Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Creating A Multi-Criteria Decision Analysis Tool to Enhance Value-Based Purchasing of Generic and Biosimilar Medications in Saudi Arabia: A Pilot Study
Authors Alruthia Y ![]() , Alhajri H, Almohammed OA
, Alhajri H, Almohammed OA ![]() , Balkhi B
, Balkhi B ![]() , Alsaqa’aby MF, Almuqbil MA, Al-Abdulkarim HA, Almutairi AR
, Alsaqa’aby MF, Almuqbil MA, Al-Abdulkarim HA, Almutairi AR ![]()
Received 19 September 2025
Accepted for publication 24 December 2025
Published 8 January 2026 Volume 2026:18 568722
DOI https://doi.org/10.2147/CEOR.S568722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Yazed Alruthia,1,2 Horiyah Alhajri,1 Omar A Almohammed,1 Bander Balkhi,1 Mai F Alsaqa’aby,2 Mohammed A Almuqbil,3– 5 Hana A Al-Abdulkarim,6 Abdulaali R Almutairi7
1Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 2Saudi Society of Pharmacoeconomics and Outcomes Research (PEOR), Riyadh, Saudi Arabia; 3College of Medicine, King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, Saudi Arabia; 4King Abdullah International Medical Research Center (KAIMRC), Ministry of National Guard, Riyadh, Saudi Arabia; 5Division of Pediatric Neurology, Department of Pediatrics, King Abdullah Specialist Children’s Hospital (KASCH), National Guard Health Affairs (NGHA), Riyadh, Saudi Arabia; 6King Abdullah International Medical Research Center (KAIMRC), Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 7Graduate School, Alfaisal University, Riyadh, Saudi Arabia
Correspondence: Yazed Alruthia, Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia, Tel +96-611-4677483, Fax +96 611-4677480, Email [email protected]
Background: Saudi Arabia is reforming its healthcare system to promote the use of generic and biosimilar medications to improve spending efficiency. However, concerns regarding therapeutic equivalence persist. This study aims to establish a stakeholder-driven, value-based procurement framework for off-patent pharmaceuticals (OPPs).
Methods: The Saudi chapter of the International Society of Pharmacoeconomics and Outcomes Research (ISPOR) convened stakeholders to define procurement criteria. Participants reviewed 29 potential criteria during a workshop, followed by a multi-criteria decision analysis (MCDA) simple scoring exercise and conjoint analysis to determine the relative weight of essential factors.
Results: Forty-nine stakeholders participated, primarily pharmacists (57%) and regulators (27%). Sixteen criteria were identified as important: published effectiveness data, drug delivery systems, bioequivalence, real-world data generation, drug stability, direct costs, supply track record, labeled indications, drug safety profile, quality assurance of production, interchangeability, contribution to national healthcare priorities, availability in reference countries, manufacturing site quality certification, pharmaceutical equivalence, and pharmacovigilance. Effectiveness data received the highest weight (11.56%), while pharmacovigilance received the lowest (3.23%).
Conclusion: This pilot study establishes the first consensus-based MCDA criteria for Saudi Arabia, prioritizing effectiveness and drug stability over costs. It emphasizes scientific validity over price, serving as a foundation for a national value-based procurement system, though further research is needed to test the framework in healthcare tenders.
Keywords: Saudi Arabia, generic drugs, biosimilars, multicriteria decision analysis, MCDA simple scoring, value-based purchasing, off-patent pharmaceuticals
Introduction
The universal and efficient delivery of healthcare remains a key policy objective for both developed and emerging economies. Nevertheless, the implementation of good manufacturing practice (GMP) standards and bioequivalence for pharmaceuticals varies significantly across countries. In many regions, strict GMP standards are enforced, along with a maximum allowable variance of 20% for defining generic products based on bioequivalence.1,2 In contrast, some emerging markets have less stringent pharmaceutical regulations, resulting in inconsistent enforcement of bioequivalence principles or pharmaceutical equivalence, where two products must contain the same active ingredient in the exact dosage.2–5 Moreover, the rates of approval of biosimilars in different countries are variable, with some developing countries having more relaxed biosimilarity requirements to increase access to biological therapies, while others maintain stricter standards.6,7 Countries with more relaxed biosimilarity requirements may experience higher rates of adverse events.8–12
In Saudi Arabia, the Saudi Food and Drug Authority (SFDA) mandates that all manufacturers of generic and biosimilar medications provide evidence of bioequivalence or biosimilarity compared to their original products, adhering to top-tier international standards.5 However, there have been numerous reports of therapeutic equivalence failures from various healthcare organizations, particularly within public healthcare institutions, which are required to procure generic and biosimilar medications to improve spending efficiency.4,13 These reports have led the SFDA to initiate a comprehensive investigation into the quality of the implicated medications. If the allegations are substantiated, this inquiry could result in the withdrawal of particular products from the market.14 Such withdrawals may lead to treatment delays, shortages of specific medications, and an increased dependence on more expensive medications.15,16
As a result, there is a growing advocacy among researchers in the pharmaceutical domain, pharmaceutical planning and purchasing specialists, and healthcare providers for the adoption of a more refined set of value-based criteria framework.1,17–19 This approach emphasizes the use of multi-criteria decision analysis (MCDA) incorporating simplified scoring methodologies to mitigate the risk of procuring low-quality off-patent pharmaceuticals (OPPs) and to improve the efficiency of public healthcare spending. In November 2015, the International Society of Pharmacoeconomics and Outcomes Research (ISPOR) organized a workshop focused on identifying the most critical criteria for OPP procurement, bringing together 57 healthcare experts from various emerging economies.1 During the workshop, participants were presented with 22 criteria organized into four primary domains: service, manufacturer, product, and cost-effectiveness. Each criterion was subsequently ranked based on its significance from the participants’ perspectives, using a scale from 5 (highly important) to 1 (unimportant). The top 14 criteria that emerged from this ranking included drug safety, manufacturing site quality certification, quality assurance of active pharmaceutical ingredients (APIs), clinical efficacy and effectiveness, pharmacovigilance, bioequivalence, level of interchangeability, pharmaceutical equivalence, supply track record, indication, formulation, strength, direct costs, excipients, process technology, delivery system, real-world evidence, and local investment.1
In the field of biosimilars, the literature identified several important value-based criteria. These include post-marketing safety, immunogenicity, and effectiveness data, as well as cost savings, value-added services, patient support programs, and educational initiatives.20
In Egypt, an MCDA framework employing a weighted sum method was created to guide the oncology drugs procurement through central tenders.21 The initial MCDA tool included 13 criteria, which were refined to seven after a 2-day workshop involving 35 experts in pharmaceutical purchasing and planning from various governmental organizations, this list was shortened to seven essential criteria based on participants’ votes. The final criteria included use in reference countries, equivalence with the reference product, manufacturing quality, pharmacovigilance services, supply reliability, previous use in local contexts, and macroeconomic benefits.21 Each criterion was assigned different weights based on participant votes collected using the Simple Multi-Attribute Rating Technique (SMART) swing weighting method. Furthermore, a minimum score of 65 points was established as a requirement for any product to successfully navigate the MCDA tool and qualify for the tender.21
In Indonesia, a new MCDA tool was developed following a two-day workshop focused on the tendering decisions for OPPs. In contrast to the Egyptian MCDA tool designed for oncology drug procurement in central tenders, this Indonesian tool assigned approximately 40% of the weight to price advantage among the seven selected criteria. These criteria include price advantage, quality assurance, equivalence with the reference product, product stability and formulation, supply reliability, real-world clinical or economic data, and pharmacovigilance.22
In Saudi Arabia, the pharmaceutical market is the largest in the Middle East and North Africa (MENA) region, with an estimated market size of $9.4 billion as of 2024.23,24 By law, all public health institutions are required to procure their pharmaceutical needs through centralized tenders to promote spending efficiency.23,25 The procurement of generic drugs and biosimilars for public health entities primarily depends on the direct costs of these medications.23 Currently, there is no officially endorsed value-based framework at the national level to improve spending efficiency and ensure high-quality care. This study serves as a pilot initiative designed to establish a foundational consensus for a national value-based procurement framework. Unlike a field trial of an existing tool, this pilot focuses on validating Multi-Criteria Decision Analysis (MCDA) criteria adapted explicitly to the Saudi healthcare context. It aims to identify the unique priorities of local stakeholders before the broader implementation of procurement tenders. Therefore, the objective of this study is to determine the key criteria to be integrated into any future national MCDA tool, taking into account the perspectives of all stakeholders involved in the procurement process for OPPs in Saudi Arabia.
Methods
Study Design
This study included two phases. The first phase consisted of an extensive literature review of previously published studies that involved the development of MCDA frameworks in different healthcare systems to identify all published criteria concerning the procurement of OPPs.1,17–22,26 Twenty-nine criteria have been identified from the previously published studies and reviewed by two professors in pharmaceutical outcomes and economics, one expert in drug safety from the SFDA, a health economist, and two pharmacists. These criteria included the following:
- Direct pharmaceutical costs.
- Pharmaceutical bioequivalence.
- Pharmacovigilance.
- Drug safety.
- United States Food and Drug Administration (USFDA) and/or European Medicine Agency (EMA) approval.
- Number of labelled indications.
- Manufacturing site quality certification.
- Contribution to national healthcare priorities.
- Macroeconomic benefits.
- Order of entry in the local pharmaceutical market.
- Use in reference countries (eg, USA, European Union, Canada, etc).
- Level of interchangeability.
- Technical assistance.
- Drug delivery devices and systems.
- Published data on the effectiveness of generic drugs or biosimilars in peer-reviewed scientific journals.
- Quality assurance of active pharmaceutical ingredients (APIs) and the production process.
- Drug stability.
- Pharmaceutical equivalence.
- Supply track record.
- Good distribution practices.
- History and sustainability of the company.
- Refund or return policy.
- Indirect costs.
- Process technology.
- Excipients.
- Patient support programs.
- Disease awareness and education.
- Continued Medical Education (CME).
- Real-world data generation.
The second phase involved validating these criteria through a stakeholder workshop. Prior to the workshop, the initial list of 29 criteria identified from the literature underwent a content validity check by a preliminary expert panel, consisting of two professors in pharmaceutical outcomes, a senior drug safety expert from the SFDA, and a health economist. This step ensured the criteria were technically accurate and contextually relevant to the Saudi healthcare system before wider evaluation. Subsequently, 49 key opinion leaders participated in a 5-hour interactive workshop. To ensure a balanced and holistic assessment, all expert groups (pharmacists, regulators, academics, and economists) participated equally in the same activities. There was no segregation of roles; every participant engaged in the scenario evaluations and voting processes. This cross-functional design was intended to capture the diverse perspectives of the entire healthcare ecosystem—from regulatory bodies (27%) to public healthcare institutions (49%)—on every proposed criterion.
The tool aims to capture all essential elements of concern to stakeholders in the Saudi healthcare sector, facilitating the efficient and effective procurement of OPPs at a national level. The meeting’s first two hours were interactive with a question-and-answer format using the Slido® platform and covered the criteria identified from the literature. Participants were presented with different scenarios to understand their preferences/opinions of the criteria that should be included in any future MCDA tool for OPPs procurement. The following two hours included voting on each criterion to be included in the MCDA tool using MCDA simple scoring. To ensure data integrity and participant anonymity, a Google® Form was used as the data collection instrument to rate each criterion on a scale of 1 (unimportant) to 5 (highly important), and the form was accessible to attendees only. A score of 3.5 or more was used to identify the most important criteria for OPPs procurement based on the ISPOR workshop that was held in Milan to identify important criteria for OPPs procurement in emerging economies.1
Statistical Analysis
Descriptive statistics (frequencies and percentages) were used to summarize participant characteristics. To determine the relative importance of the criteria, a rating-based conjoint analysis was performed. Participants evaluated specific procurement scenarios using a 5-point Likert scale (1=unimportant to 5=highly important). A regression-based approach was then applied to these ratings to estimate the part-worth utilities, which were converted into relative importance weights (percentages) for each criterion. Criteria with an average raw score of less than 3.5 were excluded from the final weight calculation. To assess the strength of consensus and variability among participants, 95% confidence intervals (CIs) were calculated for the derived weights. All analyses were conducted using SAS version 9.4 (SAS® Institute, Cary, NC, USA).
Confidentiality and Ethical Considerations
This study adhered to the ethical principles of the Declaration of Helsinki and was approved by the Institutional Review Board of the King Saud University College of Medicine (Approval number: E-25-9716). Participation was voluntary, and written informed consent was obtained from all attendees. All data were anonymized and securely stored to ensure participant confidentiality.
Results
Participants’ Characteristics
Out of 68 individuals invited, 49 accepted the invitation and agreed to participate. The majority of participants were male (84%), aged 36 years or older (82%), and identified as pharmacists (57%). The affiliations of participants were varied, with approximately 49% affiliated with public healthcare institutions, 27% from regulatory bodies such as the SFDA and Council of Health Insurance (CHI), 18% from academia, and 6% from other sources. Most participants held a postgraduate degree (90%) and had a minimum of six years of professional experience (92%). Additionally, around 47% of participants served on Pharmacy and Therapeutic Committees within their healthcare institutions. Furthermore, 51% were members of the Pharmaceutical Planning and Purchasing Committee at their respective institutions, as presented in Table 1.
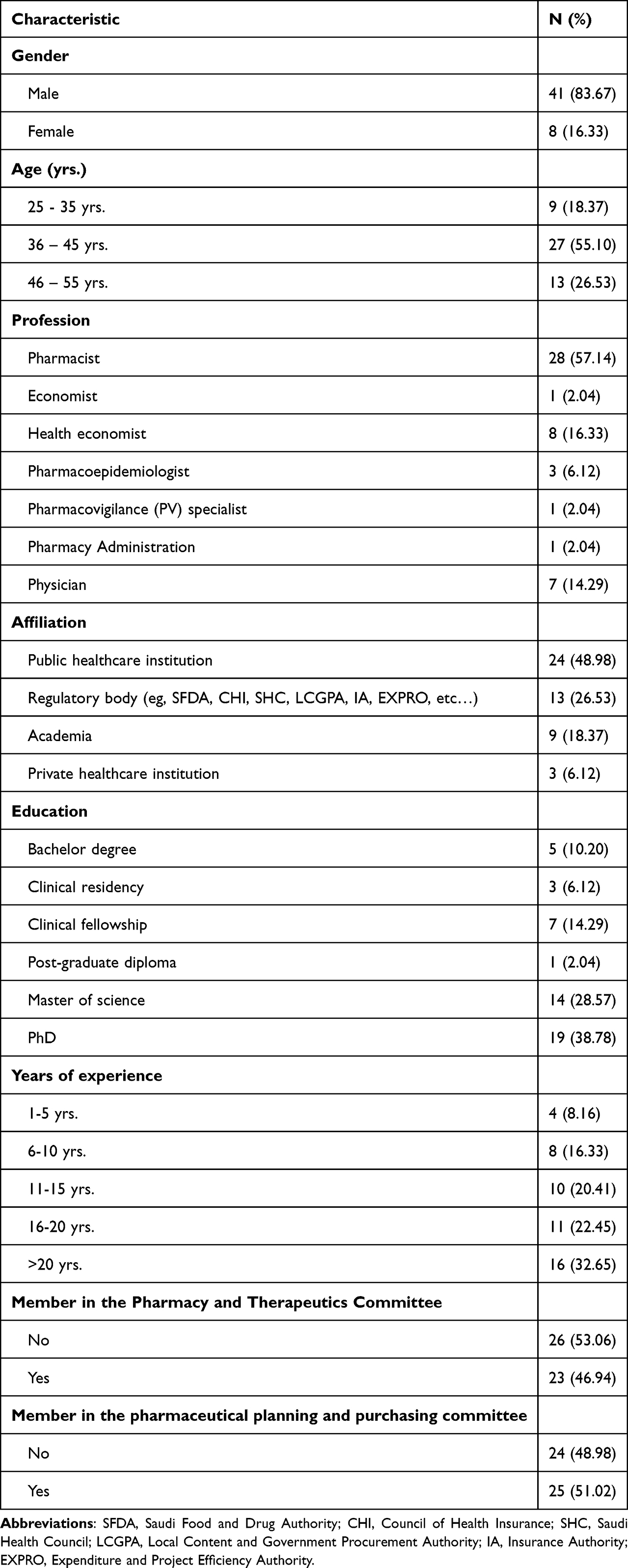 |
Table 1 Participants’ Characteristics (n=49) |
Criteria with High Ratings and Their Assigned Weight
Participants in the study were presented with a comprehensive list of 29 criteria to evaluate, highlighting the essential factors influencing the procurement of OPPs from their perspective. Among these criteria, 16 were identified as particularly important, each receiving mean scores of 3.5 or higher. This indicates a strong consensus on their significance within the procurement process. The key criteria that emerged included:
- Drug Safety: Assurance of minimal adverse effects for patients.
- Real-World Data Generation: The ability to collect and analyze data from actual patient experiences and outcomes.
- Pharmacovigilance: Systems in place for monitoring drug safety post-marketing.
- Published Effectiveness Data: Results from peer-reviewed studies that demonstrate a drug’s efficacy.
- Bioequivalence: Evidence that the generic version of the drug performs similarly to the original.
- Quality Assurance and Production Processes: Rigorous standards ensuring consistent manufacturing quality.
- Labeled Indications: Approved uses of the drug as specified in regulatory documentation.
- Pharmaceutical Equivalence: Confirmation that the drugs contain the same active ingredient in the same strength and dosage form.
- Drug Stability: Information regarding the drug’s shelf life and performance over time.
- Interchangeability Levels: The extent to which different versions of a drug can be substituted for one another.
- Supply Track Record: Historical performance regarding the reliability and consistency of supply.
- Direct Costs: The out-of-pocket expenses associated with the procurement of the drug.
- Manufacturing Site Quality Certification: Verification that the facility producing the drug meets specified quality standards.
- Contribution to National Healthcare Priorities: The drug’s alignment with the healthcare goals of the country.
- Use in Reference Countries: The prevalence and acceptance of the drug in other leading healthcare systems.
- Delivery Systems: The mechanisms employed to provide the drug to patients effectively.
These criteria are visually summarized in Figure 1, illustrating their relative importance.
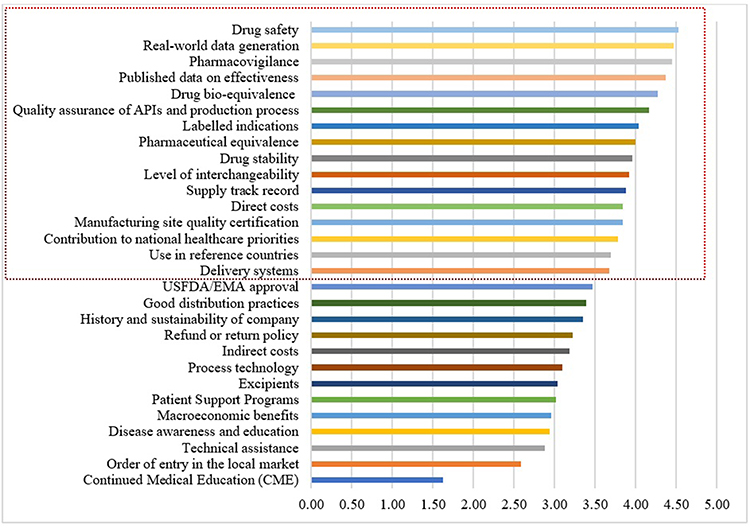 |
Figure 1 Average importance ranking of the 29 evaluated criteria for off-patent pharmaceutical procurement, derived from the MCDA simple scoring method (Scale 1–5). |
To further refine the understanding of these criteria’s significance, a conjoint analysis was conducted, assigning weights to reflect their relative importance in the context of OPPs procurement. Among the 16 criteria, the most critical factor identified was the existence of published effectiveness data from peer-reviewed journal articles, which received a substantial weight of 11.56%. This reveals the priority placed on credible and validated efficacy information in decision-making processes.
Following effectiveness data, the drug delivery system was assigned a weight of 8.84%, indicating its crucial role in ensuring patient accessibility and compliance. Drug bioequivalence followed closely with a weight of 7.56%, emphasizing the importance of consistent therapeutic outcomes between generics and branded drugs. Real-world data generation was weighted at 7.36%, reflecting the demand for insights gathered from patient experiences outside controlled clinical trials. Drug stability garnered a weight of 7.26%, underscoring its importance in maintaining efficacy over time, while direct costs were also prioritized, receiving a weight of 7.08%.
Other noteworthy criteria included the supply track record (6.58%), labeled indications (6.31%), and the drug safety profile (5.98%), all of which contribute significantly to the overall assessment of OPPs. Quality assurance and production processes were also regarded as important, with a weight of 5.58%. Additionally, levels of interchangeability were rated at 5.04%, while the contribution to national healthcare priorities received a weight of 4.77%. Availability in reference countries and manufacturing site quality certification were weighted at 4.43% and 4.39%, respectively, while pharmaceutical equivalence garnered a lower weight of 4.03%. Finally, pharmacovigilance was recognized as a valuable, albeit less prioritized, criterion with a weight of 3.23%. These findings are detailed in Table 2, providing a comprehensive overview of the criteria deemed vital by the participants in the context of OPP procurement. The table includes 95% confidence limits for each criterion, illustrating the variability in stakeholder scoring and the degree of consensus achieved. The newly created tool can be found in Appendix 1.
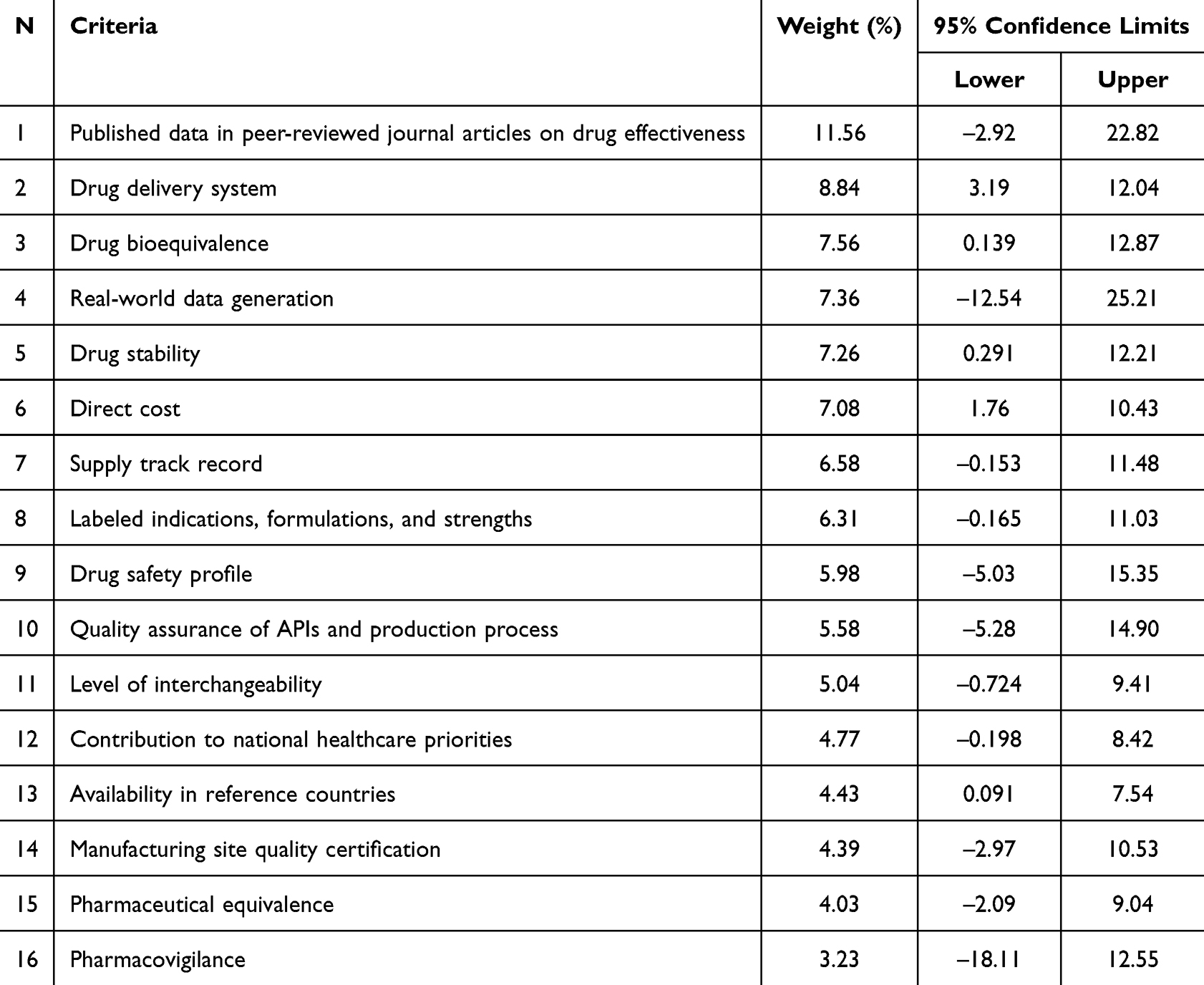 |
Table 2 Relative Weights Assigned to the 16 Prioritized Criteria Derived from Conjoint Analysis of Participant Preferences |
Discussion
The procurement process for OPPs is complex and requires an understanding of various decision-making factors in healthcare.19,20,26 A common misconception is that generic drugs and biosimilars can be directly substituted for their branded counterparts.19 In reality, the landscape is more intricate, as some pharmaceutical products offer additional value beyond cost-saving.20 The idea that “the cheapest is the best” applies only when a thorough analysis considers other critical factors.1 OPPs must also obtain approval from local regulatory authorities prior to procurement, which is particularly significant in Saudi Arabia, the largest pharmaceutical market in the Middle East and North Africa (MENA).1,17,19–22,25
This study examines the procurement criteria for OPPs, analyzing their relevance within the Saudi market and comparing them with those of similar emerging economies. A total of 16 distinct criteria were identified as essential in the procurement of OPPs. Our findings exhibit partial alignment with international frameworks, such as the 14 standards established during the ISPOR Milan workshop and the MCDA framework proposed in the United Arab Emirates (UAE).1 However, distinct divergences emerged that reflect the unique Saudi healthcare landscape. Unlike the Milan workshop results, where “macroeconomic benefits” were prioritized, this criterion was not deemed important by Saudi stakeholders.1 Furthermore, while the UAE framework weighted “real-world clinical and economic outcomes” highest (19.8%),17 our participants differentiated between real-world data generation (7.36%) and “published effectiveness data” (11.56%), prioritizing the latter. These variations likely stem from regional disparities in regulatory maturity and procurement governance across the MENA region. While some emerging markets must prioritize basic manufacturing quality and local investment due to variable regulatory standards, Saudi Arabia’s rigorous bioequivalence enforcement by the Saudi Food and Drug Authority (SFDA) shifts the focus from basic safety to higher-level clinical effectiveness. This context also explains the prioritization of criteria within the centralized tendering system managed by the National Unified Procurement Company (NUPCO). The relatively lower weight assigned to pharmacovigilance (3.23%) and drug safety (ranked ninth) likely reflects stakeholder confidence in the SFDA’s strict pre-market approval and post-market surveillance, viewing safety as a prerequisite controlled by regulation rather than a procurement variable. Consequently, the tool emphasizes criteria that drive clinical efficacy and supply sustainability, such as effectiveness data and supply track record, which support NUPCO’s mandate to ensure both spending efficiency and uninterrupted access to high-quality care.For instance, while the Indonesian MCDA tool assigned a dominant 40% weight to price advantage, our study revealed a “quality-first” approach where Drug Stability (7.26%) and Bioequivalence (7.56%) were weighted higher than Direct Costs (7.08%).22 Furthermore, unlike the UAE framework which combined “real-world clinical and economic outcomes” into a single weighted category,17 our tool differentiates between Published Peer-Reviewed Effectiveness Data (ranked #1) and Real-World Data Generation (ranked #4). This distinction advances upon previous frameworks by isolating the specific stakeholder demand for scientifically validated evidence over general market data. Additionally, where the ISPOR Milan workshop prioritized “macroeconomic benefits”, our Saudi stakeholders placed minimal weight on local investment, prioritizing clinical integrity and supply reliability instead.1 This marked divergence underscores the regional differences in the emphasis placed on procurement factors, thereby reflecting the unique healthcare landscapes and priorities inherent to each region.
The importance of the 16 identified criteria fluctuated significantly, driven by participants’ votes in various procurement scenarios involving generic and biosimilar medications. Intriguingly, the OPPs that were accorded the highest importance, valued at 11.56%, were those underpinned by real-world data published in peer-reviewed journals, demonstrating the medication’s effectiveness. This finding may reveal a degree of skepticism among participants regarding the efficacy of generic and biosimilar medications, pointing to a preference for products with established effectiveness, particularly those substantiated by reputable research. However, this heavy reliance on published peer-reviewed data (11.56%) carries potential implications for procurement equity. While it supports evidence-based decision-making, it may inadvertently disadvantage newer generic entrants that are bioequivalent but lack a history of large-scale effectiveness studies. This could create a barrier to market entry for cost-effective alternatives that have not yet generated extensive academic literature. This inclination aligns with findings from a proposed Multi-Criteria Decision Analysis (MCDA) framework for generic drug procurement developed in the United Arab Emirates (UAE). Within this framework, “real-world clinical and economic outcomes” were given the most considerable weight (19.8%), followed closely by “quality assurance of manufacturing” (17.3%), alongside various other essential criteria.17 However, it is essential to note that previous research did not specify whether the real-world clinical and economic data originated from peer-reviewed publications or were generated after market entry. Our current study made a clear distinction between published data and real-world data generation, assigning a weight of 7.36% to the latter, positioning it as the fourth most critical criterion among the sixteen identified.
Additional findings of particular interest included the rankings associated with drug stability, which was identified as the fifth most important criterion, thus taking precedence over direct costs related to drug acquisition and other associated expenses, such as preparation and administration. This ranking contrast sharply with the conclusions of the ISPOR Milan workshop, where direct costs occupied the 11th position among the 14 criteria, with a scoring scale of 3.5 or higher out of 5, indicating it was not considered the paramount factor in that context.1 Furthermore, the relative ranking of the drug safety profile, positioned ninth among the identified criteria, and the lowest ranking of pharmacovigilance (3.23%), suggests that the participants may not have expressed significant concern regarding drug safety as a procurement differentiator. This perception likely stems from the long-standing use of these medications before they expired patent protection as well as the trust in the SFDA. Stakeholders may view pharmacovigilance as a mandatory regulatory function strictly enforced by the SFDA for all market entrants, rather than a variable criterion to be scored during the tendering process. Thus, the low weight reflects confidence in the existing national safety surveillance infrastructure rather than an undervaluation of post-marketing safety. As a result, considerations such as supply track records, labeled indications, strengths, and formulations appeared to outweigh the emphasis on drug safety in the procurement decisions among participants.
Collectively, these results provide novel contributions to the available knowledge by highlighting distinct shifts in regional procurement priorities compared to global benchmarks. First, the methodological distinction between “published effectiveness data” and “real-world data generation” reveals that stakeholders prioritize pre-existing, peer-reviewed evidence (11.56% weight) significantly over the capacity to generate post-market data (7.36%). Second, the prioritization of “drug stability” (7.26%) over “direct costs” (7.08%) challenges the traditional cost-centric tender model often seen in emerging markets, suggesting a shift toward value-based procurement that prioritizes product integrity over immediate savings.
Limitations
This study represents an important initial step in examining the key criteria for procuring OPPs, which include both generic medications and biosimilar products. It also highlights a notable diversity among the expert participants, who come from various regulatory agencies, academic institutions, and healthcare sectors. However, several limitations must be acknowledged, as they may impact the findings. Firstly, the research was conducted during a single one-day workshop. This format inherently restricts the depth of exploration and validation of the findings, as there was no opportunity for follow-up sessions or continued discussions that could refine the outcomes. The lack of multiple sessions limits the robustness of the conclusions drawn from this study. Additionally, due to this cross-sectional pilot design, formal validation procedures such as test-retest reliability or sensitivity analyses were not conducted. While this limits the assessment of the tool’s stability, future research iterations should incorporate these measures to ensure reproducibility. Secondly, the methodology asked participants to rate various criteria and scenarios involving OPPs with differing characteristics. While this approach aimed to gain insights into expert preferences and the weights they might assign to each criterion, it did not directly ask for their input on prioritizing these criteria. Instead, the responses were obtained through a conjoint analysis framework, which may have introduced unintended biases in how preferences were expressed and understood.
Lastly, potential sampling bias must be acknowledged due to the demographic composition of the panel. The majority of participants were pharmacists (57%) and representatives from regulatory bodies (27%), with a significant portion actively involved in pharmacy and therapeutics or pharmacy planning committees. This predominance may have skewed the study’s outcomes toward a clinical and regulatory perspective, potentially underemphasizing commercial or broader macroeconomic factors. Consequently, the weighting scheme derived in this study should be viewed as provisional; it may evolve as the tool is validated and if future iterations include a more proportional representation of private-sector stakeholders and economic experts.
Conclusion
This study serves as a foundational pilot initiative to facilitate the adoption of a value-based framework for the procurement of OPPs. It advances upon previous MCDA tools developed in the region (eg, Egypt, Indonesia, UAE) by employing a conjoint analysis that specifically separates peer-reviewed clinical effectiveness from real-world data generation, identifying a unique “quality-first” hierarchy where drug stability and bioequivalence outweigh direct costs. This distinction highlights that Saudi stakeholders prioritize therapeutic assurance over the price-centric or macro-economic priorities seen in earlier regional frameworks.
Aligning closely with Saudi Arabia’s Vision 2030 and healthcare reform agenda, this pilot successfully validates the consensus criteria required for a national tool. Future research must build upon this foundational validation by implementing these criteria in real-world procurement scenarios (field-testing). Furthermore, it is crucial to quantitatively assess the outcomes following the adoption of this tool, specifically focusing on the impact on pharmaceutical service quality and the overall health spending efficiency. Such evaluations will ensure the procurement framework delivers tangible benefits to both patients and the healthcare system.
Data Sharing Statement
The data are available upon reasonable request from the corresponding author.
Acknowledgments
We want to express our gratitude to the logistics team at the Saudi ISPOR chapter, particularly Hassan Asiri and Nasser Khodah, for their immense support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Sandoz Saudi Arabia funded this research project. The funder had no role in the design, data collection, or data analysis. The funders were not involved in the preparation or writing of the manuscript.
Disclosure
Yazed Alruthia received speaker fees from Sandoz for educational presentations. The other authors report no conflicts of interest in this work.
References
1. Brixner D, Maniadakis N, Kaló Z, et al. Applying multi-criteria decision analysis (MCDA) simple scoring as an evidence-based HTA methodology for evaluating off-patent pharmaceuticals (OPPs) in emerging markets. Value Health Regional Issues. 2017;13:1–11. doi:10.1016/j.vhri.2017.02.001
2. Patel N, Shah J, Patel A, et al. Bioequivalence requirements of pharmaceutical products in US, Europe and Australia. Int J Drug Regulat Affairs. 2022;10(2):56–61. doi:10.22270/ijdra.v10i2.524
3. Mathur A, Bate R. Generics substitution, bioequivalence standards, and oversight of international pharmaceutical producers: complex issues facing the FDA. 2015, AEI Economics Working Paper.
4. AlRuthia Y, Aljohani B, Alsharif WR, et al. Prospects of establishing a Saudi version of the United States food and drug administration orange book. Health Policy Technol. 2021;10(1):120–125. doi:10.1016/j.hlpt.2020.08.018
5. Kaushal N, Singh S, Gulati M, et al. Study of regulatory requirements for the conduct of bioequivalence studies in US, Europe, Canada, India, ASEAN and SADC countries: impact on generic drug substitution. J Appl Pharm Sci. 2016;6(4):206–222. doi:10.7324/JAPS.2016.60430
6. Rahalkar H, Sheppard A, Santos GM, et al. Current regulatory requirements for biosimilars in six member countries of BRICS-TM: challenges and opportunities. Front Med. 2021;8.
7. Blackstone EA, Joseph PF. The economics of biosimilars. Am Health Drug Benefits. 2013;6(8):469–478.
8. Monga A, Jamwal P, Sharma S, et al. Biosimilars: a critical review of development, regulatory landscape, and clinical implications. AAPS Pharm Sci Tech. 2025;26(1):46. doi:10.1208/s12249-025-03038-2
9. Liu Y, Wang Y, Wang M, et al. Evaluating biosimilars: safety, efficacy, and regulatory considerations in clinical studies. Int J Clin Pharm. 2025;47(1):232–236. doi:10.1007/s11096-024-01825-8
10. Raposo MC, Feiteira C, Ribeiro MH. Regulatory and clinical aspects in biosimilar medicines: comparability, extrapolation, interchangeability, and safety. Drugs Therapy Perspect. 2025;1–15.
11. Erick ME, Umesh S, Athalye SN. Increasing adoption of quality-assured biosimilars to address access challenges in low-and middle-income countries. 2024.
12. Müller R, Renner C, Gabay C, et al. The advent of biosimilars: challenges and risks. Swiss Med Weekly. 2014;144(2728):w13980–w13980. doi:10.4414/smw.2014.13980
13. Alsultan AS, Hakeam HA. Withdrawal of two generic clopidogrel products in Saudi Arabia for non-bioequivalence. Ann Saudi Med. 2018;38(3):233–234. doi:10.5144/0256-4947.2018.233
14. AlQuadeib BT, Alfagih IM, Alnahdi AH, et al. Medicine recalls in Saudi Arabia: a retrospective review of drug alerts (January 2010–January 2019). Future J Pharm Sci. 2020;6(1):1–10. doi:10.1186/s43094-020-00112-3
15. Alruthia YS, Alwhaibi M, Alotaibi MF, et al. Drug shortages in Saudi Arabia: root causes and recommendations. Saudi Pharm J. 2018;26(7):947–951. doi:10.1016/j.jsps.2018.05.002
16. AlRuthia Y, Mohammed Almutiri N, Musa Almutairi R, et al. Local causes of essential medicines shortages from the perspective of supply chain professionals in Saudi Arabia. Saudi Pharm J. 2023;31(6):948–954. doi:10.1016/j.jsps.2023.04.019
17. Farghaly MN, Al Dallal SAM, Fasseeh AN, et al. Recommendation for a pilot MCDA tool to support the value-based purchasing of generic medicines in the UAE. Front Pharmacol. 2021;12:680737. doi:10.3389/fphar.2021.680737
18. Holtorf A-P, Kristin E, Assamawakin A, et al. Case studies for implementing MCDA for tender and purchasing decisions in hospitals in Indonesia and Thailand. J Pharmaceut Policy Pract. 2021;14(1):52. doi:10.1186/s40545-021-00333-8
19. Kolasa K, Zah V, Kowalczyk M. How can multi criteria decision analysis support value assessment of pharmaceuticals?-findings from a systematic literature review. Expert Rev Pharmacoecon Outcomes Res. 2018;18(4):379–391. doi:10.1080/14737167.2018.1467759
20. Simoens S, Cheung R. Tendering and biosimilars: what role for value-added services? J Market Access Health Policy. 2020;8(1):1705120. doi:10.1080/20016689.2019.1705120
21. Elezbawy B, Fasseeh AN, Sedrak A, et al. A multi-criteria decision analysis (MCDA) tool for purchasing off-patent oncology medicines in Egypt. J Pharmaceut Policy Pract. 2022;15(1):10. doi:10.1186/s40545-022-00414-2
22. Inotai A, Brixner D, Maniadakis N, et al. Development of multi-criteria decision analysis (MCDA) framework for off-patent pharmaceuticals–an application on improving tender decision making in Indonesia. BMC Health Serv Res. 2018;18(1):1–12. doi:10.1186/s12913-018-3805-3
23. Hamad A, Alsaqa’aby M, Alruthia Y, et al. Overview of procurement and reimbursement of pharmaceuticals in Saudi Arabia, United Arab Emirates, Qatar, and Egypt: challenges and opportunities. Global J Quality Safety Healthcare. 2023;6(4):127–136. doi:10.36401/JQSH-23-1
24. Alghaith T, et al. Strengthening the Pharmaceutical System in the Kingdom of Saudi Arabia: Towards a Medicine Policy to Support Vision 2030. World Bank; 2020.
25. AlRuthia Y, Aldallal S, Al-Abdulkarim HA, et al. Healthcare systems and health economics in GCC countries: informing decision-makers from the perspective of the Gulf health economics association. Front Public Health. 2025;13:1510401. doi:10.3389/fpubh.2025.1510401
26. Sullivan T. Using MCDA (Multi-Criteria Decision Analysis) to Prioritise Publicly-Funded Health Care. University of Otago; 2012.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.