Back to Journals » Cancer Management and Research » Volume 17

Cross-Lag Analysis of Prognostic Nutritional Index and Psychosomatic Symptom Clusters in Patients with Lung Cancer: A Longitudinal Study
Authors Li T, Wu Y, Yang Q, Zheng Y, Xu Y, Lin H
Received 24 July 2025
Accepted for publication 23 December 2025
Published 31 December 2025 Volume 2025:17 Pages 3349—3358
DOI https://doi.org/10.2147/CMAR.S556061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Shari Youngblood
Tingting Li,1,* Ying Wu,1,* Qun Yang,1,* Yuanyuan Zheng,1 Yunyun Xu,1 Huan Lin2
1Department of Cardiothoracic Surgery, Jiangsu Province Hospital of Chinese Medicine, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, Nanjing First Hospital, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tingting Li, Department of Cardiothoracic surgery, Jiangsu Province Hospital of Chinese Medicine, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210029, People’s Republic of China, Email [email protected]
Objective: To investigate the development trend of prognostic nutritional index and psychosomatic symptom clusters (multidimensional fatigue, generalized anxiety, difficulty in emotional regulation) in patients with lung cancer, and to analyze their correlation and predictive relationship.
Methods: One hundred and eighty-five patients with lung cancer were selected as the research objects using the convenience sampling method. The prognostic nutritional index and psychosomatic symptom cluster were followed up at T1, T2, and T3 after the operation. Repeated measures ANOVA and cross - lag model were used for statistical testing.
Results: A total of 185 questionnaires were distributed, and 7 invalid questionnaires were excluded, with an effective recovery rate of 96.22%. The results of repeated measurement showed the scores of prognostic nutritional index (F = 3.342, P = 0.031), multidimensional fatigue (F = 5.362, P < 0.001), generalized anxiety (F = 6.003, P < 0.001), and emotional regulation difficulties (F = 0.885, P = 0.420) at the three time points. Results of the cross - lag model: The level of prognostic nutritional index negatively predicted multidimensional fatigue symptoms (T1→T2: β = - 0.415, P = 0.003; T2→T3: β = - 0.433, P = 0.005) and generalized anxiety symptoms (T1→T2: β = - 0.364, P = 0.007; T2→T3: β = - 0.350, P = 0.012). The prognostic nutritional index at T2 significantly and negatively predicted emotional adjustment difficulties at T3 (T1→T2: β = 0.158, P = 0.151; T2→T3: β = - 0.233, P = 0.024). While in the psychosomatic symptom cluster, only multidimensional fatigue negatively predicted the prognostic nutritional index at the next node (T1→T2: β = - 0.314, P = 0.003; T2→T3: β = - 0.342, P = 0.001).
Conclusion: The prognostic nutritional index of patients with lung cancer after surgery is closely related to the psychosomatic symptom cluster. The prognostic nutritional index has a negative predictive effect on the psychosomatic symptom cluster, and the multidimensional fatigue symptom also has a negative predictive effect on the prognostic nutritional index.
Keywords: lung cancer, prognostic nutritional index, psychosomatic symptom clusters, multidimensional fatigue, generalized anxiety, difficulty in emotional regulation, relevance, cross - lag model, nursing
Introduction
The data indicates that lung cancer has become the second most prevalent cancer globally, with 2.35 million new cases and 1.8 million deaths in 2024. In China, lung cancer is the leading cause of both morbidity and mortality.1 The incidence of lung cancer is high among people over 60 years old, which is associated with factors such as smoking, air pollution, and occupational exposure. The mortality rate of lung cancer also ranks among the top across all types of cancers.2 With the improvement of treatment regimens, the 5 - year survival rate of lung cancer patients has gradually risen from 4% to 26%.3
The Prognostic Nutritional Index (PNI), which is calculated based on serum albumin and lymphocyte count, can evaluate patients’ nutritional and immune status and predict the clinical outcome.4 Research indicates that postoperative chemotherapy for lung cancer may lead to a variety of physical and mental symptom clusters in patients, such as fatigue, anxiety, emotional distress, and weakened anti - tumor ability. In some cases, it may even require a reduced dosage or delayed surgery.5
The theoretical framework of the “symptoms–malnutrition–immunosuppression” vicious cycle reveals that chemotherapy-induced gastrointestinal symptom clusters, such as nausea, vomiting, loss of appetite, and taste alterations, serve as the starting point of the cycle. They directly impair nutritional intake and lead to malnutrition.5–7 Meanwhile, emotional and psychological symptom clusters stemming from the disease and its treatment, including anxiety, distress, and cancer-related fatigue, further suppress appetite and increase the body’s energy expenditure. The resulting malnourished state not only weakens physical strength and exacerbates fatigue but also directly induces immunosuppression. This decline in immune function heightens susceptibility to infections, reduces treatment tolerance, and may even undermine antitumor efficacy, thereby creating a self-perpetuating cycle. In this cycle, symptoms worsen malnutrition, malnutrition intensifies immunosuppression, and immunosuppression, in turn, makes symptoms more difficult to control.8 Systematic management of symptom clusters in postoperative lung cancer patients undergoing chemotherapy, particularly early intervention targeting sentinel symptoms and nutritional status, is essential to break this vicious cycle and improve patient outcomes.
However, at present, research on the prognostic nutritional index and psychosomatic symptom clusters in postoperative lung cancer patients is only limited to cross - sectional surveys, and it is not possible to dynamically understand their changes. Understanding the high - incidence stage and the mutual predictive relationship between the prognostic nutritional index and psychosomatic symptom clusters in lung cancer patients is conducive to more targeted interventions. Based on the above research, we make the following assumptions:
Prognostic nutritional indices could predict the psychosomatic symptom clusters at that time and in the next stage.
The psychosomatic symptom cluster may partially predict the prognostic nutritional index at that time and in the next stage.
This study adopts a longitudinal design and uses a cross - lag model to explore the changing trends and mutual predictive relationship between the prognostic nutritional index and mind - body symptom clusters in postoperative lung cancer patients, so as to provide new ideas for clinical staff to improve the prognostic nutritional index and mind - body symptom clusters in lung cancer patients.
Materials and Methods
General Information
The convenience sampling method was used to select lung cancer patients admitted to our hospital from January 2024 to February 2025 as the research subjects.
Inclusion Criteria
- The patients met the standard of clinical diagnosis of non-small cell lung cancer, quasi lung cancer radical;9 for postoperative chemotherapy, and the treatment cycle was 4 cycles.
- Diagnosed less than one month ago;
- Stage IB, Stage II;
- They were adults aged 18 years and above.
- They signed the informed consent and voluntarily provided relevant information.
Exclusion Criteria
- Metastatic lung cancer;
- The patients had concurrent radiotherapy after surgery.
- The missing items in the questionnaire accounted for more than 20% of the total number of items.
- They left the group for any reason.
This study has received ethical approval from Jiangsu Province Hospital of Chinese Medicine (NO: 2023–12,052). This research complies with the Declaration of Helsinki.
Sample Size Calculation
This study uses the method of repeated measurement and the sample size formula.10

According to preliminary experiments, K = 3, repeated measurement error  = 127.2560, the condition of correlation coefficient
= 127.2560, the condition of correlation coefficient  = 0.705, the difference between individual variances
= 0.705, the difference between individual variances  = 183.223, which results in n = 121. Considering that the sample loss rate in the longitudinal study is relatively high, the dropout rate is set to 20n=%. Then, 121/0.80 = 178. A total of 185 lung cancer patients were enrolled in this study.
= 183.223, which results in n = 121. Considering that the sample loss rate in the longitudinal study is relatively high, the dropout rate is set to 20n=%. Then, 121/0.80 = 178. A total of 185 lung cancer patients were enrolled in this study.
Measurement Tools
Questionnaire for Basic Information
The contents include general demographic data (including age, marital status, education level, place of residence, living style, income level), tumor information (tumor type, tumor stage), and previous disease information (hypertension, coronary heart disease, diabetes, etc).
Prognostic Nutritional Index (PNI)
Prognostic nutritional index was calculated from lymphocyte (immune index) and albumin (nutritional index), PNI= serum albumin value (g/L) +5× total number of peripheral blood lymphocytes (×109/ L). PNI≥50 was defined as normal nutritional status, 45 ≤PNI < 50 as mild malnutrition, 40 ≤PNI < 45 as moderate malnutrition, and PNI < 40 as severe malnutrition.
Multidimensional Fatigue Inventory (MFI)
The MFI scale was developed by Han Qiufeng et al.11 It includes 5 dimensions: general fatigue (4 items), physical fatigue (4 items), mental fatigue (4 items), weakened motivation (4 items), and reduced activity (4 items). Each item is scored from “strongly disagree” to “strongly agree” on a scale of 1 to 5 points. The total score of the scale ranges from 20 to 100, and the higher the score, the higher the degree of fatigue. The original scale has good reliability and validity. In this study, the Cronbach’s α coefficients of the scale measured three times were 0.802, 0.850, and 0.833.
Generalized Anxiety Disorder (GAD - 7)
The scale was translated into Chinese by He Xiaoyuan et al.12 The scale consists of 7 symptom items, and each item is scored from 0 to 3 points, ranging from “not at all” to “almost every day”. The total score ranges from 0 to 21 points, and the higher the score, the higher the level of anxiety. In this study, the Cronbach’s α coefficients of the scale measured three times were 0.814, 0.798, and 0.825.
The State Difficulties in Emotion Regulation Scale (S - DERS)
The scale was prepared by Gratz,13 localized by Liu Qiqin,14 and its validation was completed. It includes four dimensions, namely acceptance (5 items), resolution (2 items), reason adjustment (3 items), and reaction adjustment (5 items), with a total of 15 items. From “completely does not conform to” to “completely in line with”, scores are assigned from 1 to 5 points respectively, with a total score ranging from 15 to 75 points. The higher the score, the greater the difficulty of individual emotion regulation. The reliability and validity of the original scale are good. In this study, the Cronbach’s α coefficients of the scale measured three times were 0.826, 0.844, and 0.801.
Questionnaire Recovery and Quality Control
After obtaining the consent of hospitals and lung cancer patients themselves, the researchers conducted a questionnaire survey. The basic information questionnaire of this study was collected upon the admission of lung cancer patients. The time nodes for the prognostic nutritional index and psychosomatic symptom cluster questionnaires were selected as follows: The research team members calculated the prognostic nutritional index at postoperative (T1), 1 - month (T2), 3 - month (T3), and T1 - T3 time points from the patients’ blood reports during the postoperative follow - up. The researchers distributed the psychosomatic symptom cluster questionnaires (each scale) to the patients during the follow - up and asked the patients to complete the questionnaires independently. The privacy of lung cancer patients was not affected. One trained researcher in the research group collected the scores of the prognostic nutritional index and psychosomatic symptom cluster (each scale) and entered them into Excel, and another researcher checked the data to ensure the accuracy of data entry. The lung cancer patients who participated in this study were sent certain random red envelopes via WeChat to ensure their enthusiasm for participation.
Statistical Methods
SPSS 26.0 and Mplus 8.0 software were employed for statistical analysis. Count data and measurement data were respectively presented as the number of cases/percentage and mean ± standard deviation. Pearson correlation analysis was utilized to examine the correlation. A cross - lag model was constructed to analyze the bidirectional relationship between the prognostic nutritional index and psychosomatic symptom clusters at the three time points, and the Maximum Likelihood Robust Estimator (MLR) was applied to evaluate the model.
Results
Basic Information
A total of 185 questionnaires were distributed, and 7 invalid questionnaires were excluded, resulting in an effective recovery rate of 96.22%. The patient information is shown in Table 1.
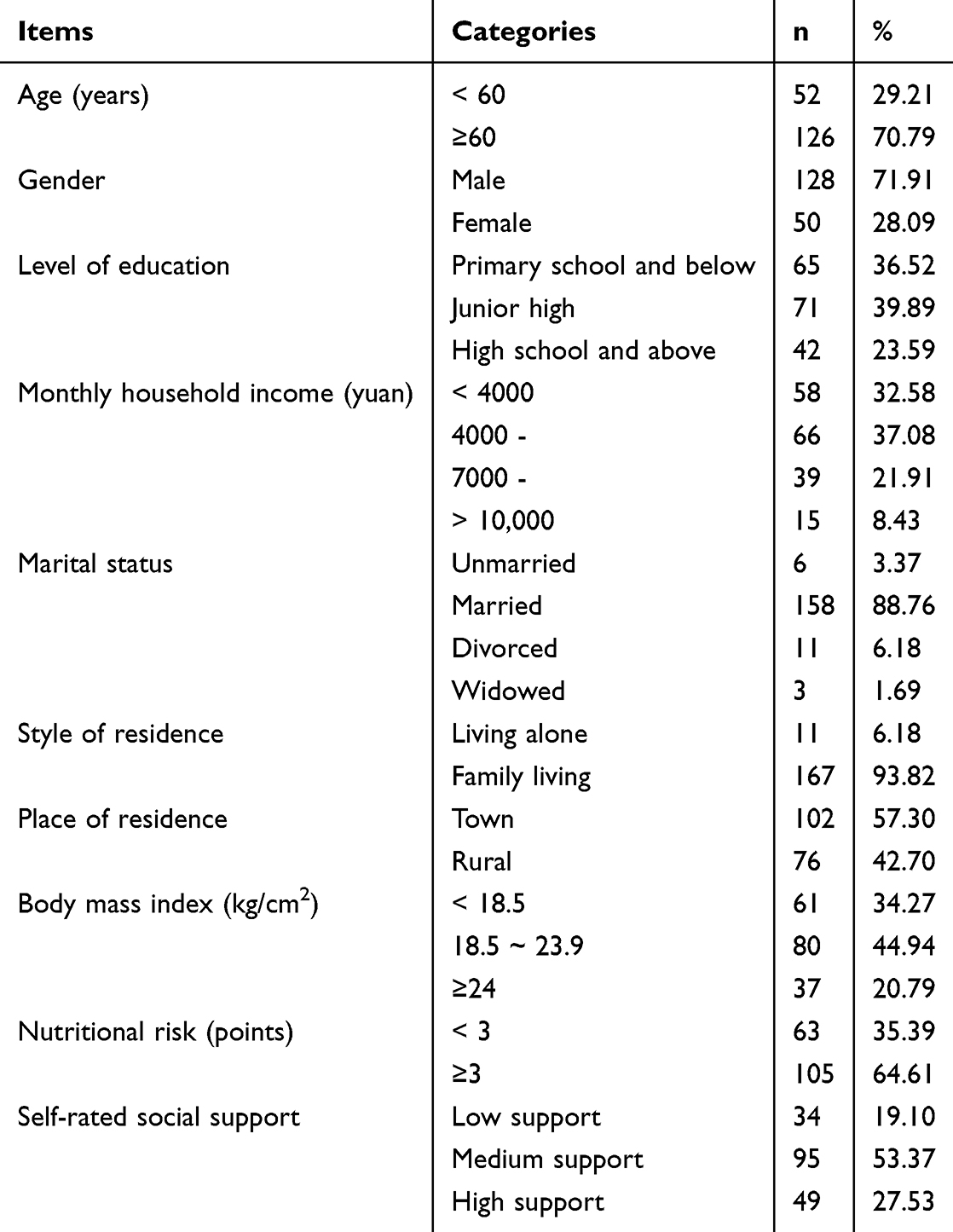 |
Table 1 General Information of the Respondents (n=178) |
Common Method Bias Test
The common method deviation test was conducted on the three sets of data using the Harman single - factor test. The variances of the three measurements were 16.62%, 19.67%, and 23.24% respectively, all of which were less than the 40% critical value level.15
Comparison of the Nutritional Index and Psychosomatic Symptom Scores of Lung Cancer Patients at Three Time - Points in Terms of Prognosis
By measuring the prognostic nutritional index and psychosomatic symptom clusters of lung cancer patients, the repeated - measurement results showed that: The scores of the prognostic nutritional index (F = 3.342, P = 0.031), multidimensional fatigue (F = 5.362, P < 0.001), generalized anxiety (F = 6.003, P < 0.001), and emotional regulation difficulties (F = 0.885, P = 0.420) at the three time points are shown in Table 2.
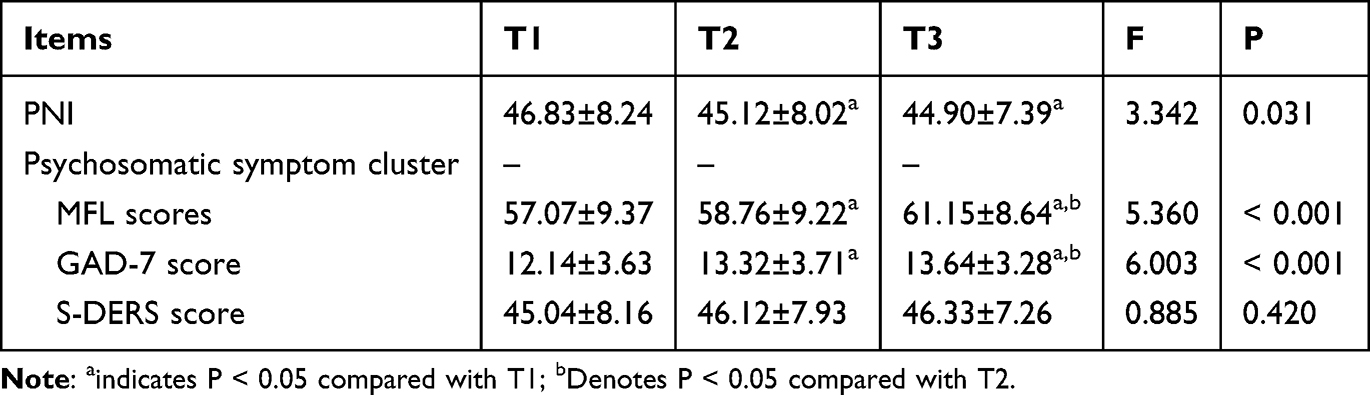 |
Table 2 Prognostic Nutritional Index and Scores of Psychosomatic Symptom Cluster in Lung Cancer Patients at Three Time Points (n=178) |
Correlation Analysis of Prognostic Nutritional Index and Psychosomatic Symptom Cluster Scores at Three Time Points in Patients with Lung Cancer
Pearson correlation analysis was employed to analyze the prognostic nutritional index and psychosomatic symptom cluster at three time points. The results indicated that there was a significant correlation between the two at the three time nodes (P < 0.05), which met the prerequisite of the cross - lag model. The matrix relationship is presented in Table 3.
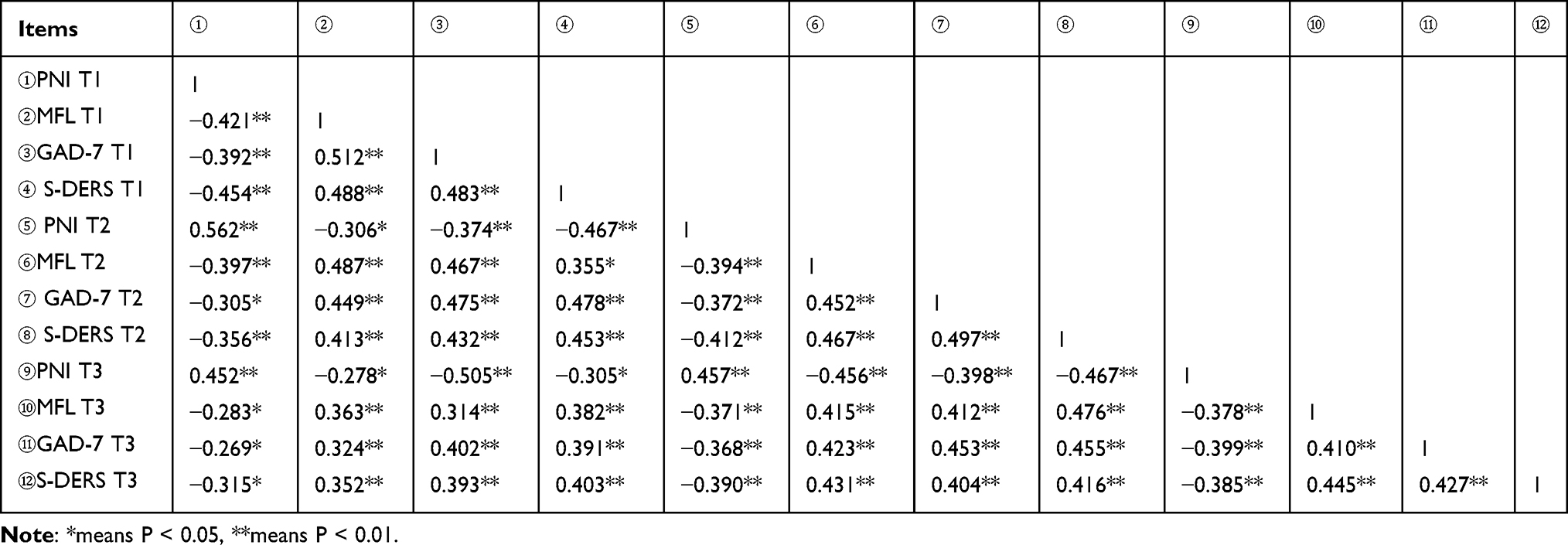 |
Table 3 Prognostic Nutritional Index and Psychosomatic Symptom Cluster Scores and Correlation Coefficient Matrix of Lung Cancer Patients at Three Time Points (r Value, n=178) |
Cross - Lag Model of Prognostic Nutritional Index and Psychosomatic Symptom Cluster in Patients with Lung Cancer
The relationship between the Prognostic Nutritional Index (PNI) and psychosomatic symptom clusters was determined by constructing and comparing a series of nested cross-lagged panel models. Initially, a baseline model (M1) confirmed the variables’ significant temporal stability. Subsequently, unidirectional predictive models were tested—one (M2) examining the effect of PNI on subsequent symptom clusters, and a reverse model (M3) examining the effect of symptom clusters on subsequent PNI. Finally, a fully saturated bidirectional cross-lagged model (M4) was evaluated. In comparison to the restricted nested models (M1, M2, M3), the bidirectional M4 model not only demonstrated excellent absolute model fit indices (CFI > 0.98, RMSEA < 0.05) but also showed a statistically significant improvement in model fit (Δχ2 = 141.253, P < 0.001). Furthermore, all the cross-lagged path coefficients within the M4 model were statistically significant. Consequently, there is robust statistical evidence to support that the bidirectional M4 model best represents the true underlying dynamic relationship between the variables, indicating a reciprocal and mutually reinforcing causal influence between the Prognostic Nutritional Index and psychosomatic symptom clusters, see Table 4 for details.
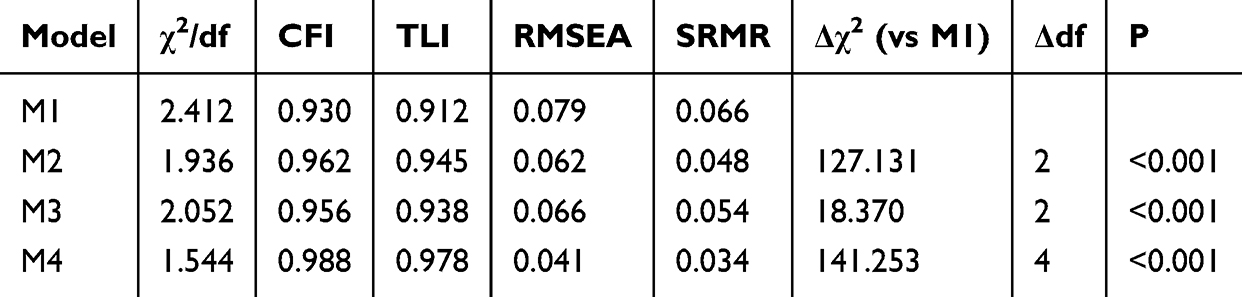 |
Table 4 Comparison of Model Fitting |
As shown in Figure 1, the level of the prognostic nutritional index on average negatively predicted multidimensional fatigue at the next node (T1→T2: β = - 0.415, P = 0.003; T2→T3: β = - 0.433, P = 0.005). Also, the level of the prognostic nutritional index negatively predicted generalized anxiety at the next node (T1→T2: β = - 0.364, P = 0.007; T2→T3: β = - 0.350, P = 0.012). The level of the prognostic nutritional index at T2 negatively predicted the symptoms of emotional regulation difficulties at T3 (T1→T2: β = - 0.158, P = 0.151; T2→T3: β = - 0.233, P = 0.024).
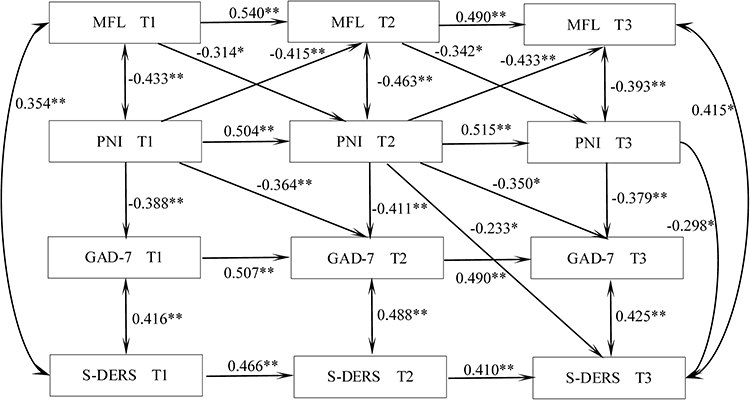 |
Figure 1 The predictive pathways of prognostic nutritional indices and psychosomatic symptom clusters in lung cancer patients at three time points. Note: ** denotes P < 0.01, * denotes P < 0.05; Only statistically significant paths are identified in the figure. |
Meanwhile, only multidimensional fatigue in the psychosomatic symptom cluster negatively predicted the prognostic nutritional index at the next node (T1→T2: β = - 0.314, P = 0.003; T2→T3: β = - 0.342, P = 0.001). The specific path is shown in Figure 1.
Discussion
Changes of Nutritional Index and Psychosomatic Symptom Clusters in Postoperative Patients with Lung Cancer
The prognostic nutritional index of postoperative patients with lung cancer shows a downward trend, while the psychosomatic symptom clusters (scores of multidimensional fatigue, generalized anxiety) show an upward trend. The decline of the prognostic nutritional index and the aggravation of the psychosomatic symptom cluster are the results of the joint action of multiple factors.
At the physiological level, surgical trauma directly leads to metabolic disorders and impaired digestion and absorption functions. Moreover, postoperative pain and the side - effects of chemotherapy further inhibit appetite, resulting in insufficient nutritional intake.16,17 Meanwhile, the hypermetabolic state of the tumor itself and the postoperative inflammatory response continuously consume the body’s energy reserves, accelerate muscle breakdown, and lead to the deterioration of nutritional indicators.18
In terms of psychosocial factors, patients’ fear of cancer recurrence, the uncertainty of treatment side - effects, and the stress caused by social role changes all induce generalized anxiety. Long - term pain can weaken their emotional regulation ability, causing patients to fall into a negative emotional cycle.19 Fatigue results from the superposition effect of surgical stress response, anemia, sleep disorders, depression, and anxiety, leading to the mutual deterioration of the physical and psychological states.20
In addition, treatment - related adverse reactions such as taste changes and dysphagia aggravate malnutrition, which in turn further exacerbates fatigue by affecting neurotransmitter synthesis and immune function.21 This vicious cycle between nutritional status and psychosomatic symptoms can significantly reduce the quality of life of patients and even affect the effectiveness of anti - tumor treatment. Therefore, early nutritional intervention combined with psychological support is needed.
The Relationship Between Postoperative Prognostic Nutritional Index and Psychosomatic Symptom Clusters in Patients with Lung Cancer
By constructing a cross - lag model, it was found that the level of the prognostic nutritional index negatively predicted multidimensional fatigue symptoms at the next time point on average (T1→T2: β = - 0.415, P = 0.003; T2→T3: β = - 0.433, P = 0.005). Moreover, the level of the prognostic nutritional index negatively predicted generalized anxiety symptoms at the next time point (T1→T2: β = - 0.364, P = 0.007; T2→T3: β = - 0.350, P = 0.012). The level of the prognostic nutritional index at T2 negatively predicted the symptoms of emotional regulation difficulties at T3 (T1→T2: β = - 0.158, P = 0.151; T2→T3: β = - 0.233, P = 0.024).
The prognostic nutritional index negatively predicted multidimensional fatigue and generalized anxiety from T1 to T2 and from T2 to T3, indicating that the deterioration of nutritional and immune status was an independent risk factor for the aggravation of symptoms. Postoperative chemotherapy drugs inhibit bone marrow hematopoietic function, resulting in lymphopenia and a decrease in serum albumin. This leads to an increase in inflammatory factors and neuroendocrine disorders, which aggravate fatigue and anxiety.22 A persistently low Prognostic Nutritional Index (PNI), indicative of a state of chronic immunosuppression and systemic inflammation, leads to elevated levels of various pro - inflammatory cytokines, including interleukin - 1β (IL - 1β), interleukin - 6 (IL - 6), and tumor necrosis factor - α (TNF - α). These circulating pro - inflammatory mediators can influence the central nervous system through several mechanisms. On one hand, they can act directly on the endothelial cells of the blood - brain barrier (BBB). For example, by activating signaling pathways such as the caspase - 11/GSDMD pathway, they can induce pore formation in endothelial cells, thereby increasing BBB permeability and allowing macromolecules normally restricted to the periphery to enter the brain parenchyma more readily. On the other hand, these cytokines can bind to specific receptors on the BBB, triggering local inflammatory signaling that indirectly affects brain function. Once within the CNS, these pro - inflammatory mediators disrupt neurotransmitter balance, for example, by inhibiting the synthesis of serotonin. They can also activate microglia, initiating neuroinflammation which may lead to excessive phagocytosis of neuronal synapses. This process impairs neural circuit function and neuroplasticity, further diminishing the emotional regulatory capacity of key brain regions such as the prefrontal cortex and hippocampus. Consequently, this cascade amplifies the patient’s experience of negative emotions and significantly exacerbates difficulties in emotional regulation.23
In the psychosomatic symptom cluster, only the multidimensional fatigue symptom negatively predicted the prognostic nutritional index at the next time point (T1→T2: β = - 0.314, P = 0.003; T2→T3: β = - 0.342, P = 0.001), while generalized anxiety and difficulty in emotional regulation showed no similar effect, reflecting the heterogeneous effect of symptom clusters. Fatigue is highly correlated with inflammatory markers, which can directly inhibit albumin synthesis.
In the early postoperative period (T1→T2), fatigue indirectly affects appetite mainly through psychological stress. At this time, the levels of inflammatory factors have not increased significantly, albumin synthesis and lymphocyte regeneration can be maintained, and the prognostic nutritional index has not decreased significantly.24 With the progress of postoperative chemotherapy (T2→T3), fatigue continues to lead to a sharp reduction in activity and insufficient intake, as well as the accumulation of inflammatory factors. This reduces albumin synthesis and accelerates muscle breakdown, and the prognostic nutritional index decreases significantly.25
This suggests that clinical medical staff should give priority to fatigue intervention, such as nutritional support and anti - inflammatory treatment. At the same time, emotional management should be strengthened during chemotherapy to delay the cumulative damage of emotional problems to the physiological state.
Deficiencies and Prospects
In this study, 185 lung cancer patients were dynamically monitored via a longitudinal tracking design, and the evolution of the prognostic nutritional index and psychosomatic symptom cluster was systematically analyzed. The results indicated that there was a significant time - series correlation between nutritional status and symptom clusters, which provided an empirical basis for the clinical dynamic monitoring of patients’ nutritional and symptom changes. However, this study has the following methodological limitations: the sample was restricted to a single center, which might affect the external validity of the results; the observation period was short, covering only three postoperative time points; and the sample size was relatively small, which could reduce the statistical test power. Furthermore, this study does not adequately account for potential confounding variables—such as CRP or other inflammatory markers, comorbidities, specific chemotherapy regimens, or supportive care measures—all of which may influence both nutritional status and psychological outcomes. Future research plans include extending the follow - up period, expanding the multi - center sample size, and systematically collecting data on these confounders to enable a deeper investigation into the dynamic interplay between the prognostic nutritional index and symptom clusters.
Conclusion
The prognostic nutritional index of postoperative lung cancer patients is closely associated with the psychosomatic symptom cluster. The prognostic nutritional index has a negative predictive effect on the psychosomatic symptom cluster, and the multidimensional fatigue symptom has a negative predictive effect on the prognostic nutritional index.
This study offers significant insights for clinical practice. It is essential to systematically monitor the Prognostic Nutritional Index (PNI) and multidimensional fatigue symptoms as a core component of routine care starting from the perioperative period and the initial phase of chemotherapy. When a decline in PNI or an exacerbation of fatigue is detected, healthcare professionals should prioritize initiating targeted nutritional support and anti-fatigue interventions. This may include increasing the intake of high-quality protein in the diet and considering anti-inflammatory adjunctive therapies under medical guidance to break the vicious cycle of deteriorating nutrition and worsening fatigue.
Management of anxiety symptoms should be integrated throughout the entire treatment cycle. Particularly after time point T2, when a low PNI level indicates an increased risk of emotional regulation difficulties, non-pharmacological interventions should be intensified. Patients can be taught techniques such as deep breathing exercises and mindfulness meditation to alleviate physical tension, and encouraged to engage in regular aerobic exercise to promote endorphin secretion and thereby improve mood state.
Concurrently, dietary education for both patients and their families is crucial. It is advisable to increase the consumption of foods rich in omega-3 fatty acids and B vitamins, as these nutrients play a positive role in maintaining nervous system stability and have anti-inflammatory properties, thereby helping to improve emotional regulation capacity at a physiological level. This comprehensive strategy, which prioritizes nutrition and fatigue as key intervention targets while simultaneously integrating emotional management, can effectively delay the cumulative physiological damage caused by psychosomatic symptoms, ultimately leading to an improved overall clinical outcome for patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Luo Y, Mao D, Zhang L, et al. Identification of symptom clusters and sentinel symptoms during the first cycle of chemotherapy in patients with lung cancer. Support Care Cancer. 2021;32(6):385.
3. American Lung Association. State of lung cancer 2024 report. Available from: https://www.lung.org/research/state-of-lung-cancer.
4. Ma C, Yu R, Li J, et al. Preoperative prognostic nutritional index and systemic immune-inflammation index predict survival outcomes in osteosarcoma: a comparison between young and elderly patients. J Surg Oncol. 2021;125(4):754–765. doi:10.1002/jso.26757
5. Ju X, Bai J, She Y, et al. Symptom cluster trajectories and sentinel symptoms during the first cycle of chemotherapy in patients with lung cancer. Eur J Oncol Nurs. 2023;63:102282. doi:10.1016/j.ejon.2023.102282
6. He X, Ng M, Choi KC, et al. Effects of a 16-week dance intervention on the symptom cluster of fatigue-sleep disturbance-depression and quality of life among patients with breast cancer undergoing adjuvant chemotherapy: a randomized controlled trial. Int J Nurs Stud. 2021;133:104317. doi:10.1016/j.ijnurstu.2022.104317
7. Fox RS, Ancoli-Israel S, Roesch SC, et al. Sleep disturbance and cancer-related fatigue symptom cluster in breast cancer patients undergoing chemotherapy. Support Care Cancer. 2020;28(2):845–855. doi:10.1007/s00520-019-04834-w
8. Mokshagundam S, McGree ME, Tapia AL, et al. Physical and psychological distress amongst patients undergoing neoadjuvant chemotherapy for advanced ovarian cancer. Gynecol Oncol. 2024;190:230–235. doi:10.1016/j.ygyno.2024.08.024
9. Oncology Branch of Chinese Medical Association. Chinese Medical Association Journal. Chinese Medical Association Oncology Society clinical diagnosis and treatment guidelines for lung cancer (2021 edition). Chin J Med. 2021;101(23):1725–1757. (in Chinese with English abstract).
10. Li X, Liu GF, He DD, et al. Estimation of sample size in repeated measurement design. China Health Statistics. 2001;18(4):204–206.
11. Han Q, Tian J. Reliability and validity of multidimensional fatigue scale in cancer patients. Chin J Nurs. 2012;47(6):548–550.
12. He X, Li C, Qian J, et al. The reliability and validity of the general anxiety scale in general hospitals. Shanghai Psychiatry. 2010;22(4):200–203.
13. Gratz KL. Targeting emotion dysregulation in the treatment of self-injury. J Clin Psychol. 2007;63(11):1091–1103. doi:10.1002/jclp.20417
14. Liu Q, Wu H, Liu M. The revision and reliability and validity test of the difficulty scale of emotion regulation state. Chinese School Health. 2017;38(10):1571–1574.
15. Dandan T, Wen Z-L. Common Method bias testing: problems and suggestions. Psychol Sci. 2020;43(01):215–223.
16. Ding P, Guo H, Sun C, et al. Combined systemic immune-inflammatory index (SII) and prognostic nutritional index (PNI) predicts chemotherapy response and prognosis in locally advanced gastric cancer patients receiving neoadjuvant chemotherapy with PD-1 antibody sintilimab and XELOX: a prospective study. BMC Gastroenterol. 2021;22(1):121.
17. Salati M, Filippi R, Vivaldi C, et al. The prognostic nutritional index predicts survival and response to first-line chemotherapy in advanced biliary cancer. Liver Int. 2020;40(3):704–711. doi:10.1111/liv.14314
18. Zhang Q, Bao J, Zhu ZY, et al. Prognostic nutritional index as a prognostic factor in lung cancer patients receiving chemotherapy. Eur Rev Med Pharmacol Sci. 2021;25(18):5636–5652. (in Chinese). doi:10.26355/eurrev_202109_26783
19. Liu W, Liu J, Ma L, et al. Effect of mindfulness yoga on anxiety and depression in early breast cancer patients received adjuvant chemotherapy: a randomized clinical trial. J Cancer Res Clin Oncol. 2021;148(9):2549–2560. doi:10.1007/s00432-022-04167-y
20. Medeiros TD, Jorge KR, Da SSS. Impact on fatigue of different types of physical exercise during adjuvant chemotherapy and radiotherapy in breast cancer: systematic review and meta-analysis. Support Care Cancer. 2021;30(6):4651–4662.
21. Herranz-Gomez A, Cuenca-Martinez F, Suso-Marti L, et al. Effectiveness of therapeutic exercise models on cancer-related fatigue in patients with cancer undergoing chemotherapy: a systematic review and network meta-analysis. Arch Phys Med Rehabil. 2023;104(8):1331–1342. doi:10.1016/j.apmr.2023.01.008
22. Zhang H, Meng Y, Jiang R, et al. Effect of multimodal exercise on cancer-related fatigue in patients undergoing simultaneous radiotherapy and chemotherapy: a randomized trial in patients with breast cancer. Altern Ther Health Med. 2023;29(5):233–237.
23. Guo YQ, Ju QM, You M, et al. Depression, anxiety and stress among metastatic breast cancer patients on chemotherapy in China. BMC Nurs. 2023;22(1):33. doi:10.1186/s12912-023-01184-1
24. Fan R, Chen Y, Xu G, et al. Combined systemic immune-inflammatory index and prognostic nutritional index predict outcomes in advanced non-small cell lung cancer patients receiving platinum-doublet chemotherapy. Front Oncol. 2023;13:996312. doi:10.3389/fonc.2023.996312
25. Wang B, Zhang J, Shi Y, et al. Clinical significance of the combined systemic immune-inflammatory index and prognostic nutritional index in predicting the prognosis of patients with extensive-stage small-cell lung cancer receiving immune-combination chemotherapy. BMC Cancer. 2024;24(1):1574. doi:10.1186/s12885-024-13343-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.