Back to Journals » Journal of Pain Research » Volume 15
Cross-Sectional Brain-Predicted Age Differences in Community-Dwelling Middle-Aged and Older Adults with High Impact Knee Pain
Authors Johnson AJ ![]() , Buchanan T, Laffitte Nodarse C, Valdes Hernandez PA
, Buchanan T, Laffitte Nodarse C, Valdes Hernandez PA ![]() , Huo Z
, Huo Z ![]() , Cole JH
, Cole JH ![]() , Buford TW, Fillingim RB, Cruz-Almeida Y
, Buford TW, Fillingim RB, Cruz-Almeida Y ![]()
Received 5 August 2022
Accepted for publication 25 October 2022
Published 16 November 2022 Volume 2022:15 Pages 3575—3587
DOI https://doi.org/10.2147/JPR.S384229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Alisa J Johnson,1,2,* Taylor Buchanan,3,* Chavier Laffitte Nodarse,1,2 Pedro A Valdes Hernandez,1,2 Zhiguang Huo,4 James H Cole,5,6 Thomas W Buford,3 Roger B Fillingim,1,2,7 Yenisel Cruz-Almeida1,2,7
1Pain Research & Intervention Center of Excellence, University of Florida, Gainesville, FL, USA; 2Department of Community Dentistry & Behavioral Science, College of Dentistry, University of Florida, Gainesville, FL, USA; 3Department of Medicine, University of Alabama, Birmingham, AL, USA; 4Department of Biostatistics, College of Public Health & Health Professions College of Medicine, University of Florida, Gainesville, FL, USA; 5Centre for Medical Image Computing, Department of Computer Science, University College London, London, UK; 6Dementia Research Centre, Institute of Neurology, University College London, London, UK; 7Department of Neuroscience, College of Medicine, University of Florida, Gainesville, FL, USA
*These authors contributed equally to this work
Correspondence: Yenisel Cruz-Almeida, University of Florida, PO Box 103628, 1329 SW 16th Street, Ste 5180, Gainesville, FL, 32608, USA, Tel +1 352-294-8584, Fax +1 352-273-5985, Email [email protected]
Purpose: Knee OA-related pain varies in impact across individuals and may relate to central nervous system alterations like accelerated brain aging processes. We previously reported that older adults with chronic musculoskeletal pain had a significantly greater brain-predicted age, compared to pain-free controls, indicating an “older” appearing brain. Yet this association is not well understood. This cross-sectional study examines brain-predicted age differences associated with chronic knee osteoarthritis pain, in a larger, more demographically diverse sample with consideration for pain’s impact.
Patients and Methods: Participants (mean age = 57.8 ± 8.0 years) with/without knee OA-related pain were classified according to pain’s impact on daily function (ie, impact): low-impact (n=111), and high-impact (n=60) pain, and pain-free controls (n=31). Participants completed demographic, pain, and psychosocial assessments, and T1-weighted magnetic resonance imaging. Brain-predicted age difference (brain-PAD) was compared across groups using analysis of covariance. Partial correlations examined associations of brain-PAD with pain and psychosocial variables.
Results: Individuals with high-impact chronic knee pain had significantly “older” brains for their age compared to individuals with low-impact knee pain (p < 0.05). Brain-PAD was also significantly associated with clinical pain, negative affect, passive coping, and pain catastrophizing (p’s< 0.05).
Conclusion: Our findings suggest that high impact chronic knee pain is associated with an older appearing brain on MRI. Future studies are needed to determine the impact of pain-related interference and pain management on somatosensory processing and brain aging biomarkers for high-risk populations and effective intervention strategies.
Keywords: knee osteoarthritis, high impact chronic pain, brain aging, experimental pain, psychosocial
Introduction
Knee osteoarthritis (OA) is a leading cause of chronic pain among middle-aged and older adults, and contributes to significant physical disability and global disease burden.1,2 However, the impact of knee OA-related pain is variable,3,4 and the factors contributing to this heterogeneity are poorly understood.5,6 Recent evidence indicates that factors beyond OA radiographic pathology underlie pain in knee OA,7 including systemic factors (eg, inflammation, gut microbiome, nervous system).8–10 Specifically, structural and functional brain changes have been demonstrated in those with chronic knee OA-related pain,11,12 including gray matter decline in the primary motor cortex, left temporal lobe, and precuneus cortex,13 similar to changes observed in aging.14,15 Given the overlap in pain- and age-related changes in brain structure, it is possible that chronic pain may exacerbate typical age-related brain atrophy, and increase the risk for poor health outcomes.16
Technological advances have led to the development of brain aging biomarkers, which are able to detect deviations from healthy brain aging patterns, allowing for the investigation of accelerated biological aging specific to the brain.17–19 Brain aging biomarkers are estimated by training machine-learning algorithms using large structural magnetic resonance imaging (MRI) datasets from thousands of healthy individuals across a wide age span (eg, 18–90 years).20 In our prior work, we investigated an established brain aging biomarker,17,20 and found that older adults reporting chronic musculoskeletal (MSK) pain (ie, pain on most days during activities in the past 3 months) had an “older” appearing brain compared to pain-free age-matched controls.21 Furthermore, we found that an older appearing brain was associated with greater pain intensity, pain sensitivity and inhibition, and positive affect and other personality traits in our sample of older adults.21,22 These findings are consistent with previous research demonstrating sustained untreated pain was associated with added “age-like” brain atrophy.23,24 Furthermore, individuals with chronic pain who also experience daily pain-related limitations (ie, disability) may be at an even greater risk for brain atrophy due to restrictions in activities, decreased social engagement, and greater mental health and cognitive impairments.25
However, the role of brain aging in chronic pain is not clear. In a subsequent study,26 Soros et al did not find evidence of accelerated brain aging in a younger cohort of non-cancer chronic pain patients receiving pain treatment from several pain and rheumatology clinics and the emergency room.26 It is possible that these contrasting findings are due to differences in study population characteristics, including type of pain (eg, pain with and without physical limitation and location), cohort age, and other non-specific factors (eg, treatment seeking, pain relief). However, a recent study found that across three different pain conditions, individuals with osteoarthritis pain and trigeminal neuralgia showed significantly older appearing brains.27 Despite these findings, there has been limited examination of the global brain aging patterns in persons with chronic pain. Given that brain aging as measured employing brain aging biomarkers has been associated with worse cognitive performance, increased likelihood for chronic disease (eg, cardiovascular diseases), and increased mortality,17,28–30 it is imperative to elucidate the relationship between chronic pain and brain aging to identify adults at greater risk for cognitive and physical function decline.22,31
Therefore, we hypothesized that adults reporting chronic knee OA-related pain with high-impact chronic pain (ie, pain limiting daily function) would present with an older-appearing brain compared to those with less limiting pain, or those with no pain. We further hypothesized that brain aging would be associated with experimental pain sensitivity and psychosocial factors previously associated with knee OA pain, in line with the biopsychosocial model of chronic pain. The purpose of this study was to examine brain predicted age differences in the largest sample studied to date, including a more demographically diverse cohort of middle-aged and older adults with a specific chronic pain condition (ie, chronic knee pain), presenting with variable levels of pain-related disability.25,32 The present study furthers our understanding of the association between chronic pain and brain aging patterns by examining these associations in pain-free individuals and those with low impact and high impact chronic knee pain.
Materials and Methods
Participants
The current study sample was recruited as part of a multisite observational study aimed at examining ethnic/race group differences in individuals with or at risk for knee osteoarthritis (OA). The larger parent study was conducted at the University of Florida (UF) and the University of Alabama, Birmingham. The study was approved by the University of Florida (UF) and University of Alabama, Birmingham (UAB) Institutional Review Boards (IRB#201400209), under the Common Rule which requires the use of single IRB for US based institutions engaged in cooperative research. UF served as the Institutional Review Board of Record, providing regulatory and ethical oversight of the research. The study was carried out in accordance with the Declaration of Helsinki. Power calculations were conducted a priori to examine brain-PAD group differences (1-β = 0.80, two-sided α = 0.05) to detect a medium-sized effect ( = 0.06 and Cohen’s f=0.25). Individuals aged 45–85 years, who spoke English and self-identified as non-Hispanic, and “Black/African American” or “White/Caucasian/European” were recruited from the communities surrounding UF and UAB, between August 2015 and May 2017, using posted fliers, radio/print media, clinic and word-of-mouth referrals. All enrolled participants completed written informed consent and were compensated for their involvement. Individuals were excluded based on the following: 1) prosthetic knee replacement or other clinically significant surgery to the index (arthritic) knee; 2) heart disease, congestive heart failure, or history of acute myocardial infarction; 3) uncontrolled hypertension (blood pressure >150/95 mm Hg); 4) peripheral neuropathy; 5) systemic rheumatic disorders (ie, rheumatoid arthritis, systemic lupus erythematosus, and fibromyalgia); 6) chronic daily opioid use; 7) hospitalization within the preceding year for psychiatric illness; 8) neurological diseases (ie, Parkinson’s, multiple sclerosis, stroke with loss of sensory or motor function, or uncontrolled seizures); 10) pregnant or nursing; and 11) significantly greater body pain in a site other than the knee. Individuals with and without clinical knee OA criteria were included in the parent study.33
= 0.06 and Cohen’s f=0.25). Individuals aged 45–85 years, who spoke English and self-identified as non-Hispanic, and “Black/African American” or “White/Caucasian/European” were recruited from the communities surrounding UF and UAB, between August 2015 and May 2017, using posted fliers, radio/print media, clinic and word-of-mouth referrals. All enrolled participants completed written informed consent and were compensated for their involvement. Individuals were excluded based on the following: 1) prosthetic knee replacement or other clinically significant surgery to the index (arthritic) knee; 2) heart disease, congestive heart failure, or history of acute myocardial infarction; 3) uncontrolled hypertension (blood pressure >150/95 mm Hg); 4) peripheral neuropathy; 5) systemic rheumatic disorders (ie, rheumatoid arthritis, systemic lupus erythematosus, and fibromyalgia); 6) chronic daily opioid use; 7) hospitalization within the preceding year for psychiatric illness; 8) neurological diseases (ie, Parkinson’s, multiple sclerosis, stroke with loss of sensory or motor function, or uncontrolled seizures); 10) pregnant or nursing; and 11) significantly greater body pain in a site other than the knee. Individuals with and without clinical knee OA criteria were included in the parent study.33
Procedures
Following an initial phone screening, during which sociodemographic (eg, sex, age, ethnicity/race), and health information (eg, brief health history and symptoms of knee OA) were collected, individuals were scheduled for a baseline health assessment session (HAS). The HAS consisted of a health and pain history, and physical examination to determine the most painful (ie, index) knee. Radiographs were collected and graded by the study’s rheumatologist according to the Kellgren–Lawrence (KL) classification.34 Quantitative sensory testing (QST) occurred approximately 1 week later. Magnetic resonance imaging (MRI) was completed approximately 1 week after the QST session. Participants completed clinical pain measures within 24 hours of the QST session, and psychosocial questionnaires were completed within 24 hours of the MRI.
Measures
Clinical Pain Measures
Graded Chronic Pain Scale (GCPS)
The GCPS, a validated and reliable measure, was used to assess pain intensity and pain-related disability.35 Participants were asked to rate on a 0 (“no pain”) to 10 (“pain as bad as could be”) numerical rating scale (NRS) their current, average, and worst pain in the past 6 months. Similarly, pain-related disability items (ie, how much pain has interfered with daily activities, recreational/social/family activities, and ability to work) on average, over the past 6 months, were rated on a 0 (“no inference”) to 10 (“unable to carry out activities”) scale. Ratings were averaged and multiplied by 10 to yield a 0–100 score for each domain, with higher scores indicating greater pain intensity and pain-related disability. Another item asked “How many days in the last six months have you been kept from your usual activities because of pain?” Pain-related disability points were calculated from 1) the averaged ratings (ie, 0–29 = 0 points; 30–49 = 1 point; 50–69 = 2 points; ≥70 = 3 points) and 2) total number of disability days (ie, 0–6 days = 0 points; 7–14 days = 1 point; 15–30 days = 2 points; 31 days or more = 3 points). Disability points were summed. GCPS pain intensity and disability point scores were then combined as follows: Grade 0 = no reported pain intensity; Grade 1 = low pain intensity (ie, <50) and low disability (ie, <3 disability points); Grade 2 = high pain intensity (ie, ≥50) and low disability; Grade 3 = high disability-moderately limiting (ie, 3–4 disability points), regardless of pain intensity; Grade 4 = high disability-severely limiting (ie, 5–6 disability points), regardless of pain intensity.35 Consistent with the recommendations from the Task Force for the Classification of Chronic Pain consensus for the 11th version of the International Classification of Diseases (ICD-11) of the World Health Organization (WHO),32 and the Graded Chronic Pain Scale-Revised,36 Pain Grades were used to classify individuals without (ie, Grade 0), or with (ie, Grades 1–4) chronic pain, and as low-impact (ie, Grades 1–2), and high-impact (ie, Grades 3–4) chronic knee pain.
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The WOMAC pain subscale assessed lower extremity pain related to arthritis over the past 48 hours on a 5-point scale, with higher scores indicating greater pain severity.37
MRI Pain Ratings
Participants were asked to rate their current knee pain on a 0 (“no pain”) to 100 (“worst pain imaginable”) NRS immediately prior to MRI scanning.
Psychosocial Measures
In vivo Coping (IVC)
The IVC scale consists of 10 items which assess Passive (eg, “I felt that if the pain got any worse I wouldn’t be able to tolerate it.”), and Active (eg, “I thought of other things to get my mind off the pain.”) situational pain coping. Items were rated from 1 (“not at all”) to 5 (“very much”), with totals computed as the sum of items from each domain (ie, Passive and Active).38 The IVC was administered following quantitative sensory testing (QST) to provide a measure of in vivo coping during experimental pain.
Positive and Negative Affect Scale (PANAS)
The PANAS consists of 20 words used to describe positive (PA) and negative (NA) affect. Participants were asked to rate how they “generally feel” on a 5-point Likert-type scale, with higher scores indicating greater PA or NA.39
Pain Catastrophizing
Pain catastrophizing was assessed using the Coping Strategies Questionnaire-Revised (CSQ-R) catastrophizing subscale,40 which consists of six items that assess the helplessness dimension of pain catastrophizing, with higher scores representing greater catastrophizing.
Experimental Pain Measures
Multimodal Quantitative Sensory Testing (QST) was used to assess experimental pain sensitivity using a standardized protocol, as previously reported.41 All QST procedures were performed by trained study staff in a quiet room, with participants comfortably seated. The experimenter played recorded instructions prior to each test and participant understanding was checked.
Heat Pain
A Medoc Pathway Thermal Sensory Analyzer (Ramat Yishai, Israel) delivered heat stimuli to the medial joint line of the index knee (ie, most painful or randomly assigned for pain-free controls) and ipsilateral forearm to assess heat pain threshold (ie, first sensation of pain; HPTh), and heat pain tolerance (ie, point at which pain could no longer be tolerated; HPTol). Each trial began at a baseline temperature of 32°C and temperature gradually increased at a rate of 0.5°C/second until the participant ended the trial by pressing a button. The mean or trimmed mean of three trials within 3°C for each detection measure was used in the analysis. Participants also rated pain on a 0–100 NRS following a train of five heat pulses delivered at 44°C, 46°C, and 48°C successively to both testing sites in random order. Heat pain after sensations were also rated at 15 and 30 seconds after the last stimulus for each temperature and testing site. Heat pain threshold, tolerance and pain ratings were averaged separately for each temperature and testing site and standardized.42 Heat pain threshold and heat pain tolerance values were reversed, and all standardized values were combined to calculate a heat pain sensitivity index.
Mechanical Pain
A handheld digital pressure algometer (Algomed, Medoc, Ramat Yishai, Israel) assessed pressure pain threshold (PPT) at the medial and lateral joint line of the index knee, the ipsilateral quadriceps, and trapezius. A constant rate of pressure (30 kPa/second) was applied to each site, and ended when the participant pressed a button indicating their first experience of pain. Maximum pressure levels (600 kPa for knee sites, 1000 kPa for quadriceps and trapezius) were predetermined to maintain participant safety. The means or trimmed means of three trials within 40 kPa were calculated for each testing site and standardized (z-scored), reversed, and averaged to create an overall pressure pain sensitivity index.
Punctate Temporal Summation (TS)
Punctate TS was determined by using a nylon monofilament (Touchtest Sensory Evaluator 6.65) calibrated to bend at 300g applied to the index patella and back of the ipsilateral hand. Order of testing site was randomized across participants. Pain was rated (0–100 NRS) after a single, and a series of 10 contact(s). The procedure was repeated twice at each testing site. Difference scores of the average pain rating following a single stimulus and the average pain rating following 10 stimuli were computed for each test site, standardized, and combined to create a punctate temporal summation score used in the analysis.
Conditioned Pain Modulation (CPM)
Pressure pain threshold (PPT), as described above, was delivered to left trapezius as the test stimulus. Participants then placed their right hand, up to the wrist, into a cold-water bath (ie, conditioning stimulus) maintained at 12°C (Neslab refrigeration unit, Portsmouth, NH, USA). After 30 seconds, PPT was assessed again. CPM was calculated as follows: [(prePPT – duringPPT)/prePPT]×100, with negative values indicating pain inhibition. CPM served as a proxy measure of endogenous pain inhibition.
Neuroimaging
MRI data was collected at the University of Florida using a 3-tesla Phillips (Best, the Netherlands) scanner using a 32-channel radio-frequency coil, and an 8-channel head coil at the University of Alabama – Birmingham. A high-resolution, T1-weighted turbo field echo anatomical scan was collected using the following parameters: TR = 7.0 ms, TE = 3.2 ms, 176 slices acquired in a sagittal orientation, flip angle = 8 degrees, resolution = 1 mm3. Head movement was minimized via cushions positioned inside the head coil and instructions to participants.
Brain Aging Biomarker
The brain aging biomarker used here was derived using a previously established “brain-age” framework.20 This involved training a machine-learning model to accurately predict chronological age from neuroimaging data in a training cohort comprised 3377 healthy individuals (age mean = 40.6 ± 21.4 years; age range = 18–92 years) and a testing cohort of 857 healthy adults (mean age 40.1 ± 21.8 years, age range = 18–90 years) amalgamated from seven public datasets. Thus, the training and testing cohorts were independent, but derived from the same scanning sites. The training datasets were screened according to local study protocols to ensure that they were free of neurological and psychiatric disorders, had no history of head trauma and other major medical conditions.17 Ethical approval for each initial study and subsequent data sharing was verified for each data repository. Models used segmented and spatially normalized T1-weighted MRI scans as the predictor variables in a Gaussian process regression, with chronological age as the outcome variable. Model accuracy based on the held-out test data (using random assignment to training and test) was high, with a mean absolute error of 3.93 years and a correlation between chronological age and “brain-predicted” age of r = 0.97, R2 = 0.95. Then, using the regression model trained on the full independent dataset (n = 3377), brain-predicted age values were generated for the n = 202 participants in the current study. Consistent with our prior work,21 the individual participants’ chronological age was subtracted from the brain-predicted age value to generate the brain-predicted age difference (brain-PAD) used for the current analysis.
Data Analysis
Data were checked for normality, outliers, and conformance to assumptions. One-way analysis of variance (ANOVA) and χ2 were used to test for group differences for continuous/discrete ordinal and nominal variables, respectively. One-way analysis of covariance (ANCOVA) was conducted accounting for sex, race, age, and study site similar to our previous work,21 to compare brain-PAD between pain impact groups. These covariates were chosen based on prior literature,43 and differences between pain impact groups in the current sample. Additionally, we investigated the potential role of radiographic pathology (ie, KL grade) on the relationship between pain impact and brain-PAD, adjusting for the same covariates. A probability less than 0.05 was considered statistically significant. Bonferroni post hoc comparisons were conducted. Pearson partial correlations were used to assess associations between brain-PAD with clinical and experimental pain and psychological variables, accounting for age, sex, race, and study site in the total sample. Bootstrapping procedures with 5000 samples were employed for all analyses and reported as 95% Bias-corrected and accelerated (BCa) bootstrapped confidence intervals. For the analyses examining associations of brain-PAD with self-reported and experimental pain, as well as psychological function, we report both uncorrected (ie, p =) and corrected probability values (ie, corrected p =) adjusting for multiple comparisons applying the Holm–Bonferroni method,44 using the calculator by Gaetano.45 Data analyses were performed using IBM SPSS 27 software.
Results
Demographic Characteristics
Two-hundred and two individuals (mean age = 58.2 ± 8.2; 65.5% female) completed all study measures. Demographic and clinical characteristics by pain impact groups are presented in Table 1. There was a significant difference in race (p < 0.05), pain severity and pain-related disability (p’s < 0.001), across pain impact groups, such that non-Hispanic Blacks were overrepresented in the High Impact Chronic Pain (HICP) group, and those in the HICP group reported greater pain and pain-related disability.
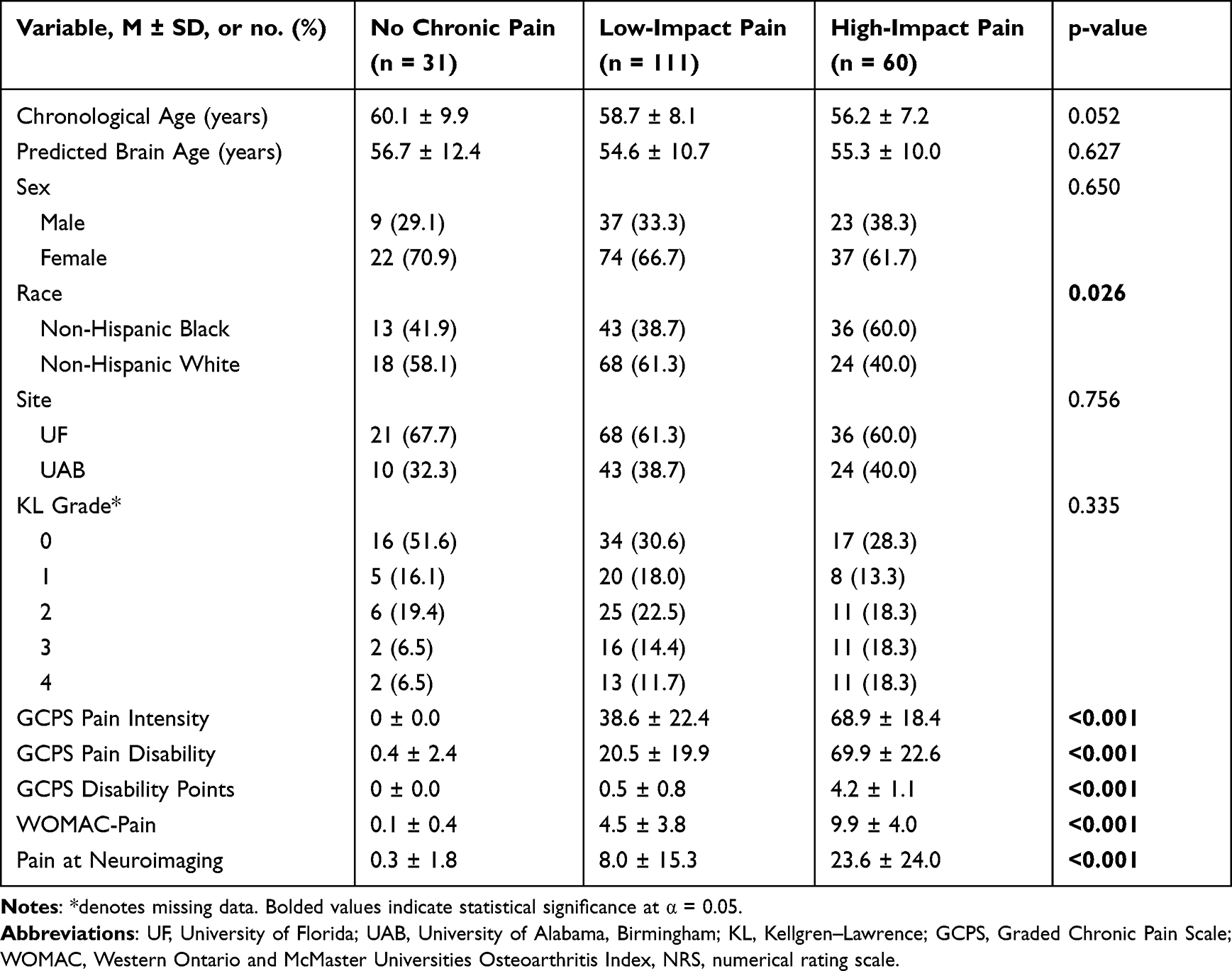 |
Table 1 Demographic and Clinical Characteristics Across Pain Impact Groups |
Brain-PAD Differences Between Pain Impact Groups
The results from an ANCOVA comparing brain-PAD between Pain Impact Groups showed significant differences in brain-PAD (F (2195) = 3.82, p = 0.024,  = 0.04, Figure 1. Post-hoc tests revealed those with High Impact Chronic knee pain had a significantly “older” brain age pattern than those with Low Impact Chronic knee pain (mean difference = 3.25 ± 1.2, Bonferroni corrected p = 0.019, BCa 95% CI: 1.15, 5.32). Pain impact groups also differed significantly on brain-PAD even when including KL grade in the analysis (F (2189) = 3.43, p = 0.034,
= 0.04, Figure 1. Post-hoc tests revealed those with High Impact Chronic knee pain had a significantly “older” brain age pattern than those with Low Impact Chronic knee pain (mean difference = 3.25 ± 1.2, Bonferroni corrected p = 0.019, BCa 95% CI: 1.15, 5.32). Pain impact groups also differed significantly on brain-PAD even when including KL grade in the analysis (F (2189) = 3.43, p = 0.034,  = 0.04).
= 0.04).
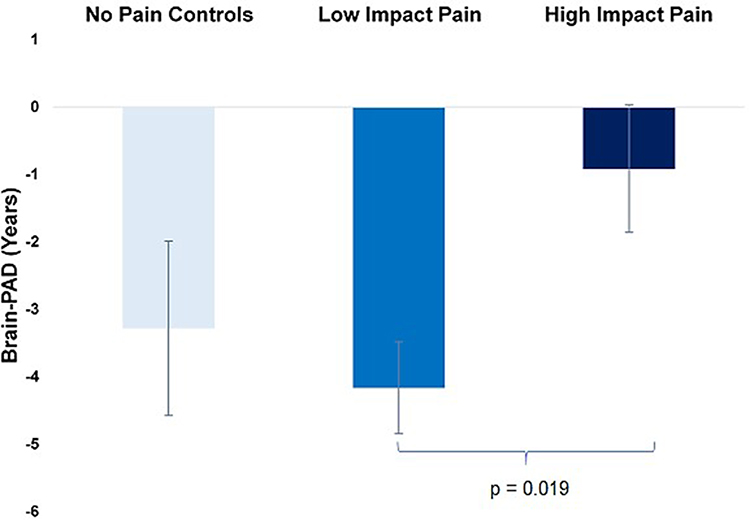 |
Figure 1 Brain-PAD in years across pain impact groups. Values above the origin indicate an increase in brain-PAD, calculated as brain-predicted age minus chronological age. Covariates include age, sex, race, and study site. Error bars represent ±2 standard errors. |
Brain-PAD Associations with Self-Reported Pain
Adjusted partial correlations suggested that brain-PAD was significantly correlated with average GCPS pain intensity (r = 0.15, p = 0.039, corrected p = 0.273, BCa 95% CI: 0.02, 0.28), clinical pain at the MRI session (r = 0.20, p = 0.006, corrected p = 0.072, BCa 95% CI: 0.08, 0.31), and WOMAC pain ratings (r = 0.14, p = 0.044, corrected p = 0.273, BCa 95% CI: 0.01, 0.27), Figure 2.
 |
Figure 2 Partial correlations between brain-PAD and (A) GCPS pain intensity, (B) Clinical knee pain at MRI, and (C) WOMAC-Pain, and (D) Heat pain sensitivity, adjusting for age, sex, race, and study site. |
Brain-PAD Associations with Experimental Pain
Adjusted partial correlations controlling for sex, race, age, and study site suggested that brain-PAD was significantly associated with experimental heat pain sensitivity (r = 0.19, p = 0.008, corrected p = 0.072, BCa 95% CI: 0.03, 0.34), Figure 2. There were no significant associations between brain-PAD with endogenous pain inhibition (r = −0.02, p = 0.848, corrected p = 1.0.), punctate temporal summation (r = 0.07, p = 0.327, corrected p = 1.0), or pressure pain sensitivity (r = 0.01, p = 0.844, corrected p = 1.0).
Brain-PAD Associations with Psychosocial Factors
Brain-PAD was significantly associated with PANAS-Negative Affect (r = 0.17, p = 0.023, corrected p = 0.184, BCa 95% CI: 0.03, 0.29), IVC-Passive (r = 0.19, p = 0.007, corrected p = 0.072, BCa 95% CI: 0.06, 0.32), and Pain Catastrophizing (r = 0.19, p = 0.006, corrected p = 0.072, BCa 95% CI: 0.08, 0.31), adjusting for age, sex, race, and study site (Figure 3).
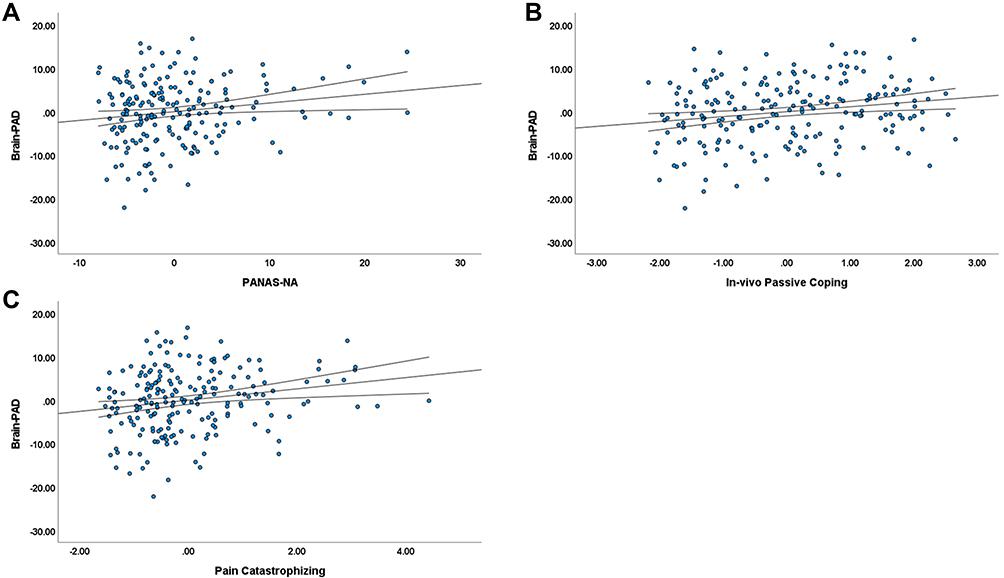 |
Figure 3 Partial correlations between brain-PAD and (A) Positive and Negative Affect Schedule – Negative Affect (PANAS-NA), (B) In vivo Passive Coping, and (C) CSQ-R Pain Catastrophizing, adjusting for age, sex, race, and study site. |
Discussion
To our knowledge, this is the first study to examine predicted brain age differences in chronic pain with consideration for the impact of both pain intensity and its daily interference (ie, pain impact). Our main hypothesis was supported, as there were significant differences in brain-predicted age differences (brain-PAD) between individuals with high- and low-impact chronic knee pain. Specifically, those with high-impact chronic knee pain (ie, chronic pain with severe physical limitations) had “older” appearing brains compared to individuals with low-impact chronic knee pain, regardless of age, sex, race, and study site. This finding did not change with consideration for radiographic joint degeneration, and is in line with our prior work demonstrating advanced brain aging among older individuals reporting chronic pain experienced during daily activities.21 High-impact chronic pain (HICP) is a relatively new pain classification conceptualized by the US National Pain Strategy, and was developed to overcome the limitations in previous definitions of chronic pain that relied solely on pain symptom duration.46,47 Population-based studies indicate that HICP places individuals at increased odds of severe pain, physical disability, and cognitive impairment.25,48 While the effects of HICP are just beginning to be examined, the relationship with brain aging is similar to that seen with other debilitating chronic diseases,17,18 and may indicate that those with HICP are at an increased risk for accelerated biological aging.
In line with our previous findings, predicted brain age was positively associated with clinical knee pain and pain reported at the MRI session, with “older” predicted brain age related to greater clinical pain.21 We found a significant positive association between predicted brain age differences and heat pain sensitivity in the current sample, with greater sensitivity associated with an “older” appearing brain. Although these findings did not survive multiple comparison corrections, the pattern of associations between clinical pain and brain-PAD indicates a positive relationship between brain aging and greater pain that warrants further examination. Also, variability in associations of brain aging with different measures of pain sensitivity may be related to stimuli-specific pain mechanisms. Future studies are needed to elucidate whether there are associations between QST measures and brain aging and further, to determine if QST may provide additional predictive value to biological aging biomarkers such as brain-predicted age.
Brain aging was also associated with passive coping, negative affect, and pain catastrophizing, indicating an “older” brain age was related to greater psychosocial distress in our participants; however, these associations were no longer significant after correction for multiple comparisons. In our previous study, we found associations between a “younger” brain age and positive affect in persons with chronic MSK pain, with no associations with negative affect.21 The significantly younger age of the present sample (mean age ~58 years) compared to our previous study in older adults (mean age ~71 years),21 may have contributed to differences in study findings. Specifically, older adults compared to younger individuals attend to, and remember more positive than negative information (ie, the “positivity effect”),49 which may help to explain why the relationship between positive affect and less brain aging was evident in our prior study, but not in the current sample. Nonetheless, our findings appear consistent with the idea that affective disorders, such as major depressive disorder, characterized by chronic negative affect, may impact brain aging processes as evidenced by the brain-PAD biomarker.50 Our findings are also supported by prior research demonstrating an apparent role for the corticolimbic circuitry, which is implicated in the emotional processing of pain, in pain chronification.23,51,52 While the brain aging algorithm used in the current study does not provide a specific location where the brain aging occurs, it does recognize that there are multiple signatures of “healthy” brain aging, and that deviations from “normal” brain aging patterns can vary. Indeed, our findings are consistent with maladaptive psychosocial characteristics associated with reductions in grey matter,53–55 and point to the importance of pain’s psychosocial impact on brain aging patterns.
A greater understanding of brain aging in relation to chronic pain holds substantial clinical utility for several reasons. First, brain aging biomarkers are clinically accessible, and can be easily calculated from routine structural MRI sequences that do not require large amounts of time to acquire or interpret. Second, brain aging biomarkers have the potential to evaluate potential treatments to improve health span in our aging population. For example, treatments such as exercise and joint replacement have reported grey matter increases comparable to changes in clinical pain.56–59 While conservative non-pharmacological interventions (eg, dry needling, manual therapy) show promise for reducing pain in knee OA,60–62 future prospective studies are needed to test whether various pharmacological and non-pharmacological pain interventions can modulate brain aging biomarkers to further understand the influence of different pain management strategies on brain aging. Third, brain age biomarkers may be used to identify individuals with chronic pain who are at a greater risk for accelerated biological aging, allowing for earlier intervention strategies and the prevention of detrimental health challenges.
Limitations
Several limitations must be considered when interpreting these results. While the current sample was diverse and included middle-aged and older adults, a larger sample would have enabled us to stratify by age group and directly compare predicted brain age differences across the lifespan. In addition, our groups were very diverse regarding pain impact, which may have contributed to the small effect sizes in the current study compared with our previous study showing larger effects among community-dwelling older adults with/without chronic pain. However, by including individuals with high- and low-impact chronic knee pain, compared to pain-free age-matched controls, we were able to examine brain aging in accordance with the biopsychosocial model of pain.63 Second, the study was cross-sectional and causality cannot be determined. It is likely that the relationship between predicted brain aging and pain is bidirectional and future longitudinal studies aimed at understanding the clinical significance of predicted brain aging differences, and its ability to predict treatment outcomes in pain are warranted. Third, screening criteria for the current study excluded those with clinical depression, cognitive impairment, and neurological diseases. While this may limit the generalizability of our current findings, it also removed potential confounders as previous research has shown associations between predicted brain age differences, cognitive impairment, and psychological function.17,28 Also, as our study focused on persons with chronic knee pain related to knee OA, generalizability to other chronic pain conditions is limited. Future studies, including participants with other specific chronic pain conditions are needed to further elucidate the association between brain age and chronic pain impact.
Conclusion
This study provides initial evidence of the effects of pain impact on predicted brain age differences in middle-aged and older adults, and provides additional evidence for an increased neurobiological burden in persons with high-impact chronic knee pain. Further, the results from this larger cohort study indicate that a brain aging biomarker is associated with pain impact regardless of chronological age or sex, and is related to clinical pain, and psychosocial factors. Applying biological aging biomarkers represents one valuable way for overcoming challenges with identifying biomarkers at the individual level and could assist in the development of targeted interventions for persons with debilitating chronic pain. Further, brain aging biomarkers can be derived from routine, short MRI sequences that can be easily implemented clinically; thus, it may be a useful, simple biomarker for identifying those individuals with pain who are at a greater risk of accelerated brain atrophy and poor health outcomes.
Acknowledgments
We are grateful to our participants and the UPLOAD2 study teams at the University of Florida and the University of Alabama, Birmingham.
Funding
This work was supported by NIH/NIA Grants R01AG059809, R01AG067757 (YCA); R37AG033906 (RBF); K02AG062498 (TWB). A portion of this work was performed in the McKnight Brain Institute at the National High Magnetic Field Laboratory’s Advanced Magnetic Resonance Imaging and Spectroscopy (AMRIS) Facility, supported by National Science Foundation Cooperative Agreement No. DMR-1157490 and DMR-1644779 and the State of Florida.
Disclosure
James H Cole reports non-financial support from and shares in BrainKey, and personal fees from and shares in Claritas HealthTech during the conduct of the study. The authors report no other potential conflicts of interest in this work. The abstract of this paper was presented at the 2022 US Association for the Study of Pain (USASP) Scientific Conference as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in May 2022, Journal of Pain; 23(5), Supplement, pg. 42.64
References
1. Cross M, Smith E, Hoy D., et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1323–1330. doi:10.1136/annrheumdis-2013-204763
2. Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain-where to from here? Am J Public Health. 2019;109(1):35–40. doi:10.2105/AJPH.2018.304747
3. Parry E, Ogollah R, Peat G. Significant pain variability in persons with, or at high risk of, knee osteoarthritis: preliminary investigation based on secondary analysis of cohort data. BMC Musculoskelet Disord. 2017;18(1):80. doi:10.1186/s12891-017-1434-3
4. Johnson AJ, Vasilopoulos T, Booker SQ, et al. Knee pain trajectories over 18 months in non-Hispanic Black and non-Hispanic White adults with or at risk for knee osteoarthritis. BMC Musculoskelet Disord. 2021;22(1):415. doi:10.1186/s12891-021-04284-8
5. Kittelson AJ, Schmiege SJ, Maluf K, George SZ, Stevens-Lapsley JE. Determination of pain phenotypes in knee osteoarthritis using latent profile analysis. Pain Med. 2021;22(3):653–662. doi:10.1093/pm/pnaa398
6. Pan F, Tian J, Cicuttini F, Jones G, Aitken D. Differentiating knee pain phenotypes in older adults: a prospective cohort study. Rheumatology. 2018;58(2):274–283. doi:10.1093/rheumatology/key299
7. Finan PH, Buenaver LF, Bounds SC, et al. Discordance between pain and radiographic severity in knee osteoarthritis: findings from quantitative sensory testing of central sensitization. Arthritis Rheum. 2013;65(2):363–372. doi:10.1002/art.34646
8. Sánchez Romero EA, Meléndez Oliva E, Alonso Pérez JL, et al. Relationship between the gut microbiome and osteoarthritis pain: review of the literature. Nutrients. 2021;13(3). doi:10.3390/nu13030716
9. Scanzello CR, Loeser RF. Editorial: inflammatory activity in symptomatic knee osteoarthritis: not all inflammation is local. Arthrit Rheumatol. 2015;67(11):2797–2800. doi:10.1002/art.39304
10. Lee YC, Nassikas NJ, Clauw DJ. The role of the central nervous system in the generation and maintenance of chronic pain in rheumatoid arthritis, osteoarthritis and fibromyalgia. Arthritis Res Ther. 2011;13(2):211. doi:10.1186/ar3306
11. Baliki MN, Geha PY, Jabakhanji R, Harden N, Schnitzer TJ, Apkarian AV. A preliminary fMRI study of analgesic treatment in chronic back pain and knee osteoarthritis. Mol Pain. 2008;4:47. doi:10.1186/1744-8069-4-47
12. Cottam WJ, Iwabuchi SJ, Drabek MM, Reckziegel D, Auer DP. Altered connectivity of the right anterior insula drives the pain connectome changes in chronic knee osteoarthritis. Pain. 2018;159(5):929–938. doi:10.1097/j.pain.0000000000001209
13. Barroso J, Vigotsky AD, Branco P, et al. Brain gray matter abnormalities in osteoarthritis pain: a cross-sectional evaluation. Pain. 2020;161(9):2167–2178. doi:10.1097/j.pain.0000000000001904
14. Fjell AM, Walhovd KB, Fennema-Notestine C, et al. One-year brain atrophy evident in healthy aging. J Neurosci. 2009;29(48):15223–15231. doi:10.1523/JNEUROSCI.3252-09.2009
15. Raz N, Lindenberger U, Rodrigue KM, et al. Regional brain changes in aging healthy adults: general trends, individual differences and modifiers. Cerebral Cortex. 2005;15(11):1676–1689. doi:10.1093/cercor/bhi044
16. Tucker-Drob EM. Neurocognitive functions and everyday functions change together in old age. Neuropsychology. 2011;25(3):368–377. doi:10.1037/a0022348
17. Cole JH, Ritchie SJ, Bastin ME, et al. Brain age predicts mortality. Mol Psychiatry. 2018;23(5):1385–1392. doi:10.1038/mp.2017.62
18. Cole JH, Underwood J, Caan MW, et al. Increased brain-predicted aging in treated HIV disease. Neurology. 2017;88(14):1349–1357. doi:10.1212/WNL.0000000000003790
19. Cole JH, Raffel J, Friede T, et al. Longitudinal assessment of multiple sclerosis with the brain-age paradigm. Ann Neurol. 2020;88(1):93–105. doi:10.1002/ana.25746
20. Cole JH, Franke K. Predicting age using neuroimaging: innovative brain ageing biomarkers. Trends Neurosci. 2017;40(12):681–690. doi:10.1016/j.tins.2017.10.001
21. Cruz-Almeida Y, Fillingim RB, Riley JL, et al. Chronic pain is associated with a brain aging biomarker in community-dwelling older adults. Pain. 2019;160(5):1119–1130. doi:10.1097/j.pain.0000000000001491
22. Cruz-Almeida Y, Cole J. Pain, aging, and the brain: new pieces to a complex puzzle. Pain. 2020;161(3):461–463. doi:10.1097/j.pain.0000000000001757
23. Apkarian AV, Hashmi JA, Baliki MN. Pain and the brain: specificity and plasticity of the brain in clinical chronic pain. Pain. 2011;152(3,Supplement):S49–S64. doi:10.1016/j.pain.2010.11.010
24. Buckalew N, Haut MW, Aizenstein H, et al. Differences in brain structure and function in older adults with self-reported disabling and nondisabling chronic low back pain. Pain Med. 2010;11(8):1183–1197. doi:10.1111/j.1526-4637.2010.00899.x
25. Pitcher MH, Von Korff M, Bushnell MC, Porter L. Prevalence and profile of high-impact chronic pain in the United States. J Pain. 2019;20(2):146–160. doi:10.1016/j.jpain.2018.07.006
26. Soros P, Bantel C. Chronic noncancer pain is not associated with accelerated brain aging as assessed by structural magnetic resonance imaging in patients treated in specialized outpatient clinics. Pain. 2020;161(3):641–650. doi:10.1097/j.pain.0000000000001756
27. Hung PS, Zhang JY, Noorani A, et al. Differential expression of a brain aging biomarker across discrete chronic pain disorders. Pain. 2022;163(8):1468–1478. doi:10.1097/j.pain.0000000000002613
28. Kolbeinsson A, Filippi S, Panagakis Y, et al. Accelerated MRI-predicted brain ageing and its associations with cardiometabolic and brain disorders. Sci Rep. 2020;10(1):19940. doi:10.1038/s41598-020-76518-z
29. Cole JH. Multimodality neuroimaging brain-age in UK biobank: relationship to biomedical, lifestyle, and cognitive factors. Neurobiol Aging. 2020;92:34–42. doi:10.1016/j.neurobiolaging.2020.03.014
30. Biondo F, Jewell A, Pritchard M, et al. Brain-age predicts subsequent dementia in memory clinic patients. medRxiv. 2021;2021. doi:10.1101/2021.04.03.21254781
31. Buckalew N, Haut MW, Aizenstein H, et al. White matter hyperintensity burden and disability in older adults: is chronic pain a contributor? Pm&r. 2013;5(6):471–480. doi:10.1016/j.pmrj.2013.03.004
32. Nugraha B, Gutenbrunner C, Barke A, et al. The IASP classification of chronic pain for ICD-11: functioning properties of chronic pain. Pain. 2019;160(1):88–94. doi:10.1097/j.pain.0000000000001433
33. Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29(8):1039–1049. doi:10.1002/art.1780290816
34. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
35. Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain. Pain. 1992;50(2):133–149.
36. Von Korff M, DeBar LL, Krebs EE, Kerns RD, Deyo RA, Keefe FJ. Graded chronic pain scale revised: mild, bothersome, and high-impact chronic pain. Pain. 2020;161(3):651–661. doi:10.1097/j.pain.0000000000001758
37. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the Hip or knee. J Rheumatol. 1988;15(12):1833–1840.
38. Edwards RR, Campbell CM, Fillingim RB. Catastrophizing and experimental pain sensitivity: only in vivo reports of catastrophic cognitions correlate with pain responses. J Pain. 2005;6(5):338–339. doi:10.1016/j.jpain.2005.02.013
39. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–1070.
40. Riley JL, Robinson ME. CSQ: five factors or fiction?. Clin J Pain. 1997;13(2):156–162.
41. Terry EL, Booker SQ, Cardoso JS, et al. Neuropathic-like pain symptoms in a community-dwelling sample with or at risk for knee osteoarthritis. Pain Med. 2020;21(1):125–137. doi:10.1093/pm/pnz112
42. Cardoso JS, Riley JL, Glover T, et al. Experimental pain phenotyping in community-dwelling individuals with knee osteoarthritis. Pain. 2016;157(9):2104–2114. doi:10.1097/j.pain.0000000000000625
43. Armstrong NM, An Y, Beason-Held L, et al. Sex differences in brain aging and predictors of neurodegeneration in cognitively healthy older adults. Neurobiol Aging. 2019;81:146–156. doi:10.1016/j.neurobiolaging.2019.05.020
44. Holm S, Simple Sequentially A. Rejective multiple test procedure. Scand J Stat. 1979;6(2):65–70.
45. Gaetano J. Data from: Holm-Bonferroni sequential correction: an EXCEL calculator - Ver. 1.2; 2013. doi:10.13140/RG.2.1.3920.0481.
46. Committee IPRC. A Comprehensive Population Health Level Strategy for Pain: National Pain Strategy. Washington, DC: HHS; 2015.
47. Von Korff M, Scher AI, Helmick C, et al. United States national pain strategy for population research: concepts, definitions, and pilot data. J Pain. 2016;17(10):1068–1080.
48. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
49. Mather M, Carstensen LL. Aging and motivated cognition: the positivity effect in attention and memory. Trends Cogn Sci. 2005;9(10):496–502. doi:10.1016/j.tics.2005.08.005
50. Han LKM, Dinga R, Hahn T, et al. Brain aging in major depressive disorder: results from the ENIGMA major depressive disorder working group. Mol Psychiatry. 2020. doi:10.1038/s41380-020-0754-0
51. Yang S, Chang MC. Chronic pain: structural and functional changes in brain structures and associated negative affective states. Int J Mol Sci. 2019;20(13). doi:10.3390/ijms20133130
52. Baliki MN, Apkarian AV. Nociception, pain, negative moods, and behavior selection. Neuron. 2015;87(3):474–491. doi:10.1016/j.neuron.2015.06.005
53. Ikeda E, Li T, Kobinata H, Zhang S, Kurata J. Anterior insular volume decrease is associated with dysfunction of the reward system in patients with chronic pain. Eur J Pain. 2018;22(6):1170–1179. doi:10.1002/ejp.1205
54. Ivo R, Nicklas A, Dargel J, et al. Brain structural and psychometric alterations in chronic low back pain. Eur Spine J. 2013;22(9):1958–1964. doi:10.1007/s00586-013-2692-x
55. Li L, Wu M, Liao Y, et al. Grey matter reduction associated with posttraumatic stress disorder and traumatic stress. Neurosci Biobehav Rev. 2014;43:163–172. doi:10.1016/j.neubiorev.2014.04.003
56. Liu J, Chen L, Tu Y, et al. Different exercise modalities relieve pain syndrome in patients with knee osteoarthritis and modulate the dorsolateral prefrontal cortex: a multiple mode MRI study. Brain Behav Immun. 2019;82:253–263. doi:10.1016/j.bbi.2019.08.193
57. Rodriguez-Raecke R, Niemeier A, Ihle K, Ruether W, May A. Structural brain changes in chronic pain reflect probably neither damage nor atrophy. PLoS One. 2013;8(2):e54475. doi:10.1371/journal.pone.0054475
58. Lewis GN, Parker RS, Sharma S, Rice DA, McNair PJ. Structural brain alterations before and after total knee arthroplasty: a longitudinal assessment. Pain Med. 2018;19(11):2166–2176.
59. Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain. 2011;152(3):566–572. doi:10.1016/j.pain.2010.11.023
60. Sánchez-Romero EA, Pecos-Martín D, Calvo-Lobo C, Ochoa-Sáez V, Burgos-Caballero V, Fernández-Carnero J. Effects of dry needling in an exercise program for older adults with knee osteoarthritis: a pilot clinical trial. Medicine. 2018;97(26):e11255. doi:10.1097/md.0000000000011255
61. Sánchez-Romero EA, González-Zamorano Y, Arribas-Romano A, et al. Efficacy of manual therapy on facilitatory nociception and endogenous pain modulation in older adults with knee osteoarthritis: a case series. Appl Sci. 2021;11(4):1895.
62. Perlman A, Fogerite SG, Glass O, et al. Efficacy and safety of massage for osteoarthritis of the knee: a randomized clinical trial. J Gen Intern Med. 2019;34(3):379–386. doi:10.1007/s11606-018-4763-5
63. Miaskowski C, Blyth F, Nicosia F, et al. A biopsychosocial model of chronic pain for older adults. Pain Med. 2020;21(9):1793–1805. doi:10.1093/pm/pnz329
64. Johnson A, Buchanan T, Laffitte C, et al. Added “Age-like” Brain Patterns with Increasing Pain Impact in Persons with Knee Osteoarthritis Pain: Considerations by Race. The Journal of Pain. 2022;23(5)
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.