")
Back to Journals » Infection and Drug Resistance » Volume 16
Declined Humoral Immunity of Kidney Transplant Recipients to SARS-CoV-2 Vaccines
Authors Mahallawi WH , Alharbi WA, Aloufi SA, Ibrahim NA , Abdelrahman MM, Alhomayeed BA, Aboonq MS , Alqahtani SAM, Rajih ES , Bakhsh AM , Sandokji I
Received 2 March 2023
Accepted for publication 3 May 2023
Published 9 May 2023 Volume 2023:16 Pages 2829—2840
DOI https://doi.org/10.2147/IDR.S408686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Waleed H Mahallawi,1 Wael A Alharbi,1 Sultan A Aloufi,1 Nadir A Ibrahim,1 Muntasir M Abdelrahman,2 Bader A Alhomayeed,2 Moutasem S Aboonq,3 Saeed Awad M Alqahtani,3 Emad S Rajih,4 Abdulaziz M Bakhsh,4 Ibrahim Sandokji5
1Medical Laboratory Technology Department, College of Applied Medical Sciences, Taibah University, Madinah, Saudi Arabia; 2King Fahad Hospital, Ministry of Health, Madinah, Saudi Arabia; 3Department of Physiology, College of Medicine, Taibah University, Madinah, Saudi Arabia; 4Urology Department, College of Medicine, Taibah University, Madinah, Saudi Arabia; 5Department of Pediatrics, College of Medicine, Taibah University, Madinah, Saudi Arabia
Correspondence: Waleed H Mahallawi, Medical Laboratory Technology Department, College of Applied Medical Sciences, Taibah University, Madinah, Saudi Arabia, Email [email protected]
Background: Kidney transplant recipients (KTRs) commonly suffer from impaired immunity. KTRs’ compromised immune response to COVID-19 vaccines indicates urgent revision of immunisation policies.
Methods: A cross-sectional study was conducted in Madinah, Saudi Arabia of 84 KTRs who had received at least one dose of a COVID-19 vaccine. ELISA was used to evaluate anti-spike SARS-CoV-2 IgG and IgM antibody levels in blood samples obtained one month and seven months after vaccination. Univariate and multivariate analyses were performed to identify associations between seropositive status and factors such as the number of vaccine doses, transplant age, and immunosuppressive therapies.
Results: The mean age of KTRs was 44.3 ± 14.7 years. The IgG antibody seropositivity rate (n=66, 78.5%) was significantly higher than the seronegativity rate (n=18, 21.4%) in the whole cohort (p< 0.001). In KTRs seroconverting after one month (n=66), anti-SARS-CoV-2 IgG levels declined significantly between one month (median [IQR]:3 [3– 3]) and seven months (2.4 [1.7– 2.6]) after vaccination (p< 0.01). In KTRs with hypertension, IgG levels significantly decreased between one and seven months after vaccination (p< 0.01). IgG levels also decreased significantly in KTRs with a transplant of > 10 years (p=0.02). Maintenance immunosuppressive regimens (triple immunosuppressive therapy and steroid-based and antimetabolite-based regimens) led to a significant decrease in IgG levels between the first and second sample (p< 0.01). KTRs receiving three vaccine doses showed higher antibody levels than those receiving a single dose or two doses, but the levels decreased significantly between one (median [IQR]: 3 [3– 3]) and seven months (2.4 [1.9– 2.6]) after vaccination (p< 0.01).
Conclusion: KTRs’ humoral response after SARS-CoV-2 vaccination is dramatically inhibited and wanes. Antibody levels show a significant decline over time in KTRs with hypertension; receiving triple immunosuppressive therapy or steroid-based or antimetabolite-based regimens; receiving mixed mRNA and viral vector vaccines; and with a transplant of > 10 years.
Keywords: SARS-CoV-2, kidney transplant recipients, booster, immunosuppression, COVID-19 vaccines, humoral immune response
Introduction
In late December 2019, Wuhan, China witnessed an outbreak of severe pneumonia. Its aetiology was identified as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) which causes COVID-19 disease.1 The symptoms of COVID-19 disease range from mild upper respiratory tract symptoms to severe acute respiratory syndrome.2 Over 671,314,131 confirmed cases and 6,730,278 deaths have been caused by SARS-CoV-2 worldwide (https://www.worldometers.info/coronavirus/. Accessed on 15-01-2023).
The humoral response to SARS-CoV-2 was used to monitor stages of disease progression early in the pandemic.3 The IgM antibody can be detected from 3–6 days after the onset of symptoms and disappears after 12 weeks. The IgG antibody appears 16 to 18 days after infection and its level gradually declines by the 14th week, but its presence has been noted more than a year after infection.4,5
Solid organ transplant recipients are believed to be at greater risk of infection and development of COVID-19 because of their proportionally higher frequency of underlying comorbidities, regular contact with medical support settings, and the need for systemic immunosuppression.6 Thus, they are more vulnerable to infection and disease complications.
Triple immunosuppressive therapy commonly comprises tacrolimus, mycophenolate mofetil, and prednisone. In addition, azathioprine is used with some patients, including some in the present study, who cannot endure the gastrointestinal side effects of mycophenolate mofetil. Prednisone is a type of corticosteroid that inhibits nuclear factor κB, a transcription factor essential for the expression of some cytokines that are important for T-cell stimulation. Mycophenolate mofetil is an antiproliferative drug specifically intended to inhibit T-cell proliferation. Tacrolimus and cyclosporine are calcineurin inhibitors that block signal 1 and inhibit T-cell proliferation. Azathioprine is a purine analogue that combines with cellular DNA and deters purine nucleotide synthesis and gene replication, in addition to finally activating T-cells.7–10 Furthermore, antimetabolites have been shown to worsen B-cell proliferation and formation of plasmablasts.11 They mechanistically inhibit IL-6-mediated STAT3 signalling, essential for plasma cell differentiation and vital for their endurance and immunoglobulin secretion in bone marrow.12
In this study, we aimed to investigate primarily the effect of immunosuppressive drugs on the persistence of COVID 19 vaccine-induced antibody of KTRs. Additionally, to find out other factors that could influence the antibody levels over the time since vaccination.
We used the enzyme-linked immunosorbent assay (ELISA) to assess the durability of the anti-SARS-CoV-2 IgG and IgM antibodies in KRTs by measuring antibodies against viral receptor-binding domain SARS-CoV-2 spike proteins one month and seven months after vaccination.
Materials and Methods
Study Population
This study was conducted at a dialysis centre in Madinah, Saudi Arabia. Patients treated in this center include patients with all kidney diseases such as transplants and those on dialysis. One hundred and three KTRs agreed to participate in this study. We used a convenience sampling method to select patients. After exclusion of patients based on the criteria described below, 84 patients were finally recruited for the study.
Inclusion and Exclusion Criteria
We included in this study only kidney transplant patients who had received at least one dose of a COVID-19 vaccine. We excluded dialysis patients and/or patients that did not receive a transplant.
Sample and Blood Collection
On the follow-up date of each KTR, blood samples were collected and then transported to the Virology Research Laboratory of the College of Applied Medical Sciences, Taibah University. Samples were centrifuged at 2500 rpm for 10 minutes within one hour of collection; serum was separated and kept at −20 °C until analysis.
We took two samples from the participants: one month and seven months after vaccination.
Enzyme-Linked Immunosorbent Assays
We evaluated the presence of anti-SARS-CoV-2 antibody in patients’ serum using IgG and IgM kits (BGI) according to the manufacturer’s instructions. Positive, negative, and blank controls were included on each ELISA plate. The assay’s specificity and sensitivity to IgG were 98.38% and 98.71%, respectively, and to IgM were 96.76% and 98.06%, respectively (https://www.bgi.com/global/service/covid-19). In brief, serum samples diluted at a 1:100 ratio were added to microtiter plates that were coated with SARS-CoV-2 S1/S2 viral antigens and then incubated at 37 °C for 30 minutes. After incubation was completed, the plates were washed and secondary anti-human IgG /IgM conjugated with horseradish peroxidase was added. The plates were then incubated for 20 minutes at 37 °C, followed by washing and addition of substrate. The substrate was incubated in the dark for 10 minutes and a stop solution was added. After colour development was completed, optical density was measured at 450 nm. Cut off values of anti-SARS-CoV-2 antibodies were reported qualitatively as positive or negative according to the manufacturer’s instructions. Samples with values above the cut off were reported as positive. Samples with values below the cut off were reported as negative and those equal to the cut off were re-tested.
Ethical Approval
All KTRs were provided with information about the study before obtaining their informed consent to participate in this study. The study was conducted according to the guidelines of the Declaration of Helsinki. The King Salman Medical City Institutional Review Board (KSMC), National Registration Number with: H-03-M-11) reviewed and approved this study (IRB Number: 22-010). KSMC is the official governmental ethics committee that authorized from the Ministry of Health (MOH) to issue ethical approvals on humans. It is worth noting that there are just two sources of kidney donation in Saudi Arabia. One, from living kidney donation and the second, from deceased kidney donation. Moreover, all the donated kidneys were obtained with full informed consent from the donors or next of kin, if the donors were deceased. Lastly, all donors donated their kidneys with a free well.
Statistical Analysis
Descriptive analyses were performed to describe the demographic and clinical data of KTRs. Categorical data are presented as percentages and were compared using Fisher’s exact test due to small sample sizes. Data for continuous variables were evaluated for normality using the Shapiro–Wilk test. Normally distributed data are presented as means (with standard deviations) and were compared using the t-test. Non-normally distributed data are presented as medians (with interquartile ranges) and were compared using the Mann–Whitney U (Wilcoxon rank-sum) test. Paired data, such as IgG levels, for patients’ samples obtained one month and seven months after vaccination were compared using the Wilcoxon signed-rank test. Univariate and multivariate regression analyses were performed to examine the associations between predictor (independent) variables and outcome (dependent) variables. Logistic regression analyses were performed with categorical outcome (dependent) variables, such as seropositivity, and linear regression analyses were performed with continuous outcome (dependent) variables, such as IgG levels. Spearman correlation test was used to demonstrate the associations between continuous variables. Statistical analyses were performed using Stata 15.1 (Stata Corp LLC, Texas, USA).
Results
Characteristics of Kidney Transplant Recipients After COVID-19 Vaccination
Of the 103 KTRs enrolled in this study between 15 January 2022 and 28 October 2022, 84 fulfilling the criterion of receiving at least one dose of a SARS-CoV-2 vaccine were eventually recruited. The characteristics of the KTRs were compared between those with seropositive and those with seronegative IgG levels one month after COVID-19 vaccination (Table 1). All the of patients who recruited at the current study were on haemodialysis before the transplantation. Additionally, all of them had their transplant from living donors. The seroconversion status one month after vaccination of participants receiving only one dose, two doses or three doses of a vaccine are shown in Table 1. The IgG antibody seropositivity rate (n = 66, 78.5%) was significantly higher than the seronegativity rate (n=18, 21.4; p<0.001). The KTRs’ mean age was 44.3 ± 14.7 (mean ± SD) years.
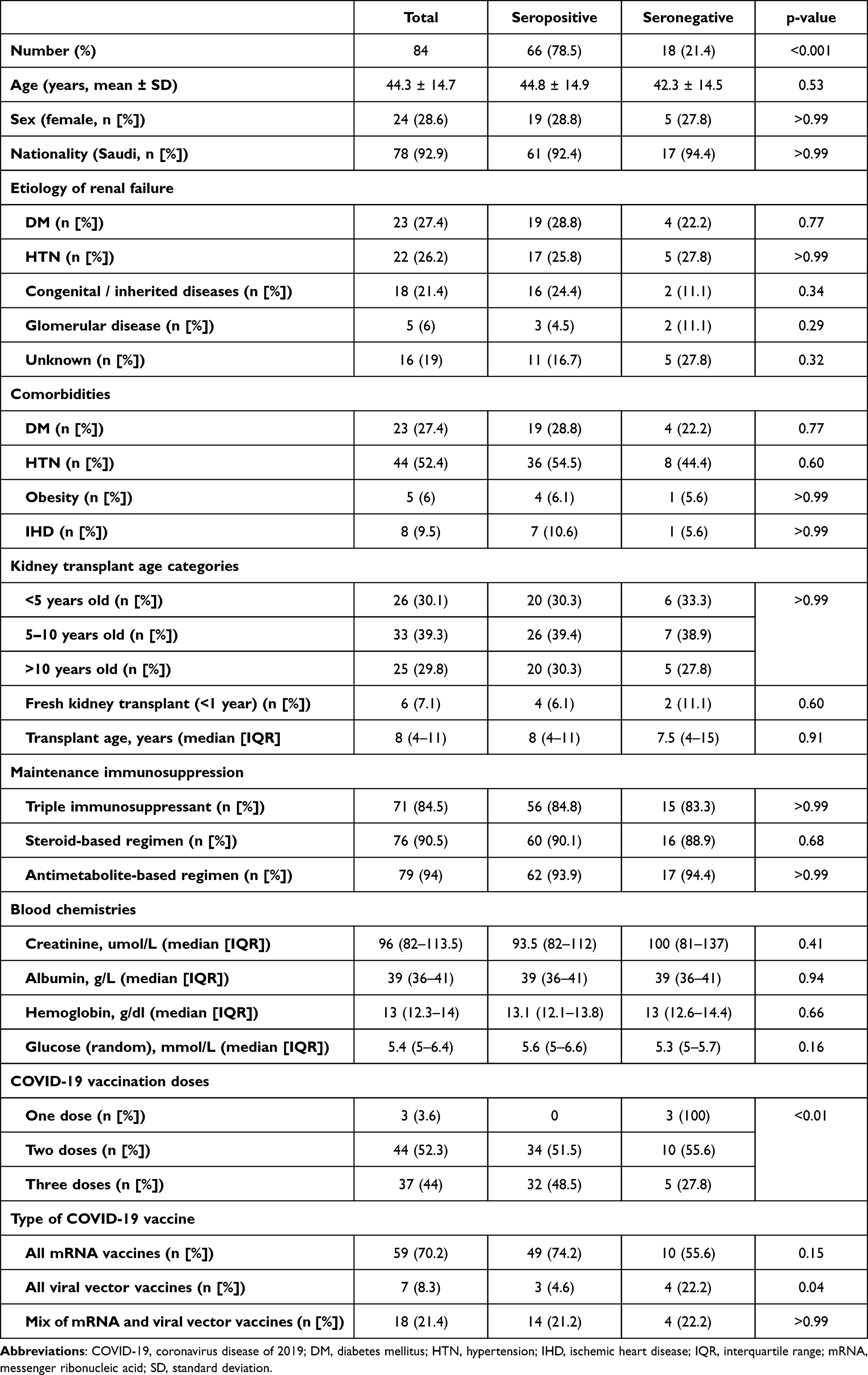 |
Table 1 Characteristics of Kidney Transplant Recipients After COVID-19 Vaccination |
Age did not differ significantly between those with seropositive and those with seronegative status (p=0.53). In addition, no significant differences were found in the aetiology of renal failure (diabetes mellitus [DM], hypertension, congenital/inherited diseases, glomerular disease, and unknown aetiology) between KTRs with positive serostatus for anti-SARS-CoV-2 IgG antibody and those with negative status. The IgG antibody serostatus (seropositive vs seronegative) of participants who received one vaccine dose (n=3, 0 vs.3), those who received two doses (n=44, 34 vs.10), and those who received three doses (n=37, 32 vs.5) differed significantly (p<0.01). Moreover, no significant differences were observed in the biochemical markers creatinine, albumin, haemoglobin, and glucose (random) between KTRs with positive serostatus and those with negative serostatus. We further investigated the associations between seropositivity status and transplant age and immunosuppressive therapies (triple immunosuppressant, steroid-based regimen, and antimetabolite-based regimen). No associations were found between anti-SARS-CoV-2 IgG seropositivity status and these factors (Table 2).
 |
Table 2 Factors Associated with Antibody Seropositivity in Kidney Transplant Recipients After COVID-19 Vaccination |
Analysis of SARS-CoV-2 IgG Antibody Levels One Month and Seven Months After COVID-19 Vaccination in KRTs and Subgroups Based on Risk Factors
To monitor the durability of anti-SARS-CoV-2 IgG antibody levels in KTRs, we further analysed seropositive individuals one month and seven months after vaccination. We excluded individuals who appeared seronegative for anti-SARS-CoV-2 IgG antibody after one month and then seroconverted to positive after seven months. Eighteen patients were seronegative for anti-SARS-CoV-2 IgG one month after vaccination and became seropositive for anti-SARS-CoV-2 IgG and IgM antibodies after seven months Table 3. It is important to note that none of the participants received any vaccination or were hospitalised between the first and second samples. Therefore, we tested the association between anti-SARS-CoV-2 IgG and IgM antibodies using paired samples after seven months (Figure 1) and found a significant positive correlation (rho=0.28, p=0.02). Consequently, those who seroconverted were most likely infected, as they appeared to be positive for SARS-CoV-2 IgM antibody.
 |
Table 3 Factors Associated with the Differences Between IgG Antibody Levels at One- and Seven-Months Post Vaccination in Patients Who Showed Seropositivity at One-Month Post Vaccination |
 |
Figure 1 Correlation between IgG and IgM antibody levels at six months after vaccination. |
Moreover, KTRs receiving three vaccine doses showed significantly decreased levels of anti-SARS-CoV-2 IgG between one month (median:3; IQR: 3–3) and seven months (median: 2.4; IQR: 1.9–2.6) after vaccination (p<0.01). Although the KRTs maintained a higher level of anti-SARS-CoV-2 IgG, they still showed a significant loss in vaccine-induced antibodies over time. Furthermore, we performed datapoints for IgG levels at one and six months post vaccination to show the decline in IgG antibody levels of each patients (Figure 2). Additionally, we found no correlation between antibody levels after one and seven months post vaccination (data not shown).
 |
Figure 2 Display of individual kidney transplant patients datapoints for IgG levels at 1- and 6-months post vaccination. Each line represents an individual patient. |
We found that in patients with hypertension as a major cause of renal failure, anti-SARS-CoV-2 IgG significantly decreased when the levels at one month and seven months after vaccination were compared (p<0.01). No significant differences were found in anti-SARS-CoV-2 IgG between the two samples for those with DM, congenital/inherited diseases, or glomerular disease, or those with an unknown aetiology.
We found a significant decrease in anti-SARS-CoV-2 IgG levels between the first and second samples in KTRs who had had a transplant for more than 10 years (p=0.02). In contrast, those with a kidney transplant of <1 year, of <5 years or of 5–10 years showed no significant decrease in anti-SARS-CoV-2 IgG levels between the first and second sample (p=0.47, p=0.08 or p=0.08, respectively). In addition, we found that all maintenance immunosuppressive regimens, ie triple immunosuppressive therapy, steroid-based regimen and antimetabolite-based regimen, were associated with a significant decrease in anti-SARS-CoV-2 IgG levels between the first and second sample (p<0.01).
Interestingly, we found that those receiving homogenous all mRNA vaccines or heterogeneous mRNA and viral vector vaccines showed significantly decreased levels of anti-SARS-CoV-2 IgG between the first (median [IQR]: 3 [2.4–3] and 3 [3–3], respectively) and second (median (IQR): 2.3 [1.7–2.6] and 2.5 [2.2–2.5], respectively) samples (p=0.02 and p=0.01, respectively), whereas those receiving homogenous all viral vector vaccines showed no significant differences in anti-SARS-CoV-2 IgG levels between the two samples (p=0.17). However, they showed a high decline in antibody levels seven months after vaccination compared to one month after vaccination. Additionally, linear regression analysis showed that there were no significant differences between IgG antibody levels at one and six-months post vaccination in patients who were seropositive at one-month post vaccination in association with the different factors (Table 4).
 |
Table 4 Linear Regression Analysis Showing the Factors Associated with the Difference Between IgG Antibody Level at One- and Six-Months Post Vaccination in Kidney Transplant Recipients Who Demonstrated Seropositivity at One-Month Post Vaccination |
Discussion
SARS-CoV-2 infection is associated with increased morbidity and mortality of solid organ transplant recipients. COVID-19 vaccines are a valuable approach to controlling the pandemic.13,14 The vaccines’ immunogenicity has been well demonstrated in the general population.15 However, recent investigations have shown a lesser immune response in transplant recipients, but the findings vary widely between studies.16,17 Thus, it is essential to perform further investigations to determine the patterns of COVID-19 vaccine immunogenicity in these patient populations.
While both viral vector-based and mRNA vaccines provoke strong anti-spike IgG antibodies that deliver more than 94% protection against severe COVID-19 in the general population, several investigations have shown that only 4–48% of KTRs have measurable anti-spike IgG antibodies after receiving two vaccine doses. Consequently, vaccinated KTRs tend to succumb to severe COVID-19 infections.18
The efficiency ratios of COVID-19 vaccines have not been investigated exclusively for KTRs in Saudi Arabia. The COVID-19 pandemic has had notable effects on health services worldwide and has interrupted nearly all clinical settings, including those involving organ donation and transplantation, with intensive-care services experiencing tremendous pressures caused by increased COVID-19 admissions.19,20
This study shows significantly higher IgG antibody seropositivity rates than seronegativity rates in participants. Our finding is similar to that of another study showing seroconversion in KTRs with increased antibody titres after a second dose of a COVID-19 vaccine.21 In contrast, other studies assessing vaccination of KTRs have shown poor immunological responses. They found a seropositivity rate of only 22% after the first and the second dose.22,23 Several factors could influence the discrepancies between studies: sample size and genetic differences between the populations studied; the sensitivity of the assays used; and other unknown factors. Therefore, we cannot generalize our findings to all KTRs who have received vaccines. Thus, multiple studies of different populations and different geographical territories are needed on a global scale to obtain conclusive data and develop guidelines for healthcare policy makers.
Our study shows significant differences between KTR vaccinees receiving different numbers of vaccine doses. Those receiving three vaccine doses showed the highest IgG antibody seropositivity rate compared to those receiving one or two doses. In addition, those receiving two doses had a higher IgG antibody seropositivity rate than those receiving only a single dose. Therefore, these results suggest a dose-dependent response. Our finding supports the results of a previous study that investigated the effect of the third dose of SARS-Cov-2 vaccine on KTRs and showed considerable improvement in vaccine-derived antibody levels. The study found that IgG antibody seropositivity increased from 4% after the first dose to 40% after the second dose and to 68% after the third dose.24 Another study of solid organ transplant recipients found that the humoral immunogenicity rate increased from 49% to 77% following the third COVID-19 vaccine dose.25 These findings reflect the critical need for booster doses in this special population to ensure protection from infection and prevention of severe complications from the disease Another study of KTRs suggests that SARS-CoV-2 mRNA vaccines are safe and are not associated with significant alloimmune threats or deterioration in allograft function.26
We narrowed our investigation to focus more on KTRs showing seroconversion and immunogenicity following vaccination. We further analysed only individuals seroconverting one month after vaccination and excluded those seroconverting seven months after vaccination. We found 18 patients seronegative for anti-SARS-CoV-2 IgG one month after vaccination but who became seropositive for anti-SARS-CoV-2 IgG and IgM antibodies after seven months. We investigated the relationship between anti-SARS-CoV-2 IgG and IgM antibodies seven months after vaccination and found a significant positive correlation between the two antibody classes. This suggests that the vaccine nonresponders testing negative after one month and then seroconverting were most likely infected before the second sample was obtained, as they appeared positive for the SARS-CoV-2 IgM antibody. Furthermore, none of the participants were hospitalised during the study. Many studies have shown that the vast majority of people infected with SARS-CoV-2 are asymptomatic.27–32 Therefore, we omitted the KTRs who might have been infected after the first sample was obtained and further investigated the other KTRs for the durability of COVID-19 vaccine immunogenicity by considering the associations between antibody titres and multiple factors. We found a significant decline in anti-SARS-CoV-2 IgG levels in the comparison of paired serum samples obtained one month and seven months after vaccination (p<0.01). Although the KRTs maintained higher anti-SARS-CoV-2 IgG levels, they still showed a significant loss of vaccine-induced antibodies over time. Our result matches those of other investigations that showed waning humoral immunity in KTRs after vaccination.33–35 Therefore, the recommendation for booster vaccine doses for KTRs is of high importance,36–38 especially since vaccination is associated with decreased risk of SARS-CoV-2 infection in KTRs.39
Many end-stage renal disease cases are attributed to hypertension, making it a major cause of renal failure.40–42 In this study, we found that KTRs with a history of hypertension showed significantly reduced levels of anti-SARS-CoV-2 IgG in the comparison of samples obtained one month and seven months after vaccination (p<0.01). Previous studies have also found that patients with high blood pressure and a history of hypertension have considerably poorer antibody titres following COVID-19 vaccination.43–45
We investigated the association between anti-SARS-CoV-2 IgG levels and kidney transplant age. We found a significant decrease in antibody levels between the first and second samples in KTRs who received a transplant more than 10 years ago. In contrast, those with a kidney transplant of <1 year, of <5 years or of 5–10 years showed no significant decrease in anti-SARS-CoV-2 IgG levels between the first and second sample; however, lower antibody levels were observed after seven months. A previous study also found that kidney transplantation duration was negatively correlated with the level of anti-SARS-CoV-2 IgG.46
Moreover, we found that maintenance immunosuppressive regimens, ie triple immunosuppressive therapy, steroid-based regimen and antimetabolite-based regimen, all led to significant decreases in anti-SARS-CoV-2 IgG levels seven months after vaccination. It is worth noting that antimetabolites have been shown to worsen B-cell proliferation and formation of plasmablasts.11 They mechanistically inhibit IL-6-mediated STAT3 signalling, a requirement for plasma cell differentiation and vital for their endurance and immunoglobulin secretion in bone marrow.12 In contrast, corticosteroids and IL-6 inhibitors, like tocilizumab, might be able to decrease mortality and prevent mechanical ventilation of patients with COVID-19. As experimental investigations have contradictory outcomes, the probability of bias is high.47
We also investigated the differences between KTRs receiving different numbers of vaccine doses. KTRs receiving three vaccine doses showed a significant decrease in anti-SARS-CoV-2 IgG after seven months; nonetheless, they retained higher levels of the antibody compared those receiving a single dose or two doses. Previous studies evaluating humoral and cellular responses to a third mRNA vaccine dose found a higher seropositivity rate compared to the rates for a single dose or double doses.48,49
Several previous studies have observed that heterologous vaccines are better at elite antibody production than homologous vaccines in both the general population and KTRs.48,50–52 Interestingly, we found that KTRs receiving homologous mRNA vaccines and heterologous mRNA and viral vector vaccines maintained significantly higher levels of anti-SARS-CoV-2 IgG when the first and second samples were compared. However, KTRs receiving homologous all viral vector vaccines showed no significant differences in the anti-SARS-CoV-2 IgG levels between the two samples. In contrast, a previous study found that heterologous vaccination schemes with a vector-based vaccine were not significantly better than the homologous mRNA-based strategy.53 However, the previous study did not compare serostatus at different time points in the same group, but its comparisons were between two different groups of vaccinees and between vector-based vaccines and mRNA-based vaccines.
To the best of our knowledge, our study is the first in Saudi Arabia to evaluate the humoral response following administration of SARS-CoV-2 vaccines in a cohort of KTRs by measuring their anti-SARS-CoV-2 IgG levels. The findings of this study indicate that the humoral response after SARS-CoV-2 vaccination is strongly inhibited in KTRs; hypertensive KTRs; those treated with triple immunosuppressants, steroid-based regimen, or antimetabolite-based regimen; those receiving mRNA or mixed mRNA and viral vector vaccines; and those with a kidney transplant vintage of >10 years.
Our study confirmed that receiving a third vaccine dose improves the humoral response of KTRs and leads to higher levels of IgG antibody, although a significant decrease is observed seven months after vaccination. Assessment of cell-mediated immunity is essential to carefully measure the elevation in vaccine immunogenicity. KTRs are recommended to get the full vaccine doses as we found that the highest antibody levels were in the group administered three doses, a significant difference from the group receiving a single dose or double doses. Moreover, KTRs under maintenance immunosuppressive therapy are advised to receive the booster vaccine due to the waning of their humoral immunity over time.
Funding
The authors extend their appreciation to, Taibah University, represented by the Deanship of Scientific Research, for funding this project RC-442/4.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924. doi:10.1016/j.ijantimicag.2020.105924
2. Petrosillo N, Viceconte G, Ergonul O, Ippolito G, Petersen E. COVID-19, SARS and MERS: are they closely related? Clin Microbiol Infect. 2020;26(6):729–734. doi:10.1016/j.cmi.2020.03.026
3. Mahallawi WH. Humoral immune responses in hospitalized COVID-19 patients. Saudi J Biol Sci. 2021;28(7):4055–4061. doi:10.1016/j.sjbs.2021.04.032
4. Zhang G, Nie S, Zhang Z, Zhang Z. Longitudinal change of severe acute respiratory syndrome coronavirus 2 antibodies in patients with coronavirus disease 2019. J Infect Dis. 2020;222(2):183–188. doi:10.1093/infdis/jiaa229
5. Guo L, Ren L, Yang S, et al. Profiling early humoral response to diagnose novel Coronavirus Disease (COVID-19). Clin Infect Dis. 2020;71(15):778–785. doi:10.1093/cid/ciaa310
6. Ravanan R, Callaghan CJ, Mumford L, et al. SARS-CoV-2 infection and early mortality of waitlisted and solid organ transplant recipients in England: a national cohort study. Am J Transplant. 2020;20(11):3008–3018. doi:10.1111/ajt.16247
7. Voora S, Adey DB. Management of kidney transplant recipients by general nephrologists: core curriculum 2019. Am J Kidney Dis. 2019;73(6):866–879. doi:10.1053/j.ajkd.2019.01.031
8. Hricik DE. Transplant immunology and immunosuppression: core curriculum 2015. Am J Kidney Dis. 2015;65(6):956–966. doi:10.1053/j.ajkd.2015.01.026
9. Meier-Kriesche HU, Steffen BJ, Hochberg AM, et al. Mycophenolate mofetil versus azathioprine therapy is associated with a significant protection against long-term renal allograft function deterioration. Transplantation. 2003;75(8):1341–1346. doi:10.1097/01.Tp.0000062833.14843.4b
10. Muntean A, Lucan M. Immunosuppression in kidney transplantation. Clujul Med. 2013;86(3):177–180.
11. Eickenberg S, Mickholz E, Jung E, Nofer JR, Pavenstadt HJ, Jacobi AM. Mycophenolic acid counteracts B cell proliferation and plasmablast formation in patients with systemic lupus erythematosus. Arthritis Res Ther. 2012;14(3):R110. doi:10.1186/ar3835
12. Jego G, Bataille R, Pellat-Deceunynck C. Interleukin-6 is a growth factor for nonmalignant human plasmablasts. Blood. 2001;97(6):1817–1822. doi:10.1182/blood.V97.6.1817
13. Rashidi-Alavijeh J, Frey A, Passenberg M, et al. Humoral response to SARS-Cov-2 vaccination in liver transplant recipients–a single-center experience. Vaccines. 2021;9(7). doi:10.3390/vaccines9070738
14. Yanis A, Haddadin Z, Spieker AJ, et al. Humoral and cellular immune responses to the SARS-CoV-2 BNT162b2 vaccine among a cohort of solid organ transplant recipients and healthy controls. Transpl Infect Dis. 2022;24(1):e13772. doi:10.1111/tid.13772
15. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA covid-19 vaccine. N Engl J Med. 2020;383(27):2603–2615. doi:10.1056/NEJMoa2034577
16. Boyarsky BJ, Werbel WA, Avery RK, et al. Antibody response to 2-dose SARS-CoV-2 mRNA vaccine series in solid organ transplant recipients. JAMA. 2021;325(21):2204–2206. doi:10.1001/jama.2021.7489
17. Georgery H, Devresse A, Yombi JC, et al. Disappointing immunization rate after 2 doses of the BNT162b2 vaccine in a Belgian cohort of kidney transplant recipients. Transplantation. 2021;105(12):e283–e284. doi:10.1097/tp.0000000000003861
18. Benotmane I, Gautier-Vargas G, Gallais F, et al. Strong antibody response after a first dose of a SARS-CoV-2 mRNA-based vaccine in kidney transplant recipients with a previous history of COVID-19. Am J Transplant. 2021;21(11):3808–3810. doi:10.1111/ajt.16764
19. Goff RR, Wilk AR, Toll AE, McBride MA, Klassen DK. Navigating the COVID-19 pandemic: initial impacts and responses of the organ procurement and transplantation network in the United States. Am J Transplant. 2021;21(6):2100–2112. doi:10.1111/ajt.16411
20. Qu Z, Oedingen C, Bartling T, Schrem H, Krauth C. Organ procurement and transplantation in Germany during the COVID-19 pandemic. Lancet. 2020;396(10260):1395. doi:10.1016/S0140-6736(20)32213-3
21. Benotmane I, Gautier-Vargas G, Cognard N, et al. Low immunization rates among kidney transplant recipients who received 2 doses of the mRNA-1273 SARS-CoV-2 vaccine. Kidney Int. 2021;99(6):1498–1500. doi:10.1016/j.kint.2021.04.005
22. Boyarsky BJ, Werbel WA, Avery RK, et al. Immunogenicity of a single dose of SARS-CoV-2 messenger RNA vaccine in solid organ transplant recipients. JAMA. 2021;325(17):1784–1786. doi:10.1001/jama.2021.4385
23. Korth J, Jahn M, Dorsch O, et al. Impaired humoral response in renal transplant recipients to SARS-CoV-2 vaccination with BNT162b2 (Pfizer-BioNTech). Viruses. 2021;13(5):756. doi:10.3390/v13050756
24. Del Bello A, Abravanel F, Marion O, et al. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am J Transplant. 2021. doi:10.1111/ajt.16775
25. Balsby D, Nilsson AC, Petersen I, et al. Humoral immune response following a third SARS-CoV-2 mRNA vaccine dose in solid organ transplant recipients compared with matched controls. Front Immunol. 2022;13:1039245. doi:10.3389/fimmu.2022.1039245
26. Al Jurdi A, Gassen RB, Borges TJ, et al. Non-invasive monitoring for rejection in kidney transplant recipients after SARS-CoV-2 mRNA vaccination. Original research. Front Immunol. 2022;2022:13. doi:10.3389/fimmu.2022.838985
27. Mahallawi WH, Al-Zalabani AH. The seroprevalence of SARS-CoV-2 IgG antibodies among asymptomatic blood donors in Saudi Arabia. Saudi J Biol Sci. 2021;28(3):1697–1701. doi:10.1016/j.sjbs.2020.12.009
28. Mahallawi WH, Ibrahim NA, Aljohani AS, et al. Assessment of SARS-CoV-2 anti-spike IgG antibody in women and children in Madinah, Saudi Arabia: a single-center study. Int J Environ Res Public Health. 2021;18(19):9971. doi:10.3390/ijerph18199971
29. Ma Q, Liu J, Liu Q, et al. Global percentage of asymptomatic SARS-CoV-2 infections among the tested population and individuals with confirmed COVID-19 diagnosis: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(12):e2137257. doi:10.1001/jamanetworkopen.2021.37257
30. Almadhi MA, Abdulrahman A, Sharaf SA, et al. The high prevalence of asymptomatic SARS-CoV-2 infection reveals the silent spread of COVID-19. Int J Infect Dis. 2021;105:656–661. doi:10.1016/j.ijid.2021.02.100
31. Syangtan G, Bista S, Dawadi P, et al. Asymptomatic SARS-CoV-2 carriers: a systematic review and meta-analysis. Systematic review. Front Public Health. 2021;2021:8. doi:10.3389/fpubh.2020.587374
32. Mahallawi W, Ibrahim N. Unexpected detection of anti-SARS-CoV-2 antibodies before the declaration of the COVID-19 pandemic. Front Med. 2022;9:923715. doi:10.3389/fmed.2022.923715
33. Kühn T, Speer C, Morath C, et al. Immune response to COVID-19 mRNA vaccination in previous nonresponder kidney transplant recipients after short-term withdrawal of mycophenolic acid 1 and 3 months after an additional vaccine dose. Transplantation. 2023;107(5):1139–1150. doi:10.1097/tp.0000000000004516
34. Sattler A, Schrezenmeier E, Weber UA, et al. Impaired humoral and cellular immunity after SARS-CoV-2 BNT162b2 (tozinameran) prime-boost vaccination in kidney transplant recipients. J Clin Invest. 2021;131(14). doi:10.1172/jci150175
35. Grupper A, Rabinowich L, Schwartz D, et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am J Transplant. 2021;21(8):2719–2726. doi:10.1111/ajt.16615
36. Kantauskaite M, Müller L, Kolb T, et al. Intensity of mycophenolate mofetil treatment is associated with an impaired immune response to SARS-CoV-2 vaccination in kidney transplant recipients. Am J Transplant. 2022;22(2):634–639. doi:10.1111/ajt.16851
37. Benotmane I, Bruel T, Planas D, Fafi-Kremer S, Schwartz O, Caillard S. A fourth dose of the mRNA-1273 SARS-CoV-2 vaccine improves serum neutralization against the delta variant in kidney transplant recipients. Kidney Int. 2022;101(5):1073–1076. doi:10.1016/j.kint.2022.02.011
38. Osmanodja B, Ronicke S, Budde K, et al. Serological response to three, four and five doses of SARS-CoV-2 vaccine in kidney transplant recipients. J Clin Med. 2022;11(9):2565. doi:10.3390/jcm11092565
39. Zahradka I, Petr V, Modos I, Magicova M, Dusek L, Viklicky O. Association Between SARS-CoV-2 messenger RNA vaccines and lower infection rates in kidney transplant recipients: a registry-based report. Ann Intern Med. 2022;175(7):961–968. doi:10.7326/m21-2973
40. Salem MM. Pathophysiology of hypertension in renal failure. Semin Nephrol. 2002;22(1):17–26. doi:10.1053/snep.2002.28640
41. Hsu C-Y, McCulloch CE, Darbinian J, Go AS, Iribarren C. Elevated blood pressure and risk of end-stage renal disease in subjects without baseline kidney disease. Arch Intern Med. 2005;165(8):923–928. doi:10.1001/archinte.165.8.923
42. Mahallawi WH, Ibrahim NA, Mumena WA. Effectiveness of COVID-19 vaccines in patients under maintenance hemodialysis. Risk Manag Healthc Policy. 2021;14:5081–5088. doi:10.2147/rmhp.S345686
43. Soegiarto G, Wulandari L, Purnomosari D, et al. Hypertension is associated with antibody response and breakthrough infection in health care workers following vaccination with inactivated SARS-CoV-2. Vaccine. 2022;40(30):4046–4056. doi:10.1016/j.vaccine.2022.05.059
44. Lustig Y, Sapir E, Regev-Yochay G, et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: a prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir Med. 2021;9(9):999–1009. doi:10.1016/s2213-2600(21)00220-4
45. Watanabe M, Balena A, Tuccinardi D, et al. Central obesity, smoking habit, and hypertension are associated with lower antibody titres in response to COVID-19 mRNA vaccine. Diabetes Metab Res Rev. 2022;38(1):e3465. doi:10.1002/dmrr.3465
46. Hamaya T, Hatakeyama S, Yoneyama T, et al. Seroprevalence of SARS-CoV-2 spike IgG antibodies after the second BNT162b2 mRNA vaccine in Japanese kidney transplant recipients. Sci Rep. 2022;12(1):5876. doi:10.1038/s41598-022-09897-0
47. Schoot TS, Kerckhoffs APM, Hilbrands LB, van Marum RJ. Immunosuppressive drugs and COVID-19: a review. Front Pharmacol. 2020;11:1333. doi:10.3389/fphar.2020.01333
48. Yahav D, Rahamimov R, Mashraki T, et al. Immune response to third dose BNT162b2 COVID-19 vaccine among kidney transplant recipients-a prospective study. Transpl Int. 2022;35:10204. doi:10.3389/ti.2022.10204
49. Magicova M, Zahradka I, Fialova M, et al. Determinants of immune response to anti–SARS-CoV-2 mRNA vaccines in kidney transplant recipients: a prospective cohort study. Transplantation. 2022;106(4):842–852. doi:10.1097/tp.0000000000004044
50. Cheng H, Peng Z, Si S, et al. Immunogenicity and safety of homologous and heterologous prime-boost immunization with COVID-19 vaccine: systematic review and meta-analysis. Vaccines. 2022;10(5):798. doi:10.3390/vaccines10050798
51. Reiter R, Von Blanckenburg P, Mutters R, Thiemer J, Geßner R, Seifart U. Influence of a heterologous (ChAdOx1-nCoV-19/BNT162b2) or homologous (BNT162b2/BNT162b2) vaccination regimen on the antibody and T cell response to a third vaccination with BNT162b2. Vaccines. 2022;10(5):788. doi:10.3390/vaccines10050788
52. Thotsiri S, Sittiudomsuk R, Sutharattanapong N, Kantachuvesiri S, Wiwattanathum P. The effect of a booster dose mRNA vaccine on COVID-19 infection in kidney transplant recipients after inactivated or viral vector vaccine immunization. Vaccines. 2022;10(10):1690. doi:10.3390/vaccines10101690
53. Reindl-Schwaighofer R, Heinzel A, Mayrdorfer M, et al. Comparison of SARS-CoV-2 antibody response 4 weeks after homologous vs heterologous third vaccine dose in kidney transplant recipients: a randomized clinical trial. JAMA Intern Med. 2022;182(2):165–171. doi:10.1001/jamainternmed.2021.7372
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.