Back to Journals » Journal of Pain Research » Volume 18
Current Status, Trends, and Forecast Analysis of LBP Disease Burden Attributable to Occupational Ergonomic Factors in China
Authors Yang X ![]() , Li R, Shu J, Chen H
, Li R, Shu J, Chen H
Received 23 April 2025
Accepted for publication 12 August 2025
Published 16 October 2025 Volume 2025:18 Pages 5493—5506
DOI https://doi.org/10.2147/JPR.S536096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Xueneng Yang,1 Ruijuan Li,2 Jun Shu,1 Hanbo Chen1
1Department of Traumatic Orthopedics, The Second Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 2Department of Burn, The Second Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China
Correspondence: Hanbo Chen, Email [email protected]
Objective: With the acceleration of population aging and industrial structural transformation in China, LBP related to occupational ergonomic factors has become an increasingly serious public health issue. This study aims to assess the disease burden of LBP caused by occupational ergonomic factors in China, reveal its long-term trends, key driving factors, and future changes, fill existing research gaps, and provide scientific evidence for optimizing occupational health policies and intervention strategies for high-risk populations.
Methods: Data on Years Lived with Disability (YLDs), YLD rates, and age-standardized YLD rates for occupational ergonomics-related LBP from 1990 to 2021 were obtained from the Global Burden of Disease Study 2021. Joinpoint regression was used to analyze temporal trends. Age-period-cohort (APC) models assessed the effects of age, time period, and birth cohort. Decomposition analysis quantified contributions from population aging, epidemiological shifts, and growth. Bayesian APC (BAPC) models projected disease burden trends through 2040.
Results: In 2021, China had 3.314 million YLDs from occupational ergonomics-related LBP, with a crude YLD rate of 232.9/100,000 and an age-standardized rate of 178.4/100,000. Women and individuals aged 50– 54 bore higher burdens. From 1990 to 2021, total YLDs slightly increased, but YLD rate and age-standardized rate declined annually by 0.3% and 1.5%, respectively. APC modeling revealed significant period and cohort effects. Decomposition analysis identified epidemiological changes as the primary driver of burden shifts. Projections indicate that by 2040, age-standardized YLD rates will fall to 194.3/100,000, but total YLDs will rise among people aged 60+, reflecting aging and cumulative occupational exposure.
Conclusion: Occupational ergonomic-related LBP remains a significant burden in China, especially among older and high-risk workers. Although the per capita burden is decreasing, demographic shifts and work-related exposures will sustain overall burden. Comprehensive ergonomic interventions and targeted prevention for high-risk groups are essential for improving occupational health and guiding policy development.
Keywords: occupational ergonomic factors, LBP, disease burden, age-period-cohort model, trend prediction
Introduction
Low back pain (LBP) is a common musculoskeletal disorder defined as pain or discomfort in the area between the lower edge of the twelfth rib and the lower hip fold, with or without leg radiation symptoms.1,2 Epidemiological statistics show that about 23% of the global population is affected by it, of which 11–12% of patients suffer from dysfunction or disability due to it.3 LBP not only severely affects the quality of life of individuals, but is also a major public health problem leading to lost productivity.4,5 According to statistics, LBP causes about 69 million annual labor losses, and the related medical and economic expenditures of various countries are as high as 37 billion to 100 billion US dollars,6–8 which has become the core factor restricting labor efficiency and social development. Occupational ergonomics factors are the leading cause of LBP9 and cover systemic risks such as work environment design, task execution, and organization management.10 Studies have shown that occupational ergonomics abnormalities contribute to 126.1 million global epidemics of LBP11 and 15.1 million Years Lived with Disability (YLD) among the working-age population, a cumulative increase of 27% since 1997, and that such risks directly contribute to sick leave, job adjustment or early retirement for 12% of workers,10,12 resulting in a global productivity loss of US $216.1 billion. The intensity of its impact is highly correlated with the industrial structure: high-income countries are dominated by static loads of sedentary office workers, while low-income countries are concentrated on dynamic loads of manufacturing and agriculture.13 China is in the stage of rapid economic development and industrialization acceleration. The changes in labor structure and working environment make the problem of LBP related to occupational ergonomics increasingly prominent. In this context, assessing the overall disease burden of LBP caused by occupational ergonomics factors in China is of urgent significance for formulating scientific occupational health policies and optimizing worker health management strategies.
However, current systematic studies on the burden of low back pain (LBP) related to occupational ergonomic factors in China remain relatively limited, particularly in terms of long-term trends, key driving factors, and future burden projections. Existing research mostly focuses on static descriptions and has not fully accounted for the dynamic interactions between multiple factors such as population aging and occupational structure adjustments. Previous studies have shown that occupational ergonomic factors are the main contributor to the burden of LBP in China, with an attributable fraction of 24% (95% uncertainty interval: 22–26%), resulting in the loss of approximately 2.86 million Disability-adjusted Life Years (DALYs) annually.11 However, due to population aging and changes in industrial structure, patterns of ergonomic exposure have shifted. The proportion of LBP cases related to physical workload in traditional manufacturing has decreased, while cases linked to static load (prolonged sitting) among office workers and dynamic load (manual handling) in emerging service industries have increased. As a common chronic disease, LBP has been listed as a key area of prevention and control in the “Healthy China 2030” plan. Therefore, quantifying the current burden of LBP related to occupational ergonomic factors and predicting future trends based on current data are important for evaluating the effectiveness of prevention strategies and health resource allocation, and can provide evidence to support policy making and resource distribution.
Disease burden is an important measure of the impact of diseases on population health and is widely used in epidemiology and public health research. YLD is one of the core indicators for assessing disease burden, and it quantifies the loss of healthy life years caused by illness or disability.14 YLD reflects the number of years lived with disability, adjusted by disability weight (DW), to capture the overall level of health loss. Compared with traditional incidence rates, YLD accounts for both the severity and duration of disability, showing the effect of diseases on quality of life. This indicator is often used to assess the impact of non-fatal diseases (such as diabetes and LBP) and various disabilities (such as hearing loss and spinal cord injury) on population health, and it provides scientific evidence for setting priorities in disease control and allocating health resources.
This study used standardized data from the Global Burden of Disease Study 2021 (GBD 2021)14 to analyze changes in the burden of LBP caused by occupational ergonomic factors in China over the past 30 years. First, we applied the Joinpoint regression model to identify key time points in disease burden trends from 1990 to 2021, and used average annual percent change (AAPC) to quantify these trends. Second, we used the age-period-cohort (APC) model to assess the effects of age, period, and birth cohort on disease burden, and to explore differences across groups. Third, we performed decomposition analysis to quantify the contributions of population aging, epidemiological changes, and population growth to changes in disease burden. Finally, we constructed a Bayesian age-period-cohort model (BAPC) to predict future trends in the burden of LBP related to occupational ergonomic factors from 2022 to 2040. Through the above analysis, this study aims to provide quantitative evidence for optimizing occupational health policies in China, supporting the identification of high-risk populations, precise allocation of resources, and the development of long-term intervention strategies.
Materials and Methods
Data Sources
To analyze changes in the disease burden of LBP caused by occupational ergonomic factors, we used data from the Global Burden of Disease Study 2021 (GBD 2021), which follows the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER). To our knowledge, the GBD database is the most comprehensive and widely used public source for data on LBP related to occupational ergonomic factors. GBD 2021 covers the burden of 371 diseases in 204 countries and regions and 811 subnational areas worldwide. Open-access data used in this study were obtained from the GBD 2021 database, including: (1) the number of YLDs, YLD rates, and age-standardized rates of LBP due to occupational ergonomic factors in China from 1990 to 2021 for three sex groups (all, male, and female); and (2) global population projections from 2022 to 2040.
Definitions
In GBD 2021, LBP due to occupational ergonomic factors is defined as pain in the area from the lower margin of the twelfth ribs to the lower gluteal folds on the posterior aspect of the body (with or without pain radiating to one or both lower limbs) that lasts for at least one day (ICD-10: M54.3, M54.4, and M54.5). In this study, YLD was chosen as the main indicator to measure the disease burden of LBP caused by occupational ergonomic factors. The study population included individuals aged 0 to 95 years and above. Cases under 15 years of age were not included in the analysis, and due to the small number of cases in those over 85 years old, these were combined into the 80–84 age group and labeled as 80+ years. Two key indicators were analyzed: case numbers and age-standardized rates. Case number refers to the original count recorded in GBD 2021, while the age-standardized rate represents the number of cases per 100,000 people after adjusting for age structure, allowing for more consistent comparisons across regions. All original data from GBD 2021 are provided with 95% uncertainty intervals (UI), calculated through aggregation and weighting methods.
Ethics Committee
This study was exempt from ethical review by the ethics committee in accordance with Item 1 and Item 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects, effective February 18, 2023, China.
Statistical Analysis
The following statistical methods were used in this study: (1) Joinpoint regression analysis: Joinpoint software (version 5.1.0) was used to calculate annual percent change (APC) and average annual percent change (AAPC). Joinpoint regression is a common method for analyzing disease trends, allowing identification of significant inflection points and overall trends over specific time periods. (2) Age-period-cohort (APC) model: The data were analyzed from three perspectives—age, period, and cohort effects—to interpret the role of each dimension in the disease burden. (3) Decomposition analysis: This method was used to assess the independent effects of changes in population age structure, population growth, and epidemiological factors on the trend of LBP disease burden due to occupational ergonomic factors. By comparing ideal scenarios with actual results (while controlling for other variables), the contribution of each factor was evaluated. (4) Trend prediction: Based on population data from 2022 to 2040, the Bayesian age-period-cohort (BAPC) model in R was used to predict future trends. This model improves prediction accuracy and avoids issues of mixing and convergence found in traditional Bayesian methods (see supplementary materials for details).
All statistical analyses and data visualization were conducted in R version 4.3.1, with statistical significance set at P < 0.05.
Results
Burden of LBP Due to Occupational Ergonomic Factors in China, 2021
In 2021, the total number of YLDs caused by LBP related to occupational ergonomic factors in China was 3,314,128.7 (95% uncertainty interval: 2,275,895.5–4,532,168.1). The YLD rate was 232.9 (160.0–318.6) per 100,000, and the age-standardized YLD rate was 178.4 (122.5–243.6) per 100,000. All indicators were higher in females than in males. Females had 1,916,297.6 (1,268,797.0–2,697,981.0) YLDs, while males had 1,397,831.1 (934,966.0–1,938,797.6) YLDs. The YLD rate for females was 275.9 (182.7–388.4) per 100,000, and for males it was 192.0 (128.4–266.3) per 100,000. The age-standardized YLD rate for females was 208.0 (140.9–286.3) per 100,000, compared to 149.8 (100.2–207.7) per 100,000 for males.
By age group, YLDs due to occupational ergonomic factors increased with age, peaking at 530,510.7 in the 50–54 age group, and then declined. Analysis by sex showed that males had a lower burden of LBP related to occupational ergonomic factors than females, with the difference being most pronounced in the 50–59 age group (see Table 1 for details).
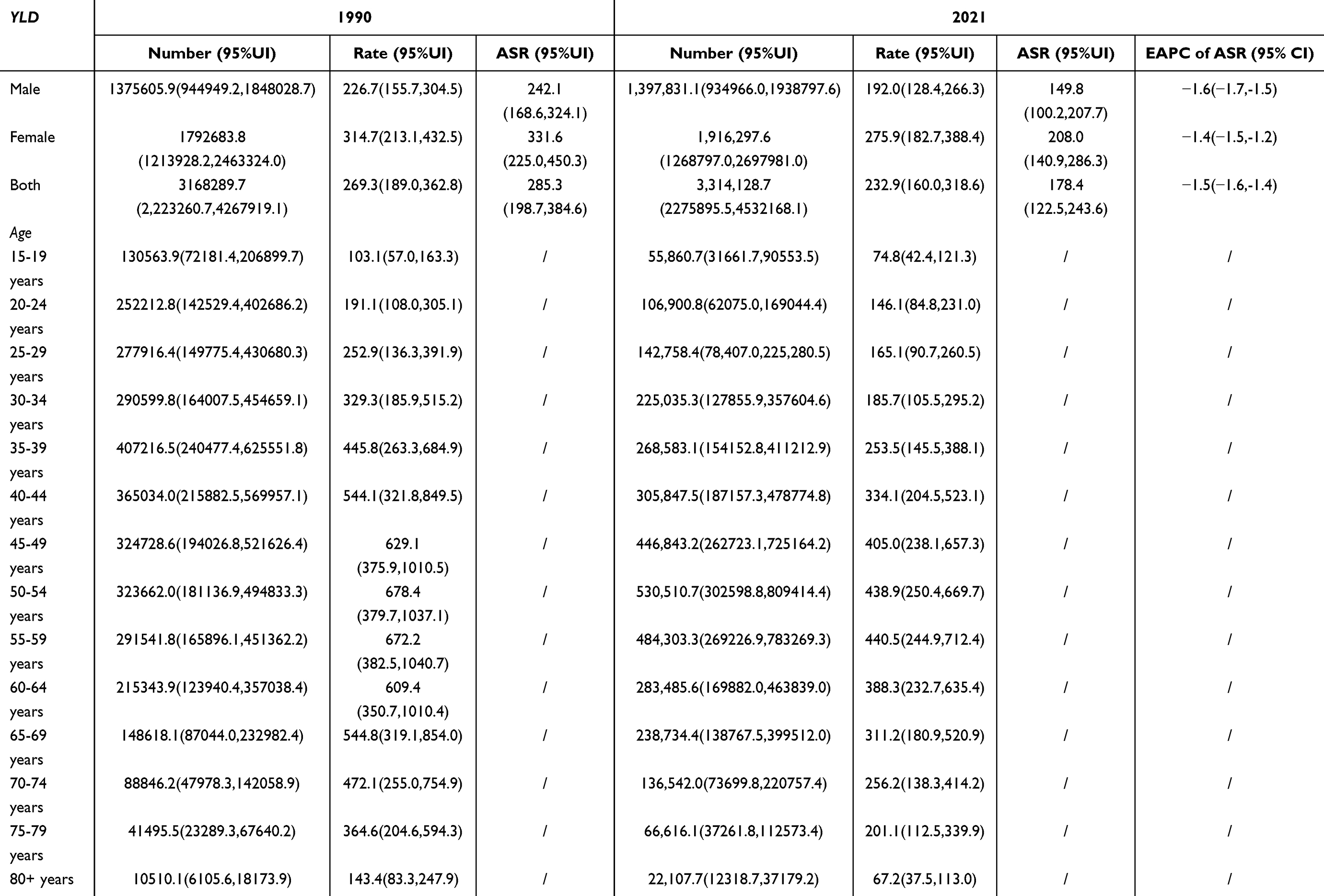 |
Table 1 Burden of Low Back Pain Attributable to Occupational Ergonomic Factors in China in 1990 and 2021 |
Trends in the Burden of LBP Due to Occupational Ergonomic Factors in China, 1990–2021
From 1990 to 2021, the overall burden of LBP caused by occupational ergonomic factors in China showed a decreasing trend. The number of YLDs increased from 3,168,289.7 (95% uncertainty interval: 2,223,260.7–4,267,919.1) in 1990 to 3,314,128.7 (2,275,895.5–4,532,168.1) in 2021, with an estimated annual percent change (EAPC) of 0.3 (0.2–0.4). The YLD rate decreased from 269.3 (189.0–362.8) per 100,000 in 1990 to 232.9 (160.0–318.6) per 100,000 in 2021 (EAPC = −0.3, 95% CI: −0.4, −0.2), and the age-standardized YLD rate declined from 285.3 (198.7–384.6) per 100,000 to 178.4 (122.5–243.6) per 100,000 (EAPC = −1.5, 95% CI: −1.6, −1.4) (see Figure 1).
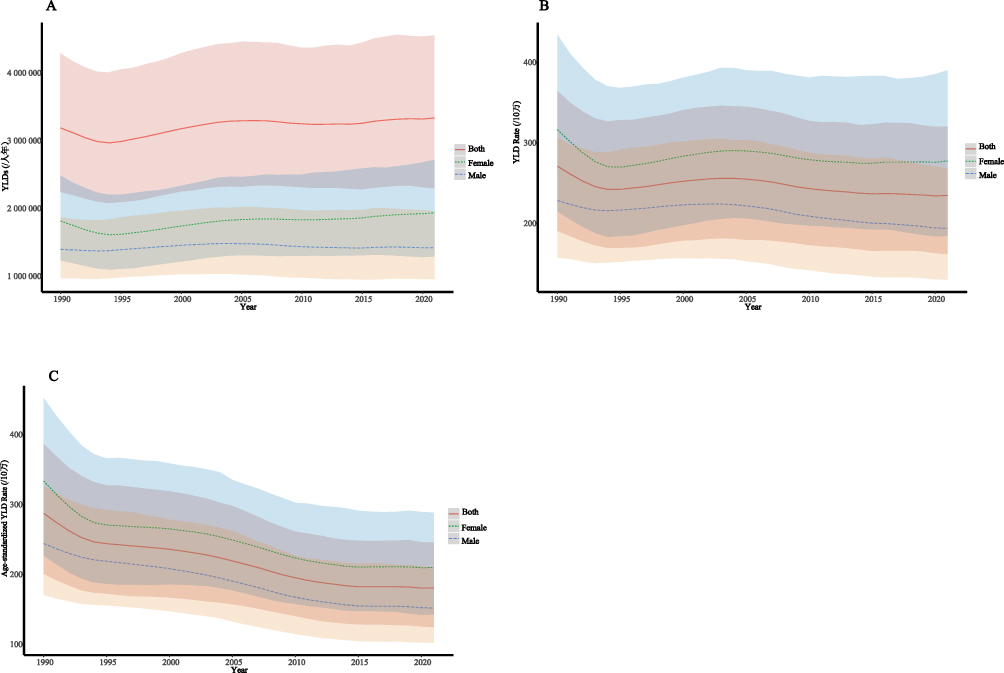 |
Figure 1 Time trends in the burden of LBP related to occupational ergonomic factors in China, 1990–2021 (A) Trends in YLDs (total, male, female); (B) Trends in YLD rate (total, male, female); (C) Trends in age-standardized YLD rate (total, male, female). |
By sex, both males and females experienced a slight increase in the number of YLDs from occupational ergonomic factors over this period, but both the YLD rate and the age-standardized YLD rate decreased. Overall, females consistently had a higher burden of LBP than males (see Figure 1).
By age group, the YLD rate for occupational ergonomic-related LBP showed a downward trend across all age groups from 1990 to 2021, with the 50–59 age group remaining the highest. In addition, the trends in the number of YLDs varied by age, with the 35–59 age group accounting for the largest number of cases throughout the period (see Figure 2).
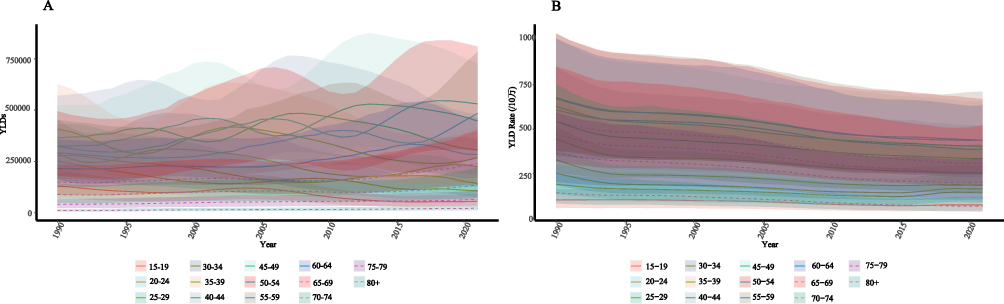 |
Figure 2 Time trends in the burden of LBP related to occupational ergonomic factors by age group in China, 1990–2021 (A) Trends in YLDs by age group (total, male, female); (B) Trends in YLD rate by age group (total, male, female). |
Joinpoint Regression Analysis of the Burden of LBP Due to Occupational Ergonomic Factors in China, 1990–2021
From 1990 to 2021, the average annual percent change (AAPC) in the number of YLDs, YLD rate, and age-standardized YLD rate for LBP caused by occupational ergonomic factors in China was 0.160 (95% CI: 0.117–0.202), −0.460 (95% CI: −0.504 - −0.416) and −1.492 (95% CI: −1.549 - −1.435), p<0.01, respectively (see Figure 3).
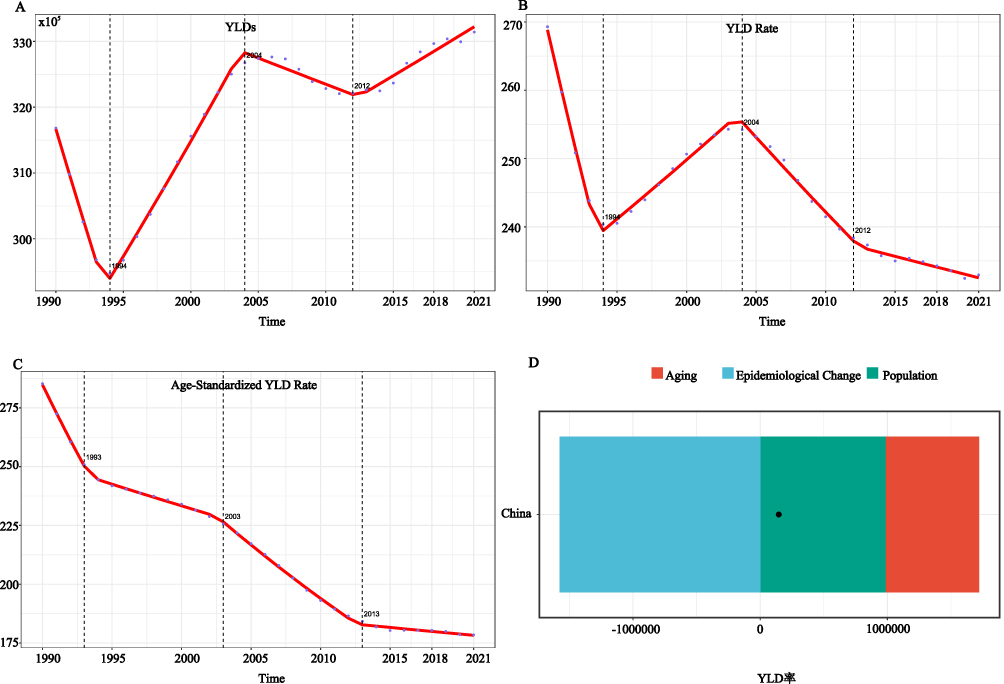 |
Figure 3 Joinpoint regression models for the burden of LBP related to occupational ergonomic factors in China, 1990–2021 (A) Joinpoint regression model for YLDs; (B) Joinpoint regression model for YLD rate; (C) Joinpoint regression model for age-standardized YLD rate; (D) Decomposition analysis of YLD rate. |
Age-Period-Cohort Analysis of the Burden of LBP Due to Occupational Ergonomic Factors in China, 1990–2021
Between 1990 and 2021, the net drift of the YLD rate for LBP caused by occupational ergonomic factors in China was −1.37, indicating an overall downward trend. The age effect showed that the YLD rate increased with age, peaked in the 52.5-year age group, and then declined. For the period effect, using 2004 as the reference year (relative risk, RR = 1.00), the YLD rate decreased steadily, reaching its lowest point in 2019 (RR = 0.79). The cohort effect showed a clear decreasing trend as well; with the 1957 birth cohort as the reference (RR = 1.00), the YLD rate declined in later cohorts, reaching the lowest level in the 2002 cohort (RR = 0.57) (see Figure 4).
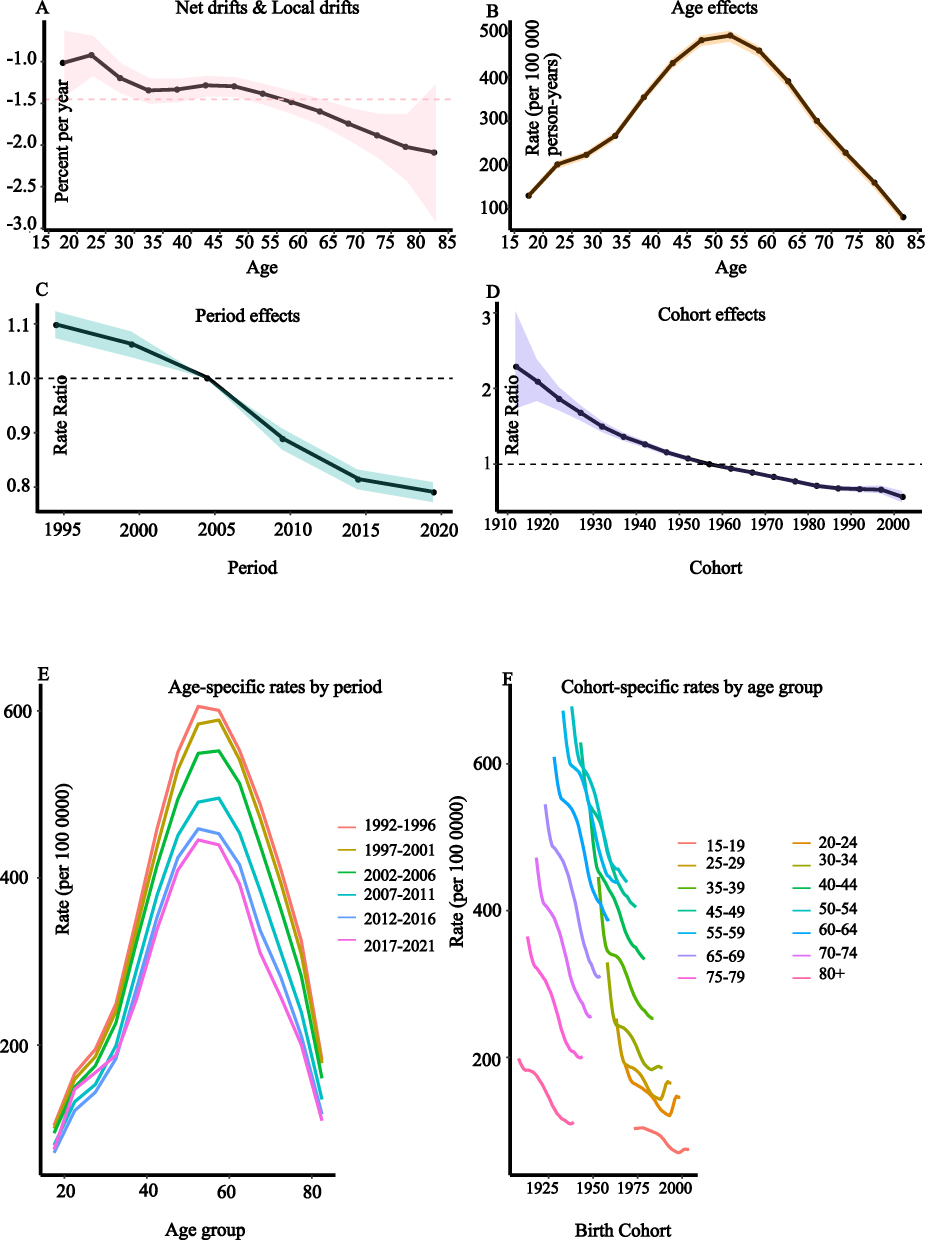 |
Figure 4 APC model of YLD rate for LBP related to occupational ergonomic factors in China (A) Overall effect on YLD rate; (B) Age effect on YLD rate; (C) Period effect on YLD rate; (D) Cohort effect on YLD rate; (E and F) Age-cohort effects on YLD rate. |
Decomposition Analysis of the Burden of LBP Due to Occupational Ergonomic Factors
To assess the effects of population aging, epidemiological changes, and population growth on the trend of LBP burden caused by occupational ergonomic factors from 1990 to 2021, a decomposition analysis was performed. The results showed that changes in the YLD rate were mainly attributed to factors other than age structure and population size. The absolute contribution of these other factors was −1,575,599.0, with a relative contribution of −1,080.4% (see Figure 3).
Projection of the Burden of LBP Due to Occupational Ergonomic Factors
Using population projections from 2022 to 2040, this study applied a Bayesian age-period-cohort (BAPC) model to predict future trends in the burden of LBP caused by occupational ergonomic factors in China over the next 20 years. In the analysis, solid lines represent observed data from the GBD 2021 report (1990–2021), while dashed lines indicate predictions for 2022–2040 based on the BAPC model within the INLA framework.
The results show that the age-standardized YLD rate for occupational ergonomic-related LBP in China is expected to continue decreasing, reaching 194.3 per 100,000 by 2040. The total number of YLDs is projected to decline to 2,278,621.6 by 2040. Age-specific analysis suggests that YLD rates will decrease across all age groups, but the total number of YLDs among people aged 60 years and above is expected to rise (see Figure 5).
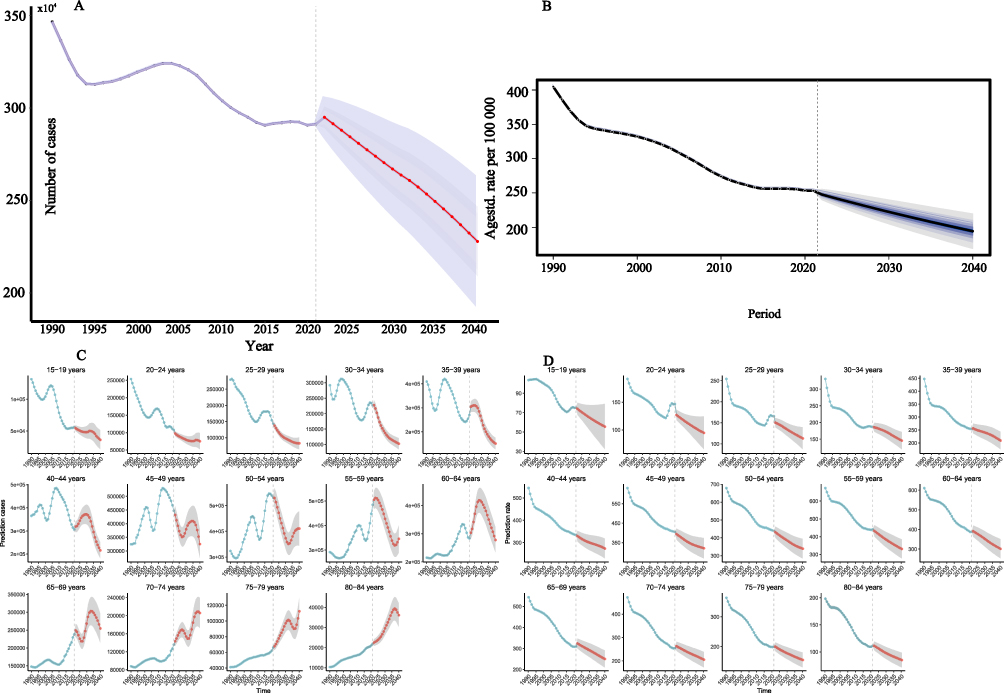 |
Figure 5 Projections of the burden of LBP related to occupational ergonomic factors in China, 2022–2040 (A) Projected YLDs; (B) Projected age-standardized YLD rate; (C) Projected YLDs by age group; (D) Projected YLD rate by age group. |
Discussion
Using data from the Global Burden of Disease Study 2021 (GBD 2021), this study systematically described the dynamic patterns, trends, and main drivers of the burden of LBP related to occupational ergonomic factors in China. The results showed significant differences in disease burden by sex, age, and over time in 2021. Specifically, the total number of YLDs from occupational ergonomic-related LBP was 3.314 million (95% uncertainty interval: 2.276–4.532 million), with an age-standardized YLD rate of 178.4 per 100,000. Females had a higher disease burden than males (age-standardized YLD rate: 208.0 vs 149.8 per 100,000), and the greatest burden was observed in the 50–54 age group (531,000 YLDs). From 1990 to 2021, the total YLDs increased (AAPC = 5,029.234%), while both the YLD rate and age-standardized YLD rate declined annually by −0.3% and −1.5%, respectively (EAPC = −0.3%, EAPC = −1.5%). Age-period-cohort (APC) analysis indicated that both the period effect after 2004 (2019 RR = 0.79) and the declining risk in younger birth cohorts (2002 cohort RR = 0.57) contributed to the overall reduction in disease burden. Decomposition analysis further confirmed that non-demographic factors, mainly epidemiological changes, were the main contributors to the decrease in the age-standardized rate, with an absolute contribution of −1,575,599.0 and a relative contribution of −1,080.4%. Future projections suggest that by 2040, the age-standardized YLD rate will decline to 194.3 per 100,000, but the total YLDs among those aged 60 and above will continue to rise, highlighting ongoing challenges from both population aging and cumulative occupational exposure. These findings underscore the public health importance of occupational ergonomic-related LBP in China and provide key evidence for optimizing industry-specific ergonomic standards and developing targeted workforce health management strategies.
High Overall Burden but Declining Trend
China has had a high global burden of LBP due to occupational ergonomic factors for many years. In 2021, the total YLDs from occupational ergonomic-related LBP reached 3,314,128.7, reflecting a significant disease burden. This can be attributed to China’s large population, rapidly changing demographics, diverse work environments, and uneven distribution of medical resources. Decomposition analysis showed that, while epidemiological changes are the main driver of changes in YLDs, population aging and growth also have substantial impacts. The relative contributions of population aging and growth to total YLDs were 503.9% and 676.5% respectively, together exceeding the contribution of epidemiological factors. This highlights the deep influence of demographic transition on disease burden. With the acceleration of population aging, the burden of LBP is expected to increase.15 By 2023, the population aged 60 years and above had reached 297 million, accounting for 21.1% of the total population, with an average annual growth rate of 3.2%.16 In the next 20 years, China is projected to become one of the most aged countries in the world.15 Aging increases the absolute number of LBP cases, and age-stratified analysis also confirms that older adults are at higher risk for a heavier disease burden. In addition, rapid urbanization and industrialization have further increased the health burden of occupational ergonomic-related LBP. Urbanization has led to more sedentary jobs (such as office and computer work), raising the risk of chronic LBP due to muscle and soft tissue strain.17–20 At the same time, industrialization has resulted in large numbers of workers engaged in high-intensity, repetitive physical labor, increasing the risk of spinal degeneration and injury.21–24 Uneven distribution of medical resources is also a key reason for the current heavy burden of LBP. There are significant differences in healthcare resources between urban and rural areas, and a shortage of specialized spine surgeons in primary healthcare means that many patients cannot receive timely, standardized treatment, which increases the health and social burden.25,26 Despite these challenges, it is notable that the burden of occupational ergonomic-related LBP in China is showing a downward trend. The annual percent change in YLD rate and age-standardized YLD rate is −0.3% and −1.5%, respectively (EAPC = −0.3%, EAPC = −1.5%), reflecting a gradual reduction in per capita burden. This trend is consistent with previous research9,11 and may be related to strengthened public health interventions, improved health policies, and the active promotion of health strategies in recent years.
Epidemiological Dominance, Sex and Age Differences, and Distinct Period and Cohort Effects in Disease Burden
This study found that the burden of LBP due to occupational ergonomic factors in China is strongly influenced by epidemiological factors, with clear differences by sex and age, as well as notable period and birth cohort effects.
By dividing the disease burden into three components—population aging, population growth, and epidemiological factors—and quantifying their effects, the analysis showed that epidemiological factors had an absolute contribution of −1,575,599.0 and a relative contribution of −1,080.4% to the burden of LBP. This indicates that epidemiological factors play a dominant role in changes in disease burden, which is consistent with previous studies.11
Sex and age differences also exhibit a distinct pattern in the burden of LBP, characterized by a generally higher burden among females and a higher incidence in middle-aged groups. This pattern has been reported across many countries.9,27 The higher burden among females may be associated with physiological, anatomical, and behavioral differences. First, hormonal fluctuations in females are more pronounced than in males. Changes in estrogen and progesterone levels before and after menstruation, as well as the withdrawal of progesterone after pregnancy, can affect pain sensitivity.28 Additionally, the sharp decline in estrogen after menopause may lead to osteoporotic LBP.29 In contrast, testosterone in males has a protective effect due to its anti-inflammatory and analgesic properties, which may reduce males’ sensitivity to pain. Anatomical differences also play a significant role. Males typically have greater muscle mass and stronger skeletal structures than females, which may offer more resistance to lumbar strain.30,31 Moreover, females tend to have wider pelvises and more pronounced lumbar lordosis, which significantly increases lumbar load during pregnancy. The anterior shift of the body’s center of gravity in pregnancy leads to increased strain on lumbar muscles and ligaments, causing relaxation and chronic overuse injuries28 Behavioral factors also contribute to the observed sex differences. Females often take on caregiving responsibilities at home, such as looking after children. Activities like frequent bending and lifting of children increase lumbar load and accelerate the onset of LBP. Additionally, specific occupational or daily movement patterns may raise LBP risk in females. For instance, female physical therapists who climb stairs less frequently may have a higher risk of developing LBP, as stair climbing strengthens the gluteus maximus, and weakness in this muscle is associated with LBP.32,33 Psychological and emotional factors may further influence the development and prognosis of LBP in females. Women are generally more susceptible to stress, which can contribute to the onset of LBP. Studies have shown that under high cognitive load and psychological stress, females may have a stronger tendency to suppress negative thoughts, which can exacerbate depressive symptoms and subsequently affect physical health, including the occurrence of LBP.34
Age-stratified analysis and the APC model both indicate that middle-aged adults, especially those aged 50–59, carry the highest burden of LBP.11 This is closely linked to degenerative changes in the spine and the cumulative effects of occupational exposure. With aging, structures such as intervertebral discs, joints, and ligaments gradually degenerate, and long-term repetitive mechanical stress can cause tissue damage and nerve sensitization, triggering or worsening LBP.35–37 Occupational exposure also shows a dose-cumulative effect, where long-term work in high-risk settings reduces the body’s self-repair capacity and increases the incidence of LBP in middle age. Some studies have found that LBP can begin in adolescence, and without effective prevention and intervention, it tends to become more common and severe in later adulthood.38
In addition, the APC model revealed clear period and cohort effects for occupational ergonomic-related LBP in China. The period effect analysis showed a downward trend in disease burden following the introduction of the Occupational Disease Prevention Law and strengthened occupational health management in the early 21st century.39,40 Advances in medical technology (such as the wider use of infrared therapy and shockwave treatments)40,41 and improved health awareness (including health education and promotion of core muscle exercises)42,43 have also played a positive role in reducing the disease burden. The decreasing cohort effect suggests that new generations of workers are benefiting from better occupational protection and greater health awareness, leading to a gradual reduction in the risk of LBP.
In summary, prevention and control of occupational ergonomic-related LBP is not only a challenge for clinical practice, but also requires effective policy implementation, balanced allocation of rehabilitation resources, and focused interventions for high-risk groups such as women and middle-aged adults. A comprehensive, multi-level approach will help build a health management system that meets the needs of China’s changing population and occupational landscape.
Public Health Recommendations: Improving Age-Standardized Rates and Addressing the Rising Burden Among Older Adults
Projections for occupational ergonomic-related LBP in China show a divided pattern: age-standardized YLD rates are expected to decline from 178.4 per 100,000 in 2021 to 194.3 per 100,000 in 2040 (an average annual decrease of 0.92%), suggesting that the use of ergonomic technologies (such as ergonomic chairs) and occupational health policies (such as the Occupational Disease Prevention Law) have had initial positive effects.39,40 However, the total YLDs among people aged 60 and above will continue to rise, mainly due to the accelerating trend of population aging and the delayed effects of cumulative occupational injuries. According to recent policy documents, the statutory retirement age in China has generally been extended by 1 to 3 years, which has, to some extent, prolonged the working period of middle-aged and older adults, thereby increasing their occupational health risks. To address these trends, it is recommended to build an integrated intervention network covering prevention, treatment, and management. At the technical level, initiatives such as the “lumbar support device trials in Yunnan” could serve as a model. Age-appropriate ergonomic designs, such as lumbar exoskeletons, should be promoted in industries with a high proportion of older workers, such as domestic services. For health management, spinal function screening should be included in routine health check-ups to help reduce the cumulative effect of physical load.3 In terms of medical resource allocation, spinal health management centers should be established within community healthcare systems to expand access to non-pharmacological therapies (such as heat therapy and core muscle training). On the policy level, linking retirement policies with chronic LBP work injury insurance, and making use of AI-based risk prediction models, can help target high-risk sectors and populations more precisely. These measures may help to mitigate the combined risks from aging and occupational exposure and offer valuable experience for global occupational health management.
Limitations
Although this study provides a comprehensive assessment and projection of the burden of LBP related to occupational ergonomic factors in China, several limitations should be noted. First, the analysis mainly relied on the GBD database, which may have incomplete or outdated data in some low-income or remote areas, potentially leading to an underestimation of the disease burden. Additionally, the reliance on secondary data from the GBD database necessitates considering the impact of data quality and potential biases, which may affect the accuracy of the results. Second, the BAPC model used for future projections did not fully account for external factors such as policy changes and advances in medical interventions, which may affect the accuracy of the predictions. Furthermore, although key factors such as sex, age, and population aging were considered, other important variables—such as socioeconomic status, access to medical resources, and chronic comorbidities—were not fully included, which may limit the overall interpretation of the disease burden. Finally, due to the lack of detailed provincial and urban data, regional differences could not be analyzed. Variations in economic development, healthcare resource allocation, and health policies across regions may lead to significant geographical differences in disease burden. Future research should use more diverse data sources, improve the adaptability of prediction models to external variables, and fully consider regional differences and potential influencing factors to enhance the scientific value and accuracy of disease burden assessments.
Conclusion
Based on data from the GBD 2021 database, this study analyzed the burden, trends, driving factors, and future projections of LBP caused by occupational ergonomic factors in China over the past 30 years. The findings indicate that the overall burden remains high, with an age-standardized rate continuing to decline. However, due to population aging and cumulative occupational exposure, the burden among older adults is increasing. The observed sex and age differences, as well as period and cohort effects, highlight high-risk groups and key intervention windows. With the aging population and changes in occupational structure, the prevention and control of occupational ergonomic-related LBP will remain a challenge in the future. Based on the study’s findings, it is recommended to: 1) develop an integrated system of prevention, treatment, and management by improving ergonomic technology, strengthening health management, balancing medical resources, and promoting policy innovation; and 2) pay special attention to older adults and high-risk occupational groups to support the ongoing improvement of occupational health policies.
Abbreviations
AAPC, Average annual percentage change; APC, Annual percentage change; BAPC, Bayesian age-period-cohort; DALYs, Disability-adjusted life years; EAPC, Estimated Annual percentage change; GBD, Global Burden of Disease; ICD, International Statistical Classification of Diseases; Uncertainty interval.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the authors used ChatGPT4.0 in order to polishing the language. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Data Sharing Statement
The relevant data from the literature is stored in the attachments. For further inquiries, please feel free to contact the author.
Ethics Approval and Consent to Participate
This study does not involve human ethical considerations.
Consent for Publication
All authors reviewed the final manuscript and provided their approval for submission.
Acknowledgments
This study did not receive any project funding.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vlaeyen M, Maher CG, Wiech K, et al. Low back pain. Nature Reviews Disease Primers. 2018;4(1):52. doi:10.1038/s41572-018-0052-1
2. Hoy M, March L, Brooks P, et al. The global burden of low back pain: estimates from the global burden of disease 2010 study. Ann Rheumatic Dis. 2014;73(6):968–974. doi:10.1136/annrheumdis-2013-204428
3. Maher U, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–747. doi:10.1016/S0140-6736(16)30970-9
4. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
5. Özüdoğru C, Canlı M, Ceylan İ, et al. Five times sit-to-stand test in people with non-specific chronic low back pain-a cross-sectional test-retest reliability study. Irish J Med Sci. 2023;192(4):1903–1908. doi:10.1007/s11845-022-03223-3
6. Hong R, Reed C, Novick D, et al. Costs associated with treatment of chronic low back pain: an analysis of the UK general practice research database. Spine. 2013;38(1):75–82. doi:10.1097/BRS.0b013e318276450f
7. Schofield S, Shrestha RN, Percival R, et al. The personal and national costs of early retirement because of spinal disorders: impacts on income, taxes, and government support payments. Spine J. 2012;12(12):1111–1118. doi:10.1016/j.spinee.2012.09.036
8. Katz JN. Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Joint Surg. 2006;88:21–24. doi:10.2106/JBJS.E.01273
9. Chen C, Chen M, Wu X, et al. Global, regional and national burden of low back pain 1990-2019: a systematic analysis of the global burden of disease study 2019. J Orthop Transl. 2022;32:49–58. doi:10.1016/j.jot.2021.07.005
10. Hulshof P, Pega F, Neupane S, et al. The effect of occupational exposure to ergonomic risk factors on osteoarthritis of hip or knee and selected other musculoskeletal diseases: a systematic review and meta-analysis from the WHO/ILO joint estimates of the work-related burden of disease and Injury. Environ Int. 2021;150:106349. doi:10.1016/j.envint.2020.106349
11. Zhang T, Tian Y, Li Y, et al. Time trends in the burden of low back pain and its associated risk factors in China from 1990 to 2019. J Orthop Transl. 2024;45:256–265. doi:10.1016/j.jot.2024.02.006
12. Schofield S, Shrestha RN, Passey ME, et al. Chronic disease and labour force participation among older Australians. Med J Aus. 2008;189(8):447–450. doi:10.5694/j.1326-5377.2008.tb02119.x
13. Sibson H, Harris AR, Yegian AK, et al. Associations of back muscle endurance with occupational back muscle activity and spinal loading among subsistence farmers and office workers in Rwanda [J]. PLoS One. 2024;19(11):e0309658. doi:10.1371/journal.pone.0309658
14. Ferrari AJ, Santomauro DF, Aali A, et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
15. Chen X, Xu P, Song P, et al. China has faster pace than Japan in population aging in next 25 years. Biosci Trends. 2019;13(4):287–291. doi:10.5582/bst.2019.01213
16. Bao Z, Zhou L, Liu G, et al. Current state of care for the elderly in China in the context of an aging population. Biosci Trends. 2022;16(2):107–118. doi:10.5582/bst.2022.01068
17. Rabal-Pelay C-O, Cimarras-Otal C, Berzosa C, et al. Spinal sagittal alignment, spinal shrinkage and back pain changes in office workers during a workday. Int J Occupational Safety Ergonomics. 2022;28(1):1–7. doi:10.1080/10803548.2019.1701238
18. Beller S, Sperlich S, Epping J, et al. Sociodemographic differences in low back pain: which subgroups of workers are most vulnerable? BMC Musculoskelet Disord. 2024;25(1):852. doi:10.1186/s12891-024-07970-5
19. Micheletti K, Bláfoss S, Sundstrup E, et al. Association between lifestyle and musculoskeletal pain: cross-sectional study among 10,000 adults from the general working population. BMC Musculoskeletal Dis. 2019;20(1):609. doi:10.1186/s12891-019-3002-5
20. Mörl B, Bradl I. Lumbar posture and muscular activity while sitting during office work. J Electromyography Kinesiol. 2013;23(2):362–368. doi:10.1016/j.jelekin.2012.10.002
21. Yang S, Kim W, Choi KH, et al. Influence of occupation on lumbar spine degeneration in men. The Korean national health and nutrition examination survey 2010-2013. Int Archiv Occupational Envir Health. 2016;89(8):1321–1328.
22. Badarin H, Hemmingsson T, Hillert L, et al. Physical workload and increased frequency of musculoskeletal pain: a cohort study of employed men and women with baseline occasional pain. Occup Environ Med. 2021;78(8):558–566. doi:10.1136/oemed-2020-107094
23. Moreira-Silva S, Seixas A, Mota J, et al. Associations between day and night-shifts, work-related musculoskeletal symptoms and absenteeism in the manufacturing industry. Int J Occupational Safety Ergonomics. 2024;30(3):867–871. doi:10.1080/10803548.2024.2358679
24. Moreira-Silva S, Seixas A, Ventura N, et al. Musculoskeletal symptoms among workers of the pulp and paper industry: the contribution of age, gender, body mass index and physical activity level. Int J Occupational Safety Ergonomics. 2024:1–8.
25. Chen Y, Yin Z, Xie Q. Suggestions to ameliorate the inequity in urban/rural allocation of healthcare resources in China. Int J Equity Health. 2014;13(1):34. doi:10.1186/1475-9276-13-34
26. Wang L, Li Y, Qin S, et al. The disequilibrium in the distribution of the primary health workforce among eight economic regions and between rural and urban areas in China. Int J Equity Health. 2020;19(1):28. doi:10.1186/s12939-020-1139-3
27. Soo A, Ang WS, Chong CH, et al. Occupational ergonomics and related musculoskeletal disorders among dentists: a systematic review. Work. 2023;74(2):469–476. doi:10.3233/WOR-211094
28. Matsuda T, Tsushima E, Yo K, et al. Relationship among childbirth, onset of lower back pain, and health-related quality of life in female patients with lower back pain: a retrospective study. Spine Surg Related Res. 2024;8(5):528–533. doi:10.22603/ssrr.2023-0295
29. Fistarol R, Campos F, Figueiredo Campos AL, et al. Time since menopause, but not age, is associated with increased risk of osteoporosis. Climacteric. 2019;22(5):523–526. doi:10.1080/13697137.2019.1634046
30. Bailey S, Sparrey CJ, Been E, et al. Morphological and postural sexual dimorphism of the lumbar spine facilitates greater lordosis in females. J Anatomy. 2016;229(1):82–91. doi:10.1111/joa.12451
31. Majchrzycki M, Mrozikiewicz PM, Kocur P, et al. Low back pain in pregnant women. Ginekologia polska. 2010;81(11):851–855.
32. Suzuki T, Tamakoshi K, Sakakibara H. Caregiving activities closely associated with the development of low-back pain among female family caregivers. J Clin Nurs. 2016;25(15–16):2156–2167. doi:10.1111/jocn.13167
33. Amabile L, Larson SL, Hoglund LT, et al. Greater number of weekly stairs climbed is associated with lower low back pain prevalence among female but not male physical therapists. PLoS One. 2023;18(10):e0292489. doi:10.1371/journal.pone.0292489
34. Konietzny C, Chehadi O, Streitlein-Böhme I, et al. Mild depression in low back pain: the interaction of thought suppression and stress plays a role, especially in female patients. Int J Behav Med. 2018;25(2):207–214. doi:10.1007/s12529-017-9657-0
35. Knezevic C, Candido KD, Vlaeyen JWS, et al. Low back pain. Lancet. 2021;398(10294):78–92. doi:10.1016/S0140-6736(21)00733-9
36. Cohen R, Raja S. Pathogenesis, diagnosis, and treatment of lumbar zygapophysial (facet) joint pain [J]. Anesthesiology. 2007;106(3):591–614. doi:10.1097/00000542-200703000-00024
37. Panjabi MM. The stabilizing system of the spine. Part I. function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383–389. doi:10.1097/00002517-199212000-00001
38. Hestbaek L-Y, Leboeuf-Yde C, Kyvik KO. Is comorbidity in adolescence a predictor for adult low back pain? A prospective study of a young population. BMC Musculoskeletal Dis. 2006;7(1):29. doi:10.1186/1471-2474-7-29
39. Wang L, Liu X, Sun X, et al. Focus and progress of the occupational health initiative. China CDC Weekly. 2020;2(47):906–909. doi:10.46234/ccdcw2020.232
40. Karppinen S, Simula AS, Holopainen R, et al. Evaluation of training in guideline-oriented biopsychosocial management of low back pain in occupational health services: protocol of a cluster randomized trial [J]. Health Sci Rep. 2021;4(1):e251. doi:10.1002/hsr2.251
41. Taheri K, Khosrawi S, Ramezani M. Extracorporeal shock wave therapy combined with oral medication and exercise for chronic low back pain: a randomized controlled trial. Arch Phys Med Rehabil. 2021;102(7):1294–1299. doi:10.1016/j.apmr.2020.12.008
42. Zhang W, Wan L, Wang X. The effect of health education in patients with chronic low back pain. J Int Med Res. 2014;42(3):815–820. doi:10.1177/0300060514527059
43. Luomajoki P, Pfeiffer F, Benz T. Low back pain - value of prevention and physiotherapy? Therapeutische Umschau Revue Therapeutique. 2023;80(4):175–182. doi:10.1024/0040-5930/a001432
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.