Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Cranial versus Extracranial Involvement in Giant Cell Arteritis: 15 Years Retrospective Cohort Analysis
Authors Wurmann P ![]() , Karsulovic C
, Karsulovic C ![]() , Sabugo F, Hernandez C, Zamorano Soto P, Mac-Namara M
, Sabugo F, Hernandez C, Zamorano Soto P, Mac-Namara M
Received 16 March 2022
Accepted for publication 27 April 2022
Published 8 June 2022 Volume 2022:14 Pages 97—101
DOI https://doi.org/10.2147/OARRR.S336925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Pamela Wurmann,1 Claudio Karsulovic,1,2 Francisca Sabugo,1 Claudia Hernandez,1 Pedro Zamorano Soto,1 Macarena Mac-Namara1
1Rheumatology Section, Hospital Clínico Universidad de Chile, Santiago, Chile; 2Laboratorio de Inmunomudulacion Neuroendocrina, Biomedical Sciences Institute, Universidad de Chile, Santiago, Chile
Correspondence: Claudio Karsulovic, Sección de Reumatología, Hospital Clínico de la Universidad de Chile, Santos Dumont 999, Independencia, Santiago, Región Metropolitana, 8380456, Chile, Email [email protected]
Giant cell arteritis (GCA) is a medium-large systemic vasculitis presenting primarily in patients over 50 years. It usually involves carotid artery branches, especially the temporary artery; nevertheless, it can affect the arterial wall of other large and medium arteries.1 Cranial manifestations are the most frequent and usually define the study.2 Extracranial involvement, otherwise frequent, can modify clinical and diagnostic features of the disease and may need higher levels of suspicion and other diagnostic strategies to address territories involved.3 Reports regarding extracranial involvement in GCA vary depending on the diagnostic method used, ranging from 3% to 92%. Using angiography, the prevalence ranges from 20% to 67%; on the other hand, positron emission tomography with 18F-fluorodeoxyglucose (FDG-PET) shows 83% and 92%.3,4 Up to 77% of these patients are asymptomatic and present isolated extracranial involvement.5 The most frequently affected extracranial sites are the carotid, subclavian, axillary, and thoracic aorta, which can be complicated with dissection and aneurysms of the affected arteries.4
There are some comparative series between cranial involvement patients and those with extracranial involvement; nevertheless, those do not include Latin American population-based cohorts, including clinical, imaging, and biopsy features.6–8 In a 15-year retrospective cohort study including the aforementioned aspects, we analyzed differences between patients diagnosed with GCA with cranial involvement and patients who had extracranial arteries affected. The latter were diagnosed upon presentation with systemic inflammatory symptoms in the absence of demonstrable infectious disease, persistently elevated inflammatory parameters, vascular symptoms and/or older age (>55 years old). We were able to gather 26 patients with cranial – and no extracranial – involvement defined by clinical aspects, imaging, and biopsy and compare it with eight patients with extracranial involvement (Table 1), including demographic, clinical, physical examination, imaging, biopsy findings, treatment, and follow-up (Table 2).
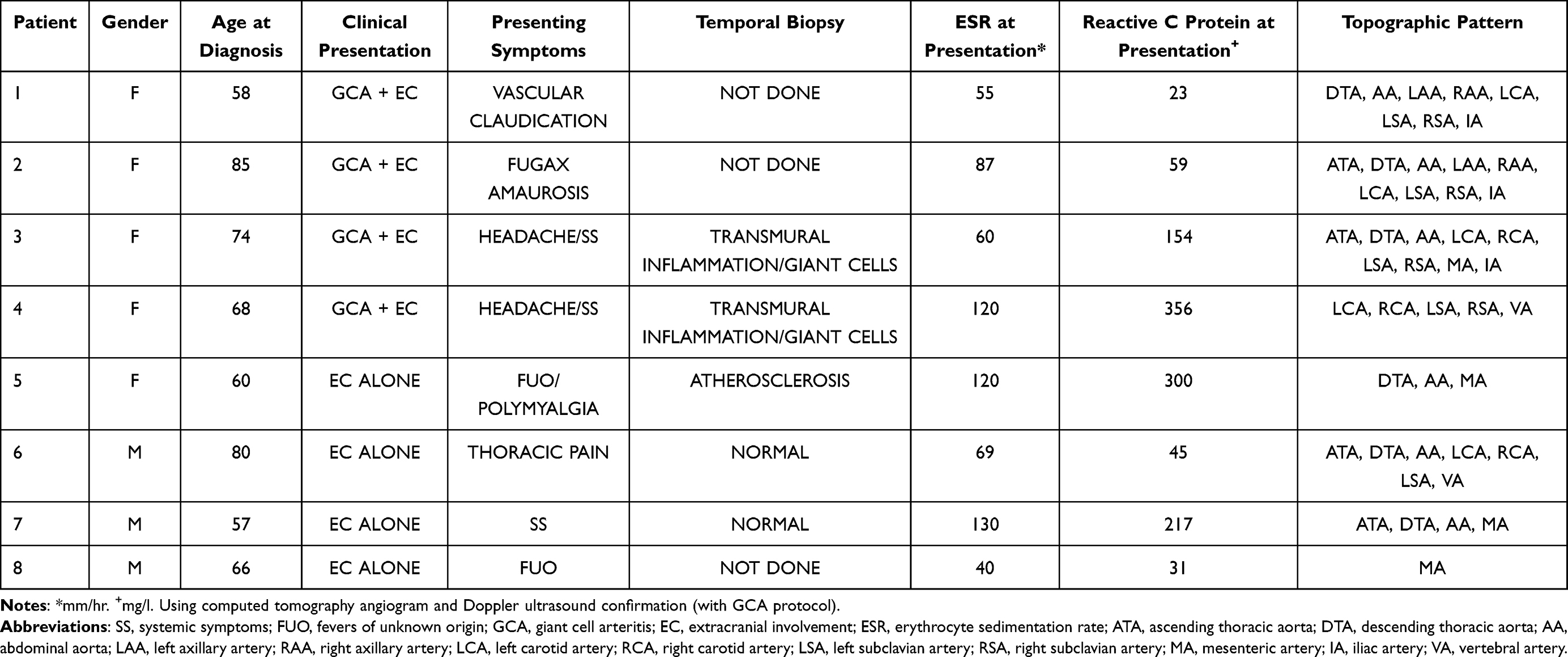 |
Table 1 Extracranial Involvement in Patients’ Clinical and Laboratory Features |
 |
Table 2 Cranial and Extracranial Groups’ Comparative |
Cranial and extracranial involvement groups were demographically homogeneous; nevertheless, headache, a cornerstone in clinical diagnosis, resulted significantly less common in extracranial involvement patients exposing the importance of keeping higher levels of suspicion (Table 2). Laboratory findings regarding inflammatory parameters were similar in both groups; however, creatinine and urinary nitrogen levels were significantly more elevated in the extracranial group, almost doubling creatinine values in the latter. No renal artery compromise was found on an imaging study, considering that those patients do not undergo more sensitive study strategies as angiographic study (Table 2). With all this information, interestingly, half of the patients with extracranial involvement did not meet ACR criteria,9 exposing a big issue: Do these criteria allow us to diagnose patients without temporal artery compromise accurately? In our patients, lack of headache and negative artery biopsy prevented them from fitting the criteria. Biopsies in both groups have the same histologic findings, suggesting no differences in the pathogenic process (Table 2).
In terms of treatment, both groups responded adequately to high doses of corticosteroids and according to reported rates. Remarkably, even when there is no more relapse in either cranial or extracranial involvement group, time to remission was significantly higher in the latter (Table 2).
Considering all this information, some aspects are important: There is no indication of differences in pathogeny between these two types of involvement, as was demonstrated in similar findings in biopsies from both groups. Nevertheless, the clinical course could be different and lead to misdiagnosis or difficulties in suspicion of the disease. Clinical presentation could miss critical symptoms, and temporal biopsy is informed negative, even having systemic inflammation and other large arteries being compromised. Given the frequent compromise of extracranial and cranial territories simultaneously, we should be vigilant, beyond the ACR criteria, of systemic symptoms or fevers of unknown origin in younger patients, which available classification criteria could miss. Given this, it is essential to keep higher suspicion of extracranial involvement in patients presenting with non-infectious inflammatory disease, with high levels of erythrocyte sedimentation rate and C-reactive protein.
Ethics Approval
This study was approved and conducted in compliance with the Declaration of Helsinki. Hospital Clinico de la Universidad de Chile’s Scientific Ethics Committee. Acta N°: 46 on September 5th, 2019 approved this study. Individual informed consent was not asked since all the data was extracted and processed anonymously from digital clinical charts.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no financial or personal conflicts of interest that could bias the work set out in the manuscript.
References
1. Braga BP, Prieto-González S, Hernández-Rodríguez JE, et al. Systemic vasculitis. Large vessel vasculitis: giant cell arteritis and Takayasu’s arteritis. Small vessel vasculitis: cryoglobulinemic vasculitis and IgA vasculitis. Medicine. 2017;12(29):1690–1703.
2. Samson M, Corbera-Bellalta M, Audia S, et al. Recent advances in our understanding of giant cell arteritis pathogenesis. Autoimmun Rev. 2017;16(8):833–844. doi:10.1016/j.autrev.2017.05.014
3. Weyand CM, Goronzy JJ, Solomon CG. Clinical practice. Giant-cell arteritis and polymyalgia rheumatica. N Engl J Med. 2014;371(1):50–57. doi:10.1056/NEJMcp1214825
4. Gribbons KB, Ponte C, Carette S, et al. Patterns of arterial disease in takayasu arteritis and giant cell arteritis. Arthritis Care Res. 2020;72(11):1615–1624. doi:10.1002/acr.24055
5. Buttgereit F, Matteson EL, Dejaco C. Polymyalgia rheumatica and giant cell arteritis. JAMA. 2020;324(10):993–994. doi:10.1001/jama.2020.10155
6. Muratore F, Kermani TA, Crowson CS, et al. Large-vessel giant cell arteritis: a cohort study. Rheumatology. 2015;54(3):463–470. doi:10.1093/rheumatology/keu329
7. Tomelleri A, Campochiaro C, Sartorelli S, Farina N, Baldissera E, Dagna L. Presenting features and outcomes of cranial-limited and large-vessel giant cell arteritis: a retrospective cohort study. Scand J Rheumatol. 2022;51(1):59–66. doi:10.1080/03009742.2021.1889025
8. Gonzalez-Gay MA, Barros S, Lopez-Diaz MJ, Garcia-Porrua C, Sanchez-Andrade A, Llorca J. Giant cell arteritis. Medicine. 2005;84(5):269–276. doi:10.1097/01.md.0000180042.42156.d1
9. Hunder GG, Arend WP, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis. Introduction. Arthritis Rheum. 1990;33(8):1065–1067. doi:10.1002/art.1780330802
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.