Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
CYP2D6 Gene Polymorphisms and Variable Metabolic Activity in Schizophrenia Patients of Han and Tibetan Populations
Authors Li YH, Huang W, Xiao MY, Huang SQ, Chen H, Li ZF, Li XS, Cheng Y ![]()
Received 27 December 2021
Accepted for publication 25 March 2022
Published 2 April 2022 Volume 2022:18 Pages 731—736
DOI https://doi.org/10.2147/NDT.S355985
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Yong-Hang Li,1,* Wei Huang,1,* Man-Yu Xiao,2 Shi-Qing Huang,1 Hui Chen,1 Zai-Fang Li,1 Xue-Song Li,1 Yong Cheng1,2
1The Third People’s Hospital of Foshan, Foshan, Guangdong, People’s Republic of China; 2Center on Translational Neuroscience, College of Life and Environmental Sciences, Minzu University of China, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong Cheng; Xue-Song Li, Email [email protected]; [email protected]
Background: It has been suggested that the pharmacogenomic response to antipsychotics in schizophrenia patients partially contributed by drug metabolism enzyme polymorphism, including P450 2D6 (CYP2D6). However, CYP2D6 gene polymorphism across populations is largely unknown.
Materials and Methods: Here, we investigated the differences of CYP2D6 gene polymorphism between Chinese Han and Tibetan schizophrenia patients. We analyzed five CYP2D6 gene related polymorphic locus in 103 patients with schizophrenia, including 60 Han ethnicity and 43 of Tibetan ethnicity, by nucleic acid MALDI-TOF.
Results: Polymorphisms of rs1065852, rs1135840 and rs16947 were significantly different between Han and Tibetan patients. rs1065852 AA genotype had a low frequency of 9.3% in Tibetan patients in comparison with a frequency of 41.7% in Han patients, whereas rs16947 AA genotype had a low frequency of 3.3% in Han patients in comparison with a frequency of 34.9% in Tibetan patients. Additionally, the two patient groups showed distinct distribution of CYP2D6 haplotypes, with the highest frequency of *10/*10 and *1/*2 in Han and Tibetan patients, respectively. Furthermore, Han and Tibetan patients showed differential CYP2D6 metabolic activity.
Discussion: Taken together, this exploratory study showed the differences of CYP2D6 gene and metabolic polymorphism between Han and Tibetan schizophrenia patients, and therefore may improve our understanding of the pharmacogenomic response to antipsychotics in schizophrenia patients across populations.
Keywords: schizophrenia, CYP2D6, Han, Tibetan
Introduction
Schizophrenia is a chronic psychotic disorder with typical onset in early adulthood, and the disease affects approximately 1% of worldwide population. Patients with schizophrenia have the hallmark symptoms of psychosis, such as delusions, hallucinations, disordered thinking, and also may experience negative symptoms, such as apathy, loss of emotional expression and cognitive deficits.1 The etiology of schizophrenia is complex and associated with genetic, environmental and behavioral risk factors, as well as higher levels of economic development, industrialization and urbanization.2 Recent studies have suggested a critical role of epigenetics in the onset and/or development of schizophrenia.3,4 The prevalence and absolute number of patients with schizophrenia is increased significantly over the last several decades in China, and it has been shown that the prevalence of schizophrenia patients in China doubled from 1990 to 2010, with rates particularly high in the most developed parts of modern China.5 However, the prevalence and treatment of schizophrenia across populations in China is still largely unknown, especially in remote parts of China.
Cytochrome P450 2D6 (CYP2D6) is an important pharmacokinetics gene involved in the metabolism of about 20% commonly used drugs including psychiatry, pain management, oncology and cardiology.6,7 CYP2D6 contributes to the metabolism of many drugs including antidepressants, antipsychotics, antineoplastic agents, adrenergic antagonists, and analgesics.8,9 However, CYP2D6 is highly polymorphic, and the frequency of CYP2D6 gene polymorphism is different across populations, which significantly affect the metabolism function, efficacy and safety of drug.10,11 The CYP2D6 gene is considered highly polymorphic since more than 105 different alleles have been identified so far, and many CYP2D6 alleles encode enzymes that have reduced or no function compared with the wild-type enzyme.12,13
It has been suggested that CYP2D6 is the main metabolic pathway of many antidepressants and a number of antipsychotics.14 The metabolic rate of antipsychotics substrate for CYP2D6 can be affected by these genetic variants.15 Patients with genetically determined CYP2D6 poor metabolizer (PMs) status may require lower doses of antipsychotic. Alternatively, CYP2D6 ultrarapid metabolizers (UMs) may need increased drug dosage to obtain optimal therapeutic response.16–18 Additionally, five CYP2D6 gene related polymorphic locus, rs1065852, rs1135840, rs16947, rs28371725 and rs3892097, have been suggested to be associated with CYP2D6 pharmacokinetics.19,20 Thus, this study used mass spectrometry to explore the differences of the five CYP2D6 gene and metabolic polymorphisms between Han and Tibetan schizophrenia patients.
Materials and Methods
Participants
The project recruited 103 schizophrenia patients, 60 of Han ethnicity and 43 of Tibetan ethnicity. Han patients were recruited from the Third People’s Hospital of Foshan, Foshan, Guangdong, China. Tibetan patients were recruited from the People’s Hospital of Ngari, Ngari, Tibet, China. The diagnosis of patients with schizophrenia were made by experienced psychiatrists according to The International Classification of Diseases-10 and The Structured Clinical Interview of DSM-5.
Before the collection of samples and data, consents were obtained for each participant or relative in the study. Patients’ oral epithelial cells were collected through standardized procedures. The study protocol was reviewed and approved by the ethics committee at the Third People’s Hospital of Foshan, and the patients and relatives were informed about the purpose of the study.The experiments were conducted in accordance with the Declaration of Helsinki.
Analysis of SNP with Mass Spectrometry
Agena MassARRAY platform was used for SNP genotyping. It is a robust tool with high accuracy and is cost-effective which combines multiplex PCR and high resolution LC-MS/MS (Triple Quad 3200, AB SCIEX,), and the detailed protocol was described in a previous literature.21 The haplotype results were determined according to the haplotype definition criteria of CYP2D6 provided by pharmGKB. For each haplotype, the standardized scoring method was used to determine the metabolic function and predicted the metabolic enzyme activity at the individual level.22
Data Analyses
In this study, Fisher’s exact test was used to compare the differences of CYP2D6 gene polymorphism and metabolic activity polymorphism between Han and Tibetan populations. Data analysis and statistical test were performed by R (version 4.0.3) statistical software.
Results
Differences of CYP2D6 Gene Polymorphism Between Han and Tibetan Patients
In this study, five CYP2D6 gene related polymorphic locus, rs1065852, rs1135840, rs16947, rs28371725, rs3892097, were assessed in 103 patients, 60 of Han ethnicity and 43 of Tibetan ethnicity. As shown in Table 1, the polymorphisms of rs1065852, rs1135840 and rs16947 were significantly different between Han and Tibetan patients. The rs1065852 and rs1135840 genotypes were more evenly distributed in Han patients compared with Tibetan patients. rs1065852 AA genotype had a low frequency of 9.3% in Tibetan patients in comparison with a frequency of 41.7% in Han patients, whereas rs16947 AA genotype had a low frequency of 3.3% in Han patients in comparison with a frequency of 34.9% in Tibetan patients. Additionally, rs1065852 GG genotype had a high frequency of 65.1% in Tibetan patients in comparison with a frequency of 18.3% an patients, whereas rs16947 GG genotype had a high frequency of 65.1% in Han patients in comparison with a frequency of 16.3% in Tibetan patients.
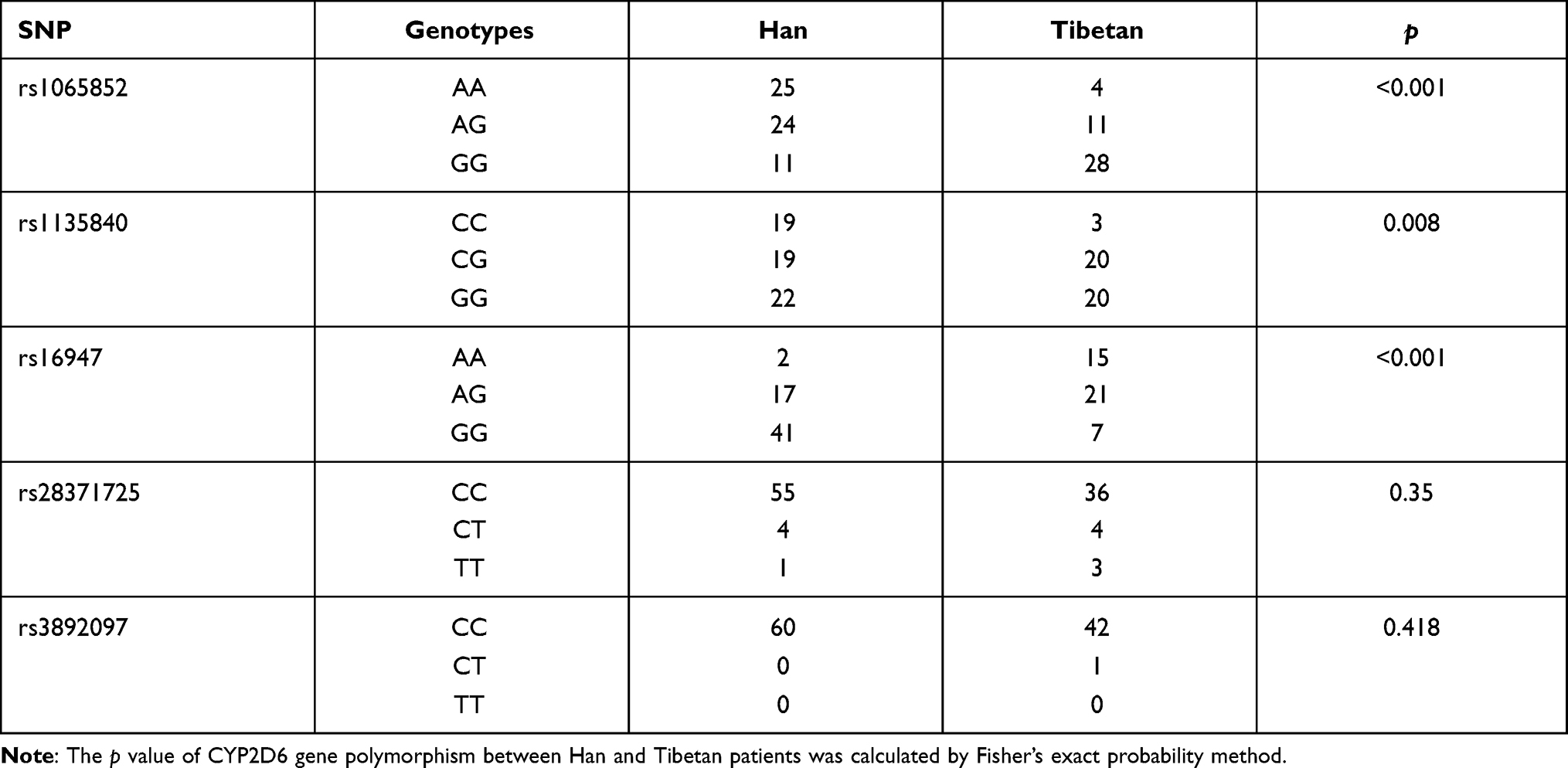 |
Table 1 CYP2D6 Gene Polymorphism Differences Between Han and Tibetan Patients |
Additonally, it should be noted that the five SNPs tested in this study followed the Hardy-Weinberg equilibrium (p > 0.05 in all the analyses).
Distribution of CYP2D6 Haplotypes in Han and Tibetan Patients
We next analyzed the distribution of CYP2D6 haplotypes in Han and Tibetan patients (Table 2). The Han and Tibetan schizophrenia patients showed distinct haplotype distribution, with the highest frequency of *10/*10, followed by *1/*10, accounting for 61.7% of haplotypes in Han patients. The haplotype with the highest frequency in Tibetan patients was *1/*2, followed by *2/*2, accounting for 46.5% of haplotypes.
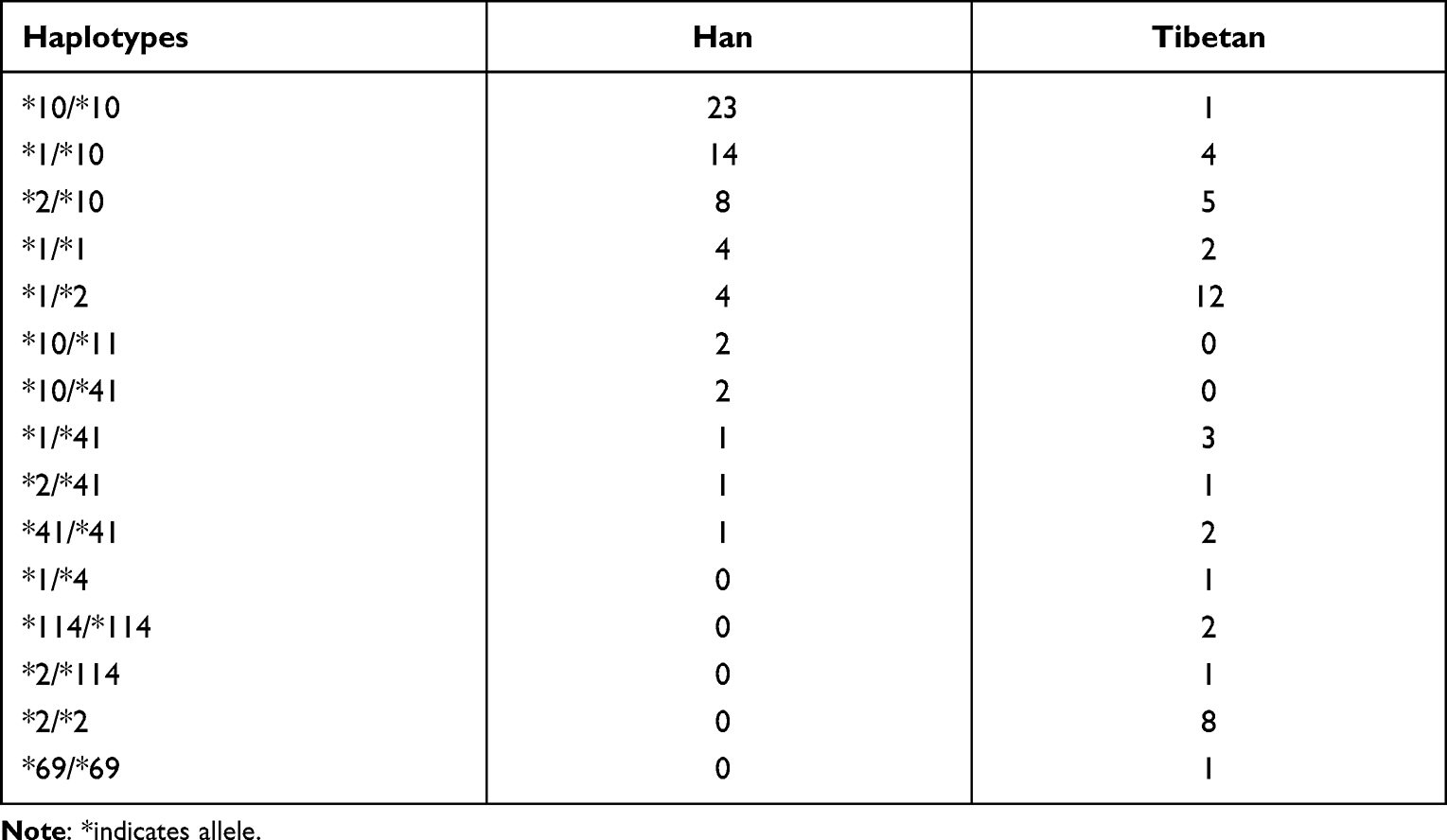 |
Table 2 Distribution of CYP2D6 Haplotype in Han and Tibetan Patients |
Differences of CYP2D6 Metabolic Activity Between Han and Tibetan Patients
Our analysis suggested that there was significant difference in CYP2D6 metabolic activity between Han and Tibetan patients (P < 0.001) (Table 3). Normal and intermediate metabolism in Han patients were 53% and 47%, respectively. However, fast metabolism or poor metabolism was not detected in Han patients. Tibetan patients were mostly normal metabolism, accounting for 81.4%, and the patients with intermediate metabolism and poor metabolism accounted for 11.6% and 7%, respectively.
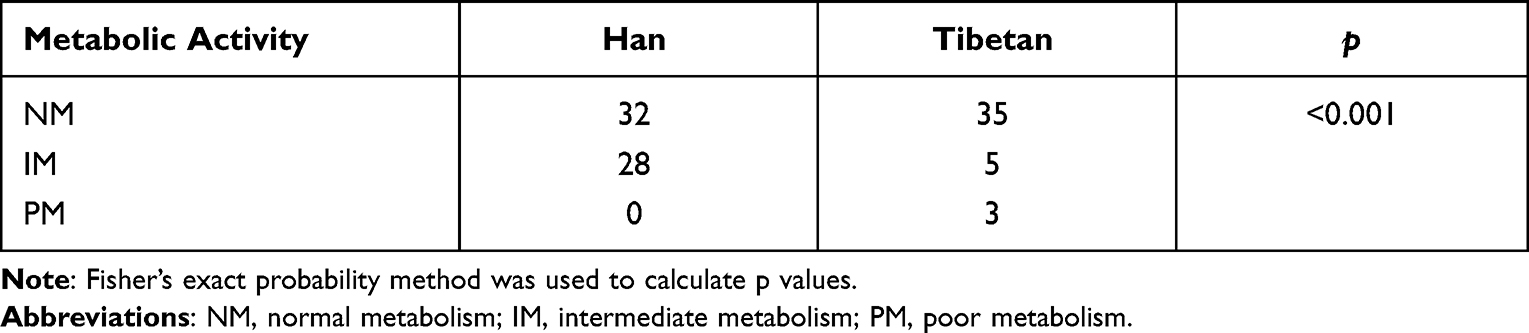 |
Table 3 Differences of CYP2D6 Metabolic Activity Between Han and Tibetan Patients |
Discussion
Schizophrenia affects nearly 1% of the world population and is among the top 10 global causes of disability.23 The disease is considered caused by genetic and environmental factor interactions, the environmental factors include obstetrical complications, early-life adversity, and childhood residence in urban.24,25 Therefore, schizophrenia is a very heterogeneous disease across populations and even at the individual level. There is an increased awareness that the treatment of schizophrenia should be more individualized. Now, the “precision medicine” has become very populous in recent years. Precision medicine focus on the stratification of patients, including clinical, lifestyle, genetic and biomarker information.26 This study analyzed the key drug metabolism gene of schizophrenia patients across populations, and also in dramatic different environments, might help to make better treatment strategies in schizophrenia across populations. For example, Tibetan patients had rare haplotypes *69/*69 and *114/*114, and these are metabolically inactive haplotypes which were not found in Han patients from our present study. Therefore, these patients with rare haplotypes may need lower dose of antipsychotics, due to the poor metabolism of CYP2D6 in Tibetan patients.Additionally, our study showed high frequency of CYP2D6 *10/*10 and *1/*10 in Han patients, but not in Tibetan patients, and it has been demonstrated that schizophrenia patients with CYP2D6 *10 genotype had poor metabolic activity.27
China is a multi-ethnic country with vast territory, and the cause of mental disorders across populations may be affected by multiple factors, including genetics, culture, education and geographical location. Our research showed differences of CYP2D6 gene polymorphisms and haplotypes between Han and Tibetan patients, and poor metabolism was more common in Tibetan patients. However, the limitation of our study is that it is unclear whether the differences in CYP2D6 gene and metabolic polymorphisms in schizophrenia patients are simply due to different populations, or contributed by the environment factors. In fact, samples of Tibetan patients were collected from Ngari, with an average elevation of over 4500 meters, also known as the “Roof of the World”. People in Tibetan areas, especially in Ngari, have been affected by high altitude and low oxygen for a long time. Over thousands of years, some high-altitude populations have adapted to this environment, with genetic signatures revealing natural selection around hypoxia-sensing pathways.28,29 Additionally, studies showed the changes in the blood-brain barrier and gut microbiota of people living at high altitudes.30,31 Therefore, the environmental factors should be especially considered for understanding of mental disease etiology and treatment in these populations.
Now the genetic testing is slowly coming to fruition, individualized medicine will take advantage of available tests, and utilize the information as part of the clinical decision. Our results showed the differences in gene polymorphism and metabolic polymorphism of in Han and Tibetan patients of schizophrenia, and therefore may improve our understanding of the pharmacogenomic response to antipsychotics in schizophrenia patients across populations.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (82071676), the High-Level Hospital Development Program for Foshan “Climbing” Project, the Natural Science Foundation of Guangdong Province (2114050002827), and Foshan Science and technology innovation project (2020001005608). Additionally, the authors would like to thank all the patients and controls for providing blood samples, Dr Chengchen Huang for the technique support, and Mr Yang Hu, Mr Yun Yu and Ms Huang-Tong Wu for their assistance in blood sample collection.
Disclosure
The authors declare that there is no conflict of interest involved in this work.
References
1. Goff DC. The pharmacologic treatment of schizophrenia-2021. JAMA. 2021;325(2):175–176. doi:10.1001/jama.2020.19048
2. McGrath JJ. Myths and plain truths about schizophrenia epidemiology–the NAPE lecture 2004. Acta Psychiatr Scand. 2005;111(1):4–11. doi:10.1111/j.1600-0447.2004.00467.x
3. Du Y, Yu Y, Hu Y, et al. Genome-Wide, Integrative Analysis Implicates Exosome-Derived MicroRNA Dysregulation in Schizophrenia. Schizophr Bull. 2019;45(6):1257–1266. doi:10.1093/schbul/sby191
4. Du Y, Tan WL, Chen L, et al. Exosome Transplantation From Patients With Schizophrenia Causes Schizophrenia-Relevant Behaviors in Mice: an Integrative Multi-omics Data Analysis. Schizophr Bull. 2021;47(5):1288–1299. doi:10.1093/schbul/sbab039
5. Chan KY, Zhao FF, Meng S, et al. Prevalence of schizophrenia in China between 1990 and 2010. J Glob Health. 2015;5(1):010410. doi:10.7189/jogh.05.010410
6. Yang Y, Botton MR, Scott ER, Scott SA. Sequencing the CYP2D6 gene: from variant allele discovery to clinical pharmacogenetic testing. Pharmacogenomics. 2017;18(7):673–685. doi:10.2217/pgs-2017-0033
7. Jarvis JP, Peter AP, Shaman JA. Consequences of CYP2D6 Copy-Number Variation for Pharmacogenomics in Psychiatry. Front Psychiatry. 2019;10:432. doi:10.3389/fpsyt.2019.00432
8. Thuerauf N, Lunkenheimer J. The impact of the CYP2D6-polymorphism on dose recommendations for current antidepressants. Eur Arch Psychiatry Clin Neurosci. 2006;256(5):287–293. doi:10.1007/s00406-006-0663-5
9. Nofziger C, Turner AJ, Sangkuhl K, et al. PharmVar GeneFocus: CYP2D6. Clin Pharmacol Ther. 2020;107(1):154–170. doi:10.1002/cpt.1643
10. Taylor C, Crosby I, Yip V, et al. A Review of the Important Role of CYP2D6 in Pharmacogenomics. Genes. 2020;11(11):11. doi:10.3390/genes11111295
11. Gaedigk A. Complexities of CYP2D6 gene analysis and interpretation. Int Rev Psychiatry. 2013;25(5):534–553. doi:10.3109/09540261.2013.825581
12. Haufroid V, Hantson P. CYP2D6 genetic polymorphisms and their relevance for poisoning due to amfetamines, opioid analgesics and antidepressants. Clin Toxicol. 2015;53(6):501–510. doi:10.3109/15563650.2015.1049355
13. Li XY, Hu XX, Yang F, et al. Effects of 24 CYP2D6 variants found in Chinese population on the metabolism of clonidine in vitro. Chem Biol Interact. 2019;313:108840. doi:10.1016/j.cbi.2019.108840
14. Bertilsson L, Dahl ML, Dalen P, Al-Shurbaji A. Molecular genetics of CYP2D6: clinical relevance with focus on psychotropic drugs. Br J Clin Pharmacol. 2002;53(2):111–122. doi:10.1046/j.0306-5251.2001.01548.x
15. Arranz MJ, de Leon J. Pharmacogenetics and pharmacogenomics of schizophrenia: a review of last decade of research. Mol Psychiatry. 2007;12(8):707–747. doi:10.1038/sj.mp.4002009
16. Kirchheiner J, Nickchen K, Bauer M, et al. Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the phenotype of drug response. Mol Psychiatry. 2004;9(5):442–473. doi:10.1038/sj.mp.4001494
17. de Leon J, Susce MT, Pan RM, et al. The CYP2D6 poor metabolizer phenotype may be associated with risperidone adverse drug reactions and discontinuation. J Clin Psychiatry. 2005;66(1):15–27. doi:10.4088/JCP.v66n0103
18. Riedel M, Schwarz MJ, Strassnig M, et al. Risperidone plasma levels, clinical response and side-effects. Eur Arch Psychiatry Clin Neurosci. 2005;255(4):261–268. doi:10.1007/s00406-004-0556-4
19. Caudle KE, Sangkuhl K, Whirl-Carrillo M, et al. Standardizing CYP2D6 Genotype to Phenotype Translation: consensus Recommendations from the Clinical Pharmacogenetics Implementation Consortium and Dutch Pharmacogenetics Working Group. Clin Transl Sci. 2020;13(1):116–124. doi:10.1111/cts.12692
20. Abdullah-Koolmees H, van Keulen AM, Nijenhuis M, Deneer VHM. Pharmacogenetics Guidelines: overview and Comparison of the DPWG, CPIC, CPNDS, and RNPGx Guidelines. Front Pharmacol. 2021;11:595219. doi:10.3389/fphar.2020.595219
21. Ellis JA, Ong B. The MassARRAY® System for Targeted SNP Genotyping. Methods Mol Biol. 2017;1492:77–94.
22. Caudle KE, Sangkuhl K, Whirl-Carrillo M, et al. Standardizing CYP2D6 Genotype to Phenotype Translation: consensus Recommendations from the Clinical Pharmacogenetics Implementation Consortium and Dutch Pharmacogenetics Working Group. Clin Transl Sci. 2020;13(1):116–124.
23. Fleischhacker WW, Arango C, Arteel P, et al. Schizophrenia–time to commit to policy change. Schizophr Bull. 2014;40(Suppl 3):S165–94. doi:10.1093/schbul/sbu006
24. Bennett MR. Schizophrenia: susceptibility genes, dendritic-spine pathology and gray matter loss. Prog Neurobiol. 2011;95(3):275–300. doi:10.1016/j.pneurobio.2011.08.003
25. Marder SR, Cannon TD. Schizophrenia. N Engl J Med. 2019;381(18):1753–1761. doi:10.1056/NEJMra1808803
26. Konig IR, Fuchs O, Hansen G, von Mutius E, Kopp MV. What is precision medicine? Eur Respir J. 2017;50(4):478. doi:10.1183/13993003.00391-2017
27. Pei Q, Huang L, Huang J, et al. Influences of CYP2D6*10 polymorphisms on the pharmacokinetics of iloperidone and its metabolites in Chinese patients with schizophrenia: a population pharmacokinetic analysis. Acta Pharmacol Sin. 2016;37(11):1499–1508. doi:10.1038/aps.2016.96
28. Bigham AW, Lee FS. Human high-altitude adaptation: forward genetics meets the HIF pathway. Genes Dev. 2014;28(20):2189–2204. doi:10.1101/gad.250167.114
29. Murray AJ. Energy metabolism and the high-altitude environment. Exp Physiol. 2016;101(1):23–27. doi:10.1113/EP085317
30. Lafuente JV, Bermudez G, Camargo-Arce L, Bulnes S. Blood-Brain Barrier Changes in High Altitude. CNS Neurol Disord Drug Targets. 2016;15(9):1188–1197. doi:10.2174/1871527315666160920123911
31. Zeng B, Zhang S, Xu H, et al. Gut microbiota of Tibetans and Tibetan pigs varies between high and low altitude environments. Microbiol Res. 2020;235:126447. doi:10.1016/j.micres.2020.126447
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.