Back to Journals » Journal of Inflammation Research » Volume 18
Current Insights and Future Perspectives for the Use of Serological Biomarkers in Polymyalgia Rheumatica
Authors Harkins P ![]() , Cowley S, Conway R
, Cowley S, Conway R ![]()
Received 5 August 2025
Accepted for publication 2 November 2025
Published 10 November 2025 Volume 2025:18 Pages 15657—15670
DOI https://doi.org/10.2147/JIR.S558175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Shouya Feng
Patricia Harkins,1,2 Sharon Cowley,2,3 Richard Conway1,2
1Department of Rheumatology, St. James Hospital, Dublin, Ireland; 2School of Medicine, Trinity College Dublin, Dublin, Ireland; 3Department of Rheumatology, Tallaght University Hospital, Dublin, Ireland
Correspondence: Patricia Harkins, Department of Rheumatology, St. James Hospital, Dublin, Ireland, Email [email protected]
Abstract: There is currently no gold standard diagnostic test or validated serological biomarker to monitor disease activity or inform disease prognostication in isolated Polymyalgia Rheumatica (PMR). This presents significant challenges as the diagnosis of PMR is often complicated by multiple disease mimics, and the disease course remains highly variable, with no way to predict who will experience multiple disease relapses and high cumulative glucocorticoid burden. Furthermore, with the expansion of the therapeutic armamentarium of PMR, it is evident that our current one size fits all management strategy is no longer sufficient. In this narrative review, we summarise recent studies evaluating serological biomarkers for the diagnosis and prognostication of PMR, as well as their roles in disease activity monitoring and in identifying concomitant giant cell arteritis. We discuss their limitations, and explore barriers to their clinical translation, and finally highlight key directions for future research studies.
Keywords: biomarker, polymyalgia rheumatica, giant cell arteritis, cytokines
Introduction
Polymyalgia Rheumatica (PMR), one of the most common inflammatory rheumatic disorders of those aged 50 years and above, is typified by early morning stiffness and debilitating pain which has a predilection for the shoulder and pelvic girdle.1,2
The diagnosis of PMR is complex and challenging, with no definitive diagnostic test, many disease mimics and a marked heterogeneity in disease presentation.3–5
PMR can occur in isolation, so called “isolated PMR”, or in association with giant cell arteritis (GCA), a granulomatous vasculitis of medium and large calibre arteries.
The identification of GCA in those with PMR introduces a further layer of diagnostic complexity, especially concerning the identification of extracranial involvement (large vessel (LV) – GCA) where the clinical signs and symptomatology are often non- specific.
Although, isolated PMR has no direct impact on mortality or survival, it can have a detrimental impact on an individual’s health-related quality of life and is a source of much disability.6–9 Moreover, the ubiquitous use of glucocorticoids (GCs) in its management renders those with PMR susceptible to additional morbidity and unfavourable effects, especially in the significant proportion who require prolonged treatment, which is up to 40% of patients four years on from diagnosis.10–12 One of the key contributors to such prolonged GC use is disease relapse, with up to 50% of patients experiencing at least one relapse during attempted GC tapering.13 Research on GC-sparing agents has massively expanded in recent years, and the FDA approval of the interleukin-6 (IL-6) receptor antagonist, sarilumab, in refractory PMR, heralds a new era in PMR management.14 However, whilst these advancements are exciting, they also highlight significant deficiencies in our current management of those with PMR. The disease course of isolated PMR can be highly heterogenous, with the likelihood of relapses and adverse events unpredictable in frequency and severity between individual patients. At present, we have no accurate means of patient stratification from disease outset, to identify those patients at greatest risk for relapse who may require closer follow-up, and necessitate the earlier instigation of a GC-sparing therapy. Such a personalised and tailored approach to patient care is imperative in PMR, especially considering the typically older, and already more vulnerable nature of this patient cohort, with increased baseline frailty and comorbidity.4,6
Moreover, the introduction of IL-6 receptor antagonists into the management algorithm, and their associated neutralisation of the commonly employed acute phase reactants, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), further emphasise the limitations of our current methods of disease activity monitoring and underscores the need for biomarkers which are independent of the IL-6 pathway.
Therefore, there is a significant impetus to develop novel biomarkers to aid diagnosis, monitor disease activity, aid the identification of a concomitant GCA and facilitate disease prognostication in order to inform management decisions in those with isolated PMR. The use of IL-6 receptor antagonists further underscores the need for new serological biomarkers that are less dependent on the IL-6 axis.
For this narrative review, relevant English language studies were identified through searches of MEDLINE, EMBASE, Scopus and google scholar databases to summarise the specific roles of serological biomarkers investigated in isolated PMR. We also examine their limitations, discuss barriers to clinical translation and highlight key directions for future research.
Serological Biomarkers in PMR Diagnosis
The lack of a gold standard diagnostic test in PMR and the marked heterogeneity in disease presentation represents a significant diagnostic challenge for many clinicians. The vast number of disease mimics of PMR, including inflammatory arthropathies, rotator cuff tendinopathies, osteoarthritis, and paraneoplastic conditions, further compounds this diagnostic difficulty.4 Currently, the diagnosis of PMR is reliant upon the clinician assessment of often ambiguous signs and symptoms accompanied by an elevation in non-specific acute phase reactants namely erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Consequently, there is a significant risk of diagnostic delay and particularly misdiagnosis, which among other potentially devastating consequences, may result in unnecessary GC exposure, with its associated morbidity. Notably, even with specialist input, observational studies have shown that approximately one third of those initially diagnosed with PMR are reclassified during follow-up.15,16
Over the past decade there have been significant advancements in the application of imaging techniques including musculoskeletal ultrasound (MSUS), magnetic resonance imaging (MRI) and 18F-fluroodeoxyglucose positron emission tomography (FDG-PET) with/without computed tomography (CT) to aid the diagnosis of isolated PMR.17,18 Currently, there is no consensus on the optimal imaging modality. Bilateral subacromial-subdeltoid bursitis is the characteristic MSUS finding in PMR, however its diagnostic performance is suboptimal, with a reported sensitivity of 66% and specificity of 89%.19 Moreover, although safe, relatively inexpensive and widely accepted and tolerated, MSUS is highly operator dependent and requires intense training and expertise and so its routine use is limited in many rheumatology centres. MRI and FDG-PET-CT have each demonstrated superior sensitivity and specificity to US for the diagnosis of PMR.20–23 However, an inherent barrier to their routine implementation in clinical practice is their constrained accessibility and increased cost. Moreover, the use of FDG-PET-CT involves exposure to ionising radiation, and results can be affected by GC therapy.24
Given these limitations, relying solely on imaging for PMR diagnosis, is impractical and insufficient for clinical practice and so there is a significant unmet need to identify accurate and readily accessible serological biomarkers (Table 1).
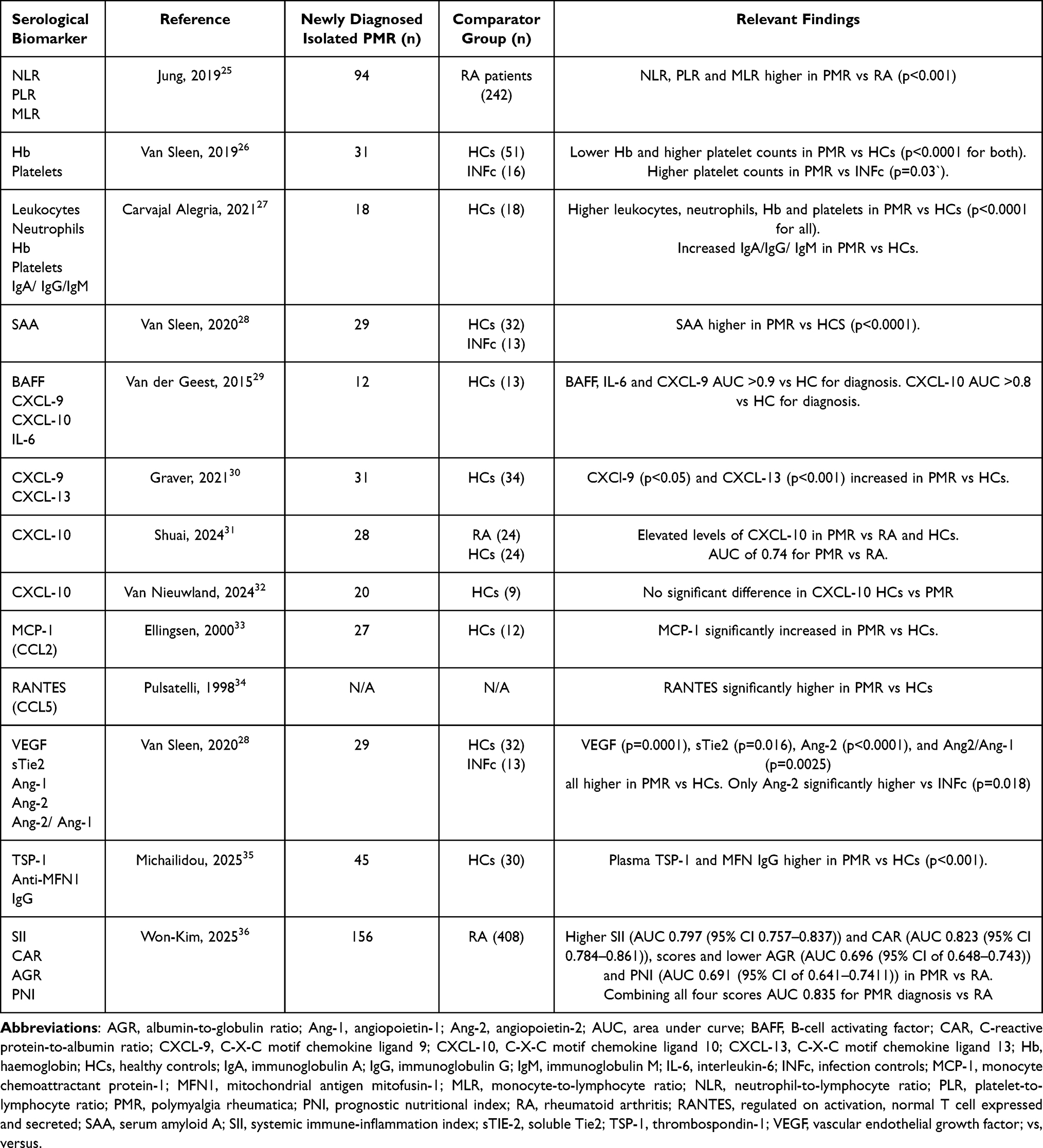 |
Table 1 Overview of Relevant Serological Biomarkers Studied in the Diagnosis of PMR |
Routine Laboratory Parameters
Various components of the complete blood count have been evaluated for their potential diagnostic role in PMR.
A Dutch cohort of 31 pre-treatment PMR patients, demonstrated significantly lower haemoglobin (Hb) levels (p<0.001) and significantly higher platelet counts (p<0.001) compared to healthy controls (HCs).26 When then compared with infection controls, platelet counts remained significantly higher in those with PMR (p=0.033), however, no significant difference in Hb levels was observed.26 These findings underscore the need to carefully select a comparator group that accurately reflects the future clinical context in which the potential biomarker will be used.
Similarly, a French cohort of 18 untreated PMR patients had significantly higher serum levels of leukocytes (p<0.001), neutrophils (p<0.001) and platelets (p<0.001), with decreased Hb (p<0.001) levels, compared with 18 age- and sex-matched HCs.27 The untreated PMR patients also demonstrated increased levels of serum gamma-globulins (immunoglobulin (Ig) – A,- G and -M) (12.1±0.6g/l) compared to matched HCs (8.8±0.8g/l).27 Interestingly, when comparing a cohort of PMR patients (n=94) to a cohort of patients with rheumatoid arthritis (RA) (n=242), the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR) were all significantly higher in patients with PMR (p<0.001), and correlated with CRP.25
As previously mentioned, the acute phase reactants, CRP and ESR are the most commonly employed serological markers to aid PMR diagnosis. However, the published literature on their efficacy and reliability is inconsistent owing largely to their non-specific nature, with alternative infectious, inflammatory and neoplastic conditions also resulting in their elevation. Moreover, normal ESR and CRP levels have been observed in up to 14% of patients at the time of diagnosis.37–40 However, these studies have a number of limitations including their retrospective design and the heterogeneity of diagnostic criteria applied. Nonetheless, the presence of an elevated ESR and/or CRP is a prerequisite in the most commonly employed PMR classification criteria.41
Increased levels of serum Amyloid A (SAA), another acute phase reactant, was demonstrated to be significantly higher in PMR patients versus HCs (p<0.001), however there was no significant difference when compared with infection controls.28
Cytokines, Chemokines and Other Proteins
Interleukin-6 (IL-6) is considered a key pathogenic molecule in isolated PMR, and therefore, unsurprisingly, its serum levels are significantly higher in those with untreated isolated PMR compared with HCs.26,28,29,42,43 However, a noteworthy finding, was the absence of a statistically significant difference in IL-6 levels between individuals newly diagnosed with PMR and a comparator infection control group.26 This suggests a lack of specificity, limiting its clinical utility as a future independent diagnostic biomarker.
In addition to IL-6, van der Geest et al, demonstrated the potential utility of the serum B-cell activating factor (BAFF), C-X-C Motif Chemokine Ligand (CXCL)- 9 and CXCL-10 in the diagnosis of PMR.29 The pathogenic role of B-cells is an emerging focus of research, supported by a growing body of evidence of a disrupted B cell homeostasis in individuals with PMR.44,45 B-cells express multiple chemokine receptors on their surface, facilitating their migration in response to several chemokines such as CXCL −9,-10 and −13, ultimately propagating systemic inflammation.46,47 BAFF is a potent B cell survival factor. Both BAFF and CXCL-9 demonstrated excellent discriminatory ability compared to HCs, with the area under the curve (AUC) values exceeding 0.9 on receiver operating characteristic curve (ROC) analysis.29 CXCL-10 also showed good diagnostic accuracy in PMR when compared to HCs, with an AUC greater than 0.8.29 These findings were confirmed in another study where serum CXCL-9 levels, in addition to CXCL-13 levels, were significantly increased in treatment naïve PMR patients (n=31) versus HCs.30 Two recent studies have reported conflicting findings regarding CXCL-10 expression at diagnosis: one observed elevated levels in PMR patients compared to HCs and RA controls,31 while the other study found no significant difference between PMR and HCs.32
Two additional chemokines; plasma monocyte chemoattractant protein-1 (MCP-1/ CCL2) and Regulated on Activation, Normal T cell expressed and Secreted (RANTES/ CCL5) were significantly higher in untreated PMR patients compared with HCs, however, they did not correlate with disease activity (Table 1, Figure 1). 33,34 Both of these studies were undertaken over twenty years ago, and the findings have not yet been validated.
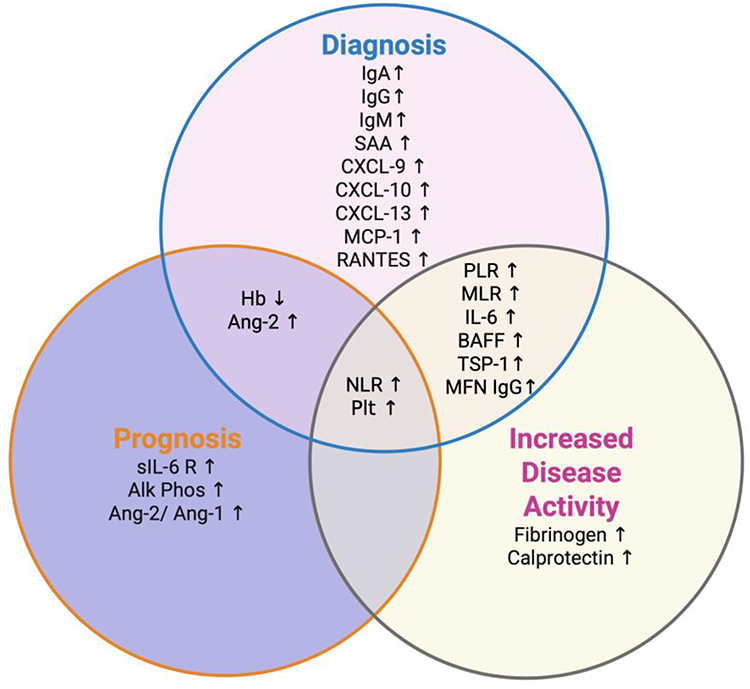 |
Figure 1 Venn diagram illustrating the current evidence on the utility of serological biomarkers in Polymyalgia Rheumatica for diagnosis, prognostication, and assessment of increased disease activity.The diagnostic biomarkers (pink circle) represent those with demonstrated utility in identifying isolated PMR. The prognostic biomarkers (purple circle) are associated with worse disease outcomes, including higher cumulative glucocorticoid exposure, delayed time to drug free remission and increased relapse rates. The disease activity biomarkers (yellow circle) reflect increased disease activity, including disease relapse, relative to a clinically defined remission state. Overlapping regions represent biomarkers with multiple clinical applications. Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio (MLR); Hb, haemoglobin; Plt, Platelets; Alk phos, Alkaline phosphatase; SAA, Serum Amyloid A; IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobin M; IL-6, interleukin-6; sIL-6 R, soluble interleukin-6 receptor; sTIE-2, soluble Tie2; ang-1, angiopoietin-1; ang-2, angiopoietin-2; BAFF, B-cell activating factor (BAFF); CXCL-9, C-X-C Motif Chemokine Ligand 9; CXCL-10, C-X-C Motif Chemokine Ligand 10; CXCL-13, C-X-C Motif Chemokine Ligand 13; IL-6, Interleukin-6; MCP-1, monocyte chemoattractant protein-1; RANTES, Regulated on Activation, Normal T cell expressed and Secreted; TSP-1, thrombospondin-1; MFN1, mitochondrial antigen mitofusin-1; ↑, increased; ↓, decreased. |
van Sleen et al, evaluated vascular angiogenesis biomarkers including vascular endothelial growth factor (VEGF), soluble Tie2 (sTIE-2), angiopoietin-1 (ang-1) and angiopoietin-2 (ang-2) in 29 newly diagnosed treatment naïve isolated PMR patients (Table 1). 28 Similar to prior studies,48,49 VEGF was elevated compared to HCs (p< 0.001).28 Furthermore, the other evaluated markers of angiogenesis, with the exception of ang-1, demonstrated statistically significant higher levels versus controls including sTIE-2 (p=0.016), ang-2 (p<0.0001) and ang-2/ ang-1 ratio (p=0.0025).28
Recently, the pathogenic role of mitochondrial-mediated platelet activation in a Swedish cohort of 45 isolated PMR patients has been reported. The potential utility for the anti-mitochondrial antibody directed towards specific mitochondrial antigen mitofusin-1 (MFN-1) in the diagnosis of isolated PMR was demonstrated, with plasma levels of anti-MFN1 IgG antibodies significantly higher than in HCs (p<0.01).35 A significantly higher level of thrombospondin-1 (TSP-1), a marker of platelet activation, in PMR vs HCs (p<0.001) was also demonstrated.35
Composite Laboratory Scores
Another newly published study, involving 156 PMR patients, and 408 RA controls, evaluated laboratory-based inflammatory scores – including the systemic immune-inflammation index (SII), C-reactive protein-to-albumin ratio (CAR), albumin-to-globulin ratio (AGR) and prognostic nutritional index (PNI) as diagnostic tools for PMR (Table 1). 36
Patients with PMR exhibited higher CAR (AUC 0.823, 95% CI 0.784–0.861) and SII (AUC 0.797, 95% CI 0.757–0.837) scores and lower AGR (AUC 0.696, 95% CI 0.648–0.743) and PNI (AUC 0.691, 95% CI 0.641–0.7411) values than those with RA.36 Moreover, combining these scores improved the diagnostic ability, with an AUC of approximately 0.835.36
Serological Biomarkers in Monitoring Disease Activity in PMR
The recently published treat-to-target recommendations for GCA and PMR suggest regular monitoring of those with PMR, as frequently as every 1–4 weeks until remission is achieved, in order to ensure optimal patient outcomes and maximise health-related quality of life.50 However, a significant unmet need in monitoring patients with isolated PMR is the lack of a practical and specific biomarker that accurately correlates with disease activity. As previously discussed, the presentation of PMR can be heterogeneous with multiple disease mimics which not only limit the diagnostic process but can also impact the effective monitoring of active disease during follow-up. Accurate identification of disease relapse is essential for clinicians to prevent unnecessary exposure to potentially harmful immunosuppressive agents in the absence of a disease relapse, while also ensuring timely intervention where appropriate to avoid suboptimal disease control.
A major obstacle in the assessment of biomarkers of disease activity in PMR is the lack of an international consensus on the definition of disease relapse and remission. This has resulted in a marked heterogeneity in the definitions used to define disease activity in clinical studies,51 which results in significant limitations not only in the interpretation of findings but also in the ability to compare results across studies in the future.
Current monitoring strategies in PMR consist primarily of a clinician-based assessment and the evaluation of traditional inflammatory markers, namely ESR and CRP. This strategy is inherently problematic considering that symptoms may be non-specific during disease relapse, and normal CRP or ESR values have been observed in up to 17% and 27% of relapses, respectively.40 Moreover, this approach has limited value in those prescribed IL-6 antagonists with their associated normalisation of both ESR and CRP.
There is, therefore, an urgent need to develop novel biomarkers for monitoring disease activity. However, compared to other clinical applications, there is a distinct paucity of studies evaluating the utility of serological biomarkers for disease monitoring in isolated PMR (Box 1).
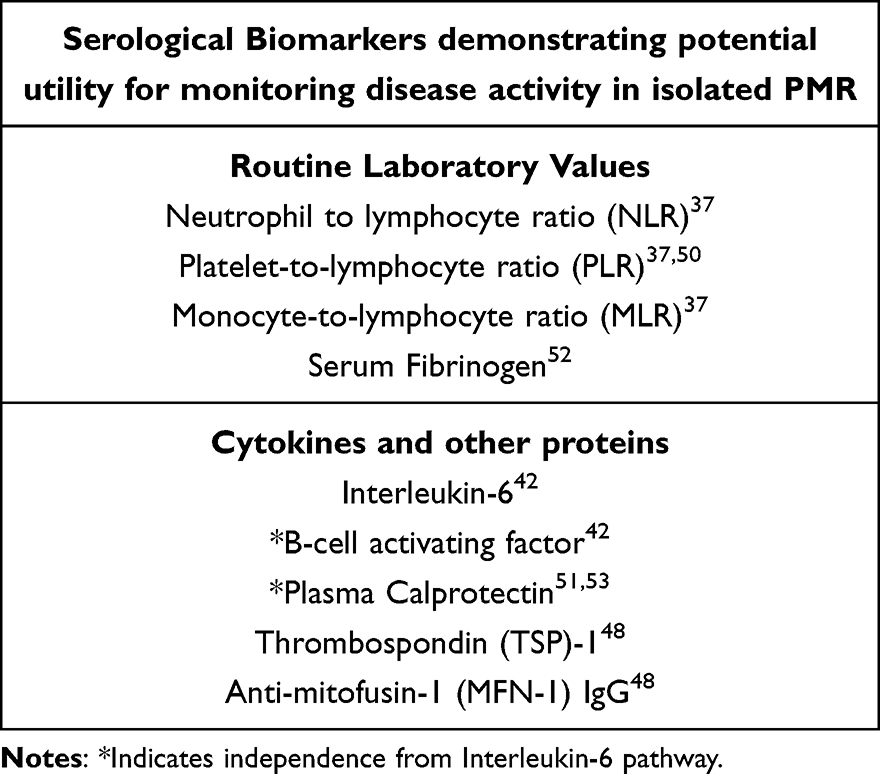 |
Box 1 Serological Biomarkers Demonstrating Potential Utility for Monitoring Disease Activity in Isolated PMR |
Routine Laboratory Markers
Two studies, using differing definitions of disease activity, and cut-off scores, have assessed components of the complete blood count, namely NLR, PLR and MLR to assess disease activity.25,53 Jung et al, demonstrated a significant decrease in NLR (p<0.001), PLR (p<0.001) and MLR (p<0.001) upon resolution of disease activity.25 Owens et al, also demonstrated the correlation of PLR with disease activity (defined by the mean PMR-activity score (PMR-AS)) during follow-up (OR 15.6; 95% CI 2.7–28.2), and there was also a trend towards significance for mean NLR and mean PMR-AS (OR 10.1, 95% CI 0.9–21.3).53
A routinely available, acute phase soluble plasma protein, fibrinogen, has also been studied, and compared to both CRP and ESR, for its potential role in assessing disease activity in PMR, where it was found to be more specific than either ESR or CRP for the detection of response to treatment, with an overall sensitivity of 92% and specificity of 96% on ROC analysis.52 Moreover, values above the upper limit of normal for fibrinogen, CRP and ESR were associated with likelihood ratios of active disease of 20.53, 2.9 and 2.8 respectively (p<0.001).52 This most certainly suggests a potential utility of fibrinogen, perhaps in combination with CRP and ESR, to aid the detection of disease activity in isolated PMR, however, since this study in 2013 these findings have not been validated.
Whilst evaluating the role of immune complex-mediated neutrophil activation in the pathogenesis of PMR, Michailidou et al, showed the significant decrease in plasma calprotectin after GC therapy (p<0.001).54 This paralleled with a previous finding where plasma calprotectin was significantly decreased after the start of treatment with GCs, and correlated with the daily dose of prednisolone (r=0.36; p<0.01).55 The investigation of plasma calprotectin is particularly notable, given its independence from the IL-6 pathway, and thus potential utility as a biomarker of disease activity for those on IL-6 receptor antagonists.
Cytokines, Chemokines and Other Proteins
Recently, the association of anti-MFN1 IgG antibodies and TSP-1 with disease activity in a Swedish cohort of isolated PMR patients was reported.35 With GC therapy, the levels of anti-MFN1 IgG antibody (p<0.001), TSP-1 (p=0.023) and platelet count (p=0.021) dropped significantly.35
Upon GC induced remission, a significant decrease in serum BAFF and IL-6 was demonstrated in a Dutch cohort of PMR patients however no significant modulation of CXCL9, CXCL10, IL-10 or sIL-2R was observed.29 Similar to calprotectin, given its independence of the IL-6 pathway, serum BAFF has a potential utility in monitoring disease activity in those receiving IL-6 receptor antagonists. Further studies are required to clarify their role in the therapeutic setting.
Serological Biomarkers in PMR Disease Prognostication
Contrary to the previously held perception of isolated PMR as a benign, GC responsive disease, a 2022 systematic literature review and meta-analysis of international studies by Floris et al, confirmed the contrasting true reality of the disease trajectory.56 The pooled prevalence of those still taking GCs at 1,2 and 5 years was 77% (95% CI 71–83%), 51% (95% CI 41–61%) and 25% (95% CI 15–36%) respectively.56 Additionally, the pooled proportion of those experiencing at least one relapse during the first year of treatment was 43% (95% CI 29–56%).56 The disease course for individual patients is heterogenous, and unfortunately, we have no way to prognosticate which patients will experience recurrent relapses, GC dependence and overall worse disease outcomes.
As the therapeutic armamentarium of PMR expands, with an increasing number of GC-sparing therapies under evaluation,57 the ability to predict disease course and risk stratify patients from disease outset is an area garnering increased scientific attention. Such a prognostic biomarker holds promise for enabling personalised treatment from the time of diagnosis, improving disease control whilst also minimising unnecessary exposure to high cumulative GC burdens with their associated morbidity.
Routine Laboratory Parameters
Van Sleen et al, demonstrated that a baseline pre-treatment Hb level higher than the median, predicted a shorter time to GC-free remission (p=0.025).26 An elevated baseline platelet count was also associated with an adverse prognosis.58 Whilst Jung et al, failed to demonstrate a prognostic role of NLR or PLR in predicting disease relapse,25 Owens et al, reported baseline NLR to be a statistically significant predictor of GC-resistant PMR (OR 14.01; 95% CI 1.49–278.06).53 Notably, a trend toward significance for baseline PLR (OR 5.02; 0.49–71.54) in predicting GC-resistance was also observed.53
There are conflicting results in the literature regarding the utility of ESR and CRP in disease prognostication and predicting glucocorticoid remission in PMR. This may be explained by the varied timelines and inconsistent outcome definitions used in these studies. Higher baseline ESR levels have been associated with failure to achieve remission at 24 months (p=0.012),59 and prolonged GC requirement (p=0.041),28 with CRP also identified as an independent risk factor for disease relapse (OR 6.296, p=0.047).60 However, studies have also reported no prognostic value for baseline CRP and ESR.26,61,62 The trajectory of CRP values does however, suggest prognostic promise, with a normal CRP value (<0.5mg/dL) at 6 months from baseline independently associated with complete remission at 12 months (p=0.017) in one study,63 and the achievement of a CRP value <0.17mg/dL at 1 month from baseline associated with a higher probability of GC-free remission at 30 months in another study.64 Moreover, persistently elevated CRP values are also associated with an increased risk of disease relapse.65 Van Sleen et al, also demonstrated higher baseline levels of the acute phase reactant, SAA, were predictive of prolonged GC therapy (p=0.041).28
Another routinely available laboratory parameter – serum alkaline phosphatase – was recently evaluated in a small, retrospective study where a high initial serum alkaline phosphatase (≥225.0 U/I) was a significant predictor of future PMR relapse risk (OR 5.65; 95% CI 1.27, 25.20; p=0.02).62
Additionally, reflective of the new therapeutic strategies, and the subsequent evolving research agenda, a quicker response to the IL-6 antagonist, tocilizumab, was observed in isolated PMR patients with higher baseline gamma globulin levels.27
Cytokines and Other Proteins
Persistently elevated IL-6 levels, especially those that remain elevated throughout the entire first year of therapy were associated with an increased frequency of disease relapse.66 Moreover, higher baseline soluble IL-6 receptor (sIL-6R) levels significantly correlated with the number of subsequent relapses, and using multivariate analysis, the combination of high sIL-6R levels with low Hb values at baseline increased the risk of relapse 10.1 fold.67 Conversely, Van Sleen et al, failed to show an association between baseline serum IL-6 and long term GC requirement.28 However, they did demonstrate levels of ang-2 and the ratio of ang-2/ang-1 at baseline were higher in those who subsequently remained on GC therapy at 24 months versus those in GC remission, with ang-2 AUC 0.87 (p=0.0045) and ang-2/ang-1 ratio AUC 0.83 (p=0.013).28 Moreover, they also reported low serum VEGF levels (p=0.031) were more predictive of prolonged GC therapy.28
Serologica Biomarkers to Identify GCA in PMR
There is a well-established association of PMR with GCA, with both sharing many epidemiologic, immunological and clinical manifestations resulting in the recently proposed “GCA-PMR Spectrum Disease” (GPSD).68 Indeed, population-based studies have shown that 16 to 21% of those with PMR have, or will develop GCA.2 Moreover, subclinical GCA (GCA with no classical cranial or ischaemic symptoms) is reported to occur in 23–29% of those with clinically perceived isolated PMR.69
GCs form the cornerstone of management for both conditions, however, the dose used to treat isolated PMR is significantly lower than that required to treat GCA. Therefore, failure to detect GCA may result in failure to appropriately manage patients, with the potential for catastrophic consequences including ischaemic and vascular complications such as vision loss, inflammatory aneurysm formation and rupture with an associated increased mortality. Whilst, in clinical practice, the classical presentation of cranial (c-) GCA alerts clinicians to actively pursue a diagnosis of c-GCA, the often non-specific and heterogeneous symptoms of LV-GCA can result in its underdiagnosis. This is further complicated by the difficulty in detecting large vessel aortitis, with the use of non-irradiating ultrasound limited to the axillary arteries and supra-aortic trunks, and the majority of cases requiring either computed tomography (CT) angiography (CTA), magnetic resonance angiography (MRA) or PET-CT. These interventions are costly, and not readily available in every rheumatology centre. Therefore, there is a need to identify a method of stratifying the patients in whom GCA is more likely, and in whom further complementary examinations such as imaging and temporal artery biopsy are warranted.
Notably, whilst the early detection and management of GCA are imperative, the clinical implications of a concomitant subclinical vasculitis have yet to be established. It is an ongoing area of active research and indeed much interest and debate within the rheumatology community.70–73
Nevertheless, as mentioned GCA is frequently underdiagnosed in those with PMR and indeed is postulated to represent a leading cause of disease relapse and GC-resistance in PMR patients. To ensure timely diagnosis of GCA, limit associated morbidity and mortality, and facilitate the instigation of appropriate management early on, the identification of sensitive serological biomarkers to detect GCA in those presenting with PMR is an area of critical investigation (Table 2).
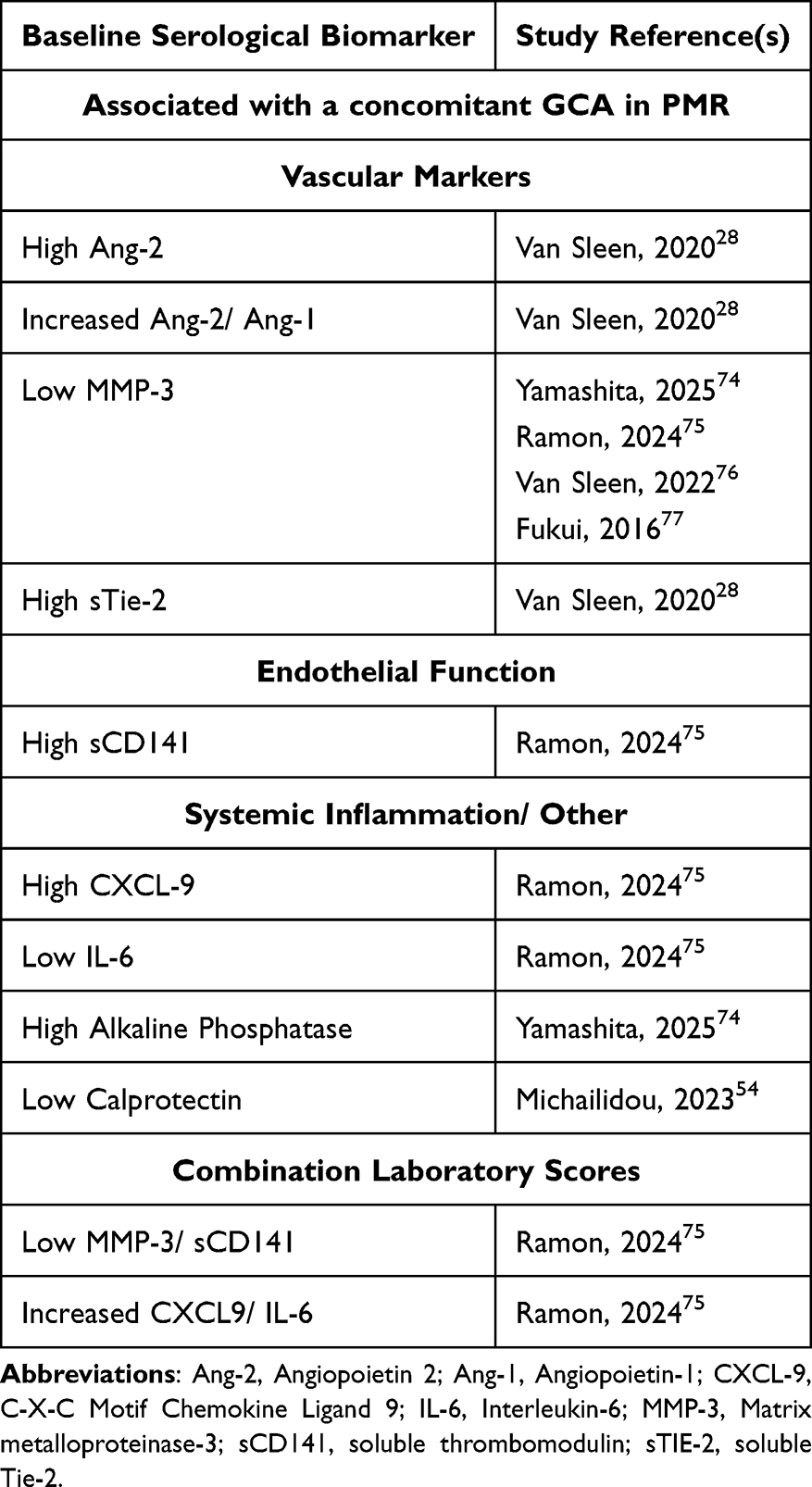 |
Table 2 Summary of Serological Biomarkers Demonstrating a Positive Association with Giant Cell Arteritis |
Routine Laboratory Parameters
Lower Hb (p=0.013), white blood count (p=0.007) and neutrophil counts (p=0.031) have been reported in those with subclinical GCA versus those with isolated PMR.78 A meta-analysis that included studies up until 2020, reported the association of elevated platelet counts (OR 1.51; CI 1.05–2.18) and subclinical GCA detected using FDG-PET-CT.69 The same meta-analysis failed to demonstrate any positive correlation between acute phase reactants, namely CRP and ESR, and the presence of subclinical GCA.69 The substantial heterogeneity in reported prevalence of subclinical GCA across the included PET studies (0–80%) should be noted however, underscoring methodological inconsistencies which may substantially limit the reliability and generalisability of these findings. Using US to detect subclinical vasculitis, a multicentre, international cohort study, also failed to demonstrate a statistically significant association between CRP and ESR levels and the presence of subclinical GCA.79 A further recent, retrospective study found no statistically significant association between CRP and ESR levels in a Belgian cohort with FDG-PET-CT confirmed subclinical vasculitis versus an isolated PMR cohort.78 However, two additional studies have reported the potential of a higher baseline ESR to distinguish those with and without GCA.28,76 There are several possible explanations for this inconsistency in findings, including the heterogeneous patient cohorts studied, the different imaging modalities employed and the varying definitions of subclinical vasculitis used across the studies.
Lower plasma calprotectin levels have been reported in those with PMR and GCA versus isolated PMR (p=0.014),54 and recently a higher median baseline alkaline phosphatase level was demonstrated in a Japanese cohort with PMR and GCA versus isolated PMR (OR 25.2, p=0.032).74
Vascular Markers
Serum vascular markers, including those implicated in vascular remodelling are gaining increased traction as potential biomarker candidates for this purpose (Table 2), owing to the logical assumption that the involvement of vessels in GCA will afford a distinguishing feature of GCA from PMR.
In particular high levels of serum ang-2, a protein involved in angiogenesis, have demonstrated promise as a marker for the presence of GCA in PMR, with an AUC of 0.90 in one study.28 Moreover, the ratio of ang-2/ang-1 also predicted the presence of GCA in PMR, with an AUC of 0.88 in one study (using a cut-off value of >0.051)28 and an AUC of 0.78 in another study (using a cut-off of >0.048).76
Matrix Metalloproteinases (MMP) play a key role in vascular remodelling and the destruction of cellular matrix proteins, inducing media destruction and internal elastic lamina fragmentation.80 The most promising, and consistently demonstrated finding is of a low serum level of MMP −3 as an excellent predictor of GCA in those with PMR.74–77 Endothelial cells also play a pivotal role in GCA pathogenesis by facilitating the recruitment of T cells via the vasa vasorum of the adventitia, where endothelial cells express adhesion molecules including intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1). However, no significant difference was observed in ICAM-1, or VCAM-1 levels in those with isolated PMR versus those with PMR/GCA overlap.75
Interestingly however, levels of soluble thrombomodulin (sCD141), a transmembrane protein expressed on the surface of endothelial cells that plays a key role in preventing inflammatory infiltration of the endothelium, were significantly higher in those with GCA/ PMR than isolated PMR with an AUC of 0.7 (p=0.002).75
Cytokines, Chemokines and Other Proteins
Low levels of serum IL-6 (p=0.004) and higher levels of serum CXCL-9 (p=0.002) have been associated with a concomitant GCA in PMR vs isolated PMR.75 Ramon et al, evaluated the utility of combinations of serological biomarkers to optimise the identification of GCA in PMR (Table 2). 75 Whilst, the AUC was <0.7 for sCD141, CXCL-9 and IL-6 when evaluated separately, the CXCL-9/ IL-6 ratio was significantly increased in those with GCA (p<0.001; cut-off >32.8, AUC 0.76), whilst the MMP-3/ sCD141 ratio was significantly lower in patients with GCA (p<0.001; cut-off <5.3, AUC 0.79).75 Finally, Ramon et al, reported both sCD141 and MMP-3/sCD141 ratio to have high diagnostic accuracy in subclinical GCA with an AUC of 0.81 (p=0.004) and 0.77, respectively (p=0.01).75 Future studies are warranted to validate these findings, and cut-off values.
Discussion/ Future Perspectives
Whilst many of the serological biomarkers described above provide promise (Figure 1), there is to date, insufficient evidence to warrant their incorporation into routine clinical practice.
Despite its high prevalence, PMR has been relatively underrepresented in studies exploring novel serological biomarkers. However, the past year has seen a noticeable rise in the publication of such studies,31,32,35,36,74,75 reflecting the increasing recognition of PMR as an important research priority.
Despite this, unfortunately the majority of studies to date are heterogenous, low powered observational studies employing differing definitions of disease activity, remission and relapse with varied follow-up duration. This lack of consistency hampers comparability, meta-analyses and ultimately their interpretation and future clinical application.
In order to elicit the translation of novel serological biomarkers into clinical practice, there are several considerations that must be incorporated into future studies. Whilst a randomised control trial (RCT) would be the gold standard study design to evaluate a novel serological biomarker, before undertaking this we need prospective, ideally multicentre and multinational studies that are adequately powered, with a sufficient follow-up duration and control for confounding variables. These will provide the preliminary data to then undertake validation studies and ultimately pursue more specific well designed RCTs.
In an effort to ensure homogeneity of such studies, there is an urgent need for an internationally accepted definition for PMR disease activity states including relapse and remission.
In the studies outlined throughout this article, the marked heterogeneity of reporting of study findings was apparent. Many studies failed to provide cut-off values for their findings and used varying statistical analyses. Whilst a statistically significant mean difference between individual biomarkers at different disease states or regarding specific outcomes fosters promise, there is no granularity to this finding. The use of ROC analysis providing an AUC with sensitivity and specificity values provides greater information on discriminatory ability and predictive performance and so, should be employed where possible. Moreover, to facilitate accurate analysis, it is of utmost importance that careful consideration is given to the choice of control group. HCs were the primary control group in the included studies, however, the comparator group should reflect those in whom the biomarker would have the most impact in differentiating clinically, such as those most likely to mimic PMR (eg late onset RA).
A further consideration is the choice of analyte measurement technique used, as this can significantly influence assay performance characteristics and consequently the interpretation of study findings - particularly for cytokines in the low concentration range. The two most commonly used methods in PMR research are single plex enzyme-linked immunosorbent assay (ELISA), which typically requires large sample volumes, and high throughput bead-based multiplex immunoassays such as Luminex. The Luminex platform offers the advantage of the simultaneous quantification of multiple analytes from a small sample volume, along with enhanced sensitivity and a broad dynamic range, albeit at the expense of higher cost, and reduced reproducibility across platforms.81 Importantly, differences in assay methodology can lead to variability in analyte cut-off values and lower detection limits, making it essential that all future studies clearly specify the assay technique employed and report relevant thresholds to ensure the reliability and comparability of results across studies.
Finally, there is an emerging focus on the evaluation of composite laboratory scores and serological ratio scores as biomarkers in isolated PMR, with positive associations thus far.36,75 This is an exciting avenue for future research and reflects how the future of biomarker research in PMR will likely not be dependent on an individual serological marker or disease parameter but instead involve an evidence based multi-modal approach.
Conclusion
Despite the significant need, to date there is no gold standard serological biomarker to aid diagnosis, assess disease activity or guide disease prognostication and stratification in those with isolated PMR.
Over the past five years, there has been a significant increase in published studies investigating the role of serological biomarkers in PMR, surpassing the total number published in the previous decade. This reflects not only the clinical need but also the growing momentum and renewed interest in biomarker research within PMR.
In particular, the development and application of composite laboratory scores is an emerging and promising area of future research. Despite this several key challenges persist in the evaluation and translational integration of novel serological biomarkers into clinical practice. Looking ahead, the successful implementation of biomarkers in PMR will likely depend on a comprehensive, multimodal approach.
Funding
No funding was obtained from any public, commercial or non-profit organisations for this article.
Disclosure
PH reports grant support from Johnson and Johnson and Novartis. SC reports grants from Novartis. RC reports being a member of speaker’s bureau for Janssen, Roche, Sanofi, Abbvie, Alfasigma, Fresenius Kabi, UCB, Viatris, Vifor; undertaking clinical trials funded by Abbvie, Novartis; receiving grant/research support from Janssen, Novartis, Celltrion, Nordic Pharma. The authors report no other conflicts of interest in this work.
References
1. Buttgereit F, Dejaco C, Matteson EL, Dasgupta B. Polymyalgia rheumatica and giant cell arteritis: a systematic review. JAMA. 2016;315(22):2442–2458. doi:10.1001/jama.2016.5444
2. Buttgereit F, Matteson EL, Dejaco C. Polymyalgia rheumatica and giant cell arteritis. JAMA. 2020;324(10):993–994. doi:10.1001/jama.2020.10155
3. Harkins P, McCann L, Harrington R, Cowley S, Kane D, Conway R. Polymyalgia rheumatica-an up-to-date review on diagnosis and management. Vessel Plus. 2024;8:14. doi:10.20517/2574-1209.2023.137
4. Cowley S, Harkins P, Kirby C, Conway R, Kane D. Real-world outcomes of a dedicated fast-track polymyalgia rheumatica clinic. Rheumatology. 2024;keae531.
5. Bond M, Dejaco C. Polymyalgia Rheumatica: Crafting the Future of a Simple (but Not Easy!) Clinical Syndrome. BMJ Publishing Group Ltd; 2024:271–273.
6. Sattui SE, Jannat-Khah D, Lally L, Lieber SB, Mandl LA, Spiera RF. Prevalence of frailty in patients with polymyalgia rheumatica and association with health-related quality of life, cognition and sarcopenia. Rheumatology. 2022;61(11):4455–4464. doi:10.1093/rheumatology/keac050
7. Leung JL, De Ross B, Gianoudis J, et al. More than pain and stiffness: persistent fatigue and sleep disturbance in polymyalgia rheumatica. J Rheumatol;2025. jrheum.2024–0980. doi:10.3899/jrheum.2024-0980
8. Twohig H, Mitchell C, Mallen C, Adebajo A, Mathers N. “I suddenly felt I’d aged”: a qualitative study of patient experiences of polymyalgia rheumatica (PMR). Patient Educ Couns. 2015;98(5):645–650. doi:10.1016/j.pec.2014.12.013
9. Mackie SL, Hughes R, Walsh M, et al. An impediment to living life”: why and how should we measure stiffness in polymyalgia rheumatica? PLoS One. 2015;10(5):e0126758. doi:10.1371/journal.pone.0126758
10. Ayoub WT, Franklin CM, Torretti D. Polymyalgia rheumatica Duration of therapy and long-term outcome. Am J Med. 1985;79(3):309–315.
11. Albrecht K, Huscher D, Buttgereit F, et al. Long-term glucocorticoid treatment in patients with polymyalgia rheumatica, giant cell arteritis, or both diseases: results from a national rheumatology database. Rheumatology International. 2018;38(4):569–577. doi:10.1007/s00296-017-3874-3
12. Hoes J, Jacobs J, Verstappen S, Bijlsma J, Van der Heijden G. Adverse events of low-to medium-dose oral glucocorticoids in inflammatory diseases: a meta-analysis. Ann Rheumatic Dis. 2009;68(12):1833–1838. doi:10.1136/ard.2008.100008
13. Weyand CM, Goronzy JJ. Giant-cell arteritis and polymyalgia rheumatica. N Engl J Med. 2014;371(1):50–57. doi:10.1056/NEJMcp1214825
14. Spiera RF, Unizony S, Warrington KJ, et al. Sarilumab for relapse of polymyalgia rheumatica during glucocorticoid taper. N Engl J Med. 2023;389(14):1263–1272. doi:10.1056/NEJMoa2303452
15. Donskov AO, Mackie SL, Hauge EM, et al. An international survey of current management practices for polymyalgia rheumatica by general practitioners and rheumatologists. Rheumatology. 2023;62(8):2797–2805. doi:10.1093/rheumatology/keac713
16. Caporali R, Montecucco C, Epis O, Bobbio-Pallavicini F, Maio T, Cimmino M. Presenting features of polymyalgia rheumatica (PMR) and rheumatoid arthritis with PMR-like onset: a prospective study. Ann Rheumatic Dis. 2001;60(11):1021–1024. doi:10.1136/ard.60.11.1021
17. Camellino D, Duftner C, Dejaco C. New insights into the role of imaging in polymyalgia rheumatica. Rheumatology. 2021;60(3):1016–1033. doi:10.1093/rheumatology/keaa646
18. Owen CE, Nakos O. Imaging findings in polymyalgia rheumatica. Rheumatology. 2025;64(Supplement_1):i59–i63. doi:10.1093/rheumatology/keae473
19. Mackie SL, Koduri G, Hill CL, et al. Accuracy of musculoskeletal imaging for the diagnosis of polymyalgia rheumatica: systematic review. RMD Open. 2015;1(1):e000100. doi:10.1136/rmdopen-2015-000100
20. Fruth M, Seggewiss A, Kozik J, Martin-Seidel P, Baraliakos X, Braun J. Diagnostic capability of contrast-enhanced pelvic girdle magnetic resonance imaging in polymyalgia rheumatica. Rheumatology. 2020;59(10):2864–2871. doi:10.1093/rheumatology/keaa014
21. Henckaerts L, Gheysens O, Vanderschueren S, Goffin K, Blockmans D. Use of 18F-fluorodeoxyglucose positron emission tomography in the diagnosis of polymyalgia rheumatica—a prospective study of 99 patients. Rheumatology. 2018;57(11):1908–1916. doi:10.1093/rheumatology/kex376
22. van der Geest KS, van Sleen Y, Nienhuis P, et al. Comparison and validation of FDG-PET/CT scores for polymyalgia rheumatica. Rheumatology. 2022;61(3):1072–1082. doi:10.1093/rheumatology/keab483
23. Owen CE, Poon AMT, Yang V, et al. Abnormalities at three musculoskeletal sites on whole-body positron emission tomography/computed tomography can diagnose polymyalgia rheumatica with high sensitivity and specificity. Eur J Nucl Med Mol Imaging. 2020;47(10):2461–2468. doi:10.1007/s00259-020-04731-z
24. Nielsen AW, Hansen IT, Nielsen BD, et al. The effect of prednisolone and a short-term prednisolone discontinuation for the diagnostic accuracy of FDG-PET/CT in polymyalgia rheumatica—a prospective study of 101 patients. Eur J Nucl Med Mol Imaging. 2024;51(9):2614–2624. doi:10.1007/s00259-024-06697-8
25. Jung JY, Lee E, Suh CH, Kim HA. Neutrophil‐to‐lymphocyte ratio and platelet‐to‐lymphocyte ratio are associated with disease activity in polymyalgia rheumatica. J Clin Lab Analysis. 2019;33(9):e23000. doi:10.1002/jcla.23000
26. Van Sleen Y, Graver JC, Abdulahad WH, et al. Leukocyte dynamics reveal a persistent myeloid dominance in giant cell arteritis and polymyalgia rheumatica. Front Immunol. 2019;10:1981. doi:10.3389/fimmu.2019.01981
27. Carvajal Alegria G, Cornec DY, Renaudineau Y, Saraux A, Devauchelle-Pensec V. Inflammatory markers are quickly improved by tocilizumab in early polymyalgia rheumatica and might predict early response to interleukin-6 blockade. Rheumatology and Therapy. 2021;8(2):751–760. doi:10.1007/s40744-021-00299-8
28. van Sleen Y, Boots AM, Abdulahad WH, et al. High angiopoietin-2 levels associate with arterial inflammation and long-term glucocorticoid requirement in polymyalgia rheumatica. Rheumatology. 2020;59(1):176–184. doi:10.1093/rheumatology/kez261
29. van der Geest KS, Abdulahad WH, Rutgers A, et al. Serum markers associated with disease activity in giant cell arteritis and polymyalgia rheumatica. Rheumatology. 2015;54(8):1397–1402. doi:10.1093/rheumatology/keu526
30. Graver JC, Abdulahad W, van der Geest KS, et al. Association of the CXCL9-CXCR3 and CXCL13-CXCR5 axes with B-cell trafficking in giant cell arteritis and polymyalgia rheumatica. J Autoimmun. 2021;123:102684. doi:10.1016/j.jaut.2021.102684
31. Shuai X, Dandan F, Liang X. Study on the changes and significance of CXCL10 level in serum of isolated polymyalgia rheumatica. Clin Rheumatol. 2024;1–6.
32. van Nieuwland M, Mulder AL, Colin EM, Alves C, van Bon L, Brouwer E. Investigating interferon type I responses in patients with suspected giant cell arteritis and polymyalgia rheumatica. Clin Exp Immunol. 2024;218(3):308–313. doi:10.1093/cei/uxae085
33. Ellingsen T, Elling P, Olson A, et al. Monocyte chemoattractant protein 1 (MCP-1) in temporal arteritis and polymyalgia rheumatica. Ann Rheumatic Dis. 2000;59(10):775–780. doi:10.1136/ard.59.10.775
34. Pulsatelli L, Meliconi R, Boiardi L, Macchioni P, Salvarani C, Facchini A. Elevated serum concentrations of the chemokine RANTES in patients with polymyalgia rheumatica. Clin Exper Rheumatol. 1998;16(3):263–268.
35. Michailidou D, Johansson L, Chapa JAG, et al. Mitochondrial‐mediated platelet activation in polymyalgia rheumatica. ACR Open Rheumatol. 2025;7(3):e70021. doi:10.1002/acr2.70021
36. Kim JW, Jung JY, Suh CH, Kim HA. Evaluation of inflammatory scores as diagnostic markers for polymyalgia rheumatica. Inter J Rheumatic Dis. 2025;28(3):e70153. doi:10.1111/1756-185X.70153
37. Manzo C, Milchert M, Natale M, Brzosko M. Polymyalgia rheumatica with normal values of both erythrocyte sedimentation rate and C-reactive protein concentration at the time of diagnosis. Rheumatology. 2019;58(5):921–923. doi:10.1093/rheumatology/key431
38. Marsman DE, den Broeder N, Boers N, van den Hoogen FH, den Broeder AA, van der Maas A. Polymyalgia rheumatica patients with and without elevated baseline acute phase reactants: distinct subgroups of polymyalgia rheumatica. Clin Exp Rheumatol. 2021;39(1):32–37. doi:10.55563/clinexprheumatol/gdps1r
39. Cantini F, Salvarani C, Olivieri I, et al. Erythrocyte sedimentation rate and C-reactive protein in the evaluation of disease activity and severity in polymyalgia rheumatica: a prospective follow-up study. In: Seminars in arthritis and rheumatism. Vol. 30. WB Saunders; 2000. pp. 17–24. doi:10.1053/sarh.2000.8366
40. Cantini F, Salvarani C, Olivieri I, et al. Erythrocyte sedimentation rate and C-reactive protein in the evaluation of disease activity and severity in polymyalgia rheumatica: a prospective follow-up study. In: Seminars in Arthritis and Rheumatism. Elsevier. 30; 2000.
41. Dasgupta B, Cimmino MA, Kremers HM, et al. provisional classification criteria for polymyalgia rheumatica: a European league against rheumatism/American college of rheumatology collaborative initiative. Arthritis Rheum. 2012;64(4):943–954. doi:10.1002/art.34356
42. Roche NE, Fulbright JW, Wagner AD, Hunder GG, Goronzy JJ, Weyand CM. Correlation of interleukin‐6 production and disease activity in polymyalgia rheumatica and giant cell arteritis. Arthritis Rheum. 1993;36(9):1286–1294. doi:10.1002/art.1780360913
43. Dasgupta B, Panayi G. Interleukin-6 in serum of patients with polymyalgia rheumatica and giant cell arteritis. Rheumatology. 1990;29(6):456–458. doi:10.1093/rheumatology/29.6.456
44. van der Geest KS, Abdulahad WH, Chalan P, et al. Disturbed B cell homeostasis in newly diagnosed giant cell arteritis and polymyalgia rheumatica. Arthritis Rheumatol. 2014;66(7):1927–1938. doi:10.1002/art.38625
45. Carvajal Alegria G, Devauchelle-Pensec V, Renaudineau Y, Saraux A, Pers J-O, Cornec D. Correction of abnormal B-cell subset distribution by interleukin-6 receptor blockade in polymyalgia rheumatica. Rheumatology. 2017;56(8):1401–1406. doi:10.1093/rheumatology/kex169
46. Proost P, Struyf S, Van Damme J, Fiten P, Ugarte-Berzal E, Opdenakker G. Chemokine isoforms and processing in inflammation and immunity. J Autoimmun. 2017;85:45–57. doi:10.1016/j.jaut.2017.06.009
47. Tokunaga R, Zhang W, Naseem M, et al. CXCL9, CXCL10, CXCL11/CXCR3 axis for immune activation–a target for novel cancer therapy. Cancer Treat Rev. 2018;63:40–47. doi:10.1016/j.ctrv.2017.11.007
48. Camellino D, Soldano S, Cutolo M, Cimmino MA. Dissecting the inflammatory response in polymyalgia rheumatica: the relative role of IL-6 and its inhibition. Rheumatol Inter. 2018;38(9):1699–1704. doi:10.1007/s00296-018-4086-1
49. Meliconi R, Pulsatelli L, Dolzani P, et al. Vascular endothelial growth factor production in polymyalgia rheumatica. Arthritis Rheum. 2000;43(11):2472–2480. doi:10.1002/1529-0131(200011)43:11<2472::AID-ANR14>3.0.CO;2-B
50. Dejaco C, Kerschbaumer A, Aletaha D, et al. Treat-to-target recommendations in giant cell arteritis and polymyalgia rheumatica. Ann Rheumatic Dis. 2024;83(1):48–57. doi:10.1136/ard-2022-223429
51. Bolhuis TE, Bosch P, Falzon L, et al. Definitions of and instruments for disease activity, remission and relapse in polymyalgia rheumatica: a systematic literature review. Rheumatology. 2025;64(2):455–469. doi:10.1093/rheumatology/keae428
52. McCarthy EM, MacMullan PA, Al-Mudhaffer S, et al. Plasma fibrinogen is an accurate marker of disease activity in patients with polymyalgia rheumatica. Rheumatology. 2013;52(3):465–471. doi:10.1093/rheumatology/kes294
53. Owen CE, McMaster C, Liew DF, Leung JL, Scott AM, Buchanan RR. Neutrophil to lymphocyte ratio predicts glucocorticoid resistance in polymyalgia rheumatica. Inter J Rheumatic Dis. 2021;24(1):56–62. doi:10.1111/1756-185X.14000
54. Michailidou D, Johansson L, Kuley R, et al. Immune complex-mediated neutrophil activation in patients with polymyalgia rheumatica. Rheumatology. 2023;62(8):2880–2886. doi:10.1093/rheumatology/keac722
55. Brun J, Madland T, Gran J, Myklebust G. A longitudinal study of calprotectin in patients with polymyalgia rheumatica or temporal arteritis: relation to disease activity. Scand J Rheumatol. 2005;34(2):125–128. doi:10.1080/03009740410009931
56. Floris A, Piga M, Chessa E, et al. Long-term glucocorticoid treatment and high relapse rate remain unresolved issues in the real-life management of polymyalgia rheumatica: a systematic literature review and meta-analysis. Clin Rheumatol. 2022;41(1):19–31. doi:10.1007/s10067-021-05819-z
57. Iorio L, Bond M, Padoan R, Dejaco C. Advances in the treatment of polymyalgia rheumatica. Rheumatology. 2025;64(Supplement_1):i48–i54. doi:10.1093/rheumatology/keae539
58. Hayashi K, Ohashi K, Watanabe H, et al. Thrombocytosis as a prognostic factor in polymyalgia rheumatica: characteristics determined from cluster analysis. Therape Adv Musculosk Dis. 2019;11:1759720X19864822. doi:10.1177/1759720X19864822
59. Perricone C, Cafaro G, Fiumicelli E, et al. Predictors of complete 24-month remission and flare in patients with polymyalgia rheumatica. Clin Exp Med. 2023;23(7):3391–3397. doi:10.1007/s10238-022-00976-0
60. Lee JH, Choi ST, Kim JS, et al. Clinical characteristics and prognostic factors for relapse in patients with polymyalgia rheumatica (PMR). Rheumatol Inter. 2013;33(6):1475–1480. doi:10.1007/s00296-012-2580-4
61. Rahimi M, Esalatmanesh K, Daneshvar S, Irvani SSN, Badali A, Khabbazi A. Outcomes of polymyalgia rheumatica in real-world practice: a longitudinal cohort study. Romanian J Internal Med. 2024;62(3):286–294. doi:10.2478/rjim-2024-0009
62. Ishiguro K, Yamashita H, Shimizu Y, Kaneko H. Biomarkers as predicting factors for relapse in polymyalgia rheumatica: the importance of alkaline phosphatase. Rheumatology. 2023;62(10):e288–e90. doi:10.1093/rheumatology/kead137
63. Birra D, Bosello SL, Peluso G, Zoli A. Sixth-month remission as a predictor for twelve-month remission in polymyalgia rheumatica. Clin Exp Rheumatol. 2020;38(3):436–441.
64. Hattori K, Hirano Y, Kojima T. Predictors of glucocorticoid‐free remission in patients with polymyalgia rheumatica treated with prednisolone. Inter J Rheumatic Dis. 2020;23(11):1581–1586. doi:10.1111/1756-185X.13978
65. Salvarani C, Cantini F, Niccoli L, et al. Acute‐phase reactants and the risk of relapse/recurrence in polymyalgia rheumatica: a prospective followup study. Arthritis Care Res. 2005;53(1):33–38. doi:10.1002/art.20901
66. Boiardi L, Casali B, Farnetti E, et al. Relationship between interleukin 6 promoter polymorphism at position-174, IL-6 serum levels, and the risk of relapse/recurrence in polymyalgia rheumatica. J Rheumatol. 2006;33(4):703–708.
67. Pulsatelli L, Boiardi L, Pignotti E, et al. Serum interleukin‐6 receptor in polymyalgia rheumatica: a potential marker of relapse/recurrence risk. Arthritis Care Res. 2008;59(8):1147–1154. doi:10.1002/art.23924
68. Tomelleri A, van der Geest KS, Khurshid MA, et al. Disease stratification in GCA and PMR: state of the art and future perspectives. Nat Rev Rheumatol. 2023;19(7):446–459. doi:10.1038/s41584-023-00976-8
69. Hemmig AK, Gozzoli D, Werlen L, et al. Subclinical giant cell arteritis in new onset polymyalgia rheumatica A systematic review and meta-analysis of individual patient data. In: Seminars in Arthritis and Rheumatism. Elsevier; 2022. doi:10.1016/j.semarthrit.2022.152017
70. Nettleton E, Carlson K, Putman M. The emerging risk of overdiagnosis in rheumatoid arthritis and polymyalgia rheumatica. Lancet Rheumatol. 2025;7(2):e141–e3. doi:10.1016/S2665-9913(24)00227-3
71. Salvarani C, Padoan R, Iorio L, et al. Subclinical giant cell arteritis in polymyalgia rheumatica: concurrent conditions or a common spectrum of inflammatory diseases? Autoimmunity Rev. 2024;23(1):103415. doi:10.1016/j.autrev.2023.103415
72. Yates M, Davies C, MacGregor AJ. Improving polymyalgia rheumatica care: considerations for routine vascular ultrasound in clinical practice. Lancet Rheumatol. 2025;7(6):e448–e50. doi:10.1016/S2665-9913(25)00031-1
73. De Miguel E, Karalilova R, Macchioni P, et al. Subclinical giant cell arteritis increases the risk of relapse in polymyalgia rheumatica. Ann Rheumatic Dis. 2024;83(3):335–341. doi:10.1136/ard-2023-224768
74. Yamashita R, Izumi Y, Hiramoto J. Alkaline phosphatase is useful for predicting giant cell arteritis complications in patients with polymyalgia rheumatica. Modern Rheumatol. 2025;35(3):529–534. doi:10.1093/mr/roae101
75. Ramon A, Greigert H, Goueslard K, et al. Diagnostic accuracy of serum biomarkers to identify giant cell arteritis in patients with polymyalgia rheumatica. RMD Open. 2024;10(3):e004488. doi:10.1136/rmdopen-2024-004488
76. van Sleen Y, Therkildsen P, Nielsen BD, et al. Angiopoietin-2/-1 ratios and MMP-3 levels as an early warning sign for the presence of giant cell arteritis in patients with polymyalgia rheumatica. Arthritis Res Therapy. 2022;24(1):65. doi:10.1186/s13075-022-02754-5
77. Fukui S, Nunokawa T, Kobayashi S, et al. MMP-3 can distinguish isolated PMR from PMR with GCA: a retrospective study regarding PMR and GCA in Japan. Modern Rheumatol. 2016;26(2):259–264. doi:10.3109/14397595.2015.1071304
78. Moreel L, Boeckxstaens L, Betrains A, et al. Prevalence, characteristics, and outcome of subclinical vasculitis in polymyalgia rheumatica: a retrospective cohort study. Rheumatology. 2024;63(12):3331–3336. doi:10.1093/rheumatology/keae208
79. De Miguel E, Macchioni P, Conticini E, et al. Prevalence and characteristics of subclinical giant cell arteritis in polymyalgia rheumatica. Rheumatology. 2024;63(1):158–164. doi:10.1093/rheumatology/kead189
80. Watanabe R, Maeda T, Zhang H, et al. MMP (matrix metalloprotease)-9–producing monocytes enable T cells to invade the vessel wall and cause vasculitis. Circul Res. 2018;123(6):700–715. doi:10.1161/CIRCRESAHA.118.313206
81. Platchek M, Lu Q, Tran H, Xie W. Comparative analysis of multiple immunoassays for cytokine profiling in drug discovery. Slas Discovery. 2020;25(10):1197–1213. doi:10.1177/2472555220954389
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.