Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Customers’ Perception Towards Accountability of Diagnostic Centres: Evidence from India
Received 27 June 2023
Accepted for publication 22 September 2023
Published 4 October 2023 Volume 2023:16 Pages 2947—2961
DOI https://doi.org/10.2147/JMDH.S425011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Suman Agarwal, Ranjit Singh
Department of Management Studies, Indian Institute of Information Technology Allahabad, Prayagraj, UP, India
Correspondence: Ranjit Singh, Department of Management Studies, Indian Institute of Information Technology Allahabad, Prayagraj, UP, India, Tel +91 9532766339, Email [email protected]
Introduction: A deeper comprehension of accountability is beneficial for identifying and fostering tactics to boost accountability and raise the standard of healthcare. The main objective of the present paper is to measure the level of customers’ perception of accountability of healthcare diagnostic service providers and to identify the factors that influence the perception of accountability of healthcare diagnostic service customers.
Methods: A questionnaire survey was used to collect data from 393 customers of various diagnostic centers in the city of Guwahati from the state of Assam in India. The reliability of the data was tested using Cronbach’s Alpha. Statistical tests were used for the mean, percentage, standard deviation, etc. Factor analysis was performed to find out the factors affecting customers’ perception of accountability.
Results: It was found that the overall level of perception of the customers with respect to the accountability of diagnostic centers in Guwahati is of high level. The study reveals four variables that affect how customers perceive the accountability of diagnostic service providers. These are Competency, Responsiveness, Compliance with protocol, and Problem-solving approach.
Discussion: Significant contributions have been made by the present study in terms of the development of a scale to measure customers’ perception of accountability of diagnostic centre, and the development of a theoretical model to explain this accountability.
Keywords: accountability, healthcare, diagnostic centers, customers’ perception
Introduction
Healthcare is one of the most individualized services despite being one of the most expensive, complicated, and widely used services.1 The sector makes an effort to increase quality and safety, embracing certain crucial high-accountability organization principles.2 Accountability is essential in an area as sensitive as healthcare.3 Healthcare quality, cost, and safety are increasingly important in this day and age, and value (quality/cost) and safety are the watchwords of accountability.4 Every healthcare organization has to have an appropriate structure to make accountability clear, encourage transparency, and aid in healthcare governance to improve care quality.5 In patient safety cultures, accountability is defined and practiced, and ongoing research indicates accountability may affect the effectiveness of healthcare organizations.6 Accountability covers the guidelines and techniques one party employs to justify7 and take ownership of its behavior.8 Instead of conceiving accountability as a problem to be resolved, it is to be seen as a process to be continuously refined.9 A program and strategy for accountable healthcare will continually examine and reorganize the procedures to fit the needs of the patient and enhance the standard of treatment.10 Moral responsibility supports the patient’s confidence in the physician delivering treatment by preventing professional complacency. Patients frequently assume that the therapist is operating in their best interests.11
A lack of accountability in the health sector is one of the factors for the failure of effective and efficient health services in India.12 Improving the standard of care and accessibility to healthcare services in India has been the focus of policymakers’ professional accountability. To provide the optimal healthcare outcome, it is also necessary to address patient safety, transparency, professional responsibility, and organizational accountability.12 The government’s recent efforts to build an accountable healthcare system have also impacted the accountability mechanism.13
A patient care system has a duty to gather useful research information that may be examined and used to enhance patient safety. Members of the organization must be alert, and conscious, and keep constant monitoring for this process to succeed.14 The steadfast belief that everyone working in the healthcare sector has two jobs when they report working each day is maintained by accountability policies and procedures. Healthcare will not function to its full capacity if change-making does not become an essential component of everyone’s job, every day, in all facets of the system.15
For continuous improvement of health service delivery, providers must know what their customers think of their accountability.16 Assessment of accountability is important for pursuing ongoing professional development, including acquiring and maintaining clinical skills, accessing and using the best evidence, taking part in quality planning, and analyzing and improving care delivery systems.17
There are various forms of accountability that have evolved over some time propounded by various scholars, such as legal accountability, political accountability, and professional accountability.18 Parties in the healthcare industry may be held liable for up to six different things at once: professional competency, legal and ethical behavior, financial performance, the sufficiency of access, promotion of public health, and community benefit.8
Accountability (offering transparency and proof of corrective action to the public, consumers, and other stakeholders) is becoming more and more important in the healthcare industry when developing and reporting organizational performance measurements.19,20
The research has been chosen to be based on a reputable clinic. One of India’s biggest private integrated health care systems, according to size. It has been long argued the benefits of using case studies to develop theories.21,22 Every case function as a unique experiment demonstrating its analytical entity. Inductive methodologies can be generalized, and the case study approach is one of them.
This early work, which provides an empirically grounded initial glimpse into a multi-sited ethnography, focuses on the design and development of accountability infrastructure for healthcare regulation and quality improvement in diagnostic facilities. Examined in particular is the creation of an accountability infrastructure for monitoring and improving the performance of diagnostic facilities providing pathological and radiological screening services. Perception of accountability of diagnostic centres plays an important role in the decision-making process of customers in choosing the centre to visit. There have been a lot of research in the area of accountability, however, customers perception of accountability in diagnostic services has not yet been done. Moreover, there is no specific scale yet been developed to measure the level of accountability in diagnostic services. This research attempts to fill this gap. The main objective of the present paper is to measure the level of customers’ perception of accountability of healthcare diagnostic service providers and to identify the factors that influence the perception of accountability of healthcare diagnostic service customers. The paper attempts to answer the following research questions:
- RQ1: What is the level of customers’ perception of accountability of healthcare diagnostic service providers?
- RQ2: What are the factors influencing the perception of accountability of healthcare diagnostic service customers?
Figure 1 provides the research framework adopted in this paper:
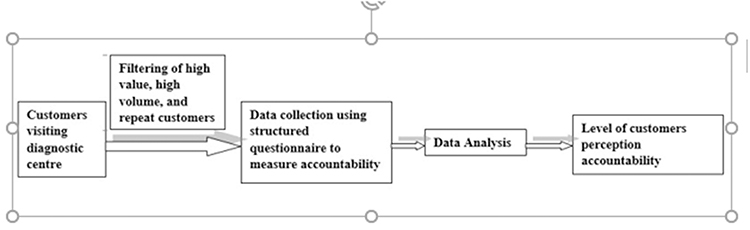 |
Figure 1 Research framework. |
The rest of the paper is organized as follows: Review of the Existing Literature and Research Gap discusses the review of the existing literature, Data and Methodology deals with the research methodology used in the study, Results describes the analysis and the findings of the study, Discussion presents the discussion, section 6 explains the implications and scope of future research finally Conclusion contains the conclusion.
Review of the Existing Literature and Research Gap
Accountability, answerability, and responsibility are three nearly equivalent phrases that are essentially defined by one another.23,24 Although the concept of accountability is growing both internationally and domestically, Schillemans25 and Bovens et al26 claimed that its definition was still murky and confusing. Accountability, often known as “answerability”, is the responsibility to educate and defend decisions or acts committed in front of others.24 Accountability relationships within health system hierarchies can be vertical, tying individuals who do tasks (actors, agents) to those for whom they are performed or who are affected by them (principals).27,28 There are numerous ways to be held accountable. Some concentrate on sanctions, others on results or outcomes, some on reporting requirements (answerability), while still, others concentrate on organizational behavior and processes.25 An approach to accountability that is frequently used is to evaluate how actors, programs, or policies are performing in comparison to predetermined goals or criteria.29 When pursuing its objective, an accountable company responds to the demands of its major stakeholders.30 Due to shifting trends and the nature of the workforce, employees must exercise greater personal accountability and self-management skills.31 When there is a lack of accountability, as when pledges are broken, criticism is disregarded, or obligations are ignored, it is clear how important accountability is. Such oversights in accountability have the potential to seriously damage relationships.17
Accountability benefits the organization (increasing credibility and legitimacy, strengthening governance structures, and encouraging learning and innovation) as well as its stakeholders (ensuring that their demands are taken into account in organizational policies and practices).30 Regulation, professionalism, and the market have all been identified as the three main elements driving accountability in the healthcare industry. Anyone directly impacted by healthcare services (patients, families), among other parties, may demand accountability.32
Accountability Theories
The term “accountability” is used to describe a set of elements that affect conduct in social environments.33 Accountability functions through formalizing expectations for behavior or actions, establishing consequences for failure, fostering trust, and supplying the drive and incentives to use resources effectively.34 Transparency, participation, evaluation, and complaint and response methods are the four elements that the GAP (Global Accountability Project) framework breaks down into when defining accountability. In order to be held accountable, a company must incorporate all of these factors into its policies, practices, and decision-making processes at all levels and stages of execution with respect to internal and external stakeholders. An organization’s rules, processes, and procedures will be more accountable if they are of a better caliber and are more deeply ingrained.30 According to a Meso-level theory of accountability developed by Frink et al,35 which has been stated to have as its goal the prediction and control of behavior, accountability is pervasive in social systems and is made more necessary in formal organizations. Deferring from others is a vital aspect of an organization, and this trait implies a blending of social and commercial activities, the people who make them up, and their various components, ranging from dyads to divisions. According to Vance, Lowry, and Eggett,36 distinguishing between accountability’s two most common uses—as a virtue and a mechanism—will help you better comprehend it. Accountability is viewed as a virtue because it is a quality that people should exhibit when they are willing to accept responsibility. This quality is desirable in public figures, governmental organizations, or fictional characters. As a mechanism, accountability is understood as a procedure in which a person may be required to explain his or her activities to a third party who will have the authority to judge them and may also expose the person to potential repercussions. According to a contingency theory of accountability, a variety of accountability mechanisms must be tailored to the needs and capabilities of the situation.37 The accountability hypothesis, developed by Vance, Lowry, and Eggett,38 describes how the need to defend one’s actions in front of a third-party drives people to think about and take responsibility for how decisions and judgements are made. As a result of this apparent need to take into account a decision-making process and outcome, there is a larger likelihood that someone will analyze their procedural actions thoroughly and methodically.
Literature Gap
Previous studies have discussed the meaning, forms, and need for accountability in the service sector. A little study has been conducted on measuring accountability in healthcare sector in general and diagnostic healthcare in particular. A comprehensive model for the identification of the factors influencing consumers’ perceptions of accountability in healthcare has not received much attention, despite the fact that numerous studies have suggested the steps that should be performed to promote accountability based on customer feedback. Also, there is a dearth of studies on healthcare diagnostic centre’s accountability. This describes the research gap we are trying to fill with this study. By examining customers’ perceptions of diagnostic centres’ accountability, this gap is intended to be closed. Studies that address how accountability can be estimated frequently fail to give a clear standard and frequently fail to address how one can find out how important accountability really is.26,39 Further empirical exploration into the workings of accountability is necessary in order to estimate normative claims on its advisability.
Data and Methodology
This research sets out to evaluate the factors that constitute the customers’ perception of the accountability of diagnostic centres. The study was conducted in one of the states of India namely Assam. The five major diagnostic centers located in the capital city of Assam, ie, Guwahati were chosen for the study. The study was descriptive in nature. The universe consisted of customers visiting those diagnostic centres. Judgment sampling was used as the sample strategy for this study. In this scenario, the client was either the patient himself/herself or, in the case of a minor and dependent individual, his/her attendant. Furthermore, all of the clients were not included in the study because of the judgement sample methodology. Only clients who fell into one of the three categories listed below were taken into account: Customers of high value, high volume, and repeat business. Those who have used at least three diagnostic services in the past three months are considered repeat clients. High-value clients were those whose total bill was more than Rs. 10,000 for the analysis’s purposes. Clients were categorized as high volume if they had at least three diagnostic tests performed in one visit yet had a charge under Rs. 10,000. Also, due to the peculiarities of the business, it was assumed that not all of the selected clients would be able to provide us with the data; as a result, the sample size was initially greater. 600 consumers were initially given the questionnaire; 422 of them responded, and 393 of those responses were deemed to be entirely accurate. Hence, in the end, 393 samples were taken into account, accounting for a 95% level of confidence and a 5% confidence interval. For this purpose, an at least three-month-old client database was taken into account. Also, only those customers were selected who agreed to take part in the study freely after reading and comprehending the material presented to them before the study started. In order to provide the appropriate context for the study area, secondary data was also gathered from pertinent sources like journals, official publications, newspapers, etc. A questionnaire survey was used to evaluate the diagnostic centers’ customers’ perspectives on the accountability of the centers. To measure the perception of accountability, a scale was framed by considering 14 items as mentioned in Table 1, which are identified from the review of the literature and theories related to accountability. The details of the items and their source are given in Table 1.
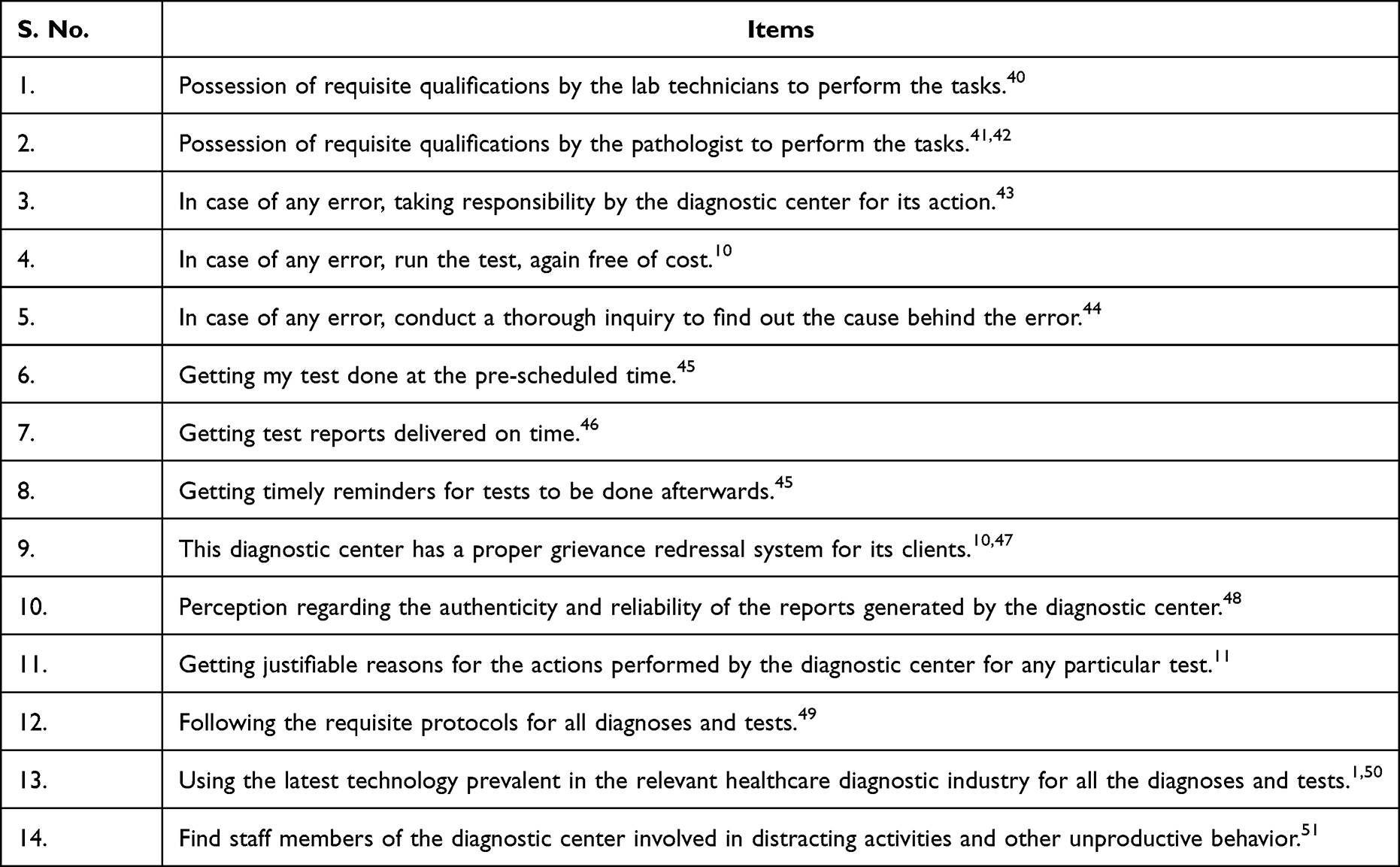 |
Table 1 Details of the Questionnaire |
The replies to the aforementioned questions were collected on a five-point Likert scale, with a response of strongly disagree receiving a score of 1, signifying a very low degree of accountability, and strongly agree receiving a score of 5, signifying a very high level of accountability. Only response number 14 is intended to be contradictory. In addition to this, there were inquiries about the respondents’ socioeconomic and demographic characteristics. When item-total correlation was applied to the aforementioned items, it was discovered that items No. 6, No. 9, and No. 14 had item-total correlation values that were less than 0.2. This indicates that these things do not correlate well with the overall score and may be eliminated. Hence, 11 items in all were used for analysis.
The reliability of the data was tested using Cronbach’s Alpha. Statistical tests such as mean, percentage, standard deviation, etc. were used. Factor analysis was used to condense data so that linkages and patterns could be quickly and simply comprehended. On the basis of shared variance, it is typically used to reorganize variables into small clusters.52
The profile of the respondents is given in Table 2.
 |
Table 2 Profile of the Respondents |
Results
Using Cronbach’s alpha, it was determined whether the scale designed to gauge the degree of perceived accountability of diagnostic facilities was reliable. Cronbach’s alpha has a value of 0.638. If a scale is created and used for the first time, a Cronbach’s alpha of higher than 0.60 is said to be a solid indicator of its reliability.53 As a result, it can be concluded from the current study that the scale is reliable and capable of measuring the latent variable known as accountability.
Table 3 lists, in descending order, the item statistics of the 11 items that were taken into consideration for the scale to assess customers perception of accountability.
 |
Table 3 Item Statistics |
Table 3 shows the factors contributing the most toward the favorable customers’ perception of accountability of diagnostic centres. The top three factors having the maximum impact on overall favourable customers’ perception of accountability are “getting the reports on time by the customers” (4.63), “agree to the authenticity and reliability of the reports” (4.57), and “getting timely reminders for the next tests” (4.56). The factors least important in framing the customers’ overall level of perception of accountability are, “in case of any error, running the test, again free of cost” (3.4784); “conducting a thorough inquiry to find out the cause behind the error” (3.3842); “using the latest technology prevalent in the relevant healthcare diagnostic industry for all the diagnoses and tests” (3.2010).
The scale used to gauge customers’ perceptions of responsibility had 11 components. The maximum possible score computes to be 55 (11x5), and the lowest score is 11 (11x1). Thus, the difference or range interval is 44 [55 (max)-11 (min)]. When 44 is divided by 5, the answer is 8.8. The range of 11–19.8 is reached by adding this 8.8 to the lowest possible score of 11. Similarly, the rest of the intervals correspond to many customers’ perception levels. The interpretations of customers’ perception of accountability score and overall accountability are given in Table 4.
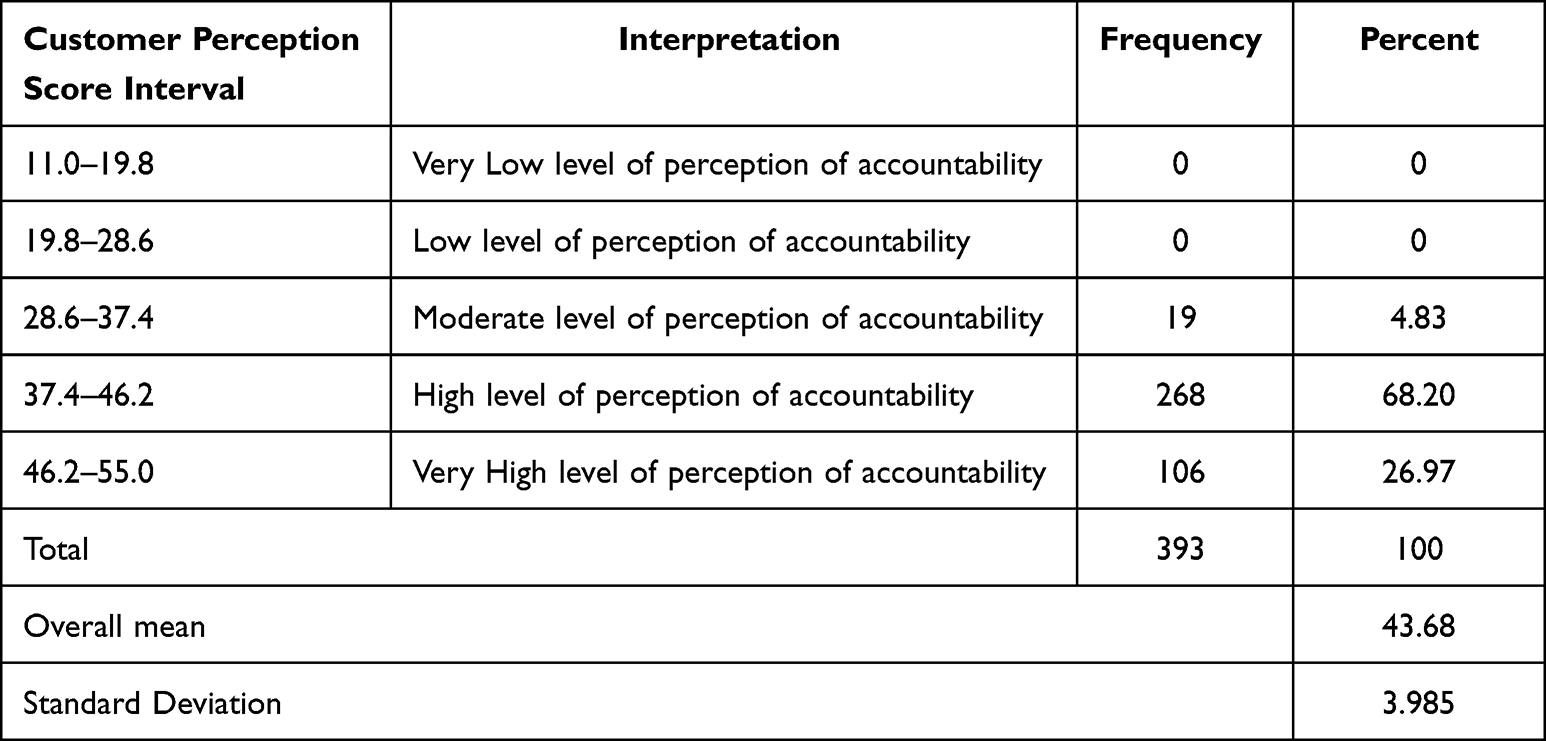 |
Table 4 Customers’ Perception of Accountability Score and Overall Accountability |
Figure 2 presents the different levels of customers perception accountability.
 |
Figure 2 Graphical representation of customers perception of accountability of diagnostic services. |
It has been noted that the overall mean score is 43.68 which lies in the interval 37.4–46.2, representing a “high level of accountability”. Hence, it may be concluded that the users of the diagnostic centres in Guwahati have a favourable perception of the accountability of diagnostic centres.
Factor Analysis
Checking the appropriateness of the sample used for the study is the first step in performing factor analysis. The Kaiser-Meyer-Olkin (KMO) measure of sample adequacy and Bartlett’s test were applied to the 393 replies in order to evaluate the data’s applicability gathered from the samples. The KMO and Bartlett’s test of sphericity determines whether there is an overlap between the variables and whether they can be reduced to a handful of parameters. The identical goal of both tests is to confirm that the original variables can be used effectively in the factor analysis. The result of the above test is presented in Table 5.
 |
Table 5 KMO and Bartlett’s Test |
The Kaiser-Meyer Olkin Measure (KMO) of Sampling Adequacy and Bartlett’s Test of Sphericity (significant level of p 0.05) should be used to examine whether the given dataset has patterned relationships and whether the data set is appropriate for exploratory factor analysis.52 The sample is sufficient as the result of KMO was 0.57, which is greater than 0.5. It is noteworthy since Bartlett’s Test of Sphericity significance value is less than 0.05.
Table 6 presents the Eigenvalues and explanation of total variance.
 |
Table 6 Total Variance Explained |
The real factors’ extraction is shown in Table 7. Only those components that satisfy the extraction method requirements are included in the section titled “Rotation Sums of Squared Loadings”. There are four components in the current study with Eigen values greater than 1. The overall variability is described in the “% of variation” column. Here, the first 4 components account for 70.78% of the total variability. As a result, the Principal Component Analysis has produced 4 components. The principal component analysis is used to identify the variables that are most closely related to each component or which of these values are of significant size. Finding the variables with low correlation to the component is made easier using this technique. Larger correlations are bolded in Table 7’s Rotated Component Matrix, which displays the results.
 |
Table 7 Rotated Component Matrix |
The rotational factor loadings are shown in Table 7. It illustrates the importance of the variables for each component and explains how the variables and components are related. Also, it highlights the things that can be put into groups and for which a single common nomenclature should be used, allowing for the reduction of the total number of elements. The final components discovered are shown in Table 8 as a last step.
 |
Table 8 Results of Factor Analysis |
Discussion
The paper addresses two research questions. RQ1 attempts to measure the level of customers’ perception of accountability of healthcare diagnostic service providers. It was found that the general level of customer perception with respect to accountability of diagnostic centres is of high level. The items such as “getting test reports delivered on time”, “perception regarding the authenticity and reliability of the reports generated by the diagnostic center”, and “getting timely reminders for tests to be done afterward”, have a substantial impact on creating the public’s favourable view of accountability. RQ2 was to find out the factors influencing the perception of accountability of healthcare diagnostic service customers. The study identifies four factors that have an impact on the perception of customers with respect to the accountability of diagnostic service providers. These are Competency, Responsiveness, Compliance with protocol, and Problem-solving approach. Meaningful accountability only results when all four factors are effective.
Veres, Locklear, and Sims (1990)54 found that the main components of competency are the information, skills, and personal qualities that employees must have in order to execute their jobs well. All of these characteristics are anticipated to have an impact on how accountable a healthcare company is. Keel (2006)55 states that competency is described as a set of behaviors that includes skills, knowledge, talents, and personal characteristics that, when combined, are essential for successfully completing work tasks. Improvements in competency lead to advancements in accountability in the same direction.56 Cherizard57 states that managerial abilities offer a solid foundation for increased accountability. This also leads to an improvement in professional accountability as propounded by Romzek and Dubnick.18 The second factor influencing the perception of customers with respect to the accountability of diagnostic service providers is responsiveness. Responsiveness entails responding readily and sympathetically to some request.9 The healthcare industry is a complicated, safety-critical field58 where technology mistakes can directly injure patients.59 A crucial component of accountability is the existence of complaint and response systems that allow interested parties to voice complaints and claim harm and obtain responses.30 Responsiveness ensures an increase in the customers’ perception of legal and professional accountability.18 The third factor influencing the perception of accountability is compliance with protocols. Compliance with protocol means adherence to laws, guidelines, regulations, and specifications applicable to healthcare diagnostic business processes. Compliance is crucial, particularly in the heavily regulated, risky healthcare sector. The ultimate purpose of compliance in the healthcare business is to offer patients with safe, high-quality care by adhering to industry norms and regulations. The fourth factor is a problem-solving approach which means identifying and analyzing the patients’ needs and providing the best solution to solve the problem which further necessitates effective communication and teamwork. Mukinda et al43 discovered that the absence of communication was perceived as a roadblock to accountability, which had an impact on the standard of care and fostered a culture of finger-pointing and shifting of blame. Proper communication facilitates solving the problem. Problem-solving approach increases the customers’ perception of political and professional accountability as suggested by Romzek and Dubnick18 and ensures the promotion of public health and community benefit as suggested by Emanuel and Emanuel.8
Hence, the four core dimensions that make an organization more accountable to its stakeholders can be explained and aligned with the accountability theories mentioned in section 2.2.
Knowledge, skills, abilities, personal traits, and other “worker-based” factors make up the first component of competency as supported by Vance, Lowry and Eggett.36 The second-factor responsiveness is responding as quickly as possible to a situation. Alertness, approachability, awareness, impartiality. Frink et al,35 supported this in the accountability theory proposed by them. The next factor is compliance with the protocol which means adherence to laws, guidelines, regulations, and specifications applicable to healthcare diagnostic business processes as supported by Blagescu et al.30 Finally, the problem-solving approach addresses the need to identify and analyze the patients’ needs and provide the best solution to solve the problem as suggested by Vance, Lowry and Eggett,38 in the accountability theory proposed by them.
Thus, it is seen that the four factors impacting the perception of customers with respect to the accountability of diagnostic service providers as identified in this study are also linked with the existing theories of accountability. A diagnostic centre to be accountable in the eyes of its customers must be responsive, comply with the protocols, employ competent personnel, and should be ready and competent enough to solve the problems of the customer. This is explained in Figure 3 as the model to study customer perception of accountability of diagnostic centres.
 |
Figure 3 Theoretical model showing customers’ perception of accountability in diagnostic centres. |
The dimensions are interconnected and have various effects on one another. A diagnostic centre must incorporate these aspects into its practices, rules, and decision-making at all levels and phases in order to be held accountable.
Academic Contribution
This paper offers the scale and accountability construct to advance healthcare research and its application. Significant contributions have been made by the present study in terms of the development of a scale to measure customers’ perception of accountability, and the development of a theoretical model to explain accountability of diagnostic centres. This study is the first of its kind in the field of healthcare diagnostics. Since customers’ perception of accountability has a crucial impact on the success of diagnostic centres, more such empirical research is expected to lead to the development of a theory in this area. Also, the scale developed in this study is reliable and since the findings of the study are validated through the existing findings, it can be inferred that the scale was valid too, and thus, the creation of a measurement scale of customers’ perception of accountability of healthcare diagnostic centres is an original theoretical contribution of this study.
Managerial Implications
Table 3 gives us the items having a mean value of more than 4 which further facilitates the management of a healthcare diagnostic centre to focus on those factors which have relatively more impact on overall accountability. These factors can be summarized as timely delivery of reports and reminders, authenticity and reliability of reports, being responsive by giving justifiable reasons, and requirement of requisite qualifications. Providers and supervisors of diagnostic services, therefore, require supportive organizational settings that better enable such accountability approaches.43 At the level of the individual and the organization, there is a requirement for the promotion of a “just culture” of accountability, education, and development.60 Training programs must put an emphasis on empowering healthcare workers.61 The training should include the particular ways in which the rules and laws relate to the work that the employees of diagnostic services undertake as well as the problems with daily healthcare compliance that they really run into. By getting this kind of targeted, hands-on training, employees may learn what to look for and how to apply policies and procedures to specific situations.
Healthcare services are particularly sensitive about time management; thus, providers and managers need supportive organizational frameworks. All healthcare workers should utilize efficient time management techniques to carry out their duties and care for patients.45,52
All workers in the healthcare sector should be aware of how to spend time effectively and efficiently in order to carry out their duties and care for patients. They must also be able to define the aims and objectives required to carry out their individual professional responsibilities. Additionally, evolving trends and the character of the workforce demand that workers take on more personal responsibility and apply self-management techniques.31
Policy Implications
The ability to detect and foster ideas to promote accountability and raise the standard of diagnostic services is made possible by this expanded understanding of accountability. Accountability comes in many forms, and there are numerous ways to fulfil it. A strong level of commitment inside the organization at the Board and senior management levels is necessary for the dimensions to be implemented effectively and for organizations and stakeholders to benefit equally from responsibility.30
Service providers and the health administration were largely held responsible for their performance by the Ministry of Health and other government authorities.62 A diagnostic centre should have a written statement of its promises to the client groups it serves regarding the services and/or plans that are being or will be offered to them. The document or charter may include protocols to be followed, the justification to be given for some procedures, timely delivery of test reports, and reminders of the next tests which would further enhance the responsiveness and problem-solving approach of the diagnostic centre.63 There should be a proper mechanism to ensure transparency regarding the qualifications and competencies of the pathologists and the lab technicians.64 The patient or the customer should be educated beforehand about the procedure and actions to be performed by the diagnostic centre for a particular test. It is imperative to make strong policies and procedures available and accessible which, in turn, helps ensure compliance.65 The policies should clearly spell out the expectations, which helps drive organizational accountability. Fines may be imposed by government regulatory agencies based on the degree of non-compliance.66 Due to this, accountability methods must emphasize empowerment and solidarity while also acknowledging the personal risk posed by those who are most negatively impacted by a lack of accountability.62 There should be a Grievance redressal System through help desks, call centres, and web portals to form a health system that is more responsive to health needs. Even though accountability is a key element in enhancing the governance and management of healthcare organizations and systems, a relationship may be developed with a focus on learning and improvement that goes beyond control and sanctions.67
Scope of Future Research
Only consumers of diagnostic centres in Guwahati are included in the current study. There is therefore potential for extensive research to be done across the entirety of Assam.68 It is possible to research both customer experience and perceptions of accountability. An exploratory study can be conducted to learn how they perceive accountability in relation to various demographic factors and to see how accountability perception levels affect patient satisfaction. Customers’ perceptions of the diagnostic centre’s accountability are influenced by a variety of variables, and not all of these variables are equally significant. There is a relationship between the parameters, and Social Network Analysis was utilized by Kajol, Nath et al,69 and Singh et al,70 to determine this association. Each of the aspects, such as the diagnostic centre’s competence, responsiveness, protocol, and problem-solving strategy, can be studied in greater detail. It is possible to conduct a cross-sectional and longitudinal investigation.
Conclusion
In summary, this study shows how important accountability in diagnostic centres is for providing clients with a great service experience.68 The overall mean score is found to be 43.68 (Table 4), which says that the perception of accountability is favourable. Most importantly, the study gives us the scale and four dimensions (Figure 3) to measure accountability in diagnostic centres, which is first of its kind, besides highlighting the most important and least important factors influencing the customers’ perception of accountability in a diagnostic centre (Table 3). Hence, the implicit commitment made by healthcare providers and organizations to patients to exercise reasonable care, behave competently, and deliver healing—is a crucial component of any complicated healthcare system.11 Accountability should be viewed as an ongoing process that may be improved, not as a problem that needs to be solved. The nature of the interactions between patients, professionals, and healthcare organizations forms the foundation of healthcare. To encourage improved learning and improvement beyond control and punishments, healthcare delivery services should be backed by their duty.71 Finally, there is a need to reconsider the issues surrounding the goals of accountability initiatives in the health sector. One could think about the citizenship of people who use it, as well as the work ethics of those who are system users, and the relationship between them in addition to the effectiveness and quality of the health services.
Ethical Statement
1. Full name of the ethics committee
(a) Prof. Vijaishri Tewari, Professor, Indian Institute of Information Technology Allahabad, Prayagraj, India
(b) Prof. Vrijendra Singh, Professor, Indian Institute of Information Technology Allahabad, Prayagraj, India
(c) Dr Shailendra Kumar, Associate Professor, Indian Institute of Information Technology Allahabad, Prayagraj, India
(d) Dr Anurag Singh, Associate Professor, Institute of Management, Banaras Hindu University, Varanasi, India
2. It is hereby declared and confirmed that informed consent was obtained from the study participants;
3. It is hereby declared and confirmed that the guidelines outlined in the Declaration of Helsinki were followed.
Acknowledgments
The first author thanks the Apollo Clinic for providing her opportunity to pursue this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Dhagarra D, Goswami M, Kumar G. Impact of trust and privacy concerns on technology acceptance in healthcare: an Indian perspective. Int J Med Inform. 2020;141:104164. doi:10.1016/j.ijmedinf.2020.104164
2. Day RM, Demski RJ, Pronovost PJ, et al. Operating management system for high reliability: leadership, accountability, learning and innovation in healthcare. J Patient Saf Risk Manag. 2018;23(4):155–166. doi:10.1177/2516043518790720
3. Brandsma GJ, Schillemans T. The accountability cube: measuring accountability. J Public Adm Res Theory. 2013;23(4):953–975. doi:10.1093/jopart/mus034
4. Hendee WR. Safety and accountability in healthcare from past to present. Int J Radiat Oncol Biol Phys. 2008;71(1):S157–S161. doi:10.1016/j.ijrobp.2007.04.096
5. Deber RB. Thinking about accountability. Healthcare Policy. 2014;10(SP):12.
6. Bearman GM, Vokes RA. Averting a betrayal of trust: system and individual accountability in healthcare infection prevention. Infect Control Hosp Epidemiol. 2019;40(8):918–919. doi:10.1017/ice.2019.137
7. Tetlock PE. Accountability and complexity of thought. J Pers Soc Psychol. 1983;45(1):74. doi:10.1037/0022-3514.45.1.74
8. Emanuel EJ, Emanuel LL. What is accountability in health care? Ann Intern Med. 1996;124(2):229–239. doi:10.7326/0003-4819-124-2-199601150-00007
9. Thomas PG. The changing nature of accountability. Taking Stock: Assessing Public Sector Reforms. 1998;2:348–393.
10. Priyadarshi M, Kumar S. Accountability in healthcare in India. Indian J Community Med. 2020;45(2):125. doi:10.4103/ijcm.IJCM_224_19
11. Habli Z, AlChamaa W, Saab R, Kadara H, Khraiche ML. Circulating tumor cell detection technologies and clinical utility: challenges and opportunities. Cancers. 2020;12(7):1930. doi:10.3390/cancers12071930
12. Kaini BK. Healthcare governance for accountability and transparency. J Nepal Health Res Counc. 2013;11(23):109–111.
13. Demirag I, Fırtın CE, Tekin Bilbil E. Managing expectations with emotional accountability: making City Hospitals accountable during the COVID-19 pandemic in Turkey. J Public Budg Account Financ Manag. 2020;32(5):889–901. doi:10.1108/JPBAFM-07-2020-0097
14. Boysen PG. Just culture: a foundation for balanced accountability and patient safety. Ochsner J. 2013;13(3):400–406.
15. Batalden PB, Davidoff F. What is “quality improvement” and how can it transform healthcare? BMJ Qual Saf. 2007;16(1):2–3. doi:10.1136/qshc.2006.022046
16. Nurunnabi M, Kamrul Islam S. Accountability in the Bangladeshi privatized healthcare sector. Int J Health Care Qual Assur. 2012;25(7):625–644. doi:10.1108/09526861211261226
17. Witvliet CV, Jang SJ, Johnson BR, et al. Transcendent accountability: construct and measurement of a virtue that connects religion, spirituality, and positive psychology. J Posit Psychol. 2023;2023:1–4.
18. Romzek BS, Dubnick MJ. Accountability. In: Defining Public Administration. Routledge; 2018:382–395.
19. Pine K, Mazmanian M. Emerging insights on building infrastructure for data-driven transparency and accountability of organizations.
20. Sánchez-Bayón A, González-Arnedo E, Andreu-Escario Á. Spanish healthcare sector management in the COVID-19 crisis under the perspective of Austrian economics and new-institutional economics. Front Public Health. 2022;10:801525. doi:10.3389/fpubh.2022.801525
21. Eisenhardt KM, Graebner ME. Theory building from cases: opportunities and challenges. Acad Manage J. 2007;50(1):25–32. doi:10.5465/amj.2007.24160888
22. Magliocca NR, Ellis EC, Allington GR, et al. Closing global knowledge gaps: producing generalized knowledge from case studies of social-ecological systems. Glob Environ Change. 2018;50:1–4. doi:10.1016/j.gloenvcha.2018.03.003
23. Elster J. Accountability in Athenian politics. Democracy Account Representation. 1999:1;253–278.
24. Schedler A, Diamond LJ, Plattner MF, editors. The Self-Restraining State: Power and Accountability in New Democracies. Lynne Rienner Publishers; 1999.
25. Schillemans T. The public accountability review. A meta-analysis of public accountability research in six academic disciplines; 2013.
26. Bovens M, Goodin RE, Schillemans T, editors. The Oxford Handbook Public Accountability. Oxford handbooks; 2014.
27. Cleary SM, Molyneux S, Gilson L. Resources, attitudes and culture: an understanding of the factors that influence the functioning of accountability mechanisms in primary health care settings. BMC Health Serv Res. 2013;13(1):1. doi:10.1186/1472-6963-13-320
28. Moncrieffe J. Relational Accountability: Complexities of Structural Injustice. Bloomsbury Publishing; 2011.
29. Brinkerhoff DW. Accountability and Health Systems: Overview, Framework, and Strategies. Bethesda, MD: Partners for Health Reformplus Project, Abt Associates; 2003.
30. Blagescu M, de Las Casas L, Lloyd R. Pathways to accountability. GAP Framework. 2005;19:2019.
31. Dose JJ, Klimoski RJ. Doing the right thing in the workplace: responsibility in the face of accountability. Empl Responsib Rights J. 1995;8(1):35–56. doi:10.1007/BF02621254
32. Pawlson LG, Torda P, Roski J, O’Kane ME. The role of accreditation in an era of market-driven accountability. Am J Manag Care. 2005;11(5):290–293.
33. Frink DD, Klimoski RJ. Advancing accountability theory and practice: introduction to the human resource management review special edition. Hum Resour Manage Review. 2004;14(1):1–7. doi:10.1016/j.hrmr.2004.02.001
34. Cavill S, Sohail M. Improving public urban services through increased accountability. J Prof Issues Eng Educ Pract. 2005;131(4):263–273. doi:10.1061/(ASCE)1052-3928(2005)131:4(263)
35. Frink DD, Hall AT, Perryman AA, et al. Meso-level theory of accountability in organizations. In: Research in Personnel and Human Resources Management. Emerald Group Publishing Limited; 2008:177–245. doi:10.1016/S0742-7301(08)27005-2
36. Vance A, Lowry PB, Eggett D. Using accountability to reduce access policy violations in information systems. J Manag Inf Syst. 2013;29(4):263–290. doi:10.2753/MIS0742-1222290410
37. Mansbridge J. A contingency theory of accountability; 2014.
38. Vance A, Lowry PB, Eggett D. Increasing accountability through user-interface design artifacts: a new approach to addressing the problem of access-policy violations. MIS Q. 2015;39(2):345–366. doi:10.25300/MISQ/2015/39.2.04
39. Black JA, Smith YS, Keels JK. The Millennial generation and personal accountability: spiritual and classroom implications. Christ Bus Acad Rev. 2014;9:1.
40. Vaishnav LM, Mehendale A. Effectiveness of training program on awareness among nursing staff, lab technicians and sanitary workers regarding bio-medical waste management in a Tertiary Care Hospital in central India. Eur J Mol Clin Med. 2020;1:2091–2098.
41. Abdallah AA, Improta G. Healthcare engineering: a lean management approach. J Healthc Eng. 2020;2020:1–17. doi:10.1155/2020/8875902
42. Bavoria S, Nongkynrih B, Krishnan A. Health workforce availability and competency to manage noncommunicable diseases at secondary care level hospitals of Delhi. Int J Noncommunicable Dis. 2019;4(2):38–42. doi:10.4103/jncd.jncd_10_19
43. Mukinda FK, Van Belle S, Schneider H. Perceptions and experiences of frontline health managers and providers on accountability in a South African health district. Int J Equity Health. 2020;19(1):1. doi:10.1186/s12939-020-01229-w
44. Nightingale A. Implementing collective leadership in healthcare organisations. Nurs standard. 2020;35(5):53–57. doi:10.7748/ns.2020.e11448
45. Kidak LB. Hastane yöneticilerinin zaman yönetimi tutumlarının belirlenmesi: izmir ili eğitim ve araştırma hastaneleri uygulaması [Determining the Time Management Attitudes of Hospital Managers: Izmir Province Training and Research Hospitals Application]. Selçuk Üniversitesi Sosyal Bilimler Enstitüsü Dergisi [Journal of Selçuk University Social Sciences Institute]. 2011;2(25):159–172.
46. Özel Y, Hasgül E, Duzcu T. The examination of time management skills of healthcare professions. Res Humanit Soc Sci. 2018;8:42.
47. Putturaj M, Van Belle S, Engel N, et al. Multilevel governance framework on grievance redressal for patient rights violations in India. Health Policy Plan. 2021;36(9):1470–1482. doi:10.1093/heapol/czab066
48. Hernandez-Boussard T, Bozkurt S, Ioannidis JP, Shah NH. MINIMAR (MINimum Information for Medical AI Reporting): developing reporting standards for artificial intelligence in health care. J Am Med Inform Assoc. 2020;27(12):2011–2015. doi:10.1093/jamia/ocaa088
49. Al-Omar LT, Anderson SL, Cizmic AD, Vlasimsky TB. Implementation of a pharmacist-led diabetes management protocol. Am Health Drug Benefits. 2019;12(1):14.
50. Taymaz S, Iyigun C, Bayindir ZP, Dellaert NP. A healthcare facility location problem for a multi-disease, multi-service environment under risk aversion. Socioecon Plann Sci. 2020;71:100755. doi:10.1016/j.seps.2019.100755
51. Shehada AK, Albelbeisi AH, Albelbeisi A, El Bilbeisi AH, El Afifi A. The fear of COVID-19 outbreak among health care professionals in Gaza Strip, Palestine. SAGE Open Med. 2021;9:20503121211022987. doi:10.1177/20503121211022987
52. Yong AG, Pearce S. A beginner’s guide to factor analysis: focusing on exploratory factor analysis. Tutor Quant Methods Psychol. 2013;9(2):79–94.
53. Nunnally JC. Psychometric Theory.
54. Veres JG, Locklear TS, Sims RR. Job analysis in practice: a brief review of the role of job analysis in human resources management. Hum Resour Manage. 1990;8(5):79–103.
55. Keel J. Toolkit, glossary state of Texas State classification; 2006. Available from: http://www.hr.state.tx.us/workforce/glossary.html.
56. Bakalikwira L, Bananuka J, Kaawaase Kigongo T, Musimenta D, Mukyala V. Accountability in the public health care systems: a developing economy perspective. Cogent Bus Manag. 2017;4(1):1334995. doi:10.1080/23311975.2017.1334995
57. Cherizard CM. Ethical Leadership Effects on Medical Laboratory Personnel Accountability Behaviors [doctoral dissertation]. Walden University; 2022.
58. Wachter RM. Personal accountability in healthcare: searching for the right balance. BMJ Qual Saf. 2013;22(2):176–180. doi:10.1136/bmjqs-2012-001227
59. Sittig DF, Singh H. A new sociotechnical model for studying health information technology in complex adaptive healthcare systems. BMJ Qual Saf. 2010;19(Suppl 3):i68–i74. doi:10.1136/qshc.2010.042085
60. Hilber AM, Blake C, Bohle LF, Bandali S, Agbon E, Hulton L. Strengthening accountability for improved maternal and newborn health: a mapping of studies in Sub-Saharan Africa. Int J Gynecol Obstet. 2016;135(3):345–357. doi:10.1016/j.ijgo.2016.09.008
61. Rao D, Dhakshaini MR, Kurthukoti A, Doddawad VG. Biomedical waste management: a study on assessment of knowledge, attitude and practices among health care professionals in a tertiary care teaching hospital. Biomed Pharmacol J. 2018;11(3):1737–1743. doi:10.13005/bpj/1543
62. Boydell V, Schaaf M, George A, Brinkerhoff DW, Van Belle S, Khosla R. Building a transformative agenda for accountability in SRHR: lessons learned from SRHR and accountability literatures. Sex Reprod Health Matter. 2019;27(2):64–75. doi:10.1080/26410397.2019.1622357
63. Brinkerhoff DW. Accountability and health systems: toward conceptual clarity and policy relevance. Health Policy Plan. 2004;19(6):371–379. doi:10.1093/heapol/czh052
64. Nunes R, Brandao C, Rego G. Public accountability and sunshine healthcare regulation. Health Care Anal. 2011;19:352–364. doi:10.1007/s10728-010-0156-6
65. Olsen JP. Accountability and ambiguity. In: The Oxford Handbook of Public Accountability. Oxford University Press Oxford; 2014:106–123.
66. Miller HD. Measuring and assigning accountability for healthcare spending. Center for Healthcare Quality and Payment Reform; 2014. Available from: http://www.chqpr.org/downloads/AccountabilityforHealthcareSpending.pdf(21.03.2017).
67. Denis JL. Accountability in healthcare organizations and systems. Healthcare Policy. 2014;10(SP):8.
68. Singh R, Agarwal S, Pandiya B. Customer experience in diagnostic centres: an empirical study. Acad Market Stud J. 2022;26(3):1–5.
69. Kajol K, Nath M, Singh R, Singh HR, Das AK. Factors affecting seasonality in the stock market: a social network analysis approach. Int J Account Finance Rev. 2020;5(4):39–59. doi:10.46281/ijafr.v5i4.888
70. Singh R, Bhattacharjee J, Kajol K. Factors affecting risk perception in respect of equity shares: a social network analysis approach. Vision. 2021;2021:09722629211046082.
71. Kerkvoorden DV, Ettema R, Minkman M. Accountability in healthcare in the Netherlands: a scoping review; 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Erosion of Healthcare and Scientific Integrity: A Growing Concern

Brücher BL
Journal of Healthcare Leadership 2025, 17:23-43
Published Date: 21 February 2025