Back to Journals » Clinical Ophthalmology » Volume 19
Comparison of Operating Room Utilization Time Between Immediate and Delayed Sequential Bilateral Cataract Surgery at a Tertiary Hospital in Thailand
Authors Nguyen CN ![]() , Somkijrungroj T, Pongsachareonnont PF
, Somkijrungroj T, Pongsachareonnont PF ![]() , Tulvatana W
, Tulvatana W ![]()
Received 29 September 2025
Accepted for publication 10 December 2025
Published 19 December 2025 Volume 2025:19 Pages 4831—4840
DOI https://doi.org/10.2147/OPTH.S570958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Cong Ngoc Nguyen,1– 3,* Thanapong Somkijrungroj,2,4,* Pear Ferreira Pongsachareonnont,4,5,* Wasee Tulvatana2,6,*
1Clinical Sciences (International Program), Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 2Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Department of Ophthalmology, Faculty of Medicine, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam; 4Center of Excellence in Retina, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 5Department of Ophthalmology, Faculty of Health Sciences, Queen’s University, Kingston, ON, Canada; 6Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand
*These authors contributed equally to this work
Correspondence: Wasee Tulvatana, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, No. 1873, Rama IV Road, Pathumwan, Bangkok, 10330, Thailand, Tel +6622564000 ext 61632, Email [email protected]
Purpose: To compare operating room (OR) utilization time between immediate sequential bilateral cataract surgery (ISBCS) and delayed sequential bilateral cataract surgery (DSBCS) at a tertiary care hospital in Thailand.
Patients and Methods: This prospective observational study was conducted at King Chulalongkorn Memorial Hospital, Bangkok, Thailand. From April to September 2024, a total of 99 patients were recruited (45 ISBCS, 54 DSBCS). Nine DSBCS patients were excluded due to surgery intervals exceeding 12 weeks, resulting in 90 patients (45 per group) for analysis. Inverse probability of treatment weighting (IPTW) was applied to balance baseline covariates. Weighted linear regression models were used to estimate treatment effects on total OR time and its components, including preparation, draping, surgical, exit, and turnover times.
Results: Baseline characteristics showed ISBCS group had more surgeries performed by younger surgeons (p = 0.014) and more frequent use of toric (p = 0.034) and preloaded IOLs (p = 0.004). Average OR utilization time was 55.8 minutes (SD = 12.0) for ISBCS and 60.0 minutes (SD = 12.9) for DSBCS. After IPTW adjustment, ISBCS reduced total OR time by 5.81 minutes (95% CI 0.87 to 10.76) compared to DSBCS. This reduction remained consistent across multivariate models (5.86– 5.99 minutes). Time savings were primarily attributed to shorter surgical time (p = 0.006), exit time (p < 0.001), and turnover times (p = 0.002). Surgeon experience had the most significant impact on OR time.
Conclusion: ISBCS reduced total OR utilization time by approximately 6 minutes (10%) per patient compared to DSBCS, enhancing operational efficiency and potentially increasing surgical capacity.
Keywords: bilateral cataract surgery, operating room utilization time, ISBCS, DSBCS
Introduction
Cataract extraction is the most commonly performed elective surgery globally, with over 20 million procedures conducted annually.1 With an aging global population, the demand for cataract surgery is steadily increasing, placing substantial pressure on healthcare systems, particularly in terms of financial and operating room (OR) resources.2,3 The OR is a critical department, generating more than two-thirds of the overall revenue for the hospital.4–6 However, it is also resource-intensive; for instance, the cost of cataract surgery has been estimated at US$11.24 per minute spent in the OR from the institution’s perspective.7 Even a one-minute reduction per procedure, when scaled across millions of annual cases, could result in significant cost savings at both national and international levels.
Although cataract surgery is exceptionally cost-effective, its growing frequency emphasizes the need to optimize OR efficiency to manage costs, enhance productivity, and maintain high standards of care. The growing demand for cataract surgery has also resulted in longer surgical waiting lists, which pose significant challenges for patients. Patients waiting over 6 months for surgery experience significantly more vision loss, reduced quality of life, and a higher incidence of falls compared to those with wait times under 6 weeks.8 These delays highlight the urgency of improving surgical access and efficiency to mitigate the adverse effects on patients’ health and well-being.
Cataract surgery can be performed using 2 approaches: delayed sequential bilateral cataract surgery (DSBCS), where each eye is operated on in separate sessions, and immediate sequential bilateral cataract surgery (ISBCS), where both eyes are treated in a single session. ISBCS has been suggested as a more efficient approach for enhancing visual recovery, reducing hospital visits, and lowering healthcare costs for institutions and patients.9–12 Additionally, ISBCS can improve operating room efficiency by reducing patient turnover time, with reports indicating potential productivity increases of up to 15% within one surgical day and average case time reductions ranging from 6.48 to 6.62 minutes across various studies.13–17 These advantages make ISBCS a promising strategy for addressing the challenges of rising demand and resource constraints.
Despite these encouraging findings, gaps in the existing literature suggest a need for further investigation. Some studies have relied on simulated data to estimate ISBCS time savings, which might not fully capture the realities of actual practice.14 Others have not accounted for patients’ baseline characteristics, which could introduce confounding factors and potentially influence surgical duration.15,17 Furthermore, variations in surgical workflows, infrastructure, and regional healthcare systems may make it challenging to apply these findings to diverse settings, such as Thailand. To address these limitations and contribute to the existing evidence, this study aimed to compare OR utilization time between ISBCS and DSBCS in a high-volume tertiary hospital in Thailand to validate these findings within a middle-income setting.
Patients and Methods
The study was approved by the Institutional Review Board of Chulalongkorn University following the principles of the Declaration of Helsinki (IRB No. 0042/67, COA No. 0481/2024). All participants were fully informed about the research and provided written consent prior to the start of the study.
Study Design
This prospective observational study was conducted from April to August 2024 at King Chulalongkorn Memorial Hospital, Bangkok, Thailand. Eligible participants were enrolled consecutively to achieve the required sample size. Inclusion criteria were patients who had bilateral senile cataracts, aged ≥18 years, and were scheduled for phacoemulsification at King Chulalongkorn Memorial Hospital. Exclusion criteria comprised patients with cognitive or behavioral impairments, complicated cataracts (eg, traumatic or pathological cataracts, lens subluxation/dislocation), intervals between surgeries exceeding 12 weeks (for DSBCS patients), a history of prior intraocular surgery, the need for complex procedures or general anesthesia, or those who declined to participate.
Setting
All patients underwent uncomplicated phacoemulsification performed by surgeons with at least four years of experience as official ophthalmologists. While operating room staff at King Chulalongkorn Memorial Hospital (KCMH) routinely records surgical times, for this study, a dedicated OR staff member documented specific operating room milestones for each case, as described in the following section. The procedures were conducted under topical anesthesia using the same phacoemulsification system (Alcon Centurion®, Alcon Surgical, Texas, USA), with a temporal clear corneal incision and foldable intraocular lens implantation. For ISBCS cases, the second eye surgery was performed under strict protocols as if starting a new case: all surgical instruments and drapes were replaced, the surgical team re-scrubbed and changed into new gowns.
Operating room milestones (Figure 1) for each case were documented in hh: mm format by an OR staff member, who was informed of the importance of accurately recording each milestone but unaware of the research question to minimize potential bias and ensure precision in data collection. These milestones included “wheel-in” (patient entry into the OR), “surgical field sterilization” (start of povidone-iodine 10% application), “incision” (corneal incision), “eye shield/eye pad placement”, and “wheel-out” (patient exit from the OR). Based on these time points, the total OR time was segmented into 5 intervals: preparation time, draping time, surgical time, exit time, and turnover time.
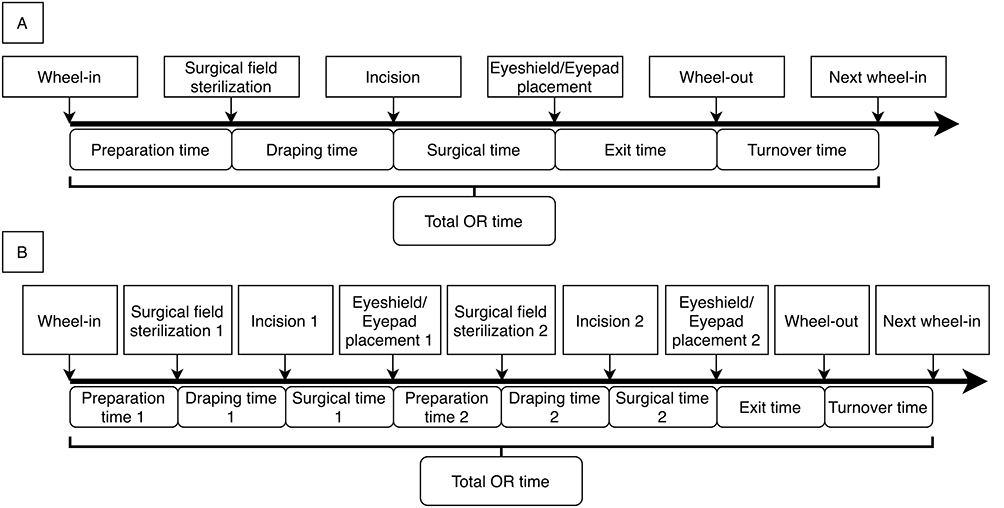 |
Figure 1 Milestones and durations of OR time for DSBCS (A) and ISBCS (B) Group. Wheel-in = patient entry into the OR; Surgical field sterilization = initiation of 10% povidone-iodine application; Incision = start of corneal incision; Eyeshield/eye pad placement = completion of surgery, marked by placement of an eyeshield or eye pad on the operated eye; Wheel-out = patient exit from the OR. In (B), numbers 1 and 2 denote the first and second eyes, respectively. |
The primary outcome was total OR utilization time to complete surgery for one patient. For DSBCS patients, it was calculated as the sum of the OR times for both eyes, with each eye’s time measured from “wheel-in” to “next wheel-in” of its respective session (Figure 1A). For ISBCS, the total OR time was measured from “wheel-in” to the “next wheel-in” within a single session (Figure 1B).
Demographic and clinical variables were collected to characterize patients and surgical factors in the DSBCS and ISBCS groups: Age (years) was categorized as ≥70 or <70 to balance groups; sex (male/female); BMI; education level (lower than high school / high school or higher); the pre-operative risk score (PORS), a validated numerical score derived from the New Zealand Cataract Risk Stratification System, assigns points based on the severity of ocular and systemic risk factors (eg, small pupil, pseudoexfoliation, dense cataract, age, ocular axial length, etc)., with higher scores indicating greater perioperative complication risk,18 was assessed separately for each eye and then averaged across both eyes; ocular axial length; surgeon’s experience (years since becoming a certified ophthalmologist) was grouped as ≤16 or >16 years based on patient volume to balance DSBCS and ISBCS; use of toric IOLs and preload IOLs were classified as no use, use in one eye, or use in both eyes.
Data Analysis
Data were analyzed using R for Mac OS (R version 4.4.1, Foundation for Statistical Computing). Continuous variables were analyzed using a t-test (reported as mean ± SD) for normally distributed data or a Mann–Whitney U-test (reported as median and IQR) for skewed data. Categorical variables were analyzed using frequency counts and the Chi-square test. A P-value < 0.05 was considered statistically significant.
As participants were enrolled consecutively, potential differences in baseline characteristics between ISBCS and DSBCS groups may have influenced treatment assignment and outcomes. To minimize this bias, we used propensity score analysis, a common method in observational studies, to adjust for baseline imbalances and mimic randomization.19 A propensity score is the probability of an individual receiving a treatment based on observed baseline variables.20 This method combines all covariates into a single score, which is particularly helpful when managing numerous covariates.21 Among the available propensity score methods, we applied inverse probability of treatment weighting (IPTW), a weighting approach that uses propensity scores to balance baseline characteristics between the ISBCS and DSBCS groups, because it preserves effective sample size (ESS) better than other methods and is particularly suitable for small sample studies.19
Propensity scores were estimated using logistic regression. Following purposeful selection, the most parsimonious model included six covariates: age, education level, surgeon’s experience, PORS, and toric and preloaded IOLs. However, based on clinical practice and literature reviews, we expanded the model to include additional potential confounders: age, sex,22 BMI,22 education level, PORS,18 ocular axial length, surgeon’s experience,22,23 and the use of toric or preloaded IOLs.24–26 This final model balanced clinical relevance and statistical considerations.
Average treatment effect (ATE) weights were computed following the estimation of the propensity score. Balance between the two groups was assessed using a standardized mean difference (SMD), with an SMD < 0.1 considered optimal.19,27 For small sample sizes, an SMD of <0.2 was deemed acceptable.28,29 To manage extreme weights and preserve effective sample size, weight truncation was applied with upper and lower cutoff points of 0.99 and 0.01, respectively. After achieving balance, a weighted regression model was used to estimate the treatment effect of ISBCS versus DSBCS on OR time utilization.
Sample Size
From our pilot study, the mean time (in minutes) to complete surgery for two eyes was 72.5 (SD = 16.59) for DSBCS and 60.13 (SD = 14.04) for ISBCS. Based on these values, a sample size calculation for comparing two independent means, with α = 0.05 and β = 0.2, determined a minimum of 30 participants per group. To accommodate the potential reduction in effective sample size due to the application of IPTW in our observational study, this sample size was adjusted using a variance inflation factor (VIF) following Austin’s suggestion.30 This adjustment increased the required sample size to approximately 40 participants per group. Accounting for an anticipated 10% dropout rate, the final sample size was set at 45 participants per group, totaling 90 participants.
Results
A total of 99 participants were enrolled: 45 in the ISBCS group and 54 in the DSBCS group. Subsequently, 9 participants in the DSBCS group were excluded due to intervals between two eye surgeries exceeding 12 weeks. The final analysis included 90 participants, 45 in each group (Figure 2). No intraoperative complications were reported.
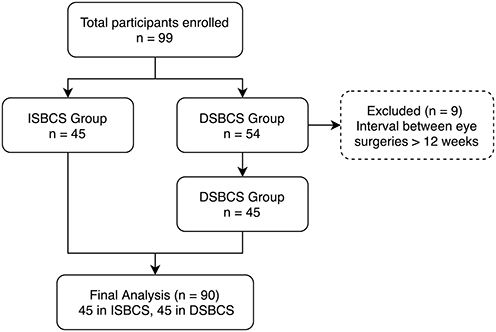 |
Figure 2 Participant recruitment flowchart of the ISBCS and DSBSC Group. |
Baseline demographics for the two groups are summarized in Table 1. Compared to the DSBCS, ISBCS was associated with younger surgeons (p = 0.014), lower PORS scores (p = 0.016), and more frequent use of toric and preloaded IOLs (p = 0.034 and p = 0.004, respectively). No significant differences were observed in other variables.
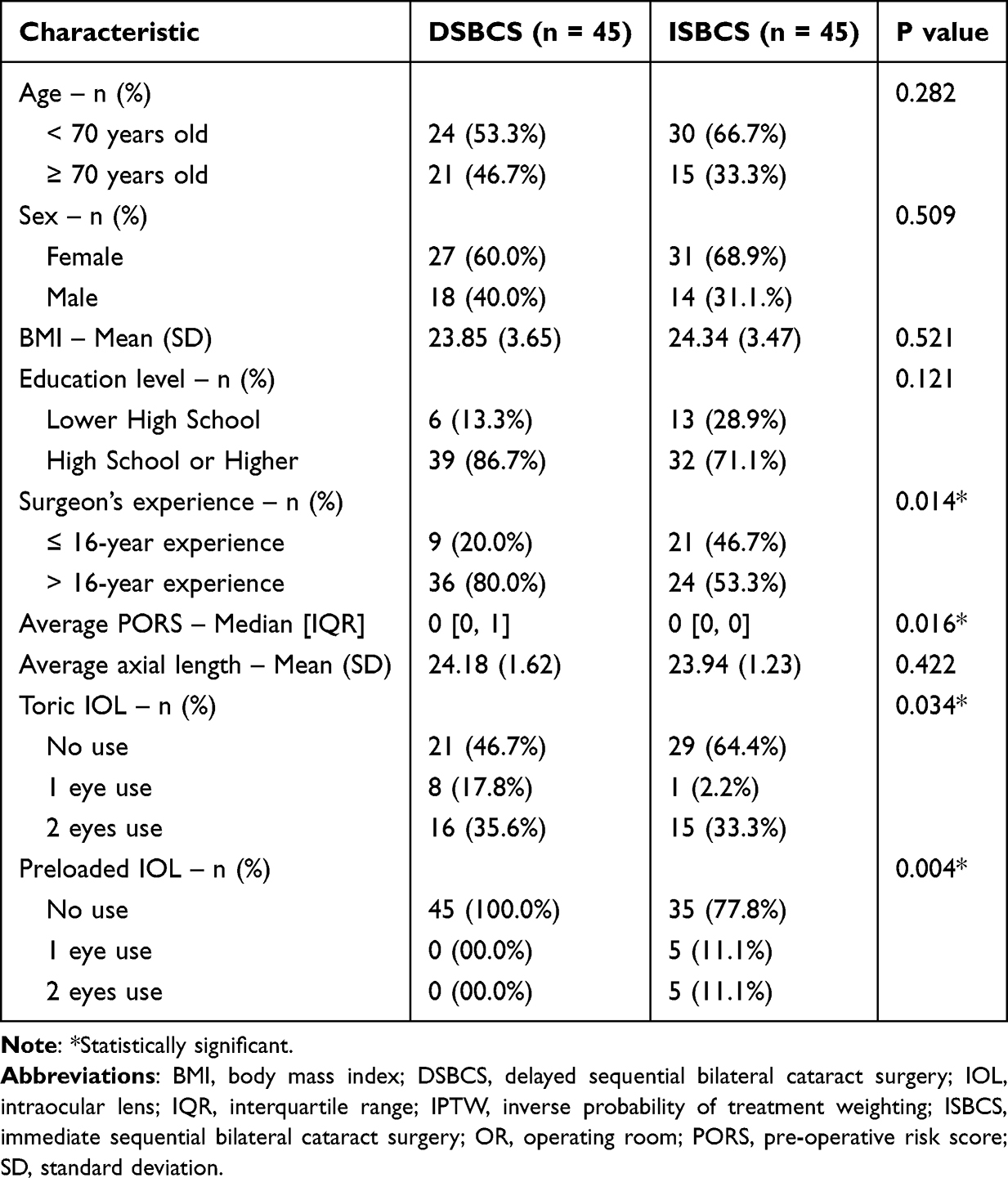 |
Table 1 Baseline Demographics of Participants |
The average OR utilization time was 55.8 minutes (SD = 12.0) for ISBCS and 60.0 minutes (SD = 12.9) for DSBCS. A simple t-test revealed no statistically significant differences between the two groups (p = 0.111).
As shown in Table 2, the original data exhibited considerable imbalances across several covariates. Following the application of IPTW to address these baseline imbalances, the ESS decreased from 45 per group to 17.83 in the DSBCS group and 31.59 in the ISBCS group. To enhance covariate balance by reducing the impact of extreme weights, weight truncation was then performed, which increased the ESS to 32.23 and 31.59 in the DSBCS and ISBCS groups, respectively.
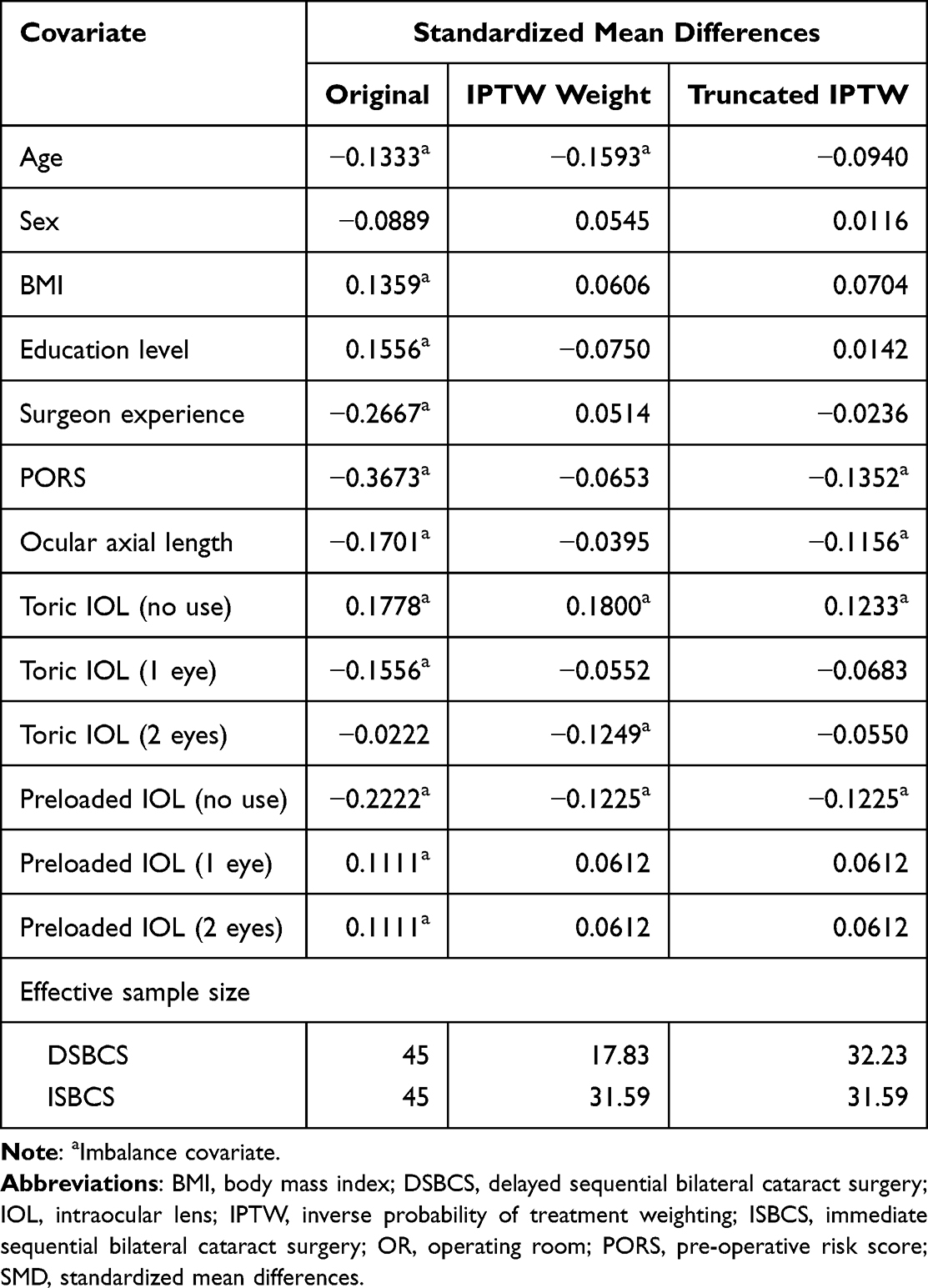 |
Table 2 Balance of Covariates Before and After Weighting |
Table 3 presents the treatment effect results following IPTW. ISBCS was associated with a significantly shorter OR utilization time compared to DSBCS, with an average reduction of 5.81 minutes (95% CI 0.87 to 10.76 minutes). This time-saving advantage of ISBCS remained consistent and statistically significant even after further adjusting for moderate imbalanced covariates from Table 2 or all nine covariates listed in Table 1, with reductions of 5.87 minutes (95% CI 1.44 to 10.29) and 5.98 minutes (95% CI 1.51 to 10.45), respectively.
 |
Table 3 The Results of the Final Weighted Linear Regression Models to Estimate the Treatment Effect on the Total OR Utilization Time |
The impact of surgical methods on various components of OR duration is detailed in Table 4, both unadjusted and adjusted with IPTW. After adjustment, there were no statistically significant differences between the two groups in preparation or draping time (p = 0.083 and p = 0.076, respectively). However, ISBCS showed considerable time-saving in key components: surgical time was reduced by 5.75 minutes (95% CI 1.77 to 9.72, p = 0.006), exit time by 2.10 minutes (95% CI 1.48 to 2.71, p < 0.001), and turnover time by 1.98 minutes (95% CI 0.77 to 3.18, p = 0.002.
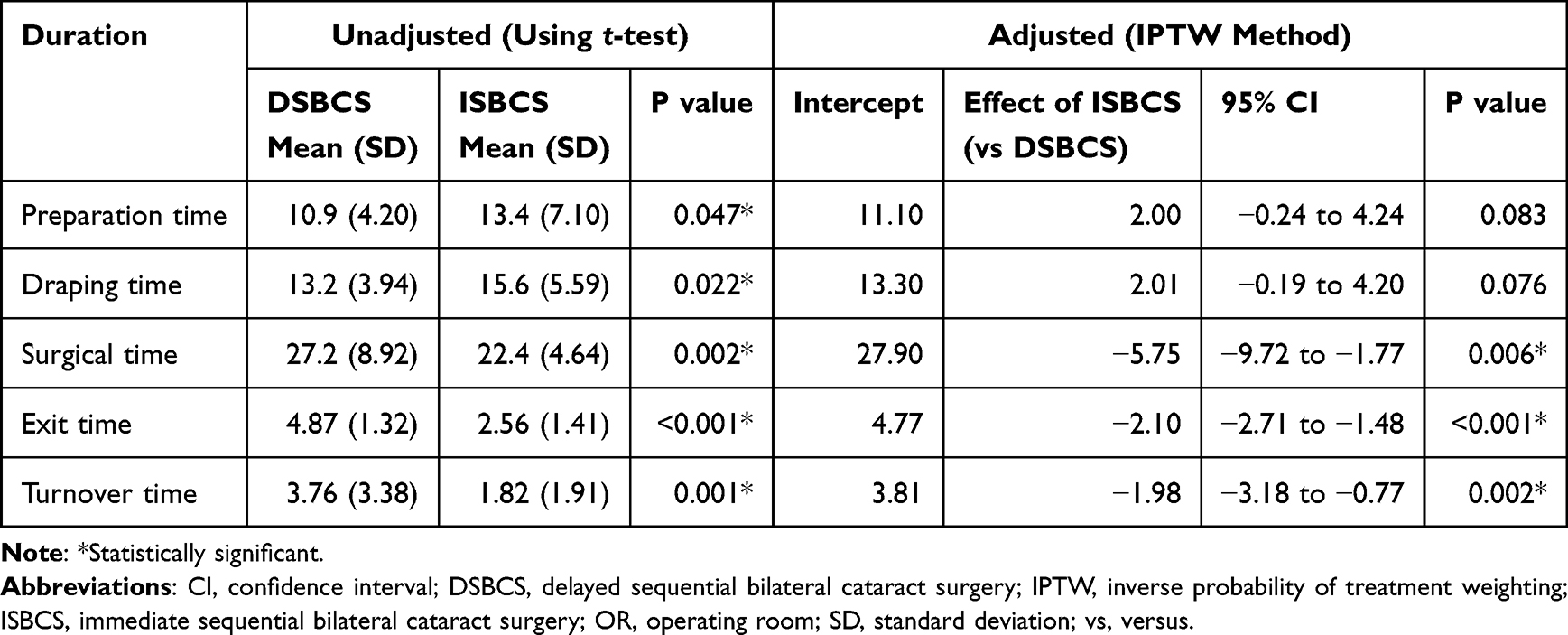 |
Table 4 Impact of Surgical Method on Different Components of the OR Time |
Table 5 illustrates the impact of surgeon experience on both total OR time and surgical time. More experienced surgeons reduced total OR time by 7.54 minutes (95% CI 2.85 to 12.23, p = 0.002) and surgical time by 5.88 minutes (95% CI 1.53 to 10.23, p = 0.009) compared to their less experienced counterparts.
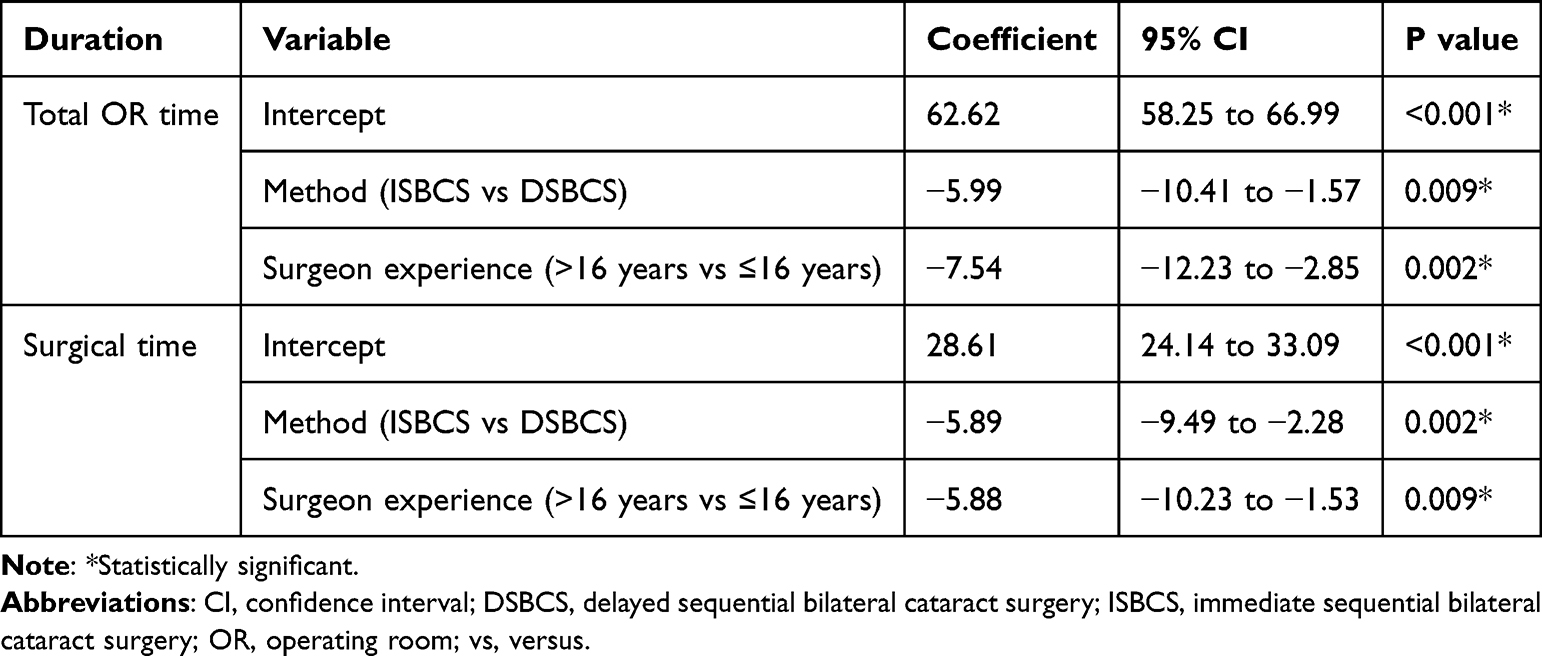 |
Table 5 Impact of “Surgeon Experience” on “Total OR Time” and “Surgical Time” Using a Weighted Linear Regression Model |
Discussion
Our study demonstrates that ISBCS significantly reduces total OR time compared to DSBCS, with an average reduction of approximately 6 minutes (around 10% of the total OR time for one patient). Our results are consistent with prior research, which reported OR time reductions from 6.48 to 6.62 minutes with ISBCS in different settings.14,15 A 10% reduction in OR time of the ISBCS approach may enhance surgical capacity, particularly in high-volume cataract surgery settings.
The consistency of the OR time reduction in ISBCS group across various covariate adjustments in Table 3 highlights the advantage of IPTW analysis over traditional regression methods in observational studies. By balancing baseline characteristics, IPTW ensured robust and consistent results, enhancing the reliability of our findings.
Further analysis of OR time components revealed significant reductions in surgical, exit, and turnover times with ISBCS compared to DSBCS after IPTW adjustment (Table 4). The time savings in exit (2.10 minutes) and turnover (1.98 minutes) were modest, likely due to the already efficient OR workflow at KCMH compared to other settings.15,31,32 These savings suggest that the overall time reduction may be more pronounced in settings with less optimized workflows, thereby enhancing the generalizability of ISBCS benefits to other high-volume ophthalmic centers.
The significant reduction in surgical time (5.75 minutes) was the primary driver of total OR time savings. Given the inclusion of multiple surgeons with varying levels of experience in the study, this decrease was likely influenced by surgeon variability, a factor that previous studies have also highlighted as significantly impacting OR time.22,32 Indeed, in the final weighted linear regression model following the application of IPTW, surgeon experience emerged as a significant factor affecting both OR time and surgical time, with more experienced surgeons (≥16 years since certification) achieving greater time savings (Table 5). Even with IPTW adjustment, unmeasured factors associated with surgeon experience, such as variations in surgical technique, case complexity management, or OR team dynamics, may contribute to procedural efficiency. A future study involving a single surgeon or a more standardized surgical team could provide a clearer and more precise estimate of the potential time-saving of ISBCS.
In contrast, other covariates, including patient age, sex, BMI, education level, axial length, PORS, and the type of IOL used (toric or preloaded), did not significantly impact OR time. These findings were not aligned with previous studies.18,22–26 This lack of effect may be attributed to the study’s small sample size. Future studies with larger cohorts could further explore whether these factors influence OR time.
Previous studies on OR time for ISBCS and DSBCS often used surgical lists dedicated to a single procedure type.15,17 This approach is useful for assessing maximum throughput and system efficiency under ideal, optimized conditions. By contrast, our study offered an additional perspective by examining the actual OR time per patient in routine practice, irrespective of whether the surgical list was dedicated or mixed. Together, these complementary approaches provide a more comprehensive assessment of ISBCS’s impact on OR time across varied clinical settings.
Additionally, this study only focused on OR time-saving for ISBCS, while other potential benefits, such as improving patient quality of life, satisfaction, or the risk of severe complications between the 2 groups, were not assessed. While previous studies have shown favourable patient-reported outcomes and high satisfaction with ISBCS,33–35 most of this evidence comes from high-income healthcare settings, where patient expectations and system efficiency may differ from those in developing countries. Therefore, the generalizability of these findings to lower-resource environments remains uncertain. Future research conducted in developing-country settings should explore these broader aspects to provide a more comprehensive evaluation of ISBCS’s overall impact across different healthcare systems.
The observational design and small sample size are considerable limitations that may impact the final result. Although propensity score analysis with IPTW and truncation method was applied, moderate imbalances remained in some covariates, with SMD between 0.1 and 0.2, likely due to the limited sample size. Furthermore, given the relatively small sample size and the use of multivariable adjusted models, there is a potential risk of overfitting, which may limit the generalizability of the adjusted estimates. This indicates the need for a randomized controlled trial or a larger observational study to improve the covariates’ balance and reliability of the findings. However, the observational nature of this study offers valuable insights by reflecting real-world surgical practices in a high-volume hospital like KCMH. By avoiding interventions that alter standard procedures, our design ensures that the results are interpretable and potentially generalizable to other hospitals without requiring strict modifications to existing workflows.
In conclusion, despite its limitations, this study demonstrates that ISBCS can enhance OR efficiency and potentially increase surgical capacity within existing resources. Surgeon experience emerged as a critical factor influencing OR time, while other patient-related variables showed no significant impact. Future research addressing the broader benefits and risks of ISBCS will further inform its adoption in clinical practice.
Acknowledgments
We would like to thank Miss Yuda Chongpison, Ph.D., M.S., from Chulalongkorn University, for her valuable statistical consultation and support for this study.
We also appreciate the contributions of our Research Assistant team from the Department of Ophthalmology, Chulalongkorn University: Miss Bubpha Puangmalee, Miss Jirawan Saothongthong, and Mr. Nattapach Prajansakunee.
We thank Ms. Sranya Phaisawang and the English editing service, Research Affairs, Faculty of Medicine, Chulalongkorn University, for their assistance in the paper preparation.
Funding
Supported by Global Health Research Promotion Grant from the School of Global Health, Faculty of Medicine, Chulalongkorn University, and Ratchadapiseksomphot Fund (Grant number MDCU GA67/074), Faculty of Medicine, Chulalongkorn University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang W, Yan W, Müller A, et al. A global view on output and outcomes of cataract surgery with national indices of socioeconomic development. Invest Ophthalmol Vis Sci. 2017;58(9):3669–3676. doi:10.1167/iovs.17-21489
2. Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(9):e888–e897. doi:10.1016/S2214-109X(17)30293-0
3. Lansingh VC, Carter MJ, Martens M. Global cost-effectiveness of cataract surgery. Ophthalmology. 2007;114(9):1670–1678. doi:10.1016/j.ophtha.2006.12.013
4. Pham D-N, Klinkert A. Surgical case scheduling as a generalized job shop scheduling problem. Eur J Oper Res. 2008;185(3):1011–1025. doi:10.1016/j.ejor.2006.03.059
5. Gür Ş, Eren T. Application of operational research techniques in operating room scheduling problems: literature overview. J Healthcare Engineer. 2018;2018:1–15. doi:10.1155/2018/5341394
6. Childers CP, Maggard-Gibbons M. Understanding costs of care in the operating room. JAMA Surg. 2018;153(4):e176233–e176233. doi:10.1001/jamasurg.2017.6233
7. Taravella MJ, Davidson R, Erlanger M, et al. Time and cost of teaching cataract surgery. J Cataract Refract Surg. 2014;40(2):212–216. doi:10.1016/j.jcrs.2013.07.045
8. Hodge W, Horsley T, Albiani D, et al. The consequences of waiting for cataract surgery: a systematic review. CMAJ. 2007;176(9):1285–1290. doi:10.1503/cmaj.060962
9. Arshinoff SA, Strube YN, Yagev R. Simultaneous bilateral cataract surgery. J Cataract Refract Surg. 2003;29(7):1281–1291. doi:10.1016/S0886-3350(03)00052-X
10. Lundström M, Albrecht S, Nilsson M, et al. Benefit to patients of bilateral same-day cataract extraction: randomized clinical study. J Cataract Refract Surg. 2006;32(5):826–830. doi:10.1016/j.jcrs.2006.01.075
11. Nassiri N, Nassiri N, Sadeghi Yarandi SH, et al. Immediate vs delayed sequential cataract surgery: a comparative study. Eye. 2009;23(1):89–95. doi:10.1038/sj.eye.6702989
12. Serrano-Aguilar P, Ramallo-Fariña Y, Cabrera-Hernández JM, et al. Immediately sequential versus delayed sequential bilateral cataract surgery: safety and effectiveness. J Cataract Refract Surg. 2012;38(10):1734–1742. doi:10.1016/j.jcrs.2012.05.024
13. Roberts HW, Myerscough J, Borsci S, et al. Time and motion studies of national health service cataract theatre lists to determine strategies to improve efficiency. Br J Ophthalmol. 2018;102(9):1259–1267. doi:10.1136/bjophthalmol-2017-310452
14. O’Brart DP, Harry R, Khayam N, et al. Economic modelling of immediately sequential bilateral cataract surgery (ISBCS) in the national health service based on possible improvements in surgical efficiency. BMJ Open Ophthalmol. 2020;5(1):e000426. doi:10.1136/bmjophth-2019-000426
15. Naderi K, Lam CFJ, Low S, et al. Time and motion studies to assess surgical productivity in cataract theatre lists within the national health service: immediate sequential bilateral cataract surgery versus delayed sequential bilateral cataract surgery. Eye. 2023;37:1–6.
16. Leivo T, Sarikkola AU, Uusitalo RJ, et al. Simultaneous bilateral cataract surgery: economic analysis; helsinki simultaneous bilateral cataract surgery study report 2. J Cataract Refract Surg. 2011;37(6):1003–1008. doi:10.1016/j.jcrs.2010.12.050
17. Arshinoff SA, Chen SH. Simultaneous bilateral cataract surgery: financial differences among nations and jurisdictions. J Cataract Refract Surg. 2006;32(8):1355–1360. doi:10.1016/j.jcrs.2006.02.064
18. Achiron A, Haddad F, Gerra M, et al. Predicting cataract surgery time based on preoperative risk assessment. Eur J Ophthalmol. 2016;26(3):226–229. doi:10.5301/ejo.5000697
19. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
20. Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika. 1983;70(1):41–55. doi:10.1093/biomet/70.1.41
21. Rosenbaum PR, Rubin DB. Reducing bias in observational studies using subclassification on the propensity score. J Am Stat Assoc. 1984;79(387):516–524. doi:10.1080/01621459.1984.10478078
22. McKay KM, Borkar DS, Moustafa GA, et al. Clinical factors affecting operating room utilization in cataract surgery: results from the PCIOL study. J Cataract Refract Surg. 2020;46(1):14–19. doi:10.1016/j.jcrs.2019.08.004
23. Park DY, Walkden A, De Klerk TA. Effect of cataract surgery training on operating room productivity: how long trainees take. J Cataract Refract Surg. 2016;42(9):1297–1301. doi:10.1016/j.jcrs.2016.07.029
24. Jones JJ, Chu J, Graham J, et al. The impact of a preloaded intraocular lens delivery system on operating room efficiency in routine cataract surgery. Clin Ophthalmol. 2016;10:1123–1129. doi:10.2147/OPTH.S107726
25. Mendicute J, Bascarán L, Pablo L, et al. Multicenter evaluation of time, operational, and economic efficiencies of a new preloaded intraocular lens delivery system versus manual intraocular lens delivery. Clin Ophthalmol. 2021;15:591–599. doi:10.2147/OPTH.S263658
26. Song X, Zhou J, Zhang G, et al. The impact of preloaded intraocular lens implantation system (TECNIS iTec®) in routine cataract surgery in China: a time-motion analysis. BMC Ophthalmol. 2023;23(1):126. doi:10.1186/s12886-023-02858-9
27. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
28. Burgette JM, Preisser JS, Rozier RG. Propensity score weighting: an application to an early head start dental study. J Public Health Dent. 2016;76(1):17–29. doi:10.1111/jphd.12106
29. Nimmo A, Latimer N, Oniscu GC, et al. Propensity score and instrumental variable techniques in observational transplantation studies: an overview and worked example relating to pre-transplant cardiac screening. Transpl Int. 2022;35:10105. doi:10.3389/ti.2022.10105
30. Austin PC. Informing power and sample size calculations when using inverse probability of treatment weighting using the propensity score. Stat Med. 2021;40(27):6150–6163. doi:10.1002/sim.9176
31. Umali MIN, Castillo TR. Efficiency of operating room processes for elective cataract surgeries done by residents in a national university hospital. Clin Ophthalmol. 2020;14:3527–3533. doi:10.2147/OPTH.S277550
32. Kang JM, Padmanabhan SP, Schallhorn J, et al. Improved utilization of operating room time for trainee cataract surgery in a public hospital setting. J Cataract Refract Surg. 2018;44(2):186–189. doi:10.1016/j.jcrs.2017.11.014
33. Arsenault R, Hébert M, You E, et al. Perception of visual outcomes in patients after delayed compared with immediately sequential bilateral cataract surgery. J Cataract Refract Surg. 2023;49(2):148–153. doi:10.1097/j.jcrs.0000000000001058
34. Nielsen MA, Bjerager J, Citirak G, et al. Patient-reported visual function outcomes in immediately sequential versus delayed sequential bilateral cataract surgery. Acta Ophthalmol. 2025;103(3):339–347. doi:10.1111/aos.16785
35. Carolan JA, Amsden LB, Lin A, et al. Patient experience and satisfaction with immediate sequential and delayed sequential bilateral cataract surgery. Am J Ophthalmol. 2022;235:241–248. doi:10.1016/j.ajo.2021.09.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Utility Analysis of Immediate Sequential and Delayed Sequential Bilateral Cataract Surgery in a Middle-Income Country
Nguyen CN, Somkijrungroj T, Pongsachareonnont PF, Tulvatana W
Clinical Ophthalmology 2026, 20:599816
Published Date: 18 April 2026