")
Back to Journals » International Journal of General Medicine » Volume 14
COVID-19 Vaccine Acceptance and Its Associated Factors Among Pregnant Women Attending Antenatal Care Clinic in Southwest Ethiopia: Institutional-Based Cross-Sectional Study
Authors Mose A , Yeshaneh A
Received 5 April 2021
Accepted for publication 18 May 2021
Published 8 June 2021 Volume 2021:14 Pages 2385—2395
DOI https://doi.org/10.2147/IJGM.S314346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ayenew Mose, Alex Yeshaneh
Department of Midwifery, College of Medicine and Health Science, Wolkite University, Wolkite, Ethiopia
Correspondence: Ayenew Mose Tel +251 974371110
Email [email protected]
Background: COVID-19 vaccination is a safe and effective approach to control the pandemic and to prevent its associated morbidity and mortality. To our knowledge, there is no study conducted to assess the prevalence of COVID-19 vaccine acceptance among pregnant women in Ethiopia. Therefore, the main objective of this study was to assess the prevalence of COVID-19 vaccine acceptance and its associated factors among pregnant women attending antenatal care clinic in Southwest Ethiopia.
Methods: An institution-based cross-sectional study was employed from January 1 up to 30, 2021. A systematic random sampling technique was used to select 396 study participants. A structured and face-to-face interview was used to collect data. Data were entered into Epi-data version 4.2.0 and exported to SPSS version 23 for analysis. Bivariate and multivariate analyses were used to identify factors associated with COVID-19 vaccine acceptance. P values < 0.05 result were considered as a statistically significant association.
Results: The COVID-19 vaccine acceptance was found to be 70.7% (95% CI, 66.7%– 74.7%). Maternal age (34– 41) years [AOR=1.464, (95% CI; 1.218– 5.129)], primary maternal educational status [AOR=3.476, (95% CI; 1.520– 7.947), good knowledge [AOR=5.946, (95% CI; 3.147– 7.065)], and good practice [AOR =9.15, (95% CI; 8.734– 12.189)] of pregnant women towards COVID-19 and its preventive measures were factors associated with COVID-19 vaccine acceptance.
Conclusion: COVID-19 vaccine acceptance was found to be 70.9%. Maternal age (34– 41) years, primary maternal educational status, good knowledge, and good practice of pregnant women towards COVID-19 and its preventive measures were factors associated with COVID-19 vaccine acceptance. Health care workers should provide health education to pregnant women to increase their knowledge about the diseases and disseminate leaflets regarding COVID-19 preventive measures. Moreover, before initiation of COVID-19 vaccine administration to pregnant women they must promote the safety and effectiveness of COVID-19 vaccine.
Keywords: vaccine acceptance, COVID-19, factors, pregnant women, Ethiopia
Background
Globally, the Corona Virus Diseases 2019 (COVID-19) has imposed enormous burdens of morbidity and mortality among the general population.1 Evidence shows that COVID-19 caused more than 2.5 million deaths globally.2 The risk of dying were higher among older adults and people who had chronic medical related disease such as lung cancer, asthma, type 2 diabetes mellitus, heart diseases, and immune compromised patients.3,4 The pregnant women are the most vulnerable group population and they are at a high risk of developing COVID-19 associated adverse pregnancy outcomes, such as preterm births, undergoing caesarean section, intensive care unit (ICU) admission, mechanical ventilation, and death.5,6
The global effort to lessen the effects of the pandemic and to reduce the health and socio-economic impact relies to a large extent on the preventive measures such as consistent use of face masks, maintaining physical distance, avoidance of going to overcrowded places, regular hand washing, and the use of hydro alcoholic solution for disinfection.7 Thus, huge efforts by the scientific community and pharmaceutical industry backed by governments’ support were directed towards developing efficacious and safe vaccines for the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic.8 These efforts were manifested by approval of more than three vaccines. Ethiopia has received Astra Zeneca COVID-19 vaccine and started immunization of high risk populations.9 Despite the manufacturing of the vaccine and the accessibility of COVID-19 vaccines, a major hindrance can exist related to vaccine hesitancy towards the approved and prospective COVID-19 vaccination.10 According to the World Health Organization (WHO), vaccine hesitancy is defined as a behavior with delay in acceptance or refusal of vaccines despite available services. Thus, in 2019 the WHO considered vaccine hesitancy as one of the top 10 potential health trait.11,12
COVID-19 vaccination is safe and effective approach to control the pandemic and in turn to prevent COVID-19 associated morbidity and mortality.13 However, not only does a vaccine need to be safe and effective, it must also be taken up by the population.14 The COVID-19 vaccine trials generated very limited data on safety and efficacy for pregnant women. However, the American College of Obstetrics and Gynecology (ACOG) recommends the pregnant women to use currently approved COVID-19 vaccines.15
COVID-19 vaccine uptake would need to be between approximately 67% and 80% in the general population to reduce spread of the disease. However, the acceptance of COVID-19 vaccine among pregnant women widely differs in countries.16 For instance, a study conducted in 16 countries depicted that vaccine acceptance among pregnant women was generally highest in India, Philippines, and Latin America (>80%); but, it was lowest in Russia, United States, and Australia (<45%).16 Another study conducted in South Africa and Nigeria showed an acceptance rate of 81.6% and 65.2% respectively in general population.17 Based on previous study, the barriers of vaccine acceptance included worrying about COVID-19, misinformation regarding the benefits, lack of confidence in vaccine safety or effectiveness, and compliance to infection prevention guidelines.18
Overall, there is no clear evidence regarding COVID-19 vaccine acceptance among pregnant women in Ethiopia and particularly in the study area. Hence, it is very crucial to understand the prevalence of COVID-19 vaccine acceptance and reasons for refusal among pregnant women which will help administration of COVID-19 vaccine when it is accessible and to design a strategy to overcome the vaccine hesitancy. Therefore, this study was aimed to assess the COVID-19 vaccine acceptance and its associated factors among pregnant women attending antenatal care clinic in Southwest Ethiopia.
Methods and Materials
Study Setting, Design, and Period
An institutional-based cross-sectional study was conducted in Gurage Zone public hospitals, Southwest Ethiopia, from January 1 up to 30, 2021. Gurage Zone is one of 15 zones found in south central Ethiopia. It is 130 km away from Addis Ababa the capital of Ethiopia, 117 km from Hawassa the capital of Southern Nation Nationality and People Region. According to the Central Statistical Agency of Ethiopia (CSA) in 2007, this Zone has a total population of 1,279,646, of whom 622,078 are men and 657,568 are women. According to the zonal health office, COVID-19 has negatively affected the health system, socio-economic system, and severely affects the educational system. The Zone has a total of 1 specialized hospital, 1 general hospital and 4 primary hospitals. These hospitals renders various services with its departments: under five Out-Patient Department (OPD) and adult OPD, Emergency OPD, Tuberculosis (TB) clinic, ART clinic, Maternal and Child Health Services (antenatal care, delivery service, family planning, abortion, and PMTCT services). All hospitals provide antenatal care and delivery service for pregnant mothers free of charge. According to the main Ethiopian Mini Demographic and Health Survey (MEDHS) report 2019, 69.4% of mothers had at least one antenatal care visit, 47.6% of mother gave birth at health institution and 32% of mothers had postnatal care follow-up, in Southern Nation Nationalities and Peoples region.19
Population
Source Population
All pregnant women attending antenatal care clinic at Gurage Zone public hospitals, southwest Ethiopia.
Study Population
All pregnant women who were found in selected hospitals and who were selected using systematic random sampling techniques during the data collection period.
Eligibility Criteria
All pregnant mothers who were attending regular antenatal care follow-up at Gurage Zone public hospitals during data collection period were included. Pregnant women who were critically ill during the study period, who had documented history of mental illness and hearing impairment, which were unable to provide the required information by themself were excluded.
Sample Size Determination and Sampling Procedure
The required sample size was calculated using a single population proportion formula, by considering the following assumption, P= 81.6% proportion of COVID-19 vaccine acceptance of respondents in South Africa,17 d= margin of error taken as 4%, Z α/2= 1.96 at 95% confidence level, and by adding 10% non-response rate the final sample was 396.
Among six hospitals found in Gurage Zone, three hospitals were selected by lottery method (Wolkite University Specialized Hospital, Butajira General Hospital, and Sodo Buye Primary Hospital). Later on, systematic random sampling technique with proportional allocation to each hospital was used to select the study unit. Accordingly, the sample was allocated proportionally to each hospital based on the number of ANC attendees on follow-up at each hospital one month preceding the survey. The total ANC attendees on follow-up within three hospitals one month before the study period were 1321. A total of 512 ANC attendees were being followed up at the ANC clinic in WKU Specialized Hospital and 153 were selected for the study. There were 452 ANC attendees at Butajira General Hospital, and 135 were selected. Finally, 357 ANC attendees at Sodo Buye Primary Hospital, 107 were selected. Sampling interval was determined by dividing the expected number of ANC attendees per month into the sample size 1321/396 which gives a sampling interval of three. Thus, every third coming to a follow up service was interviewed until the total sample size was reached, using a systematic random sampling technique. The first case was selected using lottery method at each hospital.
Data Collectors and Data Collection Procedure
To collect data, nine BSc Midwives were recruited as data collectors and two MSc holder nurse for supervising and coordinating the data collection process. Data was collected by face-to-face interview using a structured and pre-tested questionnaire. The interview was conducted after clients got the ANC service and each client was interviewed privately and assured of the confidentiality of the interview. Data collectors and supervisors were informed to follow the WHO COVID-19 prevention protocols such as using face mask, maintaining physical distancing, and using hand sanitizer during data collection time. The filled questionnaires was collected and checked for consistency every day by the investigators.
Data Collection Instrument
The instrument was prepared after reviewing relevant literature.19,21 The questionnaire was prepared in English language and translated to local language (Amharic) and checked for its consistency by translating it back to English language by those who are well oriented with the stated languages (language professionals or experts). The questionnaire contains: socio-demographic characteristic of the study respondents, knowledge, attitude, practice of the study respondents on COVID-19 preventive measures, and intention of COVID-19 vaccine acceptance among pregnant women.
Study Variable Measurements
COVID-19 vaccine acceptance: “Will you get vaccinated if you get COVID-19 vaccine?” those who respond “Yes” for this question were considered as vaccine acceptance and those pregnant women who respond “No” were considered as vaccine hesitancy.22
Knowledge about COVID-19: The respondents’ level of knowledge about COVID-19 was reported as good knowledge if the study participant correctly responded to more than or equal to 80% of knowledge assessment tools, and poor for <80%.23
Attitudes towards COVID-19: The attitude of the participant was categorized as positive or favorable if responded above or equal to 80% of the attitude related items and negative if below 80%.23
Practice of COVID-19 preventive measures: The respondents’ level of practice of COVID-19 preventive measures was reported as good practice if the study participant correctly responded to more than or equal to 80% of practice assessment tools, and poor for <80%.23
Data Quality Assurance and Control
Two-day training was given for data collectors and supervisors on the objective of the study, how to interview, how to fill the questionnaire and handle questions asked by respondents during interviewing. By considering 5% of the total sample size, pre-test was conducted one week before the start of actual data collection. Then, the questionnaire was assessed for its clarity, length, completeness, and the necessary correction was done accordingly.
Throughout the data collection, interviewers were supervised, regular meetings were held between the data collectors and the principal investigator together in which problematic issues arising from interviews during the data collection and any challenges found were discussed. Completeness of the data was evaluated on a daily basis. The collected data were again reviewed and checked for completeness before data entry. The data entry format template was prepared and programmed by the principal investigator.
Data Analysis and Processing
After data collection, the responses in the completed questionnaire were coded and entered into Epi-data version 4.2.0 and exported to SPSS version 23 for analysis. It was cleaned and edited (checking for missing values and outliers) accordingly. For COVID-19 knowledge and attitude questions internal consistency of the items was checked using Cronbach alpha (α) and the score of ≥ 0.7 was taken as an acceptable measure of internal consistency of items on the scale. Multi-collinearity was also checked to see the correlation between each independent variable, using Variance Inflation Factor (VIF).
The outcome variable of the study was COVID-19 vaccine acceptance which was assessed by asking a question “Will you get vaccinated if you get COVID-19 vaccine?” The outcome variable was coded as “1” for vaccine hesitancy/not accepting and “0” for vaccine acceptance. Binary logistic regression was run to see the crude relationship of each independent variable with COVID-19 vaccine acceptance and to select candidate variables to multi-variable logistic regression analysis. Variables with p-value < 0.25 in bi-variable logistic regression analysis were entered into multivariable logistic regression. Assumptions of logistic regression were also checked. To check the fitness of regression model, Hosmer and lemeshow test was performed and the model was fit with p>0.87. Finally, significant factors were identified based on 95% confidence level Adjusted Odd Ratio (AOR) and p-value <0.05 result were considered as a statistically significant association.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from Wolkite University College of Medicine and Health science, institutional review board (Ref. No: IRB/172/13). Permission to conduct the study was also obtained from each college department. An official letter was written to all selected hospitals. Participants were informed about the purpose and objective of the study. They were also informed that they have the right to discontinue or refuse to participate in the study if they were not comfortable with the questionnaire. Written informed consent was obtained from each study participant. Confidentiality of information and privacy has been maintained. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics
A total of 396 pregnant mothers were involved and making a response rate of 100%. The mean (±) age of study participants was 25.38 (± 3.809 SD) years. The majority of respondents, 185 (46.7%) were aged from 25 to 33 years old. Regarding ethnicity, the majority, 262 (66.2%), of the respondents were Gurage. Out of the total respondents, 365 (65.5%) mothers were married, nearly half, 196 (49.5%), mothers had completed primary education, and 212 (53.5%) mothers were employed by occupation (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Pregnant Woman Attending Antenatal Care Clinic in Southwest Ethiopia, 2021 (n=396) |
Maternal Obstetric Health Care Service Characteristics
In this study, 217 (54.8%) pregnant mothers were multigravida and 177 (44.7%) mothers were multiparous. The majority, 319 (80.6%), of mothers had an antenatal care follow-up. Of these, 131 (33.1%) mothers had 2 times ANC follow-up. Concerning medical illness, 359 (90.7%) mothers did not have any history of medical illness (Table 2).
 |
Table 2 Obstetric Health Care Service Characteristics of Pregnant Women Attending Antenatal Care Clinic in Southwest Ethiopia, 2021 (n=396) |
Maternal Knowledge, Attitude, and Practice of COVID-19 Vaccine and Its Preventive Measures
Among 396 pregnant mothers, 345 (87.1%) mothers had good knowledge, 264 (66.7%) mothers had good attitude, and 243 (61.4%) had good practice towards COVID-19 and its preventive measures (Figure 1).
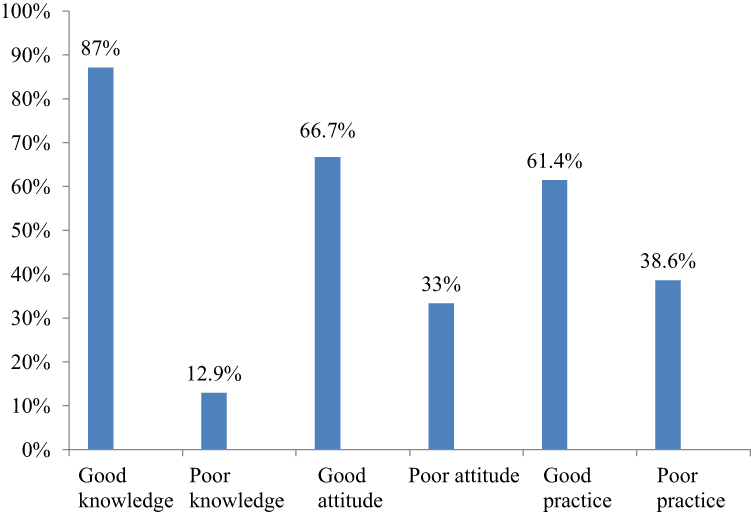 |
Figure 1 Maternal knowledge, attitude, and practice of COVID-19 vaccine and its preventive measures among pregnant women attending antenatal care clinic in Southwest Ethiopia, 2021 (n=396). |
COVID-19 Vaccine Acceptance Among Study Participants
The COVID-19 vaccine acceptance if it is available was found to be 70.7% (95% CI; 66.7%–74.7%). While 116 (29.3%) mothers did not accept to use the COVID-19 vaccine (Figure 2). The reasons for refusal of accepting COVID-19 vaccine were due to fear of side effect, 54 (13.6%), the vaccine might be ineffective, 24 (6.1%), I used other methods of COVID-19 prevention, 20 (5.1%), the vaccine might turn into COVID-19, 15 (3.8%) and the vaccine might affect my fetuses, 3 (0.8%) (Figure 3).
 |
Figure 2 COVID-19 vaccine acceptance among pregnant women attending antenatal care clinic in Southwest Ethiopia, 2021 (n=396). |
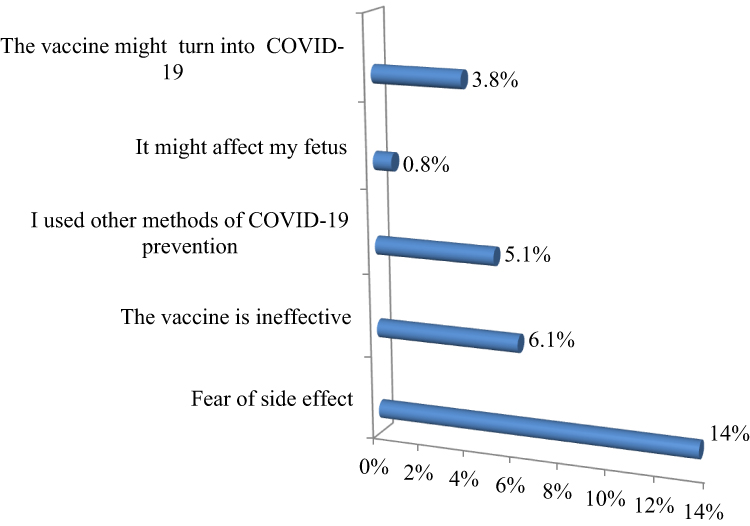 |
Figure 3 Reasons for refusal of accepting COVID-19 vaccination among pregnant women attending antenatal care clinic in Southwest Ethiopia, 2021 (n=116). |
Maternal Source of Information Regarding COVID-19 Vaccine
From the total study participants the majority, 135 (34.1%), of mothers had heard of COVID-19 vaccine from media (television/radio) and 122 (30.8%) mothers heard from health care professionals (Figure 4).
 |
Figure 4 Maternal source of information regarding COVID-19 vaccine among pregnant women attending antenatal care clinic in Southwest Ethiopia, 2021 (n=396). |
Factors Associated with COVID-19 Vaccine Acceptance
The multivariate analysis showed that maternal age (34–41 years), maternal primary educational status, good knowledge, and good practice of pregnant women towards COVID-19 and its preventive measures were significantly associated with acceptance of the COVID-19 vaccine.
The odds of acceptability of COVID-19 vaccine among pregnant mothers found between 34–41 years age group were nearly 1.5 times more likely than those pregnant mothers found in the age group between 18–24 years [AOR=1.464, (95% CI; 1.218–5.129)]. Those pregnant mothers who had completed primary education were 3.5 times more likely to accept COVID-19 vaccine compared to pregnant mothers who had no formal education [AOR=3.476, (95% CI; 1.520–7.947). Pregnant mothers who had good knowledge of COVID-19 and its preventive measures were approximately 6 times more likely to accept COVID-19 vaccine compared to those mothers who had poor knowledge [AOR=5.946, (95% CI; 3.147–7.065)]. The odds of acceptability of COVID-19 vaccine among pregnant mothers who had good practice of COVID-19 preventive measures were 9 times more likely to accept COVID-19 vaccine compared to those mothers who had poor practice towards COVID-19 preventive measures [AOR =9.15,(95% CI; 8.734–12.189)] (Table 3).
 |
Table 3 Bivariate and Multivariate Analysis to Identify Factors Associated with COVID-19 Vaccine Acceptance Among Pregnant Women Attending Antenatal Care Clinic in Southwest Ethiopia, 2021 (n=396) |
Discussion
The newly emerged COVID-19 infectious disease has adverse impact on pregnant mothers and their unborn fetuses following a 2009 pandemic H1N1 influenza virus and Zika virus.6,24,25 Though, after so many trials of vaccine, to date the World Health Organization approved more than three COVID-19 vaccines to mitigate the spread and potential threat of the diseases.8 Nevertheless, vaccine hesitancy becomes one of the greatest challenges globally.11
The finding of the present study showed that the acceptance of COVID-19 vaccine among pregnant women was 70.9%. The result was higher than studies conducted in Saudi Arabia (64.7%),21 United States (67%),26 Middle Eastern Population (36.8%),27 and Poland (31.3%).28 However, it was lower than studies conducted in Addis Ababa (80.9%),20 in China (91.3%),22 in Indonesia, Southeast Asia (93.3%),29 and South Africa (81.6%),17 would accept vaccine when it becomes available among the general population. The possible explanation for the difference might be due to the difference in access to health care service, awareness on the severity of COVID-19, and study population difference.
This study also compares the COVID-19 vaccine acceptance with pervious infectious diseases such as the 2009 influenza H1N1 pandemic and Ebola. For instance, the COVID-19 vaccine acceptance in this study was higher than the 2009 H1N1 vaccine acceptance (47%) of pregnant mothers in United States.30 The possible explanation for the difference might be due to low transmission rate of influenza virus as compared to COVID-19 in the general population that might decrease mother’s uptake of H1N1 vaccine. However, the COVID-19 vaccine acceptance in this study was lower than Ebola vaccine acceptance (76.3%).31 The possible justification might be the Ebola vaccine acceptance was studied among health care workers who might have good awareness and attitude towards vaccination.
In this study, pregnant mothers found in the age group 34 up to 41 years were approximately 1.5 times more likely to accept COVID-19 vaccine compared to those pregnant mothers found in the age group between 18 up to 24 years. The finding was comparable with study conducted in United States among teh adult population.26 This might be due to the fact that the complication of COVID-19 virus among old age population were fatal compared to young age group of population. Additionally, as the age increases there might be age associated chronic diseases such as hypertension, kidney diseases, and heart diseases that might decrease the immunity of pregnant mothers and increases the risk of COVID-19 associated morbidity and mortality. Therefore, it might create fear on the old age group population and they might have more intention to accept COVID-19 vaccine.
Pregnant mothers who had completed primary education were approximately 3.5 times more likely to accept COVID-19 vaccine compared to those pregnant mothers who had no formal education. The finding was consistent with a recent study conducted in South Africa.32 The possible explanation might be those mothers who had completed primary education had the ability to read news and follow social media related to COVID-19 virus impact on the general population, and its fatality. Therefore, they might show intention to use COVID-19 vaccine compared to their counterparts.
The present study assessed maternal knowledge, attitude, and practice of COVID-19 and its preventive measures. The finding of this study showed that 87.1% of mothers had good knowledge towards COVID-19 preventive measures. The result was higher than studies conducted in Gondar City residents, northern Ethiopia (50.7%),33 and in Dirashe district, southern Ethiopia (63.5%).34 The possible justification might be this study was conducted in health facility that expose the study participates to health care workers which enable them to have more awareness regarding knowledge of COVID-19 preventive measures. Similarly, the finding of this study showed that more than half, 66.7% of pregnant women had good attitude towards COVID-19, which was lower than study conducted in Egypt where 75.9% of study participants has positive attitude; however, it was higher than studies conducted in communities residents of Southern Ethiopia (54.5%) and Northern Ethiopia (57.5%).23,33,34 This could be due to the fact that pregnant mothers might strictly follow the healthcare workers counseling/advice during their antenatal care visit regarding COVID-19 preventive measures. This study also found that 61.4% of pregnant women had good practice towards COVID-19 and its preventive measures, which was higher than a study conducted in Gondar (51%).33 However, it was lower than a study conducted in South Africa.35 The variation of the finding could be explained that due to study area and study population difference; for instance, pregnant mothers have better awareness of COVID-19 prevention practice compared to the community due to frequent visits to health institution during their antenatal care follow-up.
Pregnant women who had good knowledge of COVID-19 and its preventive measures were approximately 6 times more likely to accept COVID-19 vaccination compared to those pregnant women who had poor knowledge. This could be explained that pregnant mothers who had good knowledge regarding COVID-19 might know the severity of COVID-19 virus to themselves as well as to their fetus, so that they could easily accept COVID-19 vaccine to decrease the effect of the pandemic. This is also supported by a “Reason Action Theory” which states that an individual’s intention to receive a specific behavior is a function of their current knowledge status towards that behaviour.36 The finding was comparable with recent studies conducted in Addis Ababa among adult population and South Africa among pregnant mothers.20,32 Similarly, those mothers who had good practice of COVID-19 and its preventive measures were 9 times more likely to accept COVID-19 vaccine compared to those who had poor practice regarding COVID-19 and its prevention measures. This could be due to pregnant mothers who had good practice knowing the impact of COVID-19 viruses on the health of the population. Therefore, to decrease the risk of the above complication they might accept COVID-19 vaccine.
The major reasons for refusals of COVID-19 vaccine acceptance among pregnant women were fear of side effect, 13.6%, followed by the vaccine is ineffective, 6.1%. The possible justification could be those mothers who had fear of side effect and considered the vaccine as ineffective might be due to rushing of most of the countries to develop the vaccine and to get more financial benefits that might result in ineffective production of the vaccine. The result was consistent with similar study conducted in Addis Ababa among general population.20
Limitation of Study
The limitation of this study was lack of qualitative data supplementations to explore socio-cultural barriers of pregnant mother’s refusal to accept COVID-19 vaccine. The other limitation of this study was the nature of the study design (cross-sectional) does not show the relationship between cause and effect.
Conclusion and Recommendation
The acceptability of COVID-19 vaccine among pregnant mothers was found 70.9% in the study area. Maternal age (34–41) years, primary maternal educational status, good knowledge, and good practice of mothers towards COVID-19 and its prevention measures were significantly and positively associated with the acceptance of COVID-19 vaccine if it becomes available.
Health care workers should provide health education to pregnant mothers during antenatal care visits to increase their knowledge about the diseases and disseminate leaflets regarding COVID-19 preventive measures to improve maternal practice of COVID-19 prevention. Besides, before initiation of COVID-19 administration to pregnant mothers, policy makers, health care workers, and health extension workers should work in collaboration to promote COVID-19 vaccine regarding its safety and effectiveness and in turn to increase the acceptance of vaccine and to control the pandemic in the study area are recommended.
Availabilities of Data and Materials
The data set used for this study is available from corresponding author upon reasonable request.
Abbreviation
ANC, antenatal care; COVID-19, Corona Virus Infectious Diseases 2019; ACOG, American College of Obstetrics and Gynaecology; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; ICU, Intensive Care Unit; WHO, World Health Organization.
Acknowledgments
The authors are grateful for the data collectors, supervisors, and study participants.
Author Contributions
All authors made substantial contribution to the developing of the proposal, data analysis, preparing manuscript, agreed to submit on this journal, revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Nersesjan V, Amiri M, Christensen HK, Benros ME, Kondziella D. Thirty-day mortality and morbidity in COVID-19 positive vs. COVID-19 negative individuals and vs. individuals tested for influenza A/B: a Population-Based Study. Front Med. 2020;7(November):1–10. doi:10.3389/fmed.2020.598272
2. WHO Coronavirus Disease (COVID-19) Dashboard. Geneva: World Health Organization; 2021. Available from: https://covid19.who.int/.
3. España PP, Bilbao A, García-Gutiérrez S, et al. Predictors of mortality of COVID-19 in the general population and nursing homes. Intern Emerg Med. 2021;(0123456789). doi:10.1007/s11739-020-02594-8
4. Hashim MJ, Alsuwaidi AR, Khan G. Population risk factors for COVID-19 mortality in 93 countries. J Epidemiol Glob Health. 2020;10(3):204–208. doi:10.2991/jegh.k.200817.001
5. Di Mascio D, Khalil A, Saccone G, Rizzo G, Buca DLM. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: a systematic review and metaanalysis. Am J Obs Gynecol. 2020;(2):100–107.
6. Huntley BJF, Huntley ES, Di Mascio D, Chen T, Berghella VCS. Rates of maternal and perinatal mortality and vertical transmission in pregnancies complicated by severe acute respiratory syndrome coronavirus 2 (SARS-Co-V-2) infection: a Systematic Review. Obs Gynecol. 2020;12:136–303.
7. Güner R, Hasanoğlu İ, Aktaş F. Covid-19: prevention and control measures in community. Turk J Med Sci. 2020;50(SI–1):571–577. doi:10.3906/sag-2004-146
8. Conte C, Sogni F, Affanni P, Veronesi L, Argentiero A, Esposito S. Vaccines against coronaviruses: the state of the art. Vaccines. 2020;8(2):1–21. doi:10.3390/vaccines8020309
9. Ababa A, Wohabrebbi Y, Cooperation E, Whetham C, Head R, Pacific A. 2 million COVID-19 vaccines allocated by the COVAX Facility arrive in Ethiopia, marking the start of the country ’ s COVID-19 vaccination campaign; 2021 (March)
10. Harrison EA, Wu JW. Vaccine confidence in the time of COVID-19. Eur J Epidemiol. 2020;35(4):325–330. doi:10.1007/s10654-020-00634-3
11. Cooper S, Betsch C, Sambala EZ, Mchiza N, Wiysonge CS. Vaccine hesitancy–a potential threat to the achievements of vaccination programmes in Africa. Hum Vaccines Immunother. 2018;14(10):2355–2357. doi:10.1080/21645515.2018.1460987
12. Dubé E. Addressing vaccine hesitancy: the crucial role of healthcare providers. Clin Microbiol Infect. 2017;23(5):279–280. doi:10.1016/j.cmi.2016.11.007
13. Readiness C. Evaluation of COVID-19 vaccine effectiveness; 2021.
14. Robertson E, Reeve KS, Niedzwiedz CL, et al. Predictors of COVID-19 vaccine hesitancy in the UK Household Longitudinal Study. Brain Behav Immun. 2021;94:41–50. doi:10.1016/j.bbi.2021.03.008
15. CDC. Investigating the Impact of COVID-19 during Pregnancy. CdcGov/Coronavirus; 2020.
16. Skjefte M, Ngirbabul M, Akeju O, et al. COVID-19 vaccine acceptance among pregnant women and mothers of young children: results of a survey in 16 countries. Eur J Epidemiol. 2021;36(2):197–211. doi:10.1007/s10654-021-00728-6
17. Lazarus JV, Ratzan SC, Palayew A, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2020;27(2):225–228. doi:10.1038/s41591-020-1124-9
18. Nalumansi A, Lutalo T, Kayiwa J, et al. Since January 2020 Elsevier has created a COVID-19 resource centre with free information in English and Mandarin on the novel coronavirus COVID- 19. The COVID-19 resource centre is hosted on Elsevier Connect, the company ’ s public news and information; 2020 (January).
19. CSA. Ethiopia Mini Demographic and Health Survey; 2019.
20. Dereje N, Tesfaye A, Tamene B, et al. COVID-19 vaccine hesitancy in Addis Ababa Ethiopia A mixed-methods study. medRxiv. 2021. Available from: https://medrxiv.org/cgi/content/short/2021.02.25.21252443.
21. Al-Mohaithef M, Padhi BK. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: a Web-Based National Survey.J Multidiscip Healthc. 2020;13:1657–1663. doi:10.2147/JMDH.S276771.
22. Wang J, Jing R, Lai X, et al. Acceptance of covid-19 vaccination during the covid-19 pandemic in china. Vaccines. 2020;8(3):1–14. doi:10.3390/vaccines8030482
23. Kasemy ZA, Bahbah WA, Zewain SK, et al. Knowledge, attitude and practice toward COVID-19 among Egyptians. J Epidemiol Glob Health. 2020;10(4):378–385. doi:10.2991/jegh.k.200909.001
24. Regan AK, Håberg SE, Fell DB, Regan AK. Current perspectives on maternal influenza immunization. Curr Trop Med Rep. 2019;6(4):239–249. doi:10.1007/s40475-019-00188-9
25. Chibueze EC, Tirado V, Lopes S, et al. Zika virus infection in pregnancy: a systematic review of disease course and complications. Reprod Heal. 2017;14(1). doi:10.1186/s12978-017-0285-6
26. Malik AA, McFadden SAM, Elharake J, Omer SB. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020;26:100495. doi:10.1016/j.eclinm.2020.100495
27. Al-Qerem WA, Jarab AS. COVID-19Vaccination acceptance and its associated factors among a middle Eastern population. Front Public Heal. 2021;9(February):1–11. doi:10.3389/fpubh.2021.632914
28. Malesza M. Acceptability of COVID-19 vaccination during pandemic phase of coronavirus in Poland: population based cross-sectional survey; 2020. Available from: https://www.researchgate.net/publication/343140383_Acceptability_of_COVID-19_vaccination_during_pandemic_phase_of_coronavirus_in_Poland_population_based_cross-sectional_survey.
29. Harapan H, Wagner AL, Yufika A, et al. Acceptance of a COVID-19 vaccine in Southeast Asia: a cross-sectional study in Indonesia. Front Public Heal. 2020;8(July):1–8. doi:10.3389/fpubh.2020.00381
30. CDC. Seasonal influenza and 2009 H1N1 influenza vaccination coverage among pregnant women–10 states, 2009–10 influenza season. MMWR Morb Mortal Wkly Rep. 2010.
31. Health R, Jendrossek M, Edmunds WJ et al. Health care worker vaccination against Ebola: vaccine acceptance and employment duration in Sierra Leone. 2018.
32. Hoque AM, Buckus S, Hoque M, Hoque ME, Van Hal G. COVID-19Vaccine acceptability among pregnant women at a primary health care facility in Durban, South Africa. Eur J Med Heal Sci. 2020;2(5):1–6. doi:10.24018/ejmed.2020.2.5.493
33. Nigussie Z, Id A, Merid MW, et al. Adherence towards COVID-19 mitigation measures and its associated factors among Gondar City residents: a community-based cross-sectional study in Northwest Ethiopia. PLoS One. 2020;12(15):1–15. doi:10.1371/journal.pone.0244265
34. Bante A, Mersha A, Azene Tesfaye BT, Shibiru S, Gistane Ayele GM. Adherence with COVID-19 preventive measures and associated factors among residents of; 2021.
35. Hoque AM, Alam AM, Hoque M, Hoque ME, Van HG. Knowledge, attitudes, and practices towards COVID-19 of pregnant women at a primary health care facility in South Africa. Eur J Med Heal Sci. 2021;3(1):50–55.
36. Zeren D, Wu Y, Wang B. Understanding the consumer behaviour during covid-19 pandemic understanding the consumer behaviour during COVID-19 pandemic. Environ Toxicol Pharmacol. 2021;(February). doi:10.1016/j.etap.2021.103672.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.