A, Etemad L, Karimi G. Resolvin D1: a key endogenous inhibitor of neuroinflammation. Biofactors. 2022;48(5):1005–1026. doi:10.1002/biof.1891
8. Ji RR, Xu ZZ, Strichartz G, Serhan CN. Emerging roles of resolvins in the resolution of inflammation and pain. Trends Neurosci. 2011;34(11):599–609. doi:10.1016/j.tins.2011.08.005
9. Wei C, Guo S, Liu W, et al. Resolvin D1 ameliorates inflammation-mediated blood-brain barrier disruption after subarachnoid hemorrhage in rats by modulating A20 and NLRP3 inflammasome. Front Pharmacol. 2021;11:610734. doi:10.3389/fphar.2020.610734
10. Liu GJ, Tao T, Zhang XS, et al. Resolvin D1 attenuates innate immune reactions in experimental subarachnoid hemorrhage rat model. Mol Neurobiol. 2021;58(5):1963–1977. doi:10.1007/s12035-020-02237-1
11. Bisicchia E, Sasso V, Catanzaro G, et al. Resolvin D1 halts remote neuroinflammation and improves functional recovery after focal brain damage via ALX/FPR2 receptor-regulated MicroRNAs. Mol Neurobiol. 2018;55(8):6894–6905. doi:10.1007/s12035-018-0889-z
12. Karayiğit O, Nurkoç SG, Başyiğit F, Kızıltunç E. The role of serum resolvin D1 levels in determining the presence and prognosis of ST-segment elevation myocardial infarction. Med Princ Pract. 2022;31(6):548–554. doi:10.1159/000527064
13. Kok Kendirlioglu B, Unalan Ozpercin P, Yuksel Oksuz O, et al. Resolvin D1 as a novel anti-inflammatory marker in manic, depressive and euthymic states of bipolar disorder. Nord J Psychiatry. 2020;74(2):83–88. doi:10.1080/08039488.2019.1673480
14. Karatay E, Utku ÖG. Serum resolvin D1 levels as a marker of inflammation in constipation dominant irritable bowel syndrome. Turk J Gastroenterol. 2020;31(2):113–119. doi:10.5152/tjg.2020.19751
15. Jung JS, Kho AR, Lee SH, et al. Changes in plasma lipoxin A4, resolvins and CD59 levels after ischemic and traumatic brain injuries in rats. Korean J Physiol Pharmacol. 2020;24(2):165–171. doi:10.4196/kjpp.2020.24.2.165
16. Hao J, Feng Y, Xu X, et al. Plasma lipid mediators associate with clinical outcome after successful endovascular thrombectomy in patients with acute ischemic stroke. Front Immunol. 2022;13:917974. doi:10.3389/fimmu.2022.917974
17. Walter J, Grutza M, Möhlenbruch M, et al. The local intraarterial administration of nimodipine might positively affect clinical outcome in patients with aneurysmal subarachnoid hemorrhage and delayed cerebral ischemia. J Clin Med. 2022;11(7):2036. doi:10.3390/jcm11072036
18. Szczuko M, Kotlęga D, Palma J, et al. Lipoxins, RevD1 and 9, 13 HODE as the most important derivatives after an early incident of ischemic stroke. Sci Rep. 2020;10(1):12849. doi:10.1038/s41598-020-69831-0
19. Makino Y, Miyahara T, Nitta J, et al. Proresolving lipid mediators resolvin D1 and protectin D1 isomer attenuate neointimal hyperplasia in the rat carotid artery balloon injury model. J Surg Res. 2019;233:104–110. doi:10.1016/j.jss.2018.07.049
20. Correia Bacarin C, Mori MA, Dias Fiuza Ferreira E, Valério Romanini C, Weffort de Oliveira RM, Milani H. Fish oil provides robust and sustained memory recovery after cerebral ischemia: influence of treatment regimen. Physiol Behav. 2013;119:61–71. doi:10.1016/j.physbeh.2013.06.001
21. Krashia P, Cordella A, Nobili A, et al. Blunting neuroinflammation with resolvin D1 prevents early pathology in a rat model of Parkinson’s disease. Nat Commun. 2019;10(1):3945. doi:10.1038/s41467-019-11928-w
22. Ren YZ, Zhang BZ, Zhao XJ, Zhang ZY. Resolvin D1 ameliorates cognitive impairment following traumatic brain injury via protecting astrocytic mitochondria. J Neurochem. 2020;154(5):530–546. doi:10.1111/jnc.14962
23. Shati AA, El-Kott AF. Resolvin D1 protects against cadmium chloride-induced memory loss and hippocampal damage in rats: a comparison with docosahexaenoic acid. Hum Exp Toxicol. 2021;40(12_suppl):S215–S232. doi:10.1177/09603271211038739
24. Bazan HA, Lu Y, Jun B, Fang Z, Woods TC, Hong S. Circulating inflammation-resolving lipid mediators RvD1 and DHA are decreased in patients with acutely symptomatic carotid disease. Prostaglandins Leukot Essent Fatty Acids. 2017;125:43–47. doi:10.1016/j.plefa.2017.08.007
25. Kotlęga D, Peda B, Drozd A, et al. Prostaglandin E2, 9S-, 13S-HODE and resolvin D1 are strongly associated with the post-stroke cognitive impairment. Prostaglandins Other Lipid Mediat. 2021;156:106576. doi:10.1016/j.prostaglandins.2021.106576
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.