Back to Journals » Clinical Epidemiology » Volume 15
Current Trends in Comorbidity Prevalence and Associated Mortality in a Population-Based Cohort of Hip Fracture Patients in Denmark
Authors Kristensen PK ![]() , Hjelholt TJ, Madsen M
, Hjelholt TJ, Madsen M ![]() , Pedersen AB
, Pedersen AB ![]()
Received 13 March 2023
Accepted for publication 21 June 2023
Published 18 July 2023 Volume 2023:15 Pages 839—853
DOI https://doi.org/10.2147/CLEP.S410055
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
Pia Kjær Kristensen,1,2 Thomas Johannesson Hjelholt,3,4 Morten Madsen,3 Alma B Pedersen2,3
1Department of Orthopedic Surgery, Aarhus University Hospital, Aarhus, Denmark; 2Department of Clinical Medicine, Aarhus University, Aarhus, Denmark; 3Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 4Department of Internal Medicine, Viborg Regional Hospital, Viborg, Denmark
Correspondence: Pia Kjær Kristensen, Department of Orthopedic Surgery, Aarhus University Hospital, Palle Juul-Jensens Boulevard 165, Aarhus, 8200, Denmark, Tel +45 78454111, Email [email protected]
Background and Purpose: Patients with hip fractures often have comorbidities, but detailed data on comorbidity and its impact on prognosis are lacking. We described the current trends in the prevalence of comorbidity and the magnitude of the associated mortality.
Patients and Methods: From the Danish Multidisciplinary Hip Fracture Registry we included 31,443 hip fracture patients (diagnosed in 2014– 2018). We calculated the prevalence of individual diseases and comorbidity measured with the Charlson Comorbidity Index (CCI), the Elixhauser Index, and the Rx-Risk Index. We calculated sex and age-adjusted odds ratios (aORs) for 30-day mortality and hazard ratios (aHRS) for one-year mortality with 95% confidence intervals (CI).
Results: The most common diseases identified with the CCI were cerebrovascular diseases (18%), malignancies (17%), chronic pulmonary disease (14%), and dementia (11%). Using the Elixhauser Index, hypertension (37%), cardiac arrhythmias (21%), and fluid and electrolyte disorders (15%) were most prevalent, while ischemic heart disease (42%), hypertension (39%), and use of antiplatelets (37%) were most prevalent when using the Rx-Risk Index. Using the Rx-Risk Index, only 28% of patients had no comorbidity compared to 38% for CCI and 44% for the Elixhauser Index, and the prevalence was stable through the years. Compared to patients with no comorbidity, patients with very severe comorbidity had an aORs for 30-day mortality of 2.6 (CI: 2.4– 2.9) using CCI, 2.6 (CI: 2.4– 3.1) using the Elixhauser Index, and 3.1 (CI: 2.7– 3.4) using the Rx-Risk Index.
Interpretation: More than 50% of the patients with hip fractures have moderate to very severe comorbidity, with considerable variation between indices. The prevalence of individual diseases varies considerably. All indices had comparable dose-response associations with mortality. These results are relevant for clinicians to amend prevention and target care, and for researchers to decide which comorbidity measure to use depending on the research question.
Keywords: Charlson Comorbidity Index, comorbidity, Elixhauser Index, hip fracture, mortality, Rx-Risk
Introduction
Along with the population aging, advances in medical care have contributed to an increase in hip fracture incidence and the prevalence of comorbidity among patients.1–3 The presence of comorbidities is associated with more complex clinical management of patients with hip fractures4 and worse patient outcomes, including prolonged length of hospital stay, poorer quality of in-hospital treatment, increase in postoperative infections, and mortality.5,6
The prevalence of comorbidity among hip fracture patients has previously been examined using the Charlson Comorbidity Index (CCI) or the Elixhauser Index based on hospital diagnoses.2,3 However, several chronic diseases included in these indices, eg, chronic pulmonary disease and diabetes mellitus, are today mainly treated by general practitioners in contrast to previous standards where patients were seen regularly at hospital outpatient clinics.7 It is therefore a concern that comorbidity estimates based on hospital diagnoses might underestimate the true comorbidity. A prescription-based index, like the Rx-Risk Index, captures comorbidities currently treated not only at hospitals but also by general practitioners and may therefore provide a more precise description of the current comorbidity.8
To our knowledge, no previous studies have examined whether the comorbidity burden measured with the hospital diagnosis-based CCI and Elixhauser Index is different than the comorbidity burden measured with the prescription-based Rx-Risk Index, and whether the prevalence of individual diseases differ between indices. Furthermore, no previous studies have examined whether the strength of the reported associations between comorbidity and mortality differs between indices. Current comprehensive data on the comorbidity, individual diseases, as well as associated mortality are necessary to inform patients and clinicians, facilitate diagnosis, improve target care, lower health care costs related to complications and increase quality of care. In addition, the study is relevant for research purposes in terms of confounding adjustment and comparison of results of the studies that use only prescriptions or diagnoses as a measure of comorbidity.9
The aim of this study was therefore to describe the current trends in the prevalence of individual diseases and comorbidity measured with two diagnosis-based indices, the CCI and the Elixhauser Index, and a prescription-based index, the Rx-Risk Index. Furthermore, we examined the strengths of the association between comorbidity and 30-day and one-year mortality using the three indices.
Methods
We conducted a population-based cohort study in Denmark, a country with 5.7 million inhabitants and with universal access to medical care, including partial reimbursement of prescription drug costs.10
Study Population and Data Sources
Study population included patients with an incident medial femoral neck or lateral fracture of the proximal femur who underwent surgery with arthroplasty or internal fixation from January 2014 through December 2018. Patients were identified in the Danish Multidisciplinary Hip Fracture Registry.11 We linked the study population with data from the Danish Civil Registration System, the Danish National Patient Registry, the Danish National Health Services Prescription Database, and socioeconomic registries from Statistics Denmark. All registries are updated once a year, except for the Danish National Patient Registry and the Danish Civil Registration System, which are updated on a monthly and a daily basis, respectively.
The Danish Multidisciplinary Hip Fracture Registry is a national clinical quality registry, which records all patients aged 65 years or older with femoral fractures who underwent surgery from 2003 onwards. The registry contains detailed data on patient characteristics and in-hospital quality indicators reflecting the guidelines for in-hospital care at the time of registration. By law, reporting to the registry is mandatory for all departments treating hip fracture patients and data are entered prospectively by the healthcare professionals during the hospital stay.11 Furthermore, the hospital only gets paid if both the diagnosis code and the surgical code are reported.
The Danish National Patient Registry holds data on all non-psychiatric hospital admissions since 1977 and on all outpatient and emergency visits since 1995, recorded according to the International Classification of Diseases Eight Revision (ICD-8) until the end of 1993 and Tenth Revision (ICD-10) thereafter.12
The Civil Registry System holds records of changes in vital status and migration for the entire Danish population since 1968.12
The Danish National Prescription Registry contains information on all dispensing of reimbursed medicine by the community pharmacies in Denmark since 2004. The pharmacies serve all inhabitants including nursing home residents.13 The recorded data include active substances of the medications recorded according to the Anatomical Therapeutic Chemical classification system (ATC codes), date of purchase, and the defined daily dose.
The socioeconomic registries at Statistics Denmark contain detailed information on the level of education, employment status, household income, cohabitant status, nursing home residence, and regional residency of all Danish residents.14,15
Patient Characteristics
We described the study population in terms of sex, age at hip fracture date (in categories 65–74 years, 75–84 years, and 85 years or older), cohabitation (living alone or living with someone), fracture type (medial or lateral fracture), type of residence (own home, nursing home, or missing) and Body mass index (BMI). BMI was classified into underweight (BMI 10–19.9 kg/m2), normal weight (BMI 20.0–24.9 kg/m2), overweight (25–29.9 kg/m2), and obese (30–51 kg/m2) according to the criteria used at the Danish Multidisciplinary Hip Fracture Registry.11 To account for variation in annual family income, we calculated the average annual total household income in the five years before admission to hospital and categorized it into three terciles of increasing income.16 We classified level of education into elementary school (≤7 years), more than elementary school, but not university degree, university degree, and missing values.16 Lastly, we described the study population by region of residence (the Capital Region of Denmark, Region Zealand, the Region of Southern Denmark, the Central Denmark Region, and the Northern Denmark Region).
Comorbidity
We defined comorbidity as medical conditions that existed before the hip fracture admission date and identified the level of comorbidity in each patient using two most common studied hospital diagnosis-based indices, the CCI17 and the Elixhauser Index,18 and an outpatient prescription-based index, the Rx-Risk Index.8
The CCI was originally developed in a cohort of 559 medical patients to predict 1-year mortality and consisted of 19 comorbidity categories, which were included in a weighted index.19 The index has been translated into ICD codes, which are used in administrative registries.20 The included codes have been validated in the Danish National Patient Registry showing positive predictive values from 82% to 100%.21 The index includes 19 medical conditions, which are weighted by 1 to 6 points according to their risk of mortality.19 The sum of all scores constitutes a single comorbidity score for each patient. In our study patients were categorized into four groups depending on the CCI score (0, 1, 2, and ≥3) corresponding to no comorbidity, moderate, severe, and very severe comorbidity.22
The Elixhauser Index was originally developed in a cohort of 438 adult inpatients from acute care hospitals in the USA to predict in-hospital mortality, length of hospital stay, and hospital charges using 30 comorbidities.18 The score was developed based on ICD-9 and did not include a summary score. However, the index has been translated into ICD-10 and a point system.20 The points assigned to each disease range from −7 to 12 depending on the association with mortality. For each patient we calculated a summary score by summing points for all included diseases in the index and categorized into four groups; no comorbidity (≤0 points), moderate comorbidity (1–5 points), severe comorbidity (6–13 points), and very severe comorbidity (≥14 points).23
The Rx-Risk Index was developed in 2003 providing an up-to-date list of the medication-based measure of comorbidity (the Chronic Disease Score, CDS), which was developed in 1992 for predicting costs of healthcare and subsequently adapted to predict mortality in outpatient populations.24 The Rx-Risk Index includes 43 comorbidities, which have been mapped to pharmacy dispensing indicative of each condition using ATC codes. Each comorbidity have a weighted index score depending on the association with mortality.8 An increasing score indicates a higher level of comorbidity. We categorized the RxRiisk score into four groups by quartiles of increasing Rx-Risk score, which correspond to no comorbidity, moderate, severe, and very severe comorbidity.
We summarized the 10-year pre-hip fracture comorbidity history using primary and secondary diagnoses from all inpatient and outpatient visits (excluding emergency department visits) recorded in the Danish National Patient Registry. We obtained information about outpatient dispensing from the Danish National Prescription Registry. For the Rx-Risk Index, the patients were categorized as having been treated for the comorbidity if they received medicine in a given disease category one or more times within one year before the hip fracture admission date. The ICD codes and the ATC codes included in the three indices are shown in Supplemental Table S1A–C.
Outcome
The outcome variables 30-day and all-cause one-year mortality were chosen as they represent short-term (likely to be related to hip fracture injury and the surgery itself) and long-term mortality (likely to be related to patient characteristics and comorbidity). All-cause mortality within 30 days and one year from the day of hip fracture surgery were obtained from the Civil Registration System.
Statistical Analysis
We tabulated the characteristics of the study population overall and by each comorbidity index. We compared the prevalence of individual diseases and the prevalence of comorbidity measured with the CCI, the Elixhauser Index, and the Rx-Risk Index. Furthermore, we compared the indices’ categorization of comorbidity level using a cross-tabulation of the distribution of comorbidity levels between two indices. Subsequently, we examined the current trend in the prevalence of comorbidity throughout the study period. Lastly, we examined the crude as well as the sex and age adjusted association between comorbidity and 30-day and one-year mortality for each index separately. The association between comorbidity level and 30-day mortality were examined using logistic regression for each index. The prognostic value of comorbidity in relation to one-year mortality was assessed by calculating Hazard Ratios (HRs) using the Cox proportional hazards regression model. The Cox proportional hazards regression is a more appropriate method when dealing with common outcomes and long follow-up time. The patients were followed from the date of surgery until the date of death or emigration, whichever occurred first within the first year after the date of surgery. We calculated HR and Odds ratio (OR) overall and stratified. We stratified on sex (in categories male and female), age groups (in categories 65–74 years, 75–84 years, and 85 years or older, and in each calendar year of surgery as the comorbidity level may have changed over the years and to examine potential effect modification. The content of this paper follows the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines.25 All statistical analyses were performed using SAS statistical software version 9.4 (SAS Institute Inc., Cary, USA).
Results
In total, we identified 31,443 patients with a hip fracture in the period 2014–2018. The overall hip fracture population mainly consisted of females and individuals above 85 years of age. Most of the population was living alone and was admitted to hospital from their own homes. The proportion of men increased with the severity of comorbidity for all indices, eg, 25% in the no comorbidity group were men compared to 40% in the very severe comorbidity group measured with CCI (Table 1)). The age distribution was comparable for all four comorbidity groups in the CCI, the Elixhauser Index, and the Rx-Risk Index (Table 1). A more detailed description of the study population is available in Supplemental Table S2.
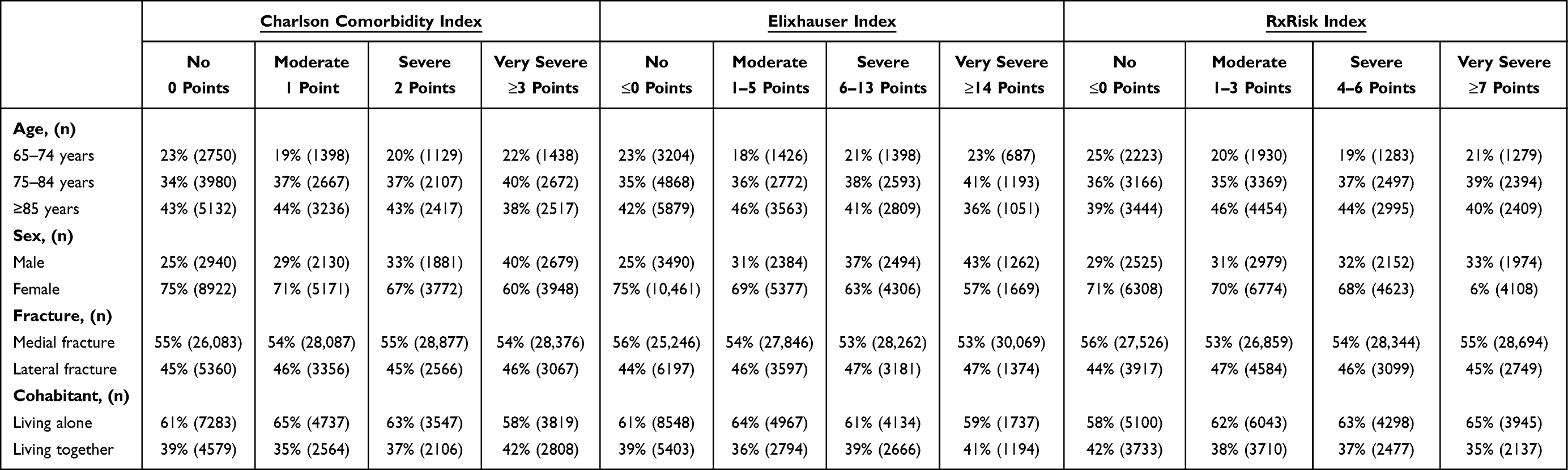 |
Table 1 Baseline Characteristics for Patients with Hip Fracture According to Comorbidity Level Measured with Charlson Comorbidity, Elixhauser, and RxRisk Indices |
The Prevalence of the Individual Diseases
Seven diseases were identified in all three indices: Chronic pulmonary disease, congestive heart failure, uncomplicated diabetes, renal disease, liver disease, malignancies, and HIV/AIDS (Figure 1). The prevalence of these diseases was the same in the CCI and the Elixhauser except for renal disease and malignancies where the CCI showed a slightly higher prevalence (Table 2). According to the Rx-Risk Index, 28% of the hip fracture patients had congestive heart failure, whereas the prevalence was only 9% in both the CCI and the Elixhauser Index. No patients with renal disease or malignancies were identified with the Rx-Risk Index in contrast to the CCI and the Elixhauser Index (Table 2). The CCI and the Elixhauser Index both included additional seven diseases compared to Rx-Risk Index, including metastatic cancer, complicated diabetes, peptic ulcer disease, rheumatological disease, lymphoma, peripheral vascular disease, and paraplegia/hemiplegia (Figure 1). The prevalence of these diseases was the same in both indices apart from those for complicated diabetes and peptic ulcer disease (Table 2). The CCI and the Rx-Risk Index both included dementia, with the CCI showing a slightly higher prevalence than the Rx-Risk Index (Table 2). The Elixhauser and Rx-Risk indices shared five diseases, including cardiac arrhythmias, hypertension, hypothyroidism, alcohol abuse, and depression (Figure 1). According to the Rx-Risk Index 29% of the hip fracture patients had depression compared to 6% according to the Elixhauser Index (Table 2). In contrast, the Elixhauser Index showed that 21% of the patients were diagnosed with cardiac arrhythmias whereas the prevalence was only 6% according to the Rx-Risk Index (Table 2).
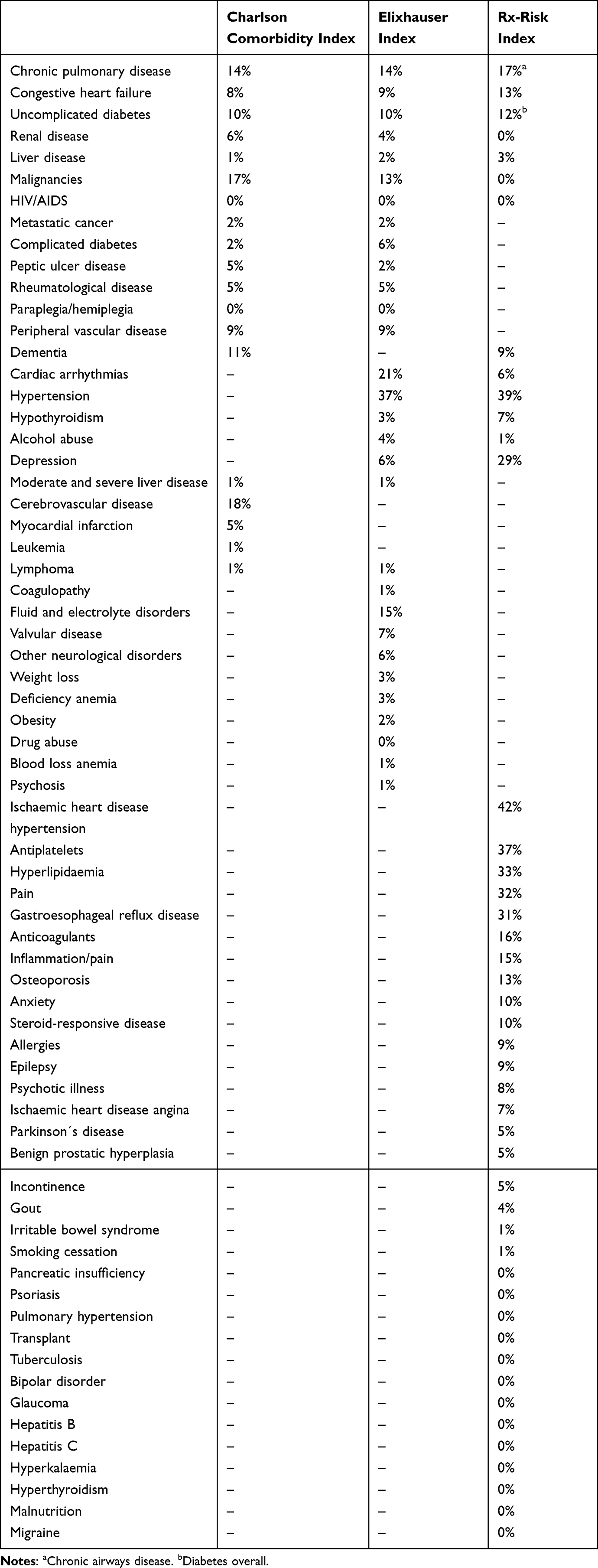 |
Table 2 Prevalence of Individual Diseases Measured with the Different Indices |
 |
Figure 1 The disease areas included in the three indices. |
The Comorbidity
The prevalence of comorbidity in our study population was highest when using the Rx-Risk Index (72%) and lowest when using the Elixhauser Index (56%). The proportion of very severe comorbidity was 21% and 19% in the CCI and the Rx-Risk Index, respectively, whereas it was only 9% in the Elixhauser Index. Using CCI, 38% of the patients were categorised as having no comorbidity, whereas 78% were categorized as having no comorbidity using the Elixhauser Index and 45% using the Rx-Risk Index (Figure 2A–C). Among the patients categorized with very severe comorbidity using the CCI, 33% and 34% were also categorized as having very severe comorbidity using the Rx-Risk Index and the Elixhauser Index, respectively (Figure 2A–C). Among the patients categorized with very severe comorbidity using the CCI, 34% were also categorized as having very severe comorbidity using the Rx-Risk Index. The prevalence of comorbidity groups within each index did not change from 2014 to 2018 for any of the indices (Figure 3A–C).
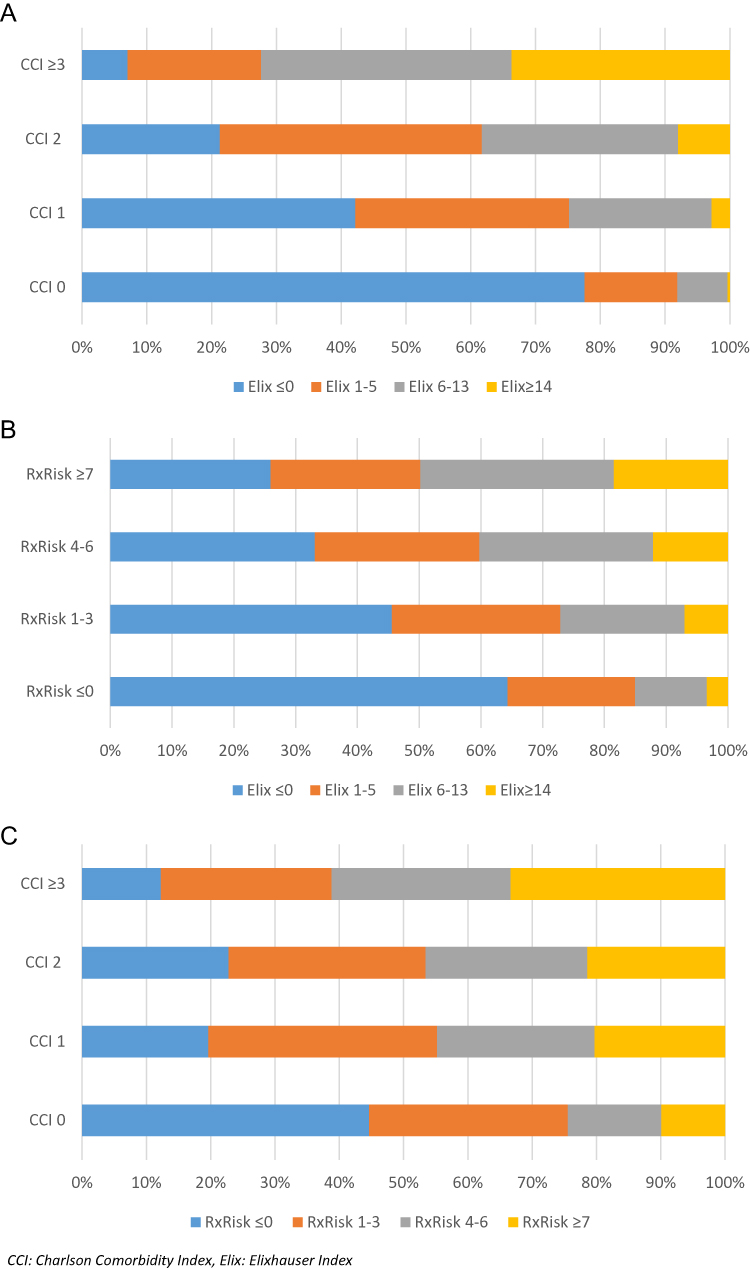 |
Figure 2 (A–C) Concordance between two indices categorisation of comorbidity level. |
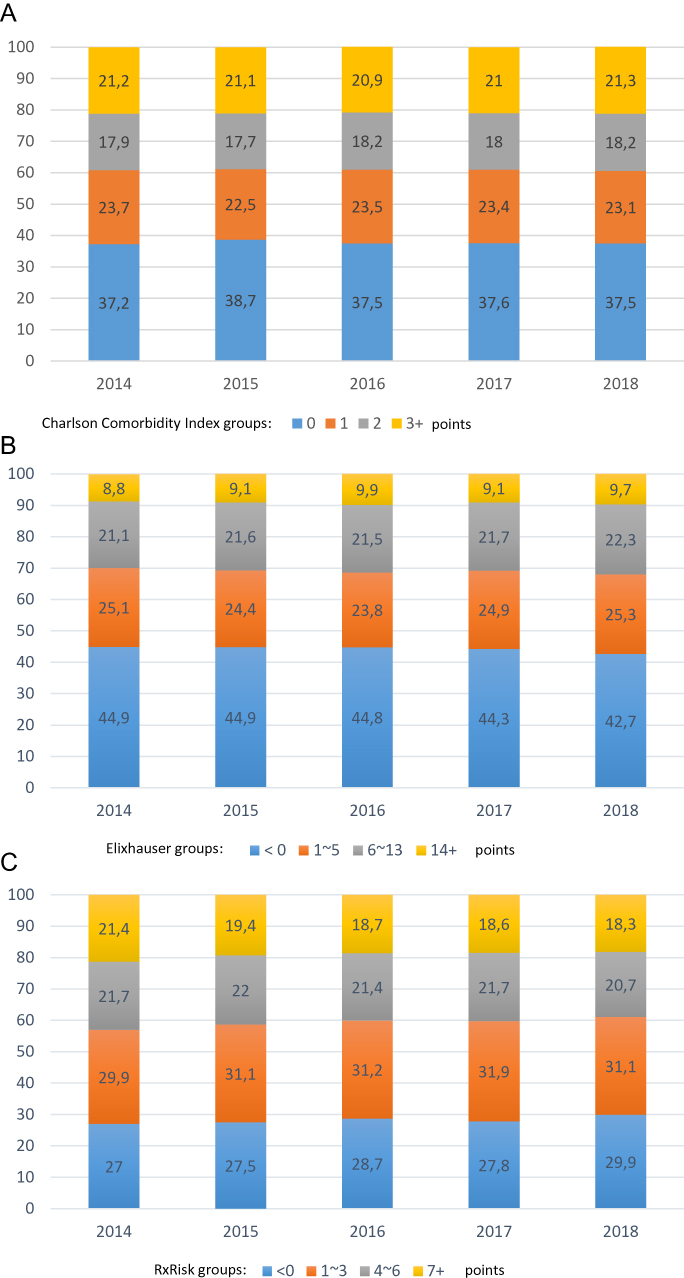 |
Figure 3 (A–C) Proportion of comorbidity level over calendar year. |
The Association Between Comorbidity and Mortality
The overall 30-day mortality and one-year mortality were 10% and 27% for the hip fracture population. A high level of comorbidity was associated with both an increase in 30-day mortality and one-year mortality irrespective of the index used (Figure 4A and B). The 30-day mortality increased from 6.5% to 15% for no comorbidity to very severe comorbidity using CCI and from 7.1% to 17.0% using the Elixhauser Index, and from 6.0% to 15.9% using the Rx-Risk Index Table 3. Adjusted for sex and age, this corresponded to 2.6-fold increased odds of 30-day mortality among patients with very severe comorbidity compared to those without comorbidity using the CCI Figure 4A. The strength of the association was consistent for the two other indices Figure 4A. One-year mortality ranged from 17.8% to 38.7% for the CCI, from 19.2% to 44.7% for the Elixhauser Index, and from 16.5% to 39.7% for the Rx-Risk Index Table 3. Adjusted for gender and age, this corresponded to a 2.5-fold increased risk of 1-year mortality for patients with very severe comorbidity compared to those without comorbidity using the CCI and a 2.8-fold increased risk using either the Elixhauser Index or the Rx-Risk Index Figure 4B. Stratification for gender, age, and calendar year of surgery did not change the relationship between the degree of comorbidity and mortality (Data not shown).
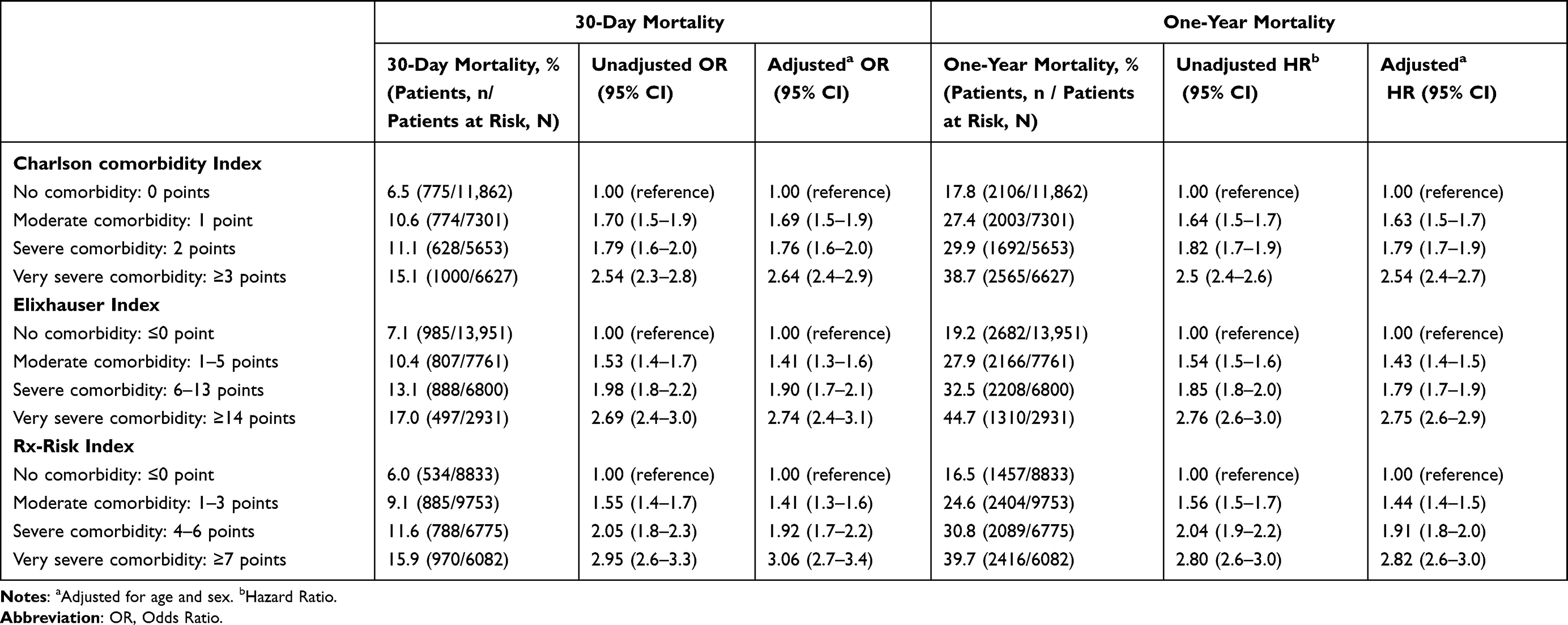 |
Table 3 Crude and Adjusted 30-Day and One-Year Mortality According to Comorbidity Level Among Patients with Hip Fractures |
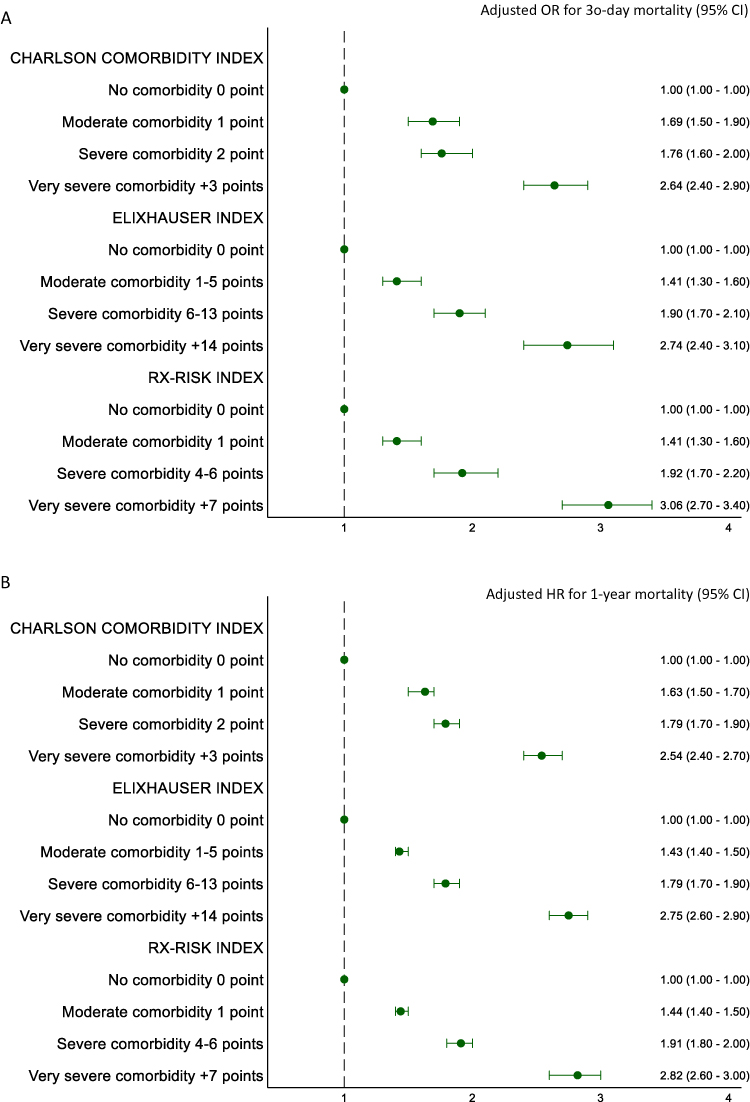 |
Figure 4 (A-B) Forest plots of adjusted associations between comorbidity level and mortality. |
Discussion
In this nationwide, population-based cohort study with complete follow-up, we found that more than 50% of the hip fracture patients had comorbidity, but the prevalence depended on the index used with the Rx-Risk index capturing the highest number of comorbidities. The prevalence of the diseases included in both the CCI and the Elixhauser Index were similar in the two indices. The Rx-Risk Index identified the highest number of comorbidities; patients with congestive heart failure, chronic pulmonary diseases, and depression, but no patients with renal disease. The prevalence of comorbidity was stable within each index during the study period. All indices had a dose-response association between comorbidity level and mortality, and the strength of the association was comparable between the three indices.
In contrast to existing studies and our hypothesis, we did not find an increase in comorbidity from 2014 to 2018 in Denmark regardless of the index used. A US study previously found that the proportion of patients with more than three comorbidities increased from 34% to 43% from 2006 to 2016.2 These differences could be explained by a shorter period examined in our study, as the increase in the US study was mainly in the early years. Furthermore, the US study only counted the number of diseases. The fact that our prevalence of patients with a CCI score of two or above (severe and very severe comorbidity) is similar to the prevalence of comorbidity among Swedish hip fracture patients in the period 2014 to 2017 further strengthens our findings.3 Contrary to our expectations of an increase in disease severity, especially for the prescription-based Rx-Risk Index, we found a minor decrease. This may be explained by a larger focus on upgrading medicine use among elderly and frail hip fracture patients with shorter life expectancies.26 Elderly and frail patients may therefore only be treated for major conditions. This also accords with our findings, which showed a lower proportion of patients with dementia captured by the prescription-based Rx-Risk Index compared to the diagnosis-based CCI. This is also in line with guideline recommendations to discontinue medical treatment for dementia in patients with end-stage dementia.27
Our study shows, along with other studies among osteoarthritis patients, that the prescription-based Rx-Risk Index and the diagnosis-based CCI and Elixhauser Index identified different prevalence of disease for the same condition.28,29 For instance, the Rx-Risk index showed a lower prevalence of renal disease/failure, alcohol abuse, and dementia whereas the CCI and the Elixhauser index identified a lower prevalence of congestive heart failure, hypertension, and depression. Furthermore, specific comorbidities such as anemia, fluid and electrolyte disorders, and weight loss were only captured with the Elixhauser Index, while the Rx-Risk Index did not capture malignancies. This may be explained by the fact that Danish cancer patients have their chemotherapy at the hospitals and not in an outpatient setting.30 Comprehensive data on individual comorbidities are relevant for patients and clinicians to target preventive measures to improve patient outcome. However, patient outcome could further be improved by better understanding the clustering of comorbidities and associated outcomes.31 All indices showed that the magnitude of the association between comorbidity level and short- and long-term mortality was similar and corresponded to previous associations.32–34 All three indices can therefore be used for case-mix adjustment. The increased mortality in hip fracture patients may, depending on the follow-up window, be caused by increased risk of complications during recovery, delayed healing, and caused by the comorbidities themselves.
Even though both the diagnosis-based indices, the CCI and the Elixhauser Index, as well as the prescription-based Rx-Risk Index can be used for case-mix adjustment in mortality analysis among hip fracture patients one index may be more applicable than another depending on the specific research question and data source available. Yet, we should remember that not all diseases are properly identified with the different indices, which may affect the adjusted risk estimates. This limitation applies to both the diagnosis-based and the prescription-based indices when estimating the prevalence of diseases as no gold standard in terms of clinical assessment was available in this study. Misclassification of the individual diseases and the comorbidities could, therefore, occur for all three indices. To our knowledge, the positive predictive values of the diseases included in the Elixhauser Index as well as the completeness of the registered diseases in the Danish population have not previously been examined. A previous Danish study showed positive predictive values between 82% to 100% for the ICD-10 diagnoses included in the CCI,21 but the completeness is unknown. Identification of diseases through prescriptions has not previously been validated in Danish registries. Misclassification could occur as prescriptions can be a proxy for different diseases, eg, patients with heart failure could be identified based on treatment with angiotensin-converting enzyme inhibitors or beta-adrenergic blocking agents, but these medications are also used for the treatment of simple hypertension without heart failure. Further validation studies are therefore needed for estimating the true prevalence of the diseases included in the Elixhauser and the Rx-Risk indices. The weight of the individual diseases in the applied indices may differ across different healthcare settings, study populations, and outcomes. Thus, they should be validated further in a hip fracture population. Our study results implicate the importance of screening for comorbidity in hip fracture patients in clinical practice and developing strategies to manage comorbid conditions in this population. In a clinical context it is important to identify and consider individual comorbidities with high prevalence to target preventive measures to improve patient outcomes whereas using an index is relevant when estimating an overall prognosis or when adjusting for comorbidity. Finally, our results indicate the need for considering a new index in studies on hip fracture patients, which combine diagnosis-based and prescription-based comorbidities in one index.35 This has previously been investigated for patients with acute myocardial infarction with success,36 but it has not been well-studied in patients with hip fractures.
Conclusions
All three indices for quantifying comorbidity seem robust for case-mix adjustment in mortality analysis among hip fracture patients, but considerable heterogeneity arises due to differences in the included diagnoses and the method utilized for capturing comorbidity (medication vs diagnoses). Therefore, researchers are advised to consider these issues when deciding which method to use and when comparing results from different studies.
Compliance with Ethical Standards
The study was reported to the Danish Data Protection Agency through registration at Aarhus University (record number: AU-2016-051-000001, sequential number 880).
Acknowledgment
We thank the staff at the hospital departments caring for patients with hip fractures for their continuous efforts and contribution to the acquisition of the data in the Danish Multidisciplinary Hip Fracture Registry.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was not supported by funds.
Disclosure
Mr Madsen reports that he is involved in studies with funding from various companies as research grants to (and administered by) Aarhus University. The authors declare that they have no other conflicts of interest in this work.
References
1. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of Hip fractures in the United States. JAMA. 2009;302(14):1573–1579. doi:10.1001/jama.2009.1462
2. Bekeris J, Wilson LA, Bekere D, et al. Trends in comorbidities and complications among patients undergoing hip fracture repair. Anesth Analg. 2021;132(2):475–484. doi:10.1213/ane.0000000000004519
3. Meyer AC, Ek S, Drefahl S, Ahlbom A, Hedström M, Modig K. Trends in hip fracture incidence, recurrence, and survival by education and comorbidity: a Swedish register-based study. Epidemiology. 2021;32(3):425–433. doi:10.1097/ede.0000000000001321
4. Schrøder CK, Hjelholt TJ, Møller H, Madsen M, Pedersen AB, Kristensen PK. Comorbidity and quality of in-hospital care for hip fracture patients. J Am Med Dir Assoc. 2022;23(4):671–677.e4. doi:10.1016/j.jamda.2022.01.078
5. Pedersen AB, Ehrenstein V, Szepligeti SK, et al. Thirty-five-year trends in first-time hospitalization for hip fracture, 1-year mortality, and the prognostic impact of comorbidity: a Danish nationwide cohort study, 1980–2014. Epidemiology. 2017;28(6):898–905. doi:10.1097/EDE.0000000000000729
6. Smith T, Pelpola K, Ball M, Ong A, Myint PK. Pre-operative indicators for mortality following Hip fracture surgery: a systematic review and meta-analysis. Age Ageing. 2014;43(4):464–471. doi:10.1093/ageing/afu065
7. Jackson RD, Mysiw WJ. Insights into the epidemiology of postmenopausal osteoporosis: the women’s health initiative. Semin Reprod Med. 2014;32(6):454–462. doi:10.1055/s-0034-1384629
8. Pratt NL, Kerr M, Barratt JD, et al. The validity of the Rx-Risk comorbidity index using medicines mapped to the anatomical therapeutic chemical (ATC) classification system. BMJ Open. 2018;8(4):e021122. doi:10.1136/bmjopen-2017-021122
9. Vesterager JD, Madsen M, Hjelholt TJ, Kristensen PK, Pedersen AB. Prediction ability of Charlson, elixhauser, and rx-risk comorbidity indices for mortality in patients with hip fracture. A Danish population-based cohort study from 2014–2018. Clin Epidemiol. 2022;14:275–287. doi:10.2147/clep.S346745
10. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563. doi:10.2147/CLEP.S179083
11. Kristensen PK, Rock ND, Christensen HC, Pedersen AB. The Danish multidisciplinary hip fracture registry 13-year results from a population-based cohort of hip fracture patients. Clin Epidemiol. 2020;12:9–21. doi:10.2147/clep.S231578
12. Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
13. Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish national prescription registry. Int J Epidemiol. 2017;46(3):798–798f. doi:10.1093/ije/dyw213
14. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–105. doi:10.1177/1403494811405098
15. Norredam M, Kastrup M, Helweg-Larsen K. Register-based studies on migration, ethnicity, and health. Scand J Public Health. 2011;39(7 Suppl):201–205. doi:10.1177/1403494810396561
16. Kristensen PK, Thillemann TM, Pedersen AB, Soballe K, Johnsen SP. Socioeconomic inequality in clinical outcome among Hip fracture patients: a nationwide cohort study. Osteoporos Int. 2017;28(4):1233–1243. doi:10.1007/s00198-016-3853-7
17. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
18. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. doi:10.1097/00005650-199801000-00004
19. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
20. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
21. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sorensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med Res Methodol. 2011;11:11–83. doi:10.1186/1471-2288-11-83
22. De Groot V, Beckerman H, Lankhorst GJ, Bouter LM. How to measure comorbidity. a critical review of available methods. J Clin Epidemiol. 2003;56(3):221–229. doi:10.1016/S0895-4356(02)00585-1
23. van Walraven C, Austin PC, Jennings A, Quan H, Forster AJ. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Medical Care. 2009;47(6):626–633. doi:10.1097/MLR.0b013e31819432e5
24. Von Korff M, Wagner EH, Saunders K. A chronic disease score from automated pharmacy data. J Clin Epidemiol. 1992;45(2):197–203. doi:10.1016/0895-4356(92)90016-g
25. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies conducted using observational routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
26. Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med. 2010;170(18):1648–1654. doi:10.1001/archinternmed.2010.355
27. Sundhedsstyrrelsen. Seponeringslisten Anbefalinger til seponering af hyppigt anvendte lægemidler hos voksne. Available from: https://www.sst.dk/-/media/Udgivelser/2021/Seponeringsliste/SEPONERINGSLISTE_2022.ashx?la=da&hash=F48D9B0B0E1B0C3F00589DF7A56D9512FE34ECD1.
28. Inacio MC, Pratt NL, Roughead EE, Graves SE. Comparing co-morbidities in total joint arthroplasty patients using the RxRisk-V, Elixhauser, and Charlson Measures: a cross-sectional evaluation. BMC Musculoskelet Disord. 2015;16:385. doi:10.1186/s12891-015-0835-4
29. Lu CY, Barratt J, Vitry A, Roughead E. Charlson and Rx-Risk comorbidity indices were predictive of mortality in the Australian health care setting. J Clin Epidemiol. 2011;64(2):223–228. doi:10.1016/j.jclinepi.2010.02.015
30. Lund JL, Frøslev T, Deleuran T, et al. Validity of the Danish national registry of patients for chemotherapy reporting among colorectal cancer patients is high. Clin Epidemiol. 2013;5:327–334. doi:10.2147/clep.S49773
31. Swain S, Coupland C, Strauss V, et al. Clustering of comorbidities and associated outcomes in people with osteoarthritis - A UK Clinical Practice Research Datalink study. Osteoarthritis Cartilage. 2022;30(5):702–713. doi:10.1016/j.joca.2021.12.013
32. Kirkland LL, Kashiwagi DT, Burton MC, Cha S, Varkey P. The Charlson comorbidity index score as a predictor of 30-day mortality after Hip fracture surgery. Am J Med Qual. 2011;26(6):461–467. doi:10.1177/1062860611402188
33. Cher EWL, Allen JC, Howe TS, Koh JSB. Comorbidity as the dominant predictor of mortality after Hip fracture surgeries. Osteoporos Int. 2019;30(12):2477–2483. doi:10.1007/s00198-019-05139-8
34. Toson B, Harvey LA, Close JC. The ICD-10 Charlson Comorbidity Index predicted mortality but not resource utilization following Hip fracture. J Clin Epidemiol. 2015;68(1):44–51. doi:10.1016/j.jclinepi.2014.09.017
35. Kristensen KB, Lund LC, Jensen PB, et al. Development and validation of a Nordic multimorbidity index based on hospital diagnoses and filled prescriptions. Clin Epidemiol. 2022;14:567–579. doi:10.2147/clep.S353398
36. Albertsen LW, Heide-Jørgensen U, Schmidt SAJ, et al. The DANish comorbidity index for acute myocardial infarction (DANCAMI): development, validation and comparison with existing comorbidity indices. Clin Epidemiol. 2020;12:1299. doi:10.2147/CLEP.S277325
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of the Surgical Outcomes in Elderly Patients with Hip Fractures Combined with Hemiplegia
Wang J, Luo H, Wang Q, Zhu X
Clinical Interventions in Aging 2022, 17:1093-1098
Published Date: 15 July 2022
Intertrochanteric Fracture Surgery Patients with Diabetes Mellitus are Prone to Suffer Perioperative Neurological and Endocrine/Metabolic Complications: A Propensity-Score Matched Analysis
Tang Y, Kang L, Guo M, Fan L
Therapeutics and Clinical Risk Management 2022, 18:775-783
Published Date: 6 August 2022
Characteristics of Elderly Hip Fracture Patients in Jordan: A Multicenter Epidemiological Study
Dawod MS, Alisi MS, Saber YO, Abdel-Hay QA, Al-Aktam BM, Alfaouri Y, Alfraihat LB, Albadaineh AA, Abuqudiri AZ, Odeh RM, Altamimi AAR, Alrawashdeh MA, Alebbini MM, Abu-Dhaim OA, Al-Omari AA, Alaqrabawi I, Alswerki MN, Abuawad A, Al Nawaiseh MR, Hammad Y, Al-Ajlouni J
International Journal of General Medicine 2022, 15:6591-6598
Published Date: 13 August 2022
Comorbid Heart Disease in Patients with COPD is Associated with Increased Hospitalization and Mortality – A 15-Year Follow-Up
Giezeman M, Sundh J, Athlin Å, Lisspers K, Ställberg B, Janson C, Montgomery S, Kisiel MA, Nager A, Sandelowsky H, Hasselgren M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:11-21
Published Date: 9 January 2023
Patient Characteristics and Clinical and Economic Outcomes Associated with Unplanned Medical and Surgical Intensive Care Unit Admissions: A Retrospective Analysis
Khanna AK, Moucharite MA, Benefield PJ, Kaw R
ClinicoEconomics and Outcomes Research 2023, 15:703-719
Published Date: 25 September 2023