")
Back to Journals » Vascular Health and Risk Management » Volume 11
Current and emerging strategies in the management of venous thromboembolism: benefit–risk assessment of dabigatran
Authors Fanola C
Received 17 March 2015
Accepted for publication 4 May 2015
Published 27 May 2015 Volume 2015:11 Pages 271—282
DOI https://doi.org/10.2147/VHRM.S62595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Daniel Duprez
Christina L Fanola
Department of Cardiovascular and Vascular Medicine, Boston University School of Medicine, Boston, MA, USA
Abstract: Venous thromboembolism (VTE) is a disease state that carries significant morbidity and mortality, and is a known cause of preventable death in hospitalized and orthopedic surgical patients. There are many identifiable risk factors for VTE, yet up to half of VTE incident cases have no identifiable risk factor and carry a high likelihood of recurrence, which may warrant extended therapy. For many years, parenteral unfractionated heparin, low-molecular weight heparin, fondaparinux, and oral vitamin K antagonists (VKAs) have been the standard of care in VTE management. However, limitations in current drug therapy options have led to suboptimal treatment, so there has been a need for rapid-onset, fixed-dosing novel oral anticoagulants in both VTE treatment and prophylaxis. Oral VKAs have historically been challenging to use in clinical practice, with their narrow therapeutic range, unpredictable dose responsiveness, and many drug–drug and drug–food interactions. As such, there has also been a need for novel anticoagulant therapies with fewer limitations, which has recently been met. Dabigatran etexilate is a fixed-dose oral direct thrombin inhibitor available for use in acute and extended treatment of VTE, as well as prophylaxis in high-risk orthopedic surgical patients. In this review, the risks and overall benefits of dabigatran in VTE management are addressed, with special emphasis on clinical trial data and their application to general clinical practice and special patient populations. Current and emerging therapies in the management of VTE and monitoring of dabigatran anticoagulant-effect reversal are also discussed.
Keywords: novel oral anticoagulants, dabigatran, venous thromboembolism, deep venous thrombosis, pulmonary embolism, oral anticoagulation
Background
Pulmonary embolism (PE) and deep venous thrombosis (DVT) are considered the two major disease entities of venous thromboembolism (VTE) or venous thromboembolic disease (VTD). The age-adjusted annual incidence of VTE is estimated at 114 cases per 100,000.1 VTE is responsible for significant morbidity and mortality. Within 1 month of diagnosis, the death rate for DVT and PE is about 6% and 12%, respectively. Further, mortality of untreated PE at 3 months may rise to over 30%.2 It is therefore critical to recognize VTE early and initiate the appropriate treatment, aiming to accomplish the following goals: control current and future symptoms, prevent embolization or extension of thrombus, prevent future recurrence, reduce incidence of post-thrombotic syndrome, and prevent chronic thromboembolic pulmonary hypertension.
There are many risk factors for VTE, but the major factors include obesity, older age, malignancy, prior VTE, hereditary thrombophilia, prolonged immobility or bed rest in hospitalized patients, and major surgery, such as total knee arthroplasty (TKA) and total hip arthroplasty (THA).3 However, up to 50% of patients with VTE will have no identifiable risk factors, being labeled as having an “unprovoked” event, which carries a high risk of recurrence.4 VTE contributes to significant but preventable mortality in the sick hospitalized and postsurgical patients. When guideline-based prophylaxis is implemented, incidence may decrease up to sixfold.5 However, prophylaxis is used appropriately in only 65% and 42% of at-risk surgical and medical populations, respectively.6
Prophylaxis and treatment of VTE
Oral vitamin K antagonists
Suboptimal therapy for VTE is in part due to clinical practice limitations in the most commonly utilized treatment options (Table 1).7 Unfractionated heparin (UFH), subcutaneous low-molecular weight heparin (LMWH), or fondaparinux, plus a concomitant vitamin K antagonist (VKA) until therapeutic blood levels are achieved, is recommended for the management of acute VTE. Overlapping parental anticoagulation is mandated for at least 5 days until the international normalized ratio (INR) becomes 2–3 for at least 24 hours, indicating adequate VKA anticoagulant activity.7
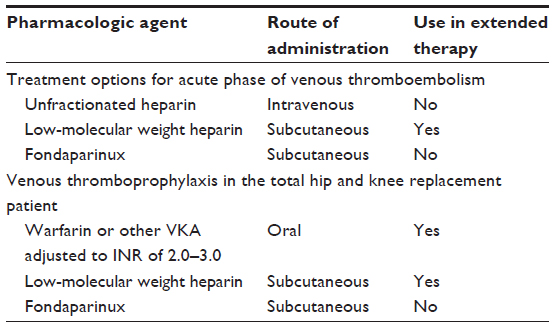 | Table 1 Guideline-based anticoagulant treatment and prophylaxis of venous thromboembolism prior to novel anticoagulant agent approval |
There are several available VKAs for use in VTE, but the one most commonly prescribed worldwide is warfarin. VKAs require frequent dose adjustments and INR monitoring, given the drugs’ narrow therapeutic range and unpredictable dose–response curve.8 Complex individualized dosing, often worsened by drug–drug interactions and drug–food interactions, can lead to prolonged hospitalizations and exorbitant health care costs.8 Genetic polymorphisms in VKA metabolism, when incorporated into individualized dosing algorithms, can reduce dose–response unpredictability. Although promising, genetic testing has not been proven cost-effective,9 and therefore is not commonly utilized in clinical practice. Advantages and disadvantages of warfarin therapy are summarized in Table 2.8
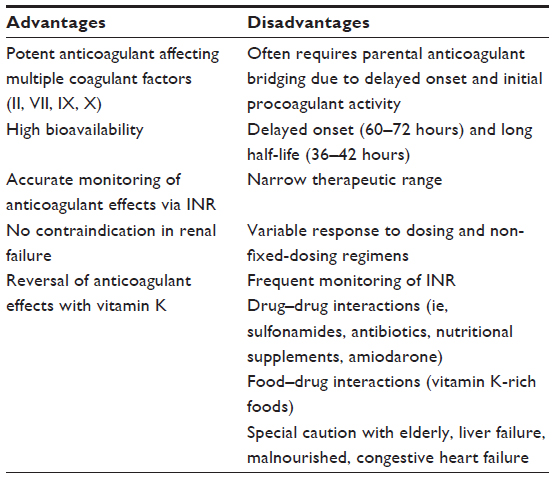 | Table 2 Advantages and disadvantages of vitamin K antagonists |
Many patients are on extended (>3 months) or lifelong oral VKA therapy for VTE if there is a high risk of recurrence, as is the case for unprovoked VTE.4,7 The unprovoked VTE can be a clinical challenge for physicians, as placing patients on lifelong or extended therapy increases potential exposure to bleeding risks. Further, bleeding risk on oral anticoagulation therapy is dynamic over time, as it increases with age and deterioration of renal function.10 It is reported that in the absence of clear contraindications to warfarin, the risk of major bleeding is relatively low at about 1% per year after VTE,11 and thus is regarded as safe as long as appropriate monitoring is performed. However, in a large study of nearly 100,000 US emergency room admissions for adverse drug reactions, warfarin was implicated in 33%.12
Parenteral anticoagulants
Parental therapy with UFH, LMWH, or fondaparinux is recommended in prophylaxis and treatment of VTE in many high-risk postsurgical patients (Table 1). LMWH offers a 50% relative risk (RR) reduction in symptomatic DVT compared to no prophylaxis following major orthopedic surgery, with minimal major bleeding events.13 There may also be some benefits in the extension of anticoagulant therapy beyond 30 days postoperatively.14 Current American College of Chest Physicians guidelines recommend medical thromboprophylaxis for at least 10 days with a preference for up to 35 days, especially with THAs.15 However, daily out-of-hospital injections of LMWH are inconvenient for patients and may contribute to suboptimal therapy utilization.16 One study surveyed patients utilizing anticoagulation for this indication, and the majority preferred oral thromboprophylaxis.17
Novel oral anticoagulants
Based on the limitations of parenteral and oral VKA anticoagulant treatment, there has been a demand for new therapeutic agents for both short- and long-term treatment and prophylaxis of VTE, with easier administration at fixed dosing, less drug and dietary interactions, and similar, if not improved, safety and efficacy profiles.18,19 Novel oral anticoagulant (NOAC) agents, which are rapidly expanding but currently include dabigatran, rivaroxaban, apixaban, and edoxaban, have been studied and approved for several indications worldwide in recent years. Some have been approved as current options in management of VTE and have favorable pharmacological profiles (Table 3).18,19 This review, however, provides a focused overview of dabigatran etexilate, which is the only direct thrombin inhibitor (DTI) approved for acute VTE treatment, extended therapy in recurrent VTE prevention, and prophylactic use in high-risk orthopedic (ie, THA and TKA) surgical patients. Risks and benefits of dabigatran in VTE management are addressed, with special emphasis on clinical trial data and their application to general clinical practice and special patient populations. Limitations in monitoring and reversibility, as well as future directions in the study of dabigatran, are also addressed.
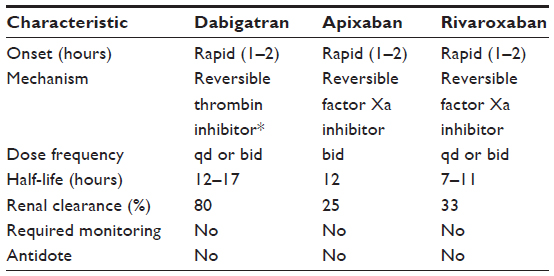 | Table 3 Comparative pharmacology of novel oral anticoagulant agents approved for use in management of venous thromboembolism |
Pharmacological properties of dabigatran
The need for oral anticoagulant therapy with an improved pharmacological profile has led to the development of dabigatran. Thrombin is an important enzyme involved in thrombogenesis associated with VTE, and unlike warfarin and heparin, DTIs can inhibit both free and fibrin-bound thrombin. Dabigatran etexilate is an orally administered prodrug that gets metabolized in the intestines, liver, and plasma to dabigatran, a small molecule that inhibits thrombin, without inhibiting thrombin generation.20 Inhibition of thrombin by dabigatran is reversible, and also specific, meaning that it will not bind to other coagulant proteins.20,21
Dabigatran has favorable pharmacokinetic and pharmacodynamic properties based on early studies in healthy human subjects (Table 3), with rapid absorption and complete metabolism to its active dabigatran form following oral administration, and a predictable dose–response curve. The dose-dependent peak plasma concentration is reached within 2 hours, and its half-life is between 14 hours and 17 hours for the typical older adult for whom dabigatran may be indicated. It is slightly less in younger, healthy subjects.20,21
Cytochrome P450 enzymes do not metabolize dabigatran etexilate; therefore, the drug does not interact with P450 inhibitors or inducers. The prodrug does, however, act as a substrate for P-glycoprotein (P-gp).21 Important medications that interfere with P-gp function, such as quinidine, ketoconazole, amiodarone, verapamil, and dronedarone, can increase peak plasma concentrations, especially in those patients with moderate renal impairment (creatinine clearance [CrCl] <50 mL/min), and must be considered prior to prescribing (Table 4).22–24 Proton pump inhibitors have also been shown to decrease the plasma concentration but without a change in efficacy and safety profile. Lastly, rifampicin is a potent inducer of P-gp and may decrease effective plasma levels of dabigatran.22,23
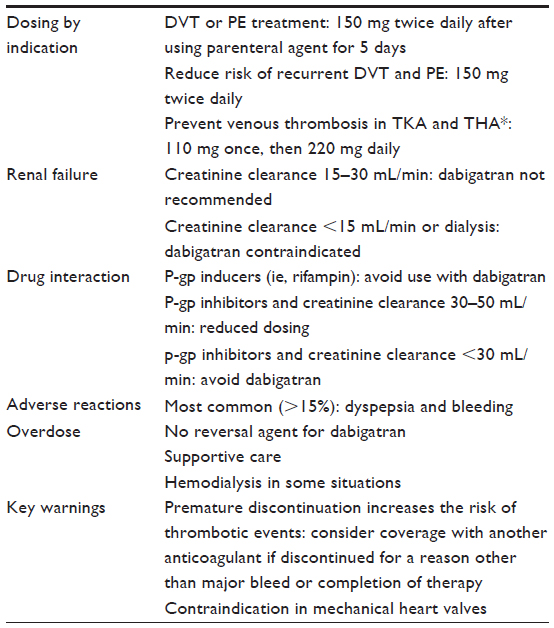 | Table 4 Dabigatran etexilate in venous thromboembolic disease |
Dabigatran (80%–85%) is eliminated unchanged via glomerular filtration in the kidneys. Less than 10% is excreted via a biliary pathway. A reduction in glomerular filtration associated with kidney injury is therefore associated with an increase in dabigatran drug exposure and a prolonged half-life, beyond 24 hours with a CrCl <30 mL/min. About 35% of dabigatran is protein bound, independent of dose and plasma concentration.20,21
Evidence behind dabigatran use being beneficial in VTE
Prophylaxis in major orthopedic surgery
Dabigatran is a safe and efficacious oral anticoagulant available for VTE prophylactic use in patients undergoing major orthopedic surgery (TKA, THA, and hip fracture surgery).25–29 For this indication, the approved dose is 220 mg once daily for 10 days in TKA patients and at least 28 days in THA patients after an initial half-dose.24 Patients at higher risk of bleeding (mainly elderly and those with renal dysfunction) are given a lower dose of 150 mg once daily (Table 4). A dose reduction is also mandated in orthopedic surgical patients concomitantly on P-gp such as amiodarone and verapamil.24
Dabigatran is approved for use in THA and TKA in more than 75 countries, mainly Europe and Canada, but not in the US. This discrepancy is based on varied results from the RE-MODEL (Dabigatran Etexilate 150 or 220 mg Once Daily vs Enoxaparin 40 mg Once Daily in Prevention of Venous Thromboembolism Post Total Knee Replacement), RE-NOVATE (Dabigatran Etexilate Compared with Enoxaparin in Prevention of Venous Thromboembolism Following Total Hip Arthroplasty) I and II, and RE-MOBILIZE (Dabigatran Etexilate 220 mg vs Enoxaparin 30 mg Twice Daily in Prevention of Venous Thromboembolism Post Total Knee Replacement) trials (Table 5). The trials implemented different dosing regimens within their corresponding enoxaparin arms. The RE-MOBILIZE investigators used the standard North American subcutaneous enoxaparin regimen of 30 mg twice-daily postoperatively. Alternatively, the RE-MODEL and RE-NOVATE investigators used 40 mg daily dosing, which began preoperatively.25–28 RE-MOBILIZE demonstrated VTE and VTE-related mortality after TKA was higher in both 220 mg and 150 mg doses of dabigatran when compared to 30 mg twice-daily enoxaparin (3.0% and 3.4%, respectively, versus 2.2%). Bleeding rates between the drug arms were similar.28
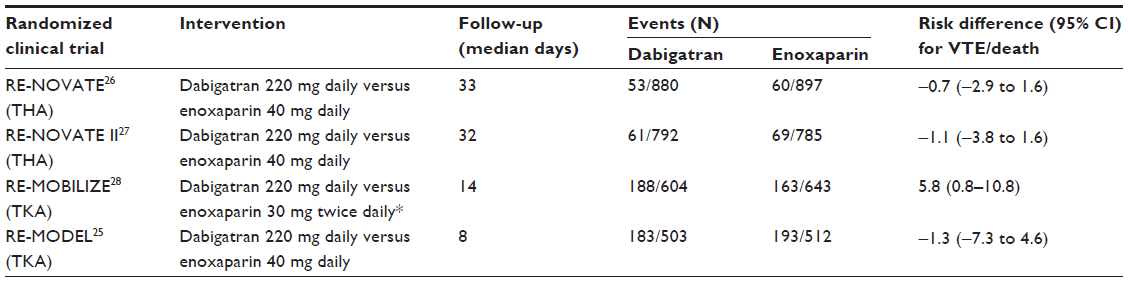 | Table 5 Randomized clinical trials for dabigatran use in prevention of venous thromboembolism after major orthopedic surgery |
Alternatively, results from RE-MODEL and RE-NOVATE trials, utilizing the European regimen of enoxaparin, demonstrated non-inferiority of both 220 mg and 150 mg dabigatran doses without significant bleeding risk.25–27 The 220 mg daily dabigatran dose ultimately gained approval for this indication based on results from a meta-analysis combining the RE-MOBILIZE, RE-MODEL, and RE-NOVATE data. Primary outcome event rates for the higher and lower dose of dabigatran, and enoxaparin, were 3.8%, 3.0%, and 3.3%, respectively.29 In an extended prophylactic treatment regimen, RE-NOVATE II randomized THA patients to the high-dose dabigatran etexilate regimen or the 40 mg daily enoxaparin regimen, concluding similar safety and efficacy endpoints as the RE-MODEL and RE-NOVATE I trials.27
Treatment of acute VTE
Based on the RE-COVER (Efficacy and Safety of Dabigatran Compared to Warfarin for 6 Month Treatment of Acute Symptomatic Venous Thromboembolism) trial, dabigatran is a safe and efficacious alternative oral anticoagulant to warfarin in the treatment of VTE after initial therapy with parenteral anticoagulation for at least 5 days.30 In a relatively small-study population, data from a total of 1,274 patients in the dabigatran group and 1,265 in the warfarin group were available for the primary analysis. Included were those with symptomatic proximal lower extremity DVT or PE (onset <14 days), for whom 6 months of anticoagulant therapy was indicated. Key exclusion criteria were hemodynamic instability from PE, VTE requiring thrombolytic therapy, concomitant indication for warfarin or long-term antiplatelet therapy, significant active cardiac disease, and a CrCl of less than 30 mL/min.30 Dabigatran at 150 mg twice-daily dosing, after initial parenteral treatment, was non-inferior to dose-adjusted warfarin in the prevention of recurrent VTE or VTE-related death at 6 months (hazard ratio [HR] 1.10, 95% confidence interval [CI] 0.65–1.84; P<0.001 for non-inferiority).30 RE-COVER II was designed as a duplicate of RE-COVER and to expand its study population. Dabigatran in RE-COVER II had a similar efficacy and safety profile when compared to warfarin. In a pooled analysis of the RE-COVER trials, there was no difference in the primary endpoint between dabigatran and warfarin (HR 1.09, 95% CI 0.76–1.57) with a favorable bleeding profile (major bleeding HR 0.73, 95% CI 0.48–1.11).31
Extended treatment of VTE
Since almost half of VTE incidence has no identifiable risk factor and is therefore “unprovoked”, a phenomenon associated with a high recurrence rate, many patients are placed on extended, often lifelong, anticoagulation.7 Dabigatran has been approved for patients who completed acute VTE treatment of at least 3 months.24 Approval is based on results from the active-controlled RE-MEDY (a Phase III, Randomised, Multicenter, Double-blind, Parallel-group, Active-Controlled Study to Evaluate the Efficacy and Safety of Oral Dabigatran Etexilate [150 mg Bid] Compared to Warfarin [INR 2.0–3.0] for the Secondary Prevention of Venous Thromboembolism) and placebo-controlled RE-SONATE trials. In RE-MEDY, although event rates were low, dabigatran was non-inferior to warfarin in the reduction of VTE and VTE-related deaths (HR 1.44, 95% CI 0.78–2.64; P<0.01 for non-inferiority).32 Patients randomized to either dose-adjusted warfarin or dabigatran 150 mg twice-daily dosing had completed 3–12 months of anticoagulant therapy for their index event. Major or clinically relevant bleeding events were fewer in the dabigatran versus warfarin arm (HR 0.54, 95% CI 0.41–0.71).32 In the placebo-controlled RE-SONATE trial, event rates for recurrent or fatal VTE or death in the dabigatran versus placebo arms were 0.4% and 5.6%, respectively (HR 0.08, 95% CI 0.02–0.25; P<0.001) with few major bleeding events.32 Based on these results, dabigatran should be considered an effective alternative to warfarin for treatment in extended (unprovoked) VTE management.
Risks associated with dabigatran use in VTE
Bleeding events
In the RE-COVER trial, bleeding episodes occurred in both the dabigatran and warfarin groups at rates of 1.6% and 1.9%, respectively (HR 0.82, 95% CI 0.45–1.48).30 Similar bleeding risk between the two drug arms was also found in the pooled analysis that included RE-COVER II data (HR 0.73, 95% CI 0.48–1.11).31 The types of bleeding events were overall similar between the two treatment arms; however, the dabigatran group had a trend (although insignificant) toward greater gastrointestinal hemorrhagic events. In terms of adverse events, those on dabigatran were more likely to report dyspepsia when compared to those on warfarin (2.9% and 0.6%, respectively; P<0.001), which in some cases was severe enough for discontinuation of study drug.30 In a meta-analysis from the thromboprophylaxis trials (RE-MODEL, RE-NOVATE, RE-MOBILIZE), bleeding rates were similar between dabigatran and enoxaparin arms (RR 1.09, 95% CI 0.74–1.61).29
Acute coronary syndromes
There exist conflicting but compelling data on myocardial infarction (MI) risk from multiple studies. The randomized evaluation of long-term anticoagulant therapy (RE-LY) trial compared two doses of dabigatran (110 mg or 150 mg twice daily) to warfarin in stroke prevention in non-valvular atrial fibrillation (AF).33 Baseline characteristics in the dabigatran arms were notably different in this trial when compared to VTE trials. For example, RE-LY compared with RE-COVER had a higher prevalence of cardiac comorbidities and a greater mean age (71.5 years and 55 years, respectively).30,33 Although dabigatran was superior to warfarin in stroke or systemic embolism at the 150 mg twice-daily dose (RR 0.66, 95% CI 0.53–0.82), there was a higher incidence of MI (RR 1.38, 95% CI 1.00–1.91; P=0.048).33 However, authors subsequently published a revision to the original analysis after adjudication of additional reported adverse events such as MIs, and found no significant difference between dabigatran and warfarin treatment arms (RR 1.27, 95% CI 0.94–1.71; P=0.12).34 Results from the acute VTE RE-COVER trial, which excluded subjects with any recent unstable cardiac diseases and those needing long-term antiplatelet therapy, concluded no difference in the incidence of MI between the study groups (0.3% versus 0.2%; P=0.69).30
In extended treatment of VTE, the placebo-controlled RE-SONATE trial resulted in no significant difference in acute coronary syndromes between the dabigatran and placebo arms.32 On the contrary, the active-controlled RE-MEDY trial resulted in a difference between drug arms; acute coronary syndromes occurred in 0.9% and 0.2% of the dabigatran and warfarin groups, respectively (P=0.02). There was, however, a higher prevalence of cardiac comorbidities in the dabigatran arm.32
Several meta-analyses have sought to address MI risk associated with dabigatran use.35–37 One such meta-analysis accounted for the updated data from RE-LY and was inclusive of the randomized controlled trials on VTD; it found the use of dabigatran (150 mg twice-daily dosing) to be associated with an increased risk of MI (odds ratio 1.34, 95% CI 1.08–1.65) compared to control.35 A major limitation in the generalizability of these meta-analyses’ results to subjects on dabigatran strictly for VTD is that AF and VTE trial populations were combined. Patients with acute VTE are typically younger and have fewer cardiac comorbidities; thus, the risk of MI in this population alone may not be significant but should be considered for the elderly patients with VTE and comorbid cardiac conditions.
The increase in MI associated with long-term dabigatran use could go beyond just differences in trial populations. For example, the placebo-controlled RE-SONATE trial showed no increased MI risk with dabigatran. MI risk was evident mainly in dabigatran versus warfarin trials. This observation could possibly be explained by a protective effect of warfarin and not a dabigatran-associated direct risk. One such study assessing platelet aggregation in patients on dabigatran who have stable coronary artery disease may add additional insights to this area.38
Although the RE-MODEL trial results concluded that dabigatran cessation is safe without an observed rebound effect,25 there are reported cases of such a phenomenon with dabigatran and other NOACs,39 and thus, a “black box warning” regarding the cessation of all NOACs exists on the package insert.24 Data on a rebound-specific effect associated with dabigatran are not widely available from the clinical trials. Thus, until further data are elucidated, present recommendations are to reduce a rebound thrombotic risk by considering another anticoagulant (ie, UFH or LMWH) if dabigatran is discontinued for any reason other than major bleeding or VTE treatment course completion.24 Further study is warranted to assess this risk in dabigatran-specific populations.
Mechanical heart valves
The RE-ALIGN (Dabigatran versus Warfarin in Patients with Mechanical Heart Valves) Phase II trial assessed efficacy and safety of dabigatran in a small number of patients with mechanical heart valves. The trial was stopped early due to an increase in thrombotic events and an increase in bleeding postsurgery with dabigatran compared with warfarin.40 A contraindication for dabigatran use exists with mechanical heart valves (both with and without AF).24 Subjects with mechanical heart valves were not included in the VTE study populations. Based on these data, patients with mechanical heart valves should not be treated with dabigatran for VTE prophylaxis, acute treatment, and/or extended treatment, given high-risk outcomes.
Monitoring of dabigatran plasma concentrations and management of major bleeding events
Plasma concentration variation of dabigatran
Alternatives to VKAs were primarily developed to meet the need for fixed-dosing and more predictable peak plasma concentrations. Dabigatran etexilate gained approval for use in general clinical practice with no monitoring required.24 The predictability of dabigatran’s pharmacokinetic profile has recently been challenged. With an initially low bioavailability, a prodrug conversion process utilizing two metabolic pathways, and a (mostly) single elimination route via the kidneys, a small difference in metabolic activation or CrCl can possibly affect plasma levels, thereby altering its safety and efficacy profile.41 In a large RE-LY trial subset analysis of 9,183 subjects with available plasma concentrations, those with major bleeding events were more likely to have higher trough and post-dose plasma concentrations than those without bleeding events.42
The major risk factors associated with higher plasma concentrations in this study were renal dysfunction (both mild and moderate), older age, female sex, and weight (<50 kg and >100 kg). No association with ethnicity was found.42 These results demonstrate a higher-than-anticipated drug variability that may exist in clinical practice compared with the initial phase trials, which illustrates the need for reliable monitoring techniques of anticoagulant activity, and potentially plasma level testing in all new patients.41
Coagulation assays
At present, no monitoring is recommended for dabigatran. However, of the existing coagulation assays, a linear relationship exists between the plasma concentration of dabigatran and the INR, thrombin clotting time (TCT), and ecarin clotting time (ECT). Both TCT and ECT are assays specific to thrombin and therefore sensitive to a detectable dabigatran plasma concentration.43 However, there are measuring limitations with both assays in regular clinical use and may not be widely available in most places. Further, INR can be problematic in that it loses sensitivity at supratherapeutic dabigatran plasma concentrations.43
The relationship between dabigatran and activated partial thromboplastin time (aPTT) prolongation is not linear but rather curvilinear. Although aPTT may provide an adequate qualitative indication of anticoagulant activity with dabigatran, it can also be problematic in clinical use; it cannot be used for precise quantification of effect, as once dabigatran reaches high plasma concentrations, aPTT may plateau.20,43,44
Reversal of anticoagulant effects and timing for procedures
Data on the dose-dependent elimination of dabigatran are now available. In one study, ECT and aPTT prolongation after 24 hours of drug cessation was analyzed. An aPTT prolongation of about 15% was observed with higher doses of dabigatran (100–400 mg), whereas for lower doses <100 mg, aPTT normalized. ECT prolongation declined to <10% of its maximum value after 24 hours, with a large drop in coagulant activity up front within 8 hours.20 Summarizing these results, a small residual anticoagulant effect of dabigatran is observable ≥24 hours after cessation of treatment, but there is an initial rapid decline. This suggests the potential safety of dabigatran use in the absence of available antidote or reversal agent should bleeding occur.20
There are inherent limitations in the understanding of anticoagulant effects of dabigatran, given the lack of a highly specific and sensitive assay. However, based on what is known about the reversal of anticoagulant activity from the available studies, current recommendations mandate patients with normal kidney function stop dabigatran 24–48 hours prior to a major surgery. Cessation beyond 48 hours is recommended for those surgeries with greater bleeding risk or for those with diminished kidney function.43,45 Studies are ongoing to develop an accurate monitoring assay that will detect the reversal of anticoagulant effects of dabigatran in the case of bleed or need for emergent surgery.46
Management options for dabigatran-related bleeding events
Recombinant activated factor VII and prothrombin complex concentrates
At the time of this review, no specific antidote was available to reverse dabigatran’s anticoagulant effects. Current recommendations in the situation of a clinically significant bleed are summarized in Table 6. These include discontinuing the drug, controlling the bleed at its source, augmenting diuresis (renal elimination) of the drug as deemed necessary, and transfusing packed red blood cells or fresh frozen plasma.45 Oral activated charcoal can also effectively absorb nearly all of dabigatran but only if performed within 2 hours of drug administration.43 In patients with normal renal function and a hemodynamically stable bleeding event, these steps may be enough without needing the additional use of pro-hemostatic agents or dialysis.45
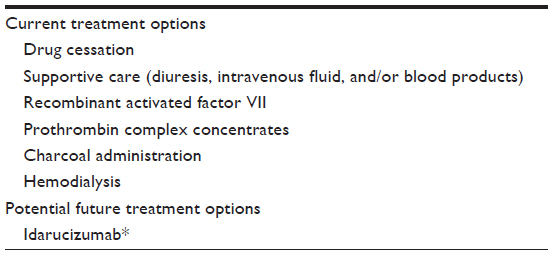 | Table 6 Management options in case of dabigatran-related major bleeding |
Recombinant activated factor VII (rFVIIa) and prothrombin complex concentrates (PCCs) in animal models have been shown useful in reversing the anticoagulant effects of dabigatran. rFVIIa directly activates platelet-surface thrombin independent of the tissue factor pathway, and has been shown to reduce aPTT prolongation associated with high-dose dabigatran.43,47 PCCs, either “three-factor” or “four-factor”, have combinations of factors II (prothrombin), VII, XI, and X, proteins C and S, and antithrombin. PCCs can stimulate thrombin formation, which in theory can bypass the anticoagulant effects of DTIs.47,48
In a recent randomized, placebo-controlled study in healthy human subjects given dabigatran etexilate, no difference was found in aPTT, TCT, and ECT with PCC administration compared to placebo, despite animal studies showing a favorable effect of PCCs on bleeding times.48 The discrepancy between animal and human studies can be partially explained by differences in PCC effect on coagulation assays and bleeding times. It is also questionable whether coagulation assays can really monitor the potential for dabigatran reversal in cases of threatening bleeds treated with PCCs.48 Lastly, there also may exist inherent differences in the ability for reversal with PCC in animals compared to humans.48 Overall, this illustrates the need for further research and the development of a suitable antidote. In the meantime, PCCs are still suggested as treatment in cases of life-threatening bleeding with dabigatran.
Emerging antidotes
Recent data exist on an emerging antidote for dabigatran. Idarucizumab is a humanized antibody fragment (Fab) that is a potent binder of dabigatran with neutralizing capabilities of its anticoagulant activity.49 It has no known affinity for thrombin substrates and exhibits no activity in blood coagulation assays. In a study of healthy volunteers who were administered dabigatran for 4 days (220 mg twice-daily dosing), there was a significant reversal of systemic anticoagulation with administration of idarucizumab.49 Data are soon emerging on the usefulness of this agent in clinical practice.50
Use of hemodialysis in dabigatran-related hemorrhage
According to the American College of Chest Physicians, experience is still lacking to firmly guide reversal in major bleeding and suspected overdose in patients who are taking dabigatran.51 At present, given the short half-life of dabigatran in patients with normal kidney function, discontinuation of drug with supportive care is recommended for mild–moderate bleeding.45 What remains controversial is the best option for those with severe bleeding, need for urgent surgery, and even more so, those with kidney dysfunction. As dabigatran is 35% protein bound, a large proportion is removed by hemodialysis (HD). In patients with CrCl <30 mL/min, the half-life of dabigatran doubles to 25–30 hours, and thus, HD becomes a reasonable option for these patients in life-threatening or high-risk situations.52
Current recommendations for management in patients with kidney dysfunction are only based on case reports and small-study outcomes but include the above recommendations for a dabigatran-related bleed plus the following: 4-hour HD treatment at a flow rate of 300–400 mL/min, after pre-dialysis administration of clotting factors for dialysis-catheter insertion.53 Further, there is to be expected a small variable rebound effect of dabigatran upon cessation of HD; thus, the possibility of a longer dialysis session is suggested, or use of a continuous modality of renal replacement therapy in high-risk patients.54
Dabigatran use in special populations
Chronic kidney disease patients
Dabigatran is renally eliminated and can be partially removed by dialysis.52 The US Food and Drug Administration approved usage of dabigatran for VTE in patients with CrCl >30 mL/min. Use in patients with CrCl ≤30 mL/min is not supported by scientific evidence and cannot be fully recommended, since Phase III clinical trials excluded such patients. But those patients in this category who are placed on dabigatran will require reduced dosing. Use of dabigatran in patients on chronic dialysis (or CrCl <15 mL/min) for kidney dysfunction is contraindicated (Table 4).24
The off-label dabigatran use in anticoagulated dialysis patients with AF was recently reported in one study of nearly 30,000 subjects, which amounted to 6%. Importantly, hemorrhagic death among those on dabigatran and dialysis was significantly increased when compared to those on warfarin and dialysis (RR 1.78, 95% CI 1.18–2.68; P=0.006).55 The prevalence of off-label dabigatran use in VTE patients at this time is unknown and warrants further analysis. But recommendations remain against its use in dialysis patients or patients at risk of severe kidney injury,24 largely in part due to increased risk of bleeding on anticoagulation associated with underlying kidney disease.10,56 Further study is warranted to fully assess the use of dialysis in reversal of dabigatran and to also assess safety of dabigatran use in dialysis patients, since off-label use is increasingly growing. Research has recently been completed in this field; however, results were not available at the time of this review.57
Elderly patients
Older age is also a known risk factor for anticoagulant-induced bleeding.10,56 After initial approval, dabigatran was readily prescribed to thousands of patients for stroke prevention in AF. Over concerns for unrecognized risks of therapy, given the overall exclusion of patients of advanced age and with kidney failure in trial populations,33 the Haematology Society of Australia and New Zealand produced an audit of bleeding events. They found that during a 2-month period, 78 episodes of bleeding occurred, with four major associative factors being prescriber error, impaired renal function, patient age (elderly), and complications due to lack of antidote. Two-thirds of the events were in patients over the age of 80 years.58
The use of dabigatran and other novel anticoagulants in elderly VTE patients has been studied. Since increased age and renal impairment are risk factors not only for venous thrombosis but also anticoagulant-induced bleeding, subset analyses were needed to determine safety and efficacy of dabigatran in these special populations. A meta-analysis was performed from the Phase III trial data of novel anticoagulant use in prevention of recurrent VTE and VTE-related death in the elderly.59 Although a study of this kind introduces heterogeneity and may confound generalizability of results, it found reduced recurrent VTE for NOAC agents (which included dabigatran) compared to warfarin, with a safety profile that was similar to that of the individual studies.59
Real-world long-term follow-up studies are needed to further demonstrate the safety of dabigatran in the elderly. A recent Medicare population cohort study has recently been completed. Among nearly 135,000 subjects with AF, dabigatran (at 75 mg twice-daily dosing) was associated with reduced risk of intracranial hemorrhage and death but increased risk of major gastrointestinal bleeding. These associations were more pronounced in those taking 150 mg twice daily when compared with warfarin.60 From these results, dabigatran can be concluded as probably safe in elderly patients with careful monitoring, but caution is warranted in those with a higher risk of gastrointestinal bleeding.
Patients with active malignancy and VTE
Patients with active malignancy represent a challenging population as not only are they at an increased risk of VTE but they also have an increased risk of anticoagulant-related bleeding events.61 Therefore, the safety and efficacy of alternative anticoagulant therapy such as dabigatran needs to be established prior to its introduction into guideline-based clinical practice. Current guidelines recommend treatment of VTE in active malignancy with LMWH. VKAs are also widely utilized although not as effective as LMWH.62 No evidence existed at the time of this review regarding the benefit of dabigatran when compared to LMWH in the treatment of malignancy-associated VTE. However, recently published was a post hoc analysis from the RE-COVER data.
The pooled analysis found dabigatran to be efficacious without significant bleeding risk in the treatment of acute VTE after initial parental therapy.31 In the post hoc analysis, subjects with cancer at baseline during enrollment or who developed cancer during study follow-up were included. The subjects were significantly older and had a lower baseline kidney function than those without cancer in the RE-COVER population, and had higher rates of recurrent VTE (HR 3.33, 95% CI 2.1–5.3). During 6-month follow-up, recurrent VTE or VTE-related death rates and bleeding rates were similar for the dabigatran and warfarin arms.63 This suggests that dabigatran may be an appropriate alternative for cancer patients who are currently on VKA for VTE. Its efficacy and safety in comparison to LMWH has yet to be determined.
Summary and conclusion
Since the approval of dabigatran for use in orthopedic surgery, venous thromboprophylaxis, acute VTE treatment, and extended prevention of recurrent VTE, there exists a promising alternative to VKAs. In relatively healthy subjects, it has a very predictable pharmacological profile, with rapid onset and peak plasma concentrations reached within 2 hours. Further, it has a predictable half-life of 24 hours with studies showing a significant drop in plasma concentration within as soon as 8 hours, thereby not requiring routine coagulation assay monitoring. Given its rapid elimination, dabigatran gained approval without the existence of an available antidote. Based on emerging data from case reports and observational studies, bleeding events are mostly controlled with discontinuation of drug and supportive care, with the possibility of adding pro-hemostatic agents and dialysis in severe cases. Fixed-dosing and rare drug–drug and food–drug interactions also make dabigatran an optimal oral anticoagulant for many patients with VTE. As a result, dabigatran is increasingly being prescribed for patients with VTE.
Robust clinical trial data have supported dabigatran’s use in VTE with an overall similar safety and efficacy profile as VKAs, however, with a small increased risk of nonfatal gastrointestinal bleeding events and adverse dyspepsia reactions. Results from clinical trials may not always translate fully and be generalizable to the population being prescribed dabigatran. Certain high-risk subgroups (ie, elderly, patients with moderate kidney dysfunction, those on long-term antiplatelet therapy, or those with active cardiac comorbidities), to whom dabigatran may still be prescribed, are often excluded from study populations or not adequately represented to formulate confident conclusions. The safety and efficacy of dabigatran is therefore, in these patient subgroups, less certain.
With the emergence of observational studies and post hoc analysis from the trial populations, dabigatran use in these high-risk populations will become better understood. For example, evidence recently surfacing on dabigatran’s efficacy compared to warfarin in cancer patients, who often are elderly and have multi-organ dysfunction and significant comorbidities, is encouraging. But until there exist adequate data on an available antidote and reversibility of anticoagulant effects, the prescribing physician should carefully consider each patient’s age, kidney function, medical history (especially cardiac comorbidities), and medication history prior to transitioning to dabigatran while there is no available antidote.
Since many patients will be transitioned to extended dabigatran for unprovoked VTE, long-term follow-up studies will be needed in the high-risk subgroups, and in those requiring surgical or endovascular interventions. Many “real-world” populations have been studied with regard to long-term effects of dabigatran. However, since the drug was first approved for stroke prevention in AF, much of the data known about dabigatran in the long term are derived from study populations that cannot be fully generalizable to the group of subjects on dabigatran for VTE. Therefore, the risks and benefits noted in study populations taking dabigatran for stroke prevention in AF should be confirmed in VTE populations in future study directions.
There is a dire need for ongoing research to fully address the overall risks and benefits of dabigatran use in VTE. In subsequent years, there will be more useful data available on use in severe chronic kidney disease or dialysis patients, available antidotes, monitoring for coagulant-activity reversal in acute bleeding events, and long-term use in malignancy. There is also an ongoing need for cost–benefit analyses specific to those prescribed dabigatran (versus warfarin) for acute VTE and for thromboprophylaxis in orthopedic surgery patients.
Limitations
This review is intended to address the risks and benefits of dabigatran use in VTD. One major limitation of this review is that the data utilized to provide such an analysis are derived from clinical trials and observational studies that included subjects on dabigatran for a different indication (ie, stroke prevention in AF). This is largely due to the fact that dabigatran was first approved for stroke prevention, and thus, more data are available from these populations. Although useful, conclusions from these studies cannot always be generalizable to subjects on dabigatran for VTE; therefore, ongoing studies are needed.
Another limitation of this review is that it does not provide adequate information for prescribers to assess the risk and benefits of prescribing dabigatran in VTE as compared to the other NOACs (ie, rivaroxaban and apixaban). This article is only intended to extrapolate risk–benefit data from the primary clinical trials assessing dabigatran use versus placebo or warfarin. Given lack of head-to-head comparisons of NOACs via use of randomized clinical trials, it becomes a clinical challenge to fully understand the risks or benefits of one NOAC over the other. Thus, ongoing research and network meta-analyses in VTE are necessary.
Disclosure
The author reports no conflicts of interest in this work.
References
Spencer FA, Emery C, Joffe SW, et al. Incidence rates, clinical profile, and outcomes of patients with venous thromboembolism. The Worcester VTE study. J Thromb Thrombolysis. 2009;28(4):401–409. | |
Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. Predictors of survival after deep vein thrombosis and pulmonary embolism: a population-based, cohort study. Arch Intern Med. 2009;159(5):445–453. | |
Hirsh J, Guyatt G, Albers GW, Harrington R, Schünemann HJ; American College of Chest Physicians. Antithrombotic and thrombolytic therapy: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest. 2008;133(6 Suppl):110S–112S. | |
Kearon C. Natural history of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):1–22. | |
Mayer RS, Streiff MB, Hobson DB, Halpert DE, Berenholtz SM. Evidence-based venous thromboembolism prophylaxis is associated with a six-fold decrease in numbers of symptomatic venous thromboembolisms in rehabilitation inpatients. PM R. 2011;3(12):1111–1115. | |
Cohen AT, Tapson VF, Bergmann JF, et al; ENDORSE Investigators. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371(9610):387–394. | |
Kearon C, Akl EA, Comerota AJ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):419S–494S. | |
Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2008;133(6 Suppl):160S–198S. | |
Eckman MH, Rosand J, Greenberg SM, Gage BF. Cost-effectiveness of using pharmacogenetic information in warfarin dosing for patients with nonvalvular atrial fibrillation. Ann Intern Med. 2009;150(2):73–83. | |
Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the euro heart survey. Chest. 2010;138(5):1093–1100. | |
Ost D, Tepper J, Mihara H, Lander O, Heinzer R, Fein A. Duration of anticoagulation following venous thromboembolism: a meta-analysis. JAMA. 2005;294(6):706–715. | |
Budnitz DS, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med. 2011;365(21):2002–2012. | |
Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):278S–325S. | |
Hull RD, Pineo GF, Francis C, et al. Low-molecular-weight heparin prophylaxis using dalteparin extended out-of-hospital vs in-hospital warfarin/out-of-hospital placebo in hip arthroplasty patients: a double-blind, randomized comparison. North American Fragmin trial investigators. Arch Intern Med. 2000;160(14):2208–2215. | |
Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2008;133(6 Suppl):381S–453S. | |
Wilke T, Moock J, Müller S, Pfannkuche M, Kurth A. Nonadherence in outpatient thrombosis prophylaxis with low molecular weight heparins after major orthopaedic surgery. Clin Orthop Relat Res. 2010;468(9):2437–2453. | |
Wilke T. Patient preferences for an oral anticoagulant after major orthopedic surgery: results of a German survey. Patient. 2009;2(1):39–49. | |
Eikelboom JW, Weitz JI. New anticoagulants. Circulation. 2010; 121(13):1523–1532. | |
Weitz JI. New oral anticoagulants: a view from the laboratory. Am J Hematol. 2012;87(S1):S133–S136. | |
Stangier J, Rathgen K, Stähle H, Gansser D, Roth W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br J Clin Pharmacol. 2007;64(3):292–303. | |
Blech S, Ebner T, Ludwig-Schwellinger E, Stangier J, Roth W. The metabolism and disposition of the oral direct thrombin inhibitor, dabigatran, in humans. Drug Metab Dispos. 2008;36(2):386–399. | |
Eisert WG, Hauel N, Stangier J, Wienen W, Clemens A, van Ryn J. Dabigatran: an oral novel potent reversible nonpeptide inhibitor of thrombin. Arterioscler Thromb Vasc Biol. 2010;30(10):1885–1889. | |
Walenga JM, Adiguzel C. Drug and dietary interactions of the new and emerging oral anticoagulants. Int J Clin Pract. 2010;64(7):956–967. | |
Pradaxa® (Dabigatran) Package Insert. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2013. | |
Eriksson BI, Dahl OE, Rosencher N, et al; RE-MODEL Study Group. Oral dabigatran etexilate vs subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trial. J Thromb Haemost. 2007;5(11):2178–2185. | |
Eriksson BI, Dahl OE, Rosencher N, et al; RE-NOVATE Study Group. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double-blind, non-inferiority trial. Lancet. 2007;370(9591):949–956. | |
Eriksson BI, Dahl OE, Huo MH, et al; RE-NOVATE II Study Group. Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty: a randomised, double-blind, non-inferiority trial. Thromb Haemost. 2011;105(4):721–729. | |
RE-MOBILIZE Writing Committee; Ginsberg JS, Davidson BL, et al. Oral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery. J Arthroplasty. 2009;24:1–9. | |
Friedman RJ, Dahl OE, Rosencher N, et al; RE-MOBILIZE, RE-MODEL, RE-NOVATE Steering Committees. Dabigatran versus enoxaparin for prevention of venous thromboembolism after hip or knee arthroplasty: a pooled analysis of three trials. Thromb Res. 2010;126(3):175–182. | |
Schulman S, Kearon C, Kakkar AK, et al; RE-COVER Study Group. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–2352. | |
Schulman S, Kakkar AK, Goldhaber SZ, et al; RE-COVER II Trial Investigators. Treatment of thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764–772. | |
Schulman S, Kearon C, Kakkar AK, et al; RE-SONATE Trial Investigators. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med. 2013;368(8):709–718. | |
Connolly SJ, Ezekowitz MD, Yusuf S, et al; RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139–1151. | |
Connolly SJ, Ezekowitz MD, Yusuf S, Reilly PA, Wallentin L. Newly identified events in the RE-LY trial. N Engl J Med. 2010;363(19):1875–1876. | |
Douxfils J, Buckinx F, Mullier F, et al. Dabigatran etexilate and risk of myocardial infarction, other cardiovascular events, major bleeding, and all-cause mortality: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. 2014;3(3):e000515. | |
Uchino K, Hernandez AV. Dabigatran association with higher risk of acute coronary events: meta-analysis of noninferiority randomized controlled trials. Arch Intern Med. 2012;172(5):397–402. | |
Mak KH. Coronary and mortality risk of novel oral antithrombotic agents: a meta-analysis of large randomised trials. BMJ Open. 2012;2(5):e001592. | |
University of Sao Paulo General Hospital. Effects of LMWH versus dabigatran on platelet aggregation in patients with stable coronary artery disease. In: ClinicalTrials.gov [Internet]. Bethesda, MD: National Library of Medicine (US); 2000 [cited April 20, 2015]. Available from: http://clinicaltrials.gov/show/NCT02389582. | |
Thorne KM, Dee S, Jayathissa S. Thrombotic events after discontinuing dabigatran: rebound or resumption? BMJ. 2012;345:e4469. | |
Van de Werf F, Brueckmann M, Connolly SJ. A comparison of dabigatran etexilate with warfarin in patients with mechanical heart valves: the randomized, phase II study to evaluate the safety and pharmacokinetics of oral dabigatran etexilate in patients after heart valve replacement (RE-ALIGN). Am Heart J. 2012;163(6):931–937. | |
Moore TJ, Cohen MR, Mattison DR. Dabigatran, bleeding, and the regulators. BMJ. 2014;349:g4517. | |
Reilly PA, Lehr T, Haertter S, et al; RE-LY Investigators. The effect of dabigatran plasma concentrations and patient characteristics on the frequency of ischemic stroke and major bleeding in atrial fibrillation patients: the RE-LY trial (randomized evaluation of long-term anticoagulation therapy). J Am Coll Cardiol. 2014;63(4):321–328. | |
van Ryn J, Stangier J, Haertter S, et al. Dabigatran etexilate-a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost. 2010;103(6):1116–1127. | |
van Ryn J, Grottke O, Spronk H. Measurement of dabigatran in standardly used clinical assays, whole blood viscoelastic coagulation, and thrombin generation assays. Clin Lab Med. 2014;34(3):479–501. | |
Hankey GJ, Eikelboom JW. Dabigatran etexilate: a new oral thrombin inhibitor. Circulation. 2011;123(13):1436–1450. | |
Herrmann RP. Assays for and reversal of new anticoagulants. In: ClinicalTrials.gov [Internet]. Bethesda, MD: National Library of Medicine (US); 2000 [cited April 20, 2015]. Available from: http://clinicaltrials.gov/show/NCT01795781. | |
Van Ryn J, Ruehl D, Priepke H, Hauel N, Wienen W. Reversibility of the anticoagulant effect of high doses of the direct thrombin inhibitor dabigatran, by recombinant factor VII. Haematologica. 2008; 93(Supple 1):148. | |
Eerenberg ES, Kamphuisen PW, Sijpkens MK, Meijers JC, Buller HR, Levi M. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011;124(14):1573–1579. | |
Schiele F, van Ryn J, Newsome C, et al. A specific antidote for dabigatran: functional and structural characterization. Blood. 2013; 121(18):3554–3562. | |
van Ryn J, Schmoll M, Pillu H, et al. Effect of Dabigatran on the Ability to Generate Fibrin At a Wound Site and its Reversal By Idarucizumab, the Antidote to Dabigatran, in Healthy Volunteers: An Exploratory Marker of Blood Loss. In: Presented on 18th November at the American Heart Association Scientific Sessions. Chicago, USA; 2014. | |
Ageno W, Gallus AS, Wittkowsky A, et al; American College of Chest Physicians. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):44S–88S. | |
Stangier J, Rathgen K, Stähle H, Mazur D. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate. Clin Pharmacokinet. 2010;49(4):259–268. | |
Knauf F, Chaknos CM, Berns JS, Perazella MA. Dabigatran and kidney disease: a bad combination. Clin J Am Soc Nephrol. 2013;8(9):1591–1597. | |
Chang DN, Dager WE, Chin AI. Removal of dabigatran by hemodialysis. Am J Kidney Dis. 2013;61(3):487–489. | |
Chan KE, Edelman ER, Wenger JB, Thadhani RI, Maddux FW. Dabigatran and rivaroxaban use in atrial fibrillation patients on hemodialysis. Circulation. 2015;131(11):972–979. | |
Roldán V, Marín F, Manzano-Fernández S, et al. The HAS-BLED score has better prediction accuracy for major bleeding than CHADS2 or CHA2DS2-VASc scores in anticoagulated patients with atrial fibrillation. J Am Coll Cardiol. 2013;62(23):2199–2204. | |
Capital District Health Authority. An evaluation of the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate in hemodialysis patients. In: ClinicalTrials.gov [Internet]. Bethesda, MD: National Library of Medicine (US); 2000 [cited April 20, 2015]. Available from: http://clinicaltrials.gov/show/NCT01590823. | |
Harper P, Young L, Merriman E. Bleeding risk with dabigatran in the frail elderly. N Engl J Med. 2012;366(9):864–866. | |
Geldhof V, Vandenbriele C, Verhamme P, Vanassche T. Venous thromboembolism in the elderly: efficacy and safety of non-VKA oral anticoagulants. Thromb J. 2014;12:21. | |
Graham DJ, Reichman ME, Wernecke M, et al. Cardiovascular, bleeding, and mortality risks in elderly Medicare patients treated with dabigatran or warfarin for non-valvular atrial fibrillation. Circulation. 2014;131:157–164. | |
Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;18:3078–3083. | |
Farge D, Debourdeau P, Beckers M, et al. International clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. J Thromb Haemost. 2013;11(1):56–70. | |
Schulman S, Goldhaber SZ, Kearon C, et al. Treatment with dabigatran or warfarin in patients with venous thromboembolism and cancer. Thromb Haemost. Epub March 5, 2015. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.