")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Current Advances in the Treatment of Fibrolamellar Carcinoma of Liver
Authors Gummadi J , Wang X, Xie C
Received 2 February 2023
Accepted for publication 5 April 2023
Published 15 May 2023 Volume 2023:10 Pages 745—752
DOI https://doi.org/10.2147/JHC.S406902
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Jörg Trojan
Jyotsna Gummadi,1 Xin Wang,2 Changqing Xie2,3
1Department of Medicine, MedStar Franklin Square Medical Center, Baltimore, MD, 21237, USA; 2Thoracic and GI Malignancies Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, 20814, USA; 3NCI CCR Liver Cancer Program, National Cancer Institute, National Institutes of Health, Bethesda, MD, 20814, USA
Correspondence: Changqing Xie, National Institute of Health, 10 Center Drive, Building 10 3B43, Bethesda, MD, 20892, USA, Email [email protected]
Abstract: Fibrolamellar carcinoma (FLC) of the liver is a rare type of liver cancer that is prevalent in children and young adults, often less than 40 years old. The etiology is unclear. It presents without underlying liver disease with distinctive histological features such as fibrous collagen bands surrounding the tumor cells. Fusion protein DNAJB1-PRKACA is found in most of the cases. The prognosis of FLC is poor. Even though curative treatment option is surgery for a certain patient population, other treatment modalities including radiation, chemotherapy are currently being used without significant improvement of overall survival. Recently, targeted therapy and immunotherapy have been studied which may provide survival advantage in the future. This review sought to compile data from clinical trials and case reports/series to outline the current state of FLC treatment.
Keywords: fibrolamellar carcinoma of liver, immunotherapy, target therapy
Introduction
In 1956, Edmondson was the first to describe fibrolamellar carcinoma (FLC) of the liver in a 14-year-old female patient with no underlying liver disease1 Currently, it is well-recognized that FLC is a rare subtype of liver cancer that mostly affects children and young adults, which accounts for 0.5–9% of primary liver cancers in various case series.2 It usually presents as a solitary mass in the liver, often diagnosed in individuals less than 40 years old and with a greater incidence in males.3–5 It differs from classical hepatocellular carcinoma (HCC) not only in the clinical, histological, but also molecular features. The etiology of FLC is largely unknown, typically arising in normal livers without any underlying liver fibrosis or cirrhosis with lack of alpha fetoprotein.6 Due to the scarcity of this tumor type, there is a lack of reports that accurately characterize patients with FLC as well as predictors of recurrence and survival. Previous studies have initially presumed focal nodular hyperplasia as a potential precursor lesion for FLC, however no causal relationship could be established.7 Multiple disease models have been established to illuminate pathological process of FLC and explore therapeutic targets.8
Although FLC has a low tumor mutation burden (TMB) with a median TMB of 1.85 mut/MB (range 0–6 mut/MB),9 the presence of a fusion protein encoded by DNAJB1-PRKACA has been found in the majority of FLC patients.10 This fusion protein results in increased protein kinase A activity through the dysregulation of catalytic PRKACA.10,11 Further, these changes cause dysfunction of c-Myc and ornithine decarboxylase, resulting in the depletion of amino acids crucial to the urea cycle.12 Dysfunction of the urea cycle in turn causes accumulation of ammonia and hyperammonemia. However, when these symptoms are treated with routine therapies for cirrhotic patients with hepatic encephalopathy, these patients tend to not respond. To reconfirm the role of DNAJB1-PRKACA, Engelholm et al used CRISPR/Cas9 to induce formation of the DNAJB1-PRKACA fusion gene in wild-type mice. This mouse model produced tumors with similar features to human FLC, but human carcinogenesis may be more complex than previously thought.13 Interestingly, another theory revolves around the Carney complex where certain cases of FLC do not have the characteristic DNAJB1-PRKACA fusion gene that is seen in sporadic FLC.11 Thus, this indicates the presence of an alternative molecular culprit other than the DNAJB1-PRKACA fusion gene for the formation of FLC. Beside the occurrence of this fusion gene, several other molecular/genetic changes in FLC were noted, including activating promoter mutation of TERT,14 mutation of MUC415 and BRAC2,16 19p13.1 focal deletion,16 and overexpression of LINC00473, CA12,17 and MDM4.18
Histologically, FLC is characterized by nests of large tumor cells with distinct granular eosinophilic cytoplasm, a prominent nucleoli encased within fibrous lamellar collagen bands and intratumoral fibrosis.19 FLC commonly expresses cytokeratin7 and CD68.20,21 Additionally, very limited immunological features have been characterized for FLC. One report showed negative programmed death-ligand 1 (PD-L1) expression among 11 patients through immunohistochemistry (IHC) staining.9 However, another study looked at two surgically resected samples which were treated with neoadjuvant f-fluorouracil and interferon prior to surgery and found that the resected samples had low expression for immune cell exhaustion markers, which included 5–6% positivity of programmed cell death protein 1 (PD-1) expression, 3–4% positivity of PD-L1 expression, 0.3–1% positivity of FoxP3 and 0.2–1% positivity of inducible costimulatory (ICOS) among total cells.22 The discordant expression of PD-L1 between FLC studies may be attributed to differing methods of processing samples.
Due to the significant histologic differences between HCC and FLC, histologic confirmation is necessary to properly diagnose FLC. In conjunction, core biopsies are recommended over fine-needle aspiration for percutaneous biopsies because malignant hepatocytes may be aspirated without collection of the distinctive fibrotic lamellae, resulting in misdiagnosis of FLC as HCC.23 Moreover, molecular testing for PRKACA gene rearrangement with fluorescence in situ hybridization (FISH) may provide more evidence for a definitive diagnosis in some cases.24
The overall prognosis of FLC is greater than conventional HCC.25 One and 5-year cause-specific survivals for FLC were 72.0% and 37.3%, respectively, with a median overall survival (OS) of 32.9 months.5 It was reported that the 5-year OS rate of all FLC patients was 40.3%, while those who were eligible for surgical resection had a 5 year OS rate of 60.7%.4 Patient age was the largest predictor of OS, followed by surgery, and tumor stage.4 High risk prognostic factors include vascular infiltration, a tumor size >7 cm, multifocality, lymph node positivity, multiple liver tumors, and metastases.26 Recently treatment of classic HCC, including immunotherapy, has made great progress in improving HCC patient survival.27–30 However, given the intrinsic significant difference of etiology, pathogenesis and molecular pattern between classic HCC and FLC, FLC is usually excluded from clinical trials designed for HCC.8
For FLC patients with early stage disease where the tumor is confined to the liver, curative treatment options include surgical resection or liver transplant. Even though more patients are diagnosed at advanced stages, curative treatment options can be offered to up to 70% of patients.23 For patients presenting with late or advanced stage of disease where FLC is unresectable, multimodality treatment can be effective. There is a lack of large-scale randomized controlled studies ascribable to disease rarity, this emphasizes the need for more standardized systemic therapeutic options. Most of the systemic treatments that are currently being used are extrapolated from sporadic case reports, where patients were treated with different systemic agents, case series, or based on established treatment for advanced HCC even though both types of cancer vary significantly. Thus, this review sought to cover recent advancements in treatment modalities reported by different case reports, research papers, and clinical trials in patients with FLC.
Surgery
Common surgical treatment modalities for FLC include partial/complete hepatectomy or liver transplantation. Previous studies have indicated that more than 70% of patients require a major hepatectomy, including hemihepatectomy or extended hepatectomy, while about 24% of patients undergo a partial or minor hepatectomy.31 A meta-analysis of 17 studies and 368 patients with FLH showed a significant increase in the mean OS for patients with FLC compared to those with non-FLC (84.9 vs 42.9 months), who underwent partial hepatectomy.31 Additionally, 30–60% of patients were noted to have lymph node involvement on presentation, thus a complete periportal lymphadenectomy must be performed routinely for all FLC patients.31 A complete resection (R0) was found to significantly improve OS.31,32 Therefore, unifocal masses confined to the liver should be pursued with the aim of R0 resection. For advanced stage FLC patients, 18–50% presented with regional lymph node involvement and 30–40% with distant metastasis.33–35 Nevertheless, regional lymph node involvement was found to be an independent risk factor36 and suggests that additional lymph node dissection may be beneficial. Although neoadjuvant/adjuvant chemotherapy has been used broadly for patients with gastrointestinal malignancy managed with surgical resection, there has not been a study that demonstrates how neo-adjuvant/adjuvant systemic therapy has improved survival for patients with surgically excised FLC.23,37
Up to 86% of patients will have disease recurrence following resection.38 The indolent nature of FLC allows for additional surgical resection of recurrent lesions. Surgical removal of recurrent FLC results in a greater median OS over 120 months compared to 35 months without subsequent surgeries.38,39
For certain patients who present with hyperammonemic encephalopathy derived from FLC, successful management of hyperammonemia with surgical debulking of FLC tumors is feasible, as described in case reports where hyperammonemia was medically managed simultaneously.40
Liver transplantation remains an option for select patients with unresectable FLC without extrahepatic disease. However, due to the rarity of FLC, there is a lack of robust evidence supporting liver transplantation as a beneficial treatment option. Most of the evidence is derived from small case reports and case series reporting improved outcomes of FLC patients who underwent liver transplantation. In a retrospective study following 13 advanced stage FLC patients who underwent liver transplantation, the mean OS ranged from 34 months to 120 months depending on tumor size, numbers, distribution, surgical margin positivity, lymph node positivity, vascular invasion, TNM stage, and adjuvant chemotherapy/radiation.41 A systematic review of a total of 35 series and 575 FLC patients showed 23% patients underwent liver transplantation and the 5 year survival ranged from 29 to 55%.42 Another systematic review of a total of 17 studies and 368 FLC patients demonstrated liver transplantation obtained mean OS of 47.5 months.43 Lastly, an analysis of the United Network of Organ Sharing (UNOS) database between October 1988 and January 2013 showed the OS for FLC patients who underwent liver transplantation at 1, 3, and 5 years was 96%, 80%, and 48% respectively.44 Therefore, these studies indicate that liver transplantation may be a potential option for patients with advanced FLC.
Chemotherapy
Although FLC is not a chemo-sensitive malignancy given the reported modest or lack of therapeutic effect in patients, chemotherapy has still been used for resectable disease in both neoadjuvant and adjuvant setting or advanced disease. A few studies have reported limited efficacy with cisplatin/5-fluorouracil/vincristine, cisplatin/doxorubicin, carboplatin/doxorubicin/cisplatin, and gemcitabine/oxaliplatin.45,46 Platinum-based chemotherapy in pediatric patients with FLC resulted in a partial response in 31% of patients upon imaging and a 3-year survival of only 22%.45 Some studies have reported that patients who have undergone chemotherapy in both neoadjuvant and adjuvant settings fared better than those with surgery alone, with patients who had front-line surgery followed by chemotherapy having the longest OS.47,48 A Phase II prospective trial showed the combination of fluorouracil and recombinant interferon alfa-2b (rIFNalpha2b) obtained a median OS of 23.1 months where one patient had a complete response and four patients had partial response. Thus this indicates an improved efficacy for chemotherapy by synergistically combining other therapeutic agents.48 With the addition of nivolumab, the overall objective response reached 50% and had a median progression-free survival (PFS) of 9 months.49 Further large, prospective clinical trials are warranted, and several studies are currently investigating different combinations of chemotherapy in patients with FLC (Table 1).
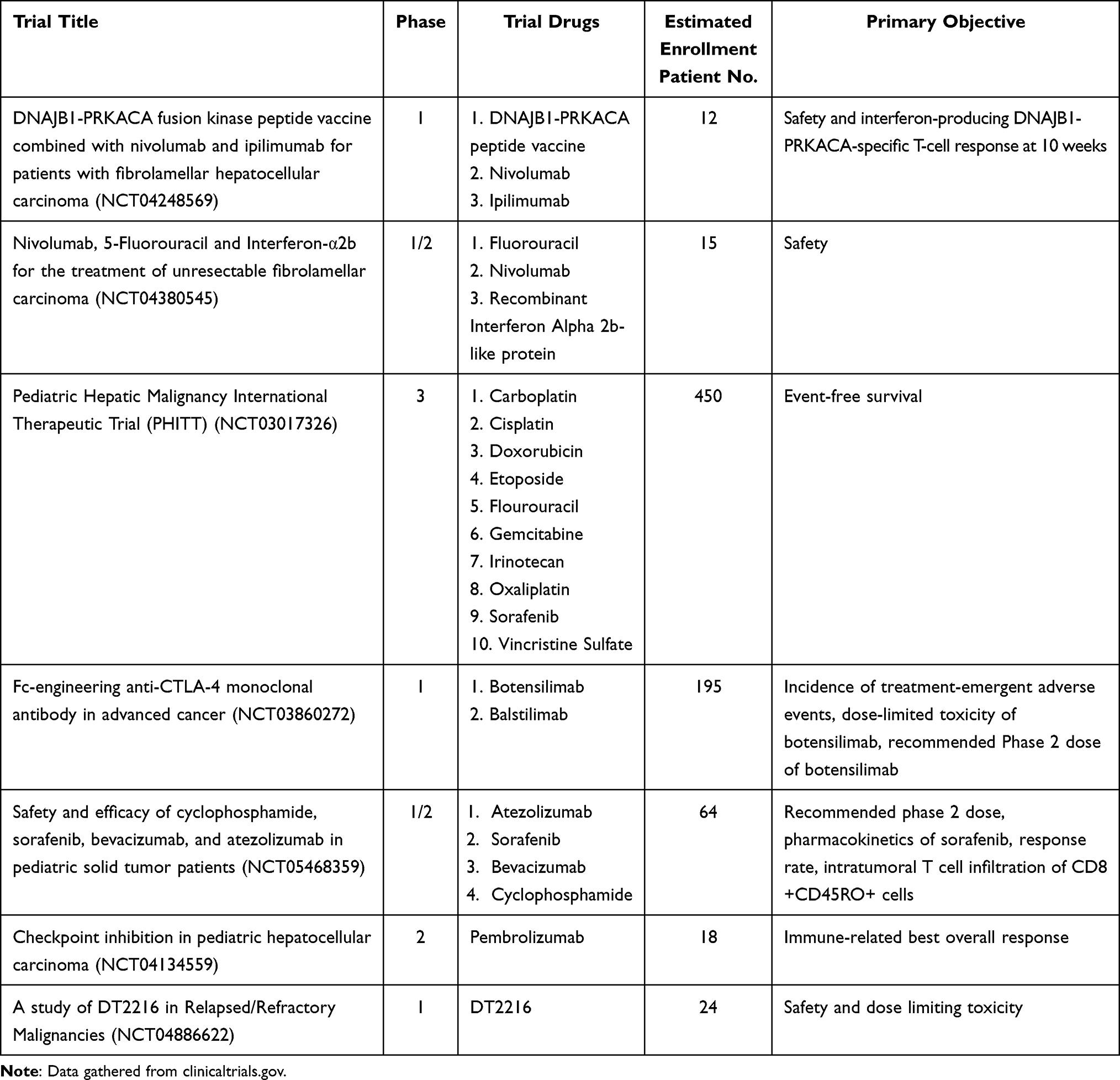 |
Table 1 Currently Recruiting Clinical Trials for Fibrolamellar Carcinoma |
Radiation/Locoregional Therapy
Radiation to the liver or metastatic lesions has been used for FLC patients who are not eligible for surgical resection or liver transplantation.50 Recent development in stereotactic body radiotherapy has been shown to be effective and a well tolerated therapeutic tool for inoperable liver malignancies,51 suggesting that this form of therapy can be extended to FLC patients. Moreover, radiation can also be combined with other modalities to better treat FLC. In a 2000–2016 observational study from SEER (Surveillance, epidemiology, end results registry), 3.0% of FLC patients underwent triple therapy (surgery, radiation, and chemotherapy).5 Other locoregional therapies have been used as either a strategy for definitive local control or a bridge to surgical resection. One such option for unresectable FLC is transarterial radioembolization with yttrium-90 (TARE-Y90)52–54 and has been reported to have a median survival of 4 months with some patients undergoing multiple rounds of treatment.53 Another option is transarterial chemoembolization (TACE), which is one of the mainstream treatments for conventional HCC, and it has been reported to be used in combination with other treatment modalities in patients with FLC.52–54
Immunotherapy
Although there are limited clear immunological features in FLC, immunotherapy remains a promising avenue for treatment of this rare liver malignancy.22 The earliest active immune agent used in FLC treatment regimens was rIFNalpha2b combined with chemotherapy,48 which showed promising efficacy. However, the addition of nivolumab to this combination failed to elicit any additional benefits.49 Recently, atezolizumab and bevacizumab were approved for the treatment of unresectable HCC based on the IMBrave150 trial, which demonstrated that this combination greatly improved patient survival when compared to sorafenib.55 FLC patients were excluded from this trial. The combination of atezolizumab and bevacizumab was used in two Arab patients with advanced FLC. Unfortunately, the treatment did not show any clinical benefits.56 Several case reports have shown the potential efficacy of immunotherapy in FLC, either with pembrolizumab,57 nivolumab monotherapy,58 or combining nivolumab and ipilimumab.59 There was a retrospective cohort study of patients with FLC identified using the Johns Hopkins Liver Cancer Database, the UT Southwestern Medical Center Liver Cancer Database, and the Fibrolamellar Registry. This study was designed to test safety and efficacy of immune checkpoint inhibitors (ICIs) in FLC. Among the 19 patients who met the eligibility criteria, the objective response rate of ICI treatment in FLC was 15.8% and median PFS and OS were 5.5 and 26.0 months, respectively. Though the data indicate treatment of FLC with ICIs produces modest efficacy, this study suggests that ICIs do have single agent activity in the context of FLC with durable partial responses observed in 2/15 (13.3%) patients who received ICIs alone. The limited response of ICIs-alone treatments described in this study was thought to be likely due to the intrinsic tumor characteristics of FLC, which include low immunogenicity due to low TMB and negative to low PD-L1 expression status, and other undefined immunosuppressive features. Additional combinations are needed and may enhance the antitumor response (Table 1).
Targeted Therapy
Small molecule inhibitors have been increasingly approved in the treatment of various cancers, either alone or in combination with other therapeutic modalities. However, the trials focusing on FLC treated with targeting agents have been largely unsuccessful, which included mTOR inhibitors with/without estrogen derivation therapy,60 anti-Aurora kinase A ENMD-2076 monotherapy,61 and EGFR inhibitor neratinib monotherapy.62 Further research is needed to develop efficacious targeted therapeutic options. Several potential targets have been studied in FLC, eg, BCL-XL and PRKACA, and the list of these targets is expanding.63
DNAJB1-PRKACA
Given the observed increased protein kinase A activity in FLC which is triggered by the DNAJB1-PRKACA fusion protein, protein kinase inhibitors, especially inhibition of cAMP-activated catalytic subunit alpha (PRKACA), have been of great interest to treat FLC. A recent study demonstrated antitumor activity in an FLC preclinical model treated with synthesized DS89002333, a novel PRKACA inhibitor.64 DS89002333 showed potent PRKACA inhibitor activity and inhibited fusion protein-dependent cell growth both in vitro and in vivo. In an FLC patient-derived xenograft model expressing the DNAJB1-PRKACA fusion gene, the inhibitor also showed antitumor activity, suggesting that DS89002333 may be an effective treatment for FLC patients (Table 1). Another study showed that use of short hairpin RNAs (shRNA) has minimal effects on the wildtype DNAJB1 or PRKACA but is able to inhibit the chimeric transcript and protein.65 Knockdown of the chimera though this shRNA resulted in cell death of FLC cells in vitro and in vivo, but this was not found to be successful in an HCC model that artificially expressed the chimera protein. Furthermore, vaccination of an FLA patient using HLA-presented neoantigens specific for DNAJB1-PRKACA fusion transcript reached a durable response and relapse-free survival for more than 21 months post-vaccination. This study suggest that DNAJB1-PRKACA is a promising therapeutic target, and a new clinical trial with the vaccine is currently under clinical investigation (NCT04248569) (Table 1).
BCL-Xl
Previous studies have found that BCL-XL transcripts were increased 83% compared to adjacent normal liver tissue in FLC. Some treatment-resistant patient-derived xenografts showed increased BCL-XL expression of up to 160% when compared to adjacent normal liver tissue. This finding has led to reprocessing of drug screens and identified dual inhibition of TOPO1 with irinotecan and BCL-XL with DT2216 as applicable options to treat FLC.66 DT2216 synergizes with HDAC inhibitors fimepinostat and panobinostat as well as the TOPO1 inhibitor SN38. The preclinical study investigating this combination has shown durable tumor control. It was anticipated that possible predictive biomarkers of this response to this combination treatment could be tumoral levels of UGT1A1 and BCL-XL. Currently, there is an ongoing clinical trial to test the therapeutic modality in FLC patients (NCT04886622) (Table 1).
Future Direction
FLC is a rare liver malignancy, with many distinguishing features that set it apart from conventional HCC. Given the lack of treatment options, the survival rate of FLC is poor, though certain patients have been shown to significantly benefit from surgical resection and liver transplantation. Studies focusing on traditional chemotherapy, targeted therapy, and immunotherapy have been discouraging, however, combinational approaches have been met with more success. Nevertheless, with established preclinical screening platforms and the discovery of multiple potential agents,63 further future testing/prospective clinical trials are warranted,8 and stratification of the patient population in such trials would be beneficial. Lastly, recent developments in single cell RNA sequencing and omics technology can provide novel insight into FLC tumor biology and tumor microenvironment, while simultaneously exploring potential targets.
Abbreviations
FISH, fluorescence in situ hybridization; FLC, fibrolamellar cancer; HCC, hepatocellular carcinoma; ICI, immune checkpoint inhibitor; ICOS, inducible costimulatory; IHC, immunohistochemistry; OS, overall survival; PD-1, programmed cell death protein-1; PD-L1, programmed death-ligand-1; PFS, progression-free survival; PRKACA, protein kinase cAMP-activated catalytic subunit alpha; SEER, Surveillance, epidemiology, end results registry; shRNA, short hairpin RNA; TMB, tumor mutation burden.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
C.X is supported by the Physician-Scientist Early Investigator Program at National Cancer Institute, National Institute of Health (ZIA BC 011888).
Disclosure
The authors declare no conflict of interest.
References
1. Edmondson HA. Differential diagnosis of tumors and tumor-like lesions of liver in infancy and childhood. AMA J Dis Child. 1956;91:168–186. doi:10.1001/archpedi.1956.02060020170015
2. Limaiem F, Bouhamed M, Sahraoui G, et al. Hepatocellular carcinoma: a clinicopathological study of 64 cases. Pan Afr Med J. 2017;27:41. doi:10.11604/pamj.2017.27.41.9584
3. Eggert T, McGlynn KA, Duffy A, et al. Epidemiology of fibrolamellar hepatocellular carcinoma in the USA, 2000-10. Gut. 2013;62:1667–1668. doi:10.1136/gutjnl-2013-305164
4. Polychronidis G, Feng J, Murtha-Lemekhova A, et al. Factors influencing overall survival for patients with fibrolamellar hepatocellular carcinoma: analysis of the surveillance, epidemiology, and end results database. Int J Gen Med. 2022;15:393–406. doi:10.2147/IJGM.S338066
5. Ramai D, Ofosu A, Lai JK, et al. Fibrolamellar hepatocellular carcinoma: a population-based observational study. Dig Dis Sci. 2021;66(1):308–314. doi:10.1007/s10620-020-06135-3
6. Lafaro KJ, Pawlik TM. Fibrolamellar hepatocellular carcinoma: current clinical perspectives. J Hepatocell Carcinoma. 2015;2:151–157. doi:10.2147/JHC.S75153
7. Lemekhova A, Hornuss D, Polychronidis G, et al. Clinical features and surgical outcomes of fibrolamellar hepatocellular carcinoma: retrospective analysis of a single-center experience. World J Surg Oncol. 2020;18:93. doi:10.1186/s12957-020-01855-2
8. Dinh TA, Utria AF, Barry KC, et al. A framework for fibrolamellar carcinoma research and clinical trials. Nat Rev Gastroenterol Hepatol. 2022;19:328–342. doi:10.1038/s41575-022-00580-3
9. Chen KY, Popovic A, Hsiehchen D, et al. Clinical outcomes in fibrolamellar hepatocellular carcinoma treated with immune checkpoint inhibitors. Cancers. 2022;14(21):5347. doi:10.3390/cancers14215347
10. Honeyman JN, Simon EP, Robine N, et al. Detection of a recurrent DNAJB1-PRKACA chimeric transcript in fibrolamellar hepatocellular carcinoma. Science. 2014;343:1010–1014. doi:10.1126/science.1249484
11. Graham RP, Lackner C, Terracciano L, et al. Fibrolamellar carcinoma in the Carney complex: PRKAR1A loss instead of the classic DNAJB1-PRKACA fusion. Hepatology. 2018;68:1441–1447. doi:10.1002/hep.29719
12. Surjan RCT, Santos ESD, Silveira SDP, et al. Fibrolamellar hepatocellular carcinoma-related hyperammonemic encephalopathy: up to now and next steps. Clin Mol Hepatol. 2020;26:231–232. doi:10.3350/cmh.2019.0084
13. Vyas M, Hechtman JF, Zhang Y, et al. DNAJB1-PRKACA fusions occur in oncocytic pancreatic and biliary neoplasms and are not specific for fibrolamellar hepatocellular carcinoma. Mod Pathol. 2020;33(4):648–656. doi:10.1038/s41379-019-0398-2
14. El Dika I, Bowman AS, Berger MF, et al. Molecular profiling and analysis of genetic aberrations aimed at identifying potential therapeutic targets in fibrolamellar carcinoma of the liver. Cancer. 2020;126:4126–4135. doi:10.1002/cncr.32960
15. Darcy DG, Chiaroni-Clarke R, Murphy JM, et al. The genomic landscape of fibrolamellar hepatocellular carcinoma: whole genome sequencing of ten patients. Oncotarget. 2015;6:755–770. doi:10.18632/oncotarget.2712
16. Cornella H, Alsinet C, Sayols S, et al. Unique genomic profile of fibrolamellar hepatocellular carcinoma. Gastroenterology. 2015;148:806–18.e10. doi:10.1053/j.gastro.2014.12.028
17. Dinh TA, Sritharan R, Smith FD, et al. Hotspots of aberrant enhancer activity in fibrolamellar carcinoma reveal candidate oncogenic pathways and therapeutic vulnerabilities. Cell Rep. 2020;31:107509. doi:10.1016/j.celrep.2020.03.073
18. Karki A, Putra J, Kim SS, et al. MDM4 expression in fibrolamellar hepatocellular carcinoma. Oncol Rep. 2019;42:1487–1496. doi:10.3892/or.2019.7241
19. Lim II, Farber BA, LaQuaglia MP. Advances in fibrolamellar hepatocellular carcinoma: a review. Eur J Pediatr Surg. 2014;24:461–466. doi:10.1055/s-0034-1396420
20. Ross HM, Daniel HD, Vivekanandan P, et al. Fibrolamellar carcinomas are positive for CD68. Mod Pathol. 2011;24:390–395. doi:10.1038/modpathol.2010.207
21. Ward SC, Huang J, Tickoo SK, et al. Fibrolamellar carcinoma of the liver exhibits immunohistochemical evidence of both hepatocyte and bile duct differentiation. Mod Pathol. 2010;23(9):1180–1190. doi:10.1038/modpathol.2010.105
22. Akce M, Vence LM, Blando JM, et al. Immune analysis of fibrolamellar hepatocellular carcinoma. J Clin Oncol. 2017;35:324. doi:10.1200/JCO.2017.35.4_suppl.324
23. Abdelhamed W, El-Kassas M. Fibrolamellar hepatocellular carcinoma: a rare but unpleasant event. World J Gastrointest Oncol. 2022;14:1103–1114. doi:10.4251/wjgo.v14.i6.1103
24. Graham RP, Yeh MM, Lam-Himlin D, et al. Molecular testing for the clinical diagnosis of fibrolamellar carcinoma. Mod Pathol. 2018;31:141–149. doi:10.1038/modpathol.2017.103
25. Smith M, Tomboc PJ, Markovich B. Fibrolamellar Hepatocellular Carcinoma. Treasure Island (FL): StatPearls; 2022.
26. Berkovitz A, Migler RD, Qureshi A, et al. Clinical and demographic predictors of survival for fibrolamellar carcinoma patients—A patient community, registry-based study. Hepatol Commun. 2022;6(12):3539–3549. doi:10.1002/hep4.2105
27. Di Federico A, Rizzo A, Carloni R, et al. Atezolizumab-bevacizumab plus Y-90 TARE for the treatment of hepatocellular carcinoma: preclinical rationale and ongoing clinical trials. Expert Opin Investig Drugs. 2022;31:361–369. doi:10.1080/13543784.2022.2009455
28. Rizzo A, Cusmai A, Gadaleta-Caldarola G, et al. Which role for predictors of response to immune checkpoint inhibitors in hepatocellular carcinoma? Expert Rev Gastroenterol Hepatol. 2022;16:333–339. doi:10.1080/17474124.2022.2064273
29. Rizzo A, Ricci AD, Di Federico A, et al. Predictive biomarkers for checkpoint inhibitor-based immunotherapy in hepatocellular carcinoma: where do we stand? Front Oncol. 2021;11:803133. doi:10.3389/fonc.2021.803133
30. Viscardi G, Tralongo AC, Massari F, et al. Comparative assessment of early mortality risk upon immune checkpoint inhibitors alone or in combination with other agents across solid malignancies: a systematic review and meta-analysis. Eur J Cancer. 2022;177:175–185. doi:10.1016/j.ejca.2022.09.031
31. Chaudhari VA, Khobragade K, Bhandare M, et al. Management of fibrolamellar hepatocellular carcinoma. Chin Clin Oncol. 2018;7(5):51. doi:10.21037/cco.2018.08.08
32. Darcy DG, Malek MM, Kobos R, et al. Prognostic factors in fibrolamellar hepatocellular carcinoma in young people. J Pediatr Surg. 2015;50:153–156. doi:10.1016/j.jpedsurg.2014.10.039
33. Stipa F, Yoon SS, Liau KH, et al. Outcome of patients with fibrolamellar hepatocellular carcinoma. Cancer. 2006;106:1331–1338. doi:10.1002/cncr.21703
34. Kakar S, Burgart LJ, Batts KP, et al. Clinicopathologic features and survival in fibrolamellar carcinoma: comparison with conventional hepatocellular carcinoma with and without cirrhosis. Mod Pathol. 2005;18(11):1417–1423. doi:10.1038/modpathol.3800449
35. Wahab MA, El Hanafy E, El Nakeeb A, et al. Clinicopathological features and surgical outcome of patients with fibrolamellar hepatocellular carcinoma (experience with 22 patients over a 15-year period). World J Gastrointest Surg. 2017;9(2):61–67. doi:10.4240/wjgs.v9.i2.61
36. Schultz SP, Holtestaul T, Marenco CW, et al. Prognostic role of lymph node sampling in adolescent and young adults with fibrolamellar carcinoma. J Surg Res. 2022;276:261–271. doi:10.1016/j.jss.2022.03.006
37. Polychronidis G, Murtha-Lemekhova A, Fuchs J, et al. A multidisciplinary approach to the management of fibrolamellar carcinoma: current perspectives and future prospects. Onco Targets Ther. 2022;15:1095–1103. doi:10.2147/OTT.S296127
38. Yamashita S, Vauthey JN, Kaseb AO, et al. Prognosis of fibrolamellar carcinoma compared to non-cirrhotic conventional hepatocellular carcinoma. J Gastrointest Surg. 2016;20:1725–1731. doi:10.1007/s11605-016-3216-x
39. Kassahun WT. Contemporary management of fibrolamellar hepatocellular carcinoma: diagnosis, treatment, outcome, prognostic factors, and recent developments. World J Surg Oncol. 2016;14:151. doi:10.1186/s12957-016-0903-8
40. Solipuram V, Baretti M, Kim AY, et al. Surgical debulking for refractory hyperammonemic encephalopathy in fibrolamellar hepatocellular carcinoma. Hepatology. 2021;74:2899–2901. doi:10.1002/hep.31998
41. Pinna AD, Iwatsuki S, Lee RG, et al. Treatment of fibrolamellar hepatoma with subtotal hepatectomy or transplantation. Hepatology. 1997;26:877–883. doi:10.1002/hep.510260412
42. Mavros MN, Mayo SC, Hyder O, et al. A systematic review: treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma. J Am Coll Surg. 2012;215(6):820–830. doi:10.1016/j.jamcollsurg.2012.08.001
43. Njei B, Konjeti VR, Ditah I. Prognosis of patients with fibrolamellar hepatocellular carcinoma versus conventional hepatocellular carcinoma: a systematic review and meta-analysis. Gastrointest Cancer Res. 2014;7:49–54.
44. Atienza LG, Berger J, Mei X, et al. Liver transplantation for fibrolamellar hepatocellular carcinoma: a national perspective. J Surg Oncol. 2017;115:319–323. doi:10.1002/jso.24515
45. Weeda VB, Murawski M, McCabe AJ, et al. Fibrolamellar variant of hepatocellular carcinoma does not have a better survival than conventional hepatocellular carcinoma – results and treatment recommendations from the Childhood Liver Tumour Strategy Group (SIOPEL) experience. Eur J Cancer. 2013;49:2698–2704. doi:10.1016/j.ejca.2013.04.012
46. Gras P, Truant S, Boige V, et al. Prolonged complete response after GEMOX chemotherapy in a patient with advanced fibrolamellar hepatocellular carcinoma. Case Rep Oncol. 2012;5:169–172. doi:10.1159/000338242
47. Kaseb AO, Shama M, Sahin IH, et al. Prognostic indicators and treatment outcome in 94 cases of fibrolamellar hepatocellular carcinoma. Oncology. 2013;85:197–203. doi:10.1159/000354698
48. Patt YZ, Hassan MM, Lozano RD, et al. Phase II trial of systemic continuous fluorouracil and subcutaneous recombinant interferon Alfa-2b for treatment of hepatocellular carcinoma. J Clin Oncol. 2003;21:421–427. doi:10.1200/JCO.2003.10.103
49. Gottlieb S, O’Grady C, Gliksberg A, et al. Early experiences with triple immunochemotherapy in adolescents and young adults with high-risk fibrolamellar carcinoma. Oncology. 2021;99(5):310–317. doi:10.1159/000513358
50. Peacock JG, Call JA, Olivier KR. Radiotherapy for metastatic fibrolamellar hepatocellular carcinoma. Rare Tumors. 2013;5:e28. doi:10.4081/rt.2013.e28
51. Yeung R, Beaton L, Rackley T, et al. Stereotactic body radiotherapy for small unresectable hepatocellular carcinomas. Clin Oncol. 2019;31:365–373. doi:10.1016/j.clon.2019.01.012
52. Mafeld S, French J, Tiniakos D, et al. Fibrolamellar hepatocellular carcinoma: treatment with Yttrium-90 and subsequent surgical resection. Cardiovasc Intervent Radiol. 2018;41:816–820. doi:10.1007/s00270-018-1903-6
53. Aguado A, Ristagno R, Towbin AJ, et al. Transarterial radioembolization with yttrium-90 of unresectable primary hepatic malignancy in children. Pediatr Blood Cancer. 2019;66:e27510. doi:10.1002/pbc.27510
54. Hawkins CM, Kukreja K, Geller JI, et al. Radioembolisation for treatment of pediatric hepatocellular carcinoma. Pediatr Radiol. 2013;43(7):876–881. doi:10.1007/s00247-012-2568-y
55. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382:1894–1905. doi:10.1056/NEJMoa1915745
56. Al Zahrani A, Alfakeeh A. Fibrolamellar hepatocellular carcinoma treated with atezolizumab and bevacizumab: two case reports. J Med Case Rep. 2021;15:132. doi:10.1186/s13256-021-02695-8
57. Bauer U, Mogler C, Braren RF, et al. Progression after immunotherapy for fibrolamellar carcinoma. Visceral Med. 2019;35:39–42. doi:10.1159/000497464
58. Chakrabarti S, Tella SH, Kommalapati A, et al. Clinicopathological features and outcomes of fibrolamellar hepatocellular carcinoma. J Gastrointest Oncol. 2019;10:554–561. doi:10.21037/jgo.2019.01.35
59. Berger R, Dinstag G, Tirosh O, et al. Fibrolamellar carcinoma transcriptomic-based treatment prediction: complete response after nivolumab and ipilimumab. J Immunother Cancer. 2022;10(12):e005620. doi:10.1136/jitc-2022-005620
60. El Dika I, Mayer RJ, Venook AP, et al. A multicenter randomized three‐arm Phase II study of (1) Everolimus, (2) Estrogen Deprivation Therapy (EDT) with Leuprolide + Letrozole, and (3) Everolimus + EDT in patients with unresectable fibrolamellar carcinoma. Oncologist. 2020;25:925–e1603. doi:10.1634/theoncologist.2020-0367
61. Abou-Alfa GK, Mayer R, Venook AP, et al. Phase II multicenter, open-label study of oral ENMD-2076 for the treatment of patients with advanced fibrolamellar carcinoma. Oncologist. 2020;25:e1837–e1845. doi:10.1634/theoncologist.2020-0093
62. Abou-Alfa GK, Meyer T, Zhang J, et al. Evaluation of neratinib (N), pembrolizumab (P), everolimus (E), and nivolumab (V) in patients (pts) with fibrolamellar carcinoma (FLC). J Clin Oncol. 2021;39:310. doi:10.1200/JCO.2021.39.3_suppl.310
63. Lalazar G, Requena D, Ramos-Espiritu L, et al. Identification of novel therapeutic targets for fibrolamellar carcinoma using patient-derived xenografts and direct-from-patient screening. Cancer Discov. 2021;11:2544–2563. doi:10.1158/2159-8290.CD-20-0872
64. Toyota A, Goto M, Miyamoto M, et al. Novel protein kinase cAMP-Activated Catalytic Subunit Alpha (PRKACA) inhibitor shows anti-tumor activity in a fibrolamellar hepatocellular carcinoma model. Biochem Biophys Res Commun. 2022;621:157–161. doi:10.1016/j.bbrc.2022.07.008
65. Neumayer C, Ng D, Jiang CS, et al. Oncogenic addiction of Fibrolamellar hepatocellular carcinoma to the fusion kinase DNAJB1-PRKACA. Clin Cancer Res. 2022;29(1):271–278.
66. Shebl B, Ng D, Lalazar G, et al. Targeting BCL-XL in fibrolamellar hepatocellular carcinoma. JCI Insight. 2022;7. doi:10.1172/jci.insight.161820
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.