")
Back to Journals » Infection and Drug Resistance » Volume 16
COVID-19 and Listeria Meningitis Treated by Ampicillin, Sulfamethoxazole/Trimethoprim and Meropenem
Authors Seki M , Karaushi H, Arai N, Hayashi T, Mitsutake K
Received 19 April 2023
Accepted for publication 29 June 2023
Published 3 July 2023 Volume 2023:16 Pages 4289—4295
DOI https://doi.org/10.2147/IDR.S414879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Masafumi Seki,1,* Haruka Karaushi,1,* Noriko Arai,2 Takeshi Hayashi,2 Kotaro Mitsutake1
1Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Hidaka City, Saitama, Japan; 2Division of Neurology, Saitama Medical University International Medical Center, Hidaka City, Saitama, Japan
*These authors contributed equally to this work
Correspondence: Masafumi Seki, Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Yamane 1397-1, Hidaka City, Saitama, 350-1298, Japan, Tel +81-42-984-4392, Fax +81-42-984-0280, Email [email protected]
Background: Secondary bacterial infection was initially rare in SARS-CoV-2 infectious disease (COVID-19) patients, but COVID-19-associated bacterial infectious diseases have recently been increasing. Furthermore, it might be difficult to distinguish COVID-19 from bacterial meningitis by the symptoms, and one might be uncertain about antibiotic therapy for Listeria meningitis infection—typically caused by eating contaminated food—in elderly persons and pregnant women.
Case Report: A 96-year-old woman who had been living alone was found to have SARS-CoV-2 infection in February 2023. She was admitted to our hospital with high fever and disturbance of consciousness and was started on treatment with remdesivir. Two days later, her consciousness was still disturbed, and she was found to have a stiff neck. In addition, increased white blood cell counts and C-reactive protein suggested bacterial infection. Therefore, a lumbar puncture was done, and Listeria monocytogenes was ultimately isolated from blood cultures and its genetic material was detected in cerebrospinal fluid. She had previously eaten refrigerated food and cheese products. Intravenous ampicillin 1.0 g 6×/day was started, but one week later, loss of consciousness continued, and the cerebrospinal findings were not improved, although nasal swab became negative for SARS-CoV-2. Intravenous sulfamethoxazole/trimethoprim (ST) 80/400 mg 3×/day was added, and her consciousness and fever improved by one week later. A drug rash appeared after ST was started, and she was switched to meropenem. Her condition finally improved.
Conclusion: COVID-19-associated secondary listeria infection was found in an elderly woman. She was treated with not only ampicillin, but also ST and meropenem. Meningitis caused by Listeria monocytogenes should be considered as a secondary complication and carefully treated with antibiotics during the period of the COVID-19 pandemic.
Keywords: penicillin, carbapenem, antibiotics, drug rash, SARS-CoV-2
Introduction
SARS-CoV-2 virus coronavirus infectious disease (COVID-19) has been a significant issue, and treatment of COVID-19, including its associated secondary bacterial infections, has become a problem recently because omicron subvariant BA.5, which is not very pathogenic, but shows high infectivity, has prevailed in Japan and caused increased mild to moderate bacterial infections in elderly persons around 2022.1,2
The antimicrobial stewardship was considered important and was emphasized around 2020, the early stage of the COVID-19 pandemic, because secondary bacterial pneumonia was suggested to be at a low rate, only 3% to 15%.3,4 It was therefore thought that pure viral pneumonia was dominant in COVID-19, although secondary bacterial pneumonia was common in influenza, and more than 30% of influenza patients were co-infected with bacteria.5 The antibiotics were used excessively and the appearance of antimicrobial resistant pathogens has been worried. Recently, however, we might have to use antibiotics in the BA.5 period in the same manner as for influenza.1,2
In addition, not only pneumonia, but also other invasive infectious diseases including meningitis were considered as COVID-19-associated bacterial infections in the omicron era, although the rate of bacterial meningitis was also decreased in the early phase of the COVID-19 pandemic.6,7 It has been reported that the omicron variant of SARS-CoV-2 induces more symptoms in the upper respiratory tract than in the lower respiratory tract, and this form of “common cold” could lead to inflammation of the Eustachian tube and the oropharynx, and such dysfunction enhances the migration of bacteria, such as Haemophilus influenzae and Streptococcus pneumoniae to the middle ear, causing otitis media, which in turn could lead to further complications including acute meningitis and mastoiditis.6
Listeria monocytogenes is a Gram-positive bacillus and facultative intracellular bacterium, and listeriosis is considered to be among the most common bacterial foodborne infections.8 The large majority of listeriosis cases are sporadic, but outbreaks occur after contamination of soft cheeses or ready-to-eat food, and L. monocytogenes was discovered on at least one food specimen in the refrigerators of 64% of 123 patients with L. monocytogenes infection.8 In recent years, an increasing rate of listeriosis has been reported, particularly in pregnant women, aged people and patients receiving immunosuppressive treatment. In addition, there was a mortality rate of up to 30% with neurological involvement.8 With the exception of natural in vitro resistance to older quinolones, fosfomycin, and expanded-spectrum cephalosporins, ampicillin (ABPC) has been regarded as the key therapeutic drug against L. monocytogenes as the bacterium is widely susceptible to clinically relevant classes of antibiotics active against Gram-positive bacteria.8
In this case report, a healthy, elderly woman who developed COVID-19-associated secondary bacterial meningitis caused by L. monocytogenes, which was isolated from the blood and its genetic material detected in cerebrospinal fluid (CSF), is described. Her initial SARS-CoV-2 antigen (Ag) was low and blood data showed highly increased white blood cell (WBC) and C-reactive protein (CRP) counts at admission suggesting SARS-CoV-2 infection followed by secondary L. monocytogenes infection. She was treated by remdesivir then ABPC, but additional sulfamethoxazole/trimethoprim (ST) was needed. Finally, treatment with meropenem (MEPM) was successful, although a drug rash had appeared by ST administration.
Case Presentation
A 96-year-old woman with mild hypertension had been living alone, but then developed general malaise and loss of consciousness in February 2023. Her nephew, who visited her house once a week, found her and brought her to the emergency department. She had been vaccinated three times for SARS-CoV-2 with BNT162b2 (Pfizer/BioNTech), and the third vaccination was about six months earlier. Green salad, cheese and other refrigerated products were her favorite foods. However, she became positive for SARS-CoV-2 on polymerase chain reaction (PCR, Cobas SARS-CoV-2, Roche, Basel, Switzerland) test, and her temperature was high (38.9°C) at that time (day 0). We were unable to confirm the specific variants of the detected virus from her nasal swab; however, omicron was the dominant variant and accounted for all cases in Japan at the time. Therefore, her variant was suggested to be the omicron variant.
Laboratory data on admission to our hospital were as follows: WBC count, 18.65 × 103/μL, with 91.5% neutrophils, 5.5% lymphocytes, 2.8% monocytes, 0.0% eosinophils, and 0.2% basophils; hemoglobin, 16.5 g/dL; platelet count, 25.3 × 103/μL; serum creatinine, 0.71 mg/dL; blood urea nitrogen, 26.6 g/L; aspartate aminotransferase (AST), 31 U/L; alanine aminotransferase (ALT), 14 U/L; and CRP, 4.226 mg/dL. Arterial oxygen saturation (SpO2) was 97% (normal) and no shadows were found on chest computed tomography (CT). SARS-CoV-2 Ag by nasal swab was positive, but at a low titer, 1.77 IU (Cobas SARS-CoV-2 Ag, Roche).
According to the treatment protocol for admitted COVID-19 patients in our hospital, remdesivir (Gilead, Foster City, CA, USA) drip infusion for 5 days was started as the antiviral therapy. On day 2, her high fever continued, and SARs-CoV-2 Ag was still positive, but not increased (1.24 IU). Meningitis was then suspected because she also had a stiff neck and because of her laboratory data at admission, such as increased WBC and CRP counts. Thus, CSF examination was performed. The CSF was yellow and cloudy, suggesting bacterial meningitis (Table 1). On the same day, the characteristic short Gram-positive rods that occur singly or in short chains were found in the blood culture bottle and L. monocytogenes was identified (Figure 1). Although L. monocytogenes was not isolated from the CSF, its RNA was detected in the CSF by a multiplex PCR system (FilmArray, Biomerieux, Lyon, France).
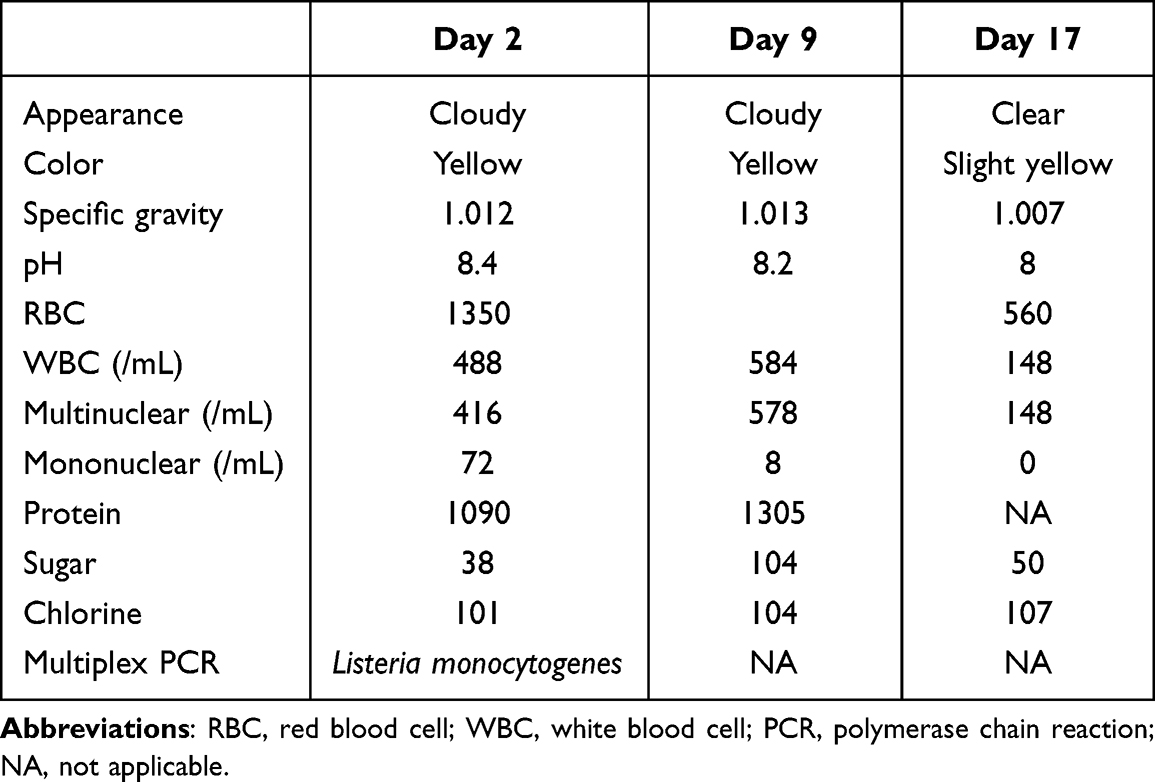 |
Table 1 The Time Course of Cerebrospinal Fluid Improvement |
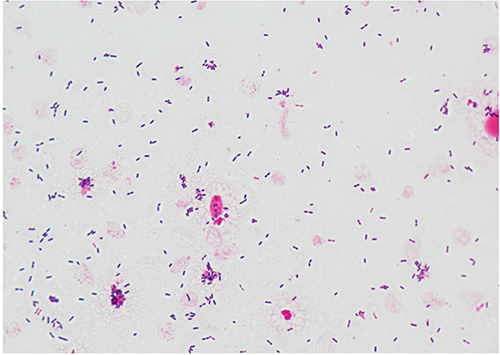 |
Figure 1 Gram stain findings of Listeria monocytogenes isolated from blood culture. Numerous chains of Gram-positive rods are visible but are Gram-variable, and some bacilli resemble Gram-negative rods. |
Because ABPC is considered as the standard antibiotic for listeriosis8 and is effective for isolated L. monocytogenes (Table 2), ABPC 1.0 g 6×/day intravenously was started after consultation with the antimicrobial stewardship team. Even though her renal function was normal and she might have tolerated a higher dosage, her body weight was only 29 kg. One week later, her fever and loss of consciousness were prolonged. The second CSF analysis on day 9 also did not show improvement. Therefore, ST 80/400 mg 3×/day intravenously was added after consultation with the antimicrobial stewardship team. The synergic effects of the combination of ABPC and ST were not confirmed by the checkerboard method in vitro;9,10 however, we expected the additional effects of ABPC followed by ST rather than either ABPC or ST alone. Her consciousness and fever improved more than one week later (day 16); CSF also improved, but a drug rash appeared that day. Both ABPC and ST were suspended for a week, and MEPM 1.5 g 3×/day was administered intravenously from day 23 after consultation with the antimicrobial stewardship team. One week later (day 30), the planned 21-day antibiotic therapy was completed, and the patient was finally moved to a chronic care hospital for rehabilitation.
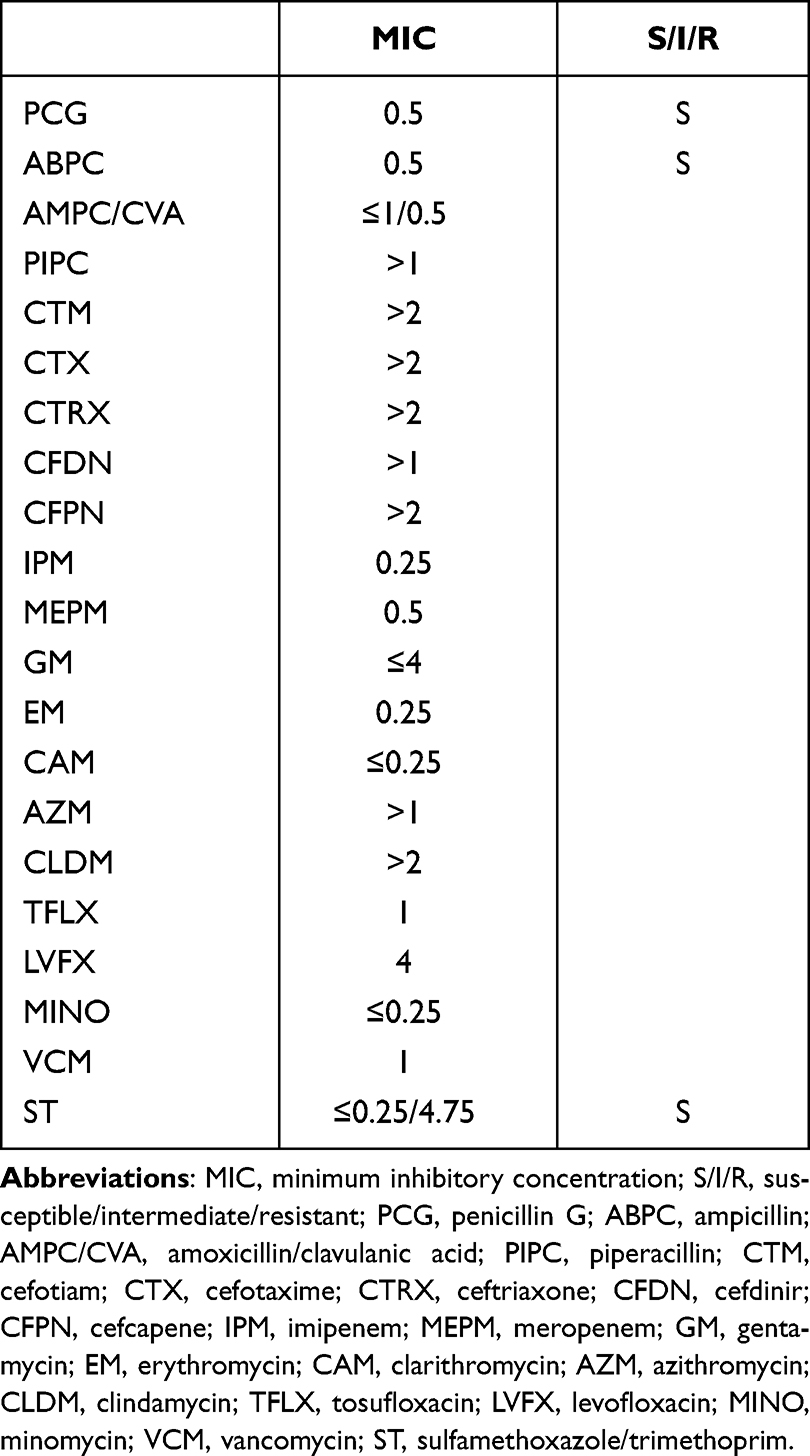 |
Table 2 Antibiotic Susceptibilities for the Isolated Listeria monocytogenes |
Discussion
L. monocytogenes is an important cause of bacteremia and meningitis in both immunocompetent and immunocompromised patients, and it has poor prognosis and high mortality in spite of the available appropriate treatment by antibiotics.11 Although L. monocytogenes is a rare pathogen, it is known that outbreaks caused by eating food, including soft cheeses, celery, sprouts, cantaloupe, and ice cream, contaminated with the bacterium L. monocytogenes have sometimes been reported.12–14 Pregnant women could be more susceptible to listeria infection, similar to newborns, adults aged 65 years or older, and people with weakened immune systems.15
In this report, a patient infected with L. monocytogenes after COVID-19 infection was described. She had been healthy and immunocompetent, but aged and possibly weakened by SARS-CoV-2 infection. Thus, secondary co-infection with L. monocytogenes became severe. SARS-CoV-2 is known to suppress the immunological reaction, including neutrophil functions.16 This case might be due to secondary infection rather than simultaneous co-infection because SARS-CoV-2 Ag values were relatively low, and laboratory data, such as increased WBC and CRP counts suggested bacterial infection at admission. The SARS-CoV-2 might have peaked by admission, and then the secondary bacterial infection became dominant.
Furthermore, it has been suggested that SARS-CoV-2 virus dysregulates the blood–brain barrier (BBB) by modulation of the virus receptors mainly located on vessel endothelium, such as angiotensin-converting enzyme 2 (ACE2) and the transmembrane protease serine subtype 2 (TMPRSS2).17,18 The bacteria could invade the central nervous system via hematogenous spread from the digestive tract.11,15 The patient ate refrigerated green salad and cheese frequently, and she might have been infected by L. monocytogenes after being weakened by the infection with SARS-CoV-2. We should have been aware of the possibility of secondary bacterial infection from the laboratory data including WBC and CRP on day 0. However, there were a lot of COV19 patients and we repeated the treatment protocol with remdesivir without antibiotics for all admitted patients routinely because secondary bacterial infection is usually rare.3,4 We should consider the possibility of secondary bacterial infection in COVID-19 patients in the future.
In addition, L. monocytogenes is notably resistant to cephalosporins, and benzylpenicillin or aminopenicillin alone or in combination with ST or gentamycin has been considered as the standard antibiotic treatment regimen for infections of L. monocytogenes,19 but additional aminoglycoside, clinical failure and increased adverse effects have been reported.20,21 Furthermore, we could not confirm the patient’s hearing ability, which is typically affected by aminoglycosides due to high penetration of the CSF;22 therefore, we used ST in addition to ABPC alone. MEPM was considered and required permission from the antimicrobial stewardship team because it is a broad-spectrum antibiotic; however, it showed good MIC for the isolated L. monocytogenes (Table 2) and was used for the patient.
In the present case, treatment started with ABPC, but her condition and CSF features did not improve (Table 1). Therefore, ST was added after one week of treatment with the ABPC alone, and she showed significant improvement of her mental status, stiff neck, and fever. Additional ST, but not aminoglycoside therapy, was selected, because there was good susceptibility to ST, but susceptibility to aminoglycosides was unclear in vitro, and gentamycin showed relatively high MIC, suggesting clinical resistance (Table 2). L. monocytogenes is a known intracellular pathogen, and has shown natural resistance to older quinolones, fosfomycin, and expanded-spectrum cephalosporins, although ABPC, ST and carbapenems including MEPM have been effective.8 Our measured MIC data also supported these previous data because ABPC, ST, and MEPM showed relatively low MIC, and the cephalosporins, aminoglycosides such as gentamycin, and quinolones including tosufloxacin and levofloxacin showed relatively high MIC (Table 2).
Furthermore, some reports recommended avoiding aminoglycoside use because of increased mortality in the ABPC+aminoglycoside group, compared with the ABPC alone group.20,21 In addition, it was reported that sulfamethoxazole demonstrated variable and generally bacteriostatic activity, but trimethoprim showed bactericidal action that was generally potentiated by sulfamethoxazole even when isolates were resistant to sulfamethoxazole alone against L. monocytogenes.23 Successful results of the treatment of refractory listeria meningitis and bacteremia with ST were also reported in an immunocompetent child.24 These results suggested that ABPC+ST, rather than ABPC+aminoglycoside and ABPC alone, should be used in the treatment of listeria meningitis and bacteremia with refractory and/or severe listeria infections, including COVID-19-associated secondary infection cases. Although ST is known to frequently induce side effects including drug rash, patients can be treated with other antibiotics, such as carbapenems including MEPM.19
There are some limitations in this case report. It is unclear whether SARS-CoV-2 and L. monocytogenes infections occurred simultaneously; however, the SARS-CoV-2 antigens at admission were decreased and symptoms of meningitis and inflammatory markers including WBC and CRP were increased. Therefore, it is suggested that SARS-CoV-2 infection occurred first, and then L. monocytogenes infection occurred secondarily. In addition, we could not determine whether some other candidate antibiotics for L. monocytogenes, including aminoglycosides, were effective or not because there are no standard protocols although we measured the MIC. Further study and analysis will be needed in the future.
Conclusions
The case of an elderly woman with COVID-19 who developed secondary severe meningitis and bacteremia caused by L. monocytogenes was described. She regularly ate green salads made from refrigerated vegetables and soft cheeses, and might have been weakened and immunodepressed by SARS-CoV-2 infection. Treatment with ABPC alone was ineffective, but additional ST improved her physical condition and laboratory data including CSF inflammation, similar to previous reports. However, MEPM was used because of the drug rash induced by ST and/or ABPC. We should be wary of COVID-19-associated secondary bacterial infection in the omicron variant era, and select combination therapy of ABPC with ST, or alternatively carbapenems, for severe listeria infections.
Ethics
This case report and the related studies were approved by the Institutional Review Board of Saitama Medical University International Medical Center as #2022-032 on July 06, 2022, and registered as UMIN000047691. The patient whose specimens were used provided written, informed consent to have her case details and any accompanying images published. The Declaration of Helsinki was also adhered to in this case presentation.
Acknowledgments
The authors would like to thank all medical staff, including physicians, pharmacists, nurses, and medical clinical microbiological technicians for their kind support with COVID-19 management in Saitama Medical University International Medical Center.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ebina S, Seki M, Karaushi H, Shimizu A, Mitsutake K. Antibiotic prescriptions for COVID 19 patients increased during the BA.5 period. World J Med Microbiol. 2023;2(2):11–13.
2. Bahceci I, Yildiz IE, Duran OF, et al. Secondary bacterial infection rates among patients with COVID-19. Cureus. 2022;14(2):e22363. doi:10.7759/cureus.22363
3. Langford BJ, So M, Nachimuthu R, Hua X, Welburn SC, Leptihn S. Secondary bacterial infections in patients with viral pneumonia. Front Med. 2020;5:420.
4. Manohar P, Loh B, Nachimuthu R, Hua X, Welburn SC, Leptihn S. Secondary bacterial infections in patients with viral pneumonia. Front Med. 2020;7:420. doi:10.3389/fmed.2020.00420
5. Mauad T, Hajjar LA, Callegari GD, et al. Lung pathology in fatal novel human influenza A (H1N1) infection. Am J Respir Crit Care Med. 2010;181(1):72–79. doi:10.1164/rccm.200909-1420OC
6. Franch-Llasat D, Bellaubí-Pallarés N, Pérez-Moreno MO, Chamarro-Martí E, García-Rodríguez E, Roche-Campo F. Pneumococcal meningitis secondary to otitis media in two patients with COVID-19 omicron variant. Int J Emerg Med. 2022;15(1):50. doi:10.1186/s12245-022-00448-y
7. Brueggemann AB, Jansen van Rensburg M, Shaw D, et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the invasive respiratory infection surveillance initiative: a prospective analysis of surveillance data. Lancet Digit Health. 2021;3(6):e360–e70. doi:10.1016/S2589-7500(21)00077-7
8. Pagliano P, Ascione T, Boccia G, De Caro F, Esposito S. Listeria monocytogenes meningitis in the elderly: epidemiological, clinical and therapeutic findings. Infez Med. 2016;24(2):105–111.
9. Tateda K, Ishii Y, Matsumoto T, Yamaguchi K. Break-point checkerboard plate’ for screening of appropriate antibiotic combinations against multidrug-resistant Pseudomonas aeruginosa. Scand J Infect Dis. 2006;38(4):268–272. doi:10.1080/00365540500440353
10. Kataoka H, Ida T, Ishii Y, et al. Analysis of the influence of drug resistance factors on the efficacy of combinations of antibiotics for multidrug-resistant Pseudomonas aeruginosa isolated from hospitals located in the suburbs of Kanto area, Japan. J Glob Antimicrob Resist. 2013;1(2):91–96. doi:10.1016/j.jgar.2013.03.005
11. de Noordhout CM, Devleesschauwer B, Angulo FJ, et al. The global burden of listeriosis: a systematic review and meta-analysis. Lancet Infect Dis. 2014;14(11):1073–1082. doi:10.1016/S1473-3099(14)70870-9
12. Jackson K, Gould L, Hunter JC, Kucerova Z, Jackson B. Listeriosis outbreaks associated with soft cheeses, United States, 1998–2014. Emerg Infect Dis. 2018;24(6):1116–1118. doi:10.3201/eid2406.171051
13. McCollum JT, Cronquist AB, Silk BJ, et al. Multistate outbreak of listeriosis associated with cantaloupe. N Engl J Med. 2013;369(10):944–953. doi:10.1056/NEJMoa1215837
14. Marcus R, Hurd S, Mank L, et al. Chicken salad as the source of a case of Listeria monocytogenes infection in Connecticut. J Food Prot. 2009;72(12):2602–2606. doi:10.4315/0362-028X-72.12.2602
15. Swaminathan B, Gerner-Smidt P. The epidemiology of human listeriosis. Microbes Infect. 2007;9(10):1236–1243. doi:10.1016/j.micinf.2007.05.011
16. Veras FP, Pontelli MC, Silva CM, et al. SARS-CoV-2-triggered neutrophil extracellular traps mediate COVID-19 pathology. J Exp Med. 2020;217(12):e20201129. doi:10.1084/jem.20201129
17. Krasemann S, Haferkamp U, Pfefferle S, et al. The blood-brain barrier is dysregulated in COVID-19 and serves as a CNS entry route for SARS-CoV-2. Stem Cell Rep. 2022;17(2):307–320. doi:10.1016/j.stemcr.2021.12.011
18. Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet. 2020;395(10234):1417–1418. doi:10.1016/S0140-6736(20)30937-5
19. Temple ME, Nahata MC. Treatment of listeriosis. Ann Pharmacother. 2000;34(5):656–661. doi:10.1345/aph.19315
20. Mitjà O, Pigrau C, Ruiz I, et al. Predictors of mortality and impact of aminoglycosides on outcome in listeriosis in a retrospective cohort study. J Antimicrob Chemother. 2009;64(2):416–423. doi:10.1093/jac/dkp180
21. Amaya-Villar R, García-Cabrera E, Sulleiro-Igual E, et al. Three-year multicenter surveillance of community-acquired Listeria monocytogenes meningitis in adults. BMC Infect Dis. 2010;11(10):324. doi:10.1186/1471-2334-10-324
22. Cunha CB, Cunha BA. Antibiotic Essentials.
23. Winslow D, Pankey GA. In vitro activities of trimethoprim and sulfamethoxazole against Listeria monocytogenes. Antimicrob Agents Chemother. 1982;22(1):1116–1118. doi:10.1128/AAC.22.1.51
24. Polat M, Kara SS, Tapısız A, Derinöz O, Çağlar K, Tezer H. Successful treatment of refractory listeria meningitis and bacteremia with trimethoprim-sulfamethoxazole in an immunocompetent child. Turk J Pediatr. 2016;58(2):220–222. doi:10.24953/turkjped.2016.02.017
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.