Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Current Strategies to Reducing Interval Breast Cancers: A Systematic Review
Authors Goh RSJ, Chong B ![]() , Yeo S, Neo SY
, Yeo S, Neo SY ![]() , Ng QX
, Ng QX ![]() , Goh SSN
, Goh SSN
Received 7 April 2025
Accepted for publication 23 June 2025
Published 27 June 2025 Volume 2025:17 Pages 531—544
DOI https://doi.org/10.2147/BCTT.S532884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Pranela Rameshwar
Rachel Sze Jen Goh,1 Bryan Chong,1 Selvie Yeo,1 Shao Yun Neo,1 Qin Xiang Ng,2,* Serene Si Ning Goh1– 3,*
1NUS Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 2Saw Swee Hock School of Public Health, National University of Singapore and National University Health System, Singapore; 3Department of Surgery, National University Hospital Singapore, Singapore
*These authors contributed equally to this work
Correspondence: Serene Si Ning Goh, Department of Surgery, National University Hospital, Singapore, Email [email protected]
Background: Interval breast cancers (IBCs) are detected between regular mammographic screenings after an initially negative result. Studies have shown that the prognosis of IBCs is similar to that of unscreened symptomatic cancers and is hence a surrogate used to assess the effectiveness of screening programs. This systematic review consolidates the current literature available on strategies to reduce the rates of IBC.
Methods: Following PRISMA guidelines, three databases were searched from inception till October 29, 2023 to identify papers, which reported IBC rates. Key search terms included “interval breast cancer”, “mammogram”, “tomosynthesis” and “screening”.
Results: A total of 32 articles were included. Fourteen studies discussed the use of digital breast tomosynthesis (DBT) as an alternative screening modality to mammograms. Six studies discussed the use of artificial intelligence (AI) on mammograms, five studies discussed the use of supplemental modalities including ultrasonography (US) in addition to mammograms, five studies discussed varying screening intervals and two studies discussed tamoxifen use.
Conclusion: The trajectory of IBCs can be altered by early detection when they are more amenable to treatment, through advanced screening techniques, adjusting inter-screening intervals and modifiable risk factors. The goal is to create a screening protocol that is economically effective and accessible to various populations.
Plain Language Summary: This study looked at ways to reduce interval breast cancers, which are cancers that appear between regular breast screening appointments after a previous scan showed no signs of cancer. These cancers are often more aggressive and harder to treat, so finding ways to detect them earlier is important. We reviewed 32 high-quality studies from around the world, covering over 5,500 cases of interval breast cancer, to understand which strategies work best. We found that using digital breast tomosynthesis (a 3D imaging method) generally reduced missed cancers compared to traditional mammograms, especially in women with dense breasts. Artificial intelligence tools also showed promise in helping radiologists detect cancers more accurately. Adding ultrasound to standard mammograms helped pick up cancers that mammograms alone might miss, particularly in women at higher risk. Shortening the time between screenings from every two years to annually was linked to lower rates of interval cancers. Some evidence also suggested that using tamoxifen, a hormone therapy that reduces breast density, may lower the risk of interval cancers. However, these strategies must be balanced with cost, accessibility, and the potential risks of overdiagnosis or unnecessary testing.
Keywords: interval breast cancer, screening, mammogram, systematic review
Introduction
Interval breast cancers (IBCs) are breast malignancies diagnosed between regular mammographic screening rounds, following a negative screening result.1 The occurrence of IBCs serves as a critical quality indicator for breast cancer screening programmes, as it reflects the sensitivity of the screening process in detecting clinically significant disease. International guidelines emphasize monitoring IBC rates, recommending that they remain below 30% of the expected incidence rate within the first year post-screening, and under 50% in the second year, in the absence of screening.2
Importantly, IBCs are often biologically more aggressive than screen-detected cancers. Studies have demonstrated that IBCs tend to exhibit greater local invasion, higher lymph node involvement, and poorer survival outcomes, with prognoses similar to that of symptom-detected cancers in unscreened populations.3,4 Consequently, the frequency and characteristics of IBCs are increasingly viewed not just as performance metrics, but as meaningful surrogates for the real-world effectiveness of screening programmes in reducing breast cancer mortality.5
Several mechanisms have been proposed to explain the occurrence of IBCs. These include the inherent limitations of mammography, particularly in women with dense breast tissue, as well as inappropriate screening intervals, radiologic interpretation errors, and patient-related risk factors such as genetic predispositions. In response, a range of strategies has emerged to mitigate IBCs, including the use of more sensitive imaging technologies (eg, digital breast tomosynthesis [DBT], magnetic resonance imaging [MRI]), incorporation of artificial intelligence (AI) into image interpretation, and the deployment of supplemental modalities like ultrasound. Adjustments to screening intervals and pharmacologic interventions, such as tamoxifen to reduce breast density, have also been explored.6,7
Despite growing interest in these proposed interventions, their comparative effectiveness in reducing IBC incidence and their feasibility within population-wide screening programs remain uncertain. High-resource modalities like DBT and MRI, while promising, are not yet widely adopted due to concerns around cost-effectiveness and implementation logistics. Meanwhile, innovations such as AI-based image triage, although showing potential in enhancing radiologist efficiency and sensitivity, face regulatory and infrastructural hurdles.
This systematic review therefore aims to (1) consolidate existing evidence on strategies to reduce IBC rates and (2) examine the effectiveness and limitations of these strategies in real-world screening contexts. By synthesizing data across diverse populations and interventions, this review seeks to inform the development of more responsive and effective breast cancer screening protocols that not only maximize detection of treatable cancers but also minimize the burden of aggressive, interval-detected disease. These insights can assist policymakers, clinicians, and healthcare administrators in optimizing screening guidelines, resource allocation, and patient outcomes.
Methods
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA)8 and was registered on the International Prospective Register of Systematic Reviews (PROSPERO), registration number CRD4203429059.
Search Strategy
In this systematic review, databases including PubMed, EMBASE, and the Cochrane Library were searched from the inception of the databases till October 29, 2023 to identify papers that reported IBC rates. Keywords synonymous with “interval breast cancer”, “mammogram”, “tomosynthesis”, and “screening” were used in the search strategy. The detailed search strategy can be found in the Supplementary Material (Table S1). The articles were exported from the search databases and duplicates were removed on Endnote 20. The eligibility assessment was then conducted on Rayyan.
Inclusion and Exclusion Criteria
The inclusion criteria were (1) cohort studies, case-control studies, cross-sectional studies or randomized controlled trials; and (2) had two or more arms comparing the reported IBC rates for different modalities or regimes of screening. Articles not written in English and other study types including editorials, commentaries, reviews, conference abstracts, systematic reviews and meta-analyses were excluded.
Data Extraction
Data extraction was done on a Microsoft Excel sheet with pre-determined variables. Three authors (R.S.J.G., B.C. and S.Y.) independently extracted the variables of interest including but not limited to study design, definition of IBC, IBC rates, country of the study, screening modality and screening intervals. To ensure accuracy and consistency, each dataset underwent blind cross-checking by the other authors. Discrepancies in the extracted data were documented and discussed in joint review meetings. These discrepancies occurred most commonly involving variations in definitions of IBC and classification of screening intervals. Resolution was achieved through group consensus, whereby all three reviewers reviewed the full text and relevant supplemental material of the original studies. In cases where consensus could not be reached, a fourth senior reviewer (S.G.) was consulted to arbitrate.
Quality Assessment
Three authors (R.S.J.G., B.C. and S.Y.) assessed the quality of the included studies using the Newcastle-Ottawa Scale9 and the revised Cochrane Risk of Bias tool (ROB 2).10 Any discrepancies in decision were resolved by a senior author (Q.X.N. or S.S.N.G). The Newcastle-Ottawa Scale was used to evaluate the quality of the study in three areas, mainly selection, comparability, and outcome, and the quality of the studies were judged according to the Agency for Health Research and Quality (AHRQ) standards to be poor, fair or good. The ROB-2 evaluates the quality and bias of the included outcomes across five domains, including the trial’s randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. The final assessment of the quality of study was presented using the Robvis visualisation tool.
Results
A total of 5,838 articles were identified through the initial search strategy, with 356 duplicates removed. Following the initial title and abstract screening, 5,155 articles were excluded. A full-text review was then conducted on the remaining 301 articles, resulting in the inclusion of 32 articles in this systematic review, articles were excluded if they were abstracts, of repeated cohorts or if there were no IBC rates reported (Figure 1). The combined cohort had a total of 5524 interval breast cancers, spanning across different countries including one from Australia,11 three from Canada,12–14 one from Germany,15 five from Italy,16–20 two from Japan,21,22 seven from Norway,14,23–28 five from Sweden7,29–32 and eight from the United States.6,33–39 One study made a comparison between screening programmes in both Norway and USA.14 All 32 articles included were double-armed retrospective or prospective cohorts or randomized controlled trials. Fourteen studies discussed the use of DBT as an alternative screening modality to mammograms. Six studies discussed the use of AI on mammograms, five studies discussed the use of supplemental modalities such as ultrasonography in addition to mammograms, five studies discussed varying screening intervals and two studies discussed Tamoxifen use. The follow-up durations for these studies ranged from between 12 and 36 months.
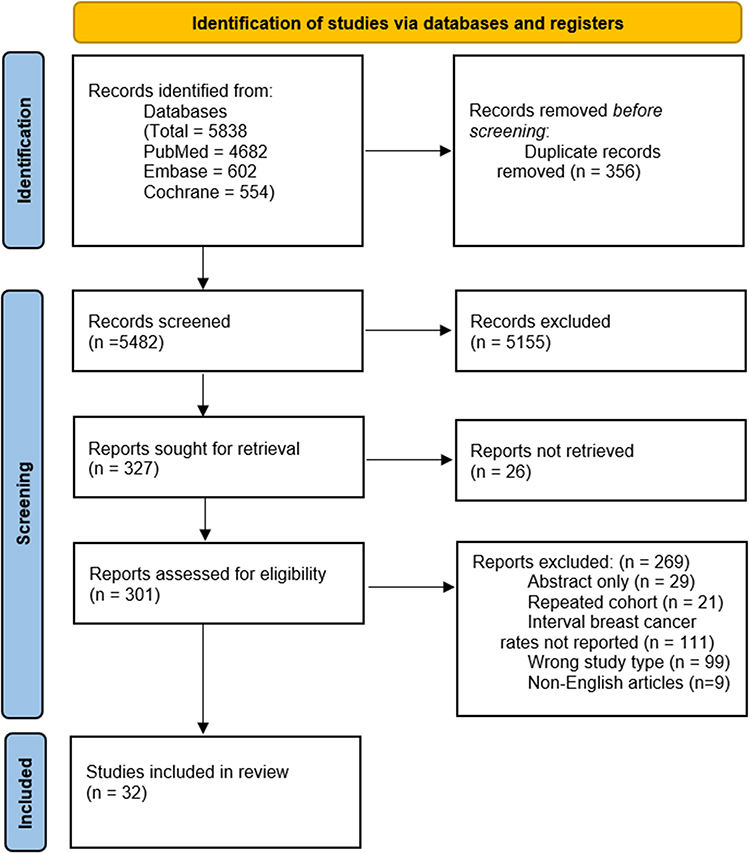 |
Figure 1 PRISMA flow chart. Summary of identified, screened and included studies from databases and registers. |
Our study found that between studies there were various strategies to reduce the incidence of IBC rates, through implementing structured screening programmes as compared to opportunistic screenings, and shorter screening intervals.14 Utilizing state-of-the-art technology including AI and DBT and supplemental imaging methods such as ultrasound also led to a decrease in IBC rates. Additionally, the use of Tamoxifen to reduce breast density was shown to reduce IBC rates.32 A summary of the characteristics and findings of the included studies is shown in Table 1.
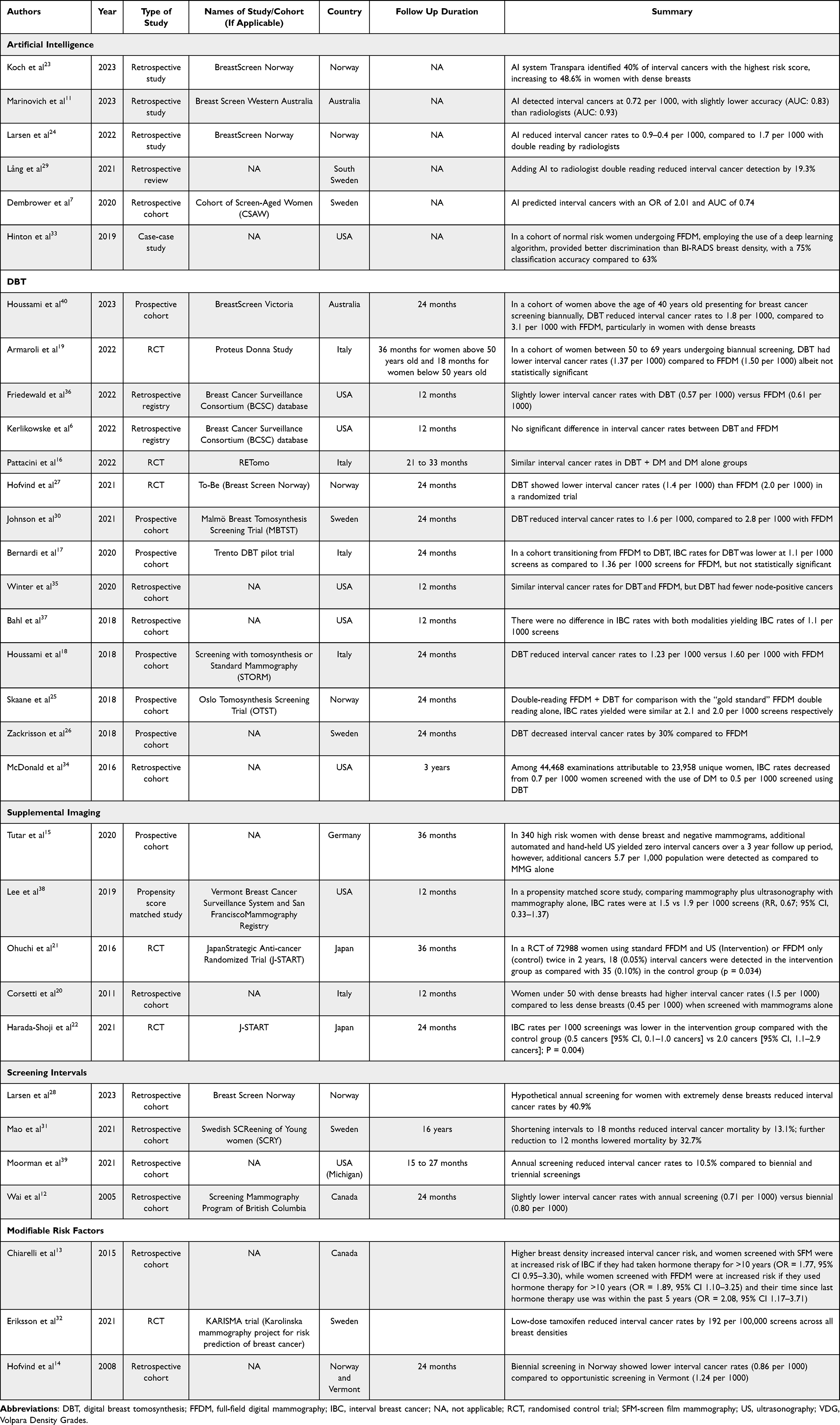 |
Table 1 Characteristics and Findings of the Included Studies |
Screening Intervals
Four articles assessed the impact of different screening intervals on IBC rates. Current guidelines recommend screening intervals of between one and three years.41–43 All studies found that shorter intervals were associated with lower incidence of IBCs. In the study by Larsen et al, a hypothetical simulation suggested that shortening screening intervals to annually instead of the current biannual guidelines could reduce the IBC rates by 40.9%.24 The most significant reduction was found in women with denser breasts (59.1%) as compared to women with the least dense breasts (28.2%). In a retrospective cohort with screening intervals between 18 and 26 months, reducing the screening intervals to 18 months was associated with a decrease in IBC mortality rates by 13.1%, while further shortening the screening interval to 12 months was associated with a 32.7% decrease in IBC mortality rates.31
Screening Modalities and Supplements
Digital Breast Tomosynthesis (DBT)
While double reader full-field digital mammography (FFDM) is currently the standard of care in many screening programmes around the world, various studies have suggested an additional benefit to utilizing DBT as compared to FFDM for screening, though the increased screening costs and radiation exposure remain a cause of concern. Of the 14 articles comparing DBT and mammograms, 12 articles suggested a reduction in IBC rates when using DBT as the screening modality as compared to FFDM, though in five articles the difference in IBC rates did not achieve statistical significance. DBT was shown to reduce IBC rates by up to 30% as compared to FFDM,26 though some articles reported no difference in IBC rates regardless of the modality of screening used.6,25 Additionally, Winter et al suggested a potentially lower proportion of node-positive IBCs in individuals screened with DBT (22.9%) as compared to individuals screened with mammograms (48%).35 When stratified by breast density, the paper by Houssami et al found that while DBT reduced IBC rates in both patients with high density (BIRADS D3-D4) and low density (BIRADS D1-D2) breasts, there was, however, a larger difference in IBC rates of 3.2 per 1000 screens for women with high-density breasts, compared to 0.7 per 1000 screens for women with low-density breasts.40
Supplemental Ultrasonography Screening
Five studies explored the use of ultrasound screening in addition to the current FFDM. While the studies are unanimous in suggesting a decrease in interval cancer rates for both, for instance, the study by Ohuchi et al comparing the use of FFDM only and FFDM with supplemental ultrasound found that the cohort screened with dual modalities had approximately half the number of IBCs as compared to the cohort screened with FFDM only.21 Similar findings were revealed in other cohorts. In the J-START randomized controlled trial, the IBC rates per 1000 screenings were lower in the group screened with both FFDM and ultrasound as compared with the group only screened with FFDM (0.5 cancers vs 2.0 cancers).21 This difference persisted in high-risk patients, where the population screened by FFDM only had an IBC rate of 5.7 per 1000 individuals, while the group with the additional supplemental ultrasound screening did not have any IBCs within the 36 month follow-up period.15 Additionally, an Italy-based study, screening patients stratified based on their breast densities, showed similar IBC rates in patients screened with FFDM (BIRADS 1 and 2) and FFDM and supplemental ultrasound (BIRADS 3 and 4). However, when stratified by age, women below the age of 50 years with denser breasts (BIRADS 3 and 4) had a significantly higher IBC rate of 1.5 per 1000 screens as compared to their counterparts with less dense breasts (BIRADS 1 to 2) with 0.45 per 1000 screens.20
Artificial Intelligence (AI)
A total of six articles discussed the use of artificial intelligence to facilitate breast cancer screening, three articles utilized the AI system Transpara developed by Screen Point Medical, while one article utilized Deep Health AI model and another utilized an unspecified deep learning method, with the remaining article utilizing the Lunit AI system. In all three studies, the Transpara AI system was shown to reduce the number of IBCs, with the study by Lång et al showing a 19.3% reduction in IBC rates,29 while the study by Larsen et al showed an IBC rate reduction of between 0.4 and 0.9 per 1000 screens.24 The retrospective study by Koch et al revealed that the AI labelled 40% of the IBCs with the maximum AI risk score of 10, which was improved to 48.6% in women with dense breasts.23 Similarly, the other studies also reported increased sensitivity with the utilization of AI systems, with the deep learning algorithms showing a 75% classification accuracy for interval breast cancer,33 superior to that of the current BIRADS classification, while the other study by Marinovich et al suggested an increase in IBC detection of 0.72 per 1000 screens.11
Modifiable Risk Factors
Two studies discussed the use of hormonal therapy (Tamoxifen) on the visualization of breast tumours on FFDM. The retrospective cohort study by Chiarelli et al observed that for women on hormone therapy screened with FFDM, use of hormonal therapy for >10 years was associated with an increased risk of IBCs (Odds Ratio (OR): 1.89, 95% CI 1.10–3.25) which was further increased if the time since last hormone therapy use was within the past 5 years (OR: 2.08, 95% CI 1.17–3.71).13 A randomized controlled trial on pre-menopausal women (KARISMA trial (Karolinska mammography project for risk prediction of breast cancer)), however, found that the use of low-dose tamoxifen to reduce breast density, reduced IBC rates by 192 per 100,000 screens as compared to placebo.32
Quality Assessment
The quality of 28 studies were assessed using the Newcastle-Ottawa scoring, while the remaining six randomized controlled trials were assessed using the ROB-2. All 28 studies assessed with the Newcastle-Ottawa scoring attained seven to eight stars, that is, were of generally good quality. The six studies assessed using the ROB-2 reported low levels of concerns overall, with individual domains mostly rated as low concerns, and a single domain rated of some concerns. The complete quality assessment is appended in the Supplementary Material (Tables S2a and S2b).
Discussion
The ongoing debate on whether early detection improves survival rates for breast cancer patients has spanned decades. There is some evidence that regular mammographic screening may lead to more frequent diagnoses and a roughly 20% reduction in breast cancer mortality.44,45 Critics, however, argue that while mammograms can identify breast cancer earlier, this does not always result in better survival outcomes, as screen-detected cancers are often slower-growing and less aggressive.44 Shifting the focus to reducing interval breast cancers could alter this perspective. IBCs are generally more aggressive, frequently involve lymph nodes, and are more locally advanced at diagnosis, contributing to poorer prognoses.46,47 By reducing the incidence of IBCs through optimized screening methods and adjusted screening intervals, it may be possible to detect these cancers at an earlier, more treatable stage, potentially changing their clinical course.48 Targeting the reduction of IBCs through modified screening protocols could lower breast cancer mortality by enabling earlier detection and treatment of more aggressive cancers. This study explores the incidence of IBCs across various screening strategies and populations, aiming to identify the most effective approaches and propose actionable measures to reduce IBCs. A summary of the key points is presented in Figure 2.
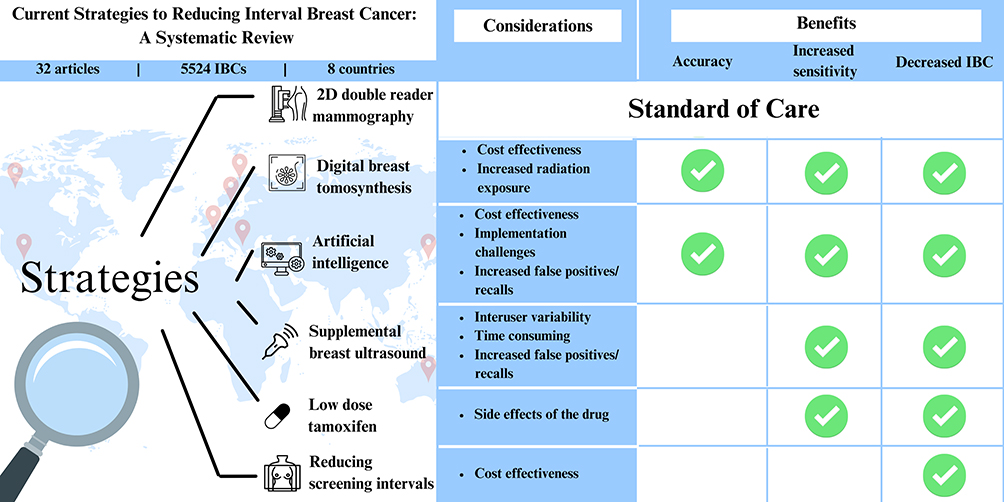 |
Figure 2 Summary of key strategies for breast cancer screening. |
Shorter Screening Intervals and Demographics
With regard to optimizing breast cancer screening strategies, particular attention should be paid to women aged 40–49, a demographic that has been observed to experience higher rates of interval cancers compared to older women.44 Studies indicate that interval cancers occur at nearly double the rate in younger women (27.7%) compared to women aged 50 and older (13.9%) within 12 months of a negative mammogram.45 This disparity is largely attributed to higher breast density in younger women, a key factor in masking tumours during mammography and reducing the sensitivity of traditional mammographic screening techniques.46
In Singapore, where women aged 40–49 are advised to undergo annual mammography, data from the Singapore Cancer Registry underscores the importance of this practice. With a reported breast cancer incidence of 139.1 per 100,000 in this age group, the implementation of more frequent screening is justified by both the higher interval cancer rates and the overall breast cancer risk in younger women. This annual screening recommendation is an important consideration, particularly given that breast cancer screening guidelines globally often suggest starting regular screening at age 50. However, the emerging evidence supporting earlier screening, starting at age 40 years, reflects a growing recognition that personalized screening schedules based on risk factors such as age and breast density may offer better outcomes.47
Increased screening frequency for breast cancer, while designed to improve early detection, presents several significant challenges that must be carefully considered. One of the most pressing issues is overdiagnosis, which occurs when screenings identify benign nodules would not have posed a threat during a person’s lifetime. This can lead to patients undergoing unnecessary core biopsy or diagnostic surgery, which carry the risk of anaesthesia, adverse physical side effects and contribute to psychological distress. The emotional toll of false positives and the uncertainty surrounding cancer diagnosis can elevate anxiety levels among patients, creating a cycle of stress related to the potential need for further testing and treatment. In addition to the psychological impact, there are substantial financial burdens associated with increased screening frequency. More frequent screenings and subsequent follow-up procedures can strain healthcare systems and result in significant out-of-pocket expenses for individuals, especially in regions where insurance coverage is limited or non-existent.
Furthermore, the cumulative demands of more frequent screening, such as increased appointments, travel time, and psychological stress, may reduce screening adherence, potentially diminishing the anticipated benefits. Given these considerations, implementing risk-stratified screening strategies that prioritize more intensive surveillance for high-risk individuals may offer a more balanced and efficient approach. Such strategies may improve outcomes while mitigating unnecessary harms and optimizing resource utilization.
Screening Modalities: DBT, AI, and Supplemental Ultrasound
The clinical effectiveness of any screening program hinges not only on the interval but also on the modality employed. DBT has demonstrated higher cancer detection rates compared to conventional digital mammography, particularly for women with dense breast tissue, eg, in a prospective cohort in by Houssami et al in women with dense breast, DBT reduced IBC rates to 1.8 per 1000, compared to 3.1 per 1000 with FFDM.40 DBT’s three-dimensional imaging capability offers improved visualization, reducing the impact of overlapping breast tissue, a significant issue in younger women.
Additionally, the integration of AI into mammographic interpretation offers further advancements. With the advent of the technological era, AI has been a novel method to improve the sensitivity and specificity of breast cancer screening programmes, though currently not the standard of care due to various implementation challenges.48 AI has been shown to enhance diagnostic accuracy, reduce false positives, and improve radiologists’ efficiency, particularly in high-volume settings where workload and error rates are significant concerns. A recent study by Lauritzen et al found that AI may decrease radiologists’ workload by approximately 33.5%.49 Although these findings are encouraging, they must be interpreted with caution. A majority of the included studies were retrospective, raising the risk of selection, flow, and timing biases. Variability in study design, population characteristics, and IBC definitions further complicates comparison. Many AI algorithms were applied post hoc to enriched datasets, which may not reflect real-world screening conditions. Nevertheless, these studies are valuable given the inherent rarity of IBC events, which limits the feasibility of large prospective trials specifically powered to detect differences in IBC outcomes. In this context, retrospective analyses and observational studies play an important role in generating early evidence and guiding the design of future prospective validation studies. As the field matures, standardized reporting frameworks and population-based trials will be crucial to confirm AI’s role in reducing IBC incidence and improving screening outcomes across diverse settings.
For women with dense breasts, supplemental modalities like ultrasound have been explored. While ultrasound can detect cancers missed by mammography, eg, in a study of high-risk women, an additional 5.7 per 1,000 cancers were detected using ultrasound, particularly in dense breast tissue,15 its cost-effectiveness remains debatable Simulation studies have shown that supplemental ultrasound adds significant costs with only marginal gains in reducing breast cancer mortality. The decision to use ultrasound should therefore be carefully considered within the context of overall healthcare resources and patient risk profiles.
Cost-Effectiveness of Screening Intervals and Modalities
From a cost-effectiveness perspective, the choice of screening interval plays a crucial role. While annual screening offers increased detection, it comes with higher costs. Studies from Canada indicate that triennial screening for women aged 50–69 has a lower incremental cost-effectiveness ratio (ICER) compared to annual screening, with annual screening yielding significantly higher ICERs.46 However, the context of Singapore and other countries with different healthcare systems and population demographics may shift these calculations. In Singapore, where breast cancer incidence peaks around age 60 and breast density tends to be higher in younger women, policies may need to prioritize balancing the benefits of early detection against the financial burden of annual screening. The study acknowledges that for women aged 40–49, shared decision-making frameworks should be employed to help individuals weigh the benefits and risks of early mammography, considering the likelihood of false positives in this age group due to higher breast density. For novel modalities like DBT, the cost-effectiveness seems more favourable. A Canadian study reported an ICER of $17,149 per quality-adjusted life year (QALY) for DBT, suggesting that it could be a valuable addition to national screening programs, especially for women with dense breasts.50 AI-assisted mammography, though still under evaluation, also shows promise in enhancing both clinical and cost outcomes by improving accuracy and reducing unnecessary callbacks and biopsies.
For low- and middle-income countries (LMICs), where mammographic infrastructure may be limited, shortening screening intervals or adopting high-cost AI solutions may not be immediately feasible. Instead, resource-stratified approaches such as targeted clinical breast examinations or ultrasound-based screening, especially in populations with higher breast density or limited access to mammography. Mobile screening units, task-shifting to trained non-physician providers, and hybrid screening models combining AI triage with manual review can also optimize efficiency. Future research should assess the feasibility, acceptability, and cost-effectiveness of these approaches, alongside investment in digital health infrastructure and workforce capacity-building tailored to local contexts.
This review excluded contrast-enhanced spectral mammography (CESM) and magnetic resonance imaging (MRI), as these modalities are not routinely used for primary population-based screening but are instead applied in stratified approaches for high-risk individuals. Notably, the DENSE trial51 demonstrated that supplemental MRI in women with extremely dense breasts significantly reduced interval cancer rates. However, due to their targeted use, higher cost, and limited availability, CESM and MRI were beyond the scope of this review.
The Role of Tamoxifen in Enhancing Mammographic Sensitivity and Reducing Breast Cancer Risk
Tamoxifen, when used in hormonal therapy, not only reduces breast cancer incidence but also lowers the rates of invasive breast cancer in women with dense breasts. The KARISMA Study underscores the importance of tamoxifen not only as a preventive measure against breast cancer but also as a tool for modifying breast density, which can enhance screening effectiveness and inform treatment decisions.52 Further research is needed to solidify these findings and explore additional implications for clinical practice. For women at high risk of breast cancer, Tamoxifen serves a dual purpose: it acts as both a preventive measure and a means to improve early detection, contributing to a lower overall cancer incidence and better long-term screening outcomes.52 However, its use must be personalized based on an individual’s risk profile, weighing the benefits of cancer prevention against potential side effects, such as an elevated cardiovascular risk. For women aged 40 to 49 at average risk, a shared decision-making process is essential.
Policy Implications and Future Directions
Beyond clinical and cost-effectiveness, there is a need for policymakers to consider how new technology and varied screening intervals will be implemented across diverse healthcare settings. The strategy has to account for the distribution of resources, ensuring that screening programs are sustainable and accessible to the majority of the population. The integration of new technologies, such as AI-assisted mammography, into national screening programs also raises important policy questions. These include determining the appropriate level of public and private investment, setting standards for technology adoption, and addressing potential disparities in access to advanced screening tools. Policies must also address the training and support required for healthcare providers to effectively use these new technologies.53 Looking ahead, risk-based assessment also has the potential to revolutionize screening programs. It allows for a more personalized approach, where screening intensity and frequency can be tailored to an individual’s specific risk profile, rather than a one-size-fits-all model. This could lead to earlier detection in high-risk individuals while reducing unnecessary screening and the associated risks of overdiagnosis and false positives in lower-risk populations. Given the heterogeneity in breast cancer screening protocols across countries such as differences in age range, screening interval, and modality, the optimal strategy for improving outcomes is likely context-specific. These adaptations, however, should not be implemented without formal evaluation. Risk-adapted screening must be supported by evidence that the stratification accurately identifies those who benefit most from specific protocols and that the selected screening approach is optimal for each subgroup. Robust outcome evaluation, including assessment of cancer detection rates, interval cancer incidence, false positives, and ultimately mortality reduction, is essential to ensure that personalized screening enhances rather than inadvertently undermines population-level effectiveness and equity.
Strengths and Limitations
This systematic review provides actionable insights for improving breast cancer screening programs and reducing the rates of IBCs. Advanced screening techniques, such as DBT and AI applied to mammograms, can be incorporated to enhance early detection and minimize the occurrence of IBCs. Additionally, the use of supplemental modalities like US alongside mammography is recommended for high-risk populations to improve diagnostic accuracy. Adjusting screening intervals based on individual risk profiles can further aid in the timely detection of IBCs when they are more amenable to treatment. The study also highlights the potential of risk reduction through pharmacological interventions, such as the use of tamoxifen, in specific populations. Finally, the findings emphasize the importance of developing economically effective and accessible screening protocols that integrate these strategies, ensuring equitable access to advanced screening tools and personalized care for diverse population. However, the review is not without limitations. One major challenge is the lack of standardized definitions and measures for IBC rates across the included studies, which may result in inconsistencies in reporting and comparison of outcomes. There is a notable absence of consensus in methodology for the recommended radiological review and classification of interval cancers in the literature.54 Additionally, the follow-up periods in many studies, ranging from 12 to 36 months, may be insufficient to fully capture the long-term impact of different screening strategies on IBC rates and survival outcomes. Demonstrating a direct mortality benefit from reduction of IBCs requires carefully designed longitudinal studies and modelling approaches that account for tumor biology, lead time, and competing risks. Another limitation is the representativeness of the included studies; most originate from developed countries with advanced healthcare systems, which may not be directly applicable LMICs. In LMICs, where access to advanced screening technologies like DBT and AI is limited due to cost and infrastructure constraints, the adoption of these strategies might be hindered.55
Conclusion
This systematic review underscores the need for a tailored approach to breast cancer screening, suggesting that integrating advanced screening modalities such as DBT and AI with individualized risk assessments, optimising screening intervals and addressing modifiable risk factors has potential in reducing the incidence of IBCs. Nevertheless, while the newer strategies offer promise, they require further validation, and their implementation must be balanced with considerations of cost, potential for false positives, and resource availability. As breast cancer screening evolves, clinicians and policymakers must engage in informed discussions with patients, weighing the benefits of early detection against the risks of overdiagnosis and unnecessary interventions. The population health goal should be to develop screening protocols that are not only clinically effective but also economically sustainable and accessible to diverse populations, thereby improving overall outcomes in breast cancer care and management.
Data Sharing Statement
Data sharing is not applicable for this article, as no data sets were generated or analysed during this study.
Ethics Approval and Consent to Participation
As this is a systematic review, there was no primary datasets assessed; ethics approval and consent for participation were hence not necessary in this case.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Niraula S, Biswanger N, Hu P, Lambert P, Decker K. Incidence, characteristics, and outcomes of interval breast cancers compared with screening-detected breast cancers. JAMA Network Open. 2020;3(9):e2018179–e. doi:10.1001/jamanetworkopen.2020.18179
2. Kirsh VA, Chiarelli AM, Edwards SA, et al. Tumor characteristics associated with mammographic detection of breast cancer in the Ontario breast screening program. J National Cancer Inst. 2011;103(12):942–950. doi:10.1093/jnci/djr138
3. McCarthy AM, Barlow WE, Conant EF, et al. Breast cancer with a poor prognosis diagnosed after screening mammography with negative results. JAMA Oncol. 2018;4(7):998–1001. doi:10.1001/jamaoncol.2018.0352
4. Collins S, Woodman CB, Threlfall A, Prior P. Survival rates from interval cancer in NHS breast screening programme. BMJ. 1998;316(7134):832–833. doi:10.1136/bmj.316.7134.832
5. Day N, McCann J, Camilleri-Ferrante C, et al. Monitoring interval cancers in breast screening programmes: the East Anglian experience. J Med Screening. 1995;2(4):180–185. doi:10.1177/096914139500200402
6. Kerlikowske K, Su Y-R, Sprague BL, et al. Association of screening with digital breast tomosynthesis vs digital mammography with risk of interval invasive and advanced breast cancer. JAMA. 2022;327(22):2220–2230. doi:10.1001/jama.2022.7672
7. Dembrower K, Wåhlin E, Liu Y, et al. Effect of artificial intelligence-based triaging of breast cancer screening mammograms on cancer detection and radiologist workload: a retrospective simulation study. Lancet Digital Health. 2020;2(9):e468–e74. doi:10.1016/S2589-7500(20)30185-0
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
9. Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses; 2000.
10. Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
11. Marinovich ML, Wylie E, Lotter W, et al. Artificial intelligence (AI) for breast cancer screening: BreastScreen population-based cohort study of cancer detection. EBioMedicine. 2023;90:104498. doi:10.1016/j.ebiom.2023.104498
12. Wai E, D’yachkova Y, Olivotto I, et al. Comparison of 1-and 2-year screening intervals for women undergoing screening mammography. Br J Cancer. 2005;92(5):961–966. doi:10.1038/sj.bjc.6602393
13. Chiarelli AM, Prummel MV, Muradali D, et al. Digital versus screen-film mammography: impact of mammographic density and hormone therapy on breast cancer detection. Breast Cancer Res Treat. 2015;154:377–387. doi:10.1007/s10549-015-3622-x
14. Hofvind S, Vacek PM, Skelly J, Weaver DL, Geller BM. Comparing screening mammography for early breast cancer detection in Vermont and Norway. J National Cancer Inst. 2008;100(15):1082–1091. doi:10.1093/jnci/djn224
15. Tutar B, Esen Icten G, Guldogan N, et al. Comparison of automated versus hand-held breast US in supplemental screening in asymptomatic women with dense breasts: is there a difference regarding woman preference, lesion detection and lesion characterization? Arch Gynecol Obstet. 2020;301(5):1257–1265. doi:10.1007/s00404-020-05501-w
16. Pattacini P, Nitrosi A, Giorgi Rossi P, et al. A randomized trial comparing breast cancer incidence and interval cancers after tomosynthesis plus mammography versus mammography alone. Radiology. 2022;303(2):256–266. doi:10.1148/radiol.211132
17. Bernardi D, Gentilini MA, De Nisi M, et al. Effect of implementing digital breast tomosynthesis (DBT) instead of mammography on population screening outcomes including interval cancer rates: results of the Trento DBT pilot evaluation. Breast. 2020;50:135–140. doi:10.1016/j.breast.2019.09.012
18. Houssami N, Bernardi D, Caumo F, et al. Interval breast cancers in the ‘screening with tomosynthesis or standard mammography’(STORM) population-based trial. Breast. 2018;38:150–153. doi:10.1016/j.breast.2018.01.002
19. Armaroli P, Frigerio A, Correale L, et al. A randomised controlled trial of digital breast tomosynthesis vs digital mammography as primary screening tests: screening results over subsequent episodes of the Proteus Donna study. Int J Cancer. 2022;151(10):1778–1790. doi:10.1002/ijc.34161
20. Corsetti V, Houssami N, Ghirardi M, et al. Evidence of the effect of adjunct ultrasound screening in women with mammography-negative dense breasts: interval breast cancers at 1 year follow-up. Eur J Cancer. 2011;47(7):1021–1026. doi:10.1016/j.ejca.2010.12.002
21. Ohuchi N, Suzuki A, Sobue T, et al. Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): a randomised controlled trial. Lancet. 2016;387(10016):341–348. doi:10.1016/S0140-6736(15)00774-6
22. Harada-Shoji N, Suzuki A, Ishida T, et al. Evaluation of adjunctive ultrasonography for breast cancer detection among women aged 40–49 years with varying breast density undergoing screening mammography: a secondary analysis of a randomized clinical trial. JAMA Netw Open. 2021;4(8):e2121505–e. doi:10.1001/jamanetworkopen.2021.21505
23. Koch HW, Larsen M, Bartsch H, Kurz KD, Hofvind S. Artificial intelligence in BreastScreen Norway: a retrospective analysis of a cancer-enriched sample including 1254 breast cancer cases. Eur Radiol. 2023;33(5):3735–3743. doi:10.1007/s00330-023-09461-y
24. Larsen M, Aglen CF, Hoff SR, Lund-Hanssen H, Hofvind S. Possible strategies for use of artificial intelligence in screen-reading of mammograms, based on retrospective data from 122,969 screening examinations. Eur Radiol. 2022;32(12):8238–8246. doi:10.1007/s00330-022-08909-x
25. Skaane P, Sebuødegård S, Bandos AI, et al. Performance of breast cancer screening using digital breast tomosynthesis: results from the prospective population-based Oslo Tomosynthesis Screening Trial. Breast Cancer Res Treat. 2018;169:489–496. doi:10.1007/s10549-018-4705-2
26. Zackrisson S, Lång K, Rosso A, et al. One-view breast tomosynthesis versus two-view mammography in the Malmö Breast Tomosynthesis Screening Trial (MBTST): a prospective, population-based, diagnostic accuracy study. Lancet Oncol. 2018;19(11):1493–1503. doi:10.1016/S1470-2045(18)30521-7
27. Hofvind S, Moshina N, Holen ÅS, et al. Interval and subsequent round breast cancer in a randomized controlled trial comparing digital breast tomosynthesis and digital mammography screening. Radiology. 2021;300(1):66–76. doi:10.1148/radiol.2021203936
28. Larsen M, Lynge E, Lee CI, Lång K, Hofvind S. Mammographic density and interval cancers in mammographic screening: moving towards more personalized screening. Breast. 2023;69:306–311. doi:10.1016/j.breast.2023.03.010
29. Lång K, Hofvind S, Rodríguez-Ruiz A, Andersson I. Can artificial intelligence reduce the interval cancer rate in mammography screening? Eur Radiol. 2021;31(8):5940–5947. doi:10.1007/s00330-021-07686-3
30. Johnson K, Lång K, Ikeda DM, Åkesson A, Andersson I, Zackrisson S. Interval breast cancer rates and tumor characteristics in the prospective population-based Malmö Breast Tomosynthesis Screening Trial. Radiology. 2021;299(3):559–567. doi:10.1148/radiol.2021204106
31. Mao Z, Nyström L, Jonsson H. Breast cancer screening with mammography in women aged 40–49 years: impact of length of screening interval on effectiveness of the program. J Med Screening. 2021;28(2):200–206.
32. Eriksson M, Czene K, Conant EF, Hall P. Use of low-dose tamoxifen to increase mammographic screening sensitivity in premenopausal women. Cancers. 2021;13(2):302. doi:10.3390/cancers13020302
33. Hinton B, Ma L, Mahmoudzadeh AP, et al. Deep learning networks find unique mammographic differences in previous negative mammograms between interval and screen-detected cancers: a case-case study. Cancer Imaging. 2019;19:1–9. doi:10.1186/s40644-019-0227-3
34. McDonald ES, Oustimov A, Weinstein SP, Synnestvedt MB, Schnall M, Conant EF. Effectiveness of digital breast tomosynthesis compared with digital mammography: outcomes analysis from 3 years of breast cancer screening. JAMA Oncol. 2016;2(6):737–743. doi:10.1001/jamaoncol.2015.5536
35. Winter AM, Kazmi S, Hardy AK, Bennett DL. Comparison of interval breast cancers with 2D digital mammography versus 3D digital breast tomosynthesis in a large community‐based practice. Breast J. 2020;26(10):1953–1959. doi:10.1111/tbj.14047
36. Friedewald SM, Grimm LJ. Digital breast tomosynthesis and detection of interval invasive and advanced breast cancers. JAMA. 2022;327(22):2198–2200. doi:10.1001/jama.2021.25018
37. Bahl M, Gaffney S, McCarthy AM, Lowry KP, Dang PA, Lehman CD. Breast cancer characteristics associated with 2D digital mammography versus digital breast tomosynthesis for screening-detected and interval cancers. Radiology. 2018;287(1):49–57. doi:10.1148/radiol.2017171148
38. Lee JM, Arao RF, Sprague BL, et al. Performance of screening ultrasonography as an adjunct to screening mammography in women across the spectrum of breast cancer risk. JAMA Intern Med. 2019;179(5):658–667. doi:10.1001/jamainternmed.2018.8372
39. Moorman SE, Pujara AC, Sakala MD, et al. Annual screening mammography associated with lower stage breast cancer compared with biennial screening. Am J Roentgenol. 2021;217(1):40–47. doi:10.2214/AJR.20.23467
40. Houssami N, Lockie D, Giles M, Noguchi N, Marr G, Marinovich ML. Two-year follow-up of participants in the BreastScreen Victoria pilot trial of tomosynthesis versus mammography: breast density-stratified screening outcomes. Br J Radiol. 2023;96(1148):20230081. doi:10.1259/bjr.20230081
41. Peintinger F. National Breast Screening Programs across Europe. Breast Care. 2019;14(6):354–358. doi:10.1159/000503715
42. Ren W, Chen M, Qiao Y, Zhao F. Global guidelines for breast cancer screening: a systematic review. Breast. 2022;64:85–99. doi:10.1016/j.breast.2022.04.003
43. Trentham-Dietz A, Kerlikowske K, Stout NK, et al. Tailoring breast cancer screening intervals by breast density and risk for women aged 50 years or older: collaborative modeling of screening outcomes. Ann Internal Med. 2016;165(10):700–712. doi:10.7326/M16-0476
44. Taylor R, Page A, Bampton D, Estoesta J, Rickard M. Age-specific interval breast cancers in New South Wales and meta-analysis of studies of women aged 40–49 years. J Med Screen. 2004;11(4):199–206. doi:10.1258/0969141042467403
45. Henderson LM, Miglioretti DL, Kerlikowske K, Wernli KJ, Sprague BL, Lehman CD. breast cancer characteristics associated with digital versus film-screen mammography for screen-detected and interval cancers. Am J Roentgenol. 2015;205(3):676–684. doi:10.2214/AJR.14.13904
46. Nguyen TL, Li S, Dite GS, et al. Interval breast cancer risk associations with breast density, family history and breast tissue aging. Int J Cancer. 2020;147(2):375–382. doi:10.1002/ijc.32731
47. Henderson JT, Webber EM, Weyrich MS, Miller M, Melnikow J. Screening for breast cancer: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2024;331(22):1931–1946. doi:10.1001/jama.2023.25844
48. Goh S, Hartman M. From promise to practice: harnessing artificial intelligence for breast cancer screening. Intelligent Oncol. 2025;1(1):4–6. doi:10.1016/j.intonc.2024.11.001
49. Lauritzen AD, Lillholm M, Lynge E, Nielsen M, Karssemeijer N, Vejborg I. Early indicators of the impact of using AI in mammography screening for breast cancer. Radiology. 2024;311(3):e232479. doi:10.1148/radiol.232479
50. Moger TA, Å H, Hanestad B, Hofvind S. Costs and effects of implementing digital tomosynthesis in a population-based breast cancer screening program: predictions using results from the to-be trial in Norway. Pharmacoecon Open. 2022;6(4):495–507. doi:10.1007/s41669-022-00343-5
51. Bakker MF, SVd L, Pijnappel RM, et al. Supplemental MRI screening for women with extremely dense breast tissue. NEJM. 2019;381(22):2091–2102. doi:10.1056/NEJMoa1903986
52. Gabrielson M, Hammarström M, Bergqvist J, et al. Baseline breast tissue characteristics determine the effect of tamoxifen on mammographic density change. Int J Cancer. 2024;155(2):339–351. doi:10.1002/ijc.34939
53. Goh S, Goh RSJ, Chong B, et al. Systematic review of challenges in implementing artificial intelligence in breast cancer screening programs: towards a framework for safe adoption; 2024.
54. Mullooly M, White G, Bennett K, O’Doherty A, Flanagan F, Healy O. Retrospective radiological review and classification of interval breast cancers within population-based breast screening programmes for the purposes of open disclosure: a systematic review. Eur J Radiol. 2021;138:109572. doi:10.1016/j.ejrad.2021.109572
55. Chia JLL, He GS, Ngiam KY, Hartman M, Ng QX, Goh SSN. harnessing artificial intelligence to enhance global breast cancer care: a scoping review of applications, outcomes, and challenges. Cancers. 2025;17(2):197. doi:10.3390/cancers17020197
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.