Back to Journals » Advances in Medical Education and Practice » Volume 16
Creating Safe Connections: A Co-Designed E-Learning Module to Advance Equity and Social Accountability in Preventative Primary Care
Authors Sayani A, Ladak Z ![]() , Manthorne J, Nicholson E, Bloch GC, Parsons J, Hwang SW, Amenu B, Freedman H, Jeji T, Pratt A
, Manthorne J, Nicholson E, Bloch GC, Parsons J, Hwang SW, Amenu B, Freedman H, Jeji T, Pratt A ![]() , Ramasamy V, Camus JC, Wathen CN, MacGregor JCD
, Ramasamy V, Camus JC, Wathen CN, MacGregor JCD ![]() , Dilkes D, Lofters A
, Dilkes D, Lofters A
Received 6 June 2025
Accepted for publication 9 October 2025
Published 25 October 2025 Volume 2025:16 Pages 1967—1979
DOI https://doi.org/10.2147/AMEP.S539091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Ambreen Sayani,1,2 Zeenat Ladak,1,3 Jackie Manthorne,4 Erika Nicholson,5 Gary C Bloch,6,7 Janet Parsons,2 Stephen W Hwang,6 Bikila Amenu,8 Howard Freedman,8 Tara Jeji,8 Angus Pratt,8 Vinesha Ramasamy,8 Jean-Claude Camus,8 C Nadine Wathen,9 Jennifer CD MacGregor,9 Danielle Dilkes,10,11 Aisha Lofters1,12,13
1Women’s College Hospital Research & Innovation Institute, Women’s College Hospital, Toronto, Ontario, Canada; 2Institute of Health Policy, Management & Evaluation, University of Toronto, Toronto, Ontario, Canada; 3Applied Psychology & Human Development, University of Toronto, Toronto, Ontario, Canada; 4Board of Directors, Canadian Cancer Survivor Network, Ottawa, Ontario, Canada; 5Executive Team, Canadian Partnership Against Cancer, Toronto, Ontario, Canada; 6Family and Community Medicine, St. Michael’s Hospital, Toronto, Ontario, Canada; 7Board of Directors, Inner City Health Associates & Health Providers Against Poverty, Toronto, Ontario, Canada; 8Patient Partner, Women’s College Hospital, Toronto, Ontario, Canada; 9Arthur Labatt Family School of Nursing, University of Western Ontario, London, Ontario, Canada; 10Centre for Teaching & Learning, University of Western Ontario, London, Ontario, Canada; 11Curriculum, Teaching, & Learning, University of Toronto, Toronto, Ontario, Canada; 12Department of Family & Community Medicine, University of Toronto, Toronto, Ontario, Canada; 13Peter Gilgan Centre for Women’s Cancers, Women’s College Hospital, Toronto, Ontario, Canada
Correspondence: Ambreen Sayani, Women’s College Hospital Research & Innovation Institute, Women’s College Hospital, 76 Grenville St, Toronto, Ontario, M5S 1B2, Canada, Tel +1 416 323 6400 ext 3772, Email [email protected]
Purpose: Lung cancer is the leading cause of cancer-related deaths worldwide and in Canada. Primary care providers (PCPs) play a vital role in incorporating lung cancer prevention and early detection into routine practice. This study outlines the co-design of Creating Safe Connections, an e-learning module developed to build PCPs’ capacity to deliver equity-oriented preventative care.
Methods: This manuscript describes the pre-design and co-design phases of the innovation process, guided by the Generative Co-Design Framework for Healthcare Innovation. The pre-design phase established a governance structure comprising patient partners with lived/living experience and interest-holders including PCPs. During the co-design phase, key module priorities and research goals were identified, including barriers to access, stigma and trauma, and operationalizing equity-oriented care. All aspects of the module—its name, logo, content, and knowledge mobilization strategies—were co-developed with the patient partners and health system partners. To inform the e-learning module content, interviews were conducted with community-based PCPs in Ontario, Canada to explore how they apply equity-oriented skills in practice. Interviews were analyzed using deductive content analysis.
Results: PCPs’ (five family physicians, two nurse practitioners) interview analysis was informed by the four pillars of Trauma- and Violence-Informed Care: recognizing the impact of trauma and violence; creating emotionally, culturally, and physically safe environments; promoting choice, collaboration, and connection; and adopting a strengths-based, capacity-building approach. These themes shaped the co-design of a Continuing Medical Education-accredited module, which includes video narratives, case studies, a learner’s notebook, and interactive assessments.
Conclusion: This work offers a model for the participatory co-design of equity-focused educational interventions that bridge gaps in provider training while aligning with the care needs and priorities identified by structurally underserved populations. The module uses lung cancer screening as a case example to illustrate approaches to addressing inequities in preventative care.
Keywords: patient-partnered, accessibility, asynchronous learning, patient-centered care, lung cancer screening, smoking cessation, trauma- and violence-informed care, co-design, lived experience expertise
Introduction
Preventative primary care is foundational to improving population health. It enables identification and management of modifiable risk factors, facilitates early disease detection, and supports timely interventions that help reduce illness and death.1 As the first point of health system contact for many individuals, primary care providers (PCPs), including family physicians, nurse practitioners, and physician assistants among others, are uniquely positioned to assess patient needs holistically, navigate complex health systems, and foster trust to encourage engagement in preventative health services.1,2
Lung cancer remains the leading cause of cancer-related deaths globally, with 1.8 million deaths and an estimated 2.2 million new cases occurring world-wide in 2020,3 and in Canada, accounting for a quarter of all cancer-related mortality.4,5 Most cases are diagnosed at an advanced stage (III or IV), when survival rates are poor.5 Early detection through low-dose computed tomography screening has been shown to reduce lung cancer mortality by identifying the disease at a more treatable stage.5,6 Lung cancer screening (LCS) must be centered in health equity.7 As reported by the Canadian Partnership Against Cancer, it is 77% more likely for people living in remote or rural areas in Canada, or with lower income, to smoke, and they are 1.2 to 1.8 times more likely to be diagnosed with lung cancer, respectively.7 When bundled with smoking cessation and harm reduction efforts, LCS is an effective preventative care strategy to reduce lung cancer incidence and improve health outcomes.5
Primary care serves as a critical interface for integrating lung cancer prevention and early detection into routine care. PCPs are well-positioned to identify individuals at high risk for lung cancer, initiate discussions about screening eligibility, and provide tailored support for smoking cessation.4 In this capacity, PCPs can play a pivotal role in connecting patients to evidence-based interventions that reduce lung cancer-related morbidity and mortality.
In Canada, participation in LCS programs is determined by eligibility criteria based on age and smoking history (for example, in the province of Ontario, this includes people between the age of 55–74 years with a ≥20 pack-year smoking history).8 Given the availability of Universal Healthcare in Canada, it might be assumed that participation in LCS programs is largely determined by these eligibility criteria to identify individuals at high risk, they fail to account for the social and structural determinants of lung cancer risk including occupational exposures, systemic racism, financial security, and discrimination based on social location, which disproportionately affect marginalized populations.9 Similarly, smoking cessation services often focus narrowly on individual behavior change, overlooking the broader social drivers of tobacco use, such as trauma, poverty, and stigma.4,10 These limitations perpetuate inequities in access to and outcomes of lung cancer prevention, excluding those most in need of intervention.9,11
Equity-Oriented Health Care (EOHC) provides a comprehensive framework to address social inequities in healthcare delivery by integrating principles of Trauma- and Violence-Informed Care (TVIC), cultural safety, and substance use health/harm reduction.12,13 These approaches aim to reduce power imbalances, challenge systemic discrimination, and create safer, more inclusive care environments, while keeping with principles of social accountability. TVIC focuses on recognizing and responding to the impacts of trauma and violence on health and healthcare experiences, while cultural safety emphasizes addressing systemic racism and fostering environments where patients feel respected and empowered.12 Harm reduction strategies enacted within the context of substance use health support individuals by removing barriers to care and prioritizing their goals of well-being without judgment or stigma.14 Despite its transformative potential, the integration of EOHC into primary care remains inconsistent, as many PCPs lack access to practical tools and training to operationalize these principles.12 Focused training can fill the gap between PCPs’ understanding of structural risks and trauma-informed approaches to care ultimately improving access to care conversations.1 Co-design, a participatory approach that centers collaboration between providers, patients, and system actors, is increasingly used to ensure interventions are grounded in lived experience.15 Without support to learn and adopt EOHC strategies, PCPs may inadvertently perpetuate inequities, particularly for patients navigating barriers such as systemic racism, prior and ongoing impacts of trauma, and poverty.4 Addressing this gap requires educational tools that are actionable, co-designed with patients to be inclusive of their perspectives, grounded in real-world clinical scenarios, and designed to equip PCPs with the skills needed to embed EOHC principles into routine practice.13 This work sought to address this gap by creating an e-learning module as a strategy to integrate EOHC principles into lung cancer care.16
By centering the voices of patients with lived/living experience of structural inequities, co-design helps to ensure that educational tools are not only practical and actionable but also directly reflective of the challenges faced by underserved populations.15 This collaborative approach bridges the disconnect between provider training and the real-world needs of structurally marginalized communities, fostering educational content that is relevant and impactful, and offers a promising pathway for addressing the gap in integrating EOHC principles into routine primary care.13,15
In this manuscript, we describe the pre-design and co-design phases of an educational intervention called Creating Safe Connections, developed to equip PCPs with the knowledge and skills to deliver equity-oriented preventative care. The module uses LCS and smoking cessation as illustrative examples of how to address inequities in preventative care. Though applicable to other preventative care contexts (eg, cervical cancer screening) LCS is used in this module as a practical context to demonstrate equity-oriented approaches in primary care. We aim to provide a model for equity-focused educational interventions, informed by lived-experiences, that strives to enhance social accountability in preventative primary care practices to better meet the needs of structurally underserved populations.
Methods
This study applied the Generative Co-Design Framework for Healthcare Innovation to guide the co-development of the Creating Safe Connections e-learning module. This framework involves three phases—pre-design, co-design, and post-design—with six defined steps (Figure 1). This manuscript focuses on the Pre-design and Co-design phases, specifically detailing the first four steps of the framework. Details from the post-design phase are described elsewhere (forthcoming). To ensure comprehensive reporting of patient involvement within this work, we followed the Guidance for Reporting Involvement of Patients and the Public version 2 (GRIPP2) reporting guidelines.17
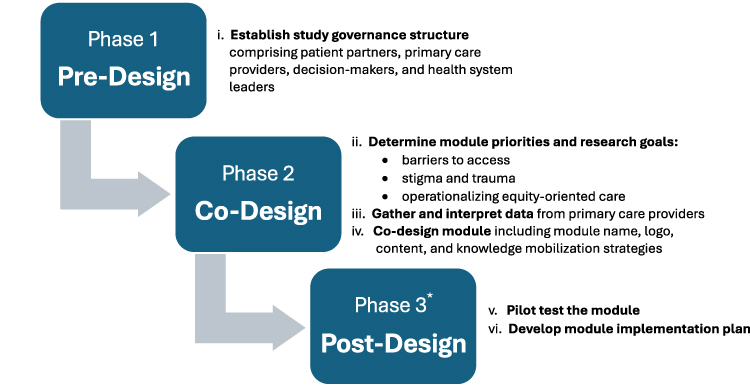 |
Figure 1 Generative Co-Design Framework for Healthcare Innovation to guide the co-development of the Creating Safe Connections e-learning module. *Phase 3: Post-Design is described elsewhere (forthcoming). |
Pre-Design
The Pre-design phase of the Generative Co-Design Framework focuses on establishing a governance structure to ensure that the research process is collaborative, inclusive, and grounded in equity-oriented principles (Figure 1). This phase lays the foundation for meaningful engagement among researchers, patient partners, and system interest-holders, enabling alignment with both community needs and healthcare priorities.18
The governance model described by Sayani et al in 202213 was designed to facilitate consensus-building among all partners through safe spaces for meaningful engagement. At the center of this structure is the principal investigator, who coordinates with all patient partners and interest-holders in separate yet aligned safe spaces to ensure consensus building across the research phases. Two key governance groups have been established which are collectively known as the Lung Health Equity Advisory Committee (LHEAC): the Research Advisory Council (RAC) and the Research Interest-Holder Council (RIC). Both councils were involved in pre-design and co-design, and continue to be engaged in ongoing implementation and evaluation of the e-learning module.
Research Advisory Council (RAC)
The RAC is comprised of patient partners with lived/living experiences of social inequities, including poverty, homelessness, and systemic discrimination. Patient partners were invited to join the RAC based on a longstanding, community-rooted relationship with the principal investigator, grounded in mutual trust and a shared commitment to improving equitable access to care, with a focus on LCS. Members meet monthly for one to two hours, virtually, with the duration and frequency of meetings determined by research needs through consensus. These meetings create a space for nurturing trust and fostering authentic dialogue for co-learning.13,18,19 To support equitable participation, meetings are held at times accessible to all members, and patient partners are compensated for their contributions ($30 CDN per hour) according to national Strategy for Patient-Oriented Research standards.20 Digital devices are provided as needed to facilitate virtual participation. Through this structure, patient partners shaped the design and strategy of the project, engaged in priority setting, and built capacity through partnerships and co-learning.
Research Interest-Holder Council (RIC)
The RIC consists of PCPs (eg, family physicians and nurses), policymakers involved in the design, delivery, accessibility and uptake of LCS at the Canadian provincial and federal levels (eg, Ontario Health, Canadian Partnership Against Cancer), and health system leaders with expertise in LCS and equity-oriented care (eg, Inner City Health Associates & Health Providers Against Poverty). RIC members were identified through the network of the principal investigator and through snowballing from the initial members. The RIC meets quarterly for one to two hours based on project needs. The RIC contributed practical insights to refine module priorities and research goals and ensure the module’s applicability in healthcare settings, and they continue to guide considerations around scalability and pan-Canadian implementation.
Every six months, as determined through consensus, the RAC and RIC collectively convene for facilitated virtual meetings to engage in collective dialogue, build relationships, revisit priorities, and make modifications to the study design based on emerging needs and findings. Meetings follow a workshop style and included the following engagement practices:
- Sharing meeting agendas, presentations, and prepared questions in advance to support discussion;
- Opening and closing circle activities as a restorative practice;21
- Round table discussions to gather all perspectives;
- Multimodal strategies to gather input for consensus building and decision-making (eg, emails, meetings, online surveys); and
- Sharing meeting minutes with all partners following meetings.
Following partner meetings, research team members debrief and practice reflexive journalling surrounding RIC and RAC discussions to ensure a written record of decisions and action items. In addition to meetings, one-on-one meetings are held with individual partners if more time for discussion and understanding is needed. This governance structure creates a foundation for equitable engagement, aligning system-level gaps with patient-identified priorities while fostering meaningful co-learning and collaboration. It sets the stage for the subsequent phases, where patient partners and interest-holders work together to shape the study’s direction and outcomes, following the same engagement practices as in the pre-design phase.
Co-Design
Identifying Module Priorities and Research Goals
The co-design process began with identifying key module priorities and research goals to guide the development of the Creating Safe Connections e-learning module. The RAC played a central role in this step, providing insights based on lived/living experiences of social inequities and highlighting areas where providers face challenges in addressing the needs of structurally underserved populations. These discussions shaped the initial focus on equity-oriented care in the contexts of LCS and smoking cessation.
Priority setting emphasized three overarching themes:
- Systemic Barriers to Access:
- Challenge: Structural factors, such as poverty, systemic racism and sexism, and stigma, significantly impact patients’ ability to engage in LCS and smoking cessation.
- Module Priority: Providers require support to better understand and address these barriers within their clinical practices.
- Stigma and Trauma in Patient-Provider Interactions:
- Challenge: Conversations about smoking cessation and lung cancer risk can unintentionally perpetuate stigma or activate past trauma.
- Module Priority: Training must focus on fostering safe, non-judgmental spaces where patients have agency to make informed decisions.
- Translating EOHC into Practice:
- Challenge: EOHC principles such as TVIC, cultural safety, and harm reduction are valuable but may be difficult to adopt into routine care
- Module Priority: Providers need actionable strategies to integrate these principles into routine care.
These themes were refined collaboratively with the RIC to align patient priorities with provider and broader system-level considerations, such as existing screening guidelines and the operational realities of primary care settings. The emphasis on these themes reflects the commitment to bridging the gap between provider training and the lived/living experiences of underserved populations, forming the foundation for the module’s development.
Gather and Interpret Data
To inform the development of the Creating Safe Connections e-learning module, semi-structured interviews were conducted with PCPs working in community-focused settings. The goal of these interviews was to explore PCPs’ perspectives on how they were applying equity-oriented care principles in practice, the structural inequities experienced by their patient populations, and barriers to LCS and smoking cessation. The interview guide is available in Appendix A.
Participant Recruitment
PCPs were recruited through the Alliance for Healthier Communities, a network of community health centers in Ontario, Canada. Recruitment focused on providers with prior experience or training in EOHC, such as those who had completed courses on cultural-safety and/or harm reduction. Eligible participants included physicians, nurse practitioners, nurses, dieticians, social workers, health promoters, and other allied health professionals actively involved in community-based primary care. PCPs working in these settings were selected as they were most likely to encounter and provide EOHC to patients facing systemic barriers, including racism, poverty, and housing instability. Recruitment was conducted through targeted newsletters and direct Email invitations, with reminders sent over a 2 to 4 week period. Each PCP received a $25 gift card compensation.
Data Collection
Semi-structured interviews were conducted virtually using Zoom or telephone, accommodating participants’ preferences and maintaining physical distancing requirements during the COVID-19 pandemic. Each interview lasted approximately 30 minutes and followed an interview guide co-developed with the RAC and RIC. Interview probes included:
- PCPs’ experiences with engaging patients eligible for LCS;
- Strategies for navigating sensitive conversations around smoking cessation;
- Perceived barriers to accessing care related to social inequities; and
- Recommendations for integrating EOHC principles, such as TVIC into routine practice.
Participants provided informed verbal consent before the interviews, which were audio-recorded and transcribed verbatim for analysis. Data was entered into NVivo 12 for qualitative data management.
Data Analysis
Interview data were analyzed using content analysis in NVivo 12, following an iterative and collaborative approach to enhance rigor and trustworthiness. Two members of the research team (AS and AL) read all transcripts and developed a preliminary inductive coding framework informed by the three module priorities. Inductive codes were then mapped deductively to the TVIC Core Competency Framework, which outlines key competencies for integrating TVIC into healthcare. These competencies emphasize understanding the impact of trauma, including structural and systemic as well as interpersonal violence, on behaviour, creating safe environments (with particular attention to the stigma and discrimination faced by some patients), fostering trust and collaboration, and promoting patient autonomy through a strengths-based and capacity development approach as essential components of equitable, TVIC.22
The final analysis was reviewed by both the RIC and RAC to enhance credibility and confirmability, reinforcing alignment between patient and provider experiences.
This collaborative and reflexive approach strengthened the qualitative analysis by ensuring that findings not only reflected provider perspectives but were also critically examined through the lens of those most affected by social inequities.
Ethics Statement
This study has been reviewed and approved by Women’s College Hospital’s Research Ethics Board (Protocol #2021-0003-E). The patient partner (HF) in Figure 2A provided written informed consent for their image to be published. Prior to the interviews, all participants received an informed consent sheet containing details of the study including dissemination processes of de-identified data such as publications of anonymized quotes. Interviews were conducted over Zoom or telephone, verbal consent was obtained and audio recorded by the interviewer prior to initiating the interviews, and informally throughout the interviews. These informed and verbal consenting processes were approved by Women’s College Hospital’s Research Ethics Board.
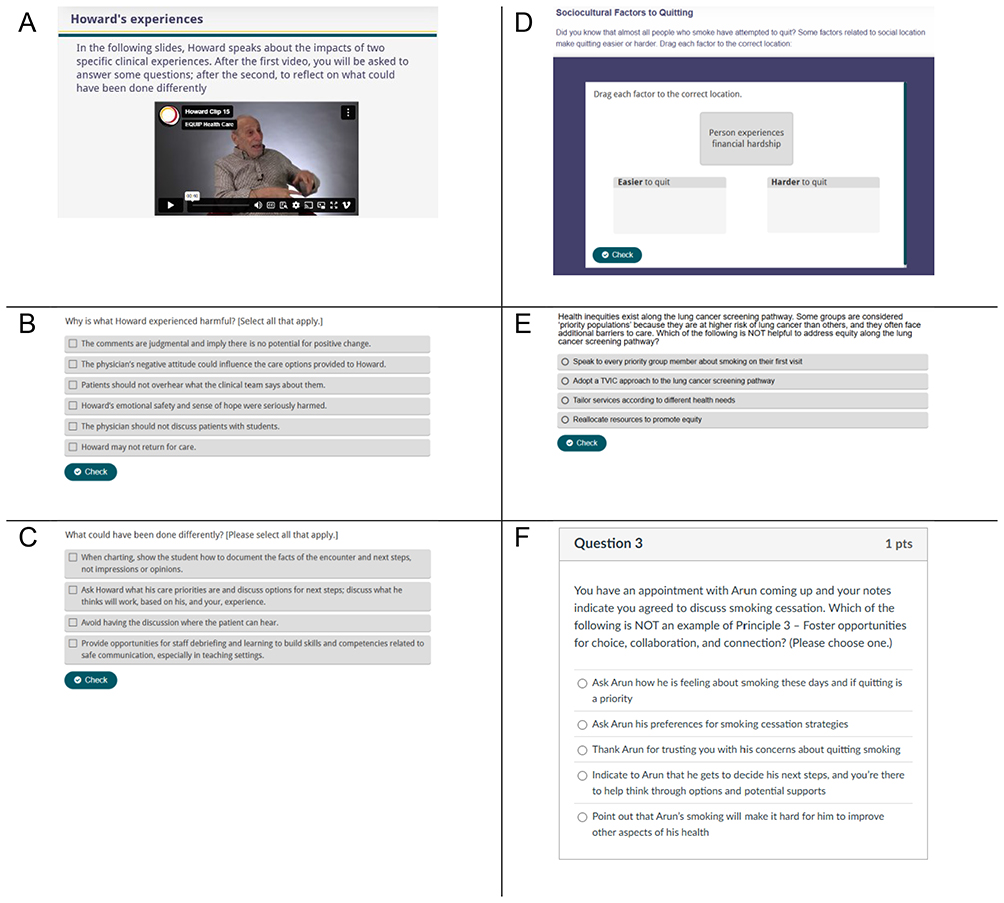 |
Figure 2 Direct examples of content from the Creating Safe Connections module. (A) Video excerpt of a patient partner, (B) Follow up case study question based on the experience of a patient partner, (C) Follow up reflection question, (D) Interactive pre-learning exercise: drag and drop, (E) Interactive post-learning exercise: multiple choice, (F) End-of-module assessment question: multiple choice. |
Results
Participant Characteristics
A total of seven PCPs were interviewed. This sample size was deemed sufficient based on the concept of information power which theorizes that the richer the information provided by a sample, the lower the required sample size. Within the context of this work, the participant sample was a narrowed scope of primary care, equity-oriented training, and harm reduction. The principles of information power state that sample adequacy depends on the relevance, depth, and quality of data in relation to the study’s aim.23
Table 1 describes the type of PCP and service setting for each participant, as reported during interviews. The majority of participants were family physicians (n=5), with two nurse practitioners. Three participants specifically identified working with people who are experiencing dehousing or have unstable housing, and/ or experiencing substance use, addictions, or harm reduction (eg, people who smoke).
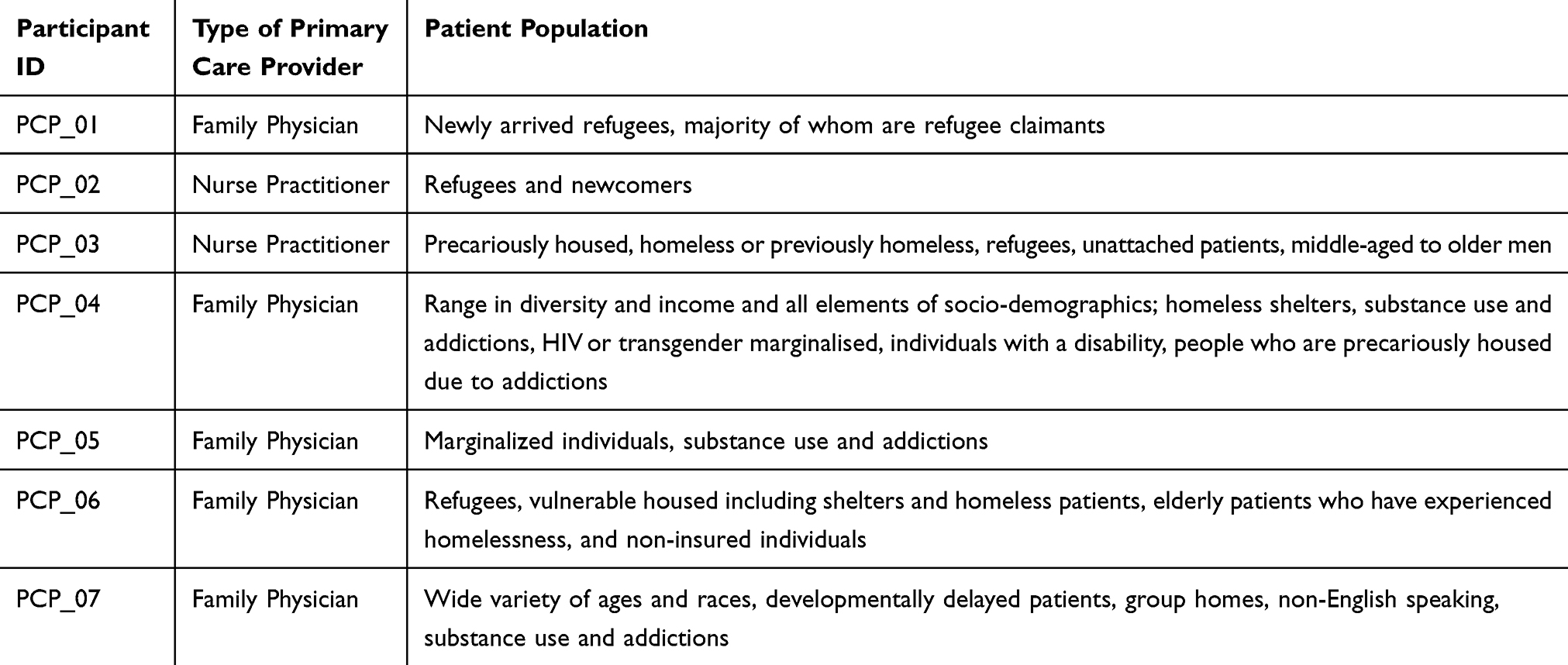 |
Table 1 Characteristics of Participants’ Practice Settings |
PCP Perspectives
Interview analysis was guided by identified module priorities and organized according to the four core themes of TVIC, with illustrative quotes presented in Table 2.
- Understand trauma, violence, and its impact on people’s lives and behaviour:22
- Organizations can develop policies and processes and train staff to understand the effects of violence and trauma, including structural, systemic and interpersonal violence and their traumatic effects.
- Providers can use a trauma lens to be mindful of potential patient histories and current life conditions by believing and validating experiences, recognizing strengths, and expressing concern.
- Create emotionally, culturally, and physically safe environments for all patients and providers:22
- Organizations can seek client input about safe and inclusive strategies and co-develop safety protocols.
- Providers can be aware of potential implicit biases, and inter-related forms of stigma and discrimination and how they operate to produce power differences. Providers should maintain safe professional boundaries, be compassionate, respectful and non-judgmental in their approach, and provide clear information, warm referrals and anticipatory guidance.
- Foster opportunities for choice, collaboration and connection:22
- Organizations can involve staff and clients in practice evaluation and develop policies and processes that allow for person-led decision making.
- Providers can actively listen, incorporate non-judgmental responses, provide realistic options for next steps, and consider choices collaboratively with clients based on their stated needs.
- Use strengths-based and capacity-building approach to support patients:22
- Organizations can allow sufficient time for meaningful engagement, tailor care options to peoples’ context, provide ongoing skill and knowledge building for staff.
- Providers can listen for, and validate patients’ strengths, acknowledge their historical context, and teach skills for calming and centering.
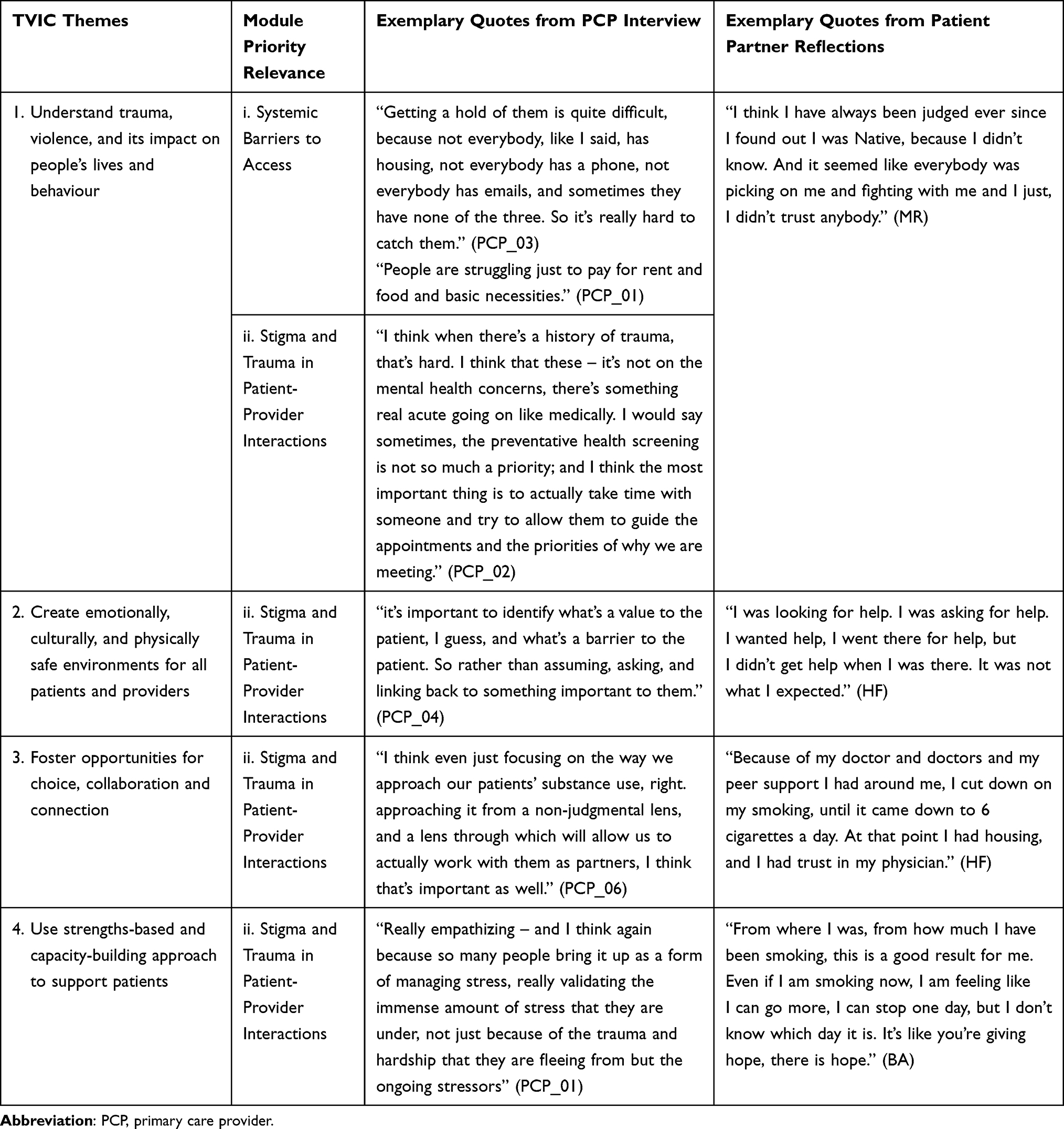 |
Table 2 Module Priorities Mapped to TVIC Themes Showcased by Exemplary Quotes from PCPs and Patient Partners |
Module priority three, translating EOHC into practice, was not mapped to any TVIC theme. Within this priority, PCPs expressed a need for practical tools and strategies to integrate TVIC and culturally safer approaches into routine care, particularly in addressing sensitive health behaviors.
“Having opportunities to learn about trauma‑informed care and thinking about how that can be applied in different spaces, so I think that continuing medical education opportunities in that can be really helpful. I think that I often find like examples and even language that you can use really helpful in that type of training, so it’s not just theoretical but it’s really thinking about how this can be applied.” (PCP_01)
“I don’t think there’s been anything formal, necessarily, I would benefit I think from something – you know, I think I would probably benefit from a bit more conversation with colleagues.” (PCP_02)
The insights gained during this step directly informed the content and structure of the module ensuring that it addressed the real-world challenges and gaps identified by providers. Data gathered by PCP participants were uniform across perspectives; we did not identify any contrasting views by PCPs. This collaborative process grounded the module in practical strategies to reduce inequities and promote safer, equity-oriented care.
Co-Design Module Content and Structure
We co-designed all components of the module with PCPs and with patient partners. Detailed and frequent conversations were undertaken to discuss the module name, creation of the module logo (Figure 3) and de-escalation strategies (which we redefined as ‘recreating safe connections’ to avoid labelling)to ensure the module was relevant, yet impactful for users. PCPs and patient partners were also involved in the decisions surrounding content and flow of the module.
 |
Figure 3 Creating Safe Connections e-learning module logo. |
The Creating Safe Connections e-learning module integrates thematic insights from PCP interviews with the lived/living experiences of patient partners, developed through a co-generative inquiry process. This participatory approach ensures the module addresses challenges faced by structurally underserved populations and aligns with the principles of EOHC and TVIC.
To incentivise learning uptake, PCPs who complete the module receive a certification. A further Continued Medical Education (CME) accreditation by the College of Family Physicians of Canada sought to increase the reach and adoption of the module during implementation. To attain certification learners must complete pre- and post-learning assessments to evaluate participants’ knowledge, attitudes, and confidence in implementing EOHC principles. The content is structured into four pedagogical outputs: video narratives, case studies, a learner’s notebook, and interactive assessments. An overview of the module’s content is detailed below and in Table 3.
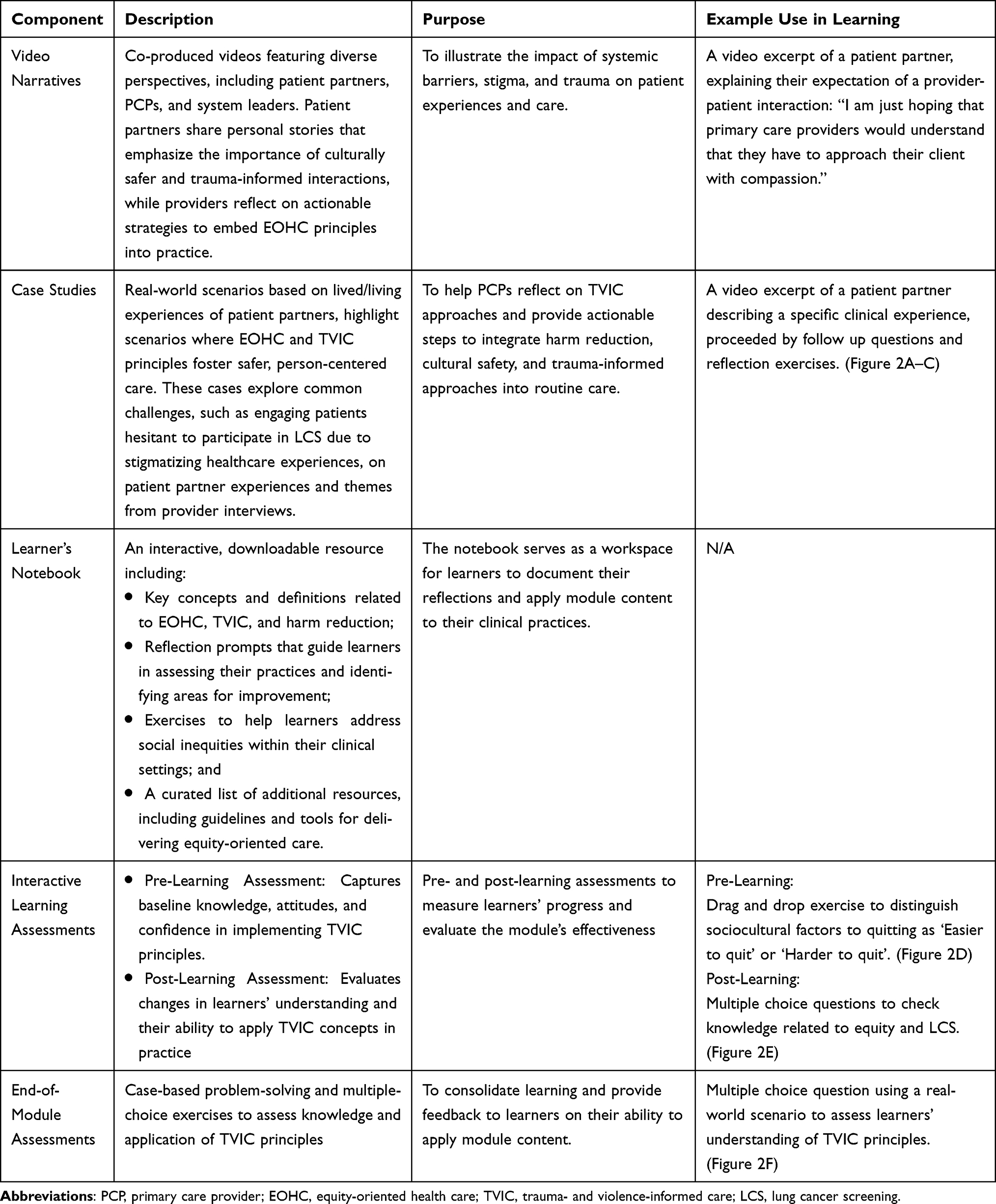 |
Table 3 Overview of Co-Design Module Content |
As we move towards the post-design phase of this work, the module is now freely available to any primary care learner. The module is widely accessible through University of British Columbia’s EQUIP Health Care platform.24
Discussion
The Creating Safe Connections e-learning module reflects a participatory approach to addressing gaps in training for PCPs by integrating TVIC principles into equity-oriented preventative care. This co-designed module centers the lived experiences of structurally underserved populations, offering providers socially accountable and actionable strategies to reduce barriers, foster safer clinical environments, and navigate conversations that can be trauma-inducing.
The co-design process emphasized the value of weaving together patient and provider perspectives to create educational content that is both practical and reflective of real-world challenges. Patient partners provided insights into how stigma, trauma, and social inequities impact access to care, while PCPs identified gaps in their ability to address these issues effectively. The resulting module incorporates video narratives, case studies, and interactive learning tools that promote culturally safer, trauma-informed, and strengths-based approaches to care. By grounding these outputs in TVIC principles, the module equips PCPs with tools to engage meaningfully with patients who often face exclusion from preventative services.
Our findings presented a need for TVIC training for PCPs to build competencies in applying equity-oriented approaches in their clinical practice in Canada. Comparable to our findings, other countries including the United States and Australia have identified skills in trauma-informed care to be of significant influence in patient care quality and health outcomes, predominantly in the area of mental health.25,26 When comparing to other initiatives that have used participatory approaches, such as embedding community and clinician experiences, to create educational interventions for healthcare professionals, the topic of implicit bias was most prominent, specifically in the United States.27 Similar to TVIC, implicit bias training also aims to address health inequities, and in some states this training has also become mandatory.27,28
Ongoing efforts build on this foundation, including the co-creation of a French-language (Canada’s other official language) version of the module and plans for co-implementation and co-evaluation to support national-level scalability. These future phases of post-design aim to refine the module further, by understanding its barriers and facilitators to implementation and evaluation, ensuring its adaptability and sustainability across diverse healthcare contexts and communities while maintaining its alignment with TVIC principles and patient partner perspectives.
Several limitations of this work should be acknowledged. Recruitment for the PCP interviews may have introduced selection bias, as participants were likely to have prior interest or experience in equity-oriented care, limiting the module’s applicability to providers with less familiarity with these concepts. Also, we did not collect demographic data of PCP participants, which limits our interpretation of data based on the unknown diversity of the participant sample. Additionally, while the RAC contributed diverse perspectives, the lived experiences of certain underserved groups, such as rural and remote populations, may not have been fully represented. The module was designed within the Canadian healthcare system, and its generalizability to other systems or contexts requires further exploration. Furthermore, as this study focused on the co-design process, the module has not yet been evaluated in clinical practice to assess its usability, effectiveness, and long-term impact on provider behaviors or patient outcomes. Future research will address these gaps, particularly in understanding how well the module translates into real-world care and its capacity to promote systemic change.
Conclusion
The Creating Safe Connections module is a patient-partnered, co-designed, equity-oriented approach which intends to strengthen primary care practices with a focus on LCS and smoking cessation. By embedding TVIC principles and centering the needs of underserved populations, the module leverages lived experiences and educational tools to address systemic barriers that hinder access to preventative care. By embedding patient voices and focusing on the realities of PCP practice, the pre-design and co-design module processes presented herein provide a model for developing equity-oriented interventions that aim to promote safer, more inclusive healthcare environments. This work underscores the role of social accountability in aligning educational interventions with community priorities, fostering equitable, patient-centered care, and advancing the responsiveness of healthcare systems to those most affected by structural inequities. Although the module was developed within a Canadian primary care context with a focus on LCS and smoking cessation, it can be tailored to support safe clinical conversations in other health settings including diabetes, immunization readiness, cervical cancer screening, and other types of substance use. Further, the module can be translated to other languages to reach non-English speaking populations across Canada and internationally; this is part of our future work to create a French-language version of the module. Future implementation and evaluation efforts will provide further insights into its scalability and effectiveness in clinical practice in addressing structural barriers to care at a broader, systemic level.
Abbreviations
PCP, primary care provider; LCS, lung cancer screening; EOHC, equity-oriented health care; TVIC, trauma- and violence-informed care; LHEAC, Lung Health Equity Advisory Committee; RAC, Research Advisory Council; RIC, Research Interest-Holder Council.
Acknowledgments
We would like to acknowledge the meaningful contributions of Marlene Rathbone, a patient-partner on our team who passed shortly after the module co-design was completed; her legacy continues on through the videos in this module. We would like to acknowledge a message from Marlene, to “be kind, be compassionate, and just listen.” Thank you to the Canadian Partnership Against Cancer for supporting the development of the e-learning module videos and logo. Lastly, the partnership and support of the EQUIP Health Care team at the University of British Columbia (British Columbia, Canada) and Western University (Ontario, Canada) were significant in the development and hosting of the module.
Funding
This study was funded by the Canadian Institutes for Health Research (Grant TLS-170674).
Disclosure
Dr Aisha Lofters reports personal fees from Ontario Health, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Hulscher ME, Wensing M, Grol RP, et al. Interventions to improve the delivery of preventive services in primary care three sources of studies on implement-ing prevention in primary care were used. Am J Public Health. 1999;89(5):737–746. doi:10.2105/AJPH.89.5.737
2. Leach B, Gradison M, Morgan P, Everett C, Dill MJ, de Oliveira JS. Patient preference in primary care provider type. Healthcare. 2018;6(1):13–16. doi:10.1016/j.hjdsi.2017.01.001
3. Leiter A, Veluswamy RR, Wisnivesky JP. The global burden of lung cancer: current status and future trends. Nat Rev Clin Oncol. 2023;20(9):624–639. doi:10.1038/s41571-023-00798-3
4. Sayani A, Vahabi M, O’Brien MA, et al. Perspectives of family physicians towards access to lung cancer screening for individuals living with low income – a qualitative study. BMC Fam Pract. 2021;22(1). doi:10.1186/s12875-020-01354-z
5. Sayani A, Ali MA, Dey P, et al. Interventions designed to increase the uptake of lung cancer screening: an equity-oriented scoping review. JTO Clin Res Rep. 2023;4(3). doi:10.1016/j.jtocrr.2023.100469
6. Roberts H, Walker-Dilks C, Sivjee K, et al. Screening high-risk populations for lung cancer guideline recommendations. J Thorac Oncol. 2013;8(10):1232–1237. doi:10.1097/JTO.0b013e31829fd3d5
7. Partnership Against Cancer C. Lung cancer and equity: a focus on income and geography. 2020.
8. Canadian Task Force on Preventative Health Care. Recommendations on screening for lung cancer. Can Med Assoc J. 2016;188(6):425–432. doi:10.1503/cmaj.151421/-/DC1
9. Sayani A, Vahabi M, O’Brien MA, et al. Advancing health equity in cancer care: the lived experiences of poverty and access to lung cancer screening. PLoS One. 2021:16. doi:10.1371/journal.pone.0251264
10. Davidson CA, Kennedy K, Jackson KT. Trauma-informed approaches in the context of cancer care in Canada and the United States: a scoping review. Trauma Violence Abuse. 2023;24(5):2983–2996. doi:10.1177/15248380221120836
11. Hart JT. The Inverse Care Law. Lancet. 1971;297:405–412. doi:10.1016/S0140-6736(71)92410-X
12. Ford-Gilboe M, Wathen CN, Varcoe C, et al. How equity-oriented health care affects health: key mechanisms and implications for primary health care practice and policy. Milbank Q. 2018;96(4):635–671. doi:10.1111/1468-0009.12349
13. Sayani A, Manthorne J, Nicholson E, et al. Toward equity-oriented cancer care: a Strategy for Patient-Oriented Research (SPOR) protocol to promote equitable access to lung cancer screening. Res Involvement Engagement. 2022;8(1). doi:10.1186/s40900-022-00344-y
14. Readings S. Substance Use and health assessment. In: Study Guide and Laboratory Manual for Physical Examination and Health Assessment. Elsevier Health Sciences; 2023:45–50.
15. Slattery P, Saeri AK, Bragge P. Research co-design in health: a rapid overview of reviews. Health Res Policy Syst. 2020;18(1). doi:10.1186/s12961-020-0528-9
16. Lambert LK, Horrill TC, Beck SM, et al. Health and healthcare equity within the Canadian cancer care sector: a rapid scoping review. Int J Equity Health. 2023;22(1). doi:10.1186/s12939-023-01829-2
17. Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017:358. doi:10.1136/bmj.j3453
18. Sayani A, Monteith L, Shahil-Feroz A, et al. Mobilizing the power of lived/living experiences to improve health outcomes for all. Health Expectations. 2025;28(2). doi:10.1111/hex.70212
19. Sayani AN, Maybee A, Manthorne J, et al. Building equitable patient partnerships during the COVID-19 pandemic: challenges and key considerations for research and policy. Healthcare Policy. 2021;17(1):17–23. doi:10.12927/hcpol.2021.26582
20. Canadian Institutes of Health Research. Strategy for patient-oriented research; 2023. Available from: https://www.cihr-irsc.gc.ca/e/41204.html.
21. Behel J, Israni ST. Restorative practice in healthcare: case studies from academic medicine. In: Roth K, Kumah-Abiwu F, Ritter Z, editors. Restorative Justice and Practice in US Education. Cham: Palgrave Macmillan; 2024:201–215.
22. Wathen CN, Varcoe C, eds.. Implementing Trauma- and Violence-Informed Care: A Handbook. University of Toronto Press; 2023.
23. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
24. Creating Safe Connections: towards Equity-Informed Preventative Care. EQUIP Health Care; 2025. Available from: https://equiphealthcare.ca/online-courses/creating-safe-connections-practical-strategies-to-support-lung-cancer-screening/.
25. Palfrey N, Reay RE, Aplin V, et al. Achieving service change through the implementation of a trauma-informed care training program within a mental health service. Commun Ment Health J. 2019;55(3):467–475. doi:10.1007/s10597-018-0272-6
26. Novilla MLB, Bird KT, Hanson CL, et al. U.S. Physicians’ training and experience in providing trauma-informed care in clinical settings. Int J Environ Res Public Health. 2024;21(2):232. doi:10.3390/ijerph21020232
27. Garrett SB, Jones L, Montague A, et al. Challenges and opportunities for clinician implicit bias training: insights from perinatal care stakeholders. Health Equity. 2023;7(1):506–519. doi:10.1089/heq.2023.0126
28. Cooper LA, Saha S, Van Ryn M. Mandated implicit bias training for health professionals - a step toward equity in health care. JAMA Health Forum Am Med Assoc. 2022;3(8). doi:10.1001/jamahealthforum.2022.3250
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Requirements for Brazilian Outpatient Centers of Excellence in Hidradenitis Suppurativa: Consensus Co-Creative Study
Bellei EA, Shirozaki MEM, Puglia ALP, Esteves de Carvalho AV, Riquena B, Vallilo CC, de Barros D, Tamashiro EY, Cintra G, Duarte GV, da Matta Rivitti-Machado MC, Magalhães RF, do Nascimento RF, Tunala R, da Silva R, Cesar WGG, Thies FG
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2029-2044
Published Date: 4 August 2023