")
Back to Journals » International Journal of Women's Health » Volume 15
Cultural Adaptation and Validation of the Amharic Version of the World Health Organization’s Self Reporting Questionnaire (SRQ-20) Screening Tool Among Pregnant Women in North West Ethiopia, 2022: A Psychometric Validation
Authors Kurbi HA , Abebe SM , Mengistu NW, Ayele TA, Toni AT
Received 13 January 2023
Accepted for publication 5 May 2023
Published 18 May 2023 Volume 2023:15 Pages 779—791
DOI https://doi.org/10.2147/IJWH.S402865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Helina Abebe Kurbi,1,2 Solomon Mekonnen Abebe,3 Nestanet Worku Mengistu,3 Tadesse Awoke Ayele,1 Alemayehu Teklu Toni4
1Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Kotebe Metropolitan University, Menelik II Health Science College, Department of Mental Health, Addis Ababa, Ethiopia; 3Department of Nutrition institute of public health, college of medicine and health sciences, university of Gondar, Gondar, Ethiopia; 4Department of Pediatrics and School of Medicine, Institute of Public health, college of Medicine and health sciences, university of Gondar, Gondar, Ethiopia
Correspondence: Helina Abebe Kurbi, Email [email protected]
Background: The prevalence of prenatal common mental disorders afflicting the global community, including Ethiopia, is thriving. Therefore, a time-efficient and valid screening tool is required. This study aimed to culturally adapt and validate the self-reporting questionnaire-20 tool developed by the World Health Organization among pregnant mothers in Ethiopia.
Methods: A total of 310 pregnant women completed the questionnaire at two selected health centers in the regional state of Amhara. The World Health Organization’s Self Reporting Questionnaire-20 tool was first translated into Amharic by two experts. The back translation was done by two English experts. Internal consistency and reliability were assessed using Cronbach’s alpha. Convergent and discriminant validity were assessed using composite reliability and extracted mean variance. SRQ-20 was tested for reliability and validity using principal components analysis and the Kaiser-Meyer-Olkin measure of sample adequacy with a cutoff value of 0.50 for each item.
Results: The Kaiser-Meyer-Olkin measure (KMO = 0.733) for sample adequacy and the Bartlett’s sphericity test for the identity matrix indicated that the data were amenable to exploratory factor analysis. Principal components analysis identified six factors that explained 64% of the variation in the self-report questionnaire 20. Cronbach’s alpha was 0.817 for the entire scale and the extracted mean variance was greater than 0.5 for all factors, indicating convergent validity. The extracted mean variance, composite reliability, and factor loadings were all greater than 0.75 for all factors in this study, indicating that convergent validity was satisfactory and that discriminatory validity was also satisfied. The composite factor reliability scores ranged from 0.74 to 0.84, and the square roots of the mean variances were greater than the factor correlation scores.
Conclusion: The interview-based, culturally-adapted 20-item Amharic version of the SRQ-20 tool demonstrated good cultural adaptation and was also found to be valid and reliable in the present context.
Keywords: antenatal common mental disorders, cultural adaptation, factor analysis, SRQ-20, Ethiopia
Introduction
Pregnant women’s mental health is a major public health concern, particularly in low-and middle-income countries (LMICs). The term “antenatal common mental disorders” (CMD) is characterized by significant levels of depressive, anxiety, panic, and somatic symptoms occurring in pregnancy.1,2 The prevalence of antenatal common mental disorders and how they are undergone in distinct settings across the world are subjects of active disputation. According to a recent systematic review, 13.1% of women in low-and middle-income countries (LMICs) and 11.4% of women in high-income countries (HICs) suffer from perinatal common mental disorders (CMDs).3 Although prevalence estimates vary tremendously across the reviews, they are typically higher for LMICs than for HICs.4–6 The prevalence of common mental disorders among pregnant women ranges from 15 to 37%,4,7 and in Ethiopia, according to a recent community-based study report, about 37.5% of women developed antenatal common mental disorders.8
Nevertheless, common mental disorders during pregnancy are often left under-diagnosed and untreated because conditions are usually recognized as typical experiences of pregnancy and the overlapping of symptoms common to both pregnancy and common mental disorders, such as changes in appetite, body weight, sleep, and energy.9 Pregnant women with CMDs are less likely to seek antenatal care,10 which increases the chance of complicated delivery11 and poor child health outcomes such as low birth weight, premature birth, and neonatal mortality.12 CMDs during pregnancy may also have an adverse effect on the neurological development of the fetus.13 When untreated, mental disorders during the antenatal period may continue into the postnatal period.14
This results in decreased emotional involvement and hostility toward newborns.15 CMDs during pregnancy may also be associated with child malnutrition,16 and affect a child’s behavioral,17 emotional, and cognitive development.18
The study of common mental disorders in a low-resource setting such as Ethiopia requires a method of measuring psychiatric symptoms that is both valid and practical to administer. Studies of psychiatric disorders in “non-western” countries require careful consideration of the impact that culture and language may have upon the validity of the measures used. Consensus has emerged that such tools will be used however that there should be a careful method of translation, back-translation, and modification to make sure cross-cultural equivalences.19 Considering the socioeconomic impact of common mental disorders in developing countries and how challenging it can be to diagnose these disorders in primary care settings, the World Health Organization (WHO) developed the Self Reporting Questionnaire (SRQ-20), a screening instrument to identify suspected CMD cases in primary care settings, which has been used in many countries.20,21
SRQ-20 was designed to improve detection of common mental illnesses in PHC settings in LMICs. The SRQ items are single-sentence questions that are easy to manage in an interview format. It consists of 20 yes/no-answer questions that examine symptoms of depression, anxiety, and physical discomfort, as well as questions about suicidal ideation and functional effects that have been present in the previous 30 days. It has been translated and validated in several African countries22,23 and has been widely used in studies of perinatal depression in developing countries.22,24–28
Some studies have identified the validation of the SRQ-20 tool in Ethiopia in a community-based study and pre-validated it for use in a mixed sample of pregnant and postnatal women in the Butajira population, with the area under the receiver operating curve estimates of 0.82 (95% CI 0.68–0.96) and 0.70 (95% CI 0.57–0.83).22,29 However, collecting the validations of SRQ-20 in the Amharic version is still necessary, especially when collecting validations based on the internal structure and psychometric properties. Additionally, to date, there is no published research that has attempted to study or investigate the factor structure of SRQ-20 in the Ethiopian population. In addition, common mental disorders are sensitive to cultural differences.30 In addition, previously validated tools may not be applicable in different environments, cultures or contexts. Furthermore, the insights gained from using these tools may not adequately reflect what they are designed to measure. There is a need to use a locally validated instrument that has also been evaluated to ensure that it can measure prenatal common mental health disorders in pregnant mothers in a given setting to provide accurate and reliable estimates.
Amharic is one of the South Semitic languages and is spoken throughout Ethiopia. Amharic is adopted as a first language by numerous societies and used as a first language by others to aid as the official Ethiopian language.31 In North West Ethiopia, many of the pregnant women attending outpatient clinics do not understand the official English language. Therefore, translation of the SRQ-20 tool into the Amharic language would increase its efficacy among this population. A validated tool, translated into the Amharic local language, could be used in a similar study population in Ethiopia.
Therefore, this study aims to translate, culturally adapt, and test the reliability and validity of the WHO SRQ-20 when measuring common mental disorders among pregnant mothers in the North West, of Ethiopia. A better understanding of cultural expressions of antenatal common mental disorders and the validation of culturally relevant mental health screening tools may improve screening efficacy, enhance risk assessments and provide valuable information on mental health symptom profiles following pregnancy in Ethiopia.
Methods
Study Design and Setting
From March to April 2022, an institution-based cross-sectional study was conducted in two selected government health centers, Koladeba and Guramba Health Centers, in Dembia District, North Gondar Zone of Amhara Regional State, Ethiopia. Dembia District is located about 772 km from Addis Ababa (the capital of Ethiopia).
Sample Size and Sampling Procedures
The psychometric analysis in this study followed Summers, A.’s recommendation.32 Assuming a subject-to-item ratio of 15:1 and a 10% non-response rate. As a result, 310 pregnant mothers were selected to validate the SRQ-20. These participants were chosen using a systematic random sampling technique from mothers who attended routine prenatal follow-ups at two government health centers.
Data Collection Procedures
The data collection tool has been pre-tested and translated locally. Maternal ANC charts were retrieved for each participant to measure obstetric and clinical variables. The data collection was carried out by four trained BSC midwives who worked in personal interviews in the maternity clinics of the respective health centers. The tool included sociodemographic characteristics, maternal and obstetric factors, and the locally translated Amharic version of the WHO SRQ-20 tool.
Translation Process and Pilot Test
Step 1: Mapping the Available Scales for This Purpose
A WHO SRQ-20 tool was selected. The tool provided an overall score for screening common mental disorders. The SRQ-20 tool consists of one-part questions that require a yes/no answer and are easily managed in an interview format. It consists of 20 questions about symptoms of depression, anxiety, and physical discomfort, as well as suicidal ideation and functional effects that have occurred in the past 30 days.
Step 2: Face, Content Validation, and Expert Panel Discussion
An expert panel consisting of mental health experts, epidemiologists, public health professionals, and bilingual reverse translators conducted face and content validation of the WHO SRQ-20 tool. Initially, seven Ethiopian experts with more than 10 years of experience in various fields evaluated the tool for face validity, independently assessing its readability, comprehension, clarity, and ease of use. Their discussions helped resolve any inconsistencies and finalize the scale for the pretest. This committee also ensured equivalence between source and target versions and examined the questionnaires for any discrepancies.
Next, nine content experts from different departments rated each item of the SRQ-20 tool for relevance as “very relevant”, “relevant”, “somewhat relevant”, or “not relevant”. The content validity index for individual items and the overall scale, as well as Kappa coefficients of agreement, were used to determine the relevance of the items. A content validity index of ≥0.78 for individual items and ≥0.90 for the overall scale were considered acceptable, while Kappa values >0.81 were deemed excellent, between 0.60 and 0.80 good, and 0.40 to 0.59 fair.
Step 3: Forward Translation and Synthesis by an Expert Panel
Two bilingual (in Amharic and English) forward translators who were able to translate the original (English) version into the Amharic version were selected. The first translator had a background in clinical perspective. The other translator had no clinical background and was considered a naïve translator who recognized the different meaning of the original better than the first translator. Translations into the Amharic language more accurately reflect the intonation of the language. The translations were compared and discrepancies were identified during the translation process. The poorer choice of words was identified and resolved in a discussion between the translators. The translators prepared a document of the translation, including the necessary steps of the translation, contents, possible answers and instructions of the questionnaires were translated in this way.
Step 4: Synthesis of the Forward Translations
The team of experts and two translators discussed the discrepancies and synthesized the results of the translations. Then, one common document (T-12) was produced from the first translator’s (T1) and the second translator’s (T2).
Step 5: Back Translation and Expert Panel Review
We were working on the T-12 version of the scale and got two bilinguals (in Amharic and English) who were blinded to the original version. The back translations (BT1 and BT2) were performed by two translators in the source language (English). Furthermore, the two translators were neither aware nor informed to clarify the concepts explored by each item and neither were medical professionals in their profession. The main reasons for this were to avoid information bias and unexpected meanings of the items in the translated scale. This was a validation process to ensure that the translated version reflected the same item content as the original versions. In addition, this step helped to clarify the wording in the translations and ensure a consistent translation.
Step 6: Pilot-Test
The final Amharic version of the questionnaire was administered to a convenience sample of the target population. A total of 20 pregnant women were recruited to evaluate the instructions, paragraphs and answer format of the Amharic version for clarity and rewording suggestions before the final version.
Submission and Documentation
This stage was considered the submission of all the reports and forms to the committee, which kept track of the translated Amharic version. It also ensures whether the recommended steps were followed in the adaptation process (see Supplementary Material File 1).
Statistical Analysis
The data set was analyzed using the IBM SPSS Statistics version 26 statistical software package. Descriptive statistics such as mean with standard deviation, frequency, and percentage were used to describe variables.
Inter-Item and Item- Total Correlations
Inter-item correlations examined the extent to which a score on one item was related to a score on other items on a scale. To perform factor analysis, an inter-item correlation of 0.30 in absolute value for each item was considered desirable.33 Item-to-total (item-to-rest) correlations, defined as the correlation between the item score and the rest of the score, were also performed to assess the extent to which an item correlated with the total scale. The Pearson correlation coefficients of the corrected item total correlation of 0.2 were considered satisfactory.34 And when included in the scale, an item-total correlation of the score of less than 0.20 indicated that the item did not correlate very well with the total scale.35 Data were extracted using exploratory factor analysis and the principal components analysis technique.
A minimum value of 0.5 was set for the commonalities of each item and the percentage of item variance that can be expressed by the combination of items extracted to retain an item. Factors with an eigenvalue of 1 and a scree plot were used to determine the optimal number of underlying factors to extract. It was considered reasonable to keep one item in each factor structure when the factor loading criterion was set at 0.30.36 Factors obtained during factor extraction were rotated using the oblique varimax rotation method with Kaiser normalization. By examining the component correlation matrix, the inter-factor correlation (IFC) or the strength of the correlation between factors was evaluated. The IFC > 0.35 in absolute value was taken into account to choose the oblique rotation method.
Reliability Assessment
In this study, Cronbach’s alpha coefficient was used to check the internal consistency and reliability of the entire tool and subdomains. Cronbach’s alpha coefficient measures a low value that is closely related to a number of items as a group, accepting 0.70 as evidence of good internal consistency for the tool.37
Content Validation
Content validity was assessed using the Content Validity Index (CVI), which is based on the assessment of seven experts in the fields of epidemiology, mental health, public health, and psychology. A four-point Likert scale with values from 1 to 4 was used to determine the item’s content validity (representing irrelevant to very relevant). According to the literature, a content validity index of 78 and above is acceptable when the number of experts is greater than or equal to six.38 We assessed acceptability qualitatively by assessing the understandability and acceptability of the items. Also note the time required to complete each interview.39
Construct Validity of the Tool
Construct validity is the extent to which an instrument measures the construct it is intended to measure.40 To examine the construct validity of the tool, convergence and discriminant validity were used. Convergent validity is the assessment of the degree of correlation of several agreed indicators of the same construct. The extracted mean variance (AVE), a measure of the amount of variance captured by a construct relative to the amount of variance due to measurement error, was used to assess the convergent validity of the construct. An AVE of > 0.50 was taken as confirmation that the items converged on the same factor.41 Discriminant validity (divergent validity), which tests constructs that should have no relationship and in fact have no relationship, was assessed by comparing the AVE of one construct to the maximum common variance (the square of the IFC) of another construct. Therefore, the level of AVE for each construct should be greater than the squared correlation affecting the constructs.42
Results
Of the 310 study participants, 283 (91.3%) were married, 193 (62.3%) were illiterate, and 209 (67.4%) were under the age of twenty. Of 310 study participants, nearly 59% of participants began ANC follow-up during their first trimester (See Supplementary File 1 Table 1).
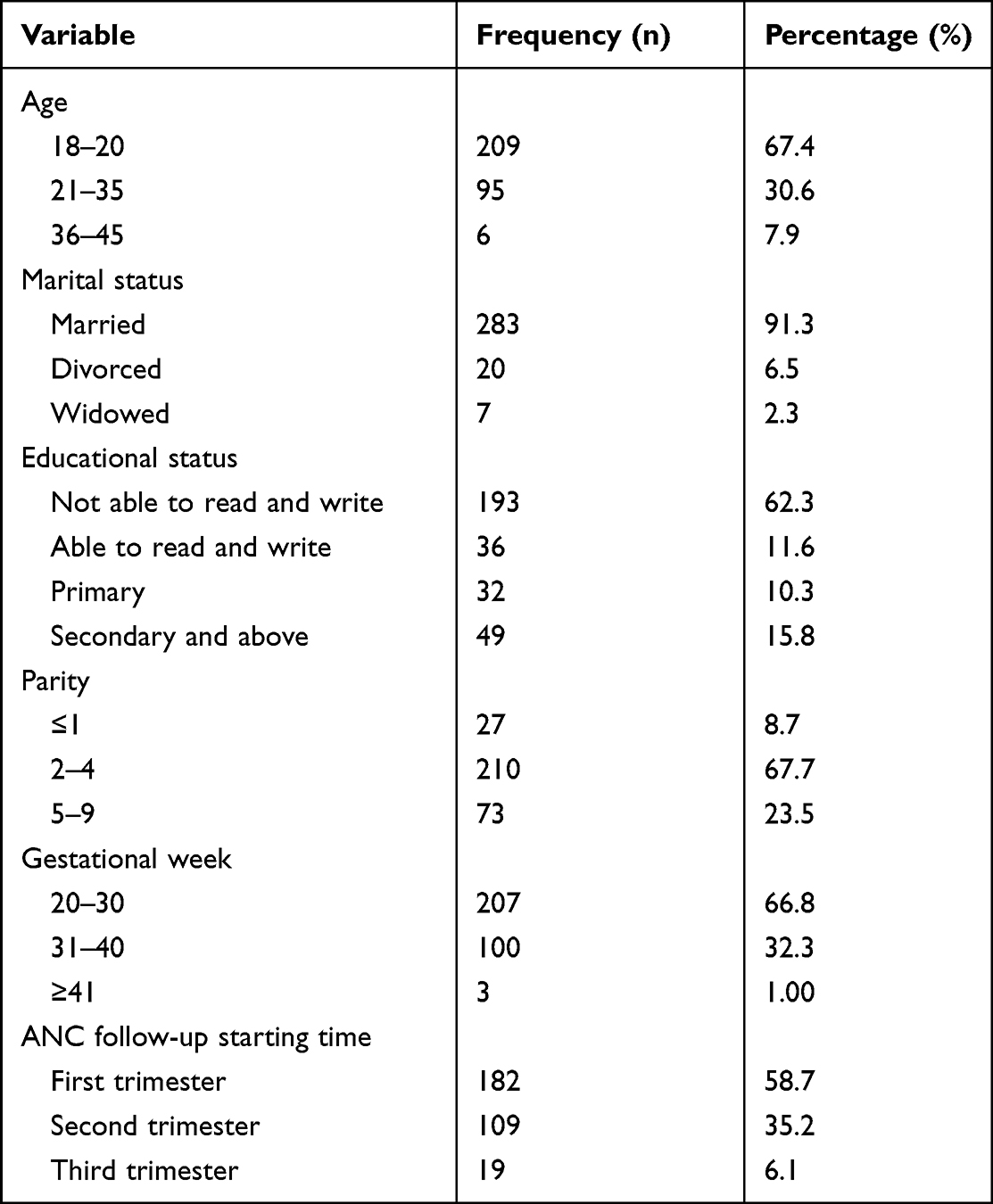 |
Table 1 Shows the Socio-Demographic and Obstetric Characteristics of Pregnant Women in Ethiopia’s North Gondar Zone in 2022 |
Face and Content Validation
The seven experts agreed that all items in the tools can be used for the current study setting. Item-level content validity ranged from 0.71 to 1.00; the scale-level content validity index was 0.942. This also indicates the appropriate content of each element in the tool. The experts did not reject any of the elements, but they recommended changing the sentences and words of a few. For example, point six was reworded to improve its power and content validity. The rewording of such elements has been calculated to remove ambiguous wording and to promote easier understanding of the layout, clarity and completeness of the elements. All items in the tool were required for domain coverage. The tool was modified based on the input from the expert panel and then subjected to another round of testing in a pilot study.
Pilot Testing
In step 6 of the pre-test, participants identified two out of 20 items (items 16 and 17) that needed to be reworded due to ambiguity. The reformulated version of the tool was tested on pregnant mothers during phase two of SRQ-20. After pre-testing the reworded items, no further problems were identified with any of the items in the WHO SRQ-20 tool. The overall responses from all participants were that the survey tool was interesting, easy to read, understandable and complete. The team also found that each pregnant woman took approximately 20 to 30 minutes to complete the tool, and the average time it took to complete the scale was 27 minutes.
Acceptability of the Amharic Version of the WHO SRQ-20 Tool
All participants answered all items in the local Amharic version of the WHO SRQ-20 tool and marked them correctly. No missing items were found. Neither the data collectors nor the respondents revealed any significant difficulties with questions or understanding the items.
Exploratory Factor Analysis
The scale showed very good sample adequacy for the Kaiser Meyer Olkin score (KMO = 0.733). Bartlett’s sphericity test, which tests the null hypothesis that the original correlation matrix is an identity matrix, was statistically significant (2 = 2129.9 DF = 190, P = 0.000) (see Supplementary File 1 Table 2). The extracted participation values of the municipalities ranged from 0.36 to 0.73, suggesting that the data are suitable for EFA. EFA confirmed a seven-factor structure based on factors with eigenvalues greater than 1 and visual examination of the scree plot (see Supplementary File Figure 1). These factors can be grouped into a smaller number of factors.
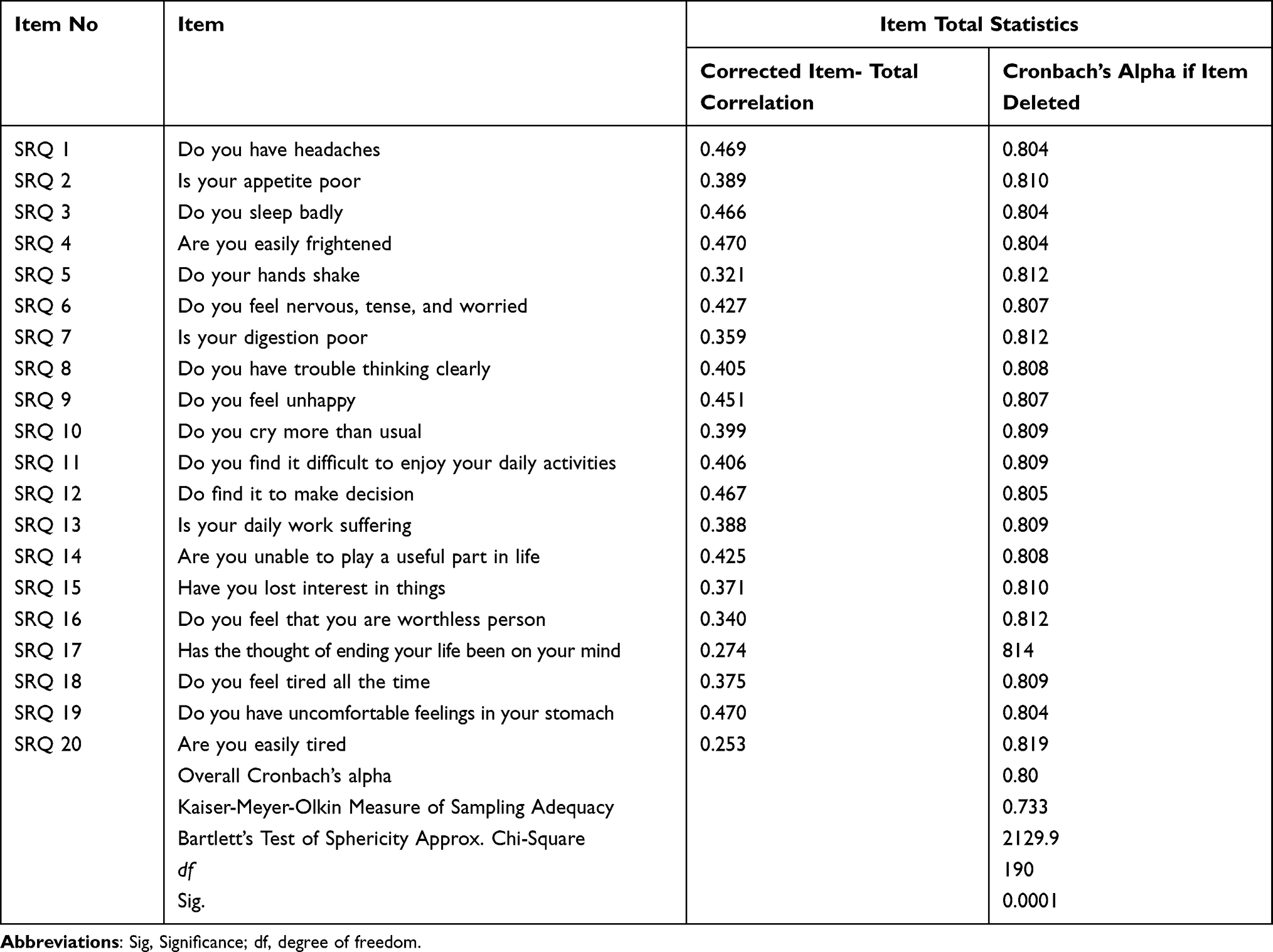 |
Table 2 Internal Consistencies, Item-Total Correlations, and Alpha if Item Deleted from the Amharic Version of the SRQ-20 Self-Reporting Questionnaire Among Pregnant Women in North West, Ethiopia 2022 |
Factor Extraction
The principal component analysis (PCA) extraction method was used and seven retained factors with eigenvalues greater than one were identified for further analysis. The seven factors together explained 69% of the total variance in SRQ-20. The study found that the first factor accounts for 24.3% of the total variance. The second factor explained 12.2% of the total variance on the rating scale. Likewise, factors 3, 4, 5, and 6 explained 7.8%, 7.2%, 6.3%, 5.4%, and 5.0% of the scale’s total variance, respectively (see Supplementary File 1 Table 3).
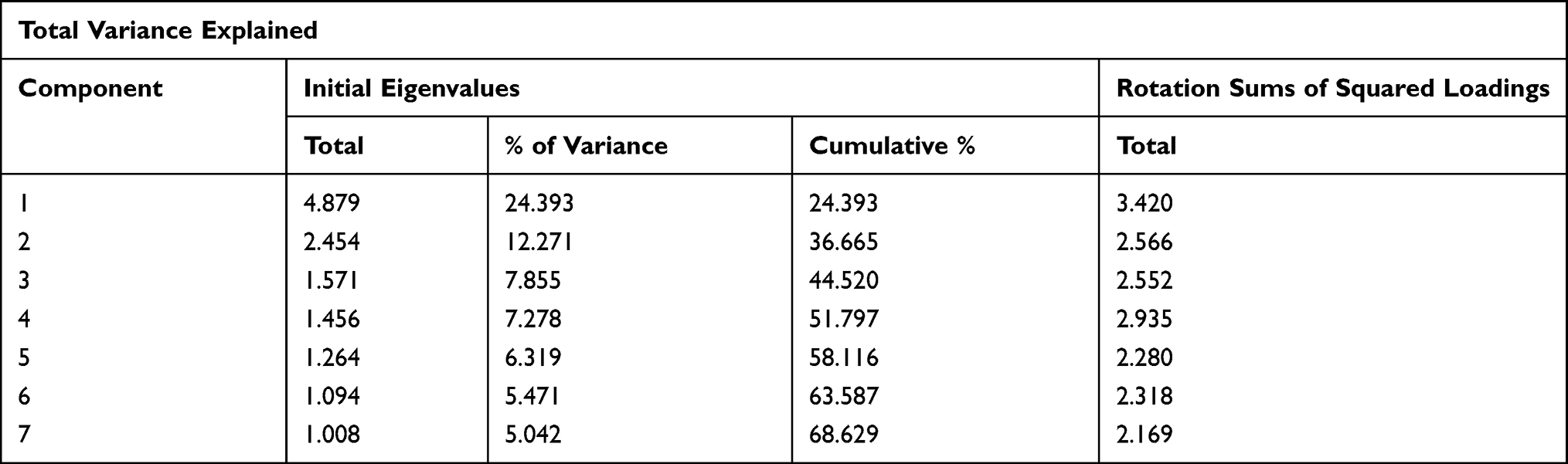 |
Table 3 Shows the Total Variance Explained for the Antenatal Common Mental Disorders SRQ-20 Screening Tool Among Pregnant Women in Ethiopia’s Northwestern Region in 2022 (n=310) |
Factor Rotation
The study shows that the rotated matrix of the components of the SRQ-20 scale was sufficient (>0.35). The rotated component matrix showed four items loaded with a factor of 1, with factor loadings ranging from 0.56 to 0.93. Four items were loaded to factor 2, finding factor loadings between 0.534 and 0.838. Under the third factor, three items with factor loadings between 0.576 and 0.901 were loaded. For the fourth factor, three items were loaded with loading factors ranging from 0.533 to 0.914. Two items were loaded on the fifth factor, with factor loading ranging from 0.803 to 0.740. At factor six, two items were loaded with a loading factor ranging from 0.733 to 0.875, and. Finally, two items were loaded with a factor of seven, with loading factors between 0.739 and 0.813.
Reliability Analysis
Internal Consistency Reliability Analysis
The self-report questionnaire (SRQ-20) has good internal reliability with an overall Cronbach’s alpha of 0.80. The study suggests that the scale is reliable. As each of the items, Cronbach’s Alpha and Factor Composite Reliability range from 0.79 to 0.8.08 and 0.736 to 0.839, respectively. Higher correlation coefficients between items and the type of material measured indicate a significant relationship between the two. In the present study, the lower limit for the item-total correlation was set at 0.2532 (see Supplementary File 1 Table 3). The study also suggested that the mean, variance, and standard deviation in the total scale statistics were 3.91, 12.27, and 3.503, respectively.
Convergent Validity
If the items are valid, a query is made as to whether the measurement relates to the variables to which it is to be assigned. Factor loading, AVE calculation, and CR scoring should all be used to assess convergent validity. The factor loading of all factors was more than an acceptable level between 0.534 and 0.936 after the low factor loading indicator was removed. All of these factors have an acceptable AVE level between 0.526 and 0.700. The study also suggested that the composite reliability of the factors had more than acceptable levels ranging from 0.736 to 0.839. Therefore, based on three conditions: factor loading, AVE and CR for convergent validity, all three were met.
Discriminant Validity
Referring to Table 4, for all constructs the CR is above 0.70 and the AVE values are between 0.526 and 0.700. Discriminant validity was assessed using Fornell and Larcker43 by comparing the square root of each AVE on the diagonal to the correlation coefficients (off-diagonal) for each construct in the relevant rows and columns. Square roots of the mean variance extractions are greater than the values the factor correlation in the left row and lower columns. We concluded that discriminatory validity between factors can be accepted and maintained (see Supplementary File 1 Table 4).
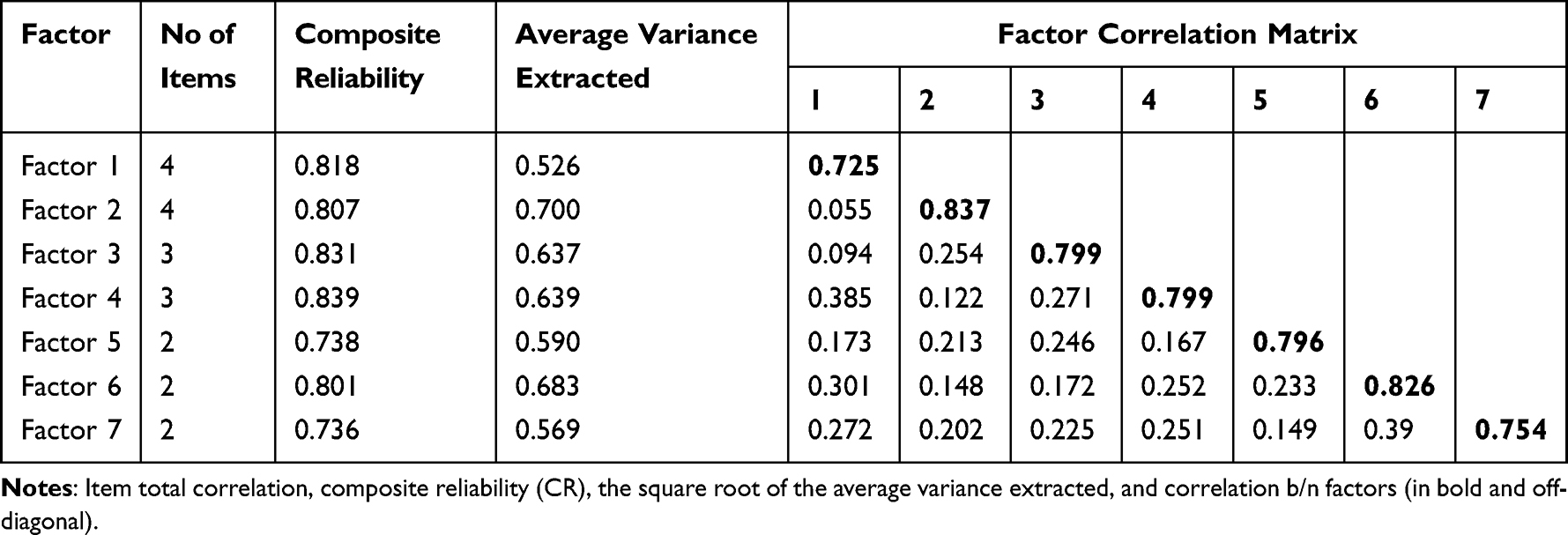 |
Table 4 Item Total Correlation, Composite Reliability, the Square Root of the Average Variance Extracted of SRQ-20 and Cultural Adaptation and Validation of the SRQ-20 Screening Tool, Northwest Ethiopia 2022 (n = 310) |
Discussion
The WHO SRQ-20 tool was evaluated as to whether it adequately measures what it intends to measure and whether the questions are relevant and clear. The content of the tool was conceptually anchored in the various works of literature22 and has been thought through and further developed over many years. A panel of experts concluded that all elements of the tool support the content validity of the WHO SRQ-20 tool. The comprehensive process of tool translation and cultural adaptation was performed on each element to adapt it to the target culture while maintaining the meaning and intent of the original elements.
Translators from the source language to the target language were people who are fluent in both languages and bring different cultural perspectives to the table This could be because the study teams proposed a meeting between translators to identify a problem in wording, differences and discrepancies between the two translated versions. Back-translated versions of the tool were compared to see if there were any discrepancies between them and the original version. We have used the original language terminology and syntax for the instructions, elements, and response format of the original tools. Similarity in meaning and relevance were taken into account. Any ambiguities and discrepancies in cultural meaning and instructions, items, response formats between the two back-translations and between each of them and the original source language tool were discussed. Issues raised were resolved by consensus among committee members to derive a preliminary version of the tool in the target language.
The same validation process was applied to the translated and back-translated versions, evaluating and repeating until no ambiguities or discrepancies were discovered. This was supported by other studies. The responsibility of the committees is to evaluate, modify, and compile the instructions, items, and response format. In addition to creating the preliminary final version of the target language for pilot and psychometric tests, the conceptual, semantic and content-related equivalence was confirmed. A pilot study was calculated using a series of cognitive interviews with pregnant women and found that the questionnaire was easy to read, understand and use. Other studies indicate this. They verified the validity, acceptance and feasibility of the tool management. This may be because every pregnant woman is asked to rate the tool’s instructions and elements and whether they find them easy to follow or not.44
The preliminary version of the translated tools has been subjected to a psychometric test. KMO was 0.733 and the result of Bartlett’s test of sphericity was (p 0.0001). This research is one of the first studies in northwestern Ethiopia that attempted to analyze the factor structure, reliability, and validity of the Amharic version of SRQ-20. This confirmed that our data were suitable for EFA and revealed pattern relationships between the variables. Since this requirement was met, it was confirmed that unique and reliable factors were generated.44
The Amharic version of the SRQ-20 version had seven factors: Cognitive, Somatic, Depressive Symptoms I and II, Anxiety, Suicidal Thoughts, and Physiological Symptoms. The results of the study support the reliability and validity of the prenatal common mental disorders scale. The construct validity of the Amharic version SRQ-20 was checked by PCA. It yielded seven theoretically meaningful and coherent factors with good internal consistencies. F1 consisted of 4 items (items 8, 12, 13 and 14) with questions about the following symptoms: distress in daily work, difficulty making decisions, difficulty thinking clearly and being unable to play a useful role in life. And factor two included questions about whether you feel tired all the time, have an uncomfortable feeling in your stomach, and get tired easily. Somatic symptoms have been accurately described in this factor; hence this factor has been named somatic. Both F3 (items 1, 2 and 3) and F4 (items 9, 10 and 11) contained three items each. Typical somatic symptoms are found in F3 items describing loss of appetite, poor sleep and often headaches. At factor 4, you cry more than usual, you feel unhappy and it is difficult to enjoy life all the time, can be related to both the feeling of depression and somatic. Therefore, the decision was made to name them Somatic and Depressive Symptoms I and Somatic and Depressive Symptoms II. Factor five included questions about whether you feel tense, nervous, or anxious, and whether you shake your hand to cite anxiety symptoms described in that factor. Factor six and seven both contained two items (items 15, 16 and items 6 and 7) and were termed loss of self-esteem and physiological symptoms. Future studies are needed to clarify the relationship between symptom overlap and the statistical difference.
There is currently no consensus on the number of factors reported for the SRQ-20, with factor solutions ranging from 2 to 7 in the literature.20,30,45,46 The EFA process revealed seven factors indicative of the structure of the SRQ-20 of the Amharic version. This finding fits into an existing literature on attempts to study the SRQ-20 factor structure that have been conducted in several countries.47–49 Depending on the context of the local culture, 27 factor structures have emerged from this so far. It is evident that there are significant cultural factors in the SRQ-20. This has been observed in several studies in different countries. These studies attempted to examine various factors or aspects of the SRQ-20. They produced different numbers of factors or the same number, but the questions describing those factors are different.21,30,48,50 Furthermore, the SRQ-20 manual (WHO, 1994) verifies that the SRQ-20 is very likely to contain more than one factor or dimension, although it depends on population and local culture. According to a study published in the Journal of Clinical Diagnosis and Prevalence (WHO, 1994), the SRQ-20 measure has good internal structural validity and can be used to screen prenatal common mental disorders.
The culturally adapted Amharic version of SRQ-20 was found to have good internal reliability for the full scale. The study suggested that the composite reliability of the factors ranged from 0.73 to 0.83 in the primary to end dimensions. The three conditions for determining convergent validity were factor loading; AVE and composite reliability passed the validation process. In this study, the square roots of the average variance extractions (AVE) were higher than each of the left rows and bottom columns of the factor correlation scores. The study also showed that discriminatory validity could be accepted and supports discriminatory validity between factors. The extracted new factor structure does not match the factor structure given in the original English version (WHO SRQ-20 tool). Because previously validated tools may not always be translated accurately, which does not mean they are valid in other contexts, cultures or environments. It is possible that the results based on such instruments do not really reflect what they are intended to measure. Other cross-cultural studies using the SRQ-20 have reported a range of three to eight extracted factors.20,51,52 Future research should focus on determining whether SRQ-20 components can be accurately interpreted as subscales. Depending on whether a study is conducted in a primary care setting or as part of a community survey, the setting in which it is conducted can affect the results. In addition, the different factor structures can be influenced by cultural differences and local idioms of common mental disorders, and future work should be directed towards exploring the relationship between the SRQ-20 and culturally relevant screening and assessment tools.
Limitation and Strengths of This Study
The study only included pregnant mothers, and we recommend future studies to test the validity of this instrument before and after childbirth, who are also prone to maternal common mental disorders. We did not evaluate responsiveness over time as we only collected data at a specific point in time. Test-retest validity was; not carried out, leaving sensitivity to changes; not tested due to feasibility issues.
Indeed, the conceptual equivalence between source and target languages was a strength of this study. In order to improve the quality of the tool’s forward translation, back translation and cross-cultural validation, qualified translators and committee members were considered. Forward translators have been carefully selected, are proficient in the target language and have in-depth knowledge of the target language culture.
Conclusions and Recommendation
Overall, the validation of the culturally adapted SRQ-20 tool is a positive step towards improving perinatal mental health outcomes in Ethiopia, and it provides a valuable resource for researchers and healthcare professionals working with pregnant women in rural settings. However, it is important to note that the validation study was conducted only in rural settings, and further research is needed to evaluate the tool’s effectiveness in urban settings. This highlights the need for ongoing research to improve mental health services for pregnant women across different regions and populations in Ethiopia.
Abbreviations
AVC, average variance extracted; CMD, common mental disorders; CR, convergent reliability; CVI, content validity index; EFA, exploratory factor analysis; IFC, inter factor correlation; KMO, Kaiser-Meyer-Olkin; LMICs low-and- middle- income countries; PHC, primary health care setting; SRQ-20 self-reporting questionnaire-20; WHO, world health organization.
Data Sharing Statement
The data sets used and/or analyzed in this study are available from the corresponding author on a reasonable request.
Ethical Consideration and Consent Form
Ethical approval was obtained from the institutional Review Board (IRB) University of Gondar with identification number (VP/RTT/Eng./051/06/2021). The consent process was acceptable and approved by the ethics committee. Letters of permission were obtained from the relevant health authorities. As all of our study participants were 18 years or older, they were deemed capable of providing informed consent on their own behalf by the ethics committee, and we obtained their consent directly from them after thoroughly explaining the study purpose and significance. We ensured data confidentiality by using identification numbers instead of names and limiting access to the data. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
Our deepest gratitude goes to the university of Gondar and the study participants in this research. The authors also would like to give great appreciation to data collectors and supervisors for their contribution to this paper.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which article will be submitted, gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This study didn’t receive any specific grant from any funding agency in the public, commercial or non- profit organizations.
Disclosure
The authors declare that they have no competing interests.
References
1. Shidhaye P, Giri P. Maternal depression: a hidden burden in developing countries. Ann Med Health Sci Res. 2014;4(4):463–465. doi:10.4103/2141-9248.139268
2. Howard LM, Piot P, Stein A. No health without perinatal mental health. Lancet. 2014;384(9956):1723–1724. doi:10.1016/S0140-6736(14)62040-7
3. Woody C, Ferrari AJ, Siskind DJ, et al. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. 2017;219:86–92. doi:10.1016/j.jad.2017.05.003
4. Fisher J, Cabral de Mello M, Patel V, et al. Prevalence and determinants of common perinatal mental disorders in women in low-and lower-middle-income countries: a systematic review. Bull World Health Organ. 2012;90(2):139–149. doi:10.2471/BLT.11.091850
5. Chandra PS, Herrman H, Fisher J, Riecher-Rössler A. Mental Health and Illness of Women. Singapore: Springer; 2020. doi:10.1007/978-981-10-2369-9
6. Gelaye B, Rondon MB, Araya R, et al. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry. 2016;3(10):973–982. doi:10.1016/S2215-0366(16)30284-X
7. Jha S, Salve HR, Goswami K, et al. Burden of common mental disorders among pregnant women: a systematic review. Asian J Psychiatr. 2018;36:46–53. doi:10.1016/j.ajp.2018.06.020
8. Tamiru D, Misgana T, Tariku M, et al. Prevalence and associated factors of common mental disorders among pregnant mothers in rural eastern Ethiopia. Front Psychiatry. 2022;13. doi:10.3389/fpsyt.2022.843984
9. Barrio L, Burt V. Depression in pregnancy: strategies for primary care management. Dealing with an underdiagnosed undertreated problem. Women’s Health Prim Care. 2000;3:490–498.
10. Satyanarayana VA, Lukose A, Srinivasan K. Maternal mental health in pregnancy and child behavior. Indian J Psychiatry. 2011;53(4):351. doi:10.4103/0019-5545.91911
11. Alder J, Fink N, Bitzer J, et al. Depression and anxiety during pregnancy: a risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. J Matern Fetal Neonatal Med. 2007;20(3):189–209. doi:10.1080/14767050701209560
12. Bao Giang K, Viet Dzung T, Kullgren G, et al. Prevalence of mental distress and use of health services in a rural district in Vietnam. Glob Health Action. 2010;3(1):2025. doi:10.3402/gha.v3i0.2025
13. Rondó PH, Ferreira RF, Nogueira F, et al. Maternal psychological stress and distress as predictors of low birth weight, prematurity and intrauterine growth retardation. Eur J Clin Nutr. 2003;57(2):266–272. doi:10.1038/sj.ejcn.1601526
14. Robertson E, Grace S, Wallington T, et al. Antenatal risk factors for postpartum depression: a synthesis of recent literature. Gen Hosp Psychiatry. 2004;26(4):289–295. doi:10.1016/j.genhosppsych.2004.02.006
15. Oates M. Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. Br Med Bull. 2003;67(1):219–229. doi:10.1093/bmb/ldg011
16. Surkan PJ, Kennedy CE, Hurley KM, et al. Maternal depression and early childhood growth in developing countries: systematic review and meta-analysis. Bull World Health Organ. 2011;89(8):607–615. doi:10.2471/BLT.11.088187
17. Ramchandani PG, Richter LM, Norris SA, et al. Maternal prenatal stress and later child behavioral problems in an urban South African setting. J Am Acad Child Adolesc Psychiatry. 2010;49(3):239–247.
18. Koutra K, Chatzi L, Bagkeris M, et al. Antenatal and postnatal maternal mental health as determinants of infant neurodevelopment at 18 months of age in a mother–child cohort (Rhea Study) in Crete, Greece. Soc Psychiatry Psychiatr Epidemiol. 2013;48(8):1335–1345. doi:10.1007/s00127-012-0636-0
19. Rahman A, Iqbal Z, Waheed W, et al. Translation and cultural adaptation of health questionnaires. J Pak Med Assoc. 2003;53(4):142–146.
20. Scholte WF, Verduin F, van Lammeren A, et al. Psychometric properties and longitudinal validation of the self-reporting questionnaire (SRQ-20) in a Rwandan community setting: a validation study. BMC Med Res Methodol. 2011;11(1):1–10. doi:10.1186/1471-2288-11-116
21. Paraventi F, Cogo-Moreira H, Paula CS, et al. Psychometric properties of the self-reporting questionnaire (SRQ-20): measurement invariance across women from Brazilian community settings. Compr Psychiatry. 2015;58:213–220. doi:10.1016/j.comppsych.2014.11.020
22. Hanlon C, Medhin G, Alem A, et al. Detecting perinatal common mental disorders in Ethiopia: validation of the self-reporting questionnaire and Edinburgh Postnatal Depression Scale. J Affect Disord. 2008;108(3):251–262. doi:10.1016/j.jad.2007.10.023
23. Harpham T, Reichenheim M, Oser R, et al. Measuring mental health in a cost-effective manner. Health Policy Plan. 2003;18(3):344–349. doi:10.1093/heapol/czg041
24. Abou‐Saleh MT, Ghubash R. The prevalence of early postpartum psychiatric morbidity in Dubai: a transcultural perspective. Acta Psychiatr Scand. 1997;95(5):428–432. doi:10.1111/j.1600-0447.1997.tb09657.x
25. Harpham T, Huttly S, De Silva MJ, et al. Maternal mental health and child nutritional status in four developing countries. J Epidemiol Community Health. 2005;59(12):1060–1064. doi:10.1136/jech.2005.039180
26. Rahman A, Creed F. Outcome of prenatal depression and risk factors associated with persistence in the first postnatal year: prospective study from Rawalpindi, Pakistan. J Affect Disord. 2007;100(1–3):115–121. doi:10.1016/j.jad.2006.10.004
27. Nakku J, Nakasi G, Mirembe F. Postpartum major depression at six weeks in primary health care: prevalence and associated factors. Afr Health Sci. 2006;6(4):207–214. doi:10.5555/afhs.2006.6.4.207
28. Dørheim Ho-Yen S, Tschudi Bondevik G, Eberhard-Gran M, et al. The prevalence of depressive symptoms in the postnatal period in Lalitpur district, Nepal. Acta Obstet Gynecol Scand. 2006;85(10):1186–1192. doi:10.1080/00016340600753158
29. Hanlon C, Medhin G, Alem A, et al. Impact of antenatal common mental disorders upon perinatal outcomes in Ethiopia: the P‐MaMiE population‐based cohort study. Trop Med Int Health. 2009;14(2):156–166. doi:10.1111/j.1365-3156.2008.02198.x
30. Stratton KJ, Aggen SH, Richardson LK, et al. Evaluation of the psychometric properties of the Self-Reporting Questionnaire (SRQ-20) in a sample of Vietnamese adults. Compr Psychiatry. 2013;54(4):398–405. doi:10.1016/j.comppsych.2012.10.011
31. Britannica T. Editors of Encyclopaedia. Argon Encyclopedia Britannica; 2020.
32. Summers A. A practical example of exploratory factor analysis and critical realism. Nurse Res. 2021;29(1):42–50. doi:10.7748/nr.2021.e1759
33. Carmines EG, Zeller RA. On establishing the empirical dimensionality of theoretical terms: an analytical example. Polit Methodol. 1974;1:75–96.
34. Zijlmans EAO, Tijmstra J, van der Ark LA, et al. Item-score reliability in empirical-data sets and its relationship with other item indices. Educ Psychol Meas. 2018;78(6):998–1020. doi:10.1177/0013164417728358
35. Henrysson S. Correction of item-total correlations in item analysis. Psychometrika. 1963;28(2):211–218. doi:10.1007/BF02289618
36. Yong AG, Pearce S. A beginner’s guide to factor analysis: focusing on exploratory factor analysis. Tutor Quant Methods Psychol. 2013;9(2):79–94. doi:10.20982/tqmp.09.2.p079
37. Cronbach LJ. Coefficient alpha and the internal structure of tests. psychometrika. 1951;16(3):297–334. doi:10.1007/BF02310555
38. DeVon HA, Block ME, Moyle-Wright P, et al. A psychometric toolbox for testing validity and reliability. J Nurs Scholarsh. 2007;39(2):155–164. doi:10.1111/j.1547-5069.2007.00161.x
39. Strauss ME, Smith GT. Construct validity: advances in theory and methodology. Annu Rev Clin Psychol. 2009;5(1):1–25. doi:10.1146/annurev.clinpsy.032408.153639
40. Cronbach LJ, Meehl PE. Construct validity in psychological tests. Psychol Bull. 1955;52(4):281. doi:10.1037/h0040957
41. Chin WW, Newsted PR. Structural equation modeling analysis with small samples using partial least squares. Stat Strat Small Sample Res. 1999;1(1):307–341.
42. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. 1981;18(1):39–50. doi:10.1177/002224378101800104
43. Reddy SK. Effects of ignoring correlated measurement error in structural equation models. Educ Psychol Meas. 1992;52(3):549–570. doi:10.1177/0013164492052003005
44. Chan LL, Idris N. Validity and reliability of the instrument using exploratory factor analysis and Cronbach’s alpha. Int J Acad Res Bus Soc Sci. 2017;7(10):400–410. doi:10.6007/IJARBSS/v7-i10/3387
45. Chen S, Zhao G, Li L, et al. Psychometric properties of the Chinese version of the Self-Reporting Questionnaire 20 (SRQ-20) in community settings. Int J Soc Psychiatry. 2009;55(6):538–547. doi:10.1177/0020764008095116
46. Ventevogel P, De Vries G, Scholte WF, et al. Properties of the Hopkins Symptom Checklist-25 (HSCL-25) and the Self-Reporting Questionnaire (SRQ-20) as screening instruments used in primary care in Afghanistan. Soc Psychiatry Psychiatr Epidemiol. 2007;42(4):328–335. doi:10.1007/s00127-007-0161-8
47. Kootbodien T, Becker P, Naicker N, et al. Gender invariance of the Self-Reporting Questionnaire (SRQ-20). S Afr J Psychol. 2015;45(3):318–331. doi:10.1177/0081246315572500
48. Netsereab TB, Kifle MM, Tesfagiorgis RB, et al. Validation of the WHO self-reporting questionnaire-20 (SRQ-20) item in primary health care settings in Eritrea. Int J Ment Health Syst. 2018;12(1):1–9. doi:10.1186/s13033-018-0242-y
49. Prasetio CE, Triwahyuni A, Prathama AG. Psychometric properties of Self-Report Questionnaire-20 (SRQ-20) Indonesian version. J Psikologi. 2022;49(1):69–86. doi:10.22146/jpsi.69782
50. van der Westhuizen C, Wyatt G, Williams JK, et al. Validation of the self reporting questionnaire 20-item (SRQ-20) for use in a low-and middle-income country emergency centre setting. Int J Ment Health Addict. 2016;14(1):37–48. doi:10.1007/s11469-015-9566-x
51. Iacoponi E, de Jesus Mari J. Reliability and factor structure of the Portuguese version of Self-Reporting Questionnaire. Int J Soc Psychiatry. 1989;35(3):213–222. doi:10.1177/002076408903500301
52. Sen B. An analysis of the nature of depressive phenomena in primary health care utilising multivariate statistical techniques. Acta Psychiatr Scand. 1987;76(1):28–32. doi:10.1111/j.1600-0447.1987.tb02858.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.