Back to Journals » International Journal of General Medicine » Volume 16
Could the Systemic Immune Inflammation Index Predict Diagnosis, Recovery Time, Hypothyroidism, and Recurrence Rates in Subacute Thyroiditis?
Received 1 February 2023
Accepted for publication 12 April 2023
Published 18 April 2023 Volume 2023:16 Pages 1375—1382
DOI https://doi.org/10.2147/IJGM.S406724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Serpil Çiftel,1 Zeynep Tüzün2
1Department of Endocrinology, Erzurum Training and Research Hospital, Erzurum, Türkiye; 2Department of Internal Medicine, Rheumatology, Atatürk University, Faculty of Medicine, Erzurum, Türkiye
Correspondence: Serpil Çiftel, Erzurum Training and Research Hospital, Kurt Deresi Caddesi:1 APT C-4, Erzurum, 25100, Türkiye, Tel +905054009897, Fax +90442 4323103, Email [email protected]
Purpose: Subacute thyroiditis (SAT) is a non-infectious inflammatory disease of the thyroid. The Systemic Immune-Inflammation Index (SII), also known as an easy economical marker, correlates with the severity of inflammatory responses. We aimed to evaluate the clinical significance of the SII and to compare it to other inflammatory markers in terms of diagnosis, recovery time, and recurrence of SAT.
Patients and Methods: The current non-interventional observational prospective study was performed at Outpatient Department of Endocrinology, Erzurum Training and Research Hospital. Sixty-nine patients with SAT and fifty-nine healthy individuals in total were enrolled in our study. The follow-up period was 6– 12 months for all patients regarding treatment response, recurrence, and hypothyroidism.
Results: The SII level was found to be significantly higher at the time of diagnosis in the SAT group compared to the control group (p=0.000). There was a significant positive correlation between the SII and SAT recovery time (p=0.000), particularly in patients receiving methyl prednisolone treatment (p=0.002). SII was not found to be significantly associated with hypothyroidism and recurrence in patients with SAT (p=0.261, p=0.568). However, compared to the ones without recurrence, thyroid stimulating hormone (TSH) and erythrocyte sedimentation rate levels at the time of diagnosis were found to be higher in those patients with recurrence (p=0.035, p=0.046).
Conclusion: SII is a low-cost, widely available, universal indicator of inflammatory processes in SAT. It could provide many benefits in the follow-up process and the selection of aggressive anti-inflammatory treatment by estimating recovery time. SII, as a practical biomarker, may be a new diagnostic and prognostic tool for SAT.
Keywords: subacute thyroiditis, methyl prednisolone, systemic immune-inflammation index, recurrence, hypothyroidism
Introduction
Subacute thyroiditis (SAT) is a self-limiting inflammatory thyroid gland disease and is characterized by a sudden onset of neck pain, fever, and thyrotoxicosis caused by follicular epithelial destruction.1,2 Females between the ages of 30 and 50 are particularly vulnerable. In recent years, significant progress has been demonstrated in SAT pathogenesis, epidemiology, and clinical courses. It is a known fact that, inflammation plays a significant role in the development of SAT. Pathogenesis of SAT depends on genetic background and triggering factors, such as several viral infections, vaccines, and some drugs.3 The disease severity may reach its peak within three to four days and continues with fluctuating intensity for three to six weeks. Pain lasts for a week to a few months. The American Thyroid Association guidelines recommend corticosteroids in moderate/severe SAT. In our clinical practice, either non-steroidal anti-inflammatory agents (NSAIDs) or 16–32 mg methylprednisolone (MPS) treatment has been administered depending on the clinician’s preference. Clinical diagnosis can be made based on history, physical examination, biochemical evidence of transient thyrotoxicosis, and reduced radio-iodine uptake on radioactive iodine uptake scan.4 A very high (>50 mm/h) erythrocyte sedimentation rate (ESR) is an additional distinctive diagnostic feature in subacute thyroiditis. C-reactive protein (CRP) may also be elevated in many cases. Thyroid ultrasonography demonstrates heterogeneously hypoechoic and suppressed vascular patterns.5
A complete blood cell count provides information on the number and morphology of various cells. Neutrophils, a part of the innate immune system, have been shown to increase and release inflammation mediators in inflammatory conditions such as SAT. However, the mechanism of lymphocytopenia in patients with SAT remains unclear. Virus infection of T cells6 and elevated cortisol levels7 may be potential factors leading to lymphopenia. Platelets are known to have regulatory effects on both the innate and adaptive immune systems and that the various cytokines they secrete in collaboration with neutrophils cause tissue destruction as a result of the activation of more and more neutrophils and platelets. It is involved in the pathogenesis of numerous acute and chronic inflammatory and autoimmune diseases.8,9
There is a growing interest in the discovery of new biomarkers as indicators of inflammation. Several new leukocyte-based inflammatory indicators, including the Systemic Immune Inflammation Index (SII), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), and neutrophil-to-lymphocyte ratio (NLR), have recently been used as diagnostic and prognostic predictors of certain diseases. These indicators have also been investigated as biomarkers for inflammatory and rheumatic diseases. SII, which was first developed in 2014, is considered to be more predictive compared to NLR and PLR.10 Besides, it has been shown to be associated with oncological outcomes in several types of cancer.11,12 It is also believed that SII may reflect the balance between host immune and inflammatory conditions.
Considering the research on this matter, our study may be the first one demonstrating the role of SII in the diagnosis and estimating the recovery time of SAT considering treatment.
The primary purpose of the present study is to evaluate the clinical significance of SII regarding recovery time, hypothyroidism, and recurrence rate in patients with SAT and to compare it to other inflammatory markers. Therefore, clinicians may have an idea about the most effective therapeutic choice and its duration by estimating recovery time.
Materials and Methods
Study Population and the Relevant Factors
Sixty-nine SAT patients (52 females and 17 males) with no comorbidities and 59 healthy volunteers (43 females and 16 males) admitted to the Outpatient Department of Endocrinology and Metabolism Diseases, Erzurum Training and Research Hospital between November 2021 and June 2022 were involved in this study. SAT was confirmed by typical symptoms, physical examination, increased ESR, elevated free T4 (fT4), decreased TSH, decreased radioactive iodine uptake and presence of hypoechoic areas with blurred margins and decreased vascularization on thyroid ultrasound in all the patients. Considering age and gender factors, there was almost no difference between the patient and control groups. The patients were followed up on 6–12 months. Anti-inflammatory medication (indomethacin or 16–32 mg MPS, depending on their clinical condition) was started for all patients. The dose titration and duration of treatment could be changed according to the patient’s clinical symptoms. The number of the patients administered indomethacin and MPS was 31 and 38, respectively. Patients below 18 years, pregnant women, patients with chronic diseases such as heart disease, renal failure, hematological diseases, cancer, or rheumatic diseases, and patients receiving medical treatment that may influence the blood system during the preceding three months were excluded from the study.
Study Methods
Biochemical and hematologic tests were studied. Complete blood count parameters – white blood cells, platelet count, neutrophil, lymphocyte, and monocyte count – were performed with a Sysmex XN 9000 brand autoanalyzer. Other biochemistry parameters were studied with a Cobas C 701 brand biochemistry autoanalyzer (Roche, Germany). TSH and fT4 were measured by the chemiluminescent immunoassay method (Beckman Coulter, DXI 800, Brea, CA, USA). Reference ranges were defined as fT4: 0.89–1.76 ng/dl, TSH: 0.55–4.78 mIU/L, ESR: 0–20 mm/h, and CRP: 0–5 mg/L.
Novel inflammation parameters were calculated using the formulas NLR = neutrophils / lymphocytes, PLR = platelets / lymphocytes, SII (neuthrophils × platelets) / lymphocytes, SLR (ESR − lymphocyte rate) = ESR / lymphocytes and CLR (CRP − lymphocyte rate) = CRP / lymphocytes.
Theoretically, CRP level increases more rapidly than ESR in early-stage inflammatory diseases and begins to decrease more quickly than ESR. Therefore, we defined the time when the CRP level decreased to normal and the clinical symptoms of patients resolved as the recovery time.
Statistical Analysis
SPSS 22.0 (SPSS Inc., Chicago, IL, USA) statistical software was used for all analyses. The variables were investigated through visual and analytic methods (Kolmogorov–Smirnov/Shapiro–Wilk test) to determine whether they were normally distributed or not. Student’s T-Test and the Mann–Whitney U-Test were used to compare normally and non-normally distributed variables, respectively. Descriptive analyses were presented using means and standard deviations for normally distributed variables, whereas medians and minimum-maximum were used for non-normally distributed variables. The chi-square test was used to compare categorical variables. On the other hand, the Spearman correlation coefficient was used. P value less than 0.05 was deemed statistically significant.
Results
Comparison of the Study Patients’ Demographic, Clinical, and Laboratory Parameters with Those of the Control Group
Table 1 displays the age and gender distributions of the patient and control groups. There was no significant difference in genders or mean ages between the two groups (p>0.05). Neutrophils, monocytes, ESR, CRP, SII, PLR, SLR, CLR, and NLR were found to be significantly higher at the time of diagnosis in the patient group compared to the control group, while LMR was found to be lower. The median recovery period in the study group was thirty-five days (Table 2).
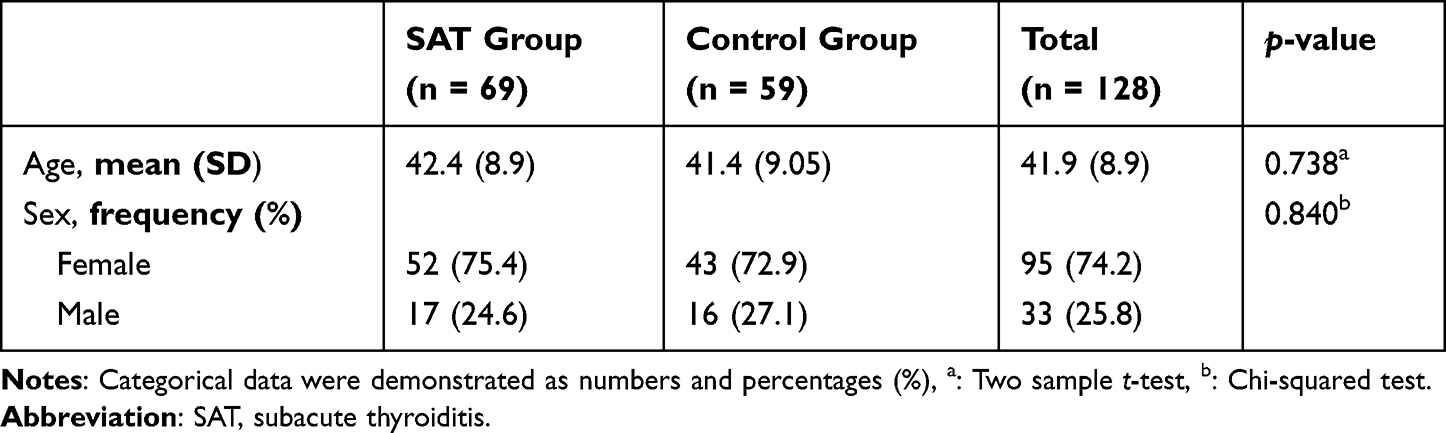 |
Table 1 The Distribution of Gender and the Means and Standard Deviations of the Participants’Age |
 |
Table 2 The Medians, Minimum, and Maximum Ranges of Parameters of the SAT Patients at the Time of Diagnosis and Healthy Controls |
According to the results of Spearman correlation analysis, a statistically significant positive correlation was detected in SII levels, compared to other inflammation markers like SLR. On the other hand, as expected, there was a statistically significant negative correlation between SII and LMR. Furthermore, our statistical analysis revealed a strong positive correlation between SII and SAT recovery time and a weak-moderate positive correlation between PLR and recovery time (Table 3). According to the correlation analysis between the recovery time and SII based upon the medication administered in the treatment of SAT, a strong positive correlation was detected only in the group given MPS, not in the group given NSAIDs (Table 4). Also, SII levels at the time of diagnosis were already higher in patients receiving MPS (Table 5).
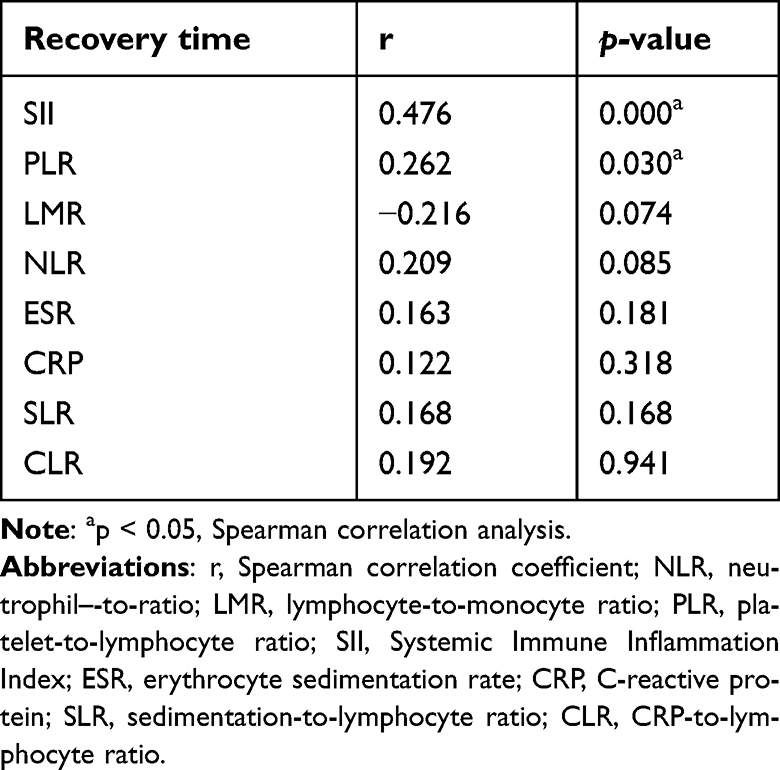 |
Table 3 Recovery Time Correlations with Other Inflammatory Markers in Patients with Subacute Thyroiditis Using Spearman Correlation Analysis |
 |
Table 4 Correlation Analyses Between Systemic Immune Inflammation Index and Recovery Time in Terms of Medical Treatment in Patient Group |
 |
Table 5 Comparisons of Some Parameters According to the Type of SAT Treatment |
There was no correlation between SII level and ESR, CRP, fT4, or age factor. Hypothyroidism developed in 12 out of 69 patients (17%) during 6–12 months follow-up period. No significant correlation was detected between the development of hypothyroidism and other parameters such as SII, NLR, LMR, PLR, fT4, CRP/lymphocyte, ESR/lymphocyte, recovery time, and gender factor. Over the course of the follow-up period, only eight (11%) patients in the MPS group had recurrence. No recurrence was observed in the NSAID group (Table 5).
SII levels did not differ between patients developing and not developing recurrence. TSH and ESR levels at the time of diagnosis were higher in patients with recurrence, compared to those without recurrence (Table 6). Considering gender factor, the recurrence rate was 11.8% for males and 11.5% for females.
 |
Table 6 Comparisons of Laboratory Test Results and Recovery Time of the Patients with and Without Recurrence |
Discussion
Subacute thyroiditis is an inflammatory disease with a high inflammatory load that can progress to long-term severe clinical symptoms and significant comorbidity. As can be seen in our study, females between the ages of 30 and 40 are exposed to subacute thyroiditis more frequently, compared to males (a ratio of 3 to 5:1). This inflammatory disease may be diagnosed with medical history and clinical, laboratory, and imaging findings. In the early phase of SAT, almost all patients may have hyperthyroidism and elevated acute-phase reactants. ESR is one of the most widely used laboratory tools for detecting inflammatory syndromes like SAT. However, it is important to take into account all factors that may influence ESR values such as age and gender factors, the lifestyles of patients, and common metabolic abnormalities.13 Occasionally, value discrepancies may be observed between CRP and ESR due to their kinetic differences. To illustrate, CRP level increases faster than ESR level and begins to decrease more quickly. However, whether one over the other or one over two tests combined has a higher predictive value remains debatable.14 Therefore, studies investigating additional parameters to guide diagnosis and prognosis of subacute thyroiditis are ongoing. Although the diagnostic role of ESR and CRP was determined in patients with SAT pursuant to other studies, we found in our study that these parameters were not clinically effective for estimating the healing process.
Some blood cell-derived indexes, including SII, NLR, PLR, and LMR, have been proposed as biomarkers for various inflammatory and non-inflammatory diseases. As a result, we felt compelled to investigate the blood cell-derived indexes, considering the severity of inflammation, duration of the disease, and treatment in patients with SAT. Although there are many studies on various hemogram-related ratios of subacute thyroiditis in the literature, the number of the studies on subacute thyroiditis and SII is limited.15,16 In these studies, as in our study, SII level has elevated significantly in the patient group with SAT when compared to the control group. However, the current study differs from the other studies in question owing to being a prospective observational study. Apart from this, whether blood cell-based inflammatory markers, particularly SII, are associated with recovery time is one of the most significant research subjects, considering the scope of our study. We found that SII may have prognostic value in predicting the healing process as well as its diagnostic role.
ESR, CRP, SII, PLR, and NLR levels in this study were found to be higher in the patient group, whereas the LMR level was found to be lower. SII and other inflammation markers such as CLR and SLR showed a statistically significant positive correlation. All these parameters might be used to assist acute-phase reactants in detecting inflammatory burden at the time of diagnosis. In the study of Taşkaldiran et al, NLR and PLR levels were found to be higher in patients with SAT than in the control group, similar to our study.17 We also revealed that patients with higher SII levels had a significantly longer recovery period. We know that the types of treatment have a strong confounding effect on the correlation between SII and recovery time. For this reason, we also studied on the correlation between the recovery time and SII based on the treatment modalities performed. We determined that SII levels affected the recovery time with a strong positive correlation in the patients receiving MPS, not NSAID. Not surprisingly, SII levels were found to be higher in patients receiving MPS due to the presence of milder clinical conditions in patients treated with NSAIDs.
In clinical practice, it is important to decide the most effective and appropriate treatment in the acute phase of the disease through the combination of all parameters such as medical history, clinical, laboratory, and imaging findings, and the severity of the disease, which accurately assess the inflammatory burden of the disease in patients with SAT suffering from severe pain and hyperthyroidism symptoms in order not to cause loss of time.
Thyroid inflammation and hyperthyroidism are usually transient, lasting two to eight weeks. Euthyroidism, hypothyroidism, and finally restoration of normal thyroid functions are experienced following hyperthyroidism. Some patients may skip the hyperthyroid phase entirely and proceed directly from the hypothyroid phase to the recovery phase, which is diagnosed clinically in general. However, 5% to 15% of patients progress to persistent thypothyroidism, which requires levothyroxine treatment.18,19 As mentioned above, hypothyroidism is generally transient, but it may nevertheless be permanent. In our study, hypothyroidism developed in 17% of the patients, pursuant to the study results in the literature. However, no correlation was found between the development of hypothyroidism and hematological parameters. The relatively short follow-up period of only 6–12 months, which is critical for progression to relapse or hypothyroidism in our study, may have affected this correlation.
In our study, patients receiving MPS had a higher SAT recurrence rate (21%), and the total recurrence rate was 11% consistent with the literature.20 In addition, TSH levels at the time of diagnosis were higher in the recurrence group, while TSH levels were lower in the non-recurrence group in accordance with the literature.21,22 Since the recurrence rate of patients with clinically severe hyperthyroidism is lower, the duration of the treatment administered may be shorter, which reduces the possibility of side effects when compared to a longer treatment period.
Conclusion
SII is a widely available, low-cost, universal, non-invasive, and easy-to-reproduce method for detecting inflammation on SAT. As a result, predicting the prognosis and the duration of the disease in the SAT acute phase could provide benefits in the follow-up process, as well as in the selection of aggressive anti-inflammatory treatment. Although SAT is a benign, self-limiting disease, the severe inflammatory burden of the disease in the acute phase may be exhausting for both patients and physicians. According to the results of our study, estimating the duration of the recovery period by considering the level of SII at the time of the diagnosis has importance. As a high SII level indicates a longer recovery period, deciding whether an aggressive treatment with a higher anti-inflammatory effect as the initial treatment would prevent loss of time. On the other hand, a low SII level indicates a shorter recovery period, which means patients may complete the treatment process without suffering any complications and side effects of a more aggressive treatment. Additionally, we found that higher pre-treatment TSH and ESR values may be a risk factor for recurrence. In clinical practice, this result may help the clinician choose an appropriate treatment without increasing recurrence risk, which is already high in the case of high TSH and ESR levels. In addition, shortening the duration of treatment may be considered in patients at low risk of recurrence.
With all these clinical data, multicenter studies involving a large number of patients and years of follow-up are required for SAT.
ESR and CRP levels play a crucial role in the diagnosis of SAT; however, SII level may also be a parameter in order to give clinicians an idea not only on the diagnosis of the disease but also on its prognosis. As a practical biomarker, SII level may be a new diagnostic and prognostic tool for SAT. According to our point of view, more comprehensive studies with a long follow-up period and a large number of patients need to be conducted to contribute to the research on SAT in the literature.
Abbreviations
SAT, Subacute thyroiditis; SII, Systemic Immune-Inflammation Index; TSH, thyroid stimulating hormone; NSAIDs, non-steroidal anti-inflammatory agents; MPS, methylprednisolone; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; SLR, sedimentation-to-lymphocyte ratio; CLR, CRP-to-lymphocyte ratio.
Data Sharing Statement
The datasets analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Erzurum Training and Research Hospital Ethics Committee (Decision KAEK 2022/07-72 Date: 06.06.2022). Written informed consent was obtained from all participants.
Acknowledgments
We would like to thank the Society of Endocrinology and Metabolism of Türkiye for their valuable contributions to the research process by providing data and to the translation process.
Funding
There is no specific funding related to this research.
Disclosure
The authors report no conflicts of interest.
References
1. Zhao N, Wang S, Cui XJ, et al. Two-years prospective follow-up study of subacute thyroiditis. Front Endocrinol. 2020;11:47. doi:10.3389/fendo.2020.00047
2. Görges J, Ulrich J, Keck C, Müller-Wieland D, Diederich S, Janssen OE. Long-term outcome of subacute thyroiditis. Exp Clin Endocrinol Diabetes. 2020;128:703–708. doi:10.1055/a-0998-8035
3. Stasiak M, Lewiński A. New aspects in the pathogenesis and management of subacute thyroiditis. Rev Endocr Metab Disord. 2021;22:1027–1039. doi:10.1007/s11154-021-09648-y
4. Intenzo CM, Park CH, Kim SM, Capuzzi DM, Cohen SN, Green P. Clinical, laboratory, and scintigraphic manifestations of subacute and chronic thyroiditis. Clin Nucl Med. 1993;18(4):302–306. doi:10.1097/00003072-199304000-00007
5. Vural Ç, Paksoy N, Gök ND, Yazal K. Subacute granulomatous (De Quervain’s) thyroiditis: fine-needle aspiration cytology and ultrasonographic characteristics of 21 cases. Cytojournal. 2015;12:9. doi:10.4103/1742-6413.157479
6. Fois AG, Paliogiannis P, Scano V, et al. The Systemic Inflammation Index on admission predicts in-hospital mortality in COVID-19 patients. Molecules. 2020;25:5725. doi:10.3390/molecules25235725
7. Calapkulu M, Sencar ME, Sakiz D, et al. The prognostic and diagnostic use of hematological parameters in subacute thyroiditis patients. Endocrine. 2020;68:138–143. doi:10.1007/s12020-019-02163-w
8. Wang J, Arase H. Regulation of immune responses by neutrophils. Ann N Y Acad Sci. 2014;1319:66–81. doi:10.1111/nyas.12445
9. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
10. Fest J, Ruiter R, Ikram MA, Voortman T, Van Eijck CHJ, Stricker BH. Reference values for white blood-cell-based inflammatory markers in the Rotterdam Study: a population-based prospective cohort study. Sci Rep. 2018;8(1):10566. doi:10.1038/s41598-018-28646-w
11. Yang R, Chang Q, Meng X, Gao N, Wang W. Prognostic value of Systemic immune-inflammation index in cancer: a meta-analysis. J Cancer. 2018;9(18):3295–3302. doi:10.7150/jca.25691
12. Zhong JH, Huang DH, Chen ZY. Prognostic role of systemic immune-inflammation index in solid tumors: a systematic review and meta-analysis. Oncotarget. 2017;8(43):75381–75388. doi:10.18632/oncotarget.18856
13. Alende-Castro V, Alonso-Sampedro M, Vazquez-Temprano N, et al. Factors influencing erythrocyte sedimentation rate in adults: new evidence for an old test. Medicine. 2019;98(34):e16816. doi:10.1097/MD.0000000000016816
14. Feldman M, Aziz B, Kang GN, Opondo MA, Belz RK, Sellers C. C-reactive protein and erythrocyte sedimentation rate discordance: frequency and causes in adults. Transl Res. 2013;161(1):37–43. doi:10.1016/j.trsl.2012.07.006
15. Keskin Ç, Dilekçi EN, Üç ZA, Cengiz D, Duran C. Can the systemic immune-inflammation index be used as a novel diagnostic tool in the diagnosis of subacute thyroiditis? Biomark Med. 2022;16(10):791–797. doi:10.2217/bmm-2022-0095
16. He P, Yang H, Lai Q, et al. The diagnostic value of blood cell-derived indexes in subacute thyroiditis patients with thyrotoxicosis: a retrospective study. Ann Transl Med. 2022;10(6):322. doi:10.21037/atm-22-719
17. Taşkaldiran I, Omma T, Önder ÇE, et al. Neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, and platelet-to-lymphocyte ratio in different etiological causes of thyrotoxicosis. Turk J Med Sci. 2019;49(6):1687–1692. doi:10.3906/sag-1901-116
18. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;348(26):2646–2655. doi:10.1056/NEJMra021194
19. Ross DS, Burch HB, Cooper DS, et al. American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343–1421. doi:10.1089/thy.2016.0229
20. Sencar ME, Calapkulu M, Sakiz D, et al. An evaluation of the results of the steroid and non-steroidal anti-inflammatory drug treatments in subacute thyroiditis in relation to persistent hypothyroidism and recurrence. Sci Rep. 2019;9(1):16899. doi:10.1038/s41598-019-53475-w
21. Stasiak M, Tymoniuk B, Stasiak B, Lewiński A. The risk of recurrence of subacute thyroiditis is HLA-dependent. Int J Mol Sci. 2019;20(5):1089. doi:10.3390/ijms20051089
22. Bahadir ÇT, Yilmaz M, Kiliçkan E. Factors affecting recurrence in subacute granulomatous thyroiditis. Arch Endocrinol Metab. 2022;66(3):286–294. doi:10.20945/2359-3997000000473
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Role of HBx Protein in Diseases Beyond the Liver
Ai L, Liu QQ, Li Y, Wang Y, Zhang HM
Infection and Drug Resistance 2023, 16:3225-3232
Published Date: 23 May 2023
Effectiveness of Infliximab in Patients with Complex Regional Pain Syndrome: A Case Series
van den Berg C, Dirckx M, Huygen FJPM, Tiemensma J
Journal of Pain Research 2023, 16:1915-1926
Published Date: 6 June 2023
Quercetin: A Flavonoid with Potential for Treating Acute Lung Injury

Huang M, Liu X, Ren Y, Huang Q, Shi Y, Yuan P, Chen M
Drug Design, Development and Therapy 2024, 18:5709-5728
Published Date: 6 December 2024
Deciphering the Role of CD36 in Gestational Diabetes Mellitus: Linking Fatty Acid Metabolism and Inflammation in Disease Pathogenesis
Huang L, Zhang T, Zhu Y, Lai X, Tao H, Xing Y, Li Z
Journal of Inflammation Research 2025, 18:1575-1588
Published Date: 4 February 2025
Inflammation in Obstructive Sleep Apnea: A Global Bibliometric Perspective
Fan H, Niu H, Zhao B, Gao X
Nature and Science of Sleep 2025, 17:2275-2295
Published Date: 22 September 2025