")
Back to Journals » The Application of Clinical Genetics » Volume 15
CTLA-4 CT-60 A/G and CTLA-4 1822 C/T Gene Polymorphisms in Indonesians with Type 1 Diabetes Mellitus
Authors Rochmah N , Faizi M, Nova S, Setyoningrum RA, Basuki S , Endaryanto A
Received 25 January 2022
Accepted for publication 13 April 2022
Published 29 April 2022 Volume 2022:15 Pages 19—25
DOI https://doi.org/10.2147/TACG.S359158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Nur Rochmah,1 Muhammad Faizi,1 Suhasta Nova,1 Retno Asih Setyoningrum,1 Sukmawati Basuki,2 Anang Endaryanto1
1Faculty of Medicine, Department of Child Health, Dr. Soetomo General Hospital, Universitas Airlangga, Surabaya, East Java, Indonesia; 2Institute of Tropical Disease, Universitas Airlangga, Surabaya, East Java, Indonesia
Correspondence: Nur Rochmah, Faculty of Medicine, Department of Child Health, Dr. Soetomo General Hospital, Universitas Airlangga, Mayjend Prof. Dr. Moestopo No. 6-8, Surabaya, East Java, 60286, Indonesia, Tel +6281703501118, Email [email protected]
Introduction: CTLA-4 gene polymorphism plays an important role in children with type 1 diabetes mellitus (T1DM). However, data on this subject vary among different races and ethnics.
Purpose: To analyze CTLA-4 CT-60 A/G and CTLA-4 1822 C/T gene polymorphism among children with T1DM compared to control.
Patients and Methods: The CTLA-4 CT-60 A/G and CTLA-4 1822 C/T gene polymorphism in children with T1DM using polymerase chain reaction-restriction fragment length polymorphism in 25 T1DM and 25 controls. The inclusion criteria were patients regularly controlled at the Pediatric Endocrine Outpatient Clinic of Dr. Soetomo Hospital, aged 4– 18 years and willing to join this study and the exclusion criteria were T1DM patients hospitalized in the pediatric intensive care unit. In the control group, the inclusion criteria were healthy children, aged 4– 18 years and willing to join this study. The exclusion criteria included children with ongoing infection, history of other autoimmune diseases, allergies, or malignancy.
Results: The mean age was 12.48 years old, and the mean of T1DM onset was 9.28 years old. The CTLA-4 1822 T allele observed in 62% T1DM and 56% in control (p = 0.388, OR = 0.78, 95% CI = 0.44– 1.37) and CTLA-4 CT-60 G allele observed in 52% T1DM and 58% in control (p = 0.393, OR = 1.27, 95% CI = 0.73– 2.22). The C/T genotypes was significantly higher in control group (p = 0.045, OR = 3.27, 95% CI = 1.00– 10.62). The A/G genotypes was commonly found in control group (p = 0.765, OR = 1.20, 95% CI = 0.37– 3.86). The Javanese was the dominant ethnic group in our study.
Conclusion: The frequency of CTLA-4 CT-60 A/G polymorphism almost equivalent in T1DM and control group. However, CTLA-4 1822 C/T polymorphism was more prevalent in the control group; thus, this genotype may have a protective effect against T1DM.
Keywords: type 1 diabetes mellitus, CTLA-4
Introduction
Diabetes mellitus (DM) is a disorder characterized by persistent hyperglycemia. Several types of DM often occur in children and adolescents: type 1 DM (T1DM), an organ-specific autoimmune disease in which CTLA-4 gene polymorphism plays an important role, especially in the T-cell mediated destruction of pancreatic islets, Type 2 DM, also called non-insulin-dependent DM and other types including maturity-onset diabetes of the young (MODY), neonatal diabetes (NDM) and drug-induced diabetes.1–3 All the forms of DM are caused by a combination of genetic and environmental risk factors.2 Cytotoxic-T-lymphocyte-antigen-4 (CTLA-4) has a higher affinity to bind with the B7 molecule on antigen-presenting cells and it down-regulates T-cell function and stops the ongoing immune response. This mechanism plays an important role in the susceptibility of T1DM.2,4–8 In recent years, many studies related to the genetic and immunological aspects of T1DM pathogenesis have been reported.9 The polymorphism of CTLA-4 that is related to autoimmune diseases (AITD and T1DM) particularly are CT 60 and CT 1822.10–14
T1DM comprises 10% of all the incidences of existing DM.2 Although T1DM prevalence is <1% in most populations, its incidence differs among different races and ethnic groups; the incidence of T1DM is 0.1/100,000 per year in China, 1.4/100,000 per year in Japan, and 43/100,000 per year in Finland, whereas the estimated incidence in Indonesia is around 0.3/100,000 per year.2 The global T1DM incidence is increasing at a rate of about 3% per year.
In the Asian population, the study of CTLA-4 polymorphism in T1DM is still limited. Meanwhile, the prevalence of CTLA-4 CT-60 and CT1822 in Indonesia remains unknown. Therefore, we investigated the association between CTLA-4 CT-60 A/G, CTLA-4 1822 C/T polymorphism, and T1DM risk in the Indonesian population.
Materials and Methods
Study Participants
This case–control study was held between March 2021 and July 2021 at the pediatric endocrine clinic at Dr. Soetomo General Hospital in Surabaya. Twenty-five children were diagnosed with T1DM (according to the International Society for Pediatric and Adolescent Diabetes Guidelines) and 25 controls are included. In the T1DM group, the inclusion criteria were patients regularly visiting the hospital during the study, aged 4–18 years, and willing to join this study. The exclusion criteria were T1DM patients hospitalized in the pediatric intensive care unit. For the control groups, the inclusion criteria were healthy children without a history of T1DM, aged 4–18 years and want to participate in the study and the exclusion criteria were children with an ongoing acute infection such as common cold who control pediatric OPC (outpatient clinic), history of other autoimmune diseases, allergies, or malignancy. This research was granted by the Clinical Research Unit at Dr. Soetomo Hospital, Surabaya, Indonesia with ethical number 1889/KEPK/III/2020.
Genetic Analysis of CTLA-4 CT 60 A/G and 1822 C/T
Human CTLA-4 is located in band q33 of chromosome 2 with 4 exons and 3 introns. The CTLA-4 polymorphism that is associated with T1DM susceptibility is CTLA-4 1822 located in intron 1 and CTLA-4 CT-60 in 3’ Untranslated Regions (UTR).13,15 The CTLA-4 CT-60 A/G and CTLA-4 1822 C/T polymorphisms were analyzed using QIAmp DNA Mini Kit (Qiagen©) from the peripheral blood mononuclear cells (PBMC) sample and detected by PCR-RFLP. Polymerase chain reaction (PCR) was performed using specific primers (CTLA-4 CT-60A/G: forward, 5′GATTTCTTCACCACTATTTGGGATATTAC3′ and reverse, 5′AGATCAAAATGGCTGCAAGG3′; CTLA-4 1822 C/T: forward, 5′TCAAAGGGATTGAGCAGATG3′ and reverse, 5′TCCCATGCTCTTTGTTCTC3′).4,8 The RLFP analysis of CTLA-4 genes was performed using restriction enzymes BsaAI and BsmAI for CTLA-4 CT-60A/G and CTLA-4 1822 C/T, respectively.8
Genomic DNA sequences containing the polymorphic region, ie, restriction enzyme, were amplified by PCR (Thermal cycler PC-818; ASTEC, Fukuoka, Japan), in a total reaction volume of 10 μL (5 μL Amplitaq Gold, 0.25 μL MgCl2, 2.25 μL H2O, 0.25 μL of each primer, and 2 μL template DNA). The following cycling conditions were applied: an initial denaturation of 2 min at 94°C, 35 cycles of annealing for 45 s at 58°C and extension for 1 min at 72°C, and a final extension of 3 min at 72°C.4,8 Approximately 11 μL of each final PCR product was incubated at 37°C for 6 h with 1 U of restriction enzyme at a total volume of 20 µL.4,8 The PCR-RLFP products (11 μL) were separated using 6% acrylamide gel at 5 V/cm for 1 h in 1× TBE (Tris/Borate/EDTA) buffer and observed under UV light (IWASAKI ASAHI TECHNO GLASS). The length of PCR-RLFP products evaluated using One Step Marker 9 were as follows: 1) CTLA 4 CT-60 A/G: 203 bp for A/A, 176 bp, and 29 bp for G/G, and both products for A/G genotype and 2) CTLA4 1822 C/T: 102 bp for T/T, 74 bp for C/C, and both products for C/T genotype. See Figures 1 and 2 for the PCR results.
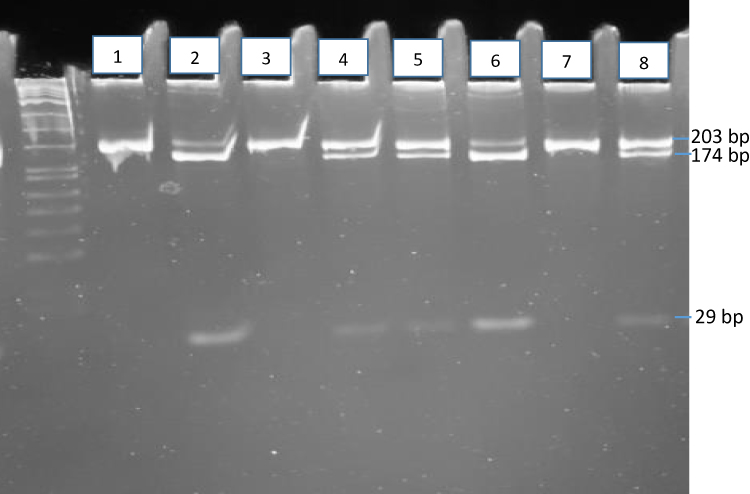 |
Figure 1 CTLA 4 CT-60 A/G: 203 bp for A/A, 176 bp and 29 bp for G/G, and both products for A/G genotype. Line 1,3,7- homozygous A/A with type 1 diabetes, line 2,4,5,6,8 - heterozygous A/G with type 1 diabetes. |
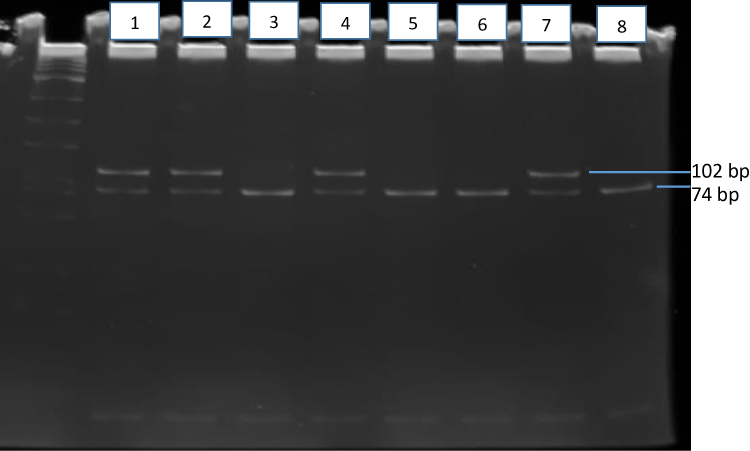 |
Figure 2 CTLA4 1822 C/T: 102 bp for T/T, 74 bp for C/C, and both products for C/T genotype. Line 1,2,4,7 - heterozygous C/T with type 1 diabetes, line 3,5,6,8 – homozygous C/C with type 1 diabetes. |
Statistical Analysis
The data analysis of this study used Statistical Package for Social Sciences, version 20.0. The distribution of the subject characteristics was explained using descriptive analysis. The genotypes polymorphisms and allele distribution differences between T1DM and controls were measured by chi-square test. Data were presented as mean or a percentage (%). Statistical significance was defined as a p-value <0.05.
Results
The study included 50 (25 T1DM and 25 Control) subjects. The characteristics of all subjects are presented in Table 1. The mean age of the study participants was 12.48 years. A majority of participants in the T1DM and control groups belonged to the Java ethnic group (88% and 100%, respectively). Childhood-onset of T1DM was reported in 20% of subjects.
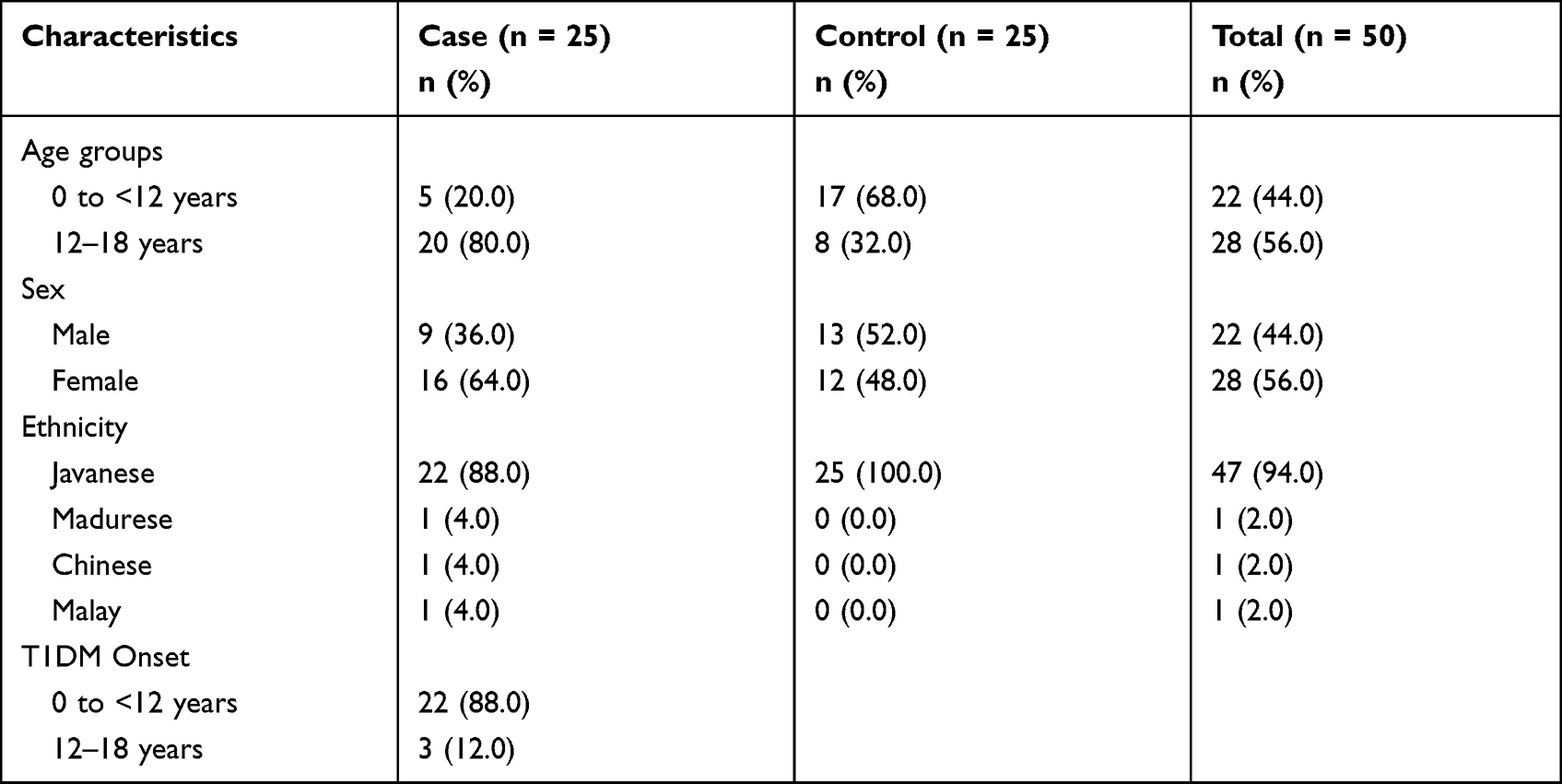 |
Table 1 Characteristics of Subjects |
The frequency of CTLA-4 CT-60 A/G in T1DM subjects was 64%, and the control was 68%. The analysis showed that A/G genotypes did not significantly differ between T1DM and control (p = 0.765; OR = 1.20). The CTLA-4 CT-60 G allele was frequently observed in the control group (58%). The CTLA-4 CT-1822 C/T genotype frequency in T1DM subjects was 44% and the control was 72%. The CTLA-4 1822 C/T genotype was significantly more frequent in the control (OR = 3.27, 95% CI = 1.00–10.62). The T allele is more frequent in T1DM subjects (62%) (Table 2).
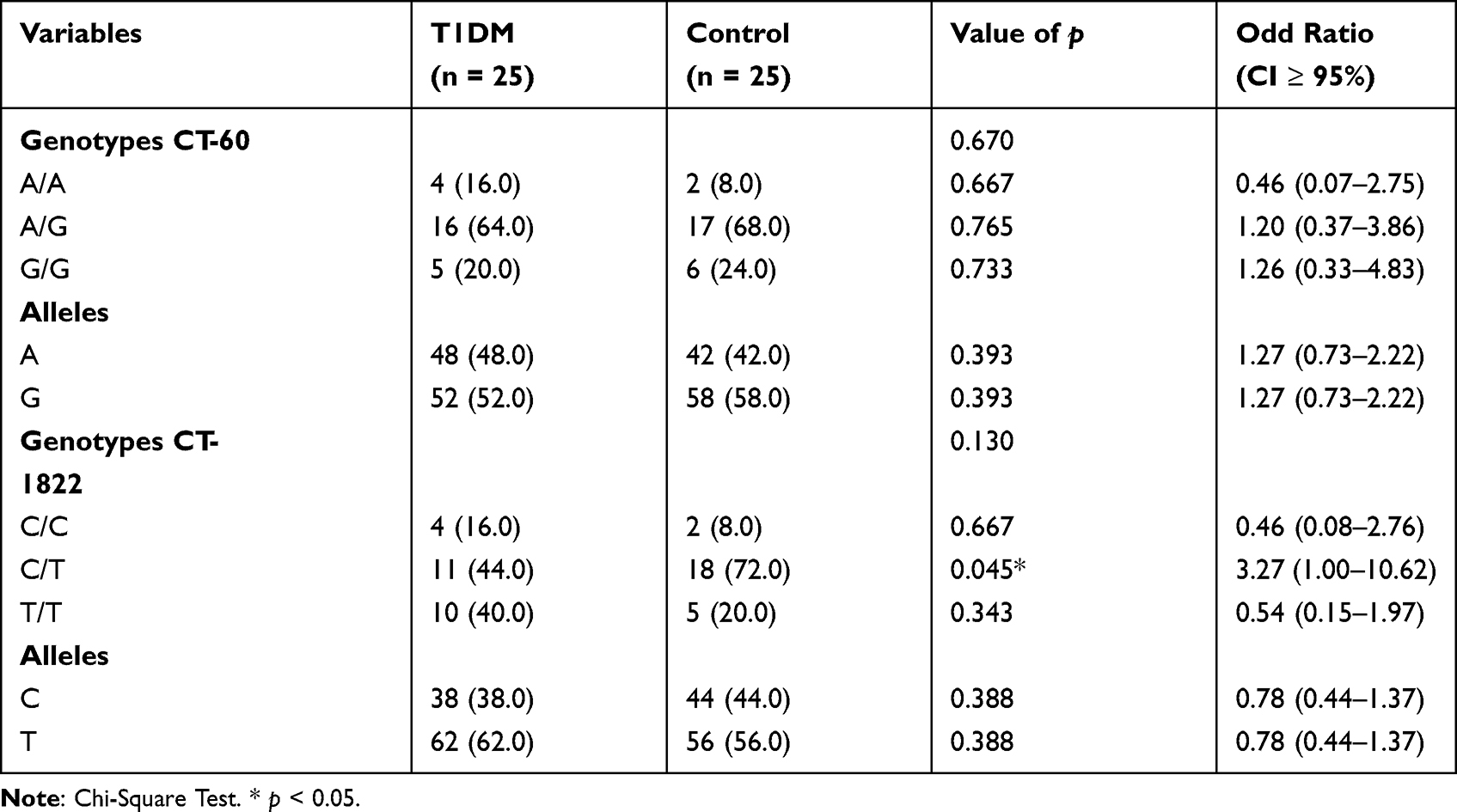 |
Table 2 The CTLA-4 CT-60 and CTLA-4 CT-1822 genotypes and alleles in T1DM |
The CTLA-4 CT-60 A/G and CTLA-4 1822 C/T genotypes mostly observed in age 12–18 years old in T1DM subject (87.5% and 81.8%, respectively). In control group, CTLA-4 CT-60 A/G and CTLA-4 1822 C/T genotypes frequently observed in age 5–11 years old (52.9% and 61.1%, respectively) (p = 0.222; p = 0.068).
In T1DM group, the frequencies of CTLA-4 CT-60 and CTLA-4 1822 polymorphisms in the Java ethnic group were 88% (16% A/A; 52% A/G; 20% G/G) and 88% (12% C/C; 36% C/T; 40% T/T), respectively (p = 0.858; p = 0364). In control group, the frequencies of both polymorphisms were 100% (8% A/A; 68% A/G; 24% G/G; 8% C/C; 72% C/T; 20% T/T, respectively).
Discussion
In this study, we found that the CTLA-4 CT-60 A/G polymorphism was frequently observed in the control group (68%) and the distributions did not significantly differ between the T1DM and control group. In some studies, CTLA-4 CT-60 G allele plays a risk factor, and the A allele plays a protective factor against autoimmune disease.16,17 Previous studies on the Chinese and Spanish populations have demonstrated that the G allele of CTLA-4 CT60A/G increased the risk of Graves’ disease and systemic lupus erythematosus.18 The CT60 polymorphism of the CTLA-4 gene is one of the strongest candidates that may involve T-cell mediated autoimmune disease. This variant has been associated with a lower mRNA level of the soluble form of CTLA-4 (sCTLA-4).34 While the association between CT 60 with T1DM risk is still controversial, the previous study showed that CT60 polymorphism has an association with T1DM in Belgian, French, Italian, Korean, Mexican, Spanish-American and Japanese, Russian, British, Moroccan, Estonian, and Croatian populations and no association in Chinese, Czech, Iranian, Argentinean, Chilean, Portuguese, and Turkish children. The difference pattern of CTLA-4 in different populations showed that CTLA-4 haplotypes may vary between races.19 Based on ethnicity, a meta-analysis study by Wang et al reported that in Caucasian, Middle Eastern, and Indian populations CT60 polymorphism showed a significantly increased risk of T1DM. In the East Asian population, the study showed only marginally significant results with a per-allele OR of 1.33 (95% CI = 1.03–1.71).13
CTLA-4 immunological pathway remains unclear. However, several mechanisms of CTLA-4 in immune homeostasis have been explained through the T cell-intrinsic and T-cell extrinsic pathways. In intrinsic models, there are 4 functions: 1) CTLA-4 delivers a negative signal which may disturb the signal generated by CD28, 2) Inhibitor signal ligand-independent, 3) Competitive inhibition for CD80 and CD86 ligands to prevent CD28 signal, 4) CTLA-4 controlled adhesion and motility between APCs and T-cell. In extrinsic models, there are also 4 functions: 1) CTLA-4 inhibit T-cell proliferation mediated by indoleamine 2.3-dioxygenase (IDO), 2) CLTA-4 induced the production of transforming growth factor β (TGFβ) and interleukin-10 (IL-10), 3) T-cells produced soluble CTLA-4 splice variant to blocking other T-cells receiving stimulatory signals, 4) CTLA-4 inhibit APCs by inducing trans-endocytosis of CD80 and CD86.20
In this study, the CTLA-4 1822 C/T polymorphism frequency in the T1DM subject was 44% and significantly lower than control (OR = 3.27, 95% CI: 1.00–10.62). Several studies have confirmed the association between CTLA-4 polymorphism (CT-1822, CT-60, and 49 A/G) and autoimmune thyroid diseases.21 A study on the Japanese population reported that the frequency of CTLA-4 49 A/G polymorphism in T1DM subjects was 37.1% and that of the G allele was 63.9%.8 However, the association between CTLA-4 CT 1822 and T1DM remains unknown. Another study on the Japanese population revealed that 4.1% of T1DM also suffered from autoimmune thyroid diseases.8 T1DM patients were at risk of developing other autoimmune diseases; it has been estimated that 1 out of 5 children with T1DM develop thyroid autoantibodies.1
The frequency of CTLA-4 CT-60 A/G polymorphism and G allele in Egyptian patients with T1DM have been reported as 49% and 44%, respectively.19 Another study on the European population has reported CTLA-4 49 A/G polymorphism and G allele frequencies of 56.8% and 52.9%, respectively, in T1DM subjects.7 Several studies in Europe, Egypt, Japan, and China have revealed a significant relationship between CTLA-4 gene polymorphisms and T1DM incidence.7,8,18,22
T1DM subjects in Chile reportedly had a CTLA-4 49 A/G gene polymorphism and G allele frequency of 45.3% and 35.6%, respectively.23 In the aforementioned study, 16.6% of T1DM subjects had CTLA-4 318C/T gene polymorphism, and the frequency of the C allele was 89.5%.23 Furthermore, a study in Turkey revealed that 43.9% of T1DM subjects had CTLA-4 49 A/G gene polymorphism, and the frequency of the G allele was 36.7%.22 The frequency of CTLA-4 49 A/G gene polymorphism and G allele in the Chinese population has been reported to be 33.6% and 76.1%, respectively.24
A study in Palembang reported the CTLA-4 49 A/G gene polymorphism to be prevalent in 36% T1Dof M subjects; the frequency of G and encylele was 71.6%.24 Unlike our study, Tanhapour et al showed that the correlation between CTLA-4 CT60 A/G polymorphism and autoimmune disorders is inconclusive.20
In this study, the mean of T1DM onset was 9.28 years old. In the T1DM subject, the CTLA-4 CT-60 A/G and 1822 C/T genotypes polymorphism was mostly found at age 12–18 years old (87.5% and 81.8%, respectively). A study on the Sudanese population revealed that the onset of T1DM occurred between 3 and 16 years of age.25 A previous study in Palembang has reported that T1DM was diagnosed at <11 years of age.20 The peak onset of T1DM occurs during childhood.26
Our study reported that both frequency of CTLA-4 CT-60 and CTLA-4 1822 polymorphisms in Java ethnic was 88% (p = 0.858; p = 0364). The frequency of polymorphism of CTLA-4 49 A/G in Palembang ethnic was 46.7%.24 A significant risk of CTLA-4 49 A/G, otherwise reported in the Indian and African populations, has been reported in the Middle East and Caucasian populations.20
The limitation of this study is the small size of the sample, although this study was conducted at a referral hospital in East Indonesia. In the Asian population, the number of T1DM cases is more limited than that of Caucasians as mentioned by several studies.27–33 Another limitation is that this study is a single-center, future multi-center study, which is important to obtain more data on Indonesian races.
Conclusion
In conclusion, the CTLA-4 CT-60 A/G gene polymorphism in T1DM groups is almost equivalent to the control group. The CTLA-4 1822 C/T genotype was more common in the control group. Therefore, this genotype may have a protective factor against T1DM. In the Javanese ethnic group, CTLA-4 CT-60 A/G and 1822 C/T genotypes occur often.
Ethical Approval
This research was granted by the Clinical Research Unit at Dr. Soetomo Hospital, Surabaya, Indonesia, with ethical number 1889/KEPK/III/2020. All participants in this study were following the Declaration of Helsinki. The informed consent was signed by all participant’s parents or legal guardians.
Acknowledgments
The authors would like to thank all the study participants and the endocrine team of Dr. Soetomo General Hospital, Surabaya, Indonesia, for their support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Diet R, Niken PY, Novina A, Aman BP. Buku Ajar Endokrinologi. Jakarta: IDAI; 2018:146–206.
2. World Health Organization. Diabetes and genetics. Available from: www.who.int/genomics/about/Diabetis-fin.pdf.
3. Sperling M, Majzoub R, Menon R. Strtakis C Sperling pediatric endocrinology; 2020.
4. Padma-malini R, Rathika C, Ramgopal S, Murali V, Dharmarajan P. Association of CTLA-4 +49 A/G dimorphism and HLA-DRB*/DQ1B1* Alleles with type 1 diabetes from South India. Biochem Genet. 2017. doi:10.1007/s10528-018-9856-7
5. Yanagawa T, Hidaka Y, Guimaraes V, Soliman M. CTLA-4 gene polymorphism associated with Graves’ disease in a Caucasian population. J Clin Endocrinol Metab. 2015;80(1):41–45.
6. Vaidya B, Pearce S. The emerging role of the CTLA-4 gene in autoimmune endocrinopathies. Eur J Endocrinol. 2004;150:619–626.
7. Kavvoura FK, Ioannidis JP. CTLA-4 gene polymorphisms and susceptibility to type 1 diabetes mellitus: a huge review and meta-analysis. Am J Epidemiol. 2005;162:3–16. doi:10.1093/aje/kwi165
8. Mochizuki M, Amemiya S, Kobayashi K, et al. Association of the CTLA-4 gene 49 A/G polymorphism with type 1 diabetes and autoimmune thyroid disease in Japanese children. Diabetes Care. 2003;26:843–847. doi:10.2337/diacare.26.3.843
9. Chen Y, Chen S, Gu Y, et al. CTLA-4+ 49 G/A, a functional T1D risk SNP, affects CTLA-4 level in treg subsets and IA-2A positivity, but not beta-cell function. Sci Rep. 2018;8:1–8. doi:10.1038/s41598-018-28423-9
10. Mie M, Shin A, Kisho K, Koji K. Association of the CTLA-4 gene 49 A/G polymorphism with type 1 diabetes and autoimmune thyroid disease in Japanese children. Diabetes Care. 2003;26:843–847. doi:10.2337/diacare.26.3.843
11. Maryam T, Asad VR, Mozafar K, Zohreh R, Tayebeh P. Cytotoxic T-lymphocyte associated antigen-4 (CTLA-4) polymorphism, cancer, and autoimmune diseases. AIMS Med Sci. 2017;4:395–412. doi:10.3934/medsci.2017.4.395
12. Rita S, Daniele S. The soluble CTLA-4 receptor and its emerging role in autoimmune diseases. Curr Immunol Rev. 2009;5:54–68. doi:10.2174/157339509787314413
13. Wang J, Liu L, Ma J, Gu M. Common variants on cytotoxic t lymphocyte antigen-4 polymorphisms contributes to type 1 diabetes susceptibility: evidence based on 58 studies. PLoS One. 2014;9:1–9.
14. Dorota PL, Ewa S, Daria D, Gładyś A, Skrzypczak R, Brzeziańska E. CTLA-4 gene polymorphisms and their influence on predisposition to autoimmune thyroid diseases (Graves’ disease and Hashimoto’s thyroiditis). Arch Med Sci. 2012;8:415–421. doi:10.5114/aoms.2012.28593
15. Gough SCL, Walker LSK, Sansom DM. CTLA-4 gene polymorphism and autoimmunity. Immunol Rev. 2005;204(1):102–115. doi:10.1111/j.0105-2896.2005.00249.x
16. Touma Z, Hamdan A, Shamseddeen W, et al. CTLA-4 gene variants are not associated with Behçet’s disease or its clinical manifestations. Clin Exp Rheumatol. 2008;26:S132.
17. Wang L, Li D, Fu Z, et al. Association of ctla-4 gene polymorphisms with sporadic breast cancer in Chinese han population. BMC Cancer. 2007;7:173. doi:10.1186/1471-2407-7-173
18. Saverino D, Simone R, Bagnasco M, Pesce G. The soluble CTLA-4 receptor and its role in autoimmune diseases: an update. Auto Immun Highlights. 2010;1:73–81. doi:10.1007/s13317-010-0011-7
19. Saleh HM, Koeleman B, Szénási G, Rosivall L, Hamar P. Association of CTLA-4 polymorphisms with type 1 diabetes in the Egyptian population. J Diabetes Metab. 2013;4:291. doi:10.4172/2155-6156.1000291
20. Tanhapour M, Vaisi-Raygani A, Khazaei M, Rahimi Z, Pourmotabbed T. Pourmotabbed, T. cytotoxic T-lymphocyte associated antigen-4 (CTLA-4) polymorphism, cancer, and autoimmune diseases. AIMS Med Sci. 2017;4:395–412. doi:10.3934/medsci.2017.4.395
21. Pastuszak-Lewandoska D, Sewerynek E, Domańska D, Gładyś A, Skrzypczak R, Brzeziańska E. CTLA-4 gene polymorphisms and their influence on predisposition to autoimmune thyroid diseases (Graves’ disease and Hashimoto’s thyroiditis). Arch Med Sci. 2012;8:415. doi:10.5114/aoms.2012.28593
22. Lee YJ, Huang FY, Lo FS, et al. Association of CTLA4 gene A–G polymorphism with type 1 diabetes in Chinese children. Clin Endocrinol. 2000;52:153–157. doi:10.1046/j.1365-2265.2000.00929.x
23. Çelmeli F, Türkkahraman D, Özel D, Akçurin S, Yeğin O. CTLA-4 (+ 49A/G) polymorphism and type-1 diabetes in Turkish children. J Clin Res Pediatr Endocrinol. 2013;5:40. doi:10.4274/Jcrpe.879
24. Jaya RI, Zettyana YR, Bakri A, Yuwono Y, Aditiawati A. Polymorphisms associated with type 1 diabetes mellitus. Paediatr Indones. 2018;58:274–279. doi:10.14238/pi58.6.2018.274-9
25. Balic I, Angel B, Codner E, Carrasco E, Pérez-Bravo F. Association of CTLA-4 polymorphisms and clinical-immunologic characteristics at onset of type 1 diabetes mellitus in children. Hum Immunol. 2009;70:116–120. doi:10.1016/j.humimm
26. Kheiralla KEK. CTLA-4 (+49A/G) polymorphism in type 1 diabetes children of Sudanese population. Glob Med Genet. 2021;8:011–018. doi:10.1055/s-0041-1723008
27. Rochmah N, Faizi M, Hisbiyah Y, Triastuti IW, Wicaksono G, Endaryanto A. Quality of life differences in pre- and post-educational treatment in type 1 diabetes mellitus during COVID-19. Diabetes Metab Syndr Obes. 2021;14:2905–2911. PMID:34234488; PMCID: PMC8254028. doi:10.2147/DMSO.S313575
28. Gomes KF, Semzezem C, Batista R, Fukui RT, Santos AS, Correia MR. Importance of Zinc Transporter 8 Autoantibody in the diagnosis of type 1 diabetes in Latin Americans. Sci Rep. 2017;7(1):207. PMID:28303020; PMCID:PMC5428214. doi:10.1038/s41598-017-00307-4
29. Bhatty A, Baig S, Fawwad A, Rubab ZE, Shahid MA. Association of Zinc Transporter-8 Autoantibody (ZnT8A) with type 1 diabetes mellitus. Cureus. 2020;12(3):1–8.
30. Braga de Souze AC, Felicio JS, Neto JF, Mileo KB, Santos FM. Brazilian Type 1 Diabetes Study Group (BrazDiab1SG). Health-related quality of life in people with type 1 diabetes mellitus: data from the Brazilian Type 1 Diabetes Study Group. AIMS Med Sci. 2015;13:13–204. PMID: 26703221; PMICD: PMC4690259.
31. Kiani AK, John P, Bhatti A, Zia A, Shahid G, Akhtar P. Association of 32 type 1 diabetes risk loci in Pakistani patients. Diabetes Res Clin Pract. 2015;108(1):137–142. doi:10.1016/j.diabres.2015.01.022
32. Achenbach P, Lampasona V, Landherr U. Autoantibodies to zinc transporter 8 and SLC30A8 genotype stratify type 1 diabetes risk. Diabetologi. 2009;52(9):1881–1888. doi:10.1007/s00125-009-1438-0
33. Mattana TC, Santos AS, Fukui RT, Mainardi-Novo DT, Costa VS, Santos RF. CD226rs763361 is associated with the susceptibility to Type 1 diabetes and a greater frequency of GAD65 autoantibody in a Brazilian cohort. Mediator Inflamm. 2014;2014:694948. doi:10.1155/2014/694948
34. Jin P, Xiang B, Huang G, Zhou Z. The association of cytotoxic T-lymphocyte antigen-4 + 49 A/G and CT 60 polymorphism with type 1 diabetes and latent autoimmune diabetes in Chinese Adults. J endocrinol Invest. 2015;38:149–154.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.