Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Current Knowledge, Satisfaction, and Use of E-Health Mobile Application (Seha) Among the General Population of Saudi Arabia: A Cross-Sectional Study
Authors Aldhahir AM ![]() , Alqahtani JS
, Alqahtani JS ![]() , Althobiani MA
, Althobiani MA ![]() , Alghamdi SM
, Alghamdi SM ![]() , Alanazi AF, Alnaim N, Alqarni AA
, Alanazi AF, Alnaim N, Alqarni AA ![]() , Alwafi H
, Alwafi H ![]()
Received 27 January 2022
Accepted for publication 23 March 2022
Published 1 April 2022 Volume 2022:15 Pages 667—678
DOI https://doi.org/10.2147/JMDH.S355093
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdulelah M Aldhahir,1 Jaber S Alqahtani,2 Malik A Althobiani,3,4 Saeed M Alghamdi,5,6 Abeer F Alanazi,7 Norah Alnaim,8 Abdullah A Alqarni,3 Hassan Alwafi9
1Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 2Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia; 3Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia; 4UCL Respiratory, University College London, London, WC1E 6BT, UK; 5Clinical Technology Department, Respiratory Care Program, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia; 6National Heart and Lung Institute, Imperial College London, London, UK; 7Department of Pharmaceutical and Biological Sciences, UCL School of Pharmacy, London, UK; 8Department of Computer Science, College of Science and Humanities in Jubail, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 9Faculty of Medicine, Umm Al-Qura University, Mecca, Saudi Arabia
Correspondence: Abdulelah M Aldhahir, Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia, Email [email protected]
Background: General population knowledge, satisfaction, and barriers to using Seha app have not been evaluated from a large-scale perspective. Therefore, this study aimed to explore current knowledge, satisfaction, and barriers of using Seha app and identify the most common mobile health application used among the general population in Saudi Arabia.
Methods: A cross-sectional online survey, consisting of 25 questions, was distributed among the general population of Saudi Arabia. Descriptive statistics were used to describe the respondents’ characteristics. Categorical variables were reported as frequencies and percentages. A chi-square (χ 2) test was conducted to assess the statistical difference between respondents’ demographic characteristics and their knowledge and use of the app.
Results: Overall, 5008 respondents, both Saudi (3723: 74%) and non-Saudi (1285: 26%) as well as male 2142 (43%) and female 2866 (57%), across the Kingdom of Saudi Arabia completed the online survey. A total of 2921 (58%) had heard of the Seha app, although only 1286 (25%) had used the app. Higher percentages of users were from the western region, females and those within the age group of ≥ 51 years old, 388 users (29%: P< 0.001), 804 (28%; P< 0.001) and 67 (35%; P=0.013), respectively. Consulting a doctor was the most frequently utilized service, 576 users (58%). Respondents strongly agreed 402 (41%) that Seha was easy to use, and 538 (54%) strongly agreed that they would recommend Seha to others. The most common barrier of using Seha was a lack of knowledge about the app and its benefits, at 1556 (35%). Overall, the Tawakkalna app was the most utilized mobile health application provided by MOH used 2170 (48%).
Conclusion: Utilization of the Seha app is quite low due to a lack of knowledge about the app and its benefits. Thus, the MOH should promote public awareness about the app and its benefits.
Keywords: E-health, telemedicine, Saudi Arabia, Saudi Ministry of Health, mobile app, user satisfaction, mHealth
Introduction
The population of Saudi Arabia will likely increase and reach 45 million by 2050.1 Currently, the average ratio of physicians to patients is 14 to 10,000 patients.2 As Saudi Arabia’s population continues to rise, healthcare services could become overwhelmed if no action is taken.2,3 Patients might not be able to seek healthcare services for multiple reasons, including pandemics such as COVID-19, which started in December 2019.
Several studies have suggested the use of technology (telemedicine) to provide better access to healthcare services for those who need it and to reduce the burden of healthcare costs.4–9
Saudi Arabia, represented by the MOH, took a step forward and started several initiatives aimed to improving the provision of healthcare services across the Kingdom of Saudi Arabia. In 2013, telemedicine was introduced in Saudi Arabia through a collaborative effort among the MOH, the Canadian Health Info way and the Ontario Telemedicine Network that aimed to adopt and implement telemedicine services in Saudi Arabia.10 In 2018, the MOH decided to further enhance its telemedicine provision by introducing the Seha mobile app, followed by several apps between 2019 and 2020, such as the Tawakkalna, Mawid, Tabaud and Tataman apps.11,12 The Tawakkalna app facilitates people’s movement during curfew and national lockdowns, request travel authorization, and notify individuals if they become into close contact with infectious zones.12 The Mawid app facilitates online booking, changing, and rescheduling patients’ appointments across primary care centers.12 The Tabaud app prompts the health and safety of the public during the Covid-19 pandemic by notifying users if they become into close contact with an infected individual.12 The Tataman app provides health care and protection to accelerate recovery for individuals who are self-isolating or in quarantine.12 The Seha app is designed to provide and enable individuals who seek medical care to receive health and preventive care at their homes through audio-video medical consultations by the MOH’s specialists (doctor consultation) and through artificial intelligence technologies (smart Seha), which provide safe medical information and health tips electronically. The Seha app also provides health assessment questions and a report (health check) that includes health scores based on disease/condition statistics. The MOH reported that around 653,000 users have used and registered for the Seha app.13 There is a limited evidence in evaluating Seha app from users perspective. A study conducted by Alharbi et al (2020) which included 528 responders which evaluated seha app concluded that users were satisfied with the Seha app.6 However, the study included a small sample size and did not evaluate each service provided by the Seha app from the user’s perspective. Therefore, this study aims to explore the current knowledge, satisfaction, and barriers to using the Seha mobile app and identify the most common health mobile application, provided by MOH, utilized among the general population in Saudi Arabia.
Methods
Study Design
A cross-sectional survey was conducted via Survey Monkey between December 15, 2020 and April 23, 2021.
Questionnaire Tool
The survey consisted of 25 questions and was developed and validated by four experts in the field of telemedicine. Content and face validity were assessed after piloting this survey with 10 volunteers. The overall, Cronbach’s alpha reliability coefficient was 0.83, demonstrating a reliable tool. Before starting to answer the questionnaire, the aim of the study was provided with information about the primary investigator. Additionally, no personal information was recorded, participation was voluntary, by asking a question if you were happy to complete the survey or not. Also, additional statement was provided in the survey which is
By answering yes in completing the survey question, you voluntarily agree to participate in this study and give your consent to use your anonymous data for research purposes.
The time required to fill in the survey statements was all provided in the description of the questionnaire. The questionnaire consisted of one-page structured responses that involved multiple-choice answers in five sections. Section 1 contained the respondents’ demographic In Section 2, respondents were asked if they had ever heard of or used the Seha app before. Based on the usage question, if the respondents’ answer was “Yes,” they were allowed to proceed with the survey, but if their answer was “No,” they were directed to the question about other apps used provided by the MOH, and barriers of not using the Seha app. Section 3 comprised five multiple-choice questions regarding the frequency of the use of the Seha app and the services provided in the Seha app. It also asked about the most common service used by respondents in the Seha app. Section 4 comprised six questions measuring satisfaction among the general population with the services provided by the Seha app using a 5-point Likert scale ranging from 1 = very unsatisfied to 5 = very satisfied in four questions. The 5-point Likert scale in the remaining two questions ranged from 1 = strongly disagree to 5 = strongly agree. In Section 5, consisted of questions asked about usefulness, easiness and would recommend the app to anyone using a 4-point Likert scale ranging from 1 = strongly disagree to 4 = strongly agree. Section 5 also comprised two multiple-choice questions about utilization of other apps provided by the MOH and barriers of using of the Seha app. The original version of the survey was developed in English and was given to a professional translator who translated it into Arabic. Then, another professional translator translated the Arabic version back into English. The two English versions were compared by both professional translators in a process known as “forward-backward translation”.14
Study Population and Sampling Strategy
Convenience sampling techniques were used to recruit the study participants because residents in Saudi Arabia (including citizens and residents) were the main target of the study. Social media tools such as WhatsApp, Twitter, and Telegram were used to distribute the survey. Institutional Review Board approval for the study was obtained from Jazan University, reference number REC42/1/010.
Sample Size
To estimate the sample size, the World Health Organization recommendations for the minimal sample size were used in this study.15 Using a confidence interval of 95%, a standard deviation of 0.5, and a margin of error of 5%, the required sample size was 385 participants from each study population.
Statistical Analysis
Data were collected and analyzed using the Statistical Package for Social Sciences (SPSS software, Version 25). The categorical variables were reported and presented in percentages and frequencies. A chi-square (χ2) test was used to assess the statistically significant difference between categorical variables. Statistical significance was considered if the P< 0.05.
Results
Overall, 5008 respondents, both Saudi 3723 (74%) and non-Saudi 1285 (26%), completed the online survey between December 15, 2020, and April 23, 2021. The survey attempted to reach all regions of the Kingdom of Saudi Arabia. Respondents were distributed across the Kingdom regions as follows: 1336 (27%) were from the central region; 1315 (26%) were from the western region; 1110 (22%) were from the eastern region; 813 (16%) were from the southern region and 434 (9%) were from the northern region (Table 1).
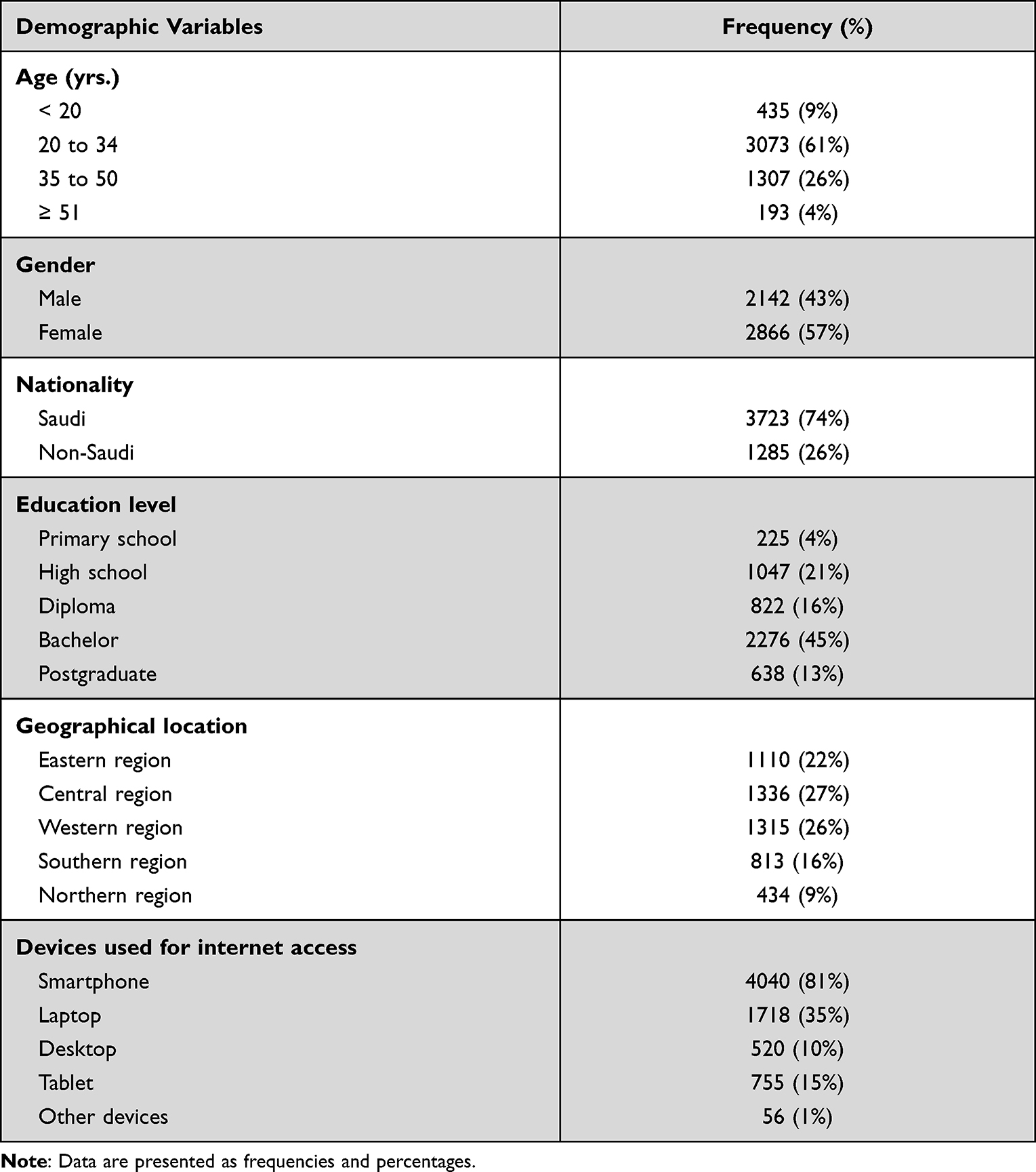 |
Table 1 Demographic Data and Characteristics of All Respondents (N= 5008) |
Out of 5008 respondents, 3073 (61%) of them were aged 20–34 years, and just over half 2855 (57%) of the respondents were female. The level of education indicated that almost half of the respondents (2279, 45%) held at least a bachelor’s degree (Table 1). The results showed that out of 5008 respondents, 4040 (81%) used smartphones to access the internet. Following the use of smartphones, 1718 (35%) used a laptop, 520 (10%) used a desktop, 755 (15%) used a tablet, and 56 (1%) used other devices for internet access (Table 1).
Awareness and Utilization of the Seha App
Out of 5008 respondents, 2921 (58%) had heard of the Seha app, and 1431 (29%) had never heard of the Seha app; although only 1286 (25%) had used Seha, and 2635 (53%) had never used the Seha before. There was no significant difference between age and awareness of the Seha app (Table 2). There was a significant difference between age and the use of the Seha app (P=0.013). The results showed that within the age group of ≥51 years, 67 (35%) out of 193 respondents used the Seha app, which was the highest percentage of usage among all age groups. Furthermore, Table 3 shows a statistically significant difference between the awareness (P=0.003) and gender, as well as the use of the Seha app (P<0.001) and gender. Among 2866 females, 1730 (60%) had heard of Seha, and 804 (28%) had used Seha, which was a higher than for males. Concerning educational level, out of 638 postgraduate respondents, there was significantly greater awareness and use of the Seha app—awareness: 428 (67%); use: 248 (39%). The analysis showed a statistically significant difference between the respondents’ region of residence and their awareness (P<0.001) and use of the Seha app (P<0.001). Out of 1315 respondents from the western region, 388 (29%) reported using the Seha app, which was the highest reported use; and out of 434 respondents from the northern region, 83 (19%) reported using the Seha app, which was the lowest reported use. Among the 1286 (25%) respondents who reported using the Seha app, only 988 (77%) answered questions related to how frequently they used the app and the most frequent service used in the Seha app. Out of the 988 respondents, 422 (43%) reported using Seha occasionally; 576 (58%) reported doctor consultations as the most frequently used service through the Seha app; 697 (70%) had never used a Smart Seha service; and 652 (66%) reported using the consult-a-doctor service. Out of 988 respondents, 463 (47%) reported using the health check service through the Seha app (Table 3).
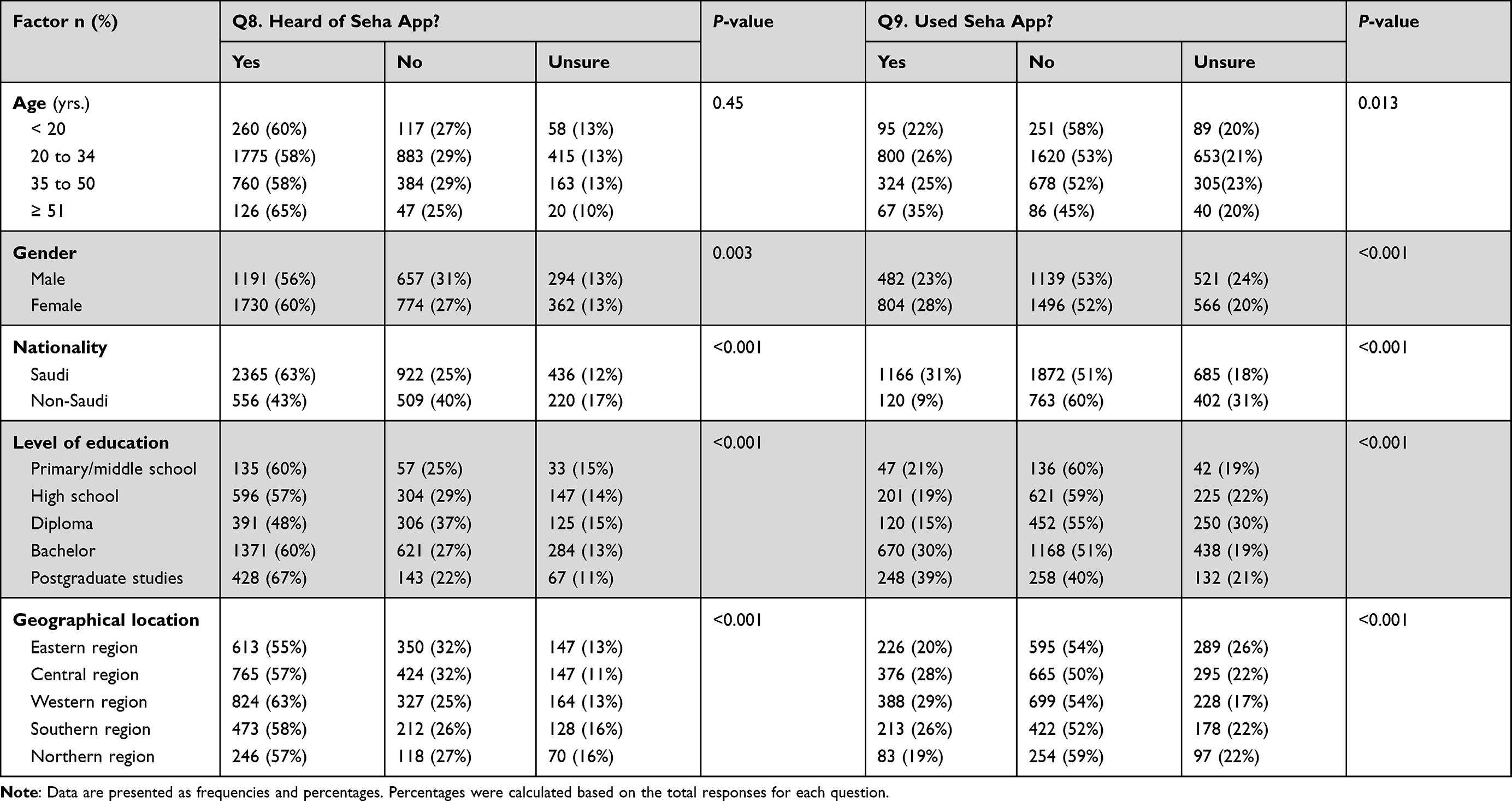 |
Table 2 Association of Demographic Variables with the Awareness and Utilization of the Seha App (n=5008) |
 |
Table 3 The Frequency and Percentage of Utilization of the Seha App Services (N= 988) |
Satisfaction with the Seha App
Among the 1286 (25%) respondents who reported using the Seha app, 988 (77%) answered all questions on satisfaction with the Seha app. The study showed that out of 988 respondents, 212 (31%) (strongly agree = [120: 12%], agree = [192: 19%]) agreed with the fact that the Smart Seha service answers were accurate and related to the condition. Out of 988 respondents, only 221 (22%) reported their satisfaction with the Smart Seha service provided (very satisfied = [53: 5%], satisfied = [168: 17%]). Out of 988 respondents, 431 (44%) reported their satisfaction with the health check service of the Seha app.
Table 4 is composed of nine multiple-choice questions regarding the usefulness, satisfaction, the ease of use of the Seha app services provided, and if respondents would recommend the app to anyone seeking medical care services. Out of 988 respondents, 402 (41%) or 471 (48%) of the respondents strongly agreed or agreed that the Seha app was easy to use, with 18 (2%) disagreeing. Moreover, out of 988 respondents, 538 (54%) strongly agreed and 343 (35%) agreed that they would recommend the app to others, with only 16 (2%) disagreeing.
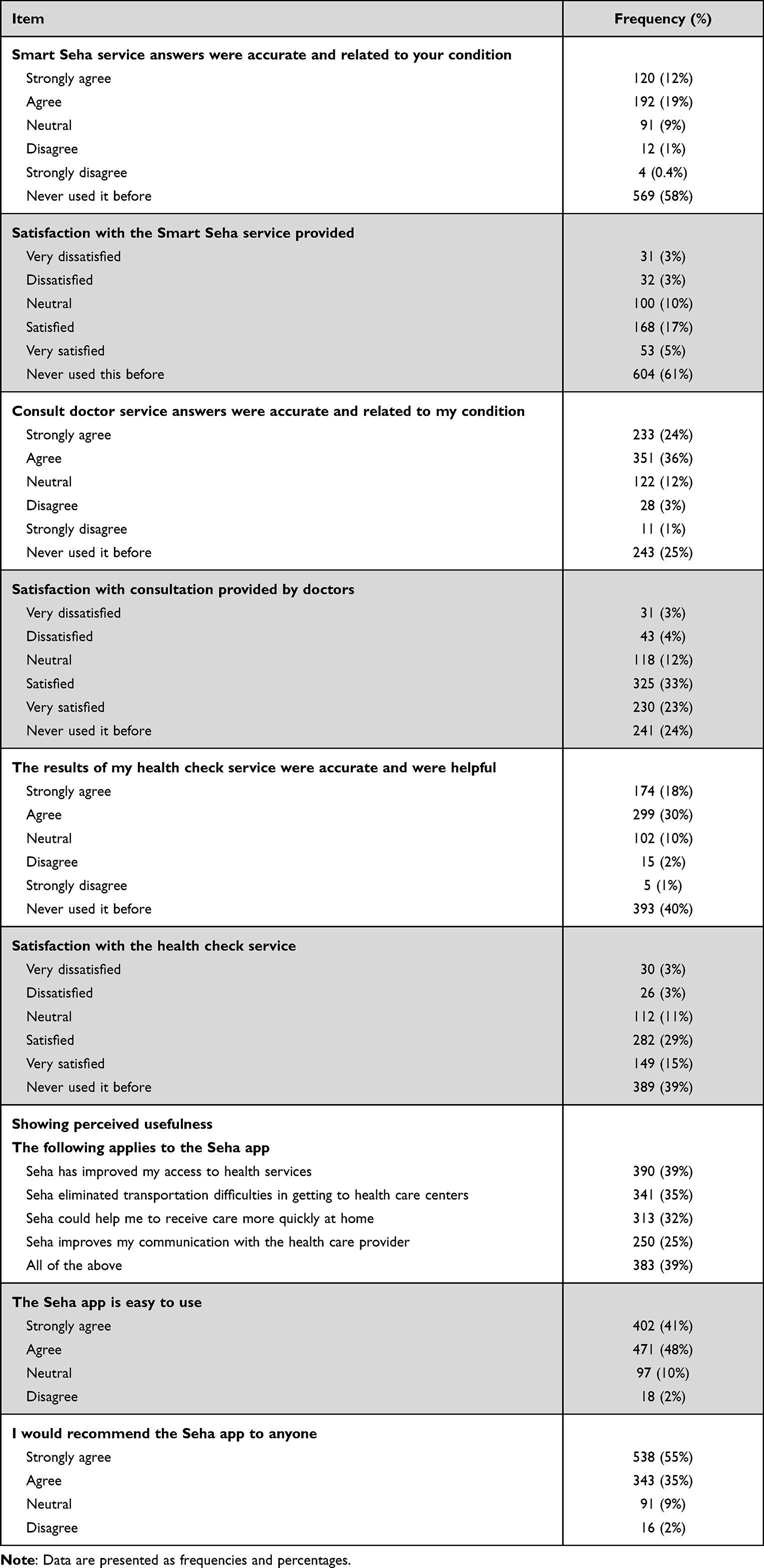 |
Table 4 Satisfaction with Seha App (N= 988) |
Respondents’ Usage of Other E-Health Apps
Respondents were asked about the most popular mobile health apps introduced by the Saudi Arabian MOH. Out of 5008 respondents, 4464 (89%) responded to this question. Out of 4464 respondents, 2170 (48%) reported using the Tawakkalna app, followed by the Tetamman app 1401 (31%), the Mawid app 1361 (30%), and the Tabaud app 1027 (23%) (Figure 1).
 |
Figure 1 Percentage of users per app(s) affiliated with the ministry of health (n =4464). |
Barriers or Limitations to Using of the Seha App
The most common barriers or limitations to using the Seha app are shown in Figure 2. From 4501 (90%) respondents who provided answers. We have classified the barriers into 10 main categories identified below. Out of 4501 respondents, 1556 (35%) reported that a lack of knowledge about the app and its benefits was the most common barrier or limitation, followed by the app not being linked to the respondents’ medical records 813 (18%), lack of awareness 761 (17%), lack of trust 508 (11%), slow app performance 485 (11%), limited or lack of internet access 447 (10%), resistance to change 437 (10%), privacy and confidentiality 418 (9%), and technical issues 417 (9%).
 |
Figure 2 The most common barriers or limitations of using the Seha app (n =4501). |
Discussion
Our study examined Seha app services, one of the primary sources of e-healthcare delivery in Saudi Arabia, from a large-scale public consumer perspective. We found that the most common device used to access the internet is the smartphone. More than half of respondents heard of the Seha app; however, the utilization was quite low, which could be from a lack of knowledge about the app and its benefits. Higher utilization was found in the western region, older adults, females, and those with postgraduate degrees. Among users, doctor consultation was the most utilized service in the Seha app. The majority of users agreed that the answers provided by all Seha services were accurate and related to their conditions and were satisfied with the services provided by the app’s services. Seha was easy to use and most respondents would recommend the app to others. For respondents who reported not using the Seha app, the Tawakkalna app was the most commonly utilized healthcare app provided by the MOH.
Our findings show that gender, nationality, and the level of education had a significant relationship with the utilization patterns of the Seha app. Our study results are also consistent with a previous study conducted in the United States, which showed that people with less education are less likely to use telemedicine.16 Therefore, the MOH should promotes public awareness especially for those with less education. Female users accessed the Seha app more often than males (60% vs 56%). This emphasizes the psychological differences between genders regarding the adoption of telemedicine and the motivation to use it, which has been discussed in previous literature.17,18
The results obtained from chi-squares showed a higher pattern of utilization of the Seha app in general compared with previous researches,6,19 which may be due to easiness of use and a higher level of trust as these were indicators of higher acceptance in previous studies.20,21 This is a considerable indicator of the improvement of digital technology adaptation against demographic barriers identified in previous research on the Seha app.6,19 Also, the public’s experience, preferences, and perceptions of the services have improved compared to previously published cross-sectional studies.22,23 This could be attributed to the awareness raised by companies, the government, individuals, and social media about health digital technology, such as Seha and other mobile health apps.24,25
Another interesting finding is the public understanding of the services provided by the Seha mobile app. In line with previous evidence,26 online doctor consultation was the most frequently used service through the app, followed by health checks, and Smart Seha (58%, 32%, and 10%), respectively. There is a likely chance that the level of trust in online consultations among the public in Saudi Arabia might be greatly impacted by the Covid-19 pandemic because people were instructed to stay at home and use digital technology to receive non-emergency care.12,25,27
The utilization patterns of the Seha mobile app and other health mobile apps has increased for several reasons including the continuous development of these apps led by the MOH and the Saudi Data and Artificial Intelligence Authority to achieve the MOH’s target goals for “Vision 2030,” namely, to make mobile apps reliable, and to improve the adoption and utilization of the technology, and to enable sustained access to telemedicine and high-quality healthcare services.28 Another reason could be due to the readiness of the internet network and the availability of professional support teams that were not available when the app launched in 2018.29 Both contributed to minimizing the gap in the factors affecting Seha’s usability.
Also, there is a supportive, high-quality internet network infrastructure (5G internet connection) in all geographical areas in Saudi Arabia as the government has prioritized telemedicine services in the local healthcare official, which has contributed to the increased utilization patterns of the Seha app. This is evident in the higher percentages of valid responses from all respondents in all geographical areas and is an indicator that a good internet infrastructure contributes to the utilization of health apps. Technical problems related to network and/or mobile apps are a common barrier and are mostly associated with low-level utilization and satisfaction.6 Reports indicated that the current year had an increased number of mobile health apps users. This could be due to the MOH’s initiatives to accelerate the digital health transformation and empowerment by developing and sustaining high-quality telemedicine services.29–32
In this study, we noticed an increase in the user’s satisfaction with the services provided in the app. This is reflected in the frequency of its use, and it has promising implications for other health apps. However, we only explored consumer satisfaction with one mobile app; consumer satisfaction with other mobile health apps and telephone line services, such as 973, requires further research.
Nevertheless, there are many opportunities to develop and sustain the usability of mobile health apps. One of them is exploring behaviors and attitudes on a large scale using advanced research methodologies, such as randomized clinical trials and qualitative research. The current body of literature mostly explores cross-sectional data in subjective instruments (such as a self-reporting questionnaire). More objective instruments are needed to explore actual usability, and future research must focus on analyzing real-time data and should use machine learning and modeling analysis, as well as artificial intelligence, to explore the patterns of use and consumer behavior regarding mobile health apps. Additionally, future research should consider patient involvement, cultural barriers, and advanced technologies in developing and designing future mobile health apps. Continued investigation should explore whether the scarcity of healthcare professionals and limited hospital capacity are key factors in the development of telemedicine services in Saudi Arabia.
Limitations
In the current research, the survey was distributed through social networks; therefore, the response rate was not available. We were not able to evaluate the satisfaction of healthcare providers and the workload of those who responded to Seha users, as professional scarcity and health system resources are current challenges to the quality of healthcare.33 Also, this survey was interrupted by the Covid-19 pandemic, which may have influenced the actual use of digital technology on a public scale. This may introduce observation bias in the current study. Additionally, cross-sectional methods were limited to identifying the key factors to evaluate the causality relationship between other covariates (such as device type, time spent on the mobile app, the strength of the network, and the frequency of use of the Seha app) and the behavior of the utilization patterns. Our sample is mainly Saudi citizens, and this might have impacted our results. Taken altogether, the results from this paper should be presented with caution, but the survey should guide future research on mobile health app usability.
Conclusion
The study shows that the utilization of Seha is particularly low from a lack of knowledge and is considered the most common barrier/limitation. Several factors—such as age, educational level, and knowledge about the Seha app—were predictors for higher utilization. Consulting a doctor was the most utilized service provided by the Seha app. Seha was considered easy to use, and the majority of respondents would recommend the Seha app to others.
Funding
This study did not receive any grants from funding agencies.
Disclosure
All authors declare no conflicts of interest for this work.
References
1. Mendonca V, Arthur VD, Beise J, Lee S, Lian B; Anastasia, Mshvidobadze aDY. Mena generation 2030: investing in children and youth today to secure a prosperous region tomorrow. Division of Data RaP; 2019: 110. Available from: https://www.unicef.org/mena/media/4141/file/MENA-Gen2030.pdf.
2. MOH vision of statistics and indicators; 2020. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/Indicator/Pages/Indicator-2020.aspx.
3. Khoja T, Rawaf S, Qidwai W, Rawaf D, Nanji K, Hamad A. Health care in gulf cooperation council countries: a review of challenges and opportunities. Cureus. 2017;9(8):e1586–e1586. doi:10.7759/cureus.1586
4. Institute of Medicine Committee on Evaluating Clinical Applications of T. The national academies collection: reports funded by national institutes of health. In: Field MJ, editor. Telemedicine: A Guide to Assessing Telecommunications in Health Care. National Academies Press (US) Copyright © 1996, National Academy of Sciences; 1996.
5. Russo JE, McCool RR, Davies L. VA telemedicine: an analysis of cost and time savings. Telemed J E Health. 2016;22(3):209–215. doi:10.1089/tmj.2015.0055
6. Alharbi A, Alzuwaed J, Qasem H. Evaluation of e-health (Seha) application: a cross-sectional study in Saudi Arabia. BMC Med Inform Decis Mak. 2021;21(1):1–9. doi:10.1186/s12911-021-01437-6
7. Polinski JM, Barker T, Gagliano N, Sussman A, Brennan TA, Shrank WH. Patients’ satisfaction with and preference for telehealth visits. J Gen Intern Med. 2016;31(3):269–275. doi:10.1007/s11606-015-3489-x
8. Uscher-Pines L, Mehrotra A. Analysis of teladoc use seems to indicate expanded access to care for patients without prior connection to a provider. Health Aff. 2014;33(2):258–264. doi:10.1377/hlthaff.2013.0989
9. Al Otaibi MN. Internet of Things (IoT) Saudi Arabia healthcare systems: state-of-the-art, future opportunities and open challenges. J Health Inform Dev Ctries. 2019;13(1). doi:10.1109/AECT47998.2020.9194213
10. Alaboudi A, Atkins A, Sharp B, Balkhair A, Alzahrani M, Sunbul T. Barriers and challenges in adopting Saudi telemedicine network: the perceptions of decision makers of healthcare facilities in Saudi Arabia. J Infect Public Health. 2016;9(6):725–733. doi:10.1016/j.jiph.2016.09.001
11. All the kingdom will be covered by telemedicine in two months. Ministry of Health-Kingdom of Saudi Arabia; 2021. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/news-2018-03-06-006.aspx.
12. Alanzi T. A review of mobile applications available in the app and google play stores used during the COVID-19 outbreak. J Multidiscip Healthc. 2021;14:45–57. doi:10.2147/jmdh.S285014
13. Health Education Activities; 2019. Available from: https://data.gov.sa/Data/en_AU/dataset/health-education-activities-moh-1440h-2019g/resource/9465d92f-1ded-4e7c-a1a9-05b131798ed0.
14. Degroot AMB, Dannenburg L, Vanhell JG. Forward and backward word translation by Bilinguals. J Mem Lang. 1994;33(5):600–629. doi:10.1006/jmla.1994.1029
15. Naing NN. Determination of sample size. Malays J Med Sci. 2003;10(2):84–86.
16. Coblentz WW. Council on Physical Therapy. J Am Med Assoc. 1937;108(20):1713–1715. doi:10.1001/jama.1937.02780200035009
17. Zhang X, Guo X, Lai K-H, Guo F, Li C. Understanding gender differences in m-health adoption: a modified theory of reasoned action model. Telemed E Health. 2014;20(1):39–46. doi:10.1089/tmj.2013.0092
18. Alam MZ, Hoque MR, Hu W, Barua Z. Factors influencing the adoption of mHealth services in a developing country: a patient-centric study. Int J Inf Manage. 2020;50:128–143. doi:10.1016/j.ijinfomgt.2019.04.016
19. Muzafar S, Jhanjhi N. Success stories of ICT implementation in Saudi Arabia. In: Employing Recent Technologies for Improved Digital Governance. IGI Global; 2020:151–163.
20. Kamal SA, Shafiq M, Kakria P. Investigating acceptance of telemedicine services through an extended technology acceptance model (TAM). Technol Soc. 2020;60:101212. doi:10.1016/j.techsoc.2019.101212
21. Sabbir MM, Islam M, Das S. Understanding the determinants of online pharmacy adoption: a two-staged SEM-neural network analysis approach. J Sci Technol Policy Manag. 2021;12(4):666–687. doi:10.1108/JSTPM-07-2020-0108
22. Alshammari F. Perceptions, preferences and experiences of telemedicine among users of Information and communication technology in Saudi Arabia. J Health Inform Dev Ctries. 2019;13(1):208–211.
23. ALOmari MO, Jenkins J. Exploring the attitudes of patients towards using the Seha application (Telehealth) in Saudi Arabia during the coronavirus epidemic. ABC J Adv Res. 2021;10(1):9–22. doi:10.18034/abcjar.v10i1.545
24. Aljohani N, Chandran D. The role of individuals and social awareness in adopting mobile health applications in Saudi Arabia: a review and preliminary findings.
25. Alghamdi SM, Alqahtani JS, Aldhahir AM. Current status of telehealth in Saudi Arabia during COVID-19. J Family Community Med. 2020;27(3):208. doi:10.4103/jfcm.JFCM_295_20
26. Fischer SH, Ray KN, Mehrotra A, Bloom EL, Uscher-Pines L. Prevalence and characteristics of telehealth utilization in the United States. JAMA Netw Open. 2020;3(10):e2022302–e2022302. doi:10.1001/jamanetworkopen.2020.22302
27. Sabbir MM, Taufique KMR, Nomi M. Telemedicine acceptance during the COVID-19 pandemic: user satisfaction and strategic healthcare marketing considerations. Health Mark Q. 2021;38(2–3):168–187. doi:10.1080/07359683.2021.1986988
28. Hassounah M, Raheel H, Alhefzi M. Digital response during the COVID-19 pandemic in Saudi Arabia. J Med Internet Res. 2020;22(9):e19338. doi:10.2196/19338
29. National digital transformation unit report; 2020. Available from: https://ndu.gov.sa/report/2020-bareport.pdf.
30. Alkhashan HI, Al-Khaldi YM, Hassanein MS, et al. Telephone consultation services in Saudi Arabia: utilization pattern and satisfaction among health care providers and consumers. J Health Inform Dev Ctries. 2020;14(2). doi:10.1101/2021.06.22.21259347
31. ElGibreen HAA. Health transformation in Saudi Arabia via connected health technologies. In: Technology and Global Public Health. Springer; 2020:83–99.
32. Rahman R, Al-Borie HM. Strengthening the Saudi Arabian healthcare system: role of vision 2030. Int J Healthc Manag. 2020;14:1–9.
33. Hoque AMA. Patient acceptance of e-health services in Saudi Arabia: an integrative perspective. Telemed E Health. 2019;25(9):847–852. doi:10.1089/tmj.2018.0107
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.