Back to Journals » Infection and Drug Resistance » Volume 15
COVID-19 Associated Bacteremia with Chryseobacterium indologenes Co-Harboring blaIND-2, blaCIA and blaCcrA
Authors Yeh TK ![]() , Li ZH
, Li ZH ![]() , Huang YT, Liu PY
, Huang YT, Liu PY ![]()
Received 5 November 2021
Accepted for publication 31 December 2021
Published 20 January 2022 Volume 2022:15 Pages 167—170
DOI https://doi.org/10.2147/IDR.S347066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Ting-Kuang Yeh,1 Zong-Hao Li,2 Yao-Ting Huang,2 Po-Yu Liu1,3,4
1Division of Infectious Diseases, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 2Department of Computer Science and Information Engineering, National Chung Cheng University, Chiayi, Taiwan; 3Ph.D. Program in Translational Medicine, National Chung Hsing University, Taichung, Taiwan; 4Rong Hsing Research Center for Translational Medicine, National Chung Hsing University, Taichung, Taiwan
Correspondence: Po-Yu Liu, Division of Infectious Diseases, Department of Internal Medicine, Taichung Veterans General Hospital, 1650 Taiwan Boulevard Sect. 4, Taichung, 40705, Taiwan, Tel +886-4-23592525-3329, Fax +886-4-23592525-83588, Email [email protected]
Abstract: We report a COVID-19 case with carbapenem resistant Chryseobacterium indologenes bacteremia. Whole genome sequencing identified the presence of blaIND-2, blaCIA and blaCcrA. To our knowledge, this is the first report of Chryseobacterium indologenes complicating COVID-19 and the detection of blaCcrA in C. indologenes. The presence of blaCcrA in Chryseobacterium was overlooked previously may related to substantial sequence divergence with the original allele in Bacteroides fragilis. Antimicrobial resistance (AMR) is a challenge to global health in the age of COVID-19 pandemic. Further study and surveillance of underlying mechanisms is needed.
Keywords: COVID-19, SARS-CoV-2, Chryseobacterium indologenes, resistance
As the COVID-19 pandemic continues, bacterial co-infections are reported globally and attributed to significant mortality. Secondary bacterial infections could occur in more than 50% of fatal COVID-19 patients.1 Considerable increase in antimicrobial resistance (AMR) in associated with heavy use of broad-spectrum antibiotics in COVID‐19 patients was expected and multidrug‐resistant (MDR) bacterial co-infections were reported.2 The prevalence of carbapenem resistance in COVID-19 bacterial co-infection cases was reported higher than 90%.1 About AMR, different resistant pattern had been classified, including MDR, extensively drug-resistant (XDR), pandrug-resistant (PDR), usual drug-resistant (UDR) and newly difficult-to-treat resistance (DTR).3 The crush of COVID-19 pandemic with increasing AMR deserved close monitor.
Chryseobacterium indologenes, a non-fermenting, non-motile gram-negative bacillus, belongs to the genus Chryseobacterium and was previously named as flavobacterium indologenes. It is distributed in nature, found in soil, plants, and water. C. indologenes has become one of nosocomial pathogens, often associated with immunocompromised and indwelling device in recent decades.4 C. indologenes frequently exhibit resistance to penicillin, cephalosporins and carbapenems.5 It has been assumed the AMR of C. indologenes is caused by class A β-lactamase blaCIA and class B carbapenem-hydrolyzing β-lactamase blaIND. The blaIND and blaCIA were the predominant AMR gene in C. indologenes and the blaIND and blaCIA co-harboring C. indologenes were also reported.6 Although C. indologenes has become one of healthcare-associated infections (HAI) pathogen, there are few reports about C. indologenes infection associated with COVID-19. Here, we reported a COVID-19 patient with superimposed C. indologenes bloodstream infection. Genomic analysis further revealed the C. indologenes co-harboring three β-lactamases gene, blaIND-2, blaCIA and blaCcrA.
A 58-year-old Taiwanese male was admitted due to COVID-19, diagnosed by reverse transcriptase polymerase chain reaction viral nucleic acid test. Bilateral pneumonia complicated with oxygenation failure developed on admission day 1. Recurrent fever to 38.6°C on 10th day after admission. Blood cultures yielded Gram-negative bacilli and was identified as C. indologenes by MALDI-TOF MS (BioMérieux). The susceptibility test, determined by VITEK®2 (bioMérieux), revealed the C. indologenes isolate was resistant to piperacillin/tazobactam, ceftazidime, ceftriaxone, cefepime, imipenem, amikacin, gentamicin, ciprofloxacin, tigecycline (Table 1). The report was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Taichung Veterans General Hospital (CE20261A).
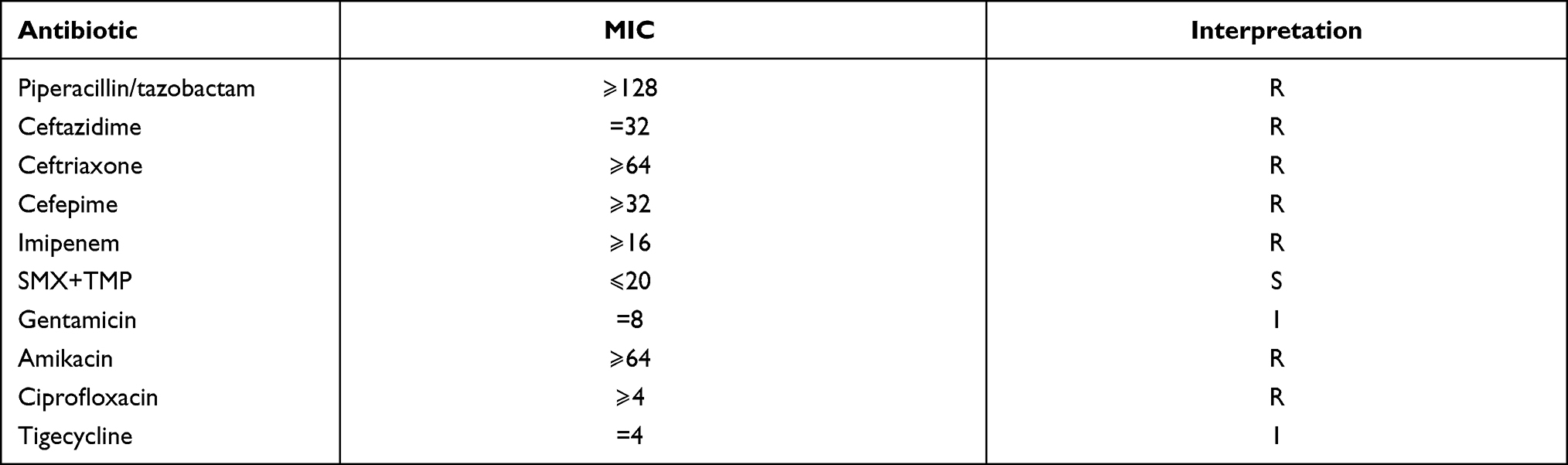 |
Table 1 Minimum Inhibitory Concentration (MIC) of the C. indologenes Strain C205 |
The whole genome of this C. indologenes strain (designated strain as C205) was sequenced using Nanopore sequencing (GridIon, R9.4 flowcells). The genome was assembled by Flye and the errors were corrected by Homopolish. The antibiotic resistant genes were annotated by NCBI AMRFinderPlus and Hidden Markov Models (HMM) search was used. Whole-genome sequencing, assembly, and resistome analysis identified two metallo β-lactamases (blaIND-2 and blaCcrA) and one extended-spectrum β-lactamase (blaCIA) in the chromosome (Figure 1). All the sequencing data have been deposited in GenBank under Accession CP085529. blaCcrA in Chryseobacterium has not been reported previously. Further investigated did not identify mobile genetic elements at either upstream nor downstream of the blaCcrA in C. indologenes C205, suggesting a possibility of vertical transmission. Subsequent search of blaCcrA in the NCBI database confirms it was also presented in the chromosomes of other C. indologenes strains and many species of Chryseobacterium (e.g., C. lactis, C. phosphatilyticum, and C. carnipullorum). No C. indologenes growth in the sputum culture of this case. Indwelling central venous catheter was considered as risk factor and infection source of C. indologenes bacteremia in this case. The patient was treated with trimethoprim-sulfamethoxazole (TMP-SMX) and discharged under clinical stable condition.
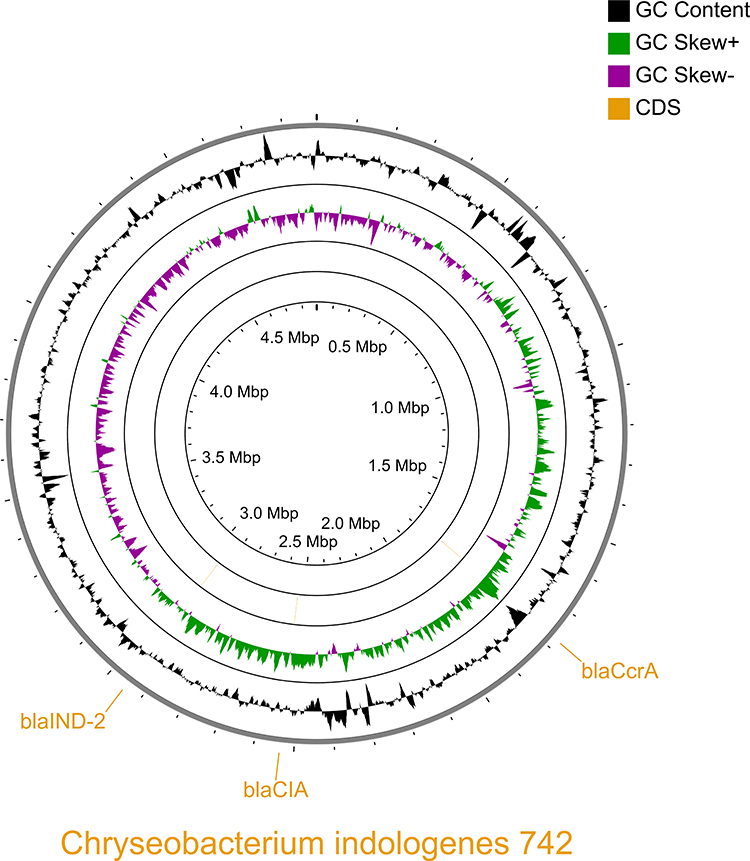 |
Figure 1 Circular maps of the chromosome of C. indologenes. The outermost ring highlights the CDS loci of three beta lactamases: blaIND-2, blaCIA, and blaCcra. The following inner ring depicts the GC content (black). The two remaining inner rings show the GC skew on the forward and reverse strands (purple/green). |
To the best of our knowledge, this is the first report COVID-19 associated bacteremia with C. indologenes co-harboring blaIND-2, blaCIA and blaCcrA. Considering secondary bacterial co-infections with AMR attributed to increasing mortality during previous pandemics,2 COVID-19 patients superimposed bacterial infection with MDR pathogen deserved more investigation.
The blaCcrA has not been reported in Chryseobacterium. The CcrA, belonging to metallo-β-lactamase, was initially identified in a clinical isolate of Bacteroides fragilis TAL3636.7 CcrA enzyme strongly hydrolyzed cefoxitin and carbapenems, but not the monocyclic β-lactam. CcrA enzyme was inhibited by tazobactam but not clavulanic acid or sulbactam. Our investigation indicated the blaCcrA is not only found in our strain but also vertically transferred in many species of Chryseobacterium. The presence of blaCcrA in Chryseobacterium was overlooked in previous studies because of substantial sequence divergence with the original allele in B. fragilis. Therefore, the homology-based search of antibiotic-resistance genes would miss this β-lactamase.
In conclusion, we reported the first case of co-harboring blaIND-2, blaCIA and blaCcrA in a C. indologenes strain isolated from a COVID-19 patient with bacteremia. The interrelationship between SRAS-CoV-2 and AMR represents a public health concern globally.
Author Contributions
All authors made a significant contribution to the work reported during the conception, study design, execution, data acquisition, analysis, interpretation, drafting, and revising, or critically reviewing the article. All authors gave their final approval of the version to be published and the chosen journal for submission, and they agreed to be accountable for all aspects of the work.
Funding
YTH was supported in part by the Ministry of Science and Technology (109-2221-E-194-038-MY3). PYL was supported in part by the Ministry of Science and Technology (110-2314-B-075A-011) and Taichung Veterans General Hospital (TCVGH-1103901C and TCVGH-1103901D).
Disclosure
All authors report no conflicts of interest relevant to this work.
References
1. Vijay S, Bansal N, Rao BK, et al. Secondary infections in hospitalized COVID-19 patients: Indian experience. Infect Drug Resist. 2021;14:1893–1903. doi:10.2147/IDR.S299774
2. Ukuhor HO. The interrelationships between antimicrobial resistance, COVID-19, past, and future pandemics. J Infect Public Health. 2021;14(1):53–60. doi:10.1016/j.jiph.2020.10.018
3. Kadri SS, Adjemian J, Lai YL, et al. Difficult-to-treat resistance in gram-negative bacteremia at 173 US hospitals: retrospective cohort analysis of prevalence, predictors, and outcome of resistance to all first-line agents. Clin Infect Dis. 2018;67(12):1803–1814. doi:10.1093/cid/ciy378
4. Mukerji R, Kakarala R, Smith SJ, Kusz HG. Chryseobacterium indologenes: an emerging infection in the USA. BMJ Case Rep. 2016;2016. doi:10.1136/bcr-2016-214486
5. Kirby JT, Sader HS, Walsh TR, Jones RN. Antimicrobial susceptibility and epidemiology of a worldwide collection of Chryseobacterium spp: report from the SENTRY Antimicrobial Surveillance Program (1997–2001). J Clin Microbiol. 2004;42(1):445–448. doi:10.1128/JCM.42.1.445-448.2004
6. Zhang Y, Li D, Yang Y, et al. Clinical and molecular characteristics of Chryseobacterium indologenes isolates at a teaching hospital in Shanghai, China. Ann Transl Med. 2021;9(8):668. doi:10.21037/atm-21-933
7. Rasmussen BA, Gluzman Y, Tally FP. Cloning and sequencing of the class B beta-lactamase gene (ccrA) from Bacteroides fragilis TAL3636. Antimicrob Agents Chemother. 1990;34(8):1590–1592. doi:10.1128/AAC.34.8.1590
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.