Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Current Physiotherapy Practice in Intensive Care Units Needs Cultural and Organizational Changes: An Observational Cross-Sectional Study in Two Albanian University Hospitals
Authors Shpata V ![]() , Kreka M, Tani K
, Kreka M, Tani K
Received 8 May 2021
Accepted for publication 14 June 2021
Published 8 July 2021 Volume 2021:14 Pages 1769—1781
DOI https://doi.org/10.2147/JMDH.S319236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vjollca Shpata,1 Manika Kreka,1,2 Klejda Tani1
1Faculty of Medical Technical Sciences, University of Medicine, Tirana, Albania; 2University Hospital Center “Mother Theresa”, Tirana, Albania
Correspondence: Vjollca Shpata
Faculty of Medical Technical Sciences, University of Medicine, Street of Dibra, Tirana, Albania
Tel +355 69 26 35 004
Fax +355 42 465298
Email [email protected]
Introduction: Although physiotherapy is beneficial to intensive care unit (ICU) patients and recommended by guidelines, the role of physiotherapy in ICU settings is not fully explored in Albania.
Purpose: To provide an overview of the current physiotherapy practice in Albanian ICUs and explore the involvement of physiotherapists and intensive care nurses regarding respiratory therapy and early mobility in the ICU.
Patients and Methods: This was an observational cross-sectional study, which included all ICU nurses working in six ICUs of University Hospital Center “Mother Theresa” and University Hospital of Trauma and all physiotherapists working in these hospitals. ICU nurses and hospital physiotherapists were approached to complete the survey regarding respiratory therapy and early mobility in critically ill patients.
Results: One hundred thirty-one completed questionnaires were returned from 189 questionnaires distributed to the survey participants (151 nurses and 38 physiotherapists); the response rate was 69.3%. Physiotherapy procedures were performed on a non-regular basis in ICUs in Tirana, Albania. Physiotherapists were not actively involved or exclusively employed in the ICU, and these ICUs did not use protocols for physiotherapist consultation. Physiotherapists occasionally performed respiratory therapy and early mobility in patients without an artificial airway. Nursing staff regularly performed airway suctioning in mechanically ventilated patients (100%) and participated in adjusting ventilator settings (82.2% regularly and 17.8% occasionally). In contrast, physiotherapists did not participate in these procedures and the early mobility of mechanically ventilated patients.
Conclusion: We report limited physiotherapy involvement in Albanian ICUs. Efforts should focus on improving physiotherapy practice in ICU, potentially making organizational and cultural changes in the ICU, and establishing protocols and guidelines.
Keywords: intensive care unit, physiotherapy, nurse, physiotherapist, critical patients care
Introduction
Critically ill patients are at risk of different complications due to their medical conditions and prolonged state of immobility, such as physical deconditioning or respiratory complications. Some of these complications can be addressed with physiotherapy procedures, such as early mobilization1,2 and respiratory care,1–3 in treating patients in the Intensive Care Unit (ICU).4
A growing body of evidence suggests that apart from being safe and feasible,5–7 physiotherapy procedures are beneficial for ICU patients and recommended by guidelines.8–13 However, the role and the involvement in the ICU of physiotherapy are not fully explored in some countries,14 including Albania.
The presence of the physiotherapists in the ICU has been recommended due to their contribution to the prevention and treatment of intensive unit care-acquired weakness,2 and early recovery of critically ill patients.15 Procedures performed by physiotherapists have been shown to reduce the length of mechanical ventilation, the length of hospitalization, the incidence of respiratory infections, and consequently, mortality.15 Hence, it is reasonable to consider that physiotherapists should be part of a multidisciplinary ICU team, caring not only for early mobilization,2,16 but also for intubated patients’ respiratory procedures.10 There have been attempts to define the role of physiotherapists in many countries,4 and provide minimum standards of clinical practice needed for physiotherapists in the ICU;17–21 however, there is still variation in ICU practices and approaches worldwide.22
In Albania, rehabilitation and physiotherapy are relatively new fields. According to the “Order of Nursing”, which is responsible for issuing the professional license to the physiotherapists, overall, 1400 physiotherapists are licensed (legitimate to work) in Albania (personal communication) for the whole population (2.862.427 inhabitants according to www.instat.gov.al). Until 2006, Physiotherapy training in Albania consisted only of 6-month courses. In 2010, a new curriculum in Physiotherapy (3 years Bachelor’s degree) was implemented by the Ministry of Education. Further education in physiotherapy includes programs: “Master of Science” and “Professional Master”. Only in the “Master of Sciences” program, students have 18 lectures about Intensive Care and rehabilitation in ICU. Physiotherapy students do not do supervised clinical practices in the ICU during their higher education.
There is currently no detailed description of the role of physiotherapists in Albanian ICUs, and ascertaining information about the current practice will help develop the role of physiotherapists in ICUs in Albania.
To address this knowledge gap, we attempt to provide an overview of the current physiotherapy practice in ICUs of two Albanian university hospitals and explore the involvement of physiotherapists and intensive care nurses regarding respiratory care and early mobility in the ICU.
Materials and Methods
Study Design and Setting
This study was an observational cross-sectional study at the University Hospital Center “Mother Theresa” and the University Hospital of Trauma, both in the capital Tirana.
University Hospital Center of Tirana “Mother Theresa” (UHCT) and University Hospital of Trauma (UHT) are the two largest university tertiary hospitals in Albania. In these hospitals, patients take the most specialized health assistance. UHCT has 1450 beds, and ICU units for adult patients are organized according to the services: medical/surgical, cardiac care, cardiac surgery, neurologic care, neurosurgery, burn and infective diseases ICU, while in UHT there is an ICU for trauma patients with 16 beds. In the UHCT, there is a physiotherapy unit with 22 physiotherapists, and in the UHT, a unit with 16 physiotherapists. Overall, only 38 physiotherapists work in these two university hospitals for all clinical settings within the hospitals.
Public health services in Albania consist of primary health-care centres, secondary hospitals (organized according to the 11 regions and 23 districts), and tertiary hospitals, which include three university hospitals for medical, surgical, and trauma treatment (UHCT, UHT and University Hospital “Shefqet Ndroqi” for the pulmonary diseases’ treatment), and two other obstetric-gynecologic university hospitals. Regarding secondary hospitals, only regional hospitals have Intensive Care Units, and the number of physiotherapists working in regional hospitals varies from one to four. There are also private hospitals in Albania, mainly in large cities.
Data Collection
A self-administered instrument with 74 questions was used to extract information in a sample of 189 critical care nurses and physiotherapists. The questionnaire was conceptualized and designed to have broad coverage of physiotherapy aspects in critically ill patients.
For the items’ generation, authors conducted literature research based on preformulated keywords:13 rehabilitation, physiotherapy, respiratory care, early mobilization, ICU acquired weakness, Intensive Care Unit, nursing, physiotherapist, standards, recommendation, guideline. The questionnaire was developed by authors in collaboration with a group of experts (two senior intensivists with academic and research backgrounds, one nurse with more than ten years of experience in the ICU, one medical doctor specialized in physiotherapy, and one physiotherapist with more than five years of clinical experience). The questionnaire was revised and validated by another panel of three experts with academic and clinical experience: an intensivist, a critical care nurse, and a physiotherapist. After that, the final version of the questionnaire was approved, aiming at having an overview of physiotherapy practice in the ICUs of two university hospitals, which offer care for medical, surgical, and trauma patients (Supplementary Material). This study was approved by the Faculty of Medical Technical Sciences, University of Medicine in Tirana. According to our institution’s politics, as the study did not collect information about patients, there was not required approval from the “Ethical Commission”. Written informed consent in providing information in the questionnaires was obtained from each participant before the questionnaire’s fulfillment.
Survey Questionnaire
The questionnaire consisted of three parts. The first and second part of the questionnaire consisted of short-form questions closed and open-ended regarding the availability of physiotherapists in the ICU and the use of guidelines and respondents’ knowledge about them.
Availability of Physiotherapists in the ICU
The first part of the questionnaire for the physiotherapists included data about the type of physiotherapist’s employment (part-time or permanent) in the ICU, shifts, and frequency of treating ICU patients. There were questions about hours that they worked in the ICU during morning shifts and after-hours physiotherapy service during weekdays or the weekend and public holidays. Physiotherapists were asked if ICU patients were referred for physiotherapy by physicians or were physiotherapists to screen the patients and determine the interventions’ plan. The questionnaire also contained three questions about participants’ education, post-graduate education/training in intensive care or respiratory care, and their working experience.
Guidelines, Application and Knowledge About Them
The second part of the questionnaire was the same for all and asked for information about the application by ICUs of guidelines for physiotherapist consultation, early mobilization, the prevention of ventilator-associated pneumonia,3 or the use of protocols for ventilator weaning and respiratory care in critically ill patients.23 Respondents were asked how they self-evaluated their knowledge of international guidelines for early mobilization, guidelines for preventing ventilator-associated pneumonia, and ventilator weaning protocols. There were questions about the respondents’ self-evaluation of their knowledge on evaluation methods of functional ability or mobility status and ICU patients’ respiratory care.
Responses about knowledge on clinical guidelines or protocols involved “yes” or “no”, while those asking information about the level of knowledge were presented as a Likert scale, no = no knowledge at all, poor = minimal knowledge, and very good = maximal knowledge on the topic. Information about the frequency of performing different interventions applied: “never performed” (0% of patients), “occasionally performed” (<50% of patients) or “regularly performed” (>75% of patients).
ICU Practice on Early Mobilization and Respiratory Care
The third part of the questionnaire consisted of 48 short-form questions, which examined the frequency of nurses’ and physiotherapists’ involvement in early mobilization, respiratory care in intubated and non-intubated patients.
Concerning early mobilization, mobilization methods were divided according to the patient’s cooperation in passive mobilization, assisted active mobilization, and active mobilization.8,11,13,24
Although evidence about electrical muscle stimulation is contradictory, not yet established,25 and consequently not recommended in the ICU,8 the authors of the questionnaire included them to have robust evidence of modalities performed on critically ill patients.13
Respondents were asked about respiratory therapy in patients with an artificial airway: airway suctioning, manual techniques to facilitate secretion removal, manual hyperinflation, and ventilator hyperinflation.24 There were questions about their participation in mechanical ventilation adjustment, the weaning from the ventilator, and extubating.4
Questions about body positioning referred to positioning for respiratory interventions, such as head-down tilt or side-lying for postural drainage or lung re-expansion.24
Questions about respiratory therapy in non-intubated patients explored procedures such as breathing exercises, coughing/huffing, incentive spirometry, and other methods that facilitate removal of airway secretions. Respondents were also asked for their participation in noninvasive ventilation or the use of nebulizers in their patients.
Participants
All critical care nurses (151 nurses) working in 5 Intensive Care Units at University Hospital Center of Tirana (neurologic care, neurosurgery, cardiac surgery, cardiac care, and medical-surgical ICU) and in the trauma ICU at University Hospital of Trauma were contacted (all of these units have a capacity of 90 beds). At the same time, all physiotherapists working at the University Hospital Center of Tirana and University Hospital of Trauma (38 physiotherapists) were contacted by the authors, and together with ICU nurses, were invited to participate in the survey. One hundred eighty-nine hard copies of the questionnaire and consent forms were distributed to each participant through the six nurses in charge of each of the ICUs and the two supervisors of physiotherapists. All questionnaires were anonymous, the respondents were not required to complete any personal data such as sex or age, and data were kept confidential at all times.
Data Analysis
Data were given in frequency and percentages of respondents’ performing different procedures of respiratory care or early mobilization, dividing them into nursing staff and physiotherapists. Chi-square tests were used to evaluate comparisons of values and identifying p-value. Statistical significance was defined as a p-value less than 0.05.
All statistical analyses were performed with IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA). Results were reported in accordance with STROBE guidelines.
Results
Demographics
Out of 189 distributed questionnaires, 131 were completed (69.3%), ie, 101 and 30 completed by nurses (66.8% of full-time ICU nursing staff) and physiotherapists (78.9% of all full-time hospital working physiotherapists) respectively. Table 1 gives data about the number of beds and nursing staff of ICUs included in the study.
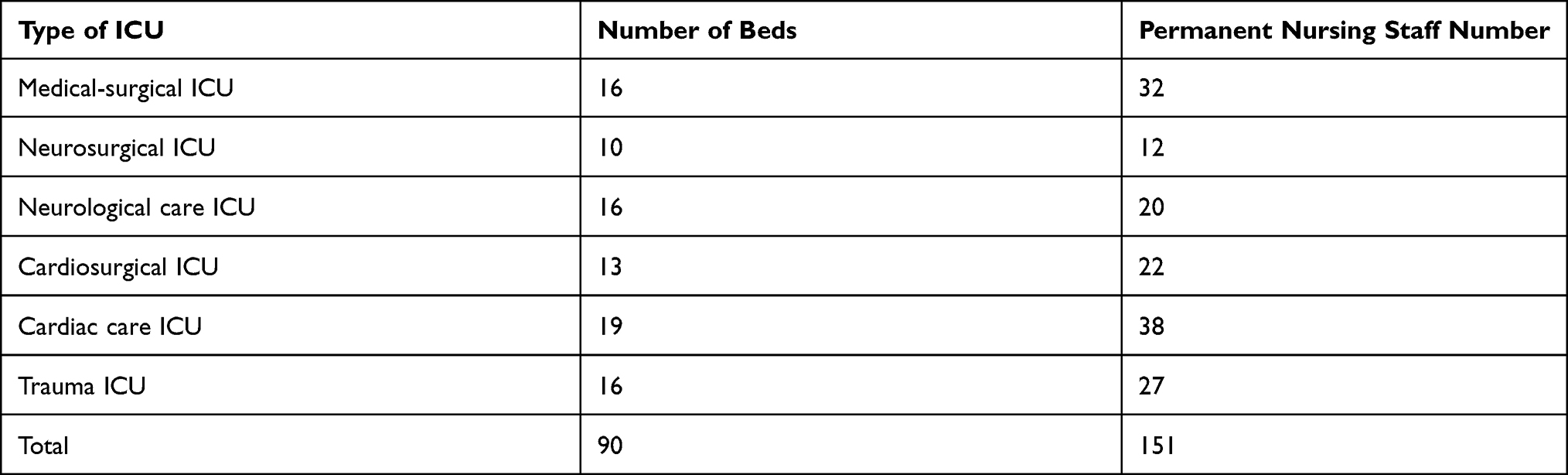 |
Table 1 Data About the Number of Beds and Nursing Staff of ICUs |
None of the physiotherapists was exclusively a part of an ICU team or worked in such a team full-time (Table 2). However, they performed physiotherapy not in all ICU admitted patients, and during the morning shifts, on a rotational basis.
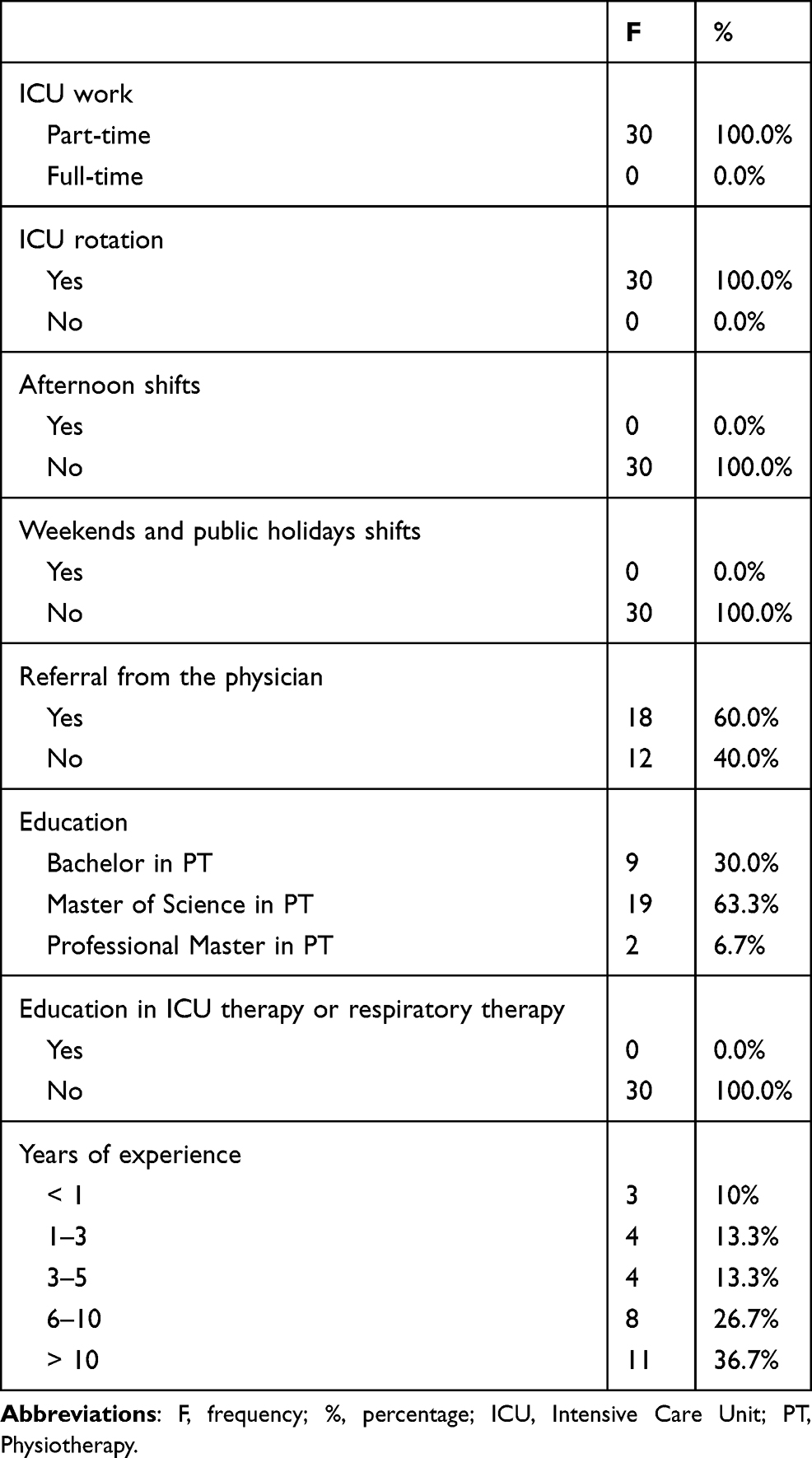 |
Table 2 Frequencies of the Physiotherapists’ Characteristics |
Twelve physiotherapists (40%) regularly performed screening of the patients and evaluated their suitability/eligibility for physiotherapy (trauma ICU, neurologic care ICU, and neurosurgical ICU). In other ICUs (ie, medical/surgical, cardiac care, and cardiac surgery), they practiced a referral system, where the intensivists determined suitability for physiotherapy for a limited number of patients. In these wards, 18 physiotherapists (60%) worked only for 4–5 hours/weekday.
Physiotherapists did not offer after-hour coverage during weekdays, as well as during weekends and public holidays.
Regarding education: 30% of physiotherapists had a Bachelor’s degree in Physiotherapy, and 70% had Master’s degrees in Physiotherapy.
All respondents confirmed that ICUs did not have their guidelines or protocols for physiotherapist consultation or early mobilization and respiratory therapy in critically ill patients. However, all nursing staff confirmed that ICUs did use protocols to prevent ventilator-associated pneumonia and wean from mechanical ventilation.
All physiotherapists reported good knowledge of international guidelines for early mobilization and respiratory therapy, good knowledge of evaluation methods of functional ability or mobility status, but 90% of them reported no knowledge of the guidelines for preventing ventilator-associated pneumonia and protocols of ventilator weaning.
All 131 respondents did not have further education in ICU therapy or respiratory therapy, and they confirmed the necessity of training in ICU patients’ care-related topics.
Respiratory Care in Patients with an Artificial Airway
The ICU practice regarding respiratory care in patients with an artificial airway, based on respondents’ answers, is presented in Table 3.
 |
Table 3 The Practice of the ICU Regarding Respiratory Care in Patients with an Artificial Airway, Based on Answers Given by Respondents |
Physiotherapists neither participated in the adjustment of mechanical ventilation nor in spontaneous breathing trials, or airway suctioning from endotracheal/tracheostomy tube; procedures performed regularly (respectively 82.2%, 25.7%, and 100%) or occasionally by nursing staff (respectively for the first two techniques 17.8% and 35.6%). None of the nursing staff performed inspiratory muscle training in patients with an artificial airway, while 60% of physiotherapists occasionally performed it.
Forty percent (n=12) of physiotherapists occasionally performed postural drainage positions in bed for secretions clearance, and 60.0% (n=18) occasionally performed chest percussion or vibration.
Respiratory Care in Patients without an Artificial Airway
The ICU practice regarding respiratory care in patients without an artificial airway, based on respondents’ answers, is presented in Table 4.
 |
Table 4 The Practice of the ICU Regarding Respiratory Care in Patients without an Artificial Airway, Based on Answers Given by Respondents |
All physiotherapists occasionally performed: body positioning of the patients in bed, chest-wall percussion, or manual/mechanical vibration; all of them occasionally assisted patients on deep breathing exercises, respiratory muscle training exercises, and coughing/huffing. Incentive spirometry was occasionally performed by 50% of physiotherapists.
Physiotherapists did not administer bronchodilators or nebulizers for humidification, which were occasionally carried out by 35.6% of nursing staff.
However, the nursing staff did not perform inspiratory muscle training in critically ill patients without an artificial airway.
Early Mobilization
The ICU practice regarding early mobilization, based on respondents’ answers, is presented in Table 5.
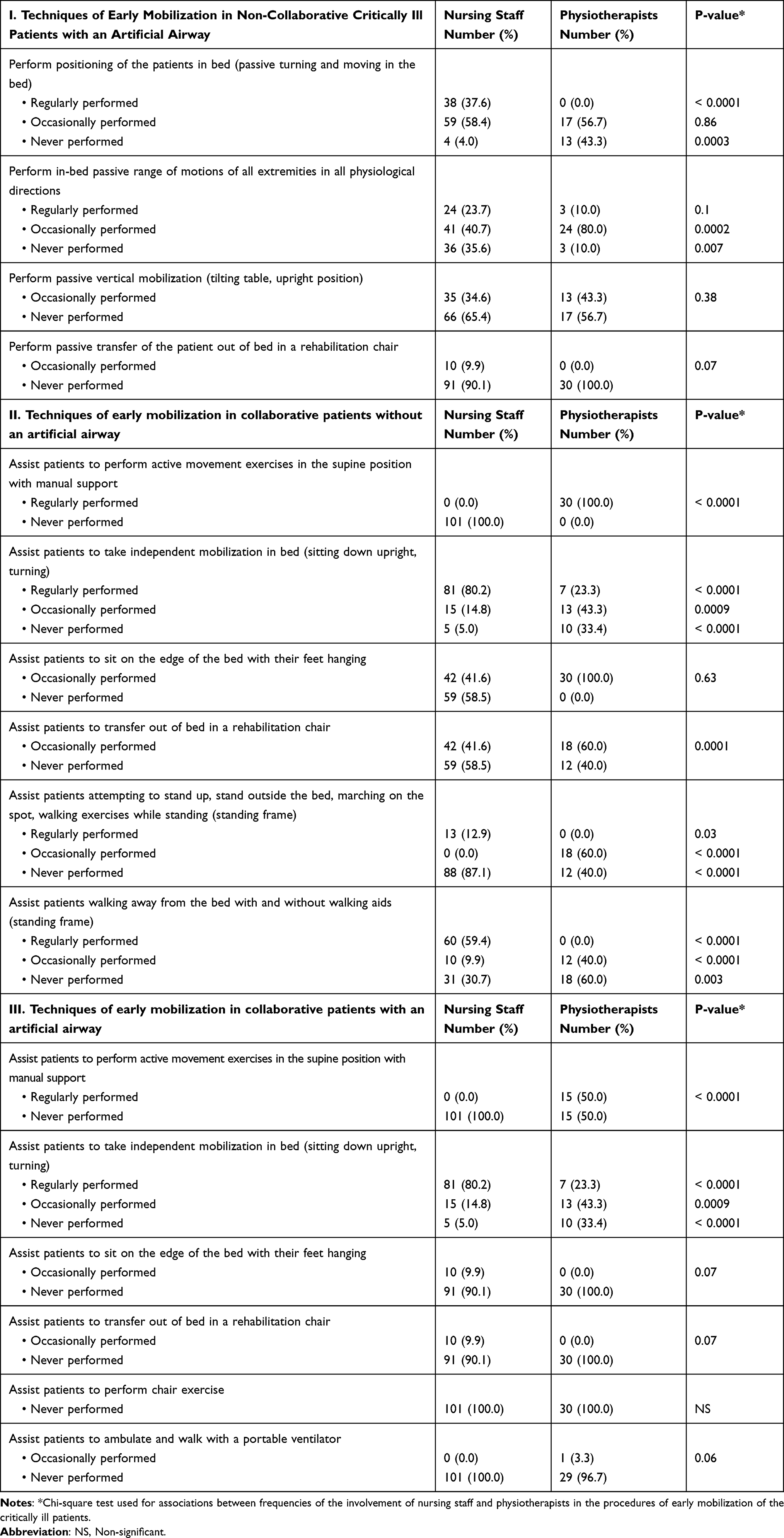 |
Table 5 The Practice of the ICU Regarding Early Mobilization, Based on Answers Given by Respondents |
Regarding early mobilization techniques for collaborative patients not mechanically ventilated, all physiotherapists regularly performed active movement exercises in the supine position with manual support. Assisting not mechanically ventilated patients to take independent mobilization in bed was regularly performed by 23.3% of physiotherapists and occasionally performed by 43.3% of them.
All physiotherapists occasionally assisted the patients not mechanically ventilated to sit on the edge of the bed with their feet hanging, while 60% of them occasionally assisted these patients to transfer out of bed in a rehabilitation chair.
All physiotherapists confirmed that they did not perform the passive transfer of the mechanically ventilated patient out of bed in a rehabilitation chair. The procedure was occasionally made by 9.9% of nursing staff in collaborative and non-collaborative mechanically ventilated patients.
There was no use of assisted/active cycling using a bed pedal exerciser for collaborative patients with an artificial airway, while only 46.7% of physiotherapists helped it in cooperative patients not mechanically ventilated. The nursing staff was not involved in assisting critically ill patients regarding assisted/active cycling using bed pedal exercise.
Respondents did not assist the patients in performing chair exercise or ambulating and walking with a portable ventilator; only one physiotherapist responded that they occasionally helped the patient ambulate and walk with a portable ventilator.
Only nine physiotherapists occasionally had administered electrical muscular stimulation in non-collaborative patients with an artificial airway.
Discussion
Physiotherapy procedures were performed irregularly in ICUs in Tirana, Albania. Physiotherapists were not actively involved or exclusively employed in the ICU, and early mobility and respiratory care procedures were performed by nursing staff and on-call/on-request physiotherapists. Physiotherapists conducted respiratory exercises and limb exercises at the patients without an artificial airway, while they were not involved in all procedures of the respiratory care and early mobility of mechanically ventilated patients. Nursing staff performed airway suctioning in mechanically ventilated patients and participated in adjusting ventilator settings, while physiotherapists did not participate in any of these procedures.
A recent review highlighted the importance of performing ventilator adjustments to facilitate mobility, improving performance and duration;26 however, there are no guidelines on the adjustments of ventilator assistance during early mobilization. One of the challenges of the mobilization teams, especially the physiotherapists, is to adjust the exercise dose and respiratory support during mobilization to avoid overload of respiratory muscle and improve exercise performance.26
The recent study results were similar to European survey results, although made two decades ago, revealing that physiotherapy in critical care was often inadequate.27 There exists essential heterogeneity among different countries concerning early mobilization practice,22 and respiratory care in ICU patients.10 Our survey confirmed previous findings that mobilization in ventilated patients remains low.24,28,29 Considering the low rate of nursing staff and physiotherapists’ involvement in assisting mechanically ventilated patients to sit on the edge of the bed, transfer out of bed, or ambulate, they imply that out-of-bed mobility of mechanically ventilated patients was sporadically performed in the ICUs under study.
Several studies have tried to identify barriers to physiotherapy implementation and its application in critical care.30–32 A recent survey revealed among barriers, those related to the physiotherapists and legal procedures, ie, lack of direct physiotherapy access by ICU specialists or non-recognition of professional autonomy.30 From the survey results, we can assume that the low rate of the involvement of physiotherapists in procedures such as respiratory care, suction, and adjusting mechanical ventilation settings maybe because they are not exclusively employed in the ICU and legal procedures related.30
Insufficient staffing was considered a barrier to providing physiotherapy,4 and early rehabilitation to critically ill patients;31,32 an inadequate number of physiotherapists in the ICUs under study (one physiotherapist per unit, with ten or more beds) may be one of the reasons why mobilization was not feasible in the patients with mechanical ventilation,6 although the survey did not explore barriers.
Our study demonstrated no exclusive physiotherapists in the ICU. Physiotherapists performed physiotherapy, not in all patients, and were not involved in all early mobilization procedures or respiratory care procedures. Working occasionally and not permanently in ICU may affect the physiotherapists’ practice in Albanian ICUs. A recent study demonstrated that respiratory therapy and musculoskeletal care performed by physiotherapists working permanently in ICU were more frequent than those performed by physiotherapists occasionally working in this setting.14
Our study aimed to give an overview of the physiotherapists and nursing staff’s involvement in early mobility and respiratory care procedures, as previous studies have illustrated that providers of these procedures were objects of variations between countries.6,10 Our survey revealed that airway suctioning had been practiced by nurses, while it has been demonstrated that doctors, nurses, or physiotherapists can practice it.10 Respiratory procedures in intubated patients were considered as part of routine nursing care,33 and were performed by them.34 As illustrated in other studies,34,35 the nursing staff in Albanian university hospital ICUs were involved in respiratory procedures of ventilated patients and in mechanical ventilation adjustment.
Although European physiotherapists had reported that it was their responsibility to provide respiratory therapy in ICUs,4 and physiotherapists provide it in different countries,4,9,14,25,36 in Albanian practice, physiotherapists were not involved in the respiratory therapy of patients with an artificial airway.
Physiotherapists, being routinely involved in ICU patient care,37,38 should be part of ICU staff involved at early mobilization,8,31 however, it has been reported that mobility modalities have been performed by physiotherapists, occupational therapists, and bedside nurses.6 Studies have shown that nursing staff provides mobility events such as out-of-bed mobility or passive movements in and out of bed,6 facts confirmed by our survey, which showed that nurses provided passive movements in bed for patients with artificial airway, and out-of-bed mobility for patients not mechanically ventilated.
Contrary to the best practice, that recommends early mobilization based on protocols,8,9,31 and respecting consensus recommendations on safety criteria before the mobilization,11 these protocols and recommendations were not implemented in the ICUs under survey.
While internationally, physiotherapists perform the individualized assessment and the active treatment of critically ill patients25 as part of the multidisciplinary team,39 60% of physiotherapists in two Albanian hospitals were involved in critically ill patients’ treatment after medical referral of patients.40,41 Respondents of the questionnaire confirmed that the ICUs did not use protocols for physiotherapist consultation. This can be one reason for various physiotherapists’ approaches to the patients in different ICU settings under the study. Twelve physiotherapists responded that they regularly performed screening of the patients and evaluated their suitability/eligibility for physiotherapy in the trauma ICU, neurologic care ICU, and neurosurgical ICU. In these settings, physiotherapists have direct access to the patients. The main reason why they work without a physician referral to physiotherapy can be because, during their shift, they work only in the critical care unit and not in other wards of the hospital. Contrary to this approach, in other ICU settings (ie, medical/surgical, cardiac care, and cardiac surgery), physiotherapists, during their shift, also treated other patients across different clinical settings within the hospital.
The Albanian ICU’s staff should increase awareness for implementing established guidelines for physiotherapist consultation,32,40 and other physiotherapy guidelines,7–13 which were not used in the ICUs under investigation.
Considering all the survey findings, we can state that providing physiotherapy in Albanian ICUs is challenging, and effort should focus on many directions,42 involving many actors.
Firstly, we advocate that organizational changes are needed to strengthen physiotherapists’ involvement routinely in critical patients’ care.9,31 It is typical for physiotherapists working in Albanian hospitals to manage patients across different clinical settings within the hospital. Hence, healthcare policy-makers in Albania should raise awareness about the importance of increasing physiotherapists’ staff according to the ICU needs,9,43 resulting in cost-saving and improving patient outcomes.44,45
Secondly, increasing physiotherapists’ staff alone may not be sufficient to enhance physiotherapy provided in our clinical practice.6 Simultaneously, the culture of ICU patients’ treatment should be changed,40 and the priority of the interventions should be revised, considering early mobility a priority.16 Implementation of a multidisciplinary rehabilitation approach, especially in mechanically ventilated critically ill patients,9,31 has to become an essential part of the work culture change in Albanian ICU wards.
Thirdly, in clinical practice, physiotherapy practice can be standardized through established protocols,31 and implementation of national protocols could be a contributor.
All physiotherapists reported good knowledge of evaluation methods of functional ability or mobility status; however, the recent study did not explore the use of physical functioning measurement instruments.46 The evaluation is essential in planning respiratory therapy and early mobilization; therefore, physiotherapists should focus on incorporating measurement instruments into clinical practice.46
The use of reliable instruments for early physical functional assessment is essential in identifying patients who may require rehabilitation interventions and evaluating interventions’ efficiency.46–48
Lastly, there is a growing need for enhancing physiotherapy in ICU, and consequently, it may require further education.25 The training level needed for physiotherapists to work in ICU varies among countries, from no specific additional training as in some countries,25 including Albania, to specialized for particular procedures like bronchoscopy, performed by physiotherapists in the United Kingdom.49 Our survey revealed that although 70% of physiotherapists had Master degrees in Physiotherapy, they did not have further education in ICU therapy or respiratory therapy; however, all respondents confirmed the necessity of training in ICU patients’ care-related topics. Designed frameworks about the minimum standards of clinical practice needed for physiotherapists in the ICU can be utilized to improve the university curriculum for the physiotherapists’ education and also the training for ICU staff in Albanian practice.19 The implementation of quality improvement projects in Albania can change routine clinical practice,31,50 and establish new Critical Care Physical Therapy and Rehabilitation Program.40
Strengths, Limitations, and Future Outlooks
This work has some strengths and limitations. To the best of our knowledge, this study is the first study reporting the physiotherapy practice in the Albanian ICUs. This study provided an overview of the physiotherapy practice in ICUs under investigation, demonstrating the need for changes and improvements. However, it was confined to two centers, and a national survey involving all university, regional and private hospitals would provide an insight into the Albanian ICU physiotherapy practice.
Furthermore, the survey questionnaire used in this study only considered procedures conducted by nursing staff or physiotherapists regarding respiratory care and early mobilization, without exploring the drivers and possible factors that may explain why some of these techniques were administered occasionally or not performed at all. The study did not consider self-perceived barriers for early mobilization or respiratory therapy, and future research should focus on elucidating the drivers and barriers to adequate physiotherapy.
The questionnaire was focused only on the physiotherapists’ knowledge about evaluation methods of functional ability or mobility status; it did not explore the use of measuring instruments, such as CAM-ICU, MRC-SS, IMS, FSS-ICU, CPAx, inspiratory muscle pressure, and others.46,48 An upcoming survey in Albania should consider asking about the use and rationale for measuring instruments to plan early ICU mobility.
The recent study provided some baseline data that may be helpful to justify the development of dedicated evidence-based critical care physiotherapy service in this setting. However, this study warrants further investigation in the field of physiotherapy in Albanian ICUs aiming to implement a dedicated physiotherapy service and integrate new practices.
Conclusion
Physiotherapy practice in Albanian ICUs is not performed according to the established international guidelines and best practice evidence. Physiotherapists are not actively involved or exclusively employed in the ICU. Procedures of early mobility and respiratory therapy in the ICU are provided on a non-regular basis or not performed at all, mainly in mechanically ventilated patients. Contrary to the current practice with limited physiotherapy involvement in ICUs, physiotherapists should be an active part of the multidisciplinary intensive care team. Efforts addressing the multidisciplinary approach should focus on improving the physiotherapy practice, making organizational and cultural changes in the ICU, and establishing protocols and guidelines.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Burtin C, Clerckx B, Robbeets C, et al. Early exercise in critically ill patients enhances short-term functional recovery. Crit Care Med. 2009;37(9):2499–2505. doi:10.1097/CCM.0b013e3181a38937
2. Hodgson CL, Tipping CJ. Physiotherapy management of intensive care unit-acquired weakness. J Physiother. 2017;63(1):4–10. doi:10.1016/j.jphys.2016.10.011
3. Ntoumenopoulos G, Presneill JJ, McElholum M, Cade JF. Chest physiotherapy for the prevention of ventilator-associated pneumonia. Intensive Care Med. 2002;28(7):850–856. doi:10.1007/s00134-002-1342-2
4. Norrenberg M, Vincent JL. A profile of European intensive care unit physiotherapists. European Society of Intensive Care Medicine. Intensive Care Med. 2000;26(7):988–994. doi:10.1007/s001340051292
5. Denehy L, Lanphere J, Needham DM. Ten reasons why ICU patients should be mobilized early. Intensive Care Med. 2017;43(1):86–90. doi:10.1007/s00134-016-4513-2
6. Jolley SE, Moss M, Needham DM, et al. Point prevalence study of mobilization practices for acute respiratory failure patients in the United States. Crit Care Med. 2017;45(2):205–215. doi:10.1097/CCM.0000000000002058
7. Nydahl P, Sricharoenchai T, Chandra S, et al. Safety of patient mobilization and rehabilitation in the intensive care unit. Systematic review with meta-analysis. Ann Am Thorac Soc. 2017;14(5):766–777. doi:10.1513/AnnalsATS.201611-843SR
8. Bein T, Bischoff M, Brückner U, et al. S2e guideline: positioning and early mobilisation in prophylaxis or therapy of pulmonary disorders: revision 2015: S2e guideline of the German Society of Anaesthesiology and Intensive Care Medicine (DGAI). Anaesthesist. 2015;64(Suppl 1):1–26.
9. Core Standards for Intensive Care Units. Edition 1 2013; 2013. Available from: https://www.ics.ac.uk/ICS/GuidelinesStandards/ICS.
10. Gosselink R, Bott J, Johnson M, et al. Physiotherapy for adult patients with critical illness: recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on physiotherapy for critically ill patients. Intensive Care Med. 2008;34(7):1188–1199. doi:10.1007/s00134-008-1026-7
11. Hodgson CL, Stiller K, Needham DM, et al. Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Crit Care. 2014;18(6):658. doi:10.1186/s13054-014-0658-y
12. National Institute for Health and Clinical Excellence. Rehabilitation after critical illness. (Clinical guideline 83); 2009. Available from: www.nice.org.uk/CG83.
13. Sommers J, Engelbert RH, Dettling-Ihnenfeldt D, et al. Physiotherapy in the intensive care unit: an evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin Rehabil. 2015;29(11):1051–1063. doi:10.1177/0269215514567156
14. Christakou A, Seitaridi A, Koutsioumba E, et al. Current physiotherapy practice in Greek intensive care units: a national study. Eur J Physiother. 2019;21:210–216. doi:10.1080/21679169.2018.1523459
15. Castro AA, Calil SR, Freitas SA, Oliveira AB, Porto EF. Chest physiotherapy effectiveness to reduce hospitalization and mechanical ventilation length of stay, pulmonary infection rate and mortality in ICU patients. Respir Med. 2013;107(1):68–74. doi:10.1016/j.rmed.2012.09.016
16. Dubb R, Nydahl P, Hermes C, et al. Barriers and strategies for early mobilization of patients in intensive care units. Ann Am Thorac Soc. 2016;13(5):724–730. doi:10.1513/AnnalsATS.201509-586CME
17. Hanekom S, Van Aswegen H, Plani N, Patman S. Developing minimum clinical standards for physiotherapy in South African intensive care units: the nominal group technique in action. J Eval Clin Pract. 2015;21(1):118–127. doi:10.1111/jep.12257
18. Plani N, van Aswegen H, Patman S, Hanekom S. Developing minimum clinical standards for physiotherapy in South African intensive care units: a mixed method approach. Eur J Physiother. 2017;19(sup1):31–33. doi:10.1080/21679169.2017.1381319
19. Skinner EH, Thomas P, Reeve JC, Patman S. Minimum standards of clinical practice for physiotherapists working in critical care settings in Australia and New Zealand: a modified Delphi technique. Physiother Theory Pract. 2016;32(6):468–482. doi:10.3109/09593985.2016.1145311
20. Twose P, Jones U, Cornell G. Minimum standards of clinical practice for physiotherapists working in critical care settings in the United Kingdom: a modified Delphi technique. J Intensive Care Soc. 2019;20(2):118–131. doi:10.1177/1751143718807019
21. van Aswegen H, Patman S, Plani N, Hanekom S. Developing minimum clinical standards for physiotherapy in South African ICUs: a qualitative study. J Eval Clin Pract. 2017;23(6):1258–1265. doi:10.1111/jep.12774
22. Bakhru RN, McWilliams DJ, Wiebe DJ, Spuhler VJ, Schweickert WD. Intensive care unit structure variation and implications for early mobilization practices. An international survey. Ann Am Thorac Soc. 2016;13(9):1527–1537. doi:10.1513/AnnalsATS.201601-078OC
23. MacIntyre NR, Cook DJ, Ely EW, et al. Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001;120(6 Suppl):375S–95S. doi:10.1378/chest.120.6_suppl.375S
24. McWilliams DJ, Duffy L, Snelson C. Current rehabilitation practices for patients admitted to critical care in the UK: a 5day point prevalence survey of 12 adult general intensive care units. J Assoc Chartered Physiotherap Respir Care. 2016;48:5–14.
25. Berney S, Haines K, Denehy L. Physiotherapy in critical care in Australia. Cardiopulm Phys Ther J. 2012;23(1):19–25. doi:10.1097/01823246-201223010-00004
26. González-Seguel F, Camus-Molina A, Jasmén A, Molina J, Pérez-Araos R, Graf J. Respiratory support adjustments and monitoring of mechanically ventilated patients performing early mobilization: a scoping review. Crit Care Explor. 2021;3(4):e0407. doi:10.1097/CCE.0000000000000407
27. Corrado A, Roussos C, Ambrosino N, et al. Respiratory intermediate care units: a European survey. Eur Respir J. 2002;20(5):1343–1350.
28. Berney SC, Harrold M, Webb SA, et al. Intensive care unit mobility practices in Australia and New Zealand: a point prevalence study. Crit Care Resusc. 2013;15(4):260–265.
29. Nydahl P, Ruhl AP, Bartoszek G, et al. Early mobilization of mechanically ventilated patients: a 1-day point-prevalence study in Germany. Crit Care Med. 2014;42(5):1178–1186. doi:10.1097/CCM.0000000000000149
30. Çakmak A, Ince Dİ, Sağlam M, et al. Physiotherapy and rehabilitation implementation in intensive care units: a survey study. Turk Thorac J. 2019;20(2):114–119. doi:10.5152/TurkThoracJ.2018.18107
31. Bakhru RN, Wiebe DJ, McWilliams DJ, Spuhler VJ, Schweikert WD. An environmental scan for early mobilization practices in United States intensive care units. Crit Care Med. 2015;43:2360–2369. doi:10.1097/CCM.0000000000001262
32. Malone D, Ridgeway K, Nordon-Craft A, Moss P, Schenkman M, Moss M. Physical therapist practice in the intensive care unit: results of a national survey. Phys Ther. 2015;95(10):1335–1344. doi:10.2522/ptj.20140417
33. Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Respiratory care modalities. Brunner, Suddarth’s, editors. Textbook of Medical-Surgical Nursing.
34. Bülbül Maraş G, Kocaçal Güler E, Eşer İ, Köse Ş. Knowledge and practice of intensive care nurses for endotracheal suctioning in a teaching hospital in western Turkey. Intensive Crit Care Nurs. 2017;39:45–54. doi:10.1016/j.iccn.2016.08.006
35. Depasse B, Pauwels D, Somers Y, et al. A profile of European ICU nursing. Intensive Care Med. 1998;24:939–945. doi:10.1007/s001340050693
36. Templeton M, Palazzo MG. Chest physiotherapy prolongs duration of ventilation in the critically ill ventilated for more than 48 hours. Intensive Care Med. 2007;33(11):1938–1945. doi:10.1007/s00134-007-0762-4
37. Ambrosino N, Janah N, Vagheggini G. Physiotherapy in critically ill patients. Rev Port Pneumol. 2011;17(6):283–288. doi:10.1016/j.rppneu.2011.06.004
38. Stiller K. Physiotherapy in intensive care: an updated systematic review. Chest. 2013;144(3):825–847. doi:10.1378/chest.12-2930
39. Wiles L, Stiller K. Passive limb movements for patients in an intensive care unit: a survey of physiotherapy practice in Australia. J Crit Care. 2010;25(3):501–508. doi:10.1016/j.jcrc.2009.07.003
40. Needham DM, Korupolu R, Zanni JM, et al. Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project. Arch Phys Med Rehabil. 2010;91(4):536–542. doi:10.1016/j.apmr.2010.01.002
41. Stiller K. Physiotherapy in intensive care: towards an evidence-based practice. Chest. 2000;118(6):1801–1813. doi:10.1378/chest.118.6.1801
42. Hodgson CL, Capell E, Tipping CJ. Early mobilization of patients in intensive care: organization, communication and safety factors that influence translation into clinical practice. Crit Care. 2018;22(1):77. doi:10.1186/s13054-018-1998-9
43. Valentin A, Ferdinande P; ESICM Working Group on Quality Improvement. Recommendations on basic requirements for intensive care units: structural and organizational aspects. Intensive Care Med. 2011;37(10):1575–1587. doi:10.1007/s00134-011-2300-7
44. Hanekom SD, Louw Q, Coetzee A. The way in which a physiotherapy service is structured can improve patient outcome from a surgical intensive care: a controlled clinical trial. Crit Care. 2012;16(6):R230. doi:10.1186/cc11894
45. Lord RK, Mayhew CR, Korupolu R, et al. ICU early physical rehabilitation programs: financial modeling of cost savings. Crit Care Med. 2013;41(3):717–724. doi:10.1097/CCM.0b013e3182711de2
46. González-Seguel F, Corner EJ, Merino-Osorio C. International classification of functioning, disability, and health domains of 60 physical functioning measurement instruments used during the adult intensive care unit stay: a scoping review. Phys Ther. 2019;99(5):627–640. doi:10.1093/ptj/pzy158
47. Parry SM, Huang M, Needham DM. Evaluating physical functioning in critical care: considerations for clinical practice and research. Crit Care. 2017;21:249. doi:10.1186/s13054-017-1827-6
48. Parry SM, Granger CL, Berney S, et al. Assessment of impairment and activity limitations in the critically ill: a systematic review of measurement instruments and their clinimetric properties. Intensive Care Med. 2015;41(5):744–762. doi:10.1007/s00134-015-3672-x
49. Barber PV, Martin J, O’Donnell PN. The development of the first nurse-led bronchoscopy post in the United Kingdom. Respir Med. 2004;98(6):504–508. doi:10.1016/j.rmed.2003.12.015
50. Eakin MN, Ugbah L, Arnautovic T, Parker AM, Needham DM. Implementing and sustaining an early rehabilitation program in a medical intensive care unit: a qualitative analysis. J Crit Care. 2015;30(4):698–704. doi:10.1016/j.jcrc.2015.03.019
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.