")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Cost-effectiveness of the COPD Patient Management European Trial home-based disease management program
Authors Bourbeau J, Granados D, Roze S, Durand-Zaleski I , Casan P, Köhler D, Tognella S, Viejo JL , Dal Negro RW , Kessler R
Received 4 May 2018
Accepted for publication 19 December 2018
Published 14 March 2019 Volume 2019:14 Pages 645—657
DOI https://doi.org/10.2147/COPD.S173057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Jean Bourbeau,1 Denis Granados,2 Stéphane Roze,3 Isabelle Durand-Zaleski,4 Pere Casan,5 Dieter Köhler,6 Silvia Tognella,7 Jose Luis Viejo,8 Roberto W Dal Negro,9 Romain Kessler10
1Department of Medicine, Division of Experimental Medicine, Respiratory Epidemiology and Clinical Research Unit, Research Institute of the McGill University Health Centre, Montreal, QC, Canada; 2Medical R&D – Real World & Clinical Evidence, Air Liquide Santé International, Gentilly, France; 3Department of Health Economics, HEVA HEOR, Lyon, France; 4URCEco Ile de France Hôpital de l’Hotel Dieu, Paris, France; 5Department of Pneumology, Asturias University Hospital, Oviedo, Spain; 6Department of Internal Medicine, Kloster Grafschaft Specialised Hospital, Schmallenberg, Germany; 7Department of Pneumology, Bussolengo General Hospital, Bussolengo, Italy; 8Department of Pneumology, Burgos University Hospital, Burgos, Spain; 9Department of Pneumology, Bussolengo Hospital, Bussolengo, Italy; 10Department of Pneumology, Fédération de Médecine Translationnelle de Strasbourg (FMTS), Université de Strasbourg, Strasbourg, France
Purpose: Efficient management of COPD represents an international challenge. Effective management strategies within the means of limited health care budgets are urgently required. This analysis aimed to evaluate the cost-effectiveness of a home-based disease management (DM) intervention vs usual management (UM) in patients from the COPD Patient Management European Trial (COMET).
Methods: Cost-effectiveness was evaluated in 319 intention-to-treat patients over 12 months in COMET. The analysis captured unplanned all-cause hospitalization days, mortality, and quality-adjusted life expectancy. Costs were evaluated from a National Health Service perspective for France, Germany, and Spain, and in a pooled analysis, and were expressed in 2015 Euros (EUR). Quality of life was assessed using the 15D health-related quality-of-life instrument and mapped to utility scores.
Results: Home-based DM was associated with improved mortality and quality-adjusted life expectancy. DM and UM were associated with equivalent direct costs (DM reduced costs by EUR -37 per patient per year) in the pooled analysis. DM was associated with lower costs in France (EUR -806 per patient per year) and Spain (EUR -51 per patient per year), but higher costs in Germany (EUR 391 per patient per year). Evaluation of cost per death avoided and cost per quality-adjusted life year (QALY) gained showed that DM was dominant (more QALYs and cost saving) in France and Spain, and cost-effective in Germany vs UM. Nonparametric bootstrapping analysis, assuming a willingness-to-pay threshold of EUR 20,000 per QALY gained, indicated that the probability of home-based DM being cost-effective vs UM was 87.7% in France, 81.5% in Spain, and 75.9% in Germany.
Conclusion: Home-based DM improved clinical outcomes at equivalent cost vs UM in France and Spain, and in the pooled analysis. DM was cost-effective in Germany with an incremental cost-effectiveness ratio of EUR 2,541 per QALY gained. The COMET home-based DM intervention could represent an attractive alternative to UM for European health care payers.
Keywords: cost-effectiveness, France, Spain, Germany, home-based disease management, COPD
Introduction
COPD affects 210 million people globally and is a leading cause of mortality, with estimates of over 3 million deaths in 2015 corresponding to 5% of global mortality.1,2 The prevalence of COPD in European adults is estimated to be between 4% and 10%, and in France, Germany, Italy, and Spain, the numbers of people living with COPD range from 1.5 to 3.5 million.3–5 In 2011, the direct costs of treatment for COPD were approximately Euros (EUR) 23.3 billion in the European Union.5 COPD exacerbations occur on average twice per year and are an important driver of costs, with around 10% of events leading to hospitalization.6,7 The economic impact of COPD is also felt at a societal level, as the condition is associated with significant workplace absenteeism.8 Lost productivity in Europe, including absence from work and early retirement, was estimated to cost approximately EUR 25.1 billion in 2011.5
The COPD Patient Management European Trial (COMET), a randomized, international, multicenter trial, compared a home-based disease management (DM) program with usual management (UM) in four European countries in patients with severe COPD.9,10 The key interventions applied (for 1 year), previously described by Bourbeau et al, included several components: a self-management program and coaching by a case manager based on the “Living Well with COPD” program (http://www.livingwellwithcopd.com), home monitoring, and an e-Health telephone/web platform for prompt detection and early treatment of exacerbations.9 The trial showed that all-cause hospital days (primary end point), expressed as mean (SD), including days in acute care wards and consecutive days in nursing facilities, were 17.4 (35.4) days/year with DM and 22.6 (41.8) days/year with UM (intention-to-treat [ITT] population, P=0.16).10 Secondary end points which showed statistically significant differences between groups were all-cause acute care hospital days (−8.3, 95% CI −16.4 to −0.1; P=0.047, per-protocol analysis), change in the Body mass index, Airflow Obstruction, Dyspnea and Exercise index (−0.5, 95% CI −0.9 to −0.1; P=0.01, ITT), and mortality (three deaths [1.9%] with DM and 23 [14.2%] with UM; P<0.001, ITT).
The aim of the present health-economic study was to perform a cost-effectiveness evaluation, based on COMET, comparing DM with the current UM. The analysis was designed to model survival, quality of life (QoL), and economic outcomes over the 12-month follow-up period based on resource use and clinical outcomes data recorded in the trial.
Methods
The health economic evaluation of COMET was based on clinical data from the trial and resource-use data from the four participating countries.11 Country-specific costs were evaluated from a national health care payer perspective, and country-specific cost-effectiveness evaluations were performed in addition to a pooled analysis of all participating countries. The within-trial cost-effectiveness model was developed using the statistical programming language R (RStudio software version 0.99.447©; RStudio, Inc., Boston, MA, USA). The analysis included patient characteristics and clinical outcomes. Data on country-specific health resource consumption collected during the trial and published cost estimates were used to evaluate direct medical and direct nonmedical costs for each country with over 25 patients in each treatment group (hospitalizations, medical and paramedical consultations, components such as coaching sessions, and technical costs of the DM intervention). Cost-effectiveness was then evaluated by generating a range of incremental cost-effectiveness ratios (ICERs) for DM vs UM. ICERs are a standard measure of cost-effectiveness calculated by dividing the cost difference (usually expressed in local currency) between two interventions by the difference in effectiveness between the same two interventions.
Patient population and clinical data
The pooled analysis was based on the ITT population from COMET (NCT01241526), which comprised 319 patients from the four countries with 157 patients in the DM group and 162 patients in the UM group. The trial was approved by the local or national ethics committees and competent authority per country for each investigational center where applicable, and all patients provided written, informed consent (Table S1). For the country-specific analyses, only France, Germany, and Spain were considered as they presented more than 25 patients in both DM and UM groups. The cohort characteristics and clinical outcomes from COMET have been published by Kessler et al.10 The economic evaluation captured unscheduled all-cause hospital days, acute exacerbations, health-related quality of life (HRQoL), and mortality from the trial.
Cost data
Costs in all three countries were expressed in 2015 EUR. Direct medical and nonmedical costs, including those associated with unscheduled hospitalizations, outpatient visits, coaching by case managers, and management of the alerts and alarms by the case managers and investigators, were accounted for each patient in the ITT population. Costs were then presented as mean annualized costs for each country. Technical costs relating to the set-up of the DM intervention included both fixed (not related to the number of patients in the group) and variable costs (related to the number of patients in the group). Fixed costs were EUR 82,339 in total and included system initiation (EUR 25,725), hosting (EUR 41,400), initiation of the toll-free number (EUR 4,320), and fixed costs of printing (EUR 10,894). Variable costs were EUR 34,136 in total and included patient calls (EUR 9,855), call durations (EUR 8,278), call-back by nurses (EUR 1,166), sending of SMS (EUR 1,971), sending of faxes (EUR 1,971), and variable costs of printing (EUR 10,894). For the ITT population, these totals corresponded to fixed costs of EUR 524.45 per patient and variable costs of EUR 217.43 per patient. Transportation costs for patients in the intervention group attending coaching group sessions were added to the variable costs. The mean transportation cost per patient to attend group sessions was EUR 247.19 for all countries with individual mean costs of EUR 280.74, EUR 342.97, and EUR 135.00 for France, Germany, and Spain, respectively. The total technical costs (including the transportation costs) were added to the overall Kaplan–Meier Sample Average (KMSA) cost analysis per patient in the base case analysis.
QoL
In COMET, HRQoL data were collected using the 15D HRQoL instrument. It is a generic, 15-dimensional, standardized, self-administered measure of HRQoL in validated local language versions (http://www.15d-instrument.net/15d/). The 15D HRQoL instrument was self-completed by study patients at study entry and every 6 months during the follow-up period. The collected data were not utilities, and needed to be mapped to utility scores using the validated Finnish algorithm. Utilities are preference health state values used to estimate quality-adjusted life years (QALYs).
Cost-effectiveness analysis
The cost-effectiveness outcomes were analyzed and presented as ICERs of the intervention (home-based DM) vs control (UM). Cost-effectiveness was evaluated based on the number of unscheduled, all-cause hospital days and the number of deaths in each study group. In addition, a cost-utility analysis was conducted using utility scores (expressed in QALYs) as the measure of effectiveness. ICERs were presented where appropriate (when interventions were not dominant/dominated). The time horizon of the analysis was 12 months (as per the follow-up duration in the study), and no discounting of costs or clinical benefits was applied.
Statistical approach
Statistical analysis was performed in the programming language R (using RStudio software version 0.99.447©). KMSA methods were used over 12 months to generate annualized costs and clinical outcomes from monthly estimates during the follow-up period.12 The proportion of patients still alive at the beginning of the month was estimated, using the probability of survival in a given month. Mean estimates were then weighted and applied to all subsequent months to obtain the mean adjusted costs/outcomes per patient. This method was applied to the mean number of unscheduled hospital days, mean number of deaths, mean QALYs per patient, and the mean overall costs.
Significance testing was performed on differences in costs between the two study groups in each country by calculating the CI of the cost difference, via a nonparametric bootstrapping approach (if the 95% CI of the cost difference included zero, the cost difference was considered as not statistically significant). The influence of statistical variance on modeled outcomes was investigated using nonparametric bootstrapping to evaluate the statistical uncertainty around the cost-effectiveness outcomes. Bootstrap methods are commonly used to estimate the accuracy of distribution and provide an alternative to CIs.13 Bootstrapping with 1,000 iterations was used to calculate the CI of the difference of average KMSA estimates of overall costs between the UM group and the DM group in each country and globally, separately, as the 2.5% and 97.5% percentiles of the bootstrap results.14 This approach was used to generate scatter plots of incremental costs vs incremental effectiveness for each country and for the pooled analysis, as well as acceptability curves to provide a probability of DM being cost-effective vs UM at a range of willingness-to-pay thresholds.
Results
Overall annual costs
Evaluation of overall annual direct medical costs indicated that DM was cost saving in the COMET population in France and Spain, but may cost more than UM in Germany (Table 1). Over 1 year, in the pooled countries analysis, DM was associated with a cost saving of approximately EUR 37 per patient per year vs UM. Cost savings were highest in France, where the annual direct costs associated with DM were approximately EUR 806 less than with UM. DM was close to cost neutral in Spain (saving of EUR 51) but was associated with higher annual costs in Germany (EUR 391) vs UM. None of the cost differences in the pooled analysis or the individual country evaluations reached statistical significance.
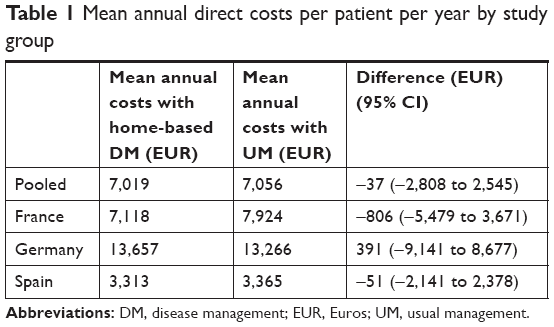 | Table 1 Mean annual direct costs per patient per year by study group |
Clinical outcomes
Between-country variation was observed in terms of annual number of unscheduled hospital days, with DM associated with fewer hospital days in France (−5.00 days) and Spain (−6.34 days), but more hospital days in Germany (+5.06 days). HRQoL was improved with DM in the overall COMET population and in all country settings (Table 2). Annual improvements were in the range 0.064 (Spain) to 0.154 (Germany), based on mapping of 15D HRQoL instrument collected during the trial. Annualized mortality rates were lower with DM than UM in all countries (Table 2). Mortality rates were reduced by 0.09 events per year in France and Spain, and 0.13 events per year in Germany.
 | Table 2 Summary of clinical outcomes by study group |
Cost-effectiveness evaluation
Cost-effectiveness evaluation based on unscheduled hospital days avoided reflected the clinical outcomes with DM dominant to UM (cost saving with a clinical benefit) in the pooled countries analysis, and in France and Spain (Table 3). In contrast, DM was dominated by UM in the German setting. Cost-effectiveness evaluation based on annualized quality-adjusted life expectancy values (cost-utility) showed that DM was likely to be dominant or cost-effective vs UM in all settings (Table 3). In the pooled COMET population, and France and Spain, the cost savings associated with DM meant that it was dominant to UM (cost saving and improved QALYs). In Germany, where annual direct costs were higher with the DM intervention, the ICER was approximately EUR 2,541 per QALY gained vs UM. Cost-effectiveness expressed in cost per death avoided showed a similar pattern to cost-utility analysis (Table 3). DM was dominant to UM in the overall COMET population, and France and Spain, where the intervention was cost saving and associated with reduced mortality. In Germany, DM was associated with an ICER of EUR 3,010 per death avoided vs UM.
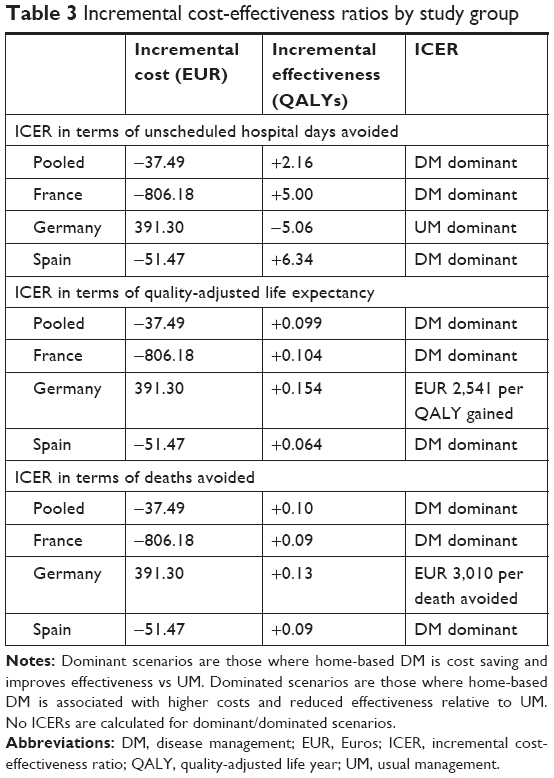 | Table 3 Incremental cost-effectiveness ratios by study group |
Statistical uncertainty
Nonparametric bootstrapping was performed to capture statistical uncertainty in the cost-effectiveness analysis. Scatter plot analysis showed that for France and Spain and the pooled countries analysis, the majority of points representing incremental costs and incremental effectiveness (QALYs) were in the bottom right quadrant of the cost-effectiveness plane, indicating that DM was dominant to UM (Figure 1). For Germany, the majority of points were in the upper right quadrant, indicating increased costs and increased effectiveness (QALYs) with DM vs UM. The same data were used to generate cost-effectiveness acceptability curves which showed that, assuming a willingness-to-pay threshold of EUR 20,000 per QALY gained, DM is very likely to be considered cost-effective vs UM in the COMET population and in all three country settings (Figure 2 and Table 4). The probability of DM being cost-effective vs UM was approximately 91% in the pooled countries analysis, 88% in France, 76% in Germany, and 82% in Spain. When using survival as the measure of effectiveness, nonparametric bootstrapping indicated that the probabilities of DM being dominant to UM were 51% in the overall COMET population, 62% in France, 50% in Germany, and 52% in Spain (Table 4 and Figures 3 and 4). Assuming a willingness-to-pay threshold of EUR 20,000 per death avoided, the probabilities of DM being cost-effective were 91% in the pooled countries analysis, 85% in France, 71% in Germany, and 85% in Spain.
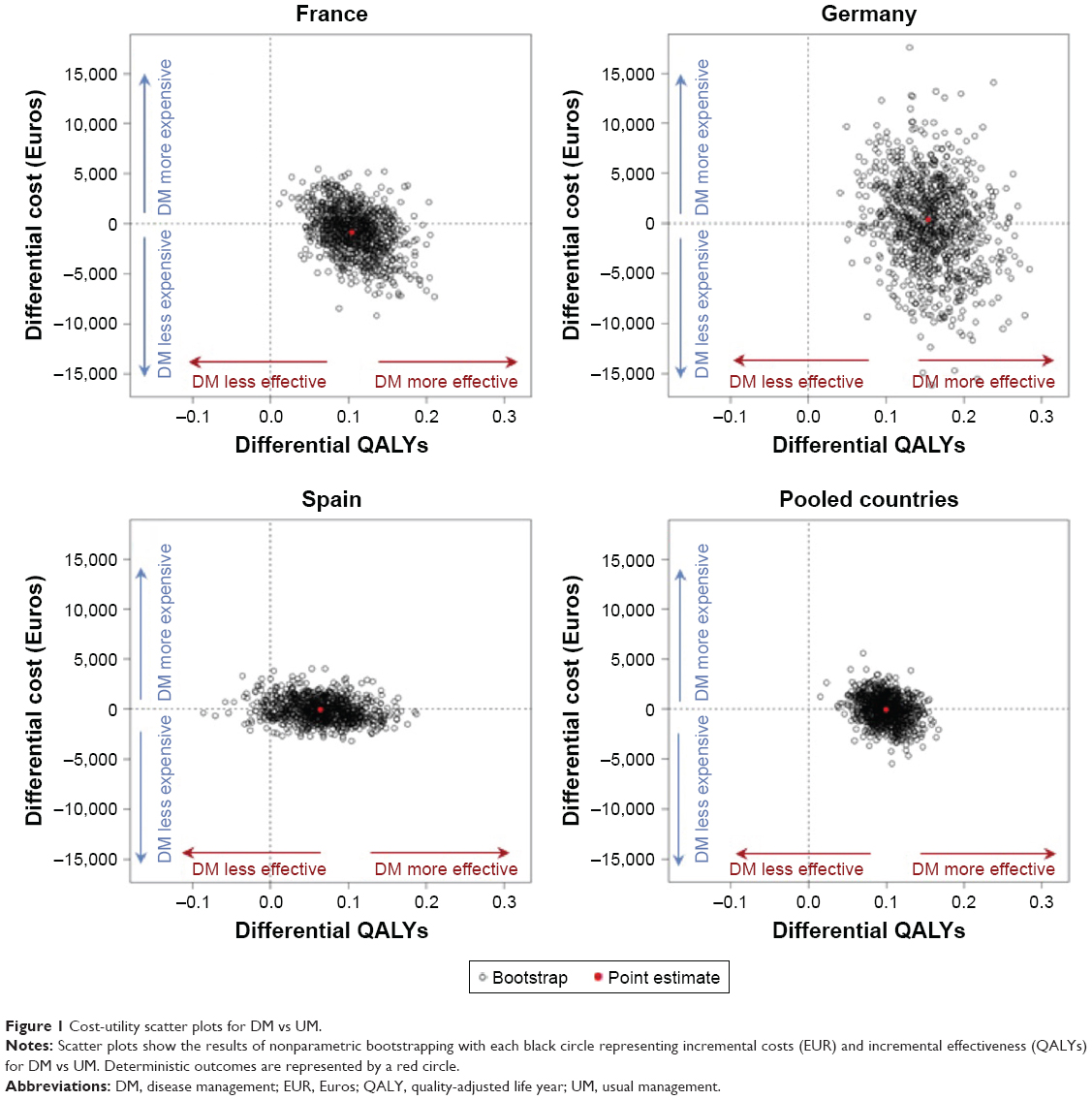 | Figure 1 Cost-utility scatter plots for DM vs UM. |
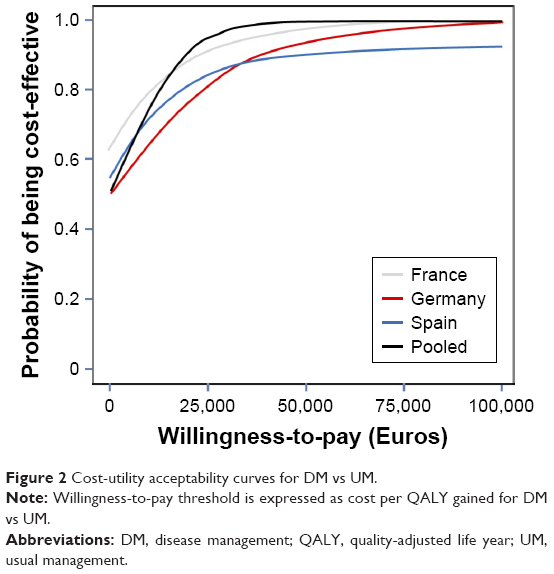 | Figure 2 Cost-utility acceptability curves for DM vs UM. |
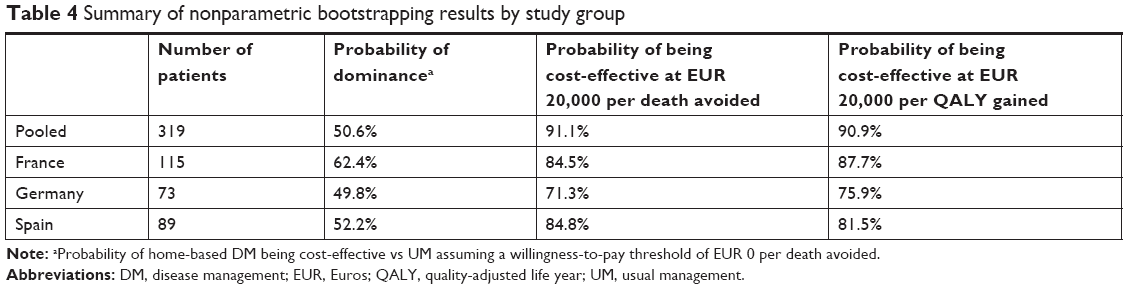 | Table 4 Summary of nonparametric bootstrapping results by study group |
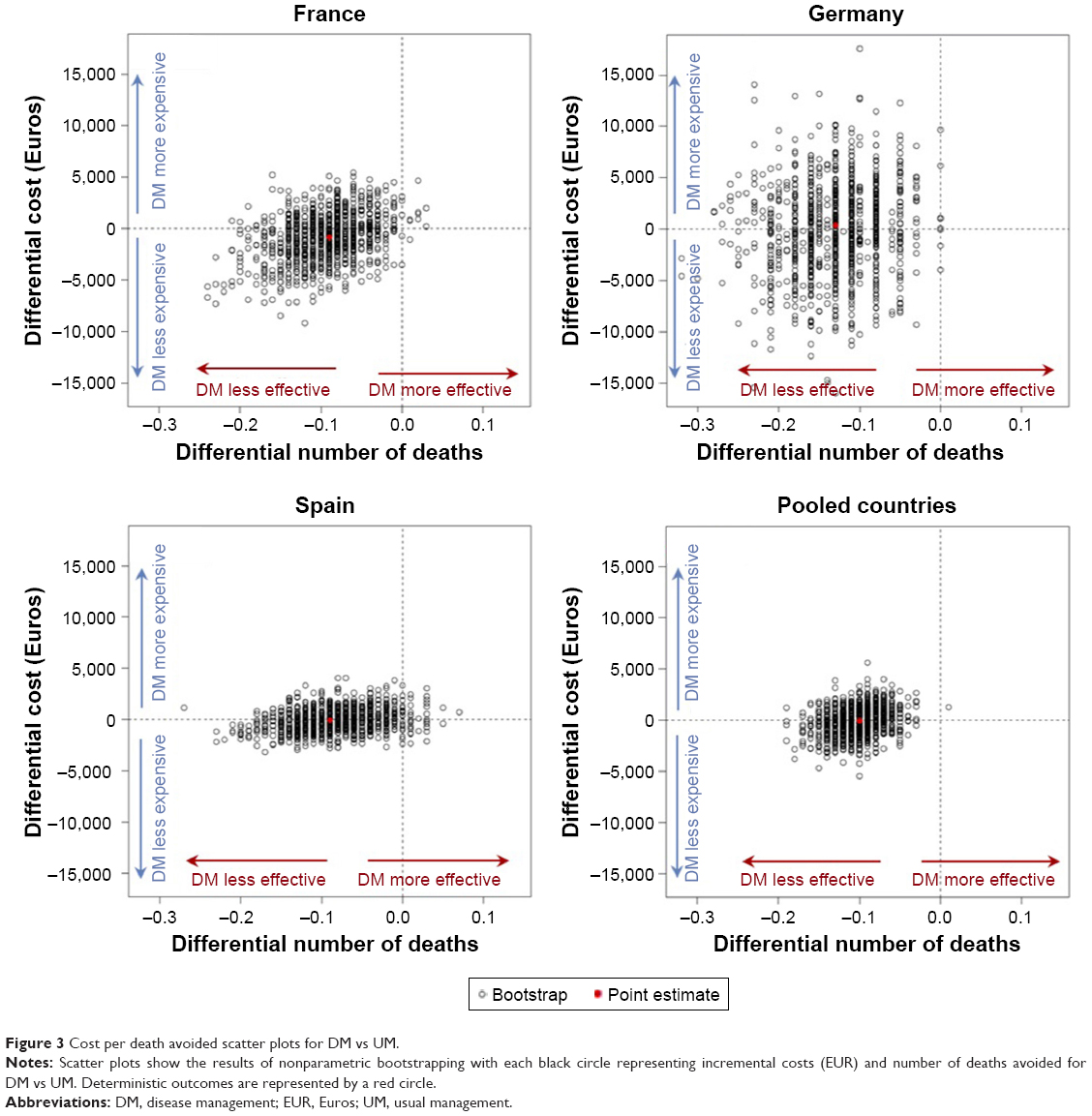 | Figure 3 Cost per death avoided scatter plots for DM vs UM. |
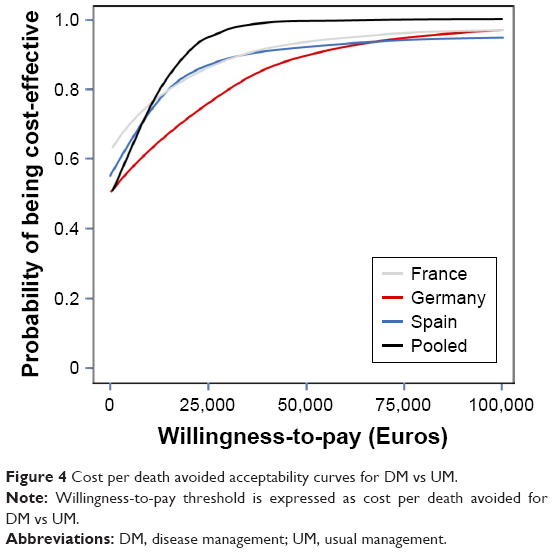 | Figure 4 Cost per death avoided acceptability curves for DM vs UM. |
Discussion
The findings of the present analysis showed that overall, across the four countries analyzed, multicomponent home-based DM intervention was associated with a cost saving of EUR 37.50 per patient per year relative to UM in patients with severe or very severe COPD (GOLD stage III/IV). The study sample size calculation in COMET was based on the primary clinical objective.10 Therefore, it was not designed to show a statistical difference in costs between study groups, resulting in large CIs. Savings of EUR 37.50 were consistent with the primary clinical result, specifically the nonsignificant overall reduction in the number of unscheduled all-cause hospital days.10 On an individual country level, DM was associated with cost savings in France and Spain, but higher overall costs relative to UM in Germany due to higher costs associated with unscheduled hospital days.
In all countries included in the analysis, DM was associated with improved self-reported QoL based on the 15D HRQoL instrument, with patients in the DM group having utility gains relative to UM ranging from 0.06 to 0.15 QALYs. These values compare favorably to the HRQoL benefits of less than 0.10 QALYs per patient typically associated with the pharmacologic treatment of COPD in a recent review.15 Improvements in HRQoL meant that DM was dominant to UM in cost-utility analyses for France and Spain (cost saving with an improvement in QALYs), and associated with an ICER of EUR 2,541 per QALY gained in Germany (Table 3). A similar pattern of outcomes was observed when cost-effectiveness was evaluated based on mortality (cost per death avoided). An important driver of cost-effectiveness outcomes was the lower mortality in the DM group compared with UM observed in COMET. In the trial, a significant difference was also observed between DM and UM in terms of days in acute care wards in the per-protocol population, and this may also contribute to the cost benefits associated with DM given that the acute care ward stays are costlier than the equivalent time in standard wards or in nursing facilities.10
The base case cost-effectiveness analysis included both the fixed and variable technical costs associated with the DM intervention. Fixed technical costs constituted the one-off costs associated with initial set-up of DM, including system initiation, data hosting, and set-up of the toll-free number. Overall, fixed technical costs exceeded EUR 82,000 (approximately EUR 524 per patient), and over a time horizon of 12 months, this constituted a considerable proportion of the overall costs. Over a longer time period or if patient numbers were increased, fixed technical costs would become a lower proportion of the overall costs, and would likely increase the cost savings associated with DM. Indeed, in an exploratory analysis excluding fixed technical costs, DM was associated with cost savings of approximately EUR 562 per patient per year in the overall COMET population. When performing this exploratory analysis by country, DM was cost saving relative to UM in France, Spain, and Germany.
There are several potential reasons for the heterogeneous outcomes between countries in the present analysis. Patient numbers in individual countries were relatively low, ranging from 73 patients in Germany to 89 in Spain and 115 in France. Moreover, the patients and disease characteristics were also heterogeneous, and more severe disease and/or comorbid conditions are known to have higher rates of exacerbations and related hospitalizations.16,17 It is well established that a small proportion of COPD patients exhibit the “frequent exacerbator phenotype”, which is associated with higher levels of medical resource utilization. However, a large proportion of the COMET population (approximately 50%) was never hospitalized during their study follow-up. Length of hospital stay and costs are also influenced by the reason for hospital admission and by the ward of admission, as well as by hospital bed availabilities.18 Therefore, in studies with low patient numbers such as the present trial, mean costs may be sensitive to small numbers of patients with high levels of resource use. Additionally, differences in management practices between countries (eg, decision making on hospitalization) may also have contributed to the differences in findings between countries in the present analysis.
QoL data were collected using the 15D HRQoL instrument. While there is no published evidence and validated tools for utility score generation by country of interest from 15D HRQoL instrument, the EuroQol project provides indirect evidence supporting the use of a reference algorithm (such as the Finnish one used in the present study) to provide utility scores for different countries. Sintonen et al reported that it is largely unnecessary to replicate expensive valuation studies in Western industrialized countries to arrive at valid preference-based instruments, owing to the degree of concordance between health state valuations across European settings.19 In the pooled analysis, DM was associated with improvements in QoL vs UM, and this was also true when all three countries were analyzed separately. Symptom burden was not examined in the present study, but symptom burden and functional impairment in COPD have been shown to be linked to impaired HRQoL. Consequently, it is possible that the patient-related benefits associated with DM extend beyond the HRQoL benefits reported here. That acknowledged, the findings from the present cost-utility analysis indicated that the benefits in terms of quality-adjusted life expectancy (expressed in QALYs) led to DM being either dominant or cost-effective vs UM, using commonly cited willingness-to-pay thresholds, across all settings analyzed.
The present analysis is one of the first to examine the cost-effectiveness of a home-based DM intervention in severe COPD patients. The self-management program used in COMET was based on the “Living Well with COPD” program developed at the Montreal Chest Institute, McGill University Health Centre, Montreal, Canada. This program, with a written action plan, has been shown to significantly reduce all-cause hospitalizations and emergency room visits by approximately 40% in reports by Bourbeau et al (1-year analysis) and Gadoury et al (2-year analysis) in patients with moderate-to-severe COPD.20,21 These data suggest that some patients may derive substantial clinical benefits from participation in DM programs with the use of written action plans and communication with case managers. This hypothesis is supported by comparison with ICERs from other interventions for COPD summarized in the “pyramid of value” originally developed by the London Respiratory Network and the London School of Economics.22 Based on the present analysis, DM compared favorably with the other COPD interventions ranked from telehealth for chronic disease (ICER of British Pounds Sterling [GBP] 92,000 per QALY gained) down to flu vaccination for at-risk populations (ICER less than GBP 1,000 per QALY gained).
Conclusion
The present health economic evaluation showed that home-based DM, as applied in COMET, was associated with cost savings compared with UM in a pooled analysis of European countries. On an individual country level, DM was associated with cost savings in both France and Spain, but with higher costs in Germany. As the analysis included fixed technical costs, these savings are likely to become greater if the time horizon is extended beyond 12 months. Improved clinical outcomes with DM (in terms of benefits in both mortality and QALYs) meant that DM was dominant to UM (cost and life saving) in the pooled analysis. This was also true in the country-level analyses for France and Spain, whereas in Germany DM was found to be cost-effective vs UM, based on willingness-to-pay thresholds of EUR 20,000 per QALY gained or EUR 20,000 per death avoided. The present study provides new evidence on the health economics of managing severe COPD patients and indicates that the COMET home-based DM intervention may represent an attractive alternative to UM for European health care payers.
Acknowledgments
This study was supported by funding from Air Liquide Santé International, and health economic analysis was performed by HEVA HEOR. The authors thank all the COMET personnel who participated in this study, in particular the VitalAire case managers from the four countries, the three members of the Endpoint Validation Committee (Dr Bucknall, Respiratory Medicine, Glasgow Royal Infirmary, Scotland, UK; Prof Burgel, Pneumologie et Centre de Mucoviscidose de l’adulte, Hôpital Cochin, Paris, France; Prof Vogelmeier, Pulmonary Division, Marburg University Hospital, Marburg, Germany), and the COMET investigators: Dr Aguar Benito, Medicina Interna, Hospital Arnau de Vilanova, Valencia, Spain; Dr Ancochea Bermudez, Neumología, Hospital La Princesa, Madrid, Spain; Dr Arnal, Réanimation, Hôpital Sainte Musse, Toulon, France; Dr Bastian, Pneumologie und Beatmungsmedizin, Marienkrankenhaus Kassel, Kassel, Germany; Prof Bergeron-Lafaurie, Pneumologie, Hôpital Saint-Louis, Paris, France; Dr Botrus, Pneumologie, Centre Hospitalier Régional Metz Thionville, Thionville, France; Prof Charpin, Pneumologie – Allergologie, Hôpital Nord, Assistance Publique, Hôpitaux de Marseille, Marseille, France; Dr Chavaillon, Pneumologie, Centre Hospitalier d’Antibes-Juan-les-Pins, Antibes, France; Prof Cornelissen, Pneumologie, Universitätsklinik, Aachen, Germany; Dr De Abajo, Pneumología, Hospital Universitario De Burgos, Burgos, Spain; Prof Devouassoux, Pneumologie, Hôpital de la Croix Rousse, Lyon, France; Dr Díaz Lobato, Neumología, Hospital Universitario Ramón y Cajal, Madrid, Spain; Dr Goupil, Pneumologie, Centre Hospitalier, Le Mans, France; Prof Herth, Pneumologie und Beatmungsmedizin, Thoraxklinik Heidelberg, Heidelberg, Germany; Dr Kropf, Pneumologie, Universitätsklinikum Ulm, Ulm, Germany; Dr Nilius, Klinik für Pneumologie, Helios Klinik Hagen-Ambrock, Hagen, Germany; Prof Pepin, Rééducation Physiologie, CHU de Grenoble, Grenoble, France; Dr Pietra, Pneumologia, Ospedale San Carlo Borromeo, Milan, Italy; Dr Rampoldi, Riabilitazione Pneumologica, Azienda Ospedaliera di Desio e Vimercate, Seregno, Italy; Prof Randerath, Pneumologie und Allergologie, Krankenhaus Bethanien, Solingen, Germany; Dr Reißig, Pneumologie, Fachkrankenhaus Kloster Grafschaft, Schmallenberg, Germany; Dr Riesco, Neumologia, Hospital San Pedro de Alcantara, Caceres, Spain; Dr Rodriguez Gonzalez-Moro, Neumologia, Hospital Gregorio Marañón, Madrid, Spain; Dr Rolo, Pneumology, Villa Marelli, Milan, Italy; Dr Salmeron, Pneumologie Allergologie/Tabacologie, Groupe Hospitalier Saint Joseph, Paris, France; Dr Scavalli, Fisiopatologia Respiratoria e Allergologia, Ospedale Andosilla di Civita Castellana, Civita Castellana, Italy; Prof Similowski, Pneumologie et Réanimation, Groupe hospitalier Pitié-Salpétrière, Paris, France; Dr Tubaldi Alberto, Pulmonary Diseases, Ospedale di Macerata, Macerata, Italy; Dr Voicu, Pneumologie, CHR Metz-Thionville – Hôpital de Mercy, Metz, France; and Dr Westhoff, Innere Medizin, Pneumologie, Lungenklinik Hemer, Hemer, Germany. The authors specially thank Joëlle Texereau and Patricia Alegre from Air Liquide Santé International and Clémentine Cartier-Bechu, Marine Sivignon, and Audrey Petitjean from HEVA HEOR. The authors are grateful for the medical writing support from Ceilidh McConnachie at Ossian Health Economics and Communications.
Disclosure
JB, IDZ, PC, DK, ST, JLV, RWDN, and RK were investigators in the COMET trial and have received honoraria from Air Liquide Healthcare, sponsors of the COMET trial. DG was an employee of Air Liquide Healthcare at the time when the study was conducted. SR is a director of HEVA HEOR, which received consulting fees from Air Liquide Healthcare to perform the health economic analysis described here. The authors report no other conflicts of interest in this work.
References
WHO Global Alliance Against Chronic Respiratory Diseases [homepage on the Internet]. World Health Organization. Available from: http://www.who.int/gard/publications/chronic_respiratory_diseases.pdf. Accessed January 19, 2017. | ||
WHO Chronic Obstructive Pulmonary Disease Fact Sheet [homepage on the Internet]. World Health Organization. Available from: http://www.who.int/en/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd). Accessed October 18, 2018. | ||
Halbert RJ, Isonaka S, George D, Iqbal A. Interpreting COPD prevalence estimates: what is the true burden of disease? Chest. 2003;123(5):1684–1692. | ||
Dal Negro R, Rossi A, Cerveri I. The burden of COPD in Italy: results from the Confronting COPD survey. Respir Med. 2003;97(Suppl C):S43–S50. | ||
Lung Health in Europe: Facts and Figures [homepage on the Internet]. European Lung Foundation and European Respiratory Society; 2013. Available from: http://www.europeanlung.org/assets/files/publications/lung_health_in_europe_facts_and_figures_web.pdf. Accessed October 18, 2018. | ||
Sullivan SD, Ramsey SD, Lee TA. The economic burden of COPD. Chest. 2000;117(2 Suppl):5S–9S. | ||
Ding B, DiBonaventura M, Karlsson N, Bergström G, Holmgren U. A cross-sectional assessment of the burden of COPD symptoms in the US and Europe using the national health and wellness survey. Int J Chron Obstruct Pulmon Dis. 2017;12:529–539. | ||
Increase Expected in Medical Care Costs for COPD [homepage on the Internet]. Centers for Disease Control and Prevention; 2014. Available from: https://www.cdc.gov/features/ds-copd-costs/. Accessed January 19, 2017. | ||
Bourbeau J, Casan P, Tognella S, Haidl P, Texereau JB, Kessler R. An international randomized study of a home-based self-management program for severe COPD: the COMET. Int J Chron Obstruct Pulmon Dis. 2016;11:1447–1451. | ||
Kessler R, Casan-Clara P, Koehler D, et al. COMET: a multicomponent home-based disease-management programme versus routine care in severe COPD. Eur Respir J. 2018;51(1):1701612. | ||
Reed SD, Anstrom KJ, Bakhai A, et al. Conducting economic evaluations alongside multinational clinical trials: toward a research consensus. Am Heart J. 2005;149(3):434–443. | ||
Gray A, Clarke P, Wolstenholme J, Wordsworth S. Applied Methods of Cost-Effectiveness Analysis in Health Care. 1st ed. Oxford, UK: Oxford University Press; 2011. | ||
Henderson AR. The bootstrap: a technique for data-driven statistics. using computer-intensive analyses to explore experimental data. Clinica Chimica Acta. 2005;359(1–2):1–26. | ||
Glick HA, Doshi JA, Sonnad SS, Polsky D. Economic Evaluation in Clinical Trials. 2nd ed. Oxford, UK: Oxford University Press; 2015. | ||
van der Schans S, Goossens LMA, Boland MRS, et al. Systematic review and quality appraisal of cost-effectiveness analyses of pharmacologic maintenance treatment for chronic obstructive pulmonary disease: methodological considerations and recommendations. Pharmacoeconomics. 2017;35(1):43–63. | ||
McGarvey L, Lee AJ, Roberts J, Gruffydd-Jones K, McKnight E, Haughney J. Characterisation of the frequent exacerbator phenotype in COPD patients in a large UK primary care population. Respir Med. 2015;109(2):228–237. | ||
Pasquale MK, Sun SX, Song F, Hartnett HJ, Stemkowski SA. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare population. Int J Chron Obstruct Pulmon Dis. 2012;7:757–764. | ||
Andersson FL, Svensson K, Gerhardsson de Verdier M. Hospital use for COPD patients during the last few years of their life. Respir Med. 2006;100(8):1436–1441. | ||
Sintonen H, Weijnen T, Nieuwenhuizen M. Comparison of EQ-5D VAS valuations: analysis of background variables. In: Brooks R, Rabin R, de Charro F, editors. The Measurement and Valuation of Health Status Using EQ-5D: A European Perspective. Dordrecht: Springer; 2003:81–101. | ||
Bourbeau J, Julien M, Maltais F, et al; Chronic Obstructive Pulmonary Disease axis of the Respiratory Network Fonds de la Recherche en Santé du Québec. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: a disease-specific self-management intervention. Arch Intern Med. 2003;163(5):585–591. | ||
Gadoury MA, Schwartzman K, Rouleau M, et al; Chronic Obstructive Pulmonary Disease axis of the Respiratory Health Network, Fonds de la recherche en santé du Québec (FRSQ). Self-management reduces both short- and long-term hospitalisation in COPD. Eur Respir J. 2005;26(5):853–857. | ||
Zoumot Z, Jordan S, Hopkinson NS. Emphysema: time to say farewell to therapeutic nihilism. Thorax. 2014;69(11):973–975. |
Supplementary material
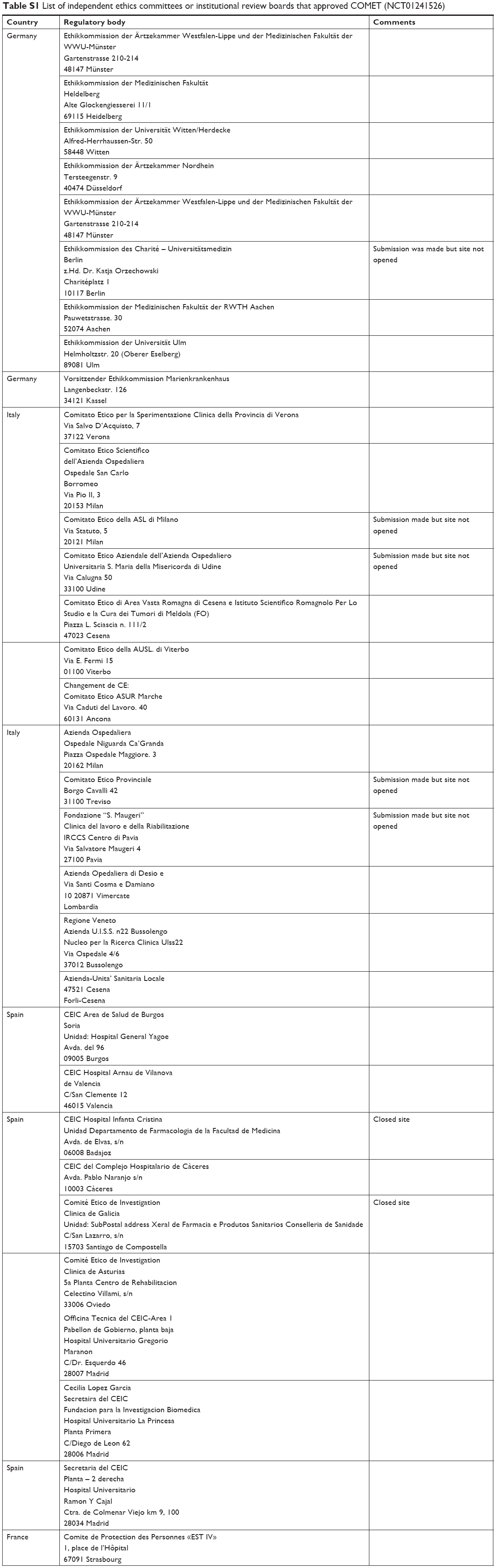 | Table S1 List of independent ethics committees or institutional review boards that approved COMET (NCT01241526) |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.