Back to Journals » Risk Management and Healthcare Policy » Volume 16
Cost-Effectiveness Analysis of Pembrolizumab Plus Chemotherapy in Squamous Non–Small-Cell Lung Cancer in China
Authors Zhang X, Zhang H ![]() , Li LF, Feng L, Liu Q
, Li LF, Feng L, Liu Q ![]()
Received 7 July 2023
Accepted for publication 1 September 2023
Published 12 September 2023 Volume 2023:16 Pages 1849—1857
DOI https://doi.org/10.2147/RMHP.S429394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Xin Zhang,1,* Huixian Zhang,1,* Lan-Fang Li,1 Lei Feng,1 Qiao Liu2
1Department of Clinical Pharmacy, Affiliated Hospital of Jining Medical University, Jining Medical University, Jining, Shandong, People’s Republic of China; 2Department of Pharmacy, The Second Xiangya Hospital of Central South University, Central South University, Changsha, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiao Liu, Department of Pharmacy, The Second Xiangya Hospital of Central South University, Central South University, Changsha, Hunan, People’s Republic of China, Email [email protected]
Purpose: The five-year update data from the KEYNOTE-407 study have unveiled noteworthy improvements in survival outcomes achieved with pembrolizumab plus chemotherapy (Pembro+Chemo) compared to placebo plus chemotherapy (Placebo+Chemo) for patients with previously untreated metastatic squamous non-small cell lung cancer (NSCLC). Building upon this finding, our study sought to evaluate the cost-effectiveness of Pembro+Chemo, utilizing the latest available data, from the perspective of the Chinese health care system.
Patients and Methods: A Markov model was employed to compare the quality-adjusted life-year (QALY), life-year (LY), total cost, and incremental cost-effectiveness ratio (ICER) between Pembro+Chemo and Placebo+Chemo. The clinical and safety data were derived from the five-year update date of the KEYNOTE-407 study. Sensitivity analyses were conducted to assess the uncertainty of the model, and additional subgroup analyses were performed to explore specific subpopulations.
Results: For patients with previously untreated metastatic squamous NSCLC, the utilization of Pembro+Chemo resulted in a improvement of 0.61 quality-adjusted life years (QALYs) along with a cost reduction of $17,491.52 when compared to Placebo+Chemo. Notably, across various subgroups with different tumor proportion scores (TPS), Pembro+Chemo demonstrated enhanced QALYs and lower total costs.
Conclusion: From the perspective of the Chinese health care system, first-line Pembro+Chemo emerges as a dominant treatment option over Placebo+Chemo for the treatment of metastatic squamous NSCLC.
Keywords: pembrolizumab, cost-effectiveness, squamous NSCLC, KEYNOTE-407
Introduction
Lung cancer stands as the predominant cause of cancer-related deaths across globe, giving rise to an estimated 2.20 million new cases and 1.79 million deaths annually.1,2 Non-small cell lung cancer (NSCLC) constituted nearly 85% of all lung cancer cases, with squamous cell carcinoma representing a subtype associated with a comparatively diminished long-term survival rate, encompassing almost 18% of NSCLC occurrences.3,4 Patients with squamous NSCLC face considerable challenges in deriving benefits from targeted therapy reliant on predictive biomarkers, given that 80% of the diagnoses reveal an absence of driver gene mutations.5 However, there is renewed hope for patients with squamous NSCLC through the emergence of immunotherapy, particularly immune checkpoint inhibitors (ICIs) that target programmed death 1 (PD-1)/programmed death ligand 1 (PD-L1) signaling.6
Pembrolizumab (Keytruda) has the distinction of being the first ICI to receive approval from the United States Food and Drug Administration (FDA). This approval was granted due to its significantly greater survival benefits compared to chemotherapy in clinical trials.7–9 In addition, pembrolizumab in combination with chemotherapy has been approved in many countries for the treatment of metastatic NSCLC. The latest Guidelines of Chinese Society of Clinical Oncology (CSCO) for NSCLC recommend pembrolizumab plus chemotherapy (Pembro+Chemo) as a class 1A first-line treatment for metastatic squamous NSCLC, regardless of PD-L1 expression.10 This recommendation is based on the primary findings from the Phase 3 KEYNOTE-407 trial. A preceding cost-effectiveness analysis conducted by Wu et al in 2020, revealed that incorporating pembrolizumab into conventional chemotherapy lacks cost-effectiveness within China setting.11 However, it is important to acknowledge that their findings might not be directly apply to the present context in China due to two pivotal factors. Firstly, the previous analysis relied upon the initial discoveries of the KEYNOTE-407 trial without an adequate follow-up duration.7 The limited period of follow-up might have impeded a comprehensive assessment of the long-term toxic effects and subsequent anticancer therapy. Secondly, in order to enhance the accessibility of pembrolizumab in China, a patient assistance program (PAP) was implemented on January 1, 2021, resulting in a significant 88% reduction in the price of pembrolizumab and a consequent decline in drug-related expenditures.12,13 This remarkable benefits of this policy have not been accounted for in the previous research. Hence, it is imperative to assess the cost-effectiveness of combining pembrolizumab with chemotherapy, utilizing the most recent data from the KEYNOTE-407 trial, while considering the current national conditions in China.
A recent publication presenting a comprehensive five-year update on the KEYNOTE-407 study has provided extensive data on overall survival (OS) and progression-free survival (PFS), along with more precise information regarding adverse events (AEs) and subsequent anticancer therapies.14 Moreover, improvements in the accuracy of the crossover rate have been observed over time. These updates have led to significant changes in clinical inputs for assessing the cost-effectiveness assessment of Pembro+Chemo. Therefore, our objective was to conduct a de novo cost-effectiveness analysis of pembrolizumab among patients with previously untreated metastatic squamous NSCLC, taking into account these recent advancements and from the perspective of the Chinese healthcare system. Furthermore, we aimed to compare the cost-effectiveness of Pembro+Chemo with placebo plus chemotherapy (Placebo+Chemo) in subgroups with varying PD-L1 expression levels. This study aims to provide valuable insights for health policymakers, patients, and physicians, enabling them to make informed clinical decisions based on value-based considerations.
Materials and Methods
Overview
With the software TreeAge Pro (version 2021, https://www.treeage.com/) for mathematical modeling and R (version 4.0.4, http://www.r-project.org) for survival fitting, an economic evaluation was conducted to investigate the cost-effectiveness of Pembro+Chemo for patients with previously untreated metastatic squamous NSCLC from the Chinese health care perspective.
The efficacy and safety outcomes of Pembro+Chemo and Placebo+Chemo were obtained from the Phase III KEYNOTE-407 study (ClinicalTrials.gov identifier: NCT02775435). Since the data used in this study was obtained from published sources, the approval from ethical review was exempted by the Clinical Ethics Committee (EC) of affiliated hospital of Jining medical university according to the Measures for Ethical Review of Life Science and Medical Research Involving Humans (2023).15 This economic evaluation was guided by the Chinese guidelines for pharmacoeconomic evaluation (2020).16
Model Construction
In the present analysis, a Markov model was selected for its widespread application in cost-effectiveness research. These models excel at capturing the progression of chronic diseases by representing sequential events and transitions between different states over time.17 For economic evaluation, the Markov model we developed consisted of three mutually exclusive health statuses: progression-free disease (PFD), progressed disease (PD), and death (Figure 1). The patients in this model mirrored those in the KEYNOTE-407 study and had histologically or cytologically confirmed and previously untreated stage IV squamous NSCLC. Based on the KEYNOTE-407 trial,7,14 the sample sizes for PD-L1 subgroups were as follows: 194 patients with PD-L1 expression level less than 1%, 207 patients with PD-L1 expression level between 1% and 49%, and 146 patients with a PD-L1 expression level equal to or greater than 50%. Following the dosing interval in KEYNOTE-407, the Markov length cycle was set to 21 days. To ensure that all patients reached the terminal of death, a 30-year time horizon was set as the running time.
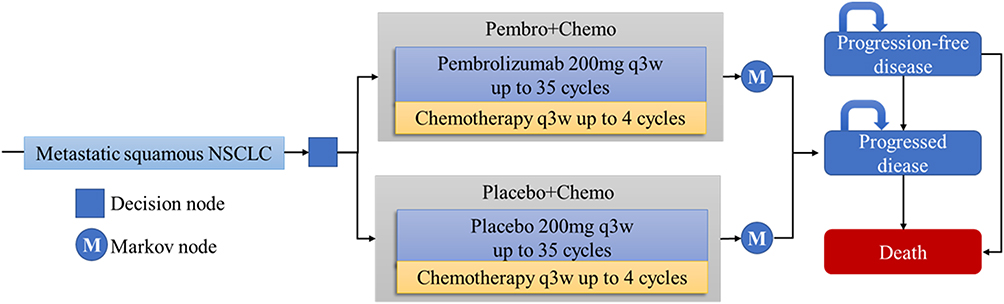 |
Figure 1 Diagram of Markov model. Abbreviations: NSCLC, non-small cell lung cancer; Pembro+Chemo, pembrolizumab plus chemotherapy; Placebo+Chemo, placebo plus chemotherapy. |
Model patients started from PFD health state and could turn to the rest health state based on transition probabilities. They were randomly assigned with a 1:1 ratio to receive first-line pembrolizumab or placebo every 3 weeks with carboplatin, paclitaxel, or nab-paclitaxel for 4 cycles, followed by pembrolizumab or placebo for up to 35 cycles. Detailed information on the first-line and pretreatment medications is provided in Tables S1 and S2, respectively. When patients progressed during first-line treatment could move to PD and receive subsequent anticancer therapies. Tables S3 and Table S4 provided additional information on subsequent anticancer therapies. Patients who were in the PD health state and did not receive subsequent anticancer therapy were modeled as receiving the best supportive care (BSC), and all patients were recommended for palliative care before death.10
The cumulative cost, quality-adjusted LYs (QALYs), and incremental cost-effectiveness ratio (ICER) were calculated and compared between the two competitive treatment regimens using this Markov model. Given that a special willing-to-pay (WTP) threshold has not been explicitly defined for China, we have interpreted our results in light of the WTP benchmark for ICER-based decision proposed by Cai et al.18 This benchmark suggests a threshold of 1.5 times China’s gross domestic product (GDP) per capita in 2022, equating to $19,112 per QALY.19 Pembro+Chemo was deemed cost-effective if its ICER fell below the predetermined threshold of WTP when compared to Placebo+Chemo. The cost was discounted at 5% annually in this study.20
Clinical Effectiveness
To ascertain the clinical effectiveness of the two competitive treatment regimens, this study relied on the utilization of QALYs. QALYs were calculated based on the transition probabilities between different health states. Initially, OS and PFS data for Pembro+Chemo and Placebo+Chemo groups were extracted using the GetData Graph Digitizer software (version 2.26; http://www.getdata-graphdigitizer.com/index.php), which was based on the Kaplan–Meier (KM) curves published in the KEYNOTE-407 trial. Subsequently, the reconstructed individual patient-level data were fitted with five commonly used survival distributions, namely exponential, Weibull, Log-normal, log-logistic and Gompertz distributions. This fitting process aimed to identify the optimal parametric survival distribution for the reconstructed data. To determine the best fit, a series of goodness-of-fit tests were conducted, including statistical evaluations such as the Akaike information criterion and Bayesian information criterion, as well as graphical assessments comparing the modeled curves against the KM curves. The results of these goodness-of-fit tests are presented in Table S5 and Figures S1–S4, providing insights into the accuracy of the fitted models. Finally, with the estimated distribution parameters, the transition probabilities between the PFD, PD, and death states were calculated.
Chinese-specific health utilities were used based on shen et al study and the assigned values for PFD health status were 0.856 and 0.768 for PD health status.21 The AEs-related disutilities coming from the treatment were also considered in this model and calculated as a frequency-weighted sum (Table S6).
Medical Costs
Direct medical costs, which consisted of costs of drug acquisition, subsequent anticancer therapy costs, AEs treatment, and other medical resource utilization (including medical service, best supportive care, and terminal care), were considered in this model. These costs were collected from the perspective of the Chinese healthcare system and reported in US dollars (USD) using an exchange rate of 1 USD, equivalent to 6.7261 Chinese Yuan (CNY) in 2022.
The latest bid-winning prices of drugs in Chinese public hospitals were derived from the Chinese Drug Bidding Database.22 The total costs of pembrolizumab were adjusted according to the PAP. To improve the affordability of immunotherapy for patients with cancer, PAP has been updated since 2021. This project was launched by the China Primary Health Care Foundation and aided by the Merck Pharmaceutical Industry in China. Patients only needed to pay for four cycles and could use pembrolizumab until disease progression. All grade III/IV AEs with ≥ 1% were considered, and these AEs costs were extracted from a local comprehensive hospital (Table S7). The duration of AEs (Table S6) was available from published articles. The proportion, cost, and disutility of the grade 3–4 AEs considered in the model are provided in Table S8. Other cancer-related management costs, including routine follow-up costs, best supportive care and terminal care costs, were obtained from published studies as with previous economic evaluations in China.23,24
Sensitivity Analysis
To validate our conclusion, sensitivity analyses were carried out to test some uncertainty parameters, including individual and multiple. Deterministic sensitivity analyses (DSA) were performed for individuals to investigate their influence on cost-effectiveness. For multiple, probabilistic sensitivity analyses (PSA) were conducted with 10,000 Monte Carlo simulations.25 The uncertainty of these parameters was reflected through plausible variation ranges and appropriate distributions outlined in Table S9.
Results
Base-Case Analysis
As displayed in Figures S1–S4, the OS and PFS imitated in our model are very similar to the cure in OS and PFS update dates after five years in KEYNOTE-407, regardless of the different tumor proportion scores (TPS), which means our model is credible.
For patients with previously untreated metastatic squamous NSCLC, Pembro+Chemo showed a 0.61 QALYs improvement in effectiveness but a cost reduction of $17,491.52 compared with Placebo+Chemo, leading to its dominance over Placebo+Chemo. For the subgroup with TPS ≥50%, Pembro+Chemo was associated with extended LYs and QALYs of 0.89 and 0.78 and lower costs of $33,822.83, respectively. In the subgroup with TPS between 1% and 49%, Pembro+Chemo revealed improved effectiveness with 0.99 and 0.86 for LYs and QALYs, respectively. $15,847.01 was reduced which was also dominant compared with Placebo+Chemo. For the less than 1% subgroup, the effectiveness improvements were 0.28 for LYs and 0.25 for QALYs. Costs were with reduction of $13,995.41, which was dominant compared with Placebo+Chemo, as well as the above two subgroups (Table 1).
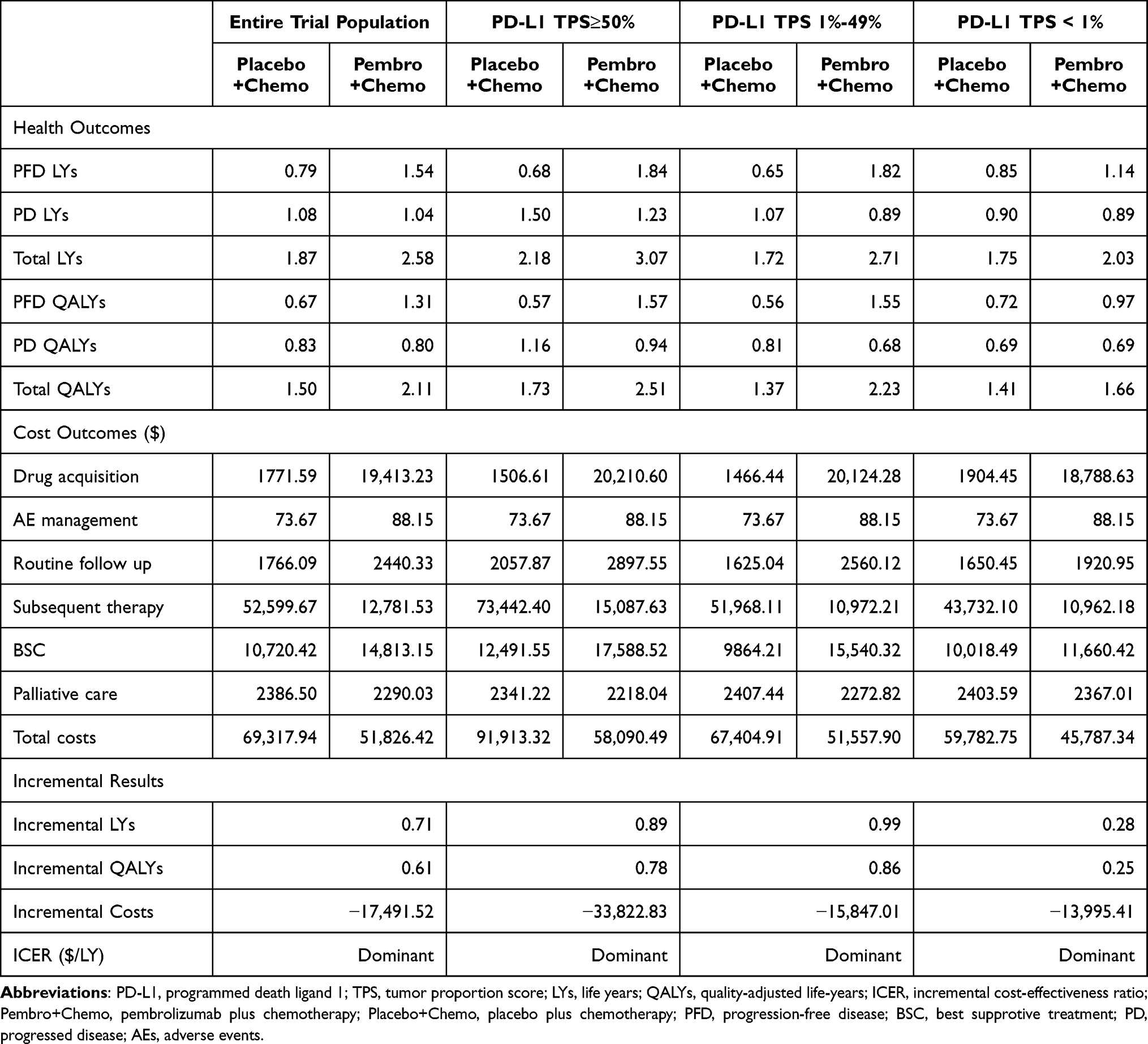 |
Table 1 Cost-Effectiveness Analysis Results |
Sensitivity Analysis
The results of the one-way sensitivity analysis were shown in the Tornado diagram (Figure 2 and Figures S5–S7), which indicated that the most influential variables were the subsequent therapy cost estimated for the Placebo+Chemo group and the pembrolizumab price per mg. Besides, the model was also sensitive to the subsequent therapy cost estimated for the Pembro+Chemo group, utility for PFD health status, and BSC cost per cycle. Overall, from the perspective of the Chinese healthcare system, when the parameters varied at the upper and lower limits, the ICER was always lower than the WTP threshold we set ($19,112 per QALY). The cost-effectiveness acceptability curves revealed that a nearly 100% probability of Pembro+Chemo being cost-effective at the WTP threshold of $19,112/QALY in China (Figure S8).
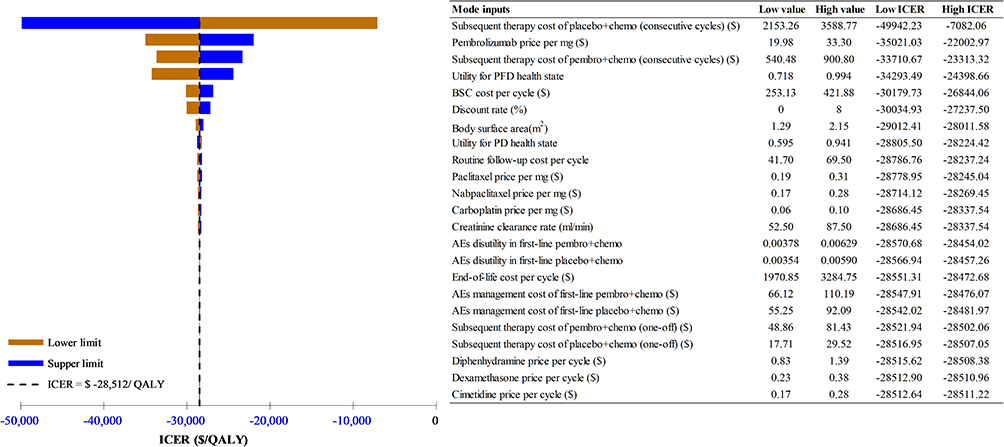 |
Figure 2 Deterministic sensitivity analysis results for first-line pembro+chemo vs placebo+chemo in the entire trial population. Abbreviations: ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year; PFD, progression-free disease; BSC, best supportive treatment; PD, progressed disease; AEs, adverse events; Pembro+Chemo, pembrolizumab plus chemotherapy; Placebo+Chemo, placebo plus chemotherapy. |
In our subgroup analyses, regardless of the varying PD-L1 TPS, the ICERs for Pembro+Chemo remained consistently below the WTP threshold employed in the model. In summary, the Pembro+Chemo group dominated the Placebo+Chemo group in all the subgroups.
Discussion
NSCLC accounts for approximately 85% of all lung cancer and remains a leading cause of cancer-related mortality. In the treatment landscape, immunotherapy agents known as ICIs, whether used alone or in combination with chemotherapy, have emerged as the cornerstone of treatment and are now considered first-line treatment therapies for patients with metastatic NSCLC.26 It is particularly noteworthy that pembrolizumab stands out as the only PD-1/L1 inhibitor that has demonstrated substantial survival benefits when employed as monotherapy or in combination with chemotherapy in comparison to chemotherapy alone for patients with metastatic squamous or nonsquamous NSCLC.27–29 The 5-year update data derived from the remarkable KEYNOTE-407 study unearthed a captivating revelation: that the OS rates of Pembro+Chemo were nearly doubled in comparison to Placebo+Chemo among patients with previously untreated metastatic squamous NSCLC. Inspired by these compelling clinical trial outcomes, we embarked on an insightful cost-effectiveness analysis aiming to compare Pembro+Chemo and Placebo+Chemo within the landscape of China. Our findings revealed that Pembro+Chemo not only showcased enhanced clinical effectiveness but also boasted a correlation with reduced expenses, thereby solidifying its unequivocal superiority over Placebo+Chemo.
Upon diligent examination of pertinent literature, two studies have assessed the cost-effectiveness of pembrolizumab in combination with chemotherapy as a first-line therapy for squamous NSCLC, drawing from the influential KEYNOTE-407 study.11,30 Wu Bin’s research findings indicated that the ICERs of Pembro+Chemo, compared to chemotherapy alone, among Chinese patients with squamous NSCLC exceeded the preset WTP threshold, thus rendering it not cost-effective. Conversely, our analysis evaluated the economics implications of Pembro+Chemo within the context of the Chinese healthcare system, revealing that when employed as a first-line therapy, pembrolizumab presents itself as a cost-effective option when combined with chemotherapy. This discrepancy can be attribute to three key factors. First, the implementation of PAP on January 1, 2021 resulted in an 88% reduction in the price of pembrolizumab. Second, the cost of subsequent anticancer treatment was adjusted to reflect prevailing market conditions. In March 2019, China introduced the National Centralized Drug Procurement (NCDP) Program, which sought to mitigate drug expenses. During the second round of NCDP, nab-paclitaxel experienced a maximum price reduction of 97%, leading to a significant decrease in chemotherapy costs for patients with squamous NSCLC. Moreover, Zhang et al conducted an evaluation of the impact of an NCDP program on the health expenditure of lung cancer inpatients, and their findings documented a notable reduction in total expenditures encompassing drugs, health services, diagnosis and consumable materials.31 Lastly, Wu Bin’s study was predicated upon the initial report of the KEYNOTE-407 trial in 2018, wherein the short follow-up time rendered the OS and PFS relatively immature. Consequently, the precision of Wu Bin’s cost-effectiveness analysis in accurately reflecting the true scenario was compromised. Our model incorporated the latest data from KEYNOTE-407, thereby rendering it more refined and capable of providing a more accurate simulation of actual scenarios.
Our study boasted several remarkable strengths. First, the impetus for our cost-effectiveness analysis stemmed from the availability of long-term survival outcomes from the KEYNOTE-407 trial, which provides a robust and accurate reflection of real-world settings. Second, we specified subsequent anticancer therapies that would be initiated either upon the completion of 35 cycles or in the case of disease progression. This approach allowed us to obtain more precise treatment costs. Thirdly, our model took into account the latest drug prices, enabling us to capture the substantial decrease in costs arising from NCDP Program. By incorporating these updated prices, we were able to provide a more comprehensive and realistic assessment of the economic implications of the treatment options. Lastly, our study ensured that the treatment protocols adhered to the local guidelines or expert consensus, aligning with the actual clinical practices observed in China. This meticulous attention to detail elevates the authenticity and relevance of our findings, making them more applicable to the local context.
It is important to acknowledge the limitations of our study. Firstly, the lack of quality-of-life data from the KEYNOTE-407 trial posed a challenge in assessing the impact of treatment on patients’ quality of life. To address this, we relied on utility values obtained from previously published literature, which may have introduced some variability in our findings. Nevertheless, sensitivity analyses conducted in our study demonstrated that the model results remained robust and were not significantly influenced by changes in utility values. Secondly, our study only accounted for the costs associated with grade 3/4 AEs, while disregarding grade 1/2 AEs due to their lower incidence rates. This approach might have resulted in an underestimation of AEs costs associated with treatment. However, our sensitivity analyses revealed that the inclusion or exclusion of these costs did not substantially impact the overall findings of the study.
Conclusion
In the context of the Chinese healthcare system, our study unequivocally demonstrated the dominance of Pembro+Chemo over Placebo+Chemo in terms of both cost and effectiveness for the treatment of metastatic squamous NSCLC, irrespective of PD-L1 expression. These compelling findings provide crucial insights that can greatly inform clinical decision-making processes.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Acknowledgments
All authors contributed to this publication were listed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Science and Technology Development Program of Medical and Health from Shandong Province (202102040505) and Nursery science research projects of affiliated hospital of Jining medical university (MP-MS-2021-001).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535–554. doi:10.1016/S0140-6736(21)00312-3
2. Nasim F, Sabath BF, Eapen GA. Lung Cancer. Med Clin North Am. 2019;103(3):463–473. doi:10.1016/j.mcna.2018.12.006
3. Travis WD, Brambilla E, Burke A, Marx A, Nicholson AG. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. Lyon: International Agency for Research on Cancer; 2015.
4. Wang M, Herbst RS, Boshoff C. Toward personalized treatment approaches for non-small-cell lung cancer. Nat Med. 2021;27(8):1345–1356. doi:10.1038/s41591-021-01450-2
5. Gou LY, Wu YL. Prevalence of driver mutations in non-small-cell lung cancers in the People’s Republic of China. Lung Cancer. 2014;5:1–9. doi:10.2147/LCTT.S40817
6. Zhou F, Qiao M, Zhou C. The cutting-edge progress of immune-checkpoint blockade in lung cancer. Cell Mol Immunol. 2021;18(2):279–293. doi:10.1038/s41423-020-00577-5
7. Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. doi:10.1056/NEJMoa1810865
8. Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
9. Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819–1830. doi:10.1016/S0140-6736(18)32409-7
10. Guidelines Working Committee of Chinese Society of Clinical Oncology. Guidelines of Chinese Society of Clinical Oncology (CSSO) Non-Small Cell Lung Cancer. Beijing: People’s medical publishing house; 2022.
11. Wu B, Lu S. The effect of PD-L1 categories-directed pembrolizumab plus chemotherapy for newly diagnosed metastatic non-small-cell lung cancer: a cost-effectiveness analysis. Transl Lung Cancer Res. 2020;9(5):1770–1784. doi:10.21037/tlcr-19-605
12. Key to life. Available from: https://smzy.ilvzhou.com/.
13. Liu G, Kang S, Wang X. Pharmacoeconomic evaluation of pembrolizumab in first- line treatment of advanced non- small cell lung cancer with high PD-L1 expression. China Pharm. 2021;32(11):1351–1356.
14. Novello S, Kowalski DM, Luft A, et al. Pembrolizumab plus chemotherapy in squamous non-small-cell lung cancer: 5-year update of the phase III KEYNOTE-407 study. J Clin Oncol. 2023;41(11):1999–2006. doi:10.1200/JCO.22.01990
15. Measures for ethical review of life science and medical research involving humans; 2023. Available from: https://www.gov.cn/zhengce/zhengceku/2023-02/28/content_5743658.htm.
16. Chinese Pharmaceutical Association. Chinese guidelines for pharmacoeconomic evaluations; 2020.
17. Briggs A, Sculpher M. An introduction to Markov modelling for economic evaluation. Pharmacoeconomics. 1998;13(4):397–409. doi:10.2165/00019053-199813040-00003
18. Cai D, Shi S, Jiang S, et al. Estimation of the cost-effective threshold of a quality-adjusted life year in China based on the value of statistical life. Eur J Health Econ. 2022;23(4):607–615. doi:10.1007/s10198-021-01384-z
19. National Bureau Of Statistics. National annual data; 2023. Available from: https://data.stats.gov.cn/easyquery.htm?cn=C01.
20. Sanders GD, Neumann PJ, Basu A, et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA. 2016;316(10):1093–1103. doi:10.1001/jama.2016.12195
21. Shen Y, Wu B, Wang X, Zhu J. Health state utilities in patients with advanced non-small-cell lung cancer in China. J Comp Ef Res. 2018;7:443–452. doi:10.2217/cer-2017-0069
22. National Health Industry Data Platform. Bid winning information of drugs; 2023. Available from: https://www.yaozh.com/.
23. Cheng R, Zhou Z, Liu Q. Cost-effectiveness of first-line versus second-line use of domestic anti-PD-1 antibody sintilimab in Chinese patients with advanced or metastatic squamous non-small cell lung cancer. Cancer Med. 2023;12(6):7389–7397. doi:10.1002/cam4.5440
24. Zhou D, Luo X, Zhou Z, et al. Cost-effectiveness analysis of tislelizumab, nivolumab and docetaxel as second- and third-line for advanced or metastatic non-small cell lung cancer in China. Front Pharmacol. 2022;13:880280. doi:10.3389/fphar.2022.880280
25. Luo X, Zhou Z, Zeng X, Liu Q. The cost-effectiveness of tislelizumab plus chemotherapy for locally advanced or metastatic nonsquamous non-small cell lung cancer. Front Pharmacol. 2022;13:935581. doi:10.3389/fphar.2022.935581
26. Lazzari C, Spagnolo CC, Ciappina G, et al. Immunotherapy in early-stage Non-Small Cell Lung Cancer (NSCLC): current evidence and perspectives. Curr Oncol. 2023;30(4):3684–3696. doi:10.3390/curroncol30040280
27. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
28. Carbone DP, Reck M, Paz-Ares L, et al. First-line nivolumab in stage IV or recurrent non-small-cell lung cancer. N Engl J Med. 2017;376(25):2415–2426. doi:10.1056/NEJMoa1613493
29. Govindan R, Szczesna A, Ahn MJ, et al. Phase III trial of ipilimumab combined with paclitaxel and carboplatin in advanced squamous non-small-cell lung cancer. J Clin Oncol. 2017;35(30):3449–3457. doi:10.1200/JCO.2016.71.7629
30. Insinga RP, Vanness DJ, Feliciano JL, et al. Cost-effectiveness of pembrolizumab in combination with chemotherapy versus chemotherapy and pembrolizumab monotherapy in the first-line treatment of squamous non-small-cell lung cancer in the US. Curr Med Res Opin. 2019;35(7):1241–1256. doi:10.1080/03007995.2019.1571297
31. Zhang YJ, Ren Y, Zheng Q, et al. The impact of national centralized drug procurement on health expenditures for lung cancer inpatients: a difference-in-differences analysis in a large tertiary hospital in China. Front Public Health. 2022;10:956823. doi:10.3389/fpubh.2022.956823
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.