Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Cost-Effectiveness of Once-Daily, Single-Inhaler Indacaterol Acetate/ Glycopyrronium Bromide/ Mometasone Furoate in Patients with Uncontrolled Moderate-to-Severe Asthma in Canada
Authors Mtibaa M, Gupta S, Muthukumar M, Marvel J ![]() , Kaur H
, Kaur H ![]() , Ishikawa R, Olivenstein R
, Ishikawa R, Olivenstein R
Received 16 September 2021
Accepted for publication 11 November 2021
Published 3 December 2021 Volume 2021:13 Pages 957—967
DOI https://doi.org/10.2147/CEOR.S336915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Mondher Mtibaa,1 Subhajit Gupta,2 Madhusubramanian Muthukumar,2 Jessica Marvel,3 Harneet Kaur,2 Ryotaro Ishikawa,3 Ron Olivenstein4
1Novartis Pharmaceuticals Canada Inc., Dorval, Quebec, Canada; 2Novartis Healthcare Private Limited, Hyderabad, India; 3Novartis Pharma AG, Basel, Switzerland; 4McGill University, Montreal, Quebec, Canada
Correspondence: Mondher Mtibaa
Novartis Pharmaceuticals Canada Inc., 385 Bouchard Blvd., Dorval, Quebec, H9S 1A9, Canada
Tel +1 514 631-6775 ext. 1367
Email [email protected]
Purpose: We evaluated the cost-effectiveness of high-dose indacaterol acetate (IND)/glycopyrronium bromide (GLY)/mometasone furoate (MF) (150/50/160 μg, once daily) compared with high-dose salmeterol/fluticasone (SAL/FLU; 50/500 μg, twice daily)+tiotropium (TIO; 5 μg, once daily) (SAL/FLU+TIO) and with high-dose SAL/FLU (50/500 μg, twice daily) for the treatment of inadequately controlled moderate-to-severe asthma.
Patients and Methods: A Markov model estimated the incremental cost-effectiveness ratio of treatment with high-dose IND/GLY/MF compared with SAL/FLU+TIO and high-dose IND/GLY/MF compared with SAL/FLU. The model included three health states (day-to-day symptoms without exacerbations, day-to-day symptoms with exacerbations, and death) with a 4-week cycle length. A lifetime time horizon was used. Exacerbation rates and utility values were derived from ARGON and IRIDIUM clinical trials. Canadian dollars (CAD$, 2020) were applied.
Results: IND/GLY/MF was the less costly and more effective treatment strategy compared with SAL/FLU+TIO and SAL/FLU in the base-case analyses. IND/GLY/MF had lower costs (CAD $33,501 versus CAD $50,907) and higher quality-adjusted life-years (QALYs) (18.37 versus 18.06 QALYs) compared with SAL/FLU+TIO. Compared with SAL/FLU, IND/GLY/MF had lower costs (CAD $33,408 versus CAD $36,577) and higher QALYs (19.33 versus 19.04 QALYs). IND/GLY/MF was the most cost-effective option in all scenarios tested.
Conclusion: IND/GLY/MF was cost-effective at a willingness-to-pay threshold of CAD $50,000/QALY in patients with uncontrolled, moderate-to-severe asthma versus SAL/FLU+TIO and SAL/FLU in the base case and all scenarios tested.
Keywords: moderate to severe asthma, indacaterol acetate, glycopyrronium bromide, mometasone furoate, cost-effectiveness, health care payer perspective, Canada, uncontrolled asthma
Introduction
Asthma is a common chronic inflammatory disease of the airways that can cause breathlessness, tightness in the chest, coughing, wheezing, limitation of activity, and flare-ups that may require urgent health care and can be fatal.1 The global prevalence of asthma is estimated to be 358 million and might increase to 400 million by 2025.2 Asthma severity can be categorized as mild, moderate, or severe.1 The severity of asthma is assessed retrospectively from the level of treatment required to control symptoms and exacerbations (ie, flare-ups of respiratory symptoms). Moderate asthma can be controlled with low-dose inhaled corticosteroids (ICS)/long-acting beta2-agonists (LABA) or medium-dose ICS.3 Severe asthma can require treatment with high-dose ICS in addition to a second controller and may still remain uncontrolled despite this therapy.3 Uncontrolled asthma increases the likelihood of patients experiencing severe exacerbations that might require hospital admissions or emergency department (ED) visits.3–5 These events can have considerable impacts on health care costs and health-related quality of life (HRQoL).
Although patients with severe asthma comprise only 10% to 20% of the total asthma population, this population accounts for up to 50% of all asthma-related costs.6 Approximately 8.4% (~2.6 million) of Canadians aged ≥12 years have reported receiving a diagnosis of asthma.7 Annual direct costs observed in Canada varied across provinces, with a range of $46 million (Canadian dollars [CAD$]; at the time of the study, 1 Canadian dollar was equivalent to 75 US cents) in British Columbia to CAD $141 million in Ontario.8 Studies suggest that moderate-to-severe asthma remains uncontrolled in up to 70% of patients despite having received treatment according to asthma management guidelines, with a range of 25% to 59% in Canada.9–11
Recently a once-daily, single-inhaler combination has been developed for adults whose asthma has not been adequately controlled with a maintenance LABA and an ICS. It is a combination of indacaterol acetate, a LABA, glycopyrronium bromide, a long-acting muscarinic antagonist (LAMA), and mometasone furoate, an ICS (IND/GLY/MF 150/50/160 μg). Two clinical trials have been completed for IND/GLY/MF, including a head-to-head comparison with high-dose salmeterol/fluticasone (SAL/FLU, 50/500 µg, twice daily) medium-dose IND/MF (150/160µg, once daily), and high-dose IND/MF (150/320 µg, once daily) in IRIDIUM12 [ClinicalTrials.gov: national clinical trial number (NCT) 02571777] and a head-to-head comparison with high-dose SAL/FLU (50/500 µg, twice daily) + tiotropium (TIO 5µg, once daily) in ARGON13 (ClinicalTrials.gov: NCT03158311). IND/GLY/MF 150/50/160 μg is the first single-inhaler LABA/LAMA/ICS combination approved for asthma in Canada (approved on July 2, 2020). A recently published cost-effectiveness study from an Italian Health Service perspective has shown high-dose IND/GLY/MF to be cost-effective compared with SAL/FLU and SAL/FLU+TIO,14 but literature on this treatment has not been published for Canada.
The purpose of this study was to evaluate, from a Canadian publicly funded health care payer perspective, the cost-effectiveness of high-dose IND/GLY/MF as a maintenance treatment for asthma in adult patients who are not adequately controlled despite using maintenance treatment with a combination of a LABA and a medium or high-dose ICS.
Materials and Methods
Model Overview
A Markov model with a cycle length of 4 weeks was developed using Excel (Microsoft, WA, United States) and R (The R Foundation, Vienna, Austria) to determine the incremental cost-effectiveness ratio (ICER) of high-dose IND/GLY/MF (150/50/160 μg, once daily) versus high-dose SAL/FLU+TIO (50/500 µg, twice daily + 5 µg, once daily) and high-dose SAL/FLU (50/500 µg, twice daily) over a lifetime time horizon (Figure 1). The model structure was adapted from cost-effectiveness models of asthma treatments submitted to the National Institute for Health and Care Excellence (NICE).15–17 Assumptions used to develop the model are presented in Table S-1. Cost-effectiveness was estimated as the incremental cost per quality-adjusted life-year (QALY) gained.18–20 The model population was composed of patients (aged ≥18 years) with a diagnosis of moderate-to-severe asthma not adequately controlled by a maintenance combination of a LABA and a medium- or high-dose ICS. The model consisted of three major health states: day-to-day symptoms without exacerbations, day-to-day symptoms with exacerbations, and death. Patients started in the “day-to-day asthma symptoms without exacerbations” state, which captured the day-to-day quality of life associated with high-dose IND/GLY/MF compared with the comparator treatments.
 |
Figure 1 Markov model. Abbreviations: ED, emergency department; OCS, oral corticosteroid; SoC, standard of care. |
In each cycle, patients could transition from a “day-to-day symptoms state without exacerbations” to a “day-to-day symptoms with exacerbations” health state and might experience one of three types of clinically significant severe exacerbations: an exacerbation requiring treatment with oral corticosteroid (OCS) burst, an exacerbation requiring an ED visit, or an exacerbation requiring hospitalization. Patients might also experience moderate exacerbations, which were defined per the ARGON trial21 as the occurrence of two or more of the following symptoms: shortness of breath, cough, wheezing, and chest tightness for at least two consecutive days; 50% increase in short-acting beta2-adrenergic agonist use compared with baseline; and 20% decrease in forced expiratory volume in 1 second from baseline value. All patients in the exacerbation health state were assumed to transition back to the no exacerbation state at the end of the 4-week cycle. Death was an absorbing health state, which included asthma-related death due to exacerbations and age- or gender-related mortality. However, since no asthma-related deaths were reported in the clinical trials, asthma mortality has not been included in the base case. Similarly, adverse events were not included in the base case due to the low incidence among all treatments included in the clinical trials.12,13 Discontinuation from the assigned treatment was not accounted for in the base case but was included in a scenario analysis where those who discontinued from high-dose IND/GLY/MF or high-dose SAL/FLU+TIO switched to SAL/FLU high dose.
The length of the model cycle of 4 weeks was selected to correspond with the average duration of an asthma exacerbation and to be consistent with the recent NICE economic evaluations of asthma in the United Kingdom (UK).16,22 Results were presented in a cost-effectiveness plane of incremental costs and QALYs. The ICERs were calculated as the difference in total costs between two interventions relative to the difference in total QALYs (Figure S-1). A cost-effectiveness acceptability curve was generated based on Monte Carlo simulations to understand the relationship between the willingness-to-pay threshold23–25 and the probability of IND/GLY/MF being cost-effective versus SAL/FLU and IND/GLY/MF being cost-effective versus SAL/FLU+TIO.
This economic analysis is not considered research involving human subjects in accordance with section 3.1.2 of the Public Health Agency of Canada’s Research Ethics Board’s Operational Policy Framework, and thus review by an institutional review board was not required.
Model Inputs
Clinical Data
The rate of transition in each model cycle from the no exacerbation health state to the exacerbation health state and the proportion of each type of exacerbation were dependent upon the therapy a patient received. The rate of transition to severe exacerbation was estimated by multiplying the overall severe exacerbation rate by the proportion of each type of treatment required for the severe exacerbation, as presented in Table 1 (eg, OCS burst exacerbation rate = overall severe exacerbation rate × proportion of OCS burst exacerbations). The rate of transition to moderate exacerbation was estimated as the difference between the overall exacerbation rate and the overall severe exacerbation rate. The duration of all asthma exacerbations was assumed to be less than or equal to the cycle length. Thus, all patients in the exacerbation health state transitioned back to the no exacerbation health state at the end of each 4-week cycle. The impact of each type of exacerbation was determined by applying a utility decrement and a cost to treat that exacerbation as described below. An annual discount rate of 1.5% was applied to outcomes and costs.4
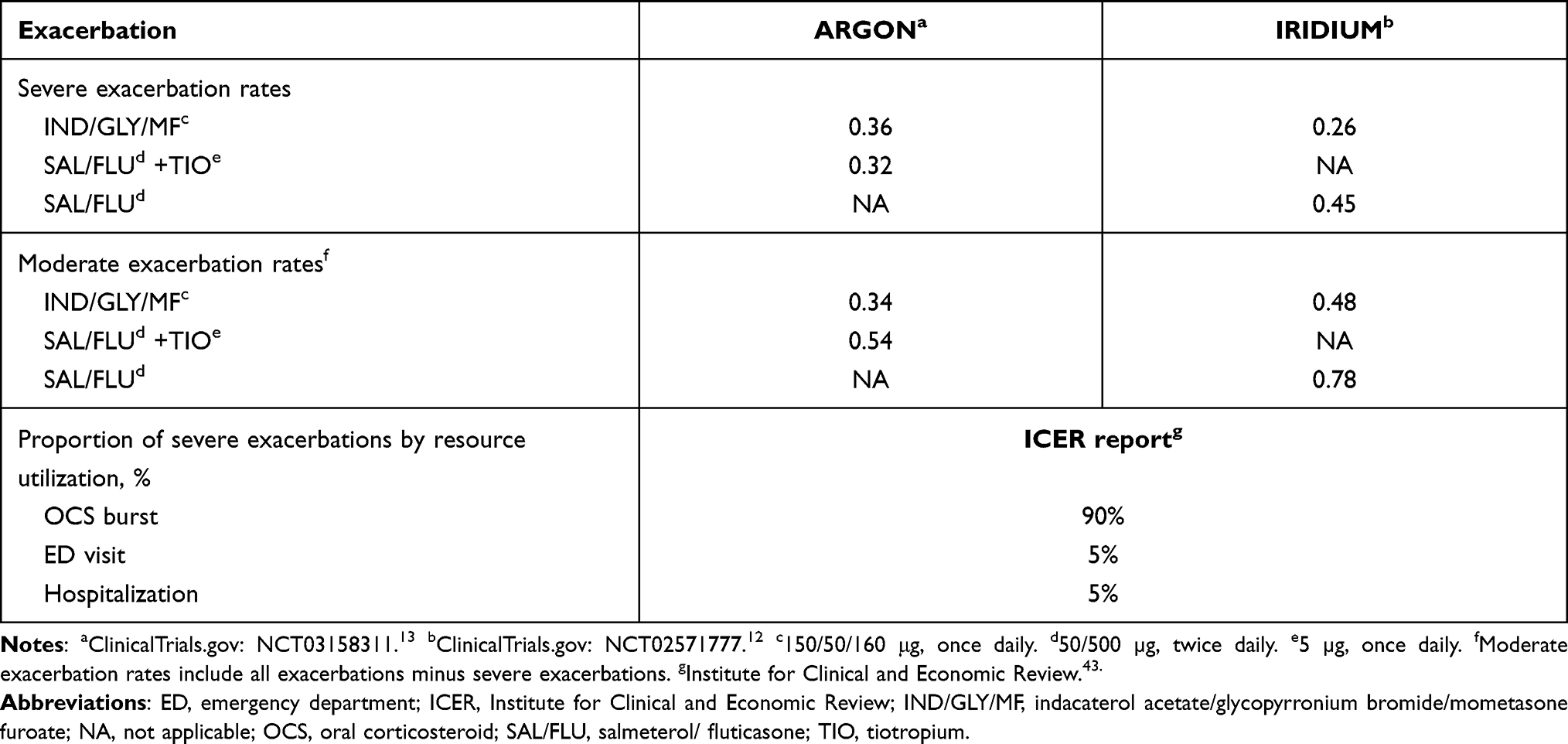 |
Table 1 Annualized Exacerbation Rates and Proportion of Severe Exacerbations by Resource Utilization |
Utility Data
The utility values for the “day-to-day asthma symptoms without exacerbations” state for the analysis comparing IND/GLY/MF with SAL/FLU+TIO were 0.755 for IND/GLY/MF and 0.742 for SAL/FLU+TIO. These utility values were derived from the ARGON13 trial and were based on reported day-to-day symptom utilities according to the Asthma Quality of Life Questionnaire (AQLQ). The AQLQ is a 32-item asthma-specific questionnaire designed to measure functional impairments that are most important to patients with asthma.26,27 The overall AQLQ score is the mean response to all 32 questions. Changes in scores of 0.5 between any two assessments can be considered clinically important.28 The AQLQ values from the ARGON trial were mapped onto the EQ-5D by using a published mapping function by the Sheffield Health Economics Group.29 For the analysis comparing IND/GLY/MF with SAL/FLU, the utility values used were 0.775 for IND/GLY/MF and 0.766 for SAL/FLU. These utility values were obtained from the EQ-5D values collected in the IRIDIUM trial.12 These values represent the overall utility of patients on each of these treatment options at the 52-week time point.
An estimated disutility of −0.1 was associated with both OCS burst and ED visit, and a disutility of −0.2 was associated with hospitalization.30 These disutilities were applied to the day-to-day asthma symptoms for those with an exacerbation. The duration of the utility loss was assumed to be 4 weeks (equal to the cycle length), as it may take a patient up to 4 weeks to recover from each exacerbation.
Cost Data
All cost inputs are presented in CAD$. Where necessary, costs were adjusted to 2020 Canadian dollars using the Bank of Canada inflation calculator.31 Drug costs were calculated based on the strength and frequency of administration contained in respective product labeling (Table 2). The cost of exacerbations was derived by using the health care resource use and associated unit costs as described in Tables S-2 and S-3. The cost per exacerbation leading to an ED visit was CAD $538.06, leading to hospitalization was CAD $4,649.38, and leading to OCS burst was CAD $78.07. No additional costs were added for moderate exacerbations.
 |
Table 2 Drug Costs |
Probabilistic Sensitivity Analyses
Probabilistic analyses were conducted to account for parameter uncertainty in the model. As part of the probabilistic analyses, Monte Carlo simulations were used to propagate uncertainty in the model by sampling the value for each input parameter according to its distribution (Tables S-4 and S-5). A total of 1000 simulations were conducted to ensure stability of model parameters.
Scenario Analyses
Scenario analyses were performed by using ARGON trial data for a comparison of IND/GLY/MF with SAL/FLU+TIO to explore the impact of changes in the discount rate, the time horizon, the societal perspective, and discontinuation rates. The reference discount rate in the discount rate scenario was changed from 1.5% (base case) to 0% and 3%. The duration for the time horizon scenario was 10 years instead of a lifetime (base case), which enabled exploration of the impact of extrapolation of downstream costs and effects on the results. The societal perspective included productivity costs for lost time to participate in paid labor for the patients in addition to health care costs. The absenteeism-related productivity loss was calculated as “productivity loss = proportion of population working × percentage of working days lost × average productivity per day worked (mean wage).” The percentage of working days lost, measured by using the Work Productivity and Activity Impairment Questionnaire in the IRIDIUM trial was estimated to be 3.2% for IND/GLY/MF and 3.4% for SAL/FLU+TIO, and the average cost per day of work missed was estimated to be $225.73. The additional productivity loss from “presenteeism” (being less productive while at work) was not included in this scenario analysis. A scenario analysis was performed to include the impact of discontinuation from the initial treatment using data from the ARGON trial. A discontinuation rate of 4.60% was applied to IND/GLY/MF and 5.70% was applied to SAL/FLU+TIO, and, after discontinuation, patients were assumed to return to SAL/FLU and therefore incur SAL/FLU efficacy, outcomes, and costs.
Results
Base-Case Analysis
The disaggregated costs and exacerbation outcomes comparing IND/GLY/MF with SAL/FLU+TIO based on the ARGON trial and with SAL/FLU based on the IRIDIUM trial are presented in Table 3. The total cost of CAD $33,501 for IND/GLY/MF was substantially less than the total cost for SAL/FLU+TIO of CAD $50,907 over a lifetime time horizon. Additionally, the number of severe and moderate exacerbations per patient were lower for IND/GLY/MF compared with SAL/FLU+TIO (17.12 versus 21.01 exacerbations) over the lifetime time horizon. However, exacerbation costs were more expensive for IND/GLY/MF due to higher event rates of severe exacerbations. The QALYs were higher for IND/GLY/MF compared with SAL/FLU+TIO (18.37 versus 18.06 QALYs), owing to the reduction in exacerbations and its associated disutility. In this analysis, IND/GLY/MF was less costly and more effective than SAL/FLU+TIO and had an 85.8% probability of being cost-effective at a willingness-to-pay threshold of CAD $50,000/QALY (Figure 2A).
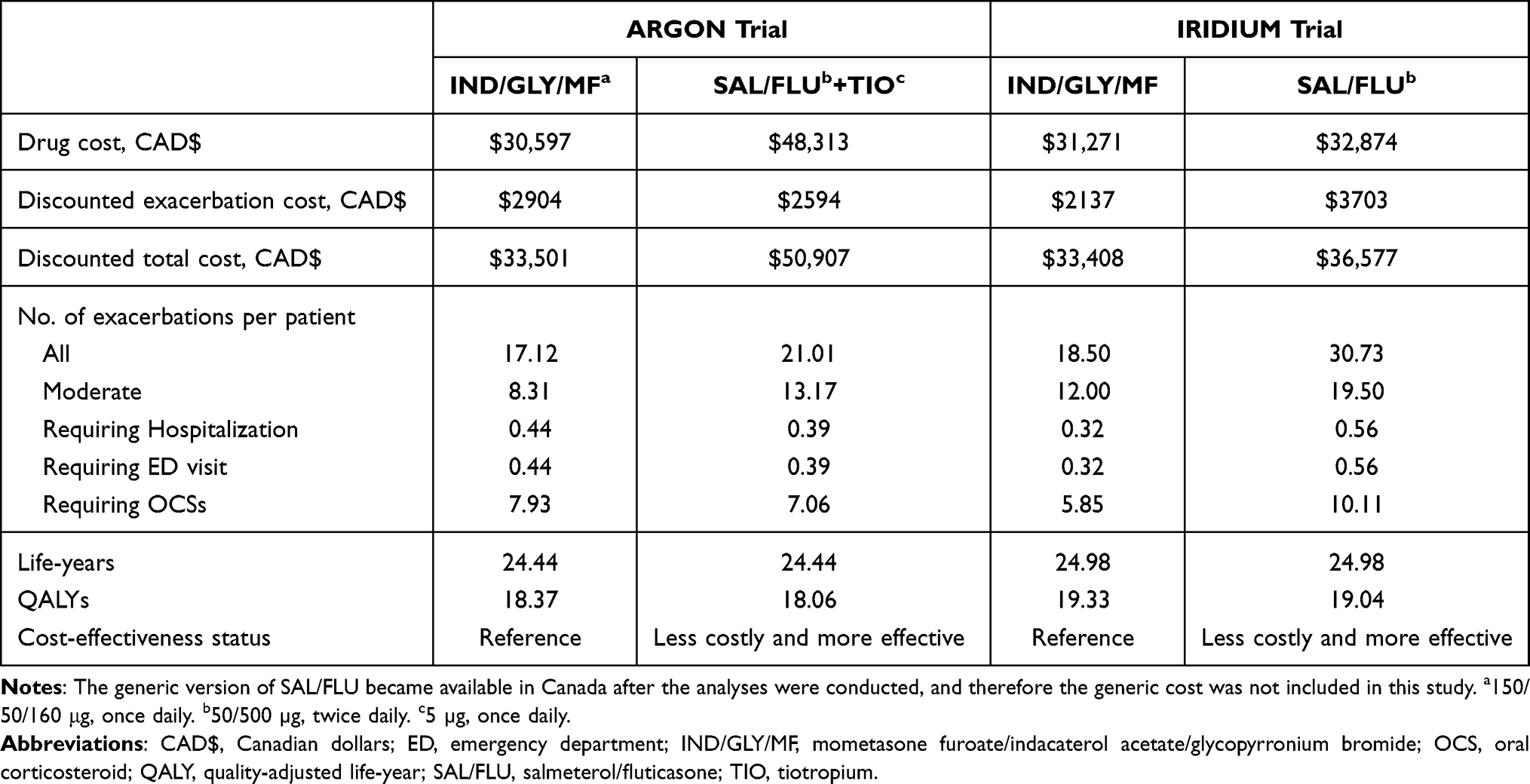 |
Table 3 Disaggregated Analysis Results |
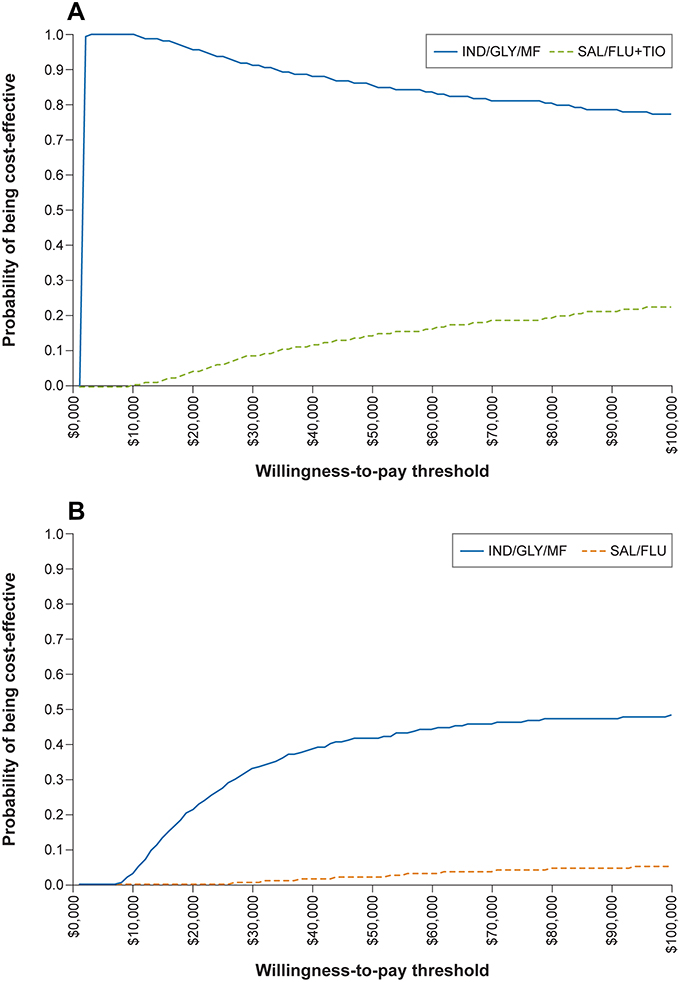 |
Figure 2 Cost-effectiveness acceptability curves using data derived from the (A) ARGON and (B) IRIDIUM trials. Abbreviations: IND/GLY/MF, mometasone furoate/indacaterol acetate/glycopyrronium bromide; SAL/FLU, salmeterol/fluticasone; TIO, tiotropium. |
The disaggregated costs and exacerbation outcomes were also lower for IND/GLY/MF when compared with SAL/FLU based on IRIDIUM trial data. The total cost of CAD $33,408 for IND/GLY/MF was less than the total cost for SAL/FLU of CAD $36,577 over a lifetime time horizon. The number of exacerbations per patient were again lower for IND/GLY/MF compared with SAL/FLU (18.50 versus 30.73 exacerbations) over the lifetime time horizon, which lowered exacerbation costs for IND/GLY/MF. The QALYs were again higher for IND/GLY/MF compared with SAL/FLU (19.33 versus 19.04 QALYs), owing to the higher reduction in exacerbations and its associated disutility. In this analysis, IND/GLY/MF was less costly and more effective than SAL/FLU and had a 42.7% probability of being cost-effective at a willingness-to-pay threshold of CAD $50,000/QALY (Figure 2B). For treatments in both trials, there was no difference in the life-years, as the age- and gender-related mortality rates are the same for all the treatments. Probabilistic scenario analyses demonstrated that varying parameters had limited impact on the results (Figure 3).
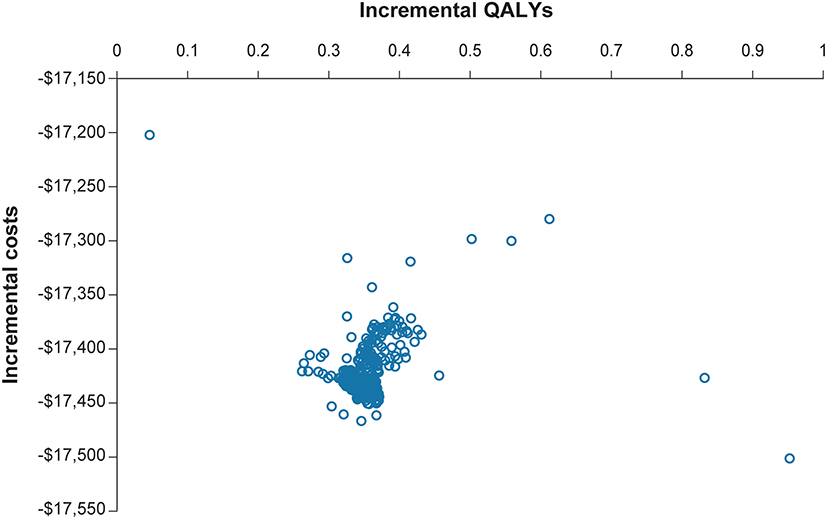 |
Figure 3 Scatterplot of the probabilistic scenario analyses. |
Scenario Analyses
IND/GLY/MF also was less costly and more effective than SAL/FLU+TIO in the discount rate, time horizon, societal perspective, and discontinuation scenarios (Table 4). When the discount rate was changed from 1.5% to 0%, IND/GLY/MF demonstrated lower total costs (CAD $42,805 versus $65,061) and higher QALYs (23.47 versus 23.08 QALYs). When the discount rate was changed from 1.5% to 3%, IND/GLY/MF demonstrated lower total costs (CAD $26,981 versus $40,998) and higher QALYs (14.79 versus 14.58 QALYs). When the time horizon was changed from lifetime to 10 years, IND/GLY/MF demonstrated lower total costs (CAD $13,561 versus $20,575) and higher QALYs (7.44 versus 7.32 QALYs). When the perspective was changed from publicly funded health care payer to societal, IND/GLY/MF demonstrated lower total costs (CAD $61,191 versus $80,403) and higher QALYs (18.42 versus 18.08 QALYs). When discontinuation was included, IND/GLY/MF demonstrated lower total costs (CAD $33,498 versus $50,893) and higher QALYs (18.41 versus 18.09 QALYs).
 |
Table 4 Results of Scenario Analyses Using ARGON Trial Data |
Discussion
This cost-utility study is the first to evaluate the incremental cost-effectiveness of IND/GLY/MF in the treatment of patients with moderate-to-severe asthma not adequately controlled with maintenance combination of a LABA and a medium- or high-dose ICS using a Canadian publicly funded health care payer perspective. In each base-case analysis, IND/GLY/MF was less costly and more effective than both SAL/FLU+TIO and SAL/FLU. IND/GLY/MF also had the highest probability of being cost-effective at most willingness-to-pay thresholds compared with SAL/FLU+TIO and SAL/FLU. For each of the four scenario analyses conducted using ARGON trial data, IND/GLY/MF still remained the most cost-effective treatment option, which provides support to results in the base case.
The base-case model included only direct health care costs in order to focus on the publicly funded health care payer perspective. Approximately 3% of patients missed days of work due to asthma-related symptoms in the IRIDIUM trial,12,15 which suggests productivity losses due to presenteeism and absenteeism imposed a substantial contribution to indirect costs. After absenteeism was incorporated into the scenario analysis, IND/GLY/MF continued to demonstrate lower total costs and higher QALYs compared with SAL/FLU+TIO (CAD $61,191 and 18.42 QALYs versus CAD $80,403 and 18.08 QALYs, respectively).
Willson et al32 compared high-dose ICS/LABA with add-on TIO versus high-dose ICS/LABA without add-on TIO in a cost-effectiveness analysis that used a similar model to that used in our analysis. The study population were patients whose asthma remained uncontrolled or symptomatic despite treatment with high-dose ICS/LABA. As with our base-case analysis, this model did not explicitly account for the costs of adverse events or loss of productivity. Other inputs and outputs were also similar. The effectiveness measure for both models was the QALY, which was calculated from HRQoL measures, including the EQ-5D. Willson et al32 considered direct costs only to the UK National Health Service (NHS), and we assessed only costs from a Canadian publicly funded health care payer perspective. Compared with high-dose ICS/LABA, add-on TIO had an estimated incremental cost per QALY of £21,906 over a lifetime horizon. In a scenario analysis, Willson et al32 found their model was sensitive to variations in time horizon when the time horizon was shortened from a lifetime horizon to 5 years or less. In contrast, our base-case analysis using data from the IRIDIUM trial estimated that IND/GLY/MF had both higher QALYs and lower costs than SAL/FLU. Also, for each of the four scenario analyses conducted using ARGON trial data, IND/GLY/MF still remained the most cost-effective treatment option, which supports the results in the base case.
Although multiple therapies for asthma are available, a substantial proportion of patients with moderate-to-severe asthma do not have adequate symptom control. Treatment nonadherence, the use of multiple inhalers, and critical errors in inhaler handling are all associated with uncontrolled, moderate-to-severe asthma.33 The probability of experiencing exacerbations, the need for emergency care and hospitalization, and the negative impact on HRQoL are all increased with uncontrolled asthma.34–38 Improving treatment adherence could improve asthma control. Patients prefer fixed-dose combination inhalers and once-daily dosing,39–41 which also help reduce treatment errors. Furthermore, a rapid and sustained onset of action could encourage patient compliance through early symptom relief.42 The majority of marketed LABA/ICS products have a twice-daily regimen, which suggests current treatment options are not meeting the preferences of patients with uncontrolled, moderate-to-severe asthma.
IND/GLY/MF is the first once-daily, single-inhaler, LABA/LAMA/ICS approved for asthma in Canada (approved on July 2, 2020). The efficacy of IND/GLY/MF has been supported by two phase 3 trials (IRIDIUM and ARGON)12,13 and has a favorable safety and tolerability profile compared with SAL/FLU+TIO and SAL/FLU. The economic evaluation presented here uses data from these clinical trials to provide further information about the cost-effectiveness of using IND/GLY/MF in the treatment of uncontrolled, moderate-to-severe asthma.
One limitation of this cost-effectiveness study was the extrapolation of 26-week and 1-year trial data used as inputs to a lifetime time horizon for the model. However, the scenario analysis incorporating a 10-year time horizon still found that IND/GLY/MF was less costly and more effective than the comparator treatment. Another limitation is that cost differences might not be sustained between the regimens, although we used the most accurate pricing data available at the time of the study. A major strength of this model was the incorporation of data from clinical trials to inform the utility data inputs.
Conclusions
Treatment with IND/GLY/MF is cost-effective at a willingness-to-pay threshold of CAD $50,000/QALY in patients with uncontrolled, moderate-to-severe asthma compared with SAL/FLU+TIO or SAL/FLU. Furthermore, scenario analyses conducted by varying different parameters confirm these results. The results of this study provide a reference for the economic impact of IND/GLY/MF from the publicly funded health payer perspective in Canada and may be generalizable to other health care systems with comparable pricing structures.
Abbreviations
AQLQ, Asthma Quality of Life Questionnaire; CAD$, Canadian dollars; ED, emergency department; FLU, fluticasone; GLY, glycopyrronium bromide; HRQoL, health-related quality of life; ICER, incremental cost-effectiveness ratio; ICS, inhaled corticosteroid; IND, indacaterol acetate; LABA, long-acting beta agonist; LAMA, long-acting muscarinic antagonist; MF, mometasone furoate; NA, not applicable; NHS, National Health Service; NICE, National Institute for Health and Care Excellence; OCS, oral corticosteroid; QALY, quality-adjusted life-year; SAL, salmeterol; TIO, tiotropium; UK, United Kingdom; US, United States.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This economic evaluation is not considered research involving human subjects in accordance with section 3.1.2 of the Public Health Agency of Canada’s Research Ethics Board’s Operational Policy Framework and thus review by an institutional review board was not required.
Acknowledgments
The authors would like to acknowledge Brian Samsell of RTI Health Solutions for medical writing assistance and Kate Lothman of RTI Health Solutions for project management assistance. A portion of this paper was presented at Virtual ISPOR Europe 2020, 16–19 November 2020.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Financial support for the study was provided by Novartis Pharma AG. RTI Health Solutions received funding to provide editorial support in the form of manuscript writing, styling, and submission.
Disclosure
MM is an employee of Novartis Pharmaceuticals Canada Inc. SG and MaM were employees of Novartis Healthcare Private Limited when the study was conducted. JM and RI are employees of Novartis Pharma AG. HK is an employee of Novartis Healthcare Private Limited. RO is a consultant of Novartis Pharma AG but received no compensation for contributions to this study. RO also reports personal fees from Astra Zeneca, and Glaxo Smith Kline, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Asthma. Pocket Guide for Asthma Management and Prevention; 2016.
2. Soriano JB, Abajobir AA, Abate KH, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30293-X
3. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention; 2020. Available from: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf.
4. CADTH. Guidelines for the economic evaluation of health technologies. Canada; 2017. Available from: https://www.cadth.ca/sites/default/files/pdf/guidelines_for_the_economic_evaluation_of_health_technologies_canada_4th_ed.pdf.
5. Wenzel SE. Asthma: defining of the persistent adult phenotypes. Lancet. 2006;368(9537):804–813. doi:10.1016/S0140-6736(06)69290-8
6. Nunes C, Pereira AM, Morais-Almeida M. Asthma costs and social impact. Asthma Res Pract. 2017;3(1):1. doi:10.1186/s40733-016-0029-3
7. Statistics Canada. Catalogue no. 82-625-X. Health fact sheets, chronic conditions; 2016. Available from: https://www150.statcan.gc.ca/n1/pub/82-625-x/2017001/article/54858-eng.htm.
8. Ismaila AS, Sayani AP, Marin M, Su Z. Clinical, economic, and humanistic burden of asthma in Canada: a systematic review. BMC Pulm Med. 2013;13(1):70. doi:10.1186/1471-2466-13-70
9. Sadatsafavi M, Chen W, Tavakoli H, et al. Saving in medical costs by achieving guideline-based asthma symptom control: a population-based study. Allergy. 2016;71(3):371–377. doi:10.1111/all.12803
10. Sastre J, Fabbri LM, Price D, et al. Insights, attitudes, and perceptions about asthma and its treatment: a multinational survey of patients from Europe and Canada. World Allergy Organ J. 2016;9:13. doi:10.1186/s40413-016-0105-4
11. Nathan RA, Thompson PJ, Price D, et al. Taking aim at asthma around the world: global results of the asthma insight and management survey in the Asia-Pacific Region, Latin America, Europe, Canada, and the United States. J Allergy Clin Immunol Pract. 2015;3(5):734–742 e735. doi:10.1016/j.jaip.2015.04.013
12. ClinicalTrials.gov: NCT02571777. Study to compare the efficacy and safety of QVM149 with QMF149 in patients with asthma; 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT02571777.
13. ClinicalTrials.gov: NCT03158311. Study to compare QVM149 and free triple combination of Salmeterol/Fluticasone + Tiotropium (ARGON); 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT03158311.
14. Mangia PP, Gallo O, Ritrovato D, Pradelli L. Cost-utility analysis of fixed-dose combination of Indacaterol Acetate Glycopyrronium Bromide and Mometasone Furoate as a maintenance treatment in adult patients with asthma not adequately controlled with a maintenance combination of a long-acting beta-agonist and a high dose of an inhaled corticosteroid who experienced one or more asthma exacerbations in the previous year. Clin Drug Investig. 2021;41(9):785–794. doi:10.1007/s40261-021-01067-w
15. National Institute for Health and Care Excellence. Omalizumab for treating severe persistent allergic asthma. Technology Appraisal guidance [TA278]; 2013. https://www.nice.org.uk/Guidance/TA278.
16. National Institute for Health and Care Excellence. Final appraisal determination – mepolizumab for treating severe refractory eosinophilic asthma; 2016. Available from: https://www.nice.org.uk/guidance/ta431/documents/final-appraisal-determination-document.
17. National Institute for Health and Care Excellence. Benralizumab for treating severe eosinophilic asthma. Technology Appraisal guidance [TA565]; 2019. Available from: https://www.nice.org.uk/Guidance/TA565.
18. Akinbami LJ, Sullivan SD, Campbell JD, et al. Asthma outcomes: healthcare utilization and costs. J Allergy Clin Immunol. 2012;129(3 Suppl):S49–S64. doi:10.1016/j.jaci.2011.12.984
19. Ehteshami-Afshar S, Zafari Z, Hamidi N, FitzGerald JM, Lynd L, Sadatsafavi M. A systematic review of decision-analytic models for evaluating cost-effectiveness of asthma interventions. Value Health. 2019;22(9):1070–1082. doi:10.1016/j.jval.2019.03.016
20. Feng X, Kim DD, Cohen JT, Neumann PJ, Ollendorf DA. Using QALYs versus DALYs to measure cost-effectiveness: how much does it matter? Int J Technol Assess Health Care. 2020;36(2):96–103. doi:10.1017/S0266462320000124
21. Gessner C, Kornmann O, Maspero J, et al. Fixed-dose combination of indacaterol/glycopyrronium/mometasone furoate once-daily versus salmeterol/fluticasone twice-daily plus tiotropium once-daily in patients with uncontrolled asthma: a randomised, phase IIIb, non-inferiority study (ARGON). Respir Med. 2020;170:106021. doi:10.1016/j.rmed.2020.106021
22. National Institute for Health and Care Excellence. Benralizumab for treating severe asthma guidance; 2019. Available from: https://www.nice.org.uk/guidance/TA565/history.
23. Canadian Agency for Drugs and Technologies in Health. Pharmacoeconomic Report: Brolucizumab (Beovu). Indication: Treatment of Neovascular (Wet) Age-Related Macular Degeneration (AMD). Ottawa (ON): Novartis Pharmaceuticals Canada Inc.; 2020.
24. Canadian Agency for Drugs and Technologies in Health. Pharmacoeconomic Report: Eculizumab (Soliris). Indication: Adult Patients with Generalized Myasthenia Gravis. Ottawa (ON): Alexion Pharma Canada Corporation; 2020.
25. Khowaja AR, Krause C, Kennedy C, Ridout B, Carriere S, Mitton C. Cost-effectiveness of a province-wide quality improvement initiative for reducing potentially inappropriate use of antipsychotics in long-term care in British Columbia, Canada. Pharmacoecon Open. 2021;5(3):491–504. doi:10.1007/s41669-021-00267-6
26. Juniper EF, Guyatt GH, Ferrie PJ, Griffith LE. Measuring quality of life in asthma. Am Rev Respir Dis. 1993;147(4):832–838. doi:10.1164/ajrccm/147.4.832
27. Juniper EF, Guyatt GH, Epstein RS, Ferrie PJ, Jaeschke R, Hiller TK. Evaluation of impairment of health related quality of life in asthma: development of a questionnaire for use in clinical trials. Thorax. 1992;47(2):76–83. doi:10.1136/thx.47.2.76
28. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a minimal important change in a disease-specific quality of life questionnaire. J Clin Epidemiol. 1994;47(1):81–87. doi:10.1016/0895-4356(94)90036-1
29. Tsuchiya A, Brazier J, McColl E, Parkin D. Deriving preference-based single indices from non-preference based condition-specific instruments: converting AQLQ into EQ5D indices. The University of Sheffield School of Health and Related Research (ScHARR); 2002. Available from: https://www.sheffield.ac.uk/polopoly_fs/1.43197!/file/HEDS-DP-02-01.pdf.
30. Lloyd A, Price D, Brown R. The impact of asthma exacerbations on health-related quality of life in moderate to severe asthma patients in the UK. Prim Care Respir J. 2007;16(1):22–27. doi:10.3132/pcrj.2007.00002
31. Bank of Canada. Inflation calculator; 2020. Available from: https://www.bankofcanada.ca/rates/related/inflation-calculator/.
32. Willson J, Bateman ED, Pavord I, Lloyd A, Krivasi T, Esser D. Cost effectiveness of tiotropium in patients with asthma poorly controlled on inhaled glucocorticosteroids and long-acting beta-agonists. Appl Health Econ Health Policy. 2014;12(4):447–459. doi:10.1007/s40258-014-0107-8
33. Lougheed MD, Lemiere C, Ducharme FM, et al. Canadian thoracic society 2012 guideline update: diagnosis and management of asthma in preschoolers, children and adults. Can Respir J. 2012;19(2):127–164. doi:10.1155/2012/635624
34. McIvor RA, Boulet LP, FitzGerald JM, Zimmerman S, Chapman KR. Asthma control in Canada: no improvement since we last looked in 1999. Can Fam Physician. 2007;53(4):672–677.
35. Chapman KR, Boulet LP, Rea RM, Franssen E. Suboptimal asthma control: prevalence, detection and consequences in general practice. Eur Respir J. 2008;31(2):320–325. doi:10.1183/09031936.00039707
36. FitzGerald JM, Boulet LP, McIvor RA, Zimmerman S, Chapman KR. Asthma control in Canada remains suboptimal: The Reality of Asthma Control (TRAC) study. Can Respir J. 2006;13(5):253–259. doi:10.1155/2006/753083
37. Klomp H, Lawson JA, Cockcroft DW, et al. Examining asthma quality of care using a population-based approach. CMAJ. 2008;178(8):1013–1021. doi:10.1503/cmaj.070426
38. Pavord ID, Mathieson N, Scowcroft A, Pedersini R, Isherwood G, Price D. The impact of poor asthma control among asthma patients treated with inhaled corticosteroids plus long-acting beta2-agonists in the United Kingdom: a cross-sectional analysis. NPJ Prim Care Respir Med. 2017;27(1):17. doi:10.1038/s41533-017-0014-1
39. Murphy KR, Bender BG. Treatment of moderate to severe asthma: patient perspectives on combination inhaler therapy and implications for adherence. J Asthma Allergy. 2009;2:63–72. doi:10.2147/JAA.S4214
40. Johansson G, Stallberg B, Tornling G, et al. Asthma treatment preference study: a conjoint analysis of preferred drug treatments. Chest. 2004;125(3):916–923. doi:10.1378/chest.125.3.916
41. Balsbaugh TA, Chambers CV, Diamond JJ. Asthma controller medications: what do patients want? J Asthma. 1999;36(7):591–596. doi:10.3109/02770909909087296
42. Cazzola M, Beeh KM, Price D, Roche N. Assessing the clinical value of fast onset and sustained duration of action of long-acting bronchodilators for COPD. Pulm Pharmacol Ther. 2015;31:68–78. doi:10.1016/j.pupt.2015.02.007
43. Institute for Clinical and Economic Review. Biologic therapies for treatment of asthma associated with type 2 inflammation: effectiveness, value, and value-based price benchmarks. Final evidence report; 2018. Available from: https://icer.org/wp-content/uploads/2020/10/Asthma-Revised-Report-FOR-PUBLICATION-11.13.2018.pdf .
44. Government of Ontario. Ontario drug benefit formulary/Comparative drug index queen’s printer for Ontario 2020; 2020. Available from: https://www.formulary.health.gov.on.ca/formulary/.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.