Back to Journals » Clinical Ophthalmology » Volume 20
Cost-Utility Analysis of Immediate Sequential and Delayed Sequential Bilateral Cataract Surgery in a Middle-Income Country
Authors Nguyen CN ![]() , Somkijrungroj T, Pongsachareonnont PF
, Somkijrungroj T, Pongsachareonnont PF ![]() , Tulvatana W
, Tulvatana W ![]()
Received 29 January 2026
Accepted for publication 8 April 2026
Published 18 April 2026 Volume 2026:20 599816
DOI https://doi.org/10.2147/OPTH.S599816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Cong Ngoc Nguyen,1– 3 Thanapong Somkijrungroj,2,4 Pear Ferreira Pongsachareonnont,4,5 Wasee Tulvatana2,6
1Clinical Sciences (International Program), Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 2Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Department of Ophthalmology, Faculty of Medicine, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam; 4Center of Excellence in Retina, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 5Department of Ophthalmology, Faculty of Health Sciences, Queen’s University, Kingston, ON, Canada; 6Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand
Correspondence: Wasee Tulvatana, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, 16th Floor, Rattanawittayaphat Building, No. 1873, Rama IV Road, Pathumwan, Bangkok, 10330, Thailand, Tel +6622564000 ext 61632, Email [email protected]
Purpose: To evaluate the cost-utility of immediate sequential versus delayed sequential bilateral cataract surgery (ISBCS vs DSBCS) in a real-world setting at a Thai government hospital.
Patients and Methods: In this prospective cohort study, eligible patients undergoing ISBCS or DSBCS followed a standardized surgical and postoperative protocol. In ISBCS, the second eye was treated as a new case with full instrument replacement. DSBCS followed the same procedure with a surgeon-determined interval between surgeries. Cost-utility analysis was conducted from a societal perspective, with cost-effectiveness defined as an incremental cost-effectiveness ratio (ICER) below Thailand’s willingness-to-pay threshold (160,000 THB per quality-adjusted life-year [~US$4600]). Sensitivity analyses (one-way and bootstrapping) tested the robustness of the results.
Results: Among 99 enrolled patients (45 ISBCS, 54 DSBCS), 89 were included in the analysis (44 ISBCS, 45 DSBCS) after excluding eight DSBCS patients and one ISBCS patient based on the study’s exclusion criteria. Compared to DSBCS, the ISBCS group was younger but similar in other baseline characteristics. No intraoperative complications occurred, and postoperative complication rates were comparable between groups. The cost-utility analysis, using a 3-month time horizon, identified ISBCS as the dominant strategy, with a cost saving of 3335 THB (~US$100) per patient and a slightly higher effectiveness. These findings were confirmed by sensitivity analyses.
Conclusion: ISBCS offers substantial cost savings, comparable safety, and a slight quality-of-life advantage over DSBCS, making it a cost-effective option for bilateral cataract surgery in Thailand.
Keywords: bilateral cataract surgery, economic evaluation, cost-utility analysis, ISBCS, DSBCS
Introduction
Cataracts are the leading cause of preventable blindness, affecting more than 65 million people globally. The estimated cost associated with the unmet need for cataract surgery is approximately US$7.0 billion.1 With an aging population, the demand for cataract treatment is expected to increase significantly, placing a substantial burden on healthcare systems and economic resources worldwide.2
Traditionally, bilateral cataracts are treated with delayed sequential bilateral cataract surgery (DSBCS), where each eye is operated on separately. However, waiting time for the second eye operation in DSBCS can lead to challenges such as anisometropia, reduced binocular vision, and an increased risk of falls.3–5 Moreover, frequent postoperative hospital visits may increase patient time and financial burdens, which could negatively impact satisfaction and quality of life.6–9 By operating both eyes in the same session, immediate sequential bilateral cataract surgery (ISBCS) may address these challenges. Several studies have shown promising benefits of this approach, including enhanced visual outcomes, faster recovery, fewer hospital visits, and reduced patient and healthcare provider costs.4,10–12
Prior research from developed countries has consistently shown the cost advantages of ISBCS compared to DSBCS from various perspectives.13–16 Notably, the recent BICAT-NL trial reported per-patient savings of EUR 388 in healthcare costs and EUR 403 from a societal perspective, further confirming the high cost-effectiveness of ISBCS across a wide range of willingness-to-pay thresholds.3
However, the applicability of these findings to low- and middle-income countries remains unclear due to significant differences in socioeconomic conditions and healthcare systems. Therefore, localized data is crucial for informing policymakers. This study aims to address this gap by providing a cost-utility analysis of ISBCS and DSBCS in a real-world setting at a Thai government hospital. The results will offer a more accurate evaluation of ISBCS’s effectiveness and feasibility within the specific context of Thailand and other developing countries.
Patients and Methods
The study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University (IRB number 0042/67), and was conducted in accordance with the principles outlined in the Declaration of Helsinki. All participants received a comprehensive explanation of the study and provided written informed consent prior to their enrollment.
Setting
This prospective cohort study was conducted at King Chulalongkorn Memorial Hospital (KCMH), a government referral tertiary hospital with medium-priced healthcare services. Therefore, the cost-effectiveness analysis results from KCMH are broadly applicable to the Thai healthcare system.
Patients undergoing phacoemulsification at the Department of Ophthalmology, KCMH, were consecutively enrolled between April and August 2024. Inclusion criteria were bilateral senile cataracts, age ≥18 years, and planned phacoemulsification. Exclusion criteria included cognitive or behavioral impairments, complicated cataracts (eg, traumatic, pathological, or with lens subluxation/dislocation), surgery gaps >12 weeks, prior intraocular surgery, need for complex procedures or general anesthesia, or refusal to participate.
All patients underwent a standardized surgical protocol, including a comprehensive preoperative assessment (slit-lamp examination, fundoscopy, fundus exam, and optical biometry), phacoemulsification under topical anesthesia via clear corneal incision, and implantation of a foldable intraocular lens (IOL). In ISBCS cases, the second eye was treated as a new case, with full replacement of instruments, drapes, and gowns. For DSBCS, both eyes followed the same procedure, with the interval determined by the surgeon’s schedule. Postoperative care included antibiotic and anti-inflammatory eye drops (separate bottles for ISBCS), with follow-up visits at 1 day, 1 week, 1 month, and 3 months, adjusted as needed.
Data Analysis
Data were analyzed using R Statistics for Mac OS (R version 4.4.1, Foundation for Statistical Computing). We used a t-test (mean ± SD) for normally distributed continuous variables and a Mann–Whitney U-test (median and IQR) for skewed data. Categorical variables were analyzed using frequency and Chi-square tests. A p-value < 0.05 was considered statistically significant.
We conducted a cost-utility analysis of ISBCS and DSBCS from a societal perspective, using a 3-month time horizon, which is considered a standard clinical recovery period of cataract surgery,17 adequate to capture common acute postoperative complications and assess early-stage quality-of-life differences between the two groups. The costs included direct medical costs (eg, examinations, surgery, medications), direct non-medical costs (eg, travel, food, caregiver fees), and indirect costs (eg, productivity loss based on Bangkok’s average daily wage). All costs are reported in Thai Baht (THB), with an exchange rate of approximately US$1 = 35 THB as of 2025.
Utility scores were measured using the Visual Function Questionnaire-Utility Index (VFQ-UI), which converts responses from 6 specific items (items 6, 11, 14, 18, 20, 25) of the National Eye Institute Visual Function Questionnaire-25 into utility values.18 Details of cost, utility calculations and assumptions are provided in Supplement 1.
Cost-effectiveness was defined as the incremental cost-effectiveness ratio (ICER) falling below the Thai willingness-to-pay (WTP) threshold of 160,000 THB per quality-adjusted life year (QALY) gained (~US$4600).19 To test the robustness of the results, one-way sensitivity analyses were performed by varying key parameters within their 95% confidence intervals and beyond (stress testing). The uncertainty of the ICER was further assessed using non-parametric bootstrapping with 10,000 iterations. The resulting ICERs were plotted on a cost-effectiveness plane, where the vertical axis represented incremental costs, and the horizontal axis represented incremental QALYs of ISBCS compared to DSBCS. Additionally, a cost-effectiveness acceptability curve (CEAC) was constructed to illustrate the probability of ISBCS being cost-effective at different WTP thresholds.20
Sample Size
Sample size calculation was based on Glick’s formula for cost-effectiveness analysis.21 The standard deviation parameters for cost and effectiveness of interventions were retrieved from the BICAT-NL study.3 A clinically and economically meaningful difference in costs was defined as the equivalent of a 5-day wage for manual labor in Bangkok, estimated at 353 THB per day (Ministry of Labour, Thailand),22 totaling 1765 THB. A minimum of 30 participants per group was required to ensure statistical significance, with α = 0.05 and β = 0.2.
Results
A total of 99 participants were enrolled, 45 in ISBCS and 54 in DSBCS group. Eight participants from DSBCS group were excluded due to the interval between surgeries exceeding 12 weeks. One participant from the ISBCS group was excluded due to ICU admission caused by a severe systemic disease unrelated to the cataract surgery (acute hemodialysis), preventing the patient from attending ophthalmology OPD for month-3 follow-up. As a result, a total of 89 participants were included in the final analysis (45 in DSBCS and 44 in ISBCS). Notably, no intraoperative complications were reported.
The ISBCS group was younger, but both groups were comparable across other baseline characteristics, including sex, education level, and home-to-hospital distance (Table 1).
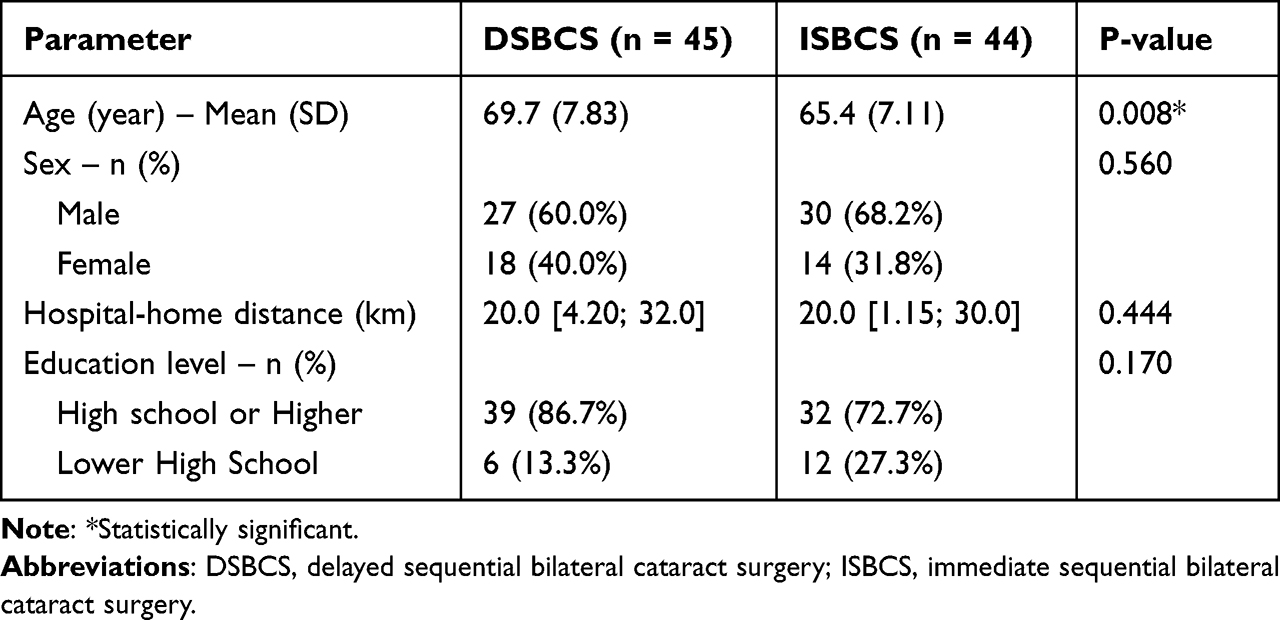 |
Table 1 Patient Demographics |
Postoperative complications did not differ significantly between the ISBCS and DSBCS groups (Supplement 2). The most common event was transient ocular hypertension, occurring in approximately one-fifth of patients in both groups. A single case of cystoid macular edema was reported in the DSBCS group and resolved fully with topical anti-inflammatory therapy. Given the overall low and comparable complication rates, these events were not analyzed separately in the cost-utility model; all cases were included in the overall cohort analysis for cost and QALY estimation.
Table 2 showed that the total cost for ISBCS was significantly lower than DSBCS (27,728 THB vs 31,063 THB, p < 0.001). This reduction was primarily driven by lower costs across components, including direct medical costs, food costs, travel costs, and indirect costs. While there were no statistically significant differences in utility values at any time points, the ISBCS group had a significantly higher QALY score (0.230 vs 0.225, p = 0.020), suggesting a modest quality-of-life benefit.
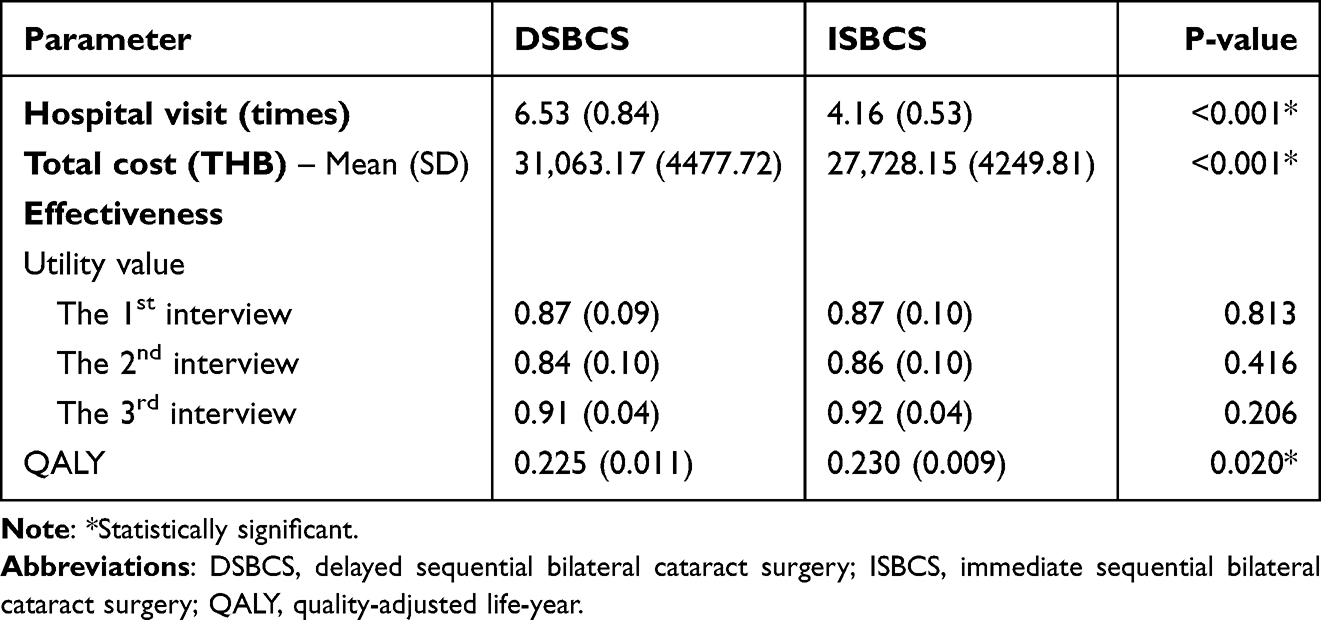 |
Table 2 Outcomes Related to Cost-Effectiveness Analysis for DSBCS and ISBCS |
The base-case cost-utility analysis in Table 3 revealed that ISBCS had a lower total cost (incremental cost saving of 3335 THB) and a higher effectiveness (incremental effectiveness of 0.005 QALY) compared to DSBCS, making it a dominant strategy with an ICER of −667,000 THB.
 |
Table 3 Incremental Cost-Effectiveness Ratio and Net Monetary Benefit of the Base Case |
The results of the one-way sensitivity analysis, presented in tornado diagrams (Figure 1), showed that the ICER was most sensitive to changes in QALY values, particularly for DSBCS. This highlights the substantial effect that minor changes in QALY can have when the difference in effectiveness is minimal. While cost parameters such as travel, indirect, and OPD costs also influenced the ICER, their effect was to a lesser extent. In all tested scenarios, all ICER values remained negative and well below the Thai WTP threshold of 160,000 THB per QALY, indicating that ISBCS remained cost-saving and economically dominant.
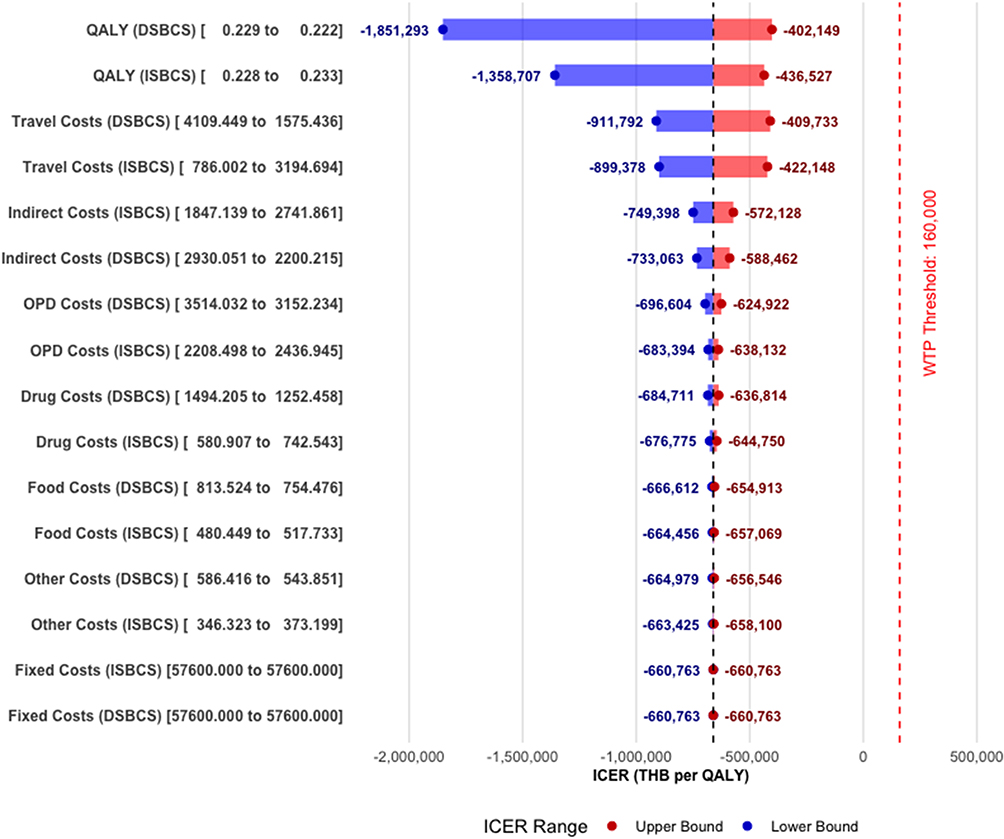 |
Figure 1 Tornado diagram of one-way sensitivity analysis. |
Additionally, to assess the influence of parameters beyond their 95% confidence intervals, a manual one-way sensitivity analysis of the ISBCS group was conducted and is presented in Table 4. It indicated that ISBCS remained cost-effective even with a 100% increase in individual cost components, including drug, outpatient department visit, travel, food, and indirect costs. Furthermore, ISBCS maintained cost-effectiveness when the second-eye reimbursement was reduced by 25% or even 50%. However, a 75% reduction in reimbursement rendered it non-cost-effective. Due to the modest difference in QALY gain between the two surgical approaches, the results were highly sensitive to changes in QALY. A decrease of just 5% was enough to render ISBCS less effective than DSBCS, making it unable to be considered an alternative.
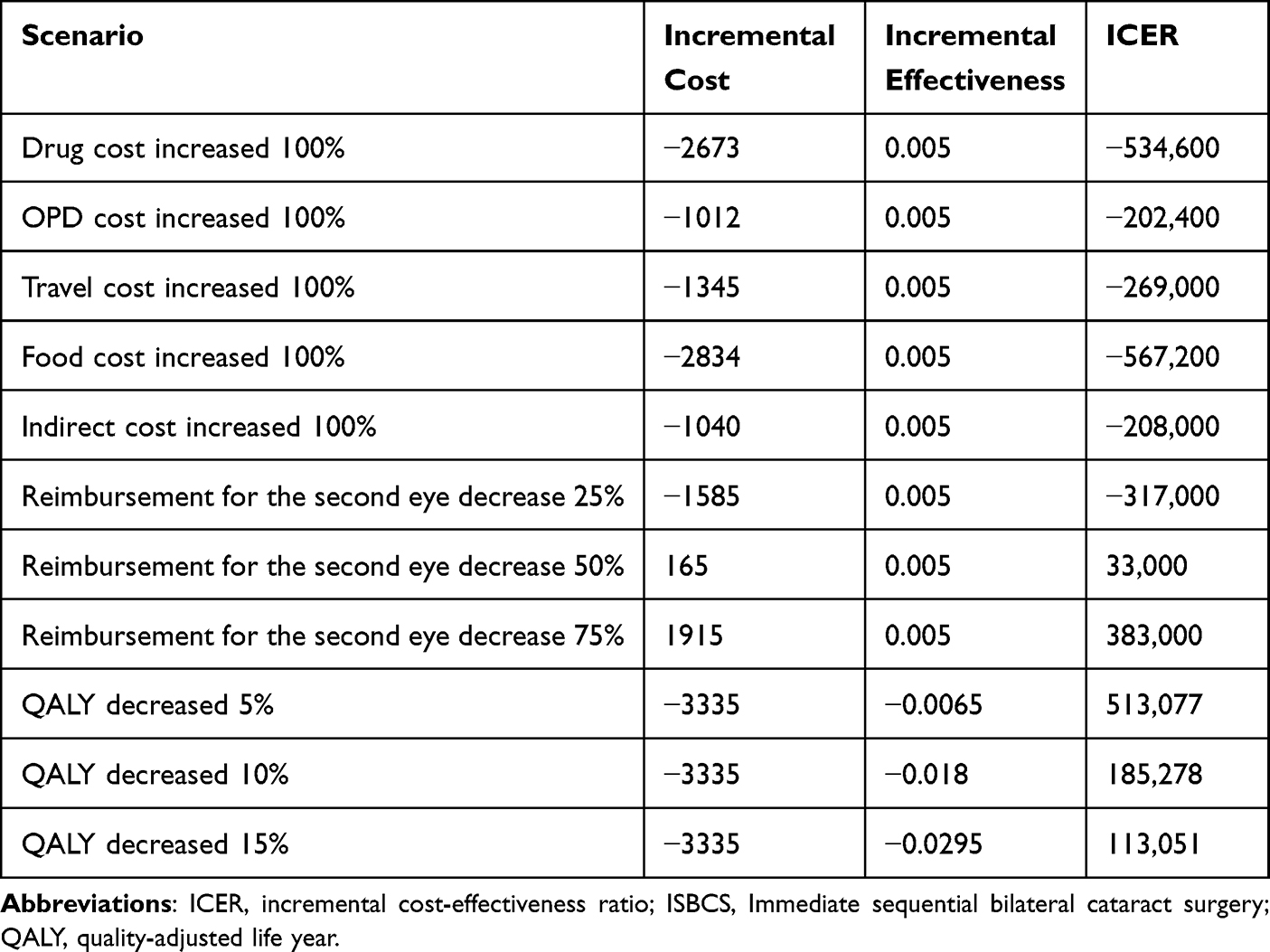 |
Table 4 Stress Testing the Cost-Effectiveness Result of the ISBCS Group |
The ICER scatterplot illustrates the distribution of 10,000 bootstrapped iterations, evaluating the incremental cost and the incremental effectiveness (ΔQALY) of ISBCS compared to DSBCS (Figure 2). Most iterations fall in the lower-right quadrant, demonstrating that ISBCS is both less costly and more effective than DSBCS, which establishes ISBCS as the dominant strategy.
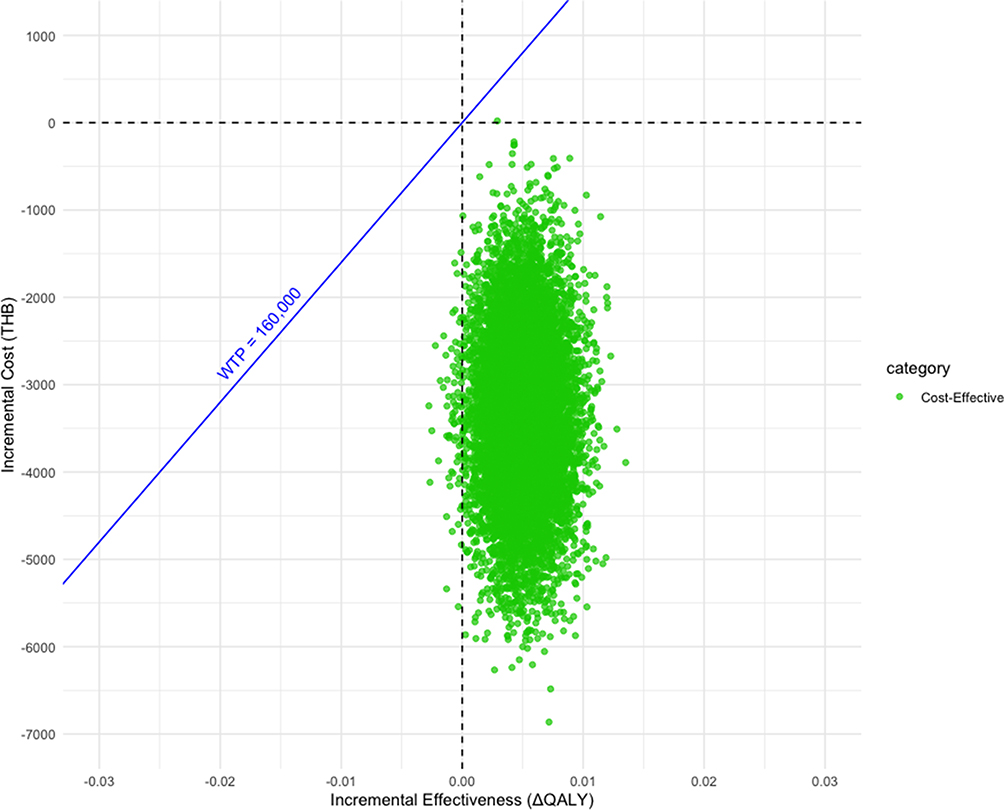 |
Figure 2 Incremental cost-effectiveness ratio plane of cost-utility analysis. |
The Cost-Effectiveness Acceptability Curve (CEAC) illustrates the probability of each approach being cost-effective at different WTP thresholds (Figure 3). ISBCS remains 100% cost-effective across all WTP values, while DSBCS consistently holds a 0% probability. At the WTP threshold of 160,000 THB per QALY in Thailand (dashed line), ISBCS remains the preferred strategy with a 100% probability of cost-effectiveness.
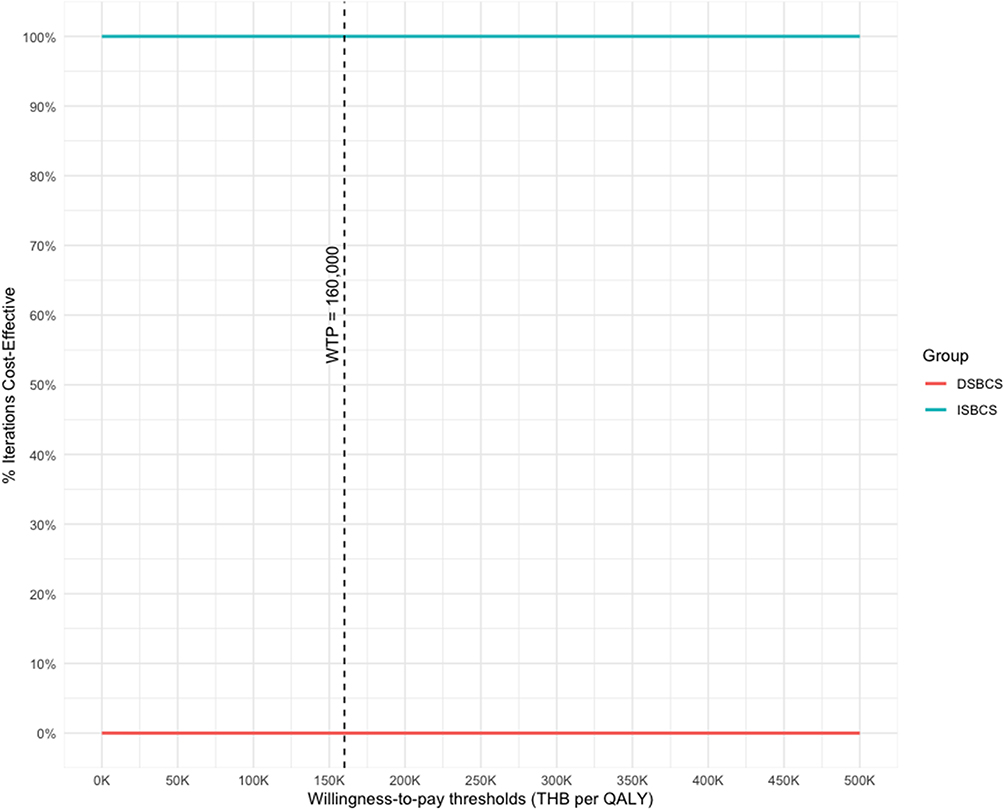 |
Figure 3 Cost-effectiveness acceptability curve of cost-utility analysis. |
Discussion
This study was designed to evaluate the cost-utility of ISBCS compared to DSBCS within a Thai healthcare context. Our findings indicate that ISBCS offers significant cost savings, comparable clinical outcomes, and a slight quality-of-life advantage, positioning it as a potentially preferable approach for bilateral cataract surgery.
The incidence of postoperative complications, such as ocular hypertension, corneal edema, and cystoid macular edema, showed no statistically significant differences between the ISBCS and DSBCS groups, aligning with findings from prior studies.3,23 Notably, no cases of endophthalmitis were observed in either group. While this study lacked the power to reliably assess rare outcomes such as endophthalmitis, the absence of cases in both groups suggests a comparable safety profile between ISBCS and DSBCS, supporting the feasibility of ISBCS as a safe alternative.
ISBCS demonstrated significantly lower total costs than DSBCS, with savings of 3335 THB (~US$100) from a societal perspective. These cost advantages stem from reductions in direct medical costs (eg, OPD visits), travel expenses, food costs, and indirect costs (eg, lost productivity). At KCMH, fixed costs - such as surgery, anesthesia, and surgeon fees - were standardized for each eye in both groups, so the cost difference was largely explained by fewer hospital visits with ISBCS (4.16 vs 6.53 for DSBCS, p < 0.001). The cost saving in our study was smaller than those reported in developed countries.3,14–16 This difference is likely attributable to several factors: firstly, lower direct non-medical costs in Thailand, such as those for OPD visits, patient travel, and food. Secondly, our calculation of productivity loss was based on the average wage for manual labor in Bangkok. This wage is relatively low compared to broader occupational averages or those in higher-income countries, which would contribute to a more conservative estimate of indirect cost savings in our analysis. In addition, we also observed that ISBCS shortened total operating-room (OR) time by about 6 minutes per patient for completing both eyes.24 We did not assign a monetary value to OR time in Thailand because a local cost-per-minute estimate is not available; however, in settings where OR time is costed, this time saving could translate into additional institutional savings (for example, cataract surgery OR time has been valued at approximately US$11.24 per minute in a U.S. setting).25
Extrapolating these findings to a national level, approximately 300,000 eyes undergo cataract surgery annually in Thailand, with around 150,000 eyes treated under the Universal Coverage Scheme (97% of these cases attributed to senile cataracts),26 and a similar number under other schemes, based on expert estimates. We assumed 300,000 eyes were operated on across 150,000 patients. If the adoption rate of ISBCS were 25%, 50%, and 75%, the cost-saving at 3335 THB per patient could result in annual savings of roughly 125, 250, and 375 million THB, respectively. This significant economic benefit highlights ISBCS’s potential to improve healthcare efficiency, particularly in resource-constrained settings.
At 3 months post-operation, patient-reported outcomes were generally comparable between the ISBCS and DSBCS groups. However, ISBCS showed a modest quality-of-life benefit with a higher QALY score (0.230 vs 0.225, p = 0.020). This finding highlights the sensitivity of vision-specific measures like VFQ-UI in capturing subtle improvements in visual function, particularly during the period between the 1-week and 3-month postoperative visits, when full recovery is expected, making it appropriate for evaluating cataract surgery outcomes.
Despite the modest difference in QALY gain, which made the results highly sensitive to minor changes, the cost-effectiveness of ISBCS was confirmed as robust through both one-way and bootstrapping sensitivity analyses across most scenarios. Furthermore, the cost-effectiveness acceptability curve demonstrated a 100% probability of ISBCS being cost-effective at any WTP threshold.
However, despite its cost-effectiveness, financial barriers may impede ISBCS adoption. In the United States, for instance, surgeons and surgery centers often receive only 50% reimbursement for the second eye in ISBCS,27 with most financial benefits accruing to third-party payers.28 This irrationality creates a disincentive for surgeons and providers. In contrast, Thailand’s healthcare insurance fully reimburses both eyes, ensuring that economic benefits are equitably distributed among stakeholders, making financial concerns less of a barrier.
This study has several limitations. First, as an observational cohort study, there is potential for selection bias, and the younger age observed in the ISBCS group may represent a confounding factor. However, the age difference was relatively modest (65.4 vs 69.7), and baseline utility scores were comparable between groups, suggesting similar preoperative health status. Therefore, although statistically significant, this difference is unlikely to have a meaningful clinical impact on short-term recovery or patient-reported utility and substantially influenced our finding. Second, the 3-month follow-up period may not fully capture long-term outcomes, such as sustained quality-of-life improvements or rare complications like endophthalmitis. A longer follow-up (eg, 12 months) could provide a more comprehensive assessment of cost-effectiveness. Third, postoperative refractive outcomes, particularly after second-eye surgery, were not specifically assessed. This may limit the ability to evaluate the potential advantage of DSBCS in refining IOL power for the second eye, as well as to detect subtle differences in visual acuity between groups. Fourth, the lack of standardization in IOL types may have influenced patient outcomes, as multifocal IOLs could potentially enhance quality of life compared to monofocal IOLs. Finally, the single-center design and small sample size (89 participants) limit the generalizability of our findings to other settings with differing cost structures or patient demographics.
In conclusion, ISBCS offers substantial cost savings, comparable safety, and a slight quality-of-life advantage over DSBCS, making it a cost-effective option for bilateral cataract surgery in Thailand. Its adoption could optimize resource use, particularly in high-volume or resource-constrained healthcare systems. However, successful implementation requires careful patient selection, robust postoperative care, and supportive reimbursement policies. Future research should prioritize larger, multicenter trials with extended follow-up periods to validate these findings and assess long-term outcomes.
Acknowledgments
We would like to thank Miss Yuda Chongpison, Ph.D., M.S., from Center of Excellence in Biostatistics, Research Affairs, Faculty of Medicine, Chulalongkorn University, for her valuable statistical consultation and support throughout this study.
We also appreciate the contributions of our Research Assistant team from the Department of Ophthalmology, Chulalongkorn University: Miss Bubpha Puangmalee, Miss Jirawan Saothongthong, and Mr. Nattapach Prajansakunee.
We would like to declare the use of ChatGPT 5.2 for grammar checking and language refinement during the preparation of this manuscript.
We thank Can Tho University of Medicine and Pharmacy for the support in the preparation of this manuscript.
Funding
Supported by Global Health Research Promotion Grant from the School of Global Health, Faculty of Medicine, Chulalongkorn University, and Ratchadapiseksomphot Fund (Grant number MDCU GA67/074), Faculty of Medicine, Chulalongkorn University.
Disclosure
The authors report no conflicts of interest in this work.
Part of the study results were presented at the Royal College of Ophthalmologists of Thailand (RCOPT) Annual Meeting 2025.
References
1. World Health Organization. World report on vision. Geneva: World Health Organization; 2019.
2. Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(9):e888–10. doi:10.1016/S2214-109X(17)30293-0
3. Spekreijse L, Simons R, Winkens B, et al. Safety, effectiveness, and cost-effectiveness of immediate versus delayed sequential bilateral cataract surgery in the Netherlands (BICAT-NL study): a multicentre, non-inferiority, randomised controlled trial. Lancet. 2023;401(10392):1951–1962. doi:10.1016/S0140-6736(23)00525-1
4. Nassiri N, Nassiri N, Sadeghi Yarandi SH, et al. Immediate vs delayed sequential cataract surgery: a comparative study. Eye. 2009;23(1):89–95. doi:10.1038/sj.eye.6702989
5. Gimbel HV, Dardzhikova AA. Consequences of waiting for cataract surgery. Curr Opin Ophthalmol. 2011;22(1):28–30. doi:10.1097/ICU.0b013e328341425d
6. Busbee BG, Brown MM, Brown GC, et al. Cost-utility analysis of cataract surgery in the second eye. Ophthalmology. 2003;110(12):2310–2317. doi:10.1016/S0161-6420(03)00796-6
7. Sach TH, Foss AJE, Gregson RM, et al. Second-eye cataract surgery in elderly women: a cost-utility analysis conducted alongside a randomized controlled trial. Eye. 2010;24(2):276–283. doi:10.1038/eye.2009.112
8. Frampton G, Harris P, Cooper K, et al. The clinical effectiveness and cost-effectiveness of second-eye cataract surgery: a systematic review and economic evaluation. Health Technol Assess. 2014;18(68):1–205, v–vi. doi:10.3310/hta18680
9. Brown MM, Brown GC, Sharma S, et al. Quality of life associated with unilateral and bilateral good vision. Ophthalmology. 2001;108(4):643–647; discussion 647–648. doi:10.1016/S0161-6420(00)00635-7
10. Arshinoff SA, Strube YN, Yagev R. Simultaneous bilateral cataract surgery. J Cataract Refract Surg. 2003;29(7):1281–1291. doi:10.1016/S0886-3350(03)00052-X
11. Lundström M, Albrecht S, Nilsson M, et al. Benefit to patients of bilateral same-day cataract extraction: randomized clinical study. J Cataract Refract Surg. 2006;32(5):826–830. doi:10.1016/j.jcrs.2006.01.075
12. Serrano-Aguilar P, Ramallo-Fariña Y, Cabrera-Hernández JM, et al. Immediately sequential versus delayed sequential bilateral cataract surgery: safety and effectiveness. J Cataract Refract Surg. 2012;38(10):1734–1742. doi:10.1016/j.jcrs.2012.05.024
13. Johansson BA, Lundh BL. Bilateral same day phacoemulsification: 220 Cases retrospectively reviewed. Br J Ophthalmol. 2003;87(3):285–290. doi:10.1136/bjo.87.3.285
14. Lundström M, Albrecht S, Roos P. Immediate versus delayed sequential bilateral cataract surgery: an analysis of costs and patient value. Acta Ophthalmol. 2009;87(1):33–38. doi:10.1111/j.1755-3768.2008.01343.x
15. Leivo T, Sarikkola AU, Uusitalo RJ, et al. Simultaneous bilateral cataract surgery: economic analysis; Helsinki simultaneous bilateral cataract surgery study report 2. J Cataract Refract Surg. 2011;37(6):1003–1008. doi:10.1016/j.jcrs.2010.12.050
16. Neel ST. A cost-minimization analysis comparing immediate sequential cataract surgery and delayed sequential cataract surgery from the payer, patient, and societal perspectives in the United States. JAMA Ophthalmol. 2014;132(11):1282–1288. doi:10.1001/jamaophthalmol.2014.2074
17. Mahmud I, Kelley T, Stowell C, et al. A Proposed minimum standard set of outcome measures for cataract surgery. JAMA Ophthalmol. 2015;133(11):1247–1252. doi:10.1001/jamaophthalmol.2015.2810
18. Kowalski JW, Rentz AM, Walt JG, et al. Rasch analysis in the development of a simplified version of the National Eye Institute Visual-Function Questionnaire-25 for utility estimation. Qual Life Res. 2012;21(2):323–334. doi:10.1007/s11136-011-9938-z
19. Nimdet K, Ngorsuraches S. Willingness-To-pay for life-saving treatments in Thailand: a discrete choice experiment. Value Health. 2017;20(9):A682. doi:10.1016/j.jval.2017.08.1710
20. Fenwick E, Claxton K, Sculpher M. Representing uncertainty: the role of cost-effectiveness acceptability curves. Health Econ. 2001;10(8):779–787. doi:10.1002/hec.635
21. Glick HA. Sample size and power for cost-effectiveness analysis (part 1). Pharmacoeconomics. 2011;29(3):189–198. doi:10.2165/11585070-000000000-00000
22. Ministry of Labour. National Wage Committee’s notification on minimum wage rate. 2023. Available from: https://www.mol.go.th/en/minimum-wage.
23. Aiello F, Gallo Afflitto G, Leviste K, et al. Immediate sequential vs delayed sequential bilateral cataract surgery: systematic review and meta-analysis. J Cataract Refract Surg. 2023;49(11):1168–1179. doi:10.1097/j.jcrs.0000000000001230
24. Nguyen CN, Somkijrungroj T, Pongsachareonnont PF, et al. Comparison of operating room utilization time between immediate and delayed sequential bilateral cataract surgery at a tertiary hospital in Thailand. Clin Ophthalmol. 2025;19:4831–4840. doi:10.2147/OPTH.S570958
25. Taravella MJ, Davidson R, Erlanger M, et al. Time and cost of teaching cataract surgery. J Cataract Refract Surg. 2014;40(2):212–216. doi:10.1016/j.jcrs.2013.07.045
26. Yospaiboon Y, Yospaiboon K, Ratanapakorn T, et al. Management of cataract in the Thai population. J Med Assoc Thai. 2012;95(Suppl 7):S177–181.
27. Arshinoff SA, Chen SH. Simultaneous bilateral cataract surgery: financial differences among nations and jurisdictions. J Cataract Refract Surg. 2006;32(8):1355–1360. doi:10.1016/j.jcrs.2006.02.064
28. Masket S. Same day bilateral cataract surgery-who benefits? Ophthalmology. 2021;128(1):11–12. doi:10.1016/j.ophtha.2020.08.017
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Operating Room Utilization Time Between Immediate and Delayed Sequential Bilateral Cataract Surgery at a Tertiary Hospital in Thailand
Nguyen CN, Somkijrungroj T, Pongsachareonnont PF, Tulvatana W
Clinical Ophthalmology 2025, 19:4831-4840
Published Date: 19 December 2025