Back to Journals » OncoTargets and Therapy » Volume 13
Current Molecular Targeted Agents for Advanced Gastric Cancer
Received 18 January 2020
Accepted for publication 20 April 2020
Published 12 May 2020 Volume 2020:13 Pages 4075—4088
DOI https://doi.org/10.2147/OTT.S246412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nicola Silvestris
Shanshan Nie,1 Guoping Yang,1 Hongwei Lu2,3
1Center for Clinical Pharmacology, The Third Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China; 2Department of Cardiology, The Third Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China; 3Center for Experimental Medical Research, The Third Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Guoping Yang; Hongwei Lu
The Third Xiangya Hospital, Central South University, Yinpenling Street, Yuelu District, Changsha, Hunan 410013, People’s Republic of China
Tel/Fax +86-731-88618626
Email [email protected]; [email protected]
Abstract: Gastric cancer is the third leading cause of malignant tumor-related mortality worldwide. Traditional cytotoxic agents prolong the overall survival and progression-free survival of patients with advanced gastric cancer (AGC) compared to that with best supportive care. Due to the occurrence of serious adverse drug reactions that result in discontinued treatment, the survival benefit in AGC remains unsatisfactory. Systemic chemotherapy regimens have changed greatly, especially since the introduction of trastuzumab. Nevertheless, HER2 positivity is present in only approximately 20% of tumors. Due to the genetic heterogeneity and complexity of patients, there are many studies in progress that are exploring novel targeted drugs as an alternative to chemotherapy or adjuvant treatment in early-stage, progressive, and advanced gastric cancer. On the basis of the differences in gene expression profiles among patients, searching for specific and sensitive predictive biomarkers is important for identifying patients who will benefit from a specific targeted drug. With the development of targeted therapies and available chemotherapeutic drugs, there is no doubt that, over time, more patients will achieve better survival outcomes. Recently, immune checkpoint blockade has been well developed as a promising anticancer strategy. This review outlines the currently available information on clinically tested molecular targeted drugs and immune checkpoint inhibitors for AGC to provide support for decision-making in clinical practice.
Keywords: advanced gastric cancer, molecular targeted drugs, immune checkpoint blockade
Introduction
During the second half of the 20th century, there was a dramatic decline in gastric cancer (GC). However, GC still ranks as the third most common cause of malignant tumor mortality worldwide.1 In 2012 alone, one million people were diagnosed with GC, making it the fourth most common cancer.2 Although many factors, including genetic background, lifestyle (e.g., alcohol consumption, smoking habits, and diet), and Helicobacter pylori infection, have been demonstrated to be related to GC,3 the pathogenesis of GC is rather complicated and has not yet been well clarified. Due to its nonspecific symptoms, similar to dyspepsia, GC is usually misdiagnosed as gastritis and diagnosed late.4 The clinical outcome of GC depends on the tumor stage at diagnosis. Surgery, chemotherapy and radiation therapy are the most common treatments. Radical gastrectomy is the preferred approach for treating localized GC, but recurrence rates remain high. Patient prognosis is poor, with a five-year survival of less than 25% and a median overall survival (OS) of 7 to 10 months after diagnosis based on most large clinical studies.5,6 Traditional chemotherapeutic drugs, including 5-fluorouracil (5-FU), oral fluoropyrimidine, platinum agents, taxanes, irinotecan, and anthracyclines, aim to kill cancer cells.7 Unfortunately, they are nonspecific and have serious adverse reactions. In addition, chemoresistance is another major obstacle for effective cancer therapy. Fortunately, in recent decades, the development of molecularly targeted agents that inhibit specific oncogenic signal pathways has promoted the personalization of cancer therapeutic treatment and has greatly improved the outcomes of GC.8 Moreover, systemic chemotherapy regimens for advanced gastric cancer (AGC) have progressed sharply, especially since the introduction of trastuzumab. Trastuzumab was approved in the United States for HER2-overexpressing AGC as the first-line treatment drug.9 However, due to the genetic heterogeneity and complexity of tumors, HER2 overexpression only occurs in approximately 20% of all GCs.10 In this scenario, other novel molecular targeted agents and immune checkpoint inhibitors have shown effectiveness after clinical verification for many years. For instance, vascular endothelial growth factor receptor-2 (VEGFR-2) inhibitors have been introduced into clinical practice.11,12 Some newly developed targeted therapies and their molecular targets are summarized in Figure 1.
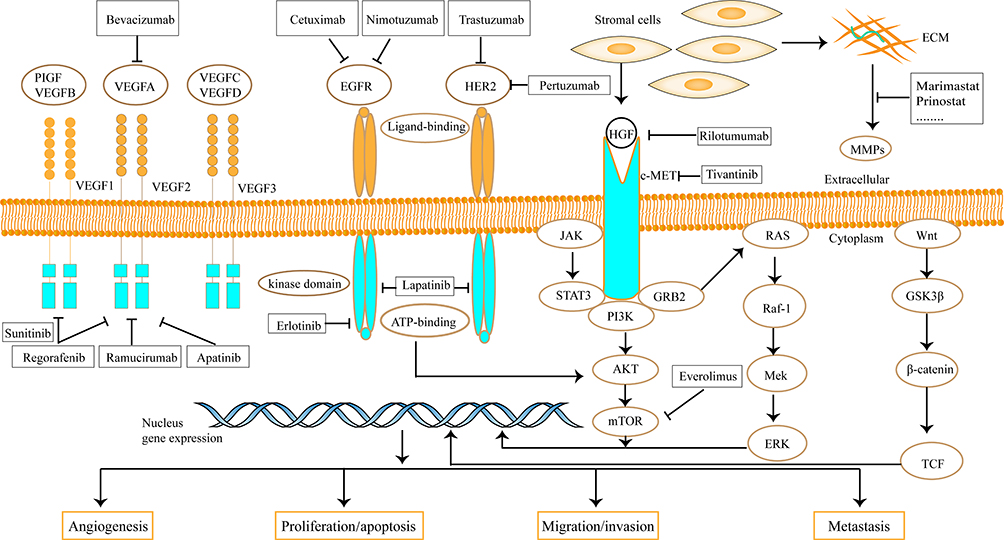 |
Figure 1 Molecular targeted agents and related action mechanism that are researched in AGC. |
This review outlines the currently available data on clinically molecular targeted agents and immune checkpoint inhibitors for AGC in order to provide strategies for decision-making in clinical practice.
Vascular Endothelial Growth Factor (VEGF) Inhibitors
Angiogenesis is necessary to promote the growth and metastasis of solid tumors. VEGF is considered an important driver of tumor angiogenesis.13 Thus, anti-VEGF inhibitors are attractive options that are making rapid progress. VEGF-A, -B, -C, -D, and placenta growth factor (PLGF) constitute the main structurally related ligands, among which VEGF-A is critical for the organization of the vasculature. Correspondingly, the related receptor tyrosine kinases (RTKs) include VEGFR-1, −2, −3, and neuropilins (NRPSs).14 The principal receptor that interacts with VEGF ligands with high affinity is VEGFR-2.15 Representative and approved VEGF inhibitors are discussed in detail below, and their relevant clinical trials are listed in Table 1.
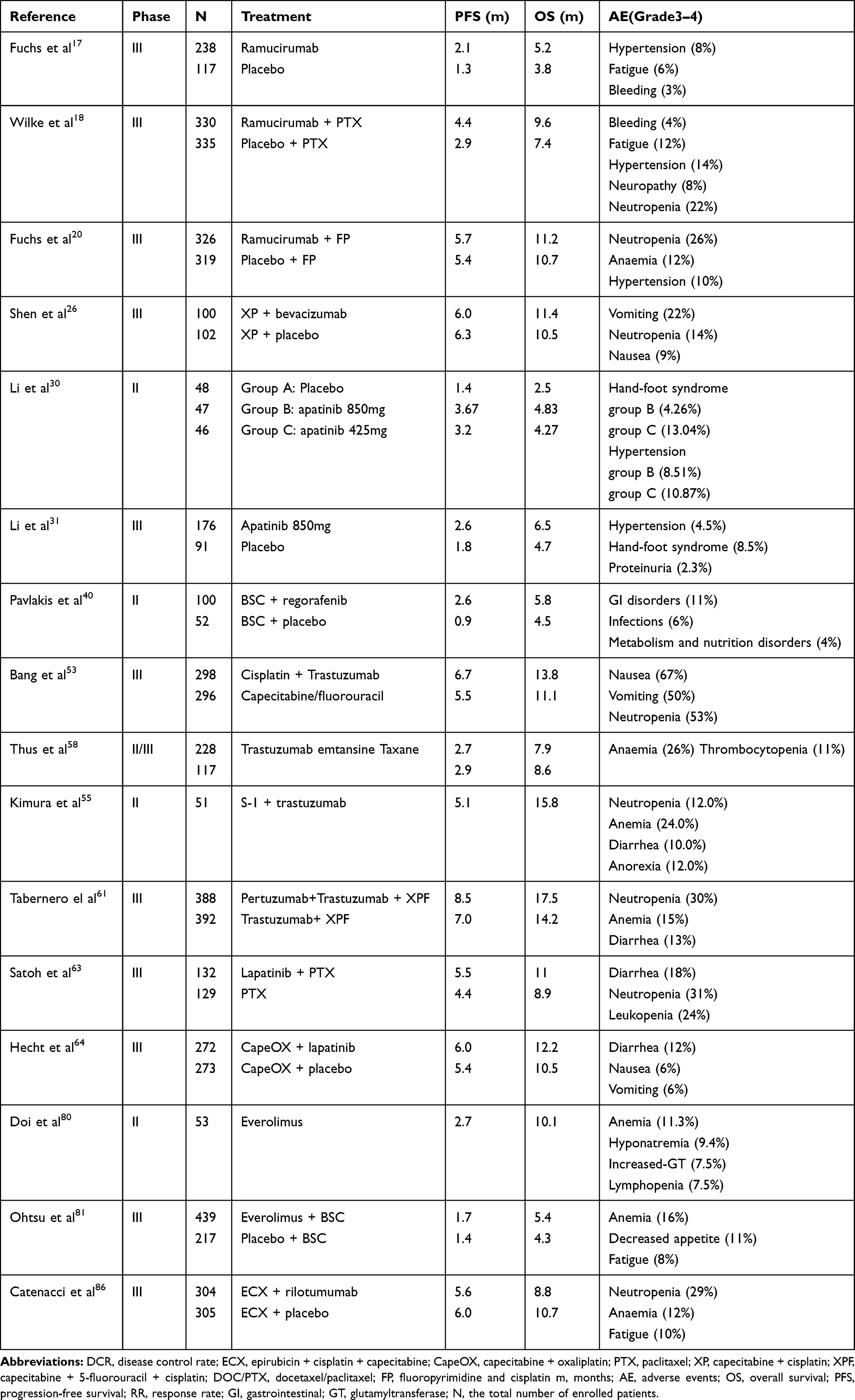 |
Table 1 Overview of Clinical Trials of Molecular Targeted Drugs in AGC |
Ramucirumab
Ramucirumab is a specific antibody against VEGFR-2 that blocks receptor binding to VEGF-A, -C and -D. Ramucirumab was initially approved in 2014 for patients with AGC/gastroesophageal junction (GEJ) adenocarcinoma.16 Ramucirumab has been proven to prolong OS and is considered a new therapy for AGC regardless of whether it is used as monotherapy or combined with paclitaxel.17,18 The REGARD trial reported that ramucirumab monotherapy offered a 1.4-month improvement in the median OS (HR = 0.776; 95% CI, 0.603–0.998).17 The RAINBOW trial also suggested that ramucirumab plus paclitaxel increased median OS in patients who previously received paclitaxel alone. Of the enrolled patients, 330 were assigned to the combined medicine group and 335 were assigned to the paclitaxel alone group. The primary endpoint was OS, and in the combined medicine group, OS was significantly superior to that in the patients in the paclitaxel alone group (9.6 vs 7.4 months), with an HR of 0.807 (95% CI, 0.678–0.962).18 Both of these trials validated VEGFR-2 as a promising therapeutic target, and subgroup analyses showed that age had no impact on the efficacy of ramucirumab in AGC.19 On the basis of these meaningful results, the RAINFALL trial was designed to assess the efficacy of ramucirumab as a first-line therapy combined with cisplatin and fluoropyrimidine in patients with HER2-negative metastatic G/GEJ adenocarcinoma. Unfortunately, the primary endpoint of PFS was only prolonged by 0.3 months in the experimental group and therefore was not clinically significant. The second endpoint, median OS, was not different between the groups. As a result, ramucirumab is not recommended as a first-line therapy when combined with cisplatin and fluoropyrimidine for HER2-negative patients.20 Ongoing trials combining ramucirumab with the FLOT regime or immune checkpoint inhibitors will provide additional benefit for specific intent to treat the population. The importance of looking for predictive biomarkers that reliably and consistently for anti-angiogenic therapies is being highlighted.
Bevacizumab
VEGF-A plays a critical role in the management of angiogenesis.21 Bevacizumab can suppress tumor growth as a specific monoclonal antibody targeting VEGF-A.22 A multicenter Phase II study suggested that bevacizumab combined with chemotherapy enhanced the primary endpoints median OS and PFS in G/GEJ adenocarcinoma.23 Another phase II trial also achieved a promising result with a median PFS of 6.6 months and median survival of 11.1 months.24 In terms of the compelling results, the large-scale AVAGAST trial also reported that bevacizumab prolonged PFS and significantly enhanced the overall response rate (ORR). Although the median OS was prolonged by 2 months, the primary objective in the trial was not reached. Subgroup analyses suggested a greater benefit in the European and Pan-American regions.25 In the meantime, AVATAR, a Phase III trial specifically designed for Chinese patients, failed to reach its preplanned goal. The median OS and PFS were similar in both arms.26 The different results between geographic regions may be attributed to the differences in prognostic factors and therapeutic schedules. In non-Asian regions, the efficacy of bevacizumab was strongly related to the levels of baseline plasma VEGF-A and tumor neuropilin-1.27 However, it should be noted that although these studies generated evidence that supports bevacizumab as an effective VEGF-A antagonist, they lack combined pharmacokinetic data and information on potential biomarkers.26
Apatinib
Apatinib is a new VEGFR-2 RTK inhibitor that blocks the intracellular ATP-binding site. Therefore, it has certain inhibitory effects on PDGFR-β, c-Kit, and c-Src.28,29 It displays antitumor efficacy in cell experiments and animal studies.29 On the basis of preclinical studies, the optimal protocol and manageable adverse profile of apatinib in metastatic GC was assessed in a phase II trial.30 The patients were assigned to group A (placebo, n = 48), group B (850 mg apatinib once a day, n = 47), or group C (425 mg apatinib twice a day, n = 46). Among these groups, patients in group B had longer median OS and PFS and fewer adverse events.30 Therefore, apatinib (850 mg once daily) was used in later phase III clinical trials. Compared to placebo, apatinib significantly improved OS and PFS.31 The CFDA (China Food and Drug Administration) has approved the drug to treat metastatic GC/GEJC after second-line chemotherapy.32 However, in the ANGEL trial (NCT03042611), a phase III study of apatinib monotherapy in AGC patients who have failed at least two prior lines of therapy, apatinib failed to significantly prolong the median OS. Subgroup analyses showed significant improvement of median OS and PFS in patients who endured three or more lines of therapy. In the meantime, inevitable treatment-related adverse events such as HFS and hypertension should not be ignored. As a third- or subsequent-line therapy, due to the convenient administration regimen and manageable safety profile, apatinib has been an emerging option for adult patients who progress or relapse after chemotherapy.
Other VEGF Inhibitors
Sunitinib can suppress tumor growth by inhibiting VEGF, PDGF, c-KIT, and FLT3 RTKs.33 Based on the superior efficacy achieved in preclinical studies, the antitumor activity of sunitinib monotherapy was evaluated in patients who previously received treatment. However, among the 78 recruited patients in the phase II trial, only 2 patients had partial responses, suggesting that sunitinib lacks sufficient clinical evidence for AGC.34 This conclusion was further confirmed by another independent phase II trial.35
Orantinib is an orally active RTK inhibitor with wide spectrum activity that has been verified in clinical trials for GC. Nevertheless, two phase II studies have found that orantinib has no synergistic effect with S-1 or oxaliplatin (SOX) in AGC.36,37
Regorafenib is a multikinase inhibitor that specifically targets angiogenic (VEGFR-1, VEGFR-2, and angiopoietin receptor Tie-2), stromal (PDGFR-β), and oncogenic (RAF, RET, and c-KIT) RTKs.38,39 In the INTEGRATE trial, regorafenib prolonged the PFS of 1.7 months in refractory AGC with an HR of 0.4 (95% CI, 0.28–0.59).40 Further study verified that regorafenib improved deterioration-free survival without an excessively negative effect on quality of life.41 Therefore, the effect of regorafenib plus chemotherapy was assessed again in refractory GC through an ongoing multinational phase III trial named INTEGRATE II.42
In addition, numerous anti-VEGF drugs are currently being explored in preclinical and clinical trials for AGC. Although aberrant angiogenesis is a key feature of solid tumors and the VEGF pathway is crucial in angiogenesis, the continuous progress in searching specific molecular biomarkers will be helpful for identifying priority patients who should benefit most from the addition of VEGF inhibitors.
Epidermal Growth Factor Receptor (EGFR) Antagonists
EGFR (ErbB-1/HER1), ErbB-2 (neu, HER2), ErbB-3 (HER3), and ErbB-4 (HER4) are the four definite receptors of the ErbB family, and they all have three common domains including a ligand-binding region, transmembrane domain and tyrosine kinase binding domain.43–45 Multiple studies have detected ErbB gene overexpression and mutations in colorectal cancer, GC, lung cancer, and ovarian cancer.46–49 Extensive preclinical studies and initial clinical trials have evaluated the practical value of inhibiting either EGFR or HER2 or both. The results suggested that targeting both EGFR and HER2 using two different antibodies has additive or even synergistic anti-GC effects.44 In GC, 44% of EGFR receptors are overexpressed, making them an exciting therapeutic target.50
Trastuzumab
Previous studies demonstrated that HER2 enhances proliferation and inhibits cell death.51,52 Treatment with trastuzumab, a HER2-targeted inhibitor, results in antibody-dependent cell-mediated cytotoxicity.53 The ToGA trial verified that trastuzumab plus chemotherapy was more efficacious in patients with HER2 overexpression (immunohistochemistry (IHC) 2+ and fluorescence in situ hybridization (FISH) positive or IHC 3+); compared to patients with low HER2 expression (IHC 0 or 1+ and FISH positive), these patients had a longer median OS of 2.7 months (HR = 0.74; 95% CI, 0.60–0.91). An exploratory, post hoc analysis supported that trastuzumab plus chemotherapy substantially increased OS (median overall survival 16·0 months) in patients with HER2 overexpression.53 The subsequent phase II study also obtained a meaningful result.54 As an adjunctive therapy combined with S-1 or B-DOCT, trastuzumab demonstrated promising antitumor effects and manageable adverse reactions in patients with HER2 overexpression.55–57 All clinical trials showed a synergistic antitumor effect of targeted agent trastuzumab and chemotherapy agents for patients with HER2 overexpression. The level of HER2 protein should be used as a biomarker to predict the clinical outcome and aid in chemotherapeutic selection in HER2-positive patients who received trastuzumab. Similar to trastuzumab, trastuzumab emtansine (comprised of trastuzumab and a tubulin inhibitor emtansine) was initially designed to inhibit HER2-mediated signaling and mediate antibody-dependent cellular cytotoxicity. However, GATSBY, a seamless, adaptive phase II/III study, revealed that trastuzumab emtansine did not benefit patients in terms of median OS (HR = 1.15; 95% CI, 0.87–1.51), and grade 3 or more adverse reactions, such as pulmonary toxicity, were higher in the trastuzumab emtansine group than in the taxane group. Imbalances in demographics or baseline disease characteristics, toxicity, drug administration and greater heterogeneity of HER2 expression are the main factors leading to the failure of trastuzumab emtansine.58 Given these inconsistent observations, more evidence is needed for AGC in regard to using trastuzumab emtansine as a HER2-targeted second-line therapy, and the reason for these inconsistencies is worth pondering.
Pertuzumab
Pertuzumab is a humanized monoclonal antibody that binds to subdomain II to block HER2 heterodimerization. In HER2-positive breast cancer, pertuzumab and trastuzumab have complementary mechanisms and improve the rates of invasive disease–free survival.59 It is logical to hypothesize that dual HER2-targeted therapy and chemotherapy have the potential to improve survival outcomes in patients with HER2-positive AGC. JOSHUA, a phase IIa trial, evaluated two different doses of pertuzumab in patients with HER2-positive AGC/GEJ cancer from the perspective of pharmacokinetic and safety files. A dosage of 840 mg q3w was considered optimum for maintaining trough concentrations above the target in at least 90% of patients.60 Subsequently, the phase III study (JACOB trial) was designed to assess the efficacy of pertuzumab combined with trastuzumab and chemotherapy as the first-line setting in patients with HER2-positive metastatic G/GEJ cancer. Although the median OS was prolonged by 3.3 months, there was no statistical significance.61 The negative result highlights the difference in HER2 biology between breast and gastric cancer. Furthermore, gastric cancer has characteristic HER2 heterogeneity, which may affect the activity of pertuzumab.
Lapatinib
Approximately 15–45% of GC patients have a overexpression of EGFR and HER2 tyrosine kinases, and lapatinib is a dual inhibitor that blocks autophosphorylation and downstream signaling.62 More importantly, HER2 status might be affected by different stages of the disease, host immune status, concomitant genomic alterations and prior first-line chemotherapy with or without trastuzumab. The TyTAN trial showed a prolonged median OS of 2.1 months with lapatinib plus paclitaxel as second-line therapy in Asian patients with HER2-amplified AGC.63 Although the median OS and PFS were increased in lapatinib recipients, the change was not statistically significant. However, the ORR was significantly improved in the experimental group. Subgroup analyses showed clinically relevant OS and PFS gains in Chinese patients with HER2 overexpression (FISH positive and IHC 3+). The TRIO-013/LOGiC phase III trial also demonstrated that lapatinib combined with CapeOx did not improve OS for HER2-amplified GC.64 Nevertheless, a subgroup analysis based on age showed that patients < 60 years of age had significant improvement (HR = 0.69; 95% CI, 0.51–0.94), but older patients had an unfortunate outcome (HR = 1.08; 95% CI, 0.81–1.45).64 Since many factors, such as race, region, age, and sex, may influence drug effects, further studies need to be performed to choose an appropriate intent-to-treat population that could obtain a favorable prognosis from lapatinib therapy. Lapatinib could be an option for second-line therapy for AGC patients younger than 60 with HER2 overexpression (FISH positive and IHC 3+).
Other EGFR Inhibitors
In addition to trastuzumab and lapatinib, several other potential targeted inhibitors of EGFR and HER2 are under clinical development. Cetuximab is an anti-EGFR antibody. In patients with BRAF V600E-mutated colorectal cancer, cetuximab combined with encorafenib showed significant benefit with respect to OS and ORR (objective response rate).65 However, the addition of cetuximab provided no additional benefit for AGC in the EXPAND trial. The median PFS was shortened by 1.2 months (HR = 1.09; 95% CI, 0.92–1.29).66 Erlotinib is another small molecule inhibitor of EGFR that binds to its ATP binding site and inhibits the intracellular phosphorylation of EGFR. Furthermore, MARK signaling, which inhibits proliferation and activation of the intrinsic apoptosis pathway, is blocked with erlotinib.67 In both pancreatic cancer and non-small-cell lung cancer, erlotinib showed compelling results.68,69 A phase II trial showed that erlotinib has antitumor activity in patients with distal esophageal/GEJ adenocarcinomas but not in distal gastric tumors. Another phase II trial reached a similar conclusion in patients receiving erlotinib plus FOLFOX6 (oxaliplatin, fluorouracil, and leucovorin).70,71 Additionally, nimotuzumab is an EGFR inhibitor that has been used to treat EGFR-expressing 3+/4+ nasopharyngeal carcinoma in China. Nimotuzumab plus irinotecan (N-IRI) has shown potential improvement in the RR, PFS, and OS in the EGFR 2+/3+ subgroup of GC patients compared to that in the N-IRI treatment alone subgroup.72 According to the promising results, more new targeted agents will be approved in the future and will benefit an increasing number of patients.
PI3K/Akt/mTOR Inhibitor
The PI3K/Akt/mTOR pathway has an important regulatory role in processes of cellular physiology, such as glucose homeostasis, protein synthesis, cell proliferation, growth, metabolism, survival, and angiogenesis.73 Dysregulation of the PI3K/Akt pathway has been related to many cancers, making this pathway an important antitumor target.73–75 Several inhibitors targeting the pathway are currently under investigation, alone or in combination, in both solid tumors and hematologic malignancies.76 Of them, everolimus has been extensively studied.
Everolimus has been demonstrated to have an encouraging clinical benefit in other cancers as an mTOR inhibitor.77,78 A Phase I trial showed that everolimus has strong antitumor activity in Japanese patients with AGC.79 On the basis of the encouraging finding, a multicenter phase II trial showed that patients receiving everolimus achieved a primary endpoint disease control rate of 56%.80 However, a later phase III trial called GRANITE-1 observed that everolimus only prolonged the median OS of 1.1 months (HR = 0.90; 95% CI, 0.75–1.08).81 In the RADPAC trial, everolimus combined with paclitaxel in patients with GC who progressed after first-line therapy containing fluoropyrimidine or platinum regimen did not show an improvement in OS or PFS.82 Thus, more high-quality clinical trials are needed to confirm the efficacy of everolimus, and potential specific biomarkers should be further explored.
HGF/c-MET Inhibitors
HGF/c-MET signaling is closely associated with the proliferation and aggressiveness of tumors.83 Deepened scientific understanding of the relationship between c-MET and HGF has enhanced the development of these molecules as potential antitumor targets.84 The c-MET inhibitor tivantinib combined with FOLFOX in AGC showed a good effect on ORR and PFS.85
Not all inhibitors of HGF/cMET have the same antitumor efficacy. The HGF-targeted antibody rilotumumab led to a shorter median OS than placebo (8.8 vs 10.7 months) in MET-positive gastroesophageal cancer in the phase III RILOMET-1 trial.86
In addition, onartuzumab is another anti-MET antibody. However, patients did not benefit from onartuzumab plus mFOLFOX6.87 Although the HGF-cMET signaling pathway plays an essential and irreplaceable role in GC, few targeted drugs have shown efficacy in clinical trials.
Matrix Metalloproteinase (MMP) Inhibitors
Extracellular matrix enzymes are necessary for all stages of the tumor, including invasiveness, migration, apoptosis, immune surveillance, and metastasis.88 There is no doubt that MMPs could be a target for anticancer drugs.89 Several MMP inhibitors, such as marimastat, prinostat, and rebimastat, are currently in preclinical studies or clinical trials. However, so far, few MMP inhibitors are available on the market, and none of them present specific indications of antitumor activity.
Immune Checkpoint Inhibitors
Tumorigenicity is partly ascribed to the malfunction of the immune system.90 Immune checkpoints refer to an inhibitory pathway that immune cells possess to regulate and control the durability of the immune response.91 CTLA-4 and PD-1 inhibit the immune response and thus enable tumor cells with immune escape from T cell-mediated killing. Inhibition of immune checkpoints has been well developed in the management of advanced GC and many other solid tumors.91–93 Table 2 lists the current immunologic checkpoint inhibitors and related clinical trials in AGC.
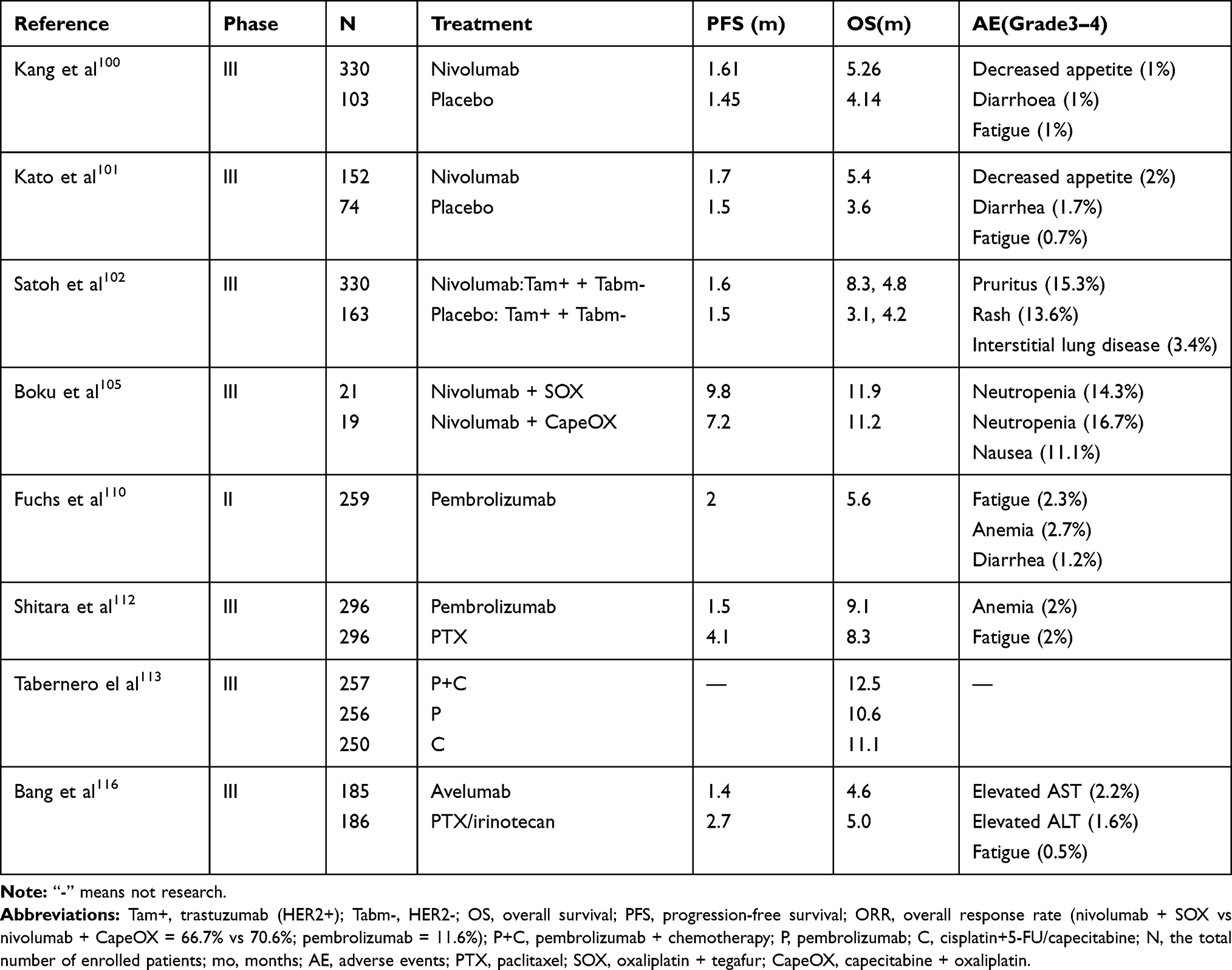 |
Table 2 Summary of Clinical Trials of Immune Checkpoint Inhibitors in AGC |
CTLA-4 Inhibitor
Ipilimumab is a monoclonal anti-CTLA-4 antibody (IgG1) that causes T-cell activation and tumor immunity. Adjuvant therapy for melanoma and non-small-cell lung cancer was stated as its use in the instruction manual.94 In the CheckMate-032 study, ipilimumab plus nivolumab demonstrated significant and durable antitumor activity in chemotherapy-refractory esophagogastric cancer.95 However, immune-related progression-free survival (irPFS) (4.90 versus 2.92 months) was not improved by ipilimumab monotherapy, resulting in study cessation.96
PD-1/PD-L1 Inhibitors
To maintain an immunosuppressive microenvironment and avoid being killed by immune surveillance, tumor cancers must activate the PD-1/PD-L1 signaling pathway.97 Tumor size, lymph node metastasis, and depth of invasion are related to the pathway; thus, inhibition of the pathway is a reasonable tactic. Moreover, high PD-1/PD-L1 expression is present in 65% of GC patients, making the pathway a promising antitumor target.98,99
Nivolumab
The PD-1 inhibitor nivolumab showed significant antitumor efficacy in the ATTRACTION-2 trial. Nivolumab extended the median OS by 1.12 months (HR = 0.63; 95% CI, 0.51–0.78) in Asian patients who had received two or more previous chemotherapy regimens.100 A subsequent analysis of a Japanese subpopulation found that nivolumab improved OS (5.4 vs 3.6 months) and reduced the risk of death (HR = 0.58; 95% CI, 0.42–0.78).101 Because the trial did not take into account HER2 status, evidence on whether patients who had previously been treated with trastuzumab influenced the efficacy of nivolumab was offered in a randomized phase III clinical trial. In both the trastuzumab+ and trastuzumab- groups, nivolumab prolonged the median OS by 5.2 months, (HR = 0.38; 95% CI, 0.22–0.66) and 0.6 months (HR = 0.71; 95% CI, 0.57–0.88), respectively. Thus, nivolumab treatment remained efficient regardless of HER2-positive or -negative status.102 The ATTRACTION-4 trial suggested that nivolumab plus chemotherapy had a good objective response in approximately two-thirds of patients as a first-line therapy, higher than that in the SOX or CapeOX alone groups.103–105
Pembrolizumab
Pembrolizumab is a monoclonal IgG4-kappa antibody that blocks PD-1 binding to PD-L1 and PD-L2.106 Pembrolizumab was approved in 2017 for PD-L1-positive AGC as a third-line (or higher) agent.107,108 In the KEYNOTE-012 study, pembrolizumab had a 22% ORR in PD-L1-positive AGC.109 Because of this result, cohort 1 of a 3-cohort KEYNOTE-059 trial evaluated the antitumor activity in patients who had experienced second- or more subsequent-line treatment. Ninety-five PD-L1-positive patients (42.4%) exhibited shrinkage of tumors; these patients also exhibited a higher ORR than PD-L1 negative patients (15.5% vs 6.4%).110 The following cohort 2 (combination therapy) and cohort 3 (monotherapy) trials showed that the ORR was 60.0% with pembrolizumab versus 25.8% with placebo.111 In the KEYNOTE-061 trial, patients who failed first-line chemotherapy containing platinum and fluoropyrimidine or trastuzumab who received pembrolizumab had a median OS that was 0.8 months longer than that in the paclitaxel group.112 The PFS was not different in either arm. Compared with paclitaxel, pembrolizumab had a more favorable safety profile and longer duration of response. Post hoc exploratory subgroup analyses suggested that patients who have a better Eastern Cooperative Oncology Group (ECOG) performance status, overexpression of PD-L1, and high microsatellite instability benefit more from pembrolizumab monotherapy. On the basis of the results, the KEYNOTE-062 trial compared the efficacy of pembrolizumab with pembrolizumab plus chemotherapy and chemotherapy alone in the first-line setting for AGC patients who were PD-L1 positive (CPS ≥1) and HER2 negative. The median OS with pembrolizumab monotherapy was noninferior to that with chemotherapy alone. However, there was a significant improvement in patients with CPS ≥10 (17.4 vs 10.8 months, HR = 0.69; 95% CI, 0.49–0.97). The combination group did not significantly prolong PFS and OS compared with that with chemotherapy alone. As a result, in PD-L1 positive patients (CPS ≥10), pembrolizumab monotherapy is recommended as an ideal option.113
Avelumab
Avelumab specifically targets PD-L1 and further blocks the binding between PD-L1 and PD-1.114 Avelumab has been approved for use in G/GEJ cancer.115 However, the JAVELIN Gastric 300 trial showed that avelumab monotherapy did not achieve a satisfactory result due to its inability to extend OS, PFS, and ORR in patients with G/GEJ cancer.116 Along with the adjustment of patients, a phase Ι trial in Japanese patients observed that avelumab exhibited durable antitumor activity with an ORR of 10%. The primary endpoints of PFS and OS were 2.4 and 9.1 months, respectively.117 In another single-arm phase Ιb trial, avelumab showed compelling results in AGC regardless of whether it was used as a first- or second-line therapy.118 However, as first-line maintenance therapy in the JAVELIN Gastric 100 trial (NCT02625610), avelumab did not show better efficacy than the continuation of chemotherapy in patients with advanced GC/GEJC who did not progress after 12 weeks of first-line oxaliplatin/fluoropyrimidine chemotherapy. However, compared with chemotherapy, avelumab had a longer duration of response and lower incidence of treatment-related adverse events. Thus, the design of further clinical trials should focus on the choice of highly selective drugs for highly selected patients.
Other Immune Checkpoint Inhibitors
Currently, many phase I or phase II trials of other PD-L1 antibodies are underway.119 Among other immune checkpoint inhibitors, atezolizumab, an anti-PD-L1 antibody, has revealed encouraging response rates and favorable safety profiles in urothelial carcinoma and lung cancer.120,121 Like atezolizumab, durvalumab, a high-affinity PD-L1 antibody, also exhibited promising results in solid tumors.122,123 However, neither showed a beneficial effect in AGC. As far as we know, immune checkpoint inhibitors are being developed in various types of cancers and certainly provide hope for cancer patients.
Conclusion and Future Perspectives
This review is an update on targeted therapy agents for AGC. Ramucirumab and apatinib have been approved in AGC as second- and third-line therapy agents with prolonged OS and PFS. Trastuzumab is considered the primary agent in HER2/neu-positive GC. Lapatinib could be an option for second-line therapy of AGC patients younger than 60 with HER2 overexpression (FISH positive and IHC 3+). Bevacizumab, regorafenib and everolimus also showed good effects, with prolonged median OS and improved disease control rate in AGC. Pembrolizumab is already approved for recurrent locally advanced or metastatic GC/GEJC with PD-L1 expression (CPS ≥1). With the progress regarding molecular targeted agents and immune checkpoint inhibitors, a wider group of patients should benefit. Most of the targeted drugs and immune checkpoint inhibitors have manageable adverse events and longer durable responses than traditional chemotherapies. As second- and subsequent-line therapy, these drugs always show compelling efficacy. However, even with the introduction of immune checkpoint inhibitors, there is still a large number of patients who fail to derive clinical benefit.124
Although research on molecular targeted agents has obtained promising results and many clinical trials involving targeted therapy agents are ongoing, efforts are still needed to select an optimal therapeutic scheme for AGC. Furthermore, we have only limited knowledge of the signaling pathway of the tumor at present. The reason why the effects of drugs targeting the same signaling pathway are not equivalent is worth exploring. For every nonspecific molecular targeted drug, the optimal time, sequence and combination should be carefully chosen in the clinic. Moreover, currently, molecular targeted drugs or immune checkpoint inhibitors are effective only for specific patients with known overexpression or activation of the targets, and the clinical benefit is modest. Many other related pathways are involved in the occurrence and development of AGC. With the advancement of network pharmacology and gene sequencing, more potential antitumor targets will be found to develop new drugs. Therefore, it is imperative to find specific clinical biomarkers for various patient subpopulations with AGC. Additionally, it is important to evaluate the influence of race, region, optimal dose, adequate endpoints, and individual chemotherapy regimens when designing a new high-quality, well-designed clinical trial.
Abbreviations
GC, gastric cancer; AGC, advanced gastric cancer; G/GEJ, gastric or gastroesophageal junction cancer; PD-1, programmed cell death 1; OS, overall survival; VEGF, vascular endothelial growth factor; NRPs, neuropilins; HR, hazard ratio; CI, confidence intervals; PDGFR, platelet-derived growth factor receptor; EGFR, Epidermal growth factor receptor; PI3K, phosphatidylinositol 3ʹ-kinase; AKT, protein kinase B; mTOR, mammalian target of rapamycin; HGF, hepatocyte growth factor; MMPs, Matrix metalloproteinases; CTLA-4, Cytotoxic T lymphocyte-associated antigen 4; BSC, best supportive care; PFS, progression-free survival; CPS, combined positive score; ORR, objective response rate; RR, response rate; GI, gastrointestinal; GT, glutamyltransferase; AE, adverse events; FDA, Food and Drug Administration; TKI, tyrosine kinase inhibitors; RTKs, receptor tyrosine kinases; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, and analysis and interpretation of data; SSN took part in drafting the article, GPY and HWL revised it critically for important intellectual content; All authors have read and approved the final version manuscript to be published. All authors agreed to be accountable for all aspects of the work.
Funding
The present study was supported by funding from the National Natural Science Foundation of China (grant no. 81870352, 81970252) and National Major New Drug Creation Project of China (grant no. 2020ZX09201-010).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Thrift AP, El-Serag HB. Burden of gastric cancer. Clin Gastroenterol Hepatol. 2019. doi:10.1016/j.cgh.2019.07.045
3. Charalampakis N, Economopoulou P, Kotsantis I, et al. Medical management of gastric cancer: a 2017 update. Cancer Med. 2018;7(1):123–133. doi:10.1002/cam4.1274
4. Kishikawa H, Ojiro K, Nakamura K, et al. Previous Helicobacter pylori infection-induced atrophic gastritis: a distinct disease entity in an understudied population without a history of eradication. Helicobacter. 2019;25(1):e12669. doi:10.1111/hel.12669
5. Wang W, Li Z, Wang J, et al. A functional polymorphism in TFF1 promoter is associated with the risk and prognosis of gastric cancer. Int J Cancer. 2018;142(9):1805–1816. doi:10.1002/ijc.31197
6. Lordick F, Shitara K, Janjigian YY. New agents on the horizon in gastric cancer. Ann Oncol. 2017;28(8):1767–1775. doi:10.1093/annonc/mdx051
7. Shitara K, Ohtsu A. Advances in systemic therapy for metastatic or advanced gastric cancer. J Natl Compr Canc Netw. 2016;14(10):1313–1320. doi:10.6004/jnccn.2016.0138
8. Lau PK, Ascierto PA, McArthur G. Melanoma: the intersection of molecular targeted therapy and immune checkpoint inhibition. Curr Opin Immunol. 2016;39:30–38. doi:10.1016/j.coi.2015.12.006
9. Song H, Zhu J, Lu D. Molecular-targeted first-line therapy for advanced gastric cancer. Cochrane Database Syst Rev. 2016;7:CD11461. doi:10.1002/14651858.CD011461.pub2
10. de Mello RA, Marques AM, Araujo A. HER2 therapies and gastric cancer: a step forward. World J Gastroenterol. 2013;19(37):6165–6169. doi:10.3748/wjg.v19.i37.6165
11. Ter Veer E, Haj MN, van Valkenhoef G, et al. Second- and third-line systemic therapy in patients with advanced esophagogastric cancer: a systematic review of the literature. Cancer Metastasis Rev. 2016;35(3):439–456. doi:10.1007/s10555-016-9632-2
12. Greig SL, Keating GM. Ramucirumab: a review in advanced gastric cancer. Biodrugs. 2015;29(5):341–351. doi:10.1007/s40259-015-0138-1
13. Karaman S, Leppanen VM, Alitalo K. Vascular endothelial growth factor signaling in development and disease. Development. 2018;145:14. doi:10.1242/dev.151019
14. Rapisarda A, Melillo G. Role of the VEGF/VEGFR axis in cancer biology and therapy. Adv Cancer Res. 2012;114:237–267. doi:10.1016/B978-0-12-386503-8.00006-5
15. Roskoski RJ. Vascular endothelial growth factor (VEGF) and VEGF receptor inhibitors in the treatment of renal cell carcinomas. Pharmacol Res. 2017;120:116–132. doi:10.1016/j.phrs.2017.03.010
16. Casak SJ, Fashoyin-Aje I, Lemery SJ, et al. FDA approval summary: ramucirumab for gastric cancer. Clin Cancer Res. 2015;21(15):3372–3376. doi:10.1158/1078-0432.CCR-15-0600
17. Fuchs CS, Tomasek J, Yong CJ, et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, Phase 3 trial. Lancet. 2014;383(9911):31–39. doi:10.1016/S0140-6736(13)61719-5
18. Wilke H, Muro K, Van Cutsem E, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224–1235. doi:10.1016/S1470-2045(14)70420-6
19. Muro K, Cho JY, Bodoky G, et al. Age does not influence efficacy of ramucirumab in advanced gastric cancer: subgroup analyses of REGARD and RAINBOW. J Gastroenterol Hepatol. 2018;33(4):814–824. doi:10.1111/jgh.14007
20. Fuchs CS, Shitara K, Di Bartolomeo M, et al. Ramucirumab with cisplatin and fluoropyrimidine as first-line therapy in patients with metastatic gastric or junctional adenocarcinoma (RAINFALL): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(3):420–435. doi:10.1016/S1470-2045(18)30791-5
21. Jang K, Kim M, Gilbert CA, et al. VEGFA activates an epigenetic pathway upregulating ovarian cancer-initiating cells. EMBO Mol Med. 2017;9(3):304–318. doi:10.15252/emmm.201606840
22. Rosen LS, Jacobs IA, Burkes RL. Bevacizumab in colorectal cancer: current role in treatment and the potential of biosimilars. Target Oncol. 2017;12(5):599–610. doi:10.1007/s11523-017-0518-1
23. Shah MA, Ramanathan RK, Ilson DH, et al. Multicenter phase II study of irinotecan, cisplatin, and bevacizumab in patients with metastatic gastric or gastroesophageal junction adenocarcinoma. J Clin Oncol. 2006;24(33):5201–5206. doi:10.1200/JCO.2006.08.0887
24. El-Rayes BF, Zalupski M, Bekai-Saab T, et al. A phase II study of bevacizumab, oxaliplatin, and docetaxel in locally advanced and metastatic gastric and gastroesophageal junction cancers. Ann Oncol. 2010;21(10):1999–2004. doi:10.1093/annonc/mdq065
25. Ohtsu A, Shah MA, Van Cutsem E, et al. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: a randomized, double-blind, placebo-controlled phase III study. J Clin Oncol. 2011;29(30):3968–3976. doi:10.1200/JCO.2011.36.2236
26. Shen L, Li J, Xu J, et al. Bevacizumab plus capecitabine and cisplatin in Chinese patients with inoperable locally advanced or metastatic gastric or gastroesophageal junction cancer: randomized, double-blind, phase III study (AVATAR study). Gastric Cancer. 2015;18(1):168–176. doi:10.1007/s10120-014-0351-5
27. Van Cutsem E, de Haas S, Kang YK, et al. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: a biomarker evaluation from the AVAGAST randomized phase III trial. J Clin Oncol. 2012;30(17):2119–2127. doi:10.1200/JCO.2011.39.9824
28. Roviello G, Ravelli A, Fiaschi AI, et al. Apatinib for the treatment of gastric cancer. Expert Rev Gastroenterol Hepatol. 2016;10(8):887–892. doi:10.1080/17474124.2016.1209407
29. Tian S, Quan H, Xie C, et al. YN968D1 is a novel and selective inhibitor of vascular endothelial growth factor receptor-2 tyrosine kinase with potent activity in vitro and in vivo. Cancer Sci. 2011;102(7):1374–1380. doi:10.1111/j.1349-7006.2011.01939.x
30. Li J, Qin S, Xu J, et al. Apatinib for chemotherapy-refractory advanced metastatic gastric cancer: results from a randomized, placebo-controlled, parallel-arm, phase II trial. J Clin Oncol. 2013;31(26):3219–3225. doi:10.1200/JCO.2013.48.8585
31. Li J, Qin S, Xu J, et al. Randomized, double-blind, placebo-controlled phase III trial of apatinib in patients with chemotherapy-refractory advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junction. J Clin Oncol. 2016;34(13):1448–1454. doi:10.1200/JCO.2015.63.5995
32. Roviello G, Ravelli A, Polom K, et al. Apatinib: a novel receptor tyrosine kinase inhibitor for the treatment of gastric cancer. Cancer Lett. 2016;372(2):187–191. doi:10.1016/j.canlet.2016.01.014
33. Lutz SZ, Ullrich A, Haring HU, et al. Sunitinib specifically augments glucose-induced insulin secretion. Cell Signal. 2017;36:91–97. doi:10.1016/j.cellsig.2017.04.018
34. Bang YJ, Kang YK, Kang WK, et al. Phase II study of sunitinib as second-line treatment for advanced gastric cancer. Invest New Drugs. 2011;29(6):1449–1458. doi:10.1007/s10637-010-9438-y
35. Moehler M, Mueller A, Hartmann JT, et al. An open-label, multicentre biomarker-oriented AIO phase II trial of sunitinib for patients with chemo-refractory advanced gastric cancer. Eur J Cancer. 2011;47(10):1511–1520. doi:10.1016/j.ejca.2011.04.006
36. Lee J, Shin SJ, Chung IJ, et al. A phase II open-label randomized multicenter trial of TSU-68 in combination with S-1 and oxaliplatin versus S-1 in combination with oxaliplatin in patients with metastatic colorectal cancer. Invest New Drugs. 2014;32(3):561–568. doi:10.1007/s10637-014-0075-8
37. Koizumi W, Yamaguchi K, Hosaka H, et al. Randomised phase II study of S-1/cisplatin plus TSU-68 vs S-1/cisplatin in patients with advanced gastric cancer. Br J Cancer. 2013;109(8):2079–2086. doi:10.1038/bjc.2013.555
38. Wilhelm SM, Dumas J, Adnane L, et al. Regorafenib (BAY 73-4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int J Cancer. 2011;129(1):245–255. doi:10.1002/ijc.25864
39. Lubberman F, van der Graaf W, Xu L, et al. The effect of gastrectomy on regorafenib exposure and progression-free survival in patients with advanced gastrointestinal stromal tumours. Br J Clin Pharmacol. 2019;85(10):2399–2404. doi:10.1111/bcp.14061
40. Pavlakis N, Sjoquist KM, Martin AJ, et al. Regorafenib for the treatment of advanced gastric cancer (INTEGRATE): a multinational placebo-controlled phase II trial. J Clin Oncol. 2016;34(23):2728–2735. doi:10.1200/JCO.2015.65.1901
41. Martin AJ, Gibbs E, Sjoquist K, et al. Health-related quality of life associated with regorafenib treatment in refractory advanced gastric adenocarcinoma. Gastric Cancer. 2018;21(3):473–480. doi:10.1007/s10120-017-0754-1
42. Sjoquist KM, Pavlakis N, Martin AJ, et al. Integrate II: a randomised phase 3 double-blind placebo-controlled study of regorafenib in refractory advanced gastro-oesophageal cancer (AGOC)—an international study organized by the Australasian Gastrointestinal Trials Group (AGITG). J Clin Oncol. 2017;35(15_suppl):S4136. doi:10.1200/JCO.2017.35.15_suppl.TPS4136
43. Sigismund S, Avanzato D, Lanzetti L. Emerging functions of the EGFR in cancer. Mol Oncol. 2018;12(1):3–20. doi:10.1002/1878-0261.12155
44. Tebbutt N, Pedersen MW, Johns TG. Targeting the ERBB family in cancer: couples therapy. Nat Rev Cancer. 2013;13(9):663–673. doi:10.1038/nrc3559
45. Wang Z. ErbB receptors and cancer. Methods Mol Biol. 2017;1652:3–35. doi:10.1007/978-1-4939-7219-7_1
46. Kavuri SM, Jain N, Galimi F, et al. HER2 activating mutations are targets for colorectal cancer treatment. Cancer Discov. 2015;5(8):832–841. doi:10.1158/2159-8290.CD-14-1211
47. Chua TC, Merrett ND. Clinicopathologic factors associated with HER2-positive gastric cancer and its impact on survival outcomes–a systematic review. Int J Cancer. 2012;130(12):2845–2856. doi:10.1002/ijc.26292
48. Mazieres J, Barlesi F, Filleron T, et al. Lung cancer patients with HER2 mutations treated with chemotherapy and HER2-targeted drugs: results from the European EUHER2 cohort. Ann Oncol. 2016;27(2):281–286. doi:10.1093/annonc/mdv573
49. Zanini E, Louis LS, Antony J, et al. The tumor-suppressor protein OPCML potentiates Anti-EGFR- and Anti-HER2-targeted therapy in HER2-positive ovarian and breast cancer. Mol Cancer Ther. 2017;16(10):2246–2256. doi:10.1158/1535-7163.MCT-17-0081
50. Habban AM, Sateesh MN, Ahmad J. Epidermal growth factor receptor based active targeting: a paradigm shift towards advance tumor therapy. Artif Cells Nanomed Biotechnol. 2018;46(sup2):1188–1198. doi:10.1080/21691401.2018.1481863
51. Jeong J, Kim W, Kim LK, et al. HER2 signaling regulates HER2 localization and membrane retention. PLoS One. 2017;12(4):e174849. doi:10.1371/journal.pone.0174849
52. Parakh S, Gan HK, Parslow AC, et al. Evolution of anti-HER2 therapies for cancer treatment. Cancer Treat Rev. 2017;59:1–21. doi:10.1016/j.ctrv.2017.06.005
53. Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687–697. doi:10.1016/S0140-6736(10)61121-X
54. Ryu MH, Yoo C, Kim JG, et al. Multicenter phase II study of trastuzumab in combination with capecitabine and oxaliplatin for advanced gastric cancer. Eur J Cancer. 2015;51(4):482–488. doi:10.1016/j.ejca.2014.12.015
55. Kimura Y, Fujii M, Masuishi T, et al. Multicenter phase II study of trastuzumab plus S-1 alone in elderly patients with HER2-positive advanced gastric cancer (JACCRO GC-06). Gastric Cancer. 2018;21(3):421–427. doi:10.1007/s10120-017-0766-x
56. Gong J, Liu T, Fan Q, et al. Optimal regimen of trastuzumab in combination with oxaliplatin/capecitabine in first-line treatment of HER2-positive advanced gastric cancer (CGOG1001): a multicenter, phase II trial. BMC Cancer. 2016;16:68. doi:10.1186/s12885-016-2092-9
57. Meulendijks D, Beerepoot LV, Boot H, et al. Trastuzumab and bevacizumab combined with docetaxel, oxaliplatin and capecitabine as first-line treatment of advanced HER2-positive gastric cancer: a multicenter phase II study. Invest New Drugs. 2016;34(1):119–128. doi:10.1007/s10637-015-0309-4
58. Thuss-Patience PC, Shah MA, Ohtsu A, et al. Trastuzumab emtansine versus taxane use for previously treated HER2-positive locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma (GATSBY): an international randomised, open-label, adaptive, Phase 2/3 study. Lancet Oncol. 2017;18(5):640–653. doi:10.1016/S1470-2045(17)30111-0
59. von Minckwitz G, Procter M, de Azambuja E, et al. Adjuvant pertuzumab and trastuzumab in early HER2-Positive breast cancer. N Engl J Med. 2017;377(2):122–131. doi:10.1056/NEJMoa1703643
60. Kang YK, Rha SY, Tassone P, et al. A phase IIa dose-finding and safety study of first-line pertuzumab in combination with trastuzumab, capecitabine and cisplatin in patients with HER2-positive advanced gastric cancer. Br J Cancer. 2014;111(4):660–666. doi:10.1038/bjc.2014.356
61. Tabernero J, Hoff PM, Shen L, et al. Pertuzumab plus trastuzumab and chemotherapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (JACOB): final analysis of a double-blind, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2018;19(10):1372–1384. doi:10.1016/S1470-2045(18)30481-9
62. Iqbal S, Goldman B, Fenoglio-Preiser CM, et al. Southwest oncology group study S0413: a phase II trial of lapatinib (GW572016) as first-line therapy in patients with advanced or metastatic gastric cancer. Ann Oncol. 2011;22(12):2610–2615. doi:10.1093/annonc/mdr021
63. Satoh T, Xu R-H, Chung HC, et al. Lapatinib plus paclitaxel versus paclitaxel alone in the second-line treatment of HER2 -amplified advanced gastric cancer in Asian populations: tyTAN—a randomized, phase III study. J Clin Oncol. 2014;32(19):2039–2049. doi:10.1200/JCO.2013.53.6136
64. Hecht JR, Bang YJ, Qin SK, et al. Lapatinib in combination with capecitabine plus oxaliplatin in human epidermal growth factor receptor 2-Positive advanced or metastatic gastric, esophageal, or gastroesophageal adenocarcinoma: TRIO-013/LOGiC–A randomized phase III trial. J Clin Oncol. 2016;34(5):443–451. doi:10.1200/JCO.2015.62.6598
65. Kopetz S, Grothey A, Yaeger R, et al. Encorafenib, binimetinib, and cetuximab in BRAF V600E-mutated colorectal cancer. N Engl J Med. 2019;381(17):1632–1643. doi:10.1056/NEJMoa1908075
66. Lordick F, Kang YK, Chung HC, et al. Capecitabine and cisplatin with or without cetuximab for patients with previously untreated advanced gastric cancer (EXPAND): a randomised, open-label phase 3 trial. Lancet Oncol. 2013;14(6):490–499. doi:10.1016/S1470-2045(13)70102-5
67. Solassol I, Pinguet F, Quantin X. FDA- and EMA-approved tyrosine kinase inhibitors in advanced EGFR-mutated non-small cell lung cancer: safety, tolerability, plasma concentration monitoring, and management. Biomolecules. 2019;9:11. doi:10.3390/biom9110668
68. Haas M, Siveke JT, Schenk M, et al. Efficacy of gemcitabine plus erlotinib in rash-positive patients with metastatic pancreatic cancer selected according to eligibility for FOLFIRINOX: a prospective phase II study of the ‘arbeitsgemeinschaft internistische onkologie’. Eur J Cancer. 2018;94:95–103. doi:10.1016/j.ejca.2018.02.008
69. Arbour KC, Riely GJ. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: a review. JAMA. 2019;322(8):764–774. doi:10.1001/jama.2019.11058
70. Dragovich T, McCoy S, Fenoglio-Preiser CM, et al. Phase II trial of erlotinib in gastroesophageal junction and gastric adenocarcinomas: SWOG 0127. J Clin Oncol. 2006;24(30):4922–4927. doi:10.1200/JCO.2006.07.1316
71. Wainberg ZA, Lin LS, DiCarlo B, et al. Phase II trial of modified FOLFOX6 and erlotinib in patients with metastatic or advanced adenocarcinoma of the oesophagus and gastro-oesophageal junction. Br J Cancer. 2011;105(6):760–765. doi:10.1038/bjc.2011.280
72. Satoh T, Lee KH, Rha SY, et al. Randomized phase II trial of nimotuzumab plus irinotecan versus irinotecan alone as second-line therapy for patients with advanced gastric cancer. Gastric Cancer. 2015;18(4):824–832. doi:10.1007/s10120-014-0420-9
73. Aoki M, Fujishita T. Oncogenic roles of the PI3K/AKT/mTOR axis. Curr Top Microbiol Immunol. 2017;407:153–189. doi:10.1007/82_2017_6
74. Asati V, Mahapatra DK, Bharti SK. PI3K/Akt/mTOR and Ras/Raf/MEK/ERK signaling pathways inhibitors as anticancer agents: structural and pharmacological perspectives. Eur J Med Chem. 2016;109:314–341. doi:10.1016/j.ejmech.2016.01.012
75. Lien EC, Dibble CC, Toker A. PI3K signaling in cancer: beyond AKT. Curr Opin Cell Biol. 2017;45:62–71. doi:10.1016/j.ceb.2017.02.007
76. Ediriweera MK, Tennekoon KH, Samarakoon SR. Role of the PI3K/AKT/mTOR signaling pathway in ovarian cancer: biological and therapeutic significance. Semin Cancer Biol. 2019;59:147–160. doi:10.1016/j.semcancer.2019.05.012
77. Pascual J, Berger SP, Witzke O, et al. Everolimus with reduced calcineurin inhibitor exposure in renal transplantation. J Am Soc Nephrol. 2018;29(7):1979–1991. doi:10.1681/ASN.2018010009
78. Hare SH, Harvey AJ. MTOR function and therapeutic targeting in breast cancer. Am J Cancer Res. 2017;7(3):383–404.
79. Okamoto I, Doi T, Ohtsu A, et al. Phase I clinical and pharmacokinetic study of RAD001 (everolimus) administered daily to Japanese patients with advanced solid tumors. Jpn J Clin Oncol. 2010;40(1):17–23. doi:10.1093/jjco/hyp120
80. Doi T, Muro K, Boku N, et al. Multicenter phase II study of everolimus in patients with previously treated metastatic gastric cancer. J Clin Oncol. 2010;28(11):1904–1910. doi:10.1200/JCO.2009.26.2923
81. Ohtsu A, Ajani JA, Bai YX, et al. Everolimus for previously treated advanced gastric cancer: results of the randomized, double-blind, phase III GRANITE-1 study. J Clin Oncol. 2013;31(31):3935–3943. doi:10.1200/JCO.2012.48.3552
82. Lorenzen S, Knorrenschild JR, Pauligk C, et al. A randomized, double-blind, multi-center phase III study evaluating paclitaxel with and without RAD001 in patients with gastric or esophagogastric junction carcinoma who have progressed after therapy with a fluoropyrimidine/platinum-containing regimen (RADPAC). J Clin Oncol. 2017;35(15_suppl):4027. doi:10.1200/JCO.2017.35.15_suppl.4027
83. Kim KH, Kim H. Progress of antibody-based inhibitors of the HGF-cMET axis in cancer therapy. Exp Mol Med. 2017;49(3):e307. doi:10.1038/emm.2017.17
84. Bradley CA, Salto-Tellez M, Laurent-Puig P, et al. Targeting c-MET in gastrointestinal tumours: rationale, opportunities and challenges. Nat Rev Clin Oncol. 2017;14(9):562–576. doi:10.1038/nrclinonc.2017.40
85. Pant S, Patel M, Kurkjian C, et al. A phase II study of the c-Met inhibitor tivantinib in combination with FOLFOX for the treatment of patients with previously untreated metastatic adenocarcinoma of the distal esophagus, gastroesophageal junction, or stomach. Cancer Invest. 2017;35(7):463–472. doi:10.1080/07357907.2017.1337782
86. Catenacci D, Tebbutt NC, Davidenko I, et al. Rilotumumab plus epirubicin, cisplatin, and capecitabine as first-line therapy in advanced MET-positive gastric or gastro-oesophageal junction cancer (RILOMET-1): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2017;18(11):1467–1482. doi:10.1016/S1470-2045(17)30566-1
87. Shah MA, Cho JY, Tan IB, et al. A randomized phase II study of FOLFOX with or without the MET inhibitor onartuzumab in advanced adenocarcinoma of the stomach and gastroesophageal junction. Oncologist. 2016;21(9):1085–1090. doi:10.1634/theoncologist.2016-0038
88. Amar S, Smith L, Fields GB. Matrix metalloproteinase collagenolysis in health and disease. Biochim Biophys Acta Mol Cell Res. 2017;1864(11):1940–1951. doi:10.1016/j.bbamcr.2017.04.015
89. Winer A, Adams S, Mignatti P. Matrix metalloproteinase inhibitors in cancer therapy: turning past failures into future successes. Mol Cancer Ther. 2018;17(6):1147–1155. doi:10.1158/1535-7163.MCT-17-0646
90. Alsina M, Moehler M, Hierro C, et al. Immunotherapy for gastric cancer: a focus on immune checkpoints. Target Oncol. 2016;11(4):469–477. doi:10.1007/s11523-016-0421-1
91. Abril-Rodriguez G, Ribas A. SnapShot: immune checkpoint inhibitors. Cancer Cell. 2017;31(6):848. doi:10.1016/j.ccell.2017.05.010
92. Moehler M, Delic M, Goepfert K, et al. Immunotherapy in gastrointestinal cancer: recent results, current studies and future perspectives. Eur J Cancer. 2016;59:160–170. doi:10.1016/j.ejca.2016.02.020
93. Abdel-Rahman O. Immune checkpoints aberrations and gastric cancer; Assessment of prognostic value and evaluation of therapeutic potentials. Crit Rev Oncol Hematol. 2016;97:65–71. doi:10.1016/j.critrevonc.2015.08.015
94. Coens C, Suciu S, Chiarion-Sileni V, et al. Health-related quality of life with adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): secondary outcomes of a multinational, randomised, double-blind, phase 3 trial. Lancet Oncol. 2017;18(3):393–403. doi:10.1016/S1470-2045(17)30015-3
95. Janjigian YY, Bendell J, Calvo E, et al. CheckMate-032 study: efficacy and safety of nivolumab and nivolumab plus ipilimumab in patients with metastatic esophagogastric cancer. J Clin Oncol. 2018;36(28):2836–2844. doi:10.1200/JCO.2017.76.6212
96. Bang YJ, Cho JY, Kim YH, et al. Efficacy of sequential ipilimumab monotherapy versus best supportive care for unresectable locally advanced/metastatic gastric or gastroesophageal junction cancer. Clin Cancer Res. 2017;23(19):5671–5678. doi:10.1158/1078-0432.CCR-17-0025
97. Yuan J, Zhang J, Zhu Y, et al. Programmed death-ligand-1 expression in advanced gastric cancer detected with RNA in situ hybridization and its clinical significance. Oncotarget. 2016;7(26):39671–39679. doi:10.18632/oncotarget.9381
98. Kawazoe A, Kuwata T, Kuboki Y, et al. Clinicopathological features of programmed death ligand 1 expression with tumor-infiltrating lymphocyte, mismatch repair, and Epstein-Barr virus status in a large cohort of gastric cancer patients. Gastric Cancer. 2017;20(3):407–415. doi:10.1007/s10120-016-0631-3
99. Sharma P, Allison JP. Immune checkpoint targeting in cancer therapy: toward combination strategies with curative potential. Cell. 2015;161(2):205–214. doi:10.1016/j.cell.2015.03.030
100. Kang YK, Boku N, Satoh T, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390(10111):2461–2471. doi:10.1016/S0140-6736(17)31827-5
101. Kato K, Satoh T, Muro K, et al. A subanalysis of Japanese patients in a randomized, double-blind, placebo-controlled, phase 3 trial of nivolumab for patients with advanced gastric or gastro-esophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2). Gastric Cancer. 2019;22(2):344–354. doi:10.1007/s10120-018-0899-6
102. Satoh T, Kang YK, Chao Y, et al. Exploratory subgroup analysis of patients with prior trastuzumab use in the ATTRACTION-2 trial: a randomized phase III clinical trial investigating the efficacy and safety of nivolumab in patients with advanced gastric/gastroesophageal junction cancer. Gastric Cancer. 2019;23(1):143–153. doi:10.1007/s10120-019-00970-8
103. Cunningham D, Starling N, Rao S, et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med. 2008;358(1):36–46. doi:10.1056/NEJMoa073149
104. Yamada Y, Higuchi K, Nishikawa K, et al. Phase III study comparing oxaliplatin plus S-1 with cisplatin plus S-1 in chemotherapy-naive patients with advanced gastric cancer. Ann Oncol. 2015;26(1):141–148. doi:10.1093/annonc/mdu472
105. Boku N, Ryu MH, Kato K, et al. Safety and efficacy of nivolumab in combination with S-1/capecitabine plus oxaliplatin in patients with previously untreated, unresectable, advanced, or recurrent gastric/gastroesophageal junction cancer: interim results of a randomized, phase II trial (ATTRACTION-4). Ann Oncol. 2019;30(2):250–258. doi:10.1093/annonc/mdy540
106. Kwok G, Yau TC, Chiu JW, et al. Pembrolizumab (Keytruda). Hum Vaccin Immunother. 2016;12(11):2777–2789. doi:10.1080/21645515.2016.1199310
107. Fashoyin-Aje L, Donoghue M, Chen H, et al. FDA approval summary: pembrolizumab for recurrent locally advanced or metastatic gastric or gastroesophageal junction adenocarcinoma expressing PD-L1. Oncologist. 2019;24(1):103–109. doi:10.1634/theoncologist.2018-0221
108. Joshi SS, Maron SB, Catenacci DV. Pembrolizumab for treatment of advanced gastric and gastroesophageal junction adenocarcinoma. Future Oncol. 2018;14(5):417–430. doi:10.2217/fon-2017-0436
109. Muro K, Chung HC, Shankaran V, et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): a multicentre, open-label, Phase 1b trial. Lancet Oncol. 2016;17(6):717–726. doi:10.1016/S1470-2045(16)00175-3
110. Fuchs CS, Doi T, Jang RW, et al. Safety and efficacy of pembrolizumab monotherapy in patients with previously treated advanced gastric and gastroesophageal junction cancer: phase 2 clinical KEYNOTE-059 trial. JAMA Oncol. 2018;4(5):e180013. doi:10.1001/jamaoncol.2018.0013
111. Bang YJ, Kang YK, Catenacci DV, et al. Pembrolizumab alone or in combination with chemotherapy as first-line therapy for patients with advanced gastric or gastroesophageal junction adenocarcinoma: results from the phase II nonrandomized KEYNOTE-059 study. Gastric Cancer. 2019;22(4):828–837. doi:10.1007/s10120-018-00909-5
112. Shitara K, Ozguroglu M, Bang Y-J, et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet. 2018;392(10142):123–133. doi:10.1016/S0140-6736(18)31257-1
113. Tabernero J, Van Cutsem E, Bang Y, et al. Pembrolizumab with or without chemotherapy versus chemotherapy for first-line treatment of advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma: the Phase 3 KEYNOTE-062 Study. Ann Oncol. 2019;30(Suppl 4):v152–v153. doi:10.1093/annonc/mdz183.001
114. Hamilton G, Rath B. Avelumab: combining immune checkpoint inhibition and antibody-dependent cytotoxicity. Expert Opin Biol Ther. 2017;17(4):515–523. doi:10.1080/14712598.2017.1294156
115. Patel MR, Ellerton J, Infante JR, et al. Avelumab in metastatic urothelial carcinoma after platinum failure (JAVELIN solid tumor): pooled results from two expansion cohorts of an open-label, phase 1 trial. Lancet Oncol. 2018;19(1):51–64. doi:10.1016/S1470-2045(17)30900-2
116. Bang YJ, Ruiz EY, Van Cutsem E, et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: primary analysis of JAVELIN gastric 300. Ann Oncol. 2018;29(10):2052–2060. doi:10.1093/annonc/mdy264
117. Doi T, Iwasa S, Muro K, et al. Phase 1 trial of avelumab (anti-PD-L1) in Japanese patients with advanced solid tumors, including dose expansion in patients with gastric or gastroesophageal junction cancer: the JAVELIN solid tumor JPN trial. Gastric Cancer. 2019;22(4):817–827. doi:10.1007/s10120-018-0903-1
118. Chung HC, Arkenau HT, Lee J, et al. Avelumab (anti-PD-L1) as first-line switch-maintenance or second-line therapy in patients with advanced gastric or gastroesophageal junction cancer: phase 1b results from the JAVELIN solid tumor trial. J Immunother Cancer. 2019;7(1):30. doi:10.1186/s40425-019-0508-1
119. Kudo M. Systemic therapy for hepatocellular carcinoma: latest advances. Cancers (Basel). 2018;10(11):412. doi:10.3390/cancers10110412
120. Balar AV, Galsky MD, Rosenberg JE, et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet. 2017;389(10064):67–76. doi:10.1016/S0140-6736(16)32455-2
121. Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255–265. doi:10.1016/S0140-6736(16)32517-X
122. Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2017;377(20):1919–1929. doi:10.1056/NEJMoa1709937
123. Powles T, O’Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 open-label study. JAMA Oncol. 2017;3(9):e172411. doi:10.1001/jamaoncol.2017.2411
124. Kyi C, Postow MA. Immune checkpoint inhibitor combinations in solid tumors: opportunities and challenges. Immunotherapy-UK. 2016;8(7):821–837. doi:10.2217/imt-2016-0002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.