Back to Journals » Infection and Drug Resistance » Volume 11
Daptomycin versus teicoplanin for bloodstream infection due to methicillin-resistant Staphylococcus aureus with a high teicoplanin minimal inhibitory concentration ≥1.5 mg/L: a propensity score-based analysis
Authors Tsai CY, Lee CH, Chen IL
Received 18 August 2018
Accepted for publication 21 September 2018
Published 26 October 2018 Volume 2018:11 Pages 2011—2020
DOI https://doi.org/10.2147/IDR.S184411
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Ching-Yen Tsai,1 Chen-Hsiang Lee,1,2 I-Ling Chen3
1Division of Infectious Diseases, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 2College of Medicine, Chang Gung University College of Medicine, Kaohsiung, Taiwan; 3Department of Pharmacy, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
Background: Recent reports have described decreased effectiveness of teicoplanin in the treatment of bacteremia due to methicillin-resistant Staphylococcus aureus (MRSA) with teicoplanin minimal inhibitory concentration (MIC) ≥1.5 mg/L. Consensus guidelines recommend considering use of alternative agents for MRSA infections involving a higher teicoplanin MIC, despite of limited data to support this recommendation.
Patients and methods: To compare the clinical outcome among patients with bacteremia due to MRSA with teicoplanin MIC ≥1.5 mg/L, we included patients who received high-dose daptomycin (≥8 mg/kg/day) and those who received standard-dose (6 mg/kg/day) or high-dose (6 mg/kg/12 hours) maintenance teicoplanin. The primary endpoint was a favorable outcome, defined as the resolution of clinical signs and symptoms and a negative culture report at the end of therapy. Adjusted analyses were performed by multivariate analysis and propensity score-based matching.
Results: Of 142 patients eligible for inclusion, 28 (19.7%) were treated with high-dose daptomycin, 27 (19.0%) with high-dose teicoplanin, and 87 (61.3%) with standard-dose teicoplanin. In multivariate regression analysis, Pittsburgh bacteremia score ≥4 (OR, 5.3; 95% CI, 1.9–14.5) was independently associated with an unfavorable outcome. After propensity-score matching with age and Pittsburgh bacteremia score ≥4, patients on high-dose daptomycin were more likely to have favorable outcomes than those on standard-dose teicoplanin (74.1% vs 42.6%; P=0.02). However, there was no significant difference in terms of favorable outcomes (P=0.12) between patients receiving high-dose daptomycin and those receiving high-dose teicoplanin after the same propensity-score matching.
Conclusion: Treatment with high-dose daptomycin resulted in significantly better outcomes than with standard-dose teicoplanin in the treatment of MRSA bacteremia with teicoplanin MIC ≥1.5 mg/L. However, the clinical outcome of the patients receiving high-dose teicoplanin was similar to that of the patients receiving high-dose daptomycin.
Keywords: gram-positive bacteria, antimicrobial susceptibility, pharmacodynamics, glycopeptide, lipopeptide
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) is an important etiology of severe infectious syndromes in the community and hospital.1 MRSA bloodstream infection (BSI) has been found to be associated with a higher risk of mortality, prolonged hospital stays, and high costs than BSI due to other pathogens.2,3 Teicoplanin, a glycopeptide, is one of the treatment options for MRSA infection. It was widely reported to be efficient with fewer adverse effects when comparable with vancomycin for MRSA infection.4 One retrospective study found out that the minimal inhibitory concentrations (MICs) ≥1.5 mg/L of teicoplanin was associated with an unfavorable outcome in patients receiving teicoplanin for MRSA bacteremia.5 The question remains as to whether the poorer outcomes with higher teicoplanin MIC are due to ineffective treatment or other microbiological characteristics of the organism. Daptomycin, a lipopeptide class antibiotic that disrupts cell membrane function via calcium-dependent binding, has bactericidal activity in a concentration-dependent fashion,6 and differs from the glycopeptides in that it exerts high bactericidal activity against both methicillin-susceptible and methicillin-resistant Staphylococcus strains.1 Several treatment guidelines include high-dose daptomycin (8–10 mg/kg/day) as a therapeutic option for difficult-to-treat infections.6–8 Furthermore, Kullar et al revealed that high-dose daptomycin, defined as ≥8 mg/kg/day, was an effective and safe antimicrobial in patients with infective endocarditis.9 As a result, Infectious Diseases Society of America (IDSA) guidelines for the treatment of MRSA BSI recommend consideration of high-dose daptomycin in patients with persistent MRSA bacteremia after vancomycin failure.6
According to IDSA guidelines, for isolates with vancomycin MIC >1 mg/L (susceptible according to Clinical and Laboratory Standards Institute [CLSI] breakpoints),10 an alternative to vancomycin should be used.6 An earlier study of the factors associated with clinical failure in patients with MRSA bacteremia demonstrated the relationship between vancomycin MIC and clinical treatment failure in univariate analysis.11 A multicenter prospective study of MRSA bacteremia reported that the success rate of treatment with vancomycin was 55.6% with vancomycin MICs ≤0.5 mg/L, whereas it was only 9.5% in cases with MICs of 1–2 mg/L.12 These results were mainly supported by the premise that there is presumably less likelihood of achieving target vancomycin pharmacodynamic parameters with higher vancomycin MIC.
Recently, clinical data supporting that daptomycin was associated with a better outcome compared with vancomycin in the treatment of BSIs due to MRSA with higher vancomycin MICs are emerging.13,14 Our previous data highlighted the importance of high-dose teicoplanin (6 mg/kg/12 hours) maintenance treatment, especially for severe MRSA infections.15 We also found that high-dose teicoplanin maintenance treatment was associated with more favorable outcomes than standard-dose teicoplanin (6 mg/kg/day) maintenance treatment in patients with MRSA bacteremia, regardless of the teicoplanin MIC.16 Therefore, the question of whether daptomycin, rather than high-dose maintenance teicoplanin therapy, confers any benefit in cases of MRSA BSI with high teicoplanin MIC remains unanswered.
Randomized clinical trials of daptomycin vs teicoplanin for MRSA BSI due to strains with high teicoplanin MIC are lacking and the findings of previous reports are limited because of differences in the severity of bacteremia and demographics between patients receiving teicoplanin therapy and those receiving daptomycin therapy. In this propensity-score matched, retrospective study, we aimed to evaluate the effectiveness of standard-dose and high-dose teicoplanin vs daptomycin in the treatment of bacteremia due to MRSA isolates with high teicoplanin MIC (≥1.5 mg/L) but still within the range of susceptibility designed by EUCAST (≤2 mg/L).
Patients and methods
Study design
Patients with MRSA BSI, who were admitted to a 2,700-bed tertiary care hospital in southern Taiwan over a 6-year period (2012–2017), were eligible for inclusion. Furthermore, patients were eligible if they 1) had an index MRSA bloodstream isolate with teicoplanin MIC of 1.5 or 2 mg/L, as determined by Etest® (bio-Merieux™, Marcy l’Etoile, France); 2) received either teicoplanin or daptomycin within 48 hours of the onset of infection; 3) received treatment with teicoplanin or daptomycin for >72 hours; and 4) were aged ≥18 years. If the patients experienced more than one episode of MRSA bacteremia, only the first episode was included. Patients with a concurrent infection by microbe(s) other than MRSA or those receiving adjunctive antibiotics for MRSA bacteremia were excluded from the study. Through the antimicrobial stewardship program in the hospital,17 teicoplanin or daptomycin was prescribed at the discretion of the attending physician and all these prescriptions were approved by specialists of infectious diseases. Clinical data were retrieved from the medical records using a standardized case report form.
Adequate teicoplanin therapy was defined as a loading dose of 6 mg/kg administered thrice 12 hours apart,18 followed by a maintenance dose of 6 mg/kg/12 hours (high-dose teicoplanin group) or 6 mg/kg/24 hours (standard-dose teicoplanin group) or the adjusted equivalent doses for patients with impaired renal function according to the package insert (Sanofi-Aventis™, Paris, France). The dose of daptomycin was ≥8 mg/kg/24 hours (high-dose daptomycin group) or the adjusted equivalents for renal insufficiency. The patients were made anonymous to maintain confidentiality of the data. The Institutional Review Board of the CGMH approved the study (No. 201601482B0) and waived the need for patient consent because of the retrospective nature of the study.
Microbiological methods
MRSA was defined as an isolate of S. aureus subjected to susceptibility testing using the disk diffusion method, in which cefoxitin (30 µg) produced an inhibition zone of ≤21 mm according to CLSI recommendation.10 The MICs of teicoplanin and daptomycin were determined using Etest teicoplanin and daptomycin strips (AB Biodisk™, Solna, Sweden), separately.
Definitions
The severity of the underlying medical illness was stratified according to the McCabe score and categorized as rapidly fatal, ultimately fatal, or nonfatal.19 The clinical severity of the illness at the time of sampling blood for cultures was stratified using the modified Pittsburgh bacteremia score, and critical illness was defined as Pittsburgh bacteremia score ≥4 points.20 Sources of bacteremia were identified according to the clinical, microbiologic, imaging findings, and the judgment of the physicians. Bacteremia in a patient with no apparent focus of infection other than blood was defined as bacteremia with no identified focus of infection. Catheter-related bacteremia was defined if the inserted catheter had been in place for more than 72 hours and culture of the clipped distant 5-cm tip of the removed catheter by rolling it on a culture medium yielded more than 15 colonies of MRSA; or the culture of purulent discharge from the catheter exit grew MRSA.21 Bone and joint infection was defined based on clinical manifestations with consistent histopathological and/or radiographical findings.22 Infective endocarditis was defined as histopathology was found in the valvular specimens obtained during surgery, or valvular vegetations were sonographically revealed regardless of an embolic phenomenon.23 Soft tissue infection was considered when MRSA grew from the specimen sampled from the affected site.22 Intra-abdominal infection was defined as the infection that extended into the peritoneal space was associated with abscess formation or peritonitis, and growth of MRSA on cultures of the peritoneal fluid, bile, or intra-abdominal abscess.24 Urinary tract infection was considered when MRSA, as the only identified pathogen, grew more than 105 colony-forming units per milliliter in the urine culture.22 Pneumonia referred to the presence of clinical symptoms/signs of lower respiratory tract infection, accompanied with consistent radiographic findings.22 Adequate source control was defined as timely 1) percutaneous or surgical intervention to drain the collection(s) of infected fluid, debride the infected tissues, and control ongoing enteric or other drainage-producing intra-abdominal source of infection; 2) removal of central venous catheter for catheter-related bacteremia; and 3) removal of urinary catheter for BSI secondary to catheter-related urinary tract infection. Subjects were classified into three groups at the time of the switch to daptomycin: no improvement during current therapy, adverse event due to current therapy, or undetermined reason.
Early clinical response was assessed on day 7 after initiating anti-MRSA therapy, while the evaluation upon completion of teicoplanin or daptomycin therapy was referred as the final clinical response. Patients were evaluated on day 7 for the presence of septic shock, persistent bacteremia, persistent fever, or persistent leukocytosis, and favorable and unfavorable early clinical responses referred to the absence and presence of any of these findings, respectively.6 The primary endpoint was a favorable outcome, which was defined as the resolution of clinical signs and symptoms and a negative culture report at the end of therapy. Clinical progression or relapse of sepsis that had previously improved clinically, mortality, and/or culture of blood sampled at the end of daptomycin or teicoplanin treatment that remained positive for MRSA were defined as “unfavorable” outcomes. Additionally, 30-day overall mortality was defined as all causes of mortality occurring within 30 days of hospitalization after the onset of MRSA BSI.
Statistical analysis
In univariate analysis, Student’s t-test or Mann–Whitney U-test was used for comparisons between continuous variables, whereas the chi-squared test or Fisher’s exact test was used for comparisons between dichotomous variables. Variables with a P-value <0.1 in univariate analyses were incorporated into a stepwise, backward logistic regression model to determine independent variables associated with favorable outcomes at the end of the initial teicoplanin or daptomycin treatment. Hosmer–Lemeshow goodness-of-fit tests were performed to evaluate the predictive performance of the logistic regression model. The propensity score was calculated using independent predictors of favorable outcomes at the end of initial teicoplanin or daptomycin treatment, which were assessed using a multivariable logistic regression model. The patients who received high-dose daptomycin were matched on a 1:1 and 1:2 basis with those treated with high-dose teicoplanin and standard-dose teicoplanin patients, respectively, and the matching by the closest total scores was performed manually based on a tolerance interval approach. As described previously,25 matching tolerance is a propensity score difference of 0.2: a patient in the high-dose daptomycin treatment group was matched with a patient in the high-dose teicoplanin or standard-dose teicoplanin group only when the estimated probability of the high-dose daptomycin group was within 20% of the estimated probability of his or her counterpart who was treated with high-dose teicoplanin or standard-dose teicoplanin. Statistical analyses were performed using SPSS® version 21 (IMB Inc.™, Armonk, NY, USA). All tests were two tailed and variables with a P-value <0.05 were regarded as statistically significant.
Results
A total of 184 adult patients with MRSA BSI with high teicoplanin MIC (≥1.5 mg/L) were identified over the study period, of which 42 who received nonadequate dosage or treatment more than 48 hours after the onset of infection with teicoplanin, daptomycin, and other treatments except teicoplanin or daptomycin for MRSA bacteremia were excluded (Figure 1). Of the 142 patients included, 28 (19.7%) were treated with high-dose daptomycin, 27 (19.0%) with high-dose teicoplanin, and 87 (61.3%) with standard-dose teicoplanin. The rate of adequate control of the source of infection in patients on standard-dose teicoplanin, high-dose teicoplanin, and high-dose daptomycin was 77.2%, 84.2%, and 76.2%, respectively. The rate of favorable outcome at the end of the initial therapy was 29.9% in the standard-dose teicoplanin group, 62.9% in the high-dose teicoplanin group, and 71.4% in the high-dose daptomycin group (Figure 1). Of the 87 patients who received initial standard-dose teicoplanin, 32 (36.8%) received sequential therapy with high-dose daptomycin. The median time to switching from teicoplanin to daptomycin was 6 days (interquartile range, 4–10 days). The reason for switching was clinical failure in 24 patients (75.0%), physician reference in 4 (12.5%), adverse events in 2 (6.3%), and unspecified reasons in 2 (6.3%). The 30-day overall mortality rate in patients on continuous standard-dose teicoplanin and that in those who were subsequently switched to daptomycin treatment was 36.6% and 21.9%, respectively (P=0.21, Fisher’s exact test). No patient in the high-dose teicoplanin or high-dose daptomycin group needed to switch to daptomycin or teicoplanin, respectively.
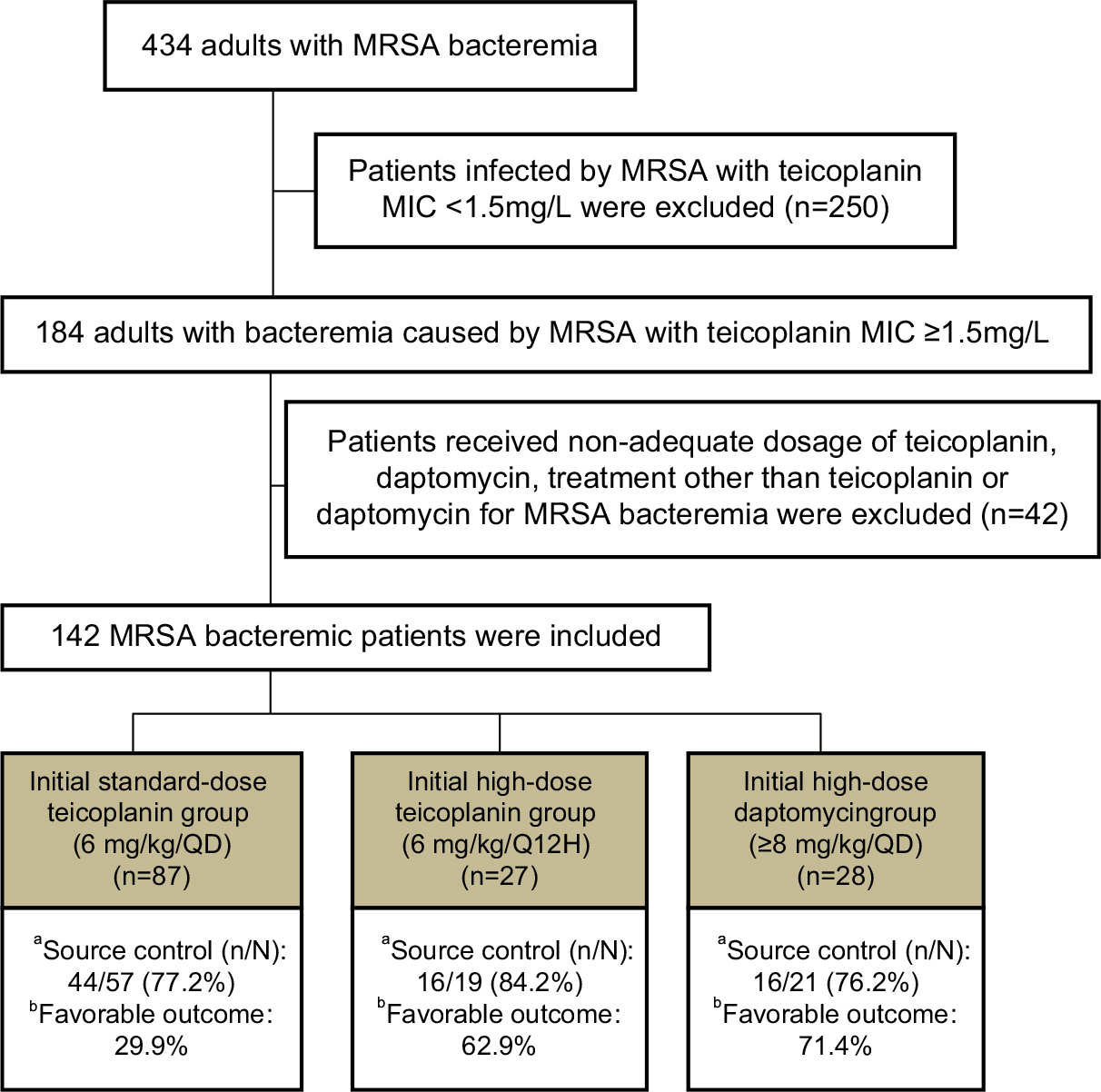 | Figure 1 Flowchart of the study. Notes: aSurgical intervention, drainage, central venous catheter removal, and urinary catheter removal were defined as source control. Patients with pneumonia or primary bacteremia were excluded. n: adequate and timely removal or debridement of the source of bacteremia, N: source of bacteremia needed to be removed or debrided. bEvaluation at the completion of initial teicoplanin or daptomycin therapy. |
Univariate analyses were used to compare the groups with favorable outcomes and those with unfavorable outcomes at the end of the initial teicoplanin or daptomycin treatment. The variables for comparison were clinical characteristics, demographics, source of bacteremia, major comorbidities, severities of the comorbidities, BSI severity at onset, adequate infection control, and initial treatment group (Table 1). We found that critical illness (Pittsburgh bacteremia score ≥4) at BSI onset and initial treatment with standard-dose teicoplanin were negatively associated with outcomes. Additionally, initial treatment with high-dose daptomycin was significantly positively associated with favorable outcomes. In subsequent multivariate regression analysis, Pittsburgh bacteremia score ≥4 (OR, 5.3; 95%CI, 1.9–14.5; P=0.01) was independently associated with unfavorable outcomes at the end of the initial teicoplanin or daptomycin treatment (Table 1). The P-values for the Hosmer–Lemeshow goodness-of-fit tests were >0.05. Hence, there is no significant evidence of lack of fit for any of the final models.
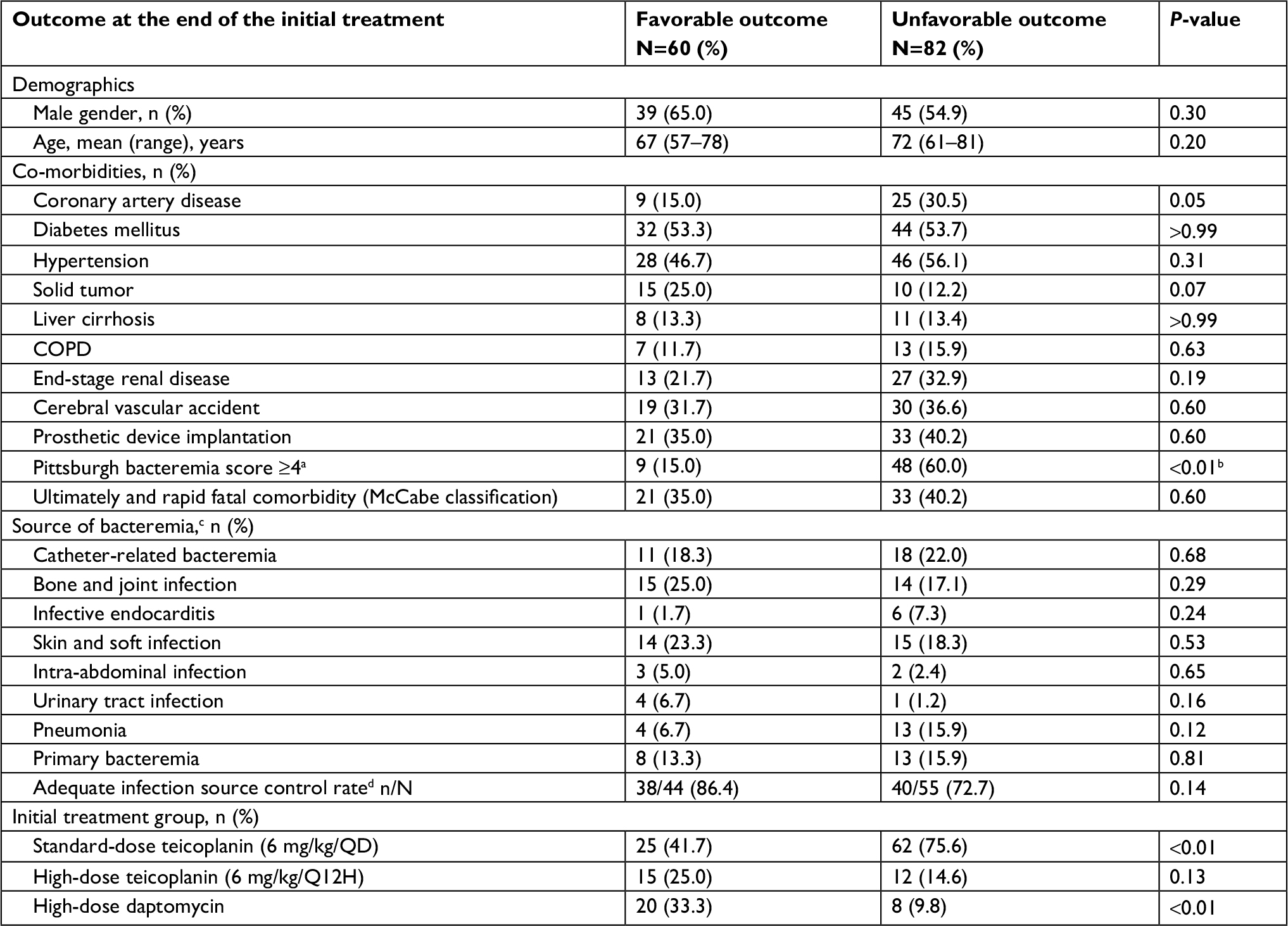 | Table 1 Risk factors for favorable outcome at the end of initial teicoplanin or daptomycin treatment in 142 adult patients with MRSA bacteremia with teicoplanin MIC ≥1.5 mg/L Notes: aAt the time of sampling blood for culture. bIn multivariate analysis, Pittsburgh bacteremia score ≥4 (OR, 5.3; 95%CI, 1.9–14.5; P=0.01) was a risk factor for unfavorable outcome at the end of the initial teicoplanin or daptomycin treatment in patients with MRSA bacteremia with teicoplanin MIC ≥1.5 mg/L. cPatients might have had more than one source of bacteremia. dSurgical intervention, drainage, central venous catheter removal, and urinary catheter removal were defined as source control. Patients with pneumonia or primary bacteremia were excluded. n: adequate and timely removal or debridement of the source of bacteremia, N: source of bacteremia that needed to be removed or debrided. Abbreviations: MIC, minimal inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus. |
The patients in the standard-dose teicoplanin group and high-dose daptomycin group were matched in a ratio of 2:1 with the closest propensity scores on the basis of age and critical illness (Pittsburgh bacteremia score ≥4; Table 2). After propensity-score matching, patients in the high-dose daptomycin group had better short-term favorable outcomes (66.7% vs 38.9%; P=0.03) and favorable outcomes at end of therapy (74.1% vs 42.6%; P=0.02) compared with those in the standard-dose teicoplanin group. Patients in the high-dose teicoplanin group and high-dose daptomycin group were matched in a ratio of 1:1 with the closest propensity scores on the basis of age and critical illness (Pittsburgh bacteremia score ≥4; Table 3). However, there was no significant difference in terms of favorable outcomes in the short term (P=0.37) and at the end of therapy (P=0.12) between these two groups.
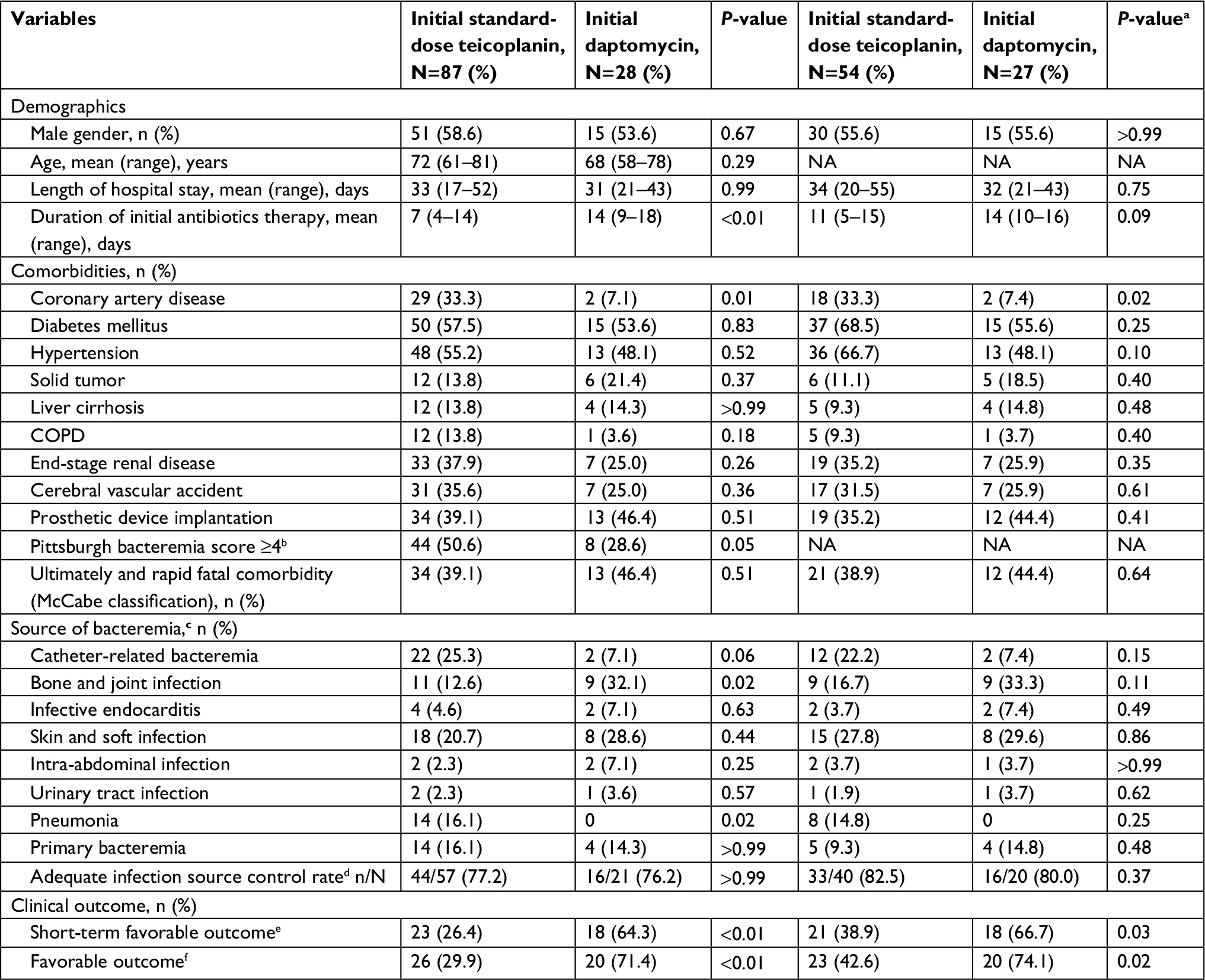 | Table 2 Clinical characteristics, responses, and outcomes in adults with MRSA bacteremia with teicoplanin MIC ≥1.5 mg/L and treated with standard-dose teicoplanin or daptomycin Notes: a2:1 Match with propensity score (age and Pittsburgh bacteremia score ≥4). bAt the time of sampling blood for culture. cPatients might have had more than one source of bacteremia. dSurgical intervention, drainage, central venous catheter removal, and urinary catheter removal were defined as source control. Patients with pneumonia or primary bacteremia were excluded. n: adequate and timely removal or debridement of the source of bacteremia, N: source of bacteremia needed to be removed or debrided. eAssessment on day 7 after starting the initial teicoplanin or daptomycin therapy. fEvaluation at the time of completion of the initial teicoplanin or daptomycin therapy. Abbreviations: MIC, minimal inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; NA, not applicable. |
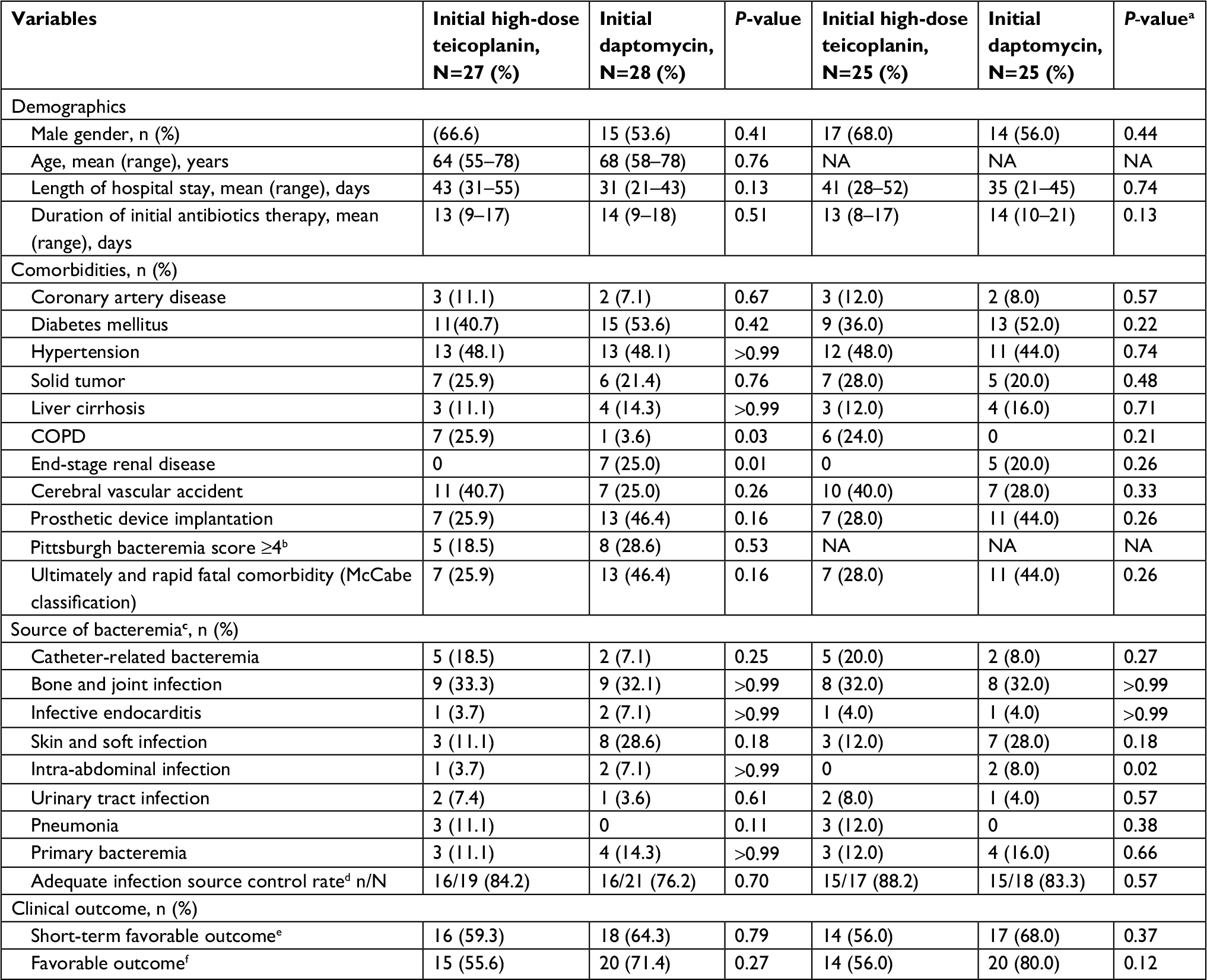 | Table 3 Clinical characteristics, responses, and outcomes in adults with MRSA bacteremia with teicoplanin MIC ≥1.5 mg/L and treated with high-dose teicoplanin or daptomycin Notes: a1:1 Match with propensity score (age and Pittsburgh bacteremia score ≥4). bAt the time of sampling blood for culture. cPatients might had more than one source of bacteremia. dSurgical intervention, drainage, central venous catheter removal, and urinary catheter removal were defined as source control. Patients with pneumonia or primary bacteremia were excluded. n: adequate and timely removal or debridement of the source of bacteremia, N: source of bacteremia needed to be removed or debrided. eAssessment on day 7 after starting the initial teicoplanin or daptomycin therapy. fEvaluation at the time of completion of the initial teicoplanin or daptomycin therapy. Abbreviations: MIC, minimal inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; NA, not applicable. |
The distribution of daptomycin MICs among the 28 patients in the high-dose daptomycin treatment group is shown in Table 4. A total of 21 (75.0%) patients were infected by MRSA strains with daptomycin MIC ≤0.25 mg/L. The favorable outcomes were found in patients who were infected by MRSA strains with daptomycin MIC ≤0.25 mg/L than those who were infected by MRSA strains with daptomycin MIC >0.25 mg/L (81.9% vs 42.9%); however, the difference was not statistically significant (P=0.14, Table 4).
 | Table 4 The outcomes at the end of the initial daptomycin therapy at different distributions of daptomycin MIC Notes: aSurgical intervention, drainage, central venous catheter removal, and urinary catheter removal were defined as source control. Patients with pneumonia or primary bacteremia were excluded. n: adequate and timely removal of central catheter, urinary catheter, or debridement of the source of bacteremia, N: source of bacteremia needed to be removed or debrided. bEvaluation at the time of completion of the initial daptomycin therapy. Abbreviation: MIC, minimal inhibitory concentration. |
Discussion
Chang et al described that MRSA bacteremia with MIC of teicoplanin ≥1.5 mg/L was a predictor of unfavorable outcomes in patients receiving teicoplanin treatment.5 In agreement with their findings,5 our previous study observed a suboptimal clinical outcome when standard-dose teicoplanin was administered as a maintenance therapy for bacteremia caused by MRSA with teicoplanin MICs ≥1.5 mg/L.16 Furthermore, patients on high-dose teicoplanin maintenance treatment had favorable outcomes in the case of MRSA bacteremia, regardless of the teicoplanin MIC values.16 These findings highlighted that a higher dosage of this antibiotic was required to reach an appropriate pharmacokinetic target to optimize its activity against MRSA, if teicoplanin MICs were ≥1.5 mg/L. Additionally, several studies reported that daptomycin might be used at higher doses for difficult-to-treat infections.26,27 Therefore, in this study, we included adults with bacteremia due to MRSA strains with teicoplanin MICs ≥1.5 mg/L, who had received high/standard-dose maintenance teicoplanin or high-dose daptomycin for further evaluation.
To the best of our knowledge, the current study is the first study to compare the clinical outcomes in these patients. Moreover, propensity-score matching analyses are especially useful for retrospective observational studies, which might overcome the differences in the distribution of baseline covariates between treatment groups because they provide a natural weighing scheme that yields unbiased estimates of the impact of the treatment.28 The current analyses controlled for the baseline factors linked to favorable outcomes at the end of initial teicoplanin or daptomycin therapy between patients in the high-dose teicoplanin, standard-dose teicoplanin, and high-dose daptomycin groups. Our results revealed that treatment with high-dose daptomycin resulted in significantly improved outcomes than did treatment with standard-dose teicoplanin (Table 2). However, the clinical outcome of the patients receiving high-dose teicoplanin was similar to that of the patients receiving high-dose daptomycin (Table 3). In this study, the therapy was changed to daptomycin in most patients of the standard-dose teicoplanin group because their clinical status was worsening or not improving on the current therapy. This delay in the initiation of daptomycin was not associated with better outcomes. The results suggest that switching the treatment from standard-dose teicoplanin to daptomycin, particularly late in the course of infection, may not lead to more favorable outcomes in comparison with the continuation of standard-dose teicoplanin. Additionally, Falcone et al reported that daptomycin treatment was associated with a reduction in the duration of antibiotic therapy in patients with MRSA BSI.29 In their study, a higher percentage of patients in the glycopeptide group had a central venous catheter or other intravascular devices in place than did those of the daptomycin group.29 The duration of antibiotic therapy was not shorter in our patients in the daptomycin group when compared with those in the high-dose teicoplanin group. It might be because of similar rates of adequate control of the source of infection between our patients in the high-dose teicoplanin and daptomycin treatment groups (Table 3).
Given that the bactericidal activity of glycopeptides is dependent on the concentration–time curve to MIC ratio (area under the curve [AUC24/MIC]) and the peak concentration to MIC ratio, administering higher doses could have a positive impact on patient outcomes. According to previous reports,30,31 the average of teicoplanin Cmin was 10 mg/L on day 6 in patients receiving teicoplanin maintenance doses of 6 mg/kg/24 hours, after loading doses of 6 mg/kg/12 hours. However, the teicoplanin Cmin achieved to 10 mg/L on day 2 in patients whom teicoplanin maintenance doses of 6 mg/kg/12 hours were continued after loading doses of 6 mg/kg/12 hours.30,31 The higher rate of clinical failure in the standard-dose regimen group might be related to the inability to achieve the AUC24/MIC target when teicoplanin MIC exceeds 1 mg/L.16 Daptomycin’s rapid bactericidal and concentration-dependent activity may have contributed to the more favorable outcomes.32 As a result, daptomycin was associated with significantly less clinical failure when compared with vancomycin or standard-dose teicoplanin in the setting of MRSA BSI with glycopeptides MICs ≥1.5 mg/L in recently published studies13,14 as well as in the current cohort.
This study still had several limitations. First, despite retrieving patient outcomes based on favorable outcomes at the end of initial teicoplanin or daptomycin treatment to minimize the confounding of the primary endpoint, this retrospective approach for other parameters has inherent limitations because of potential confounding and selection bias. Multicenter, prospective, randomized trials are needed to validate our findings. Second, to adequately assess the treatment impact for MRSA BSI, several exclusion criteria were implemented, which might have limited its external validity. However, patients receiving inadequate dosage of teicoplanin or daptomycin were excluded from our population, which should have maximal effect on the clinical outcomes. Third, this is a retrospective study in a single institution that included a limited number of patients with bacteremia due to MRSA strains with teicoplanin MICs ≥1.5 mg/L; thus, its generalizability is limited. Fourth, molecular analyses were not performed to identify the specific MRSA strains and clones with teicoplanin MICs ≥1.5 mg/L that might be prevalent in the hospital during the study period. Finally, analyses of serum teicoplanin and daptomycin levels were not performed because no commercialized methods were available to determine these levels. Nevertheless, high teicoplanin maintenance dose regimens and daptomycin dose regimens greater than the FDA-approved dose of 6 mg/kg daily have been associated with safety and potentially more favorable outcomes in previous observational studies.13,15,16
Conclusions
In patients with bacteremia due to MRSA strains with teicoplanin MICs ≥1.5 mg/L, Pittsburgh bacteremia score ≥4 was an independent risk factor for unfavorable outcomes. After propensity-score matching, patients in the high-dose daptomycin group had better short-term outcomes and outcomes at the end of therapy than did those in the standard-dose teicoplanin group. However, the clinical outcomes of the patients in the high-dose teicoplanin maintenance dose group were similar to those in the high-dose daptomycin group.
Acknowledgments
We would like to thank the Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital for the statistical analyses. We also thank Dr Chien-Ching Hung at the Department of Internal Medicine, National Taiwan University Hospital, for his critical review of this manuscript. This study was supported by grants from Chang Gung Memorial Hospital, Taiwan (CMRPG 8F1681).
Disclosure
The authors report no conflicts of interest in this work.
References
Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355(7):666–674. | ||
Cosgrove SE, Qi Y, Kaye KS, Harbarth S, Karchmer AW, Carmeli Y. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol. 2005;26(2):166–174. | ||
Reed SD, Friedman JY, Engemann JJ, et al. Costs and outcomes among hemodialysis-dependent patients with methicillin-resistant or methicillin-susceptible Staphylococcus aureus bacteremia. Infect Control Hosp Epidemiol. 2005;26(2):175–183. | ||
Svetitsky S, Leibovici L, Paul M. Comparative efficacy and safety of vancomycin versus teicoplanin: systematic review and meta-analysis. Antimicrob Agents Chemother. 2009;53(10):4069–4079. | ||
Chang HJ, Hsu PC, Yang CC, et al. Influence of teicoplanin MICs on treatment outcomes among patients with teicoplanin-treated methicillin-resistant Staphylococcus aureus bacteraemia: a hospital-based retrospective study. J Antimicrob Chemother. 2012;67(3):736–741. | ||
Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52(3):285–292. | ||
Mensa J, Barberán J, Llinares P, et al. Guidelines for the treatment on infections caused by methicillin-resistant Staphylococcus aureus. Rev Esp Quimioter. 2008;21(4):234–258. | ||
Gudiol F, Aguado JM, Almirante B, et al. Diagnosis and treatment of bacteremia and endocarditis due to Staphylococcus aureus. A clinical guideline from the Spanish Society of Clinical Microbiology and Infectious Diseases (SEIMC). Enferm Infecc Microbiol Clín. 2015;33(9):625.e1–625.e23. | ||
Kullar R, Casapao AM, Davis SL, et al. A multicentre evaluation of the effectiveness and safety of high-dose daptomycin for the treatment of infective endocarditis. J Antimicrob Chemother. 2013;68(12):2921–2926. | ||
Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; 25th Informational Supplement, CLSI Document M100-S252015. Wayne, PA: CLSI. | ||
Moise-Broder PA, Sakoulas G, Eliopoulos GM, Schentag JJ, Forrest A, Moellering RC. Accessory gene regulator group II polymorphism in methicillin-resistant Staphylococcus aureus is predictive of failure of vancomycin therapy. Clin Infect Dis. 2004;38(12):1700–1705. | ||
Sakoulas G, Moise-Broder PA, Schentag J, Forrest A, Moellering RC, Eliopoulos GM. Relationship of MIC and bactericidal activity to efficacy of vancomycin for treatment of methicillin-resistant Staphylococcus aureus bacteremia. J Clin Microbiol. 2004;42(6):2398–2402. | ||
Moore CL, Osaki-Kiyan P, Haque NZ, Perri MB, Donabedian S, Zervos MJ. Daptomycin versus vancomycin for bloodstream infections due to methicillin-resistant Staphylococcus aureus with a high vancomycin minimum inhibitory concentration: a case-control study. Clin Infect Dis. 2012;54(1):51–58. | ||
Murray KP, Zhao JJ, Davis SL, et al. Early use of daptomycin versus vancomycin for methicillin-resistant Staphylococcus aureus bacteremia with vancomycin minimum inhibitory concentration >1 mg/L: a matched cohort study. Clin Infect Dis. 2013;56(11):1562–1569. | ||
Lee CH, Tsai CY, Li CC, Chien CC, Liu JW. Teicoplanin therapy for MRSA bacteraemia: a retrospective study emphasizing the importance of maintenance dosing in improving clinical outcomes. J Antimicrob Chemother. 2015;70(1):257–263. | ||
Tsai CY, Lee CH, Chien CC, Chen IL. Impact of teicoplanin maintenance dose and MIC values on the clinical outcomes of patients treated for methicillin-resistant Staphylococcus aureus bacteremia. Infect Drug Resist. 2018;11:1205–1217. | ||
Chen IL, Lee CH, Su LH, Tang YF, Chang SJ, Liu JW. Antibiotic consumption and healthcare-associated infections caused by multidrug-resistant gram-negative bacilli at a large medical center in Taiwan from 2002 to 2009: implicating the importance of antibiotic stewardship. PLoS One. 2013;8(5):e65621. | ||
Zhou L, Gao Y, Cao W, et al. Retrospective analysis of relationships among the dose regimen, trough concentration, efficacy, and safety of teicoplanin in Chinese patients with moderate-severe Gram-positive infections. Infect Drug Resist. 2018;11:29–36. | ||
Mccabe WR. Gram-negative bacteremia. Adv Intern Med. 1974;19:135–158. | ||
Chow JW, Yu VL. Combination antibiotic therapy versus monotherapy for gram-negative bacteraemia: a commentary. Int J Antimicrob Agents. 1999;11(1):7–12. | ||
Brun-Buisson C, Abrouk F, Legrand P, Huet Y, Larabi S, Rapin M. Diagnosis of central venous catheter-related sepsis. Critical level of quantitative tip cultures. Arch Intern Med. 1987;147(5):873–877. | ||
Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988;16(3):128–140. | ||
El-Ahdab F, Benjamin DK, Wang A, et al. Risk of endocarditis among patients with prosthetic valves and Staphylococcus aureus bacteremia. Am J Med. 2005;118(3):225–229. | ||
Christou NV, Turgeon P, Wassef R, Rotstein O, Bohnen J, Potvin M. Management of intra-abdominal infections. The case for intraoperative cultures and comprehensive broad-spectrum antibiotic coverage. The Canadian Intra-abdominal Infection Study Group. Arch Surg. 1996;131(11):1193–1201. | ||
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. | ||
Bassetti M, Nicco E, Ginocchio F, Ansaldi F, de Florentiis D, Viscoli C. High-dose daptomycin in documented Staphylococcus aureus infections. Int J Antimicrob Agents. 2010;36(5):459–461. | ||
Moise PA, Hershberger E, Amodio-Groton MI, Lamp KC. Safety and clinical outcomes when utilizing high-dose (> or =8 mg/kg) daptomycin therapy. Ann Pharmacother. 2009;43(7):1211–1219. | ||
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. | ||
Falcone M, Russo A, Pompeo ME, et al. Retrospective case-control analysis of patients with staphylococcal infections receiving daptomycin or glycopeptide therapy. Int J Antimicrob Agents. 2012;39(1):64–68. | ||
Lefrock J, Ristuccia A. Teicoplanin in the treatment of bone and joint infections: an open study. J Infect Chemother. 1999;5(1):32–39. | ||
Brink AJ, Richards GA, Cummins RR, Lambson J. Gauteng Understanding Teicoplanin Serum levels (GUTS) Study Group. Recommendations to achieve rapid therapeutic teicoplanin plasma concentrations in adult hospitalized patients treated for sepsis. Int J Antimicrob Agents. 2008;32:455–458. | ||
Marconescu P, Graviss EA, Musher DM. Rates of killing of methicillin-resistant Staphylococcus aureus by ceftaroline, daptomycin, and telavancin compared to that of vancomycin. Scand J Infect Dis. 2012;44(8):620–622. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.