Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Cost-Effectiveness Analysis of Fixed-Dose Tiotropium/Olodaterol versus Tiotropium for COPD Patients in China
Authors Lan Y, Yang N, Wang Y, Yang Y, Xu M, He Q
Received 11 June 2023
Accepted for publication 14 September 2023
Published 21 September 2023 Volume 2023:18 Pages 2093—2103
DOI https://doi.org/10.2147/COPD.S425409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ying Lan,1 Nan Yang,2 Yirong Wang,1 Yan Yang,1 Min Xu,1 Qin He1
1Department of Pharmacy, Affiliated Hospital of Southwest Jiaotong University, the Third People’s Hospital of Chengdu, Chengdu, Sichuan, 610031, People’s Republic of China; 2West China School of Pharmacy, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Ying Lan, Email [email protected]
Purpose: Tiotropium/olodaterol (TIO/OLO) fixed-dose combination (FDC) can improve lung function and quality of life for patients with chronic obstructive pulmonary disease (COPD), and is not inferior to other LAMA/LABAs. The aim of this study was to assess the cost-effectiveness of TIO/OLO FDC in patients with moderate to very severe COPD in China.
Methods: A Markov model was developed to estimate the cost-effectiveness of TIO/OLO FDC versus TIO in the treatment of COPD from Chinese health system perspective. Four health states were based on 2021 Global Initiative for Chronic Obstructive Lung Disease (GOLD 2021), which included moderate (GOLD II, 50% ≤ FEV1 ≤ 80% of predicted), severe (GOLD III, 30% ≤ FEV1 ≤ 50% of predicted) and very severe (GOLD IV, FEV1 > 30% of predicted) COPD and death. The model simulated in cycles yearly. The indicators of total costs, number of COPD exacerbations, life years (LYs) and quality-adjusted life-years (QALYs) were used as the model output. Costs and outcomes were discounted at a 5% annual rate. A cost-effectiveness analysis was conducted over a 10-year time horizon. The threshold of incremental total cost per unit effectiveness gained (ICER) was 1.5 times of GDP per capita. Uncertainty was assessed by one-way and probabilistic sensitivity analysis.
Results: TIO/OLO was 0.007 QALYs more than TIO but 0.012 LYs lower, which increased the total cost by $2268.17 per patient, but the total exacerbations number was less. Incremental cost effectiveness analysis had shown that the ICER exceeded the willingness to pay threshold. Results were robust under most parameter variation, except the parameters of total drug cost of TIO/OLO FDC in univariate sensitivity analyses.
Conclusion: Although TIO/OLO FDC could reduce the exacerbation risk, it was not cost-effective, and needed to be repriced.
Keywords: tiotropium, olodaterol, cost-effectiveness, chronic obstructive pulmonary disease, COPD, Markov
Introduction
Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease, characterized by persistent airflow limitation that is not fully reversible. In mainland of China, the prevalence of COPD in people over 60 years old can reach more than 50% of the total prevalence.1,2 COPD can cause declining in the quality of life and increasing of mortality. Exacerbations may lead to hospitalization, which will further increase the disease burden.3
Among the effective drugs, the combinations of long-acting muscarinic antagonists (LAMAs) and long-acting β-receptor agonists (LABAs) are associated with a clinically significant improvement in lung function and health-related quality of life in patients with COPD, and have fewer exacerbations, a larger improvement of forced expiratory volume in one second (FEV1) and more frequent improvement in quality of life compared with inhaled LABAs + corticosteroids (ICS) or LAMA monotherapy.4–7 Tiotropium bromide/olodaterol as a LAMA/LABA has been newly approved and marketed in China.
Tiotropium bromide/olodaterol (TIO/OLO) is specially delivered via the Respimat® soft mist inhaler (SMI), which has active spray and is easy for patients to breathe in.8 The TOnado 1 and 2 trials evaluate the efficacy and safety of TIO/OLO FDC, in which 5162 patients were involved and randomized to OLO 5 μg, TIO 2.5 μg, TIO 5 μg, TIO/OLO 2.5/5 μg, or TIO/OLO 5/5 μg groups.9 The results showed that TIO/OLO 5/5 μg significantly improved FEV1 AUC0–3 and trough FEV1 in all GOLD severity groups compared to other groups. The OTEMTO 1 and 2 trials10 and VIVACITO trial11 indicated that TIO/OLO improved lung function or quality of life compared to placebo and TIO 5 μg. In ENERGITO trial, TIO/OLO was superior to salmeterol/fluticasone in several lung function end points.12 COPD exacerbations were assessed in DYNAGITO trials showed that TIO/OLO did not reduce exacerbation rate compared with TIO alone.13 In several network meta-analysis researches, TIO/OLO FDC was similar to other LAMAs/LABAs in improving trough FEV1, transition dyspnea index (TDI), St George’s Respiratory Questionnaire (SGRQ) score, exacerbation, all‑cause mortality, risks of major adverse events and incidence of pneumonia, such as aclidinium/formoterol, Glycopyrronium Bromide/indacaterol, umeclidinium/vilanterol, tiotropium/salmeterol and Glycopyrronium Bromide/Formoterol.14,15 Another network analysis indicated that TIO/OLO 5/5μg was significantly more effective than both aclidinium/formoterol 400/12μg and Glycopyrronium Bromide/formoterol 14.4/9.6μg in improving trough FEV1, significantly more effective than Glycopyrronium Bromide/formoterol 14.4/9.6μg in improving TDI, and had the best cardiovascular safety.16 So, among the LAMA/LABA combinations, TIO/OLO FDC has certain advantages.
In recent years, more studies focused on the efficacy and safety of TIO/OLO FDC compared with other treatments, but less on its economy. In addition, the economic evaluation research on TIO/OLO FDC for COPD patients under Chinese background was none. This article presented a Markov model to access the cost-effectiveness of TIO/OLO FDC versus TIO for moderate to very severe COPD from Chinese health system perspective.
Materials and Methods
Model Structure
A Markov model was developed to assess the cost-effectiveness of TIO/OLO FDC for COPD patients in China. The model was followed the Guidelines for Pharmaceutical Economic Evaluation of China (2020 edition).17 The cycle length was 1 year. The average life expectancy of Chinese residents was 76.34 years old,18 and patients with COPD had shorter lives. Too long research period may bring more uncertainty and make the results deviate from reality. Therefore, it was more appropriate to set the time horizon of the model to 10 years.
Four states were defined as follows: moderate, severe and very severe COPD, and death (Figure 1). Each of COPD health states (moderate to very severe COPD) was defined by Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations.4 Exacerbations could happen in all COPD health states, and could be treated in hospital or in community care with different associated costs and utilities. Specific values of mortality, utility, resource use, cost, and risk of exacerbation varied with different COPD disease states.
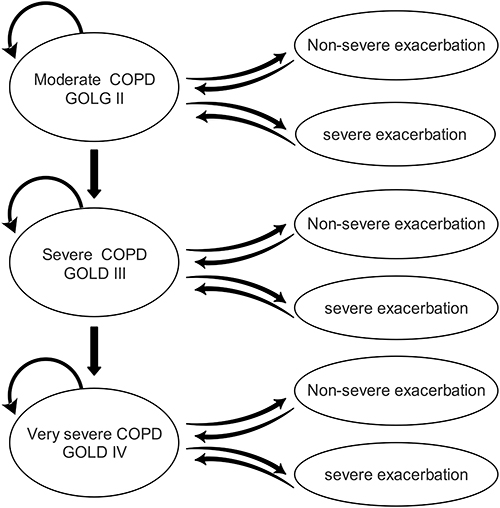 |
Figure 1 State transition diagram of Markov model. |
Comparators
The main intervention measures of this study were TIO/OLO FDC (5/5 µg, 1 inhalation administered once daily) and TIO (5 µg, 1 inhalation administered once daily). TIO was selected as the control drug because it was widely used in China and was an important inhaled drug for the treatment of COPD. Other maintenance measures of the two groups were assumed to be consistent.
Model Inputs
Clinical Data
The patient-level characteristics were mainly from the TOnado/DYNAGITO trials (Table 1).19,20 At the beginning of the simulation, 37.5% of patient had moderate COPD, 49.4% had severe COPD and 13.1% had very severe COPD in TIO/OLO FDC group, while in TIO group, 39.5% were moderate, 48.5% severe, and 12.0% very severe. An average patient age was about 65 years in the TOnado/DYNAGITO trials.20,21
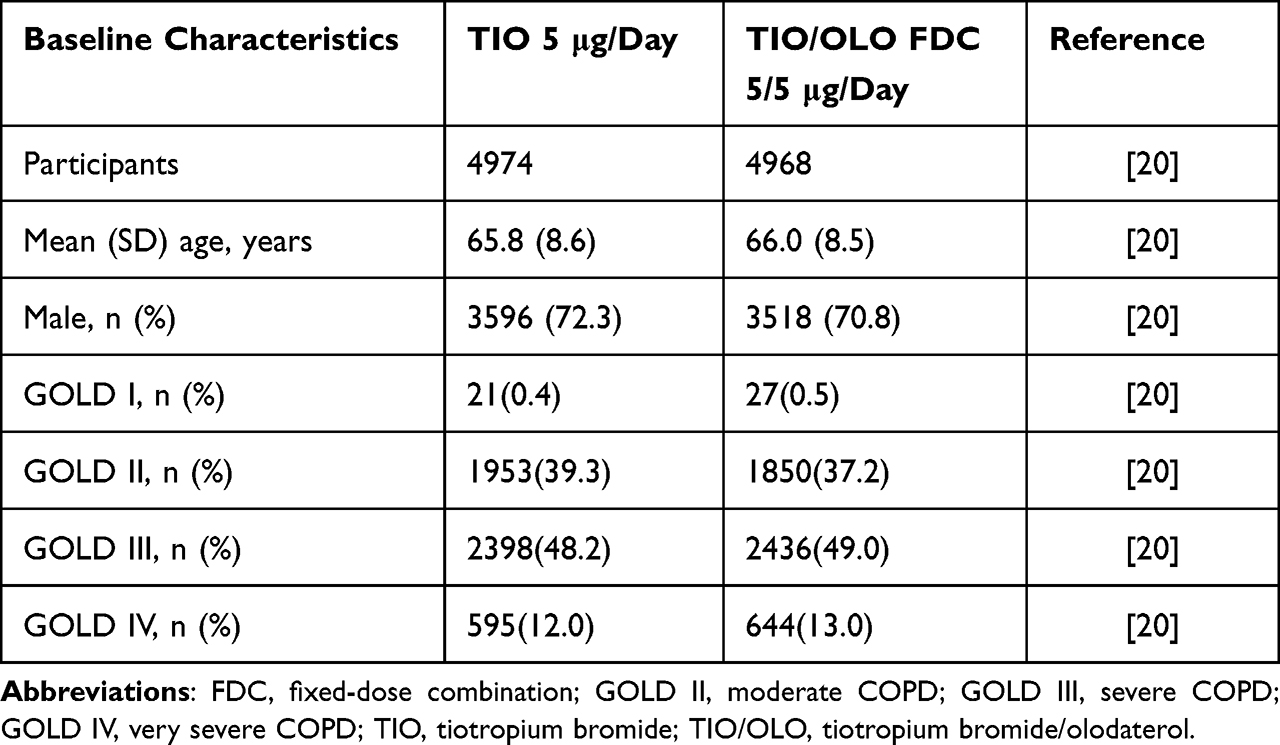 |
Table 1 Baseline Characteristics |
The annual transition probabilities between moderate, severe, and very severe COPD were based on the method described by Spencer et al.22,23 The first cycle uses the initial probability from base to new, and all subsequent cycles use the new probability (Table 2). Patients in the model could experience different levels of exacerbations or no exacerbations. Severe exacerbations were classified as events requiring hospitalization, and non-severe exacerbations as events requiring treatment such as systemic corticosteroids and/or antibiotics and/or contact with a health care provider without hospitalization. The risks of exacerbation were taken from Wedzicha et al, and varied with COPD severity and treatments (Table 2).20 The severe and non-severe exacerbation risks were adjusted proportionally. The incidences of adverse events (AEs) for each treatment were extracted from the pooled subgroup analysis of Tonado study.19
 |
Table 2 The Annual Transition Probabilities for TIO/OLO FDC and TIO |
Mortality was estimated based on a large clinical trial (TIOSPIR trial) of COPD patients (Table 3).24 TIOSPIR trial involved 17,135 participants from 50 countries and lasted for 3 years, which compared the efficacy and safety of three dosage groups of tiotropium. The annual risk of death in TIOSPIR trial was based on age and COPD severity stage, and estimated for nine groups.25 Mortality was not impacted by the incidence of exacerbations as it would be double counting the risk.
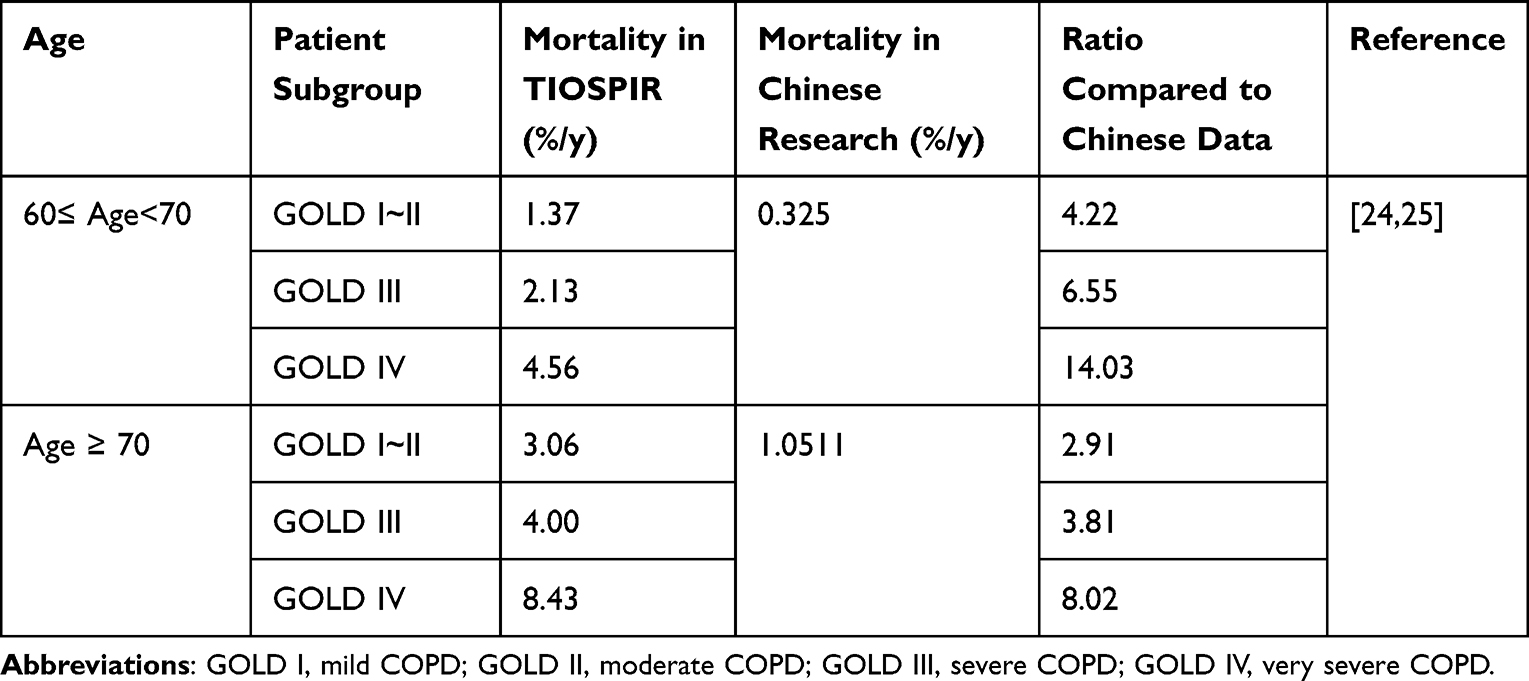 |
Table 3 COPD-Related Mortality Risk by Age and Severity Stage |
Utilities
The St. George’s Respiratory Questionnaire (SGRQ) total score was converted into utility value by mapping method, and the conversion formula came from the research of Starkie et al as below.26,27 Exacerbations led to the decline of utility value, and the decline varied with the severity of exacerbation. Monthly utility decrements were obtained from literatures and were converted into annual value, which did not vary in each COPD severity health state and each treatment group28 (Table 4). The health utility of death was 0.
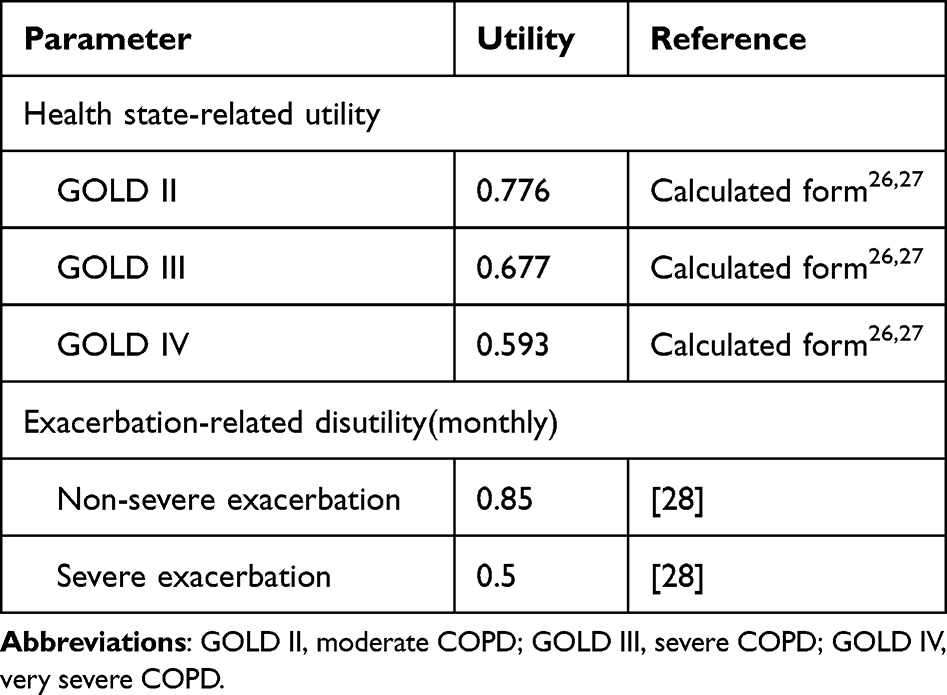 |
Table 4 Health State-Related Utility and Exacerbation-Related Disutility |
U = 0.9617- (0.0013 × SGRQ total) – (0.0001 × SGRQ total 2) + (0.0231 × male)27
Resources and Costs
As the model was performed under the perspective of health system, only direct healthcare resources and costs were included. The methods of gross-costing and micro-costing were both used in cost measure. All the costs were presented in US dollar based on 2023 prices (USD: RMB=1: 6.8767, Feb. 17th), and would be adjusted to the value in 2023 if possible (Table 5).
 |
Table 5 Resource Use and Annual Costs for Markov Model |
The costs of long-term inhaled drugs were calculated by resources and unit prices. The prices of TIO/OLO FDC (5ug/5ug/press, CN¥722.92) and TIO (2.5ug/spray, CN¥520) were consistent in most areas of China and the daily dosages were consistent with the instructions. Drug costs were determined using the average bidding prices released by the provincial Healthcare Security Administration.29 The price of TIO/OLO FDC was significantly higher than that of other LABAs/LAMAs, so the average price of other LABAs/LAMAs was used as the lower price value for TIO/OLO FDC in sensitivity analysis. The price of TIO powder for inhalation had multiple manufacturers in China, with significant price differences. The average price of TIO was used as the lower value in sensitivity analysis.
Management cost stratified by COPD severity was obtained from literature, which was estimated based on the healthcare resources consumption and the unit cost of healthcare resources. Management costs mainly consisted cost for outpatient visits, spirometry, chest imaging examinations, and influenza vaccinations, and were determined through expert consultation and the average healthcare service price in multiple provinces.
Cost for exacerbations was calculated from the results of a cross-sectional study was carried out among 678 COPD patients in four cities in China in 2011,31 including outpatient visit for non-severe exacerbations and hospital admission for severe exacerbations. The AEs treatment costs were obtained from previous research,30 including treatment costs for pneumonia, nasopharyngitis, bronchitis, dysphonia, and upper respiratory tract infection.
Model Calculation and Validation
The base case analysis was run with Treeage Pro 2021 R1.0, and the direct medical costs and COPD health outcomes discounted at a rate of 5.0% according to the recommendations of Guidelines for Pharmaceutical Economic Evaluation of China (2020 edition). The indicators of total costs, number of COPD exacerbations, life years (LYs), and quality-adjusted life-years (QALYs) were used as the model output. To avoid overestimating the incremental value, half-cycle corrections to utility were performed. Incremental total cost per unit effectiveness gained (ICER) was used to assess the cost-effectiveness of TIO/OLO FDC against TIO. The threshold of ICER in China was close to 1.5 times of GDP per capita.32 According to official data from the National Bureau of Statistics (http://www.stats.gov.cn/), the GDP per capita of China in 2020 was $11,775.42. So, the threshold of ICER was set to $17,663.12/QALY.
The model was validated against results from the Tonado trial and DYNAGITO trial. The DYNAGITO trial was a 52-week, randomized, double-blind, active-controlled, parallel-group trial. It was verified according to whether TIO/OLO FDC reduced the annual rate of exacerbations more than TIO alone,20 and the death rate was similar after 1 year.13
Sensitivity Analyses
Both one-way sensitivity analysis (OWSA) and probabilistic sensitivity analysis (PSA) were conducted. In the OWSA, except for specific value variation ranges, the following variables were conducted, with modify by ±20% for costs and ±10% for utilities and transition probability.
- Annual transition probability from one COPD state to another
- Exacerbation risk in different severities and COPD states
- Cost of routine COPD management and costs for severe and non-severe COPD exacerbation
- Health state utility values and decrements following severe and non-severe exacerbations
- Discount rate (0% to 8%)
The PSA was performed by means of Second-order Monte Carlo simulation. A total of 1000 iterations were conducted following the assignment of different distribution functions to the key parameters. Gamma distribution was applied for cost parameters, while Beta distribution for utility value and transition probability parameters and uniform distribution for discount rate. Scatter plots were developed to represent uncertainty, and cost-effectiveness acceptability curves were created based on the patient’s willingness to pay $17,663.12 per QALY (WTP=17,663.12).
Results
Base-Case Analyses
It seemed that treatment with TIO/OLO FDC was associated with lower risk of total exacerbations (both non-severe and severe exacerbations) versus TIO (Table 6). The results of base-case analysis indicated that TIO/OLO FDC was similar to TIO in QALY and LY, but the price was higher (Table 5). Patients on TIO/OLO FDC gained 4.332 QALYs and 6.655 LYs with a total cost of $20,938.21, while patients on TIO gained 4.325 QALYs and 6.667 LYs with a total cost of $18,670.04. Incremental cost effectiveness analysis had shown that incremental costs of $2268.17 per patient, incremental QALYs of 0.007 per patient, and an incremental cost-effectiveness ratio (ICER) of $324,557.91 per additional QALY over 10 years, which exceeded the willingness to pay threshold of 1.5 times of GDP in China.
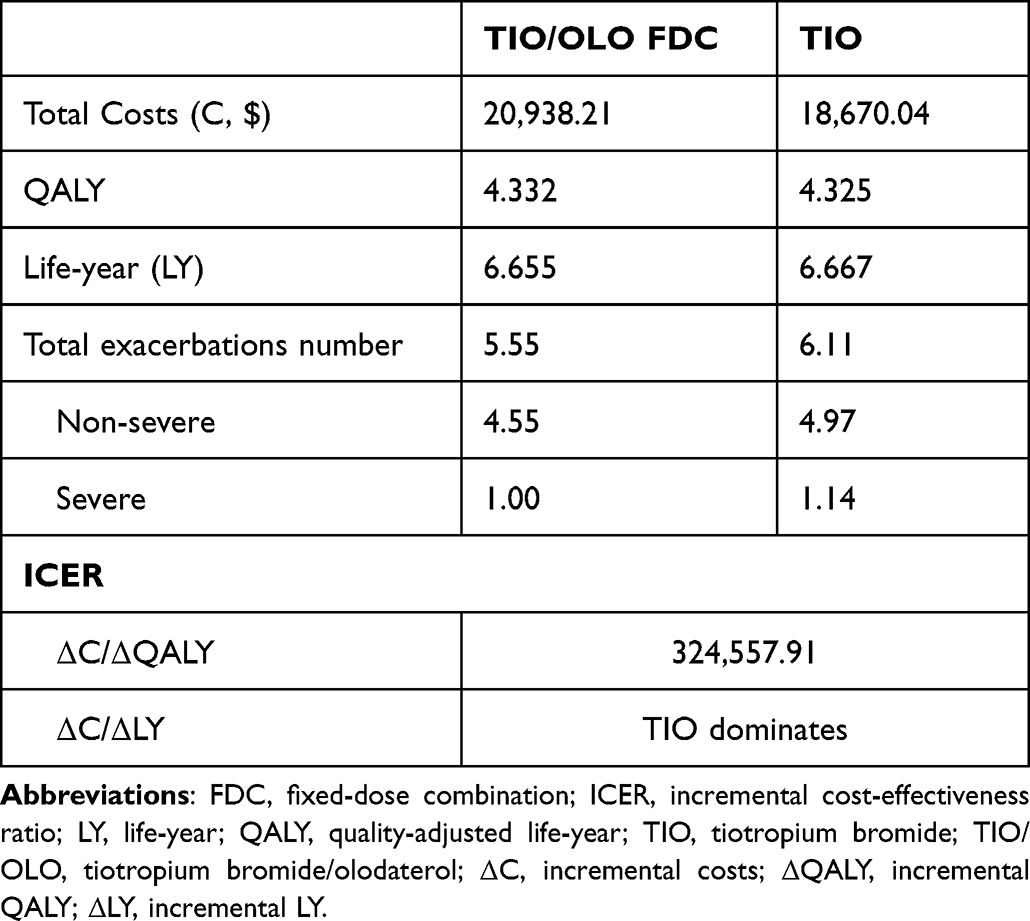 |
Table 6 Cost-Effectiveness Analysis of Two Regimens Over 10 Years |
Model Validation
One year running results of the model were compared to the Tonado trial and DYNAGITO trial with study duration of 52-week (Table 7). All-cause mortality and total exacerbations per patient-year estimated in the model on TIO arm were equivalent to Tonado trial and DYNAGITO trial.13,20 TIO/OLO FDC reduced the rate of exacerbations at 1 year more than TIO alone, which was consistent with the results of DYNAGITO trial.
 |
Table 7 Model Outcomes versus TOnado Trial on TIO Arm |
Sensitivity Analyses
Univariate sensitivity analyses were performed with the extreme values to run the model, with robust results under most parameter variation, except the parameters of total drug cost of TIO/OLO FDC. In the ICER tornado analysis (WTP=17,663.12), the 10 most sensitive parameters were shown in the tornado diagram below (Figure 2).
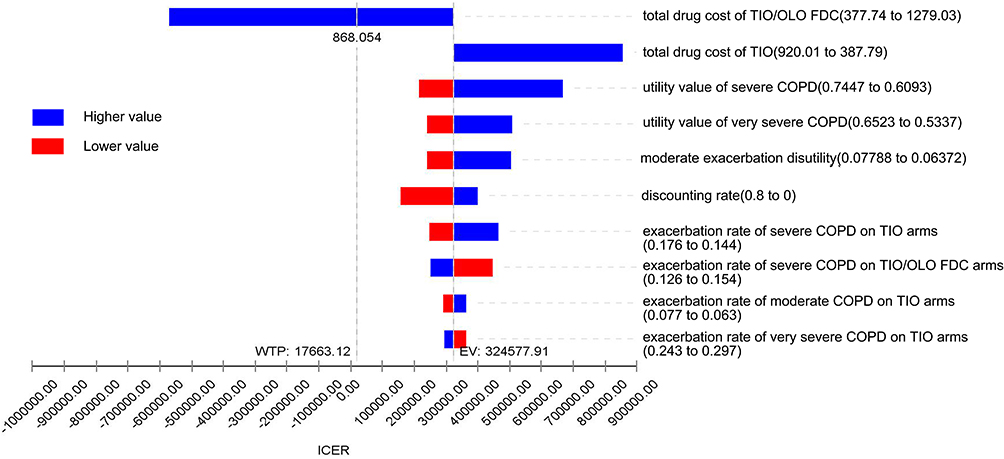 |
Figure 2 Tornado diagram (ICER, TIO OLO FDC vs TIO). |
Probabilistic sensitivity analyses showed that TIO/OLO FDC was the cost-effective treatment in 69.5% of simulations at a threshold of $17,663.12 per QALYs. The Mento Carlo ICER scatterplot running with 1000 simulations can be seen in Figure 3. Additionally, a cost-effectiveness acceptability curve and Monte Carlo acceptability at WTP indicated that TIO/OLO FDC had 70.4%, 81.7% and 79.4% probability of being cost effective at the decision thresholds of 1, 1.5 and 3 times of Chinese per capita GDP in 2020, respectively (namely $11,775.42/QALY, $17,663.12/QALY and $35,326.25/QALY, respectively) (Figure 4). And when the decision threshold was below 8000, TIO was more cost-effective.
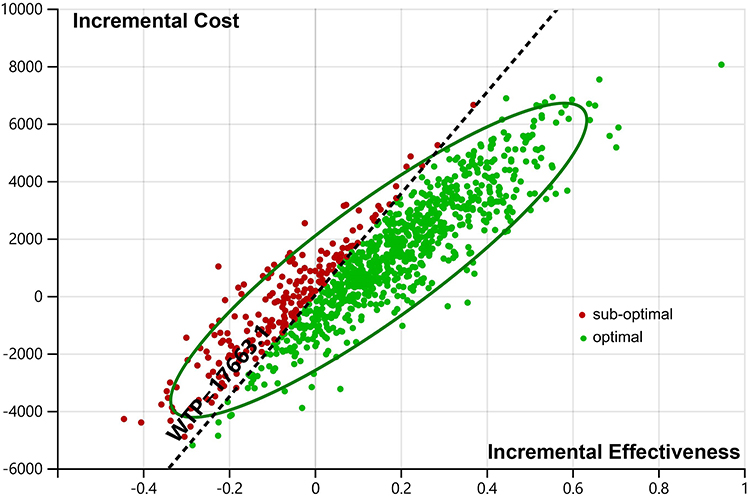 |
Figure 3 Scatter plot of incremental cost-effective of TIO OLO FDC vs TIO. |
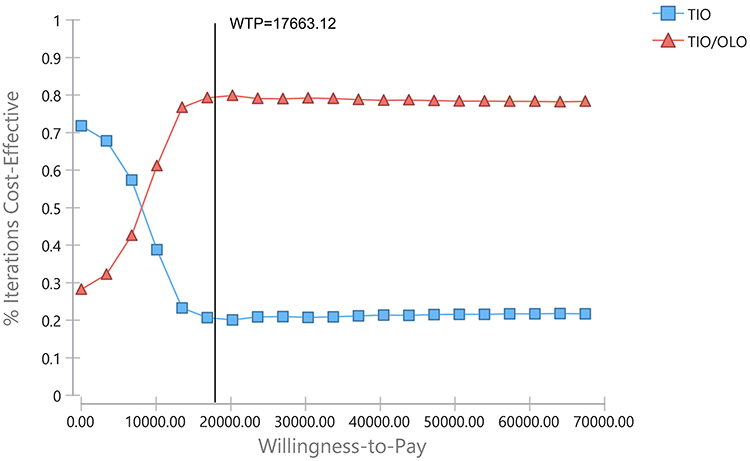 |
Figure 4 Cost-effectiveness acceptability curve of TIO OLO FDC vs TIO. |
Discussion
The base case analyses had shown that treatment with TIO/OLO FDC, compared to TIO alone, resulted in both cost increases and QALY gains, although the difference of QALY was marginal. The deterministic analysis found that the most sensitive parameter was the total drug cost of TIO/OLO FDC: when the value below $868.054, TIO/OLO FDC would switch to a cost-effective solution. There was uncertainty whether the model research results were consistent with the future situation, because there might be changes in treatment strategies and drug policies, and emergence of new drugs. Our research needs to be further confirmed in the future and adjusted according to the changes of new drug policies and treatment guidelines.
In a previous study, with the similar model structure, TIO/OLO FDC was shown different economic evaluation results. Capel et al reported that aclidinium–formoterol (ACL/FF) 400/12 μg had a same clinical effect and more cost compared with TIO/OLO 5/5 μg for patients with moderate-to-severe COPD in Spain, so the latter was worthwhile.33 An individual-level Markov model for the perspective of the UK health care system had shown that TIO/OLO FDC had equal cost-effectiveness to Indacaterol/Glycoprronium Bromide FDC and Umeclidinium/ Vilanterol FDC, and dominated to Aclidinium bromide/ Formoterol fumarate FDC.34 An individual-level Markov model, performed from the Dutch health care payer’s perspective, showed that the ICER of TIO/OLO FDC versus TIO was €7004/QALY and the former was cost-effectiveness.35 In an Italian study, TIO/OLO FDC had confirmed to be a cost-effective bronchodilator against TIO in the maintenance treatment of COPD.36 But our model showed an opposite result for TIO/OLO FDC, and this might be related to the relatively high price of TIO/OLO FDC in China.
The compliance of inhaled preparations has a great impact on the treatment effect of COPD, and poor compliance may bring more treatment costs on AECOPD. High adherence of ICS/LABA combinations could reduce the relative risk of hospitalized AECOPD by 34.8%, and the mean 1-year per-patient hospitalized AECOPD costs by 37.8% in a retrospective cohort database study in China.37 The effect of drugs could not be separated from compliance, but the evaluation of drugs could be more accurate only on the premise of good compliance. Considering that introducing compliance into the model would make the parameters too complex, the model assumes that the compliance of the two groups was consistent and good.
COPD is a smoking-related disease. Studies have shown that there were differences in the decline of FEV1 between smokers and non-smokers.38 The rate of decline in FEV1 among sustained quitters was half the rate among continuing smokers, 31±48 versus 62±55 mL (mean 6 SD), comparable to that of never-smokers with mild-to-moderate airway obstruction.39 There were few studies on the decline of lung function in Chinese smoking patients, which needed further investigation. So, the changes of lung function whether related to smoking were not considered. It may be a better research direction to carry out subgroup analysis on smoking, non-smoking population and second-hand smoke exposed population for the economic evaluation of inhaled agents in the treatment of COPD in the future.
Despite the abovementioned limitations, the assumptions considered in the present model appeared to be reasonable and passed the model validation. The sensitivity analyses confirmed the robustness of the results. Future research could focus on the impact of drug price changes on economic evaluation results, especially when China’s medical insurance policy and drug policy change greatly.
Conclusion
In this economic evaluation from a Chinese health system perspective, TIO/OLO FDC could reduce the exacerbation risk, but it was expensive and not cost-effective. Results of this analysis suggested that TIO/OLO FDC was not the first choice for patients with moderate to very severe COPD in China, and the drug company needed to reprice drugs.
Ethics Statement
This study was approved by an institutional review board from the Third People’s Hospital of Chengdu and conducted in accordance with the Declaration of Helsinki. This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors, therefore ethical review was exempted.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Sichuan Provincial Health Commission [grant numbers 18PJ539, 2018].
Disclosure
All authors have no conflicts of interest to declare in this work.
References
1. Chronic Obstructive Pulmonary Disease Group. Respiratory Diseases Branch of Chinese Medical Association Chronic Obstructive Pulmonary Disease Working Committee of the Respiratory Physician Branch of the Chinese Medical Doctor Association, Guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease. Chin J Tuberc Respir Dis. 2021;44(3):170–204.
2. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross‐sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
3. Li M, Wang F, Chen R, et al. Factors contributing to hospitalization costs for patients with COPD in China: a retrospective analysis of medical record data. Int J Chron Obstruct Pulmon Dis. 2018;13:3349–3357. doi:10.2147/COPD.S175143
4. Global Initiative for Chronic Obstructive Lung Disease (GOLD), Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Available from: https://goldcopd.org/2022-gold-reports-2/.
5. Horita N, Goto A, Shibata Y, et al. Long-acting muscarinic antagonist (LAMA) plus long-acting beta-agonist (LABA) versus LABA plus inhaled corticosteroid (ICS) for stable chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2017;2(2):CD012066. doi:10.1002/14651858.CD012066.pub2
6. Maqsood U, Ho TN, Palmer K, et al. Once daily long-acting beta2-agonists and long-acting muscarinic antagonists in a combined inhaler versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2019;3(3):CD012930. doi:10.1002/14651858.CD012930.pub2
7. Rodrigo GJ, Price D, Anzueto A, et al. LABA/LAMA combinations versus LAMA monotherapy or LABA/ICS in COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:907–922. doi:10.2147/COPD.S130482
8. Blair HA. Tiotropium/Olodaterol: a Review in COPD. Drugs. 2019;79(9):997–1008. doi:10.1007/s40265-019-01133-w
9. Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2–4). Eur Respir J. 2015;45(4):969–979. doi:10.1183/09031936.00136014
10. Singh D, Ferguson GT, Bolitschek J, et al. Tiotropium plus olodaterol shows clinically meaningful improvements in quality of life. Respir Med. 2015;109(10):1312–1319. doi:10.1016/j.rmed.2015.08.002
11. Beeh KM, Westerman J, Kirsten AM, et al. The 24-h lung-function profile of once-daily tiotropium and olodaterol fixed-dose combination in chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2015;32:53–59. doi:10.1016/j.pupt.2015.04.002
12. Beeh KM, Derom E, Echave-Sustaeta J, et al. The lung function profile of once-daily tiotropium and olodaterol via Respimat® is superior to that of twice-daily salmeterol and fluticasone propionate via Accuhaler® (ENERGITO® study). Int J Chron Obstruct Pulmon Dis. 2016;11(1):193–205. doi:10.2147/COPD.S95055
13. Calverley PMA, Anzueto AR, Carter K, et al. Tiotropium and olodaterol in the prevention of chronic obstructive pulmonary disease exacerbations (DYNAGITO): a double-blind, randomized, parallel-group, active-controlled trial. Lancet Respir Med. 2018;6(5):337–344. doi:10.1016/S2213-2600(18)30102-4
14. Lee HW, Park J, Jang EJ, et al. Comparisons of exacerbations and mortality among LAMA/LABA combinations in stable chronic obstructive pulmonary disease: systematic review and Bayesian network meta-analysis. Respir Res. 2020;21(1):310. doi:10.1186/s12931-020-01540-8
15. Schlueter M, Gonzalez-Rojas N, Baldwin M, et al. Comparative efficacy of fixed-dose combinations of long-acting muscarinic antagonists and long-acting beta2-agonists: a systematic review and network meta-analysis. Ther Adv Respir Dis. 2016;10(2):89–104. doi:10.1177/1753465815624612
16. Rogliani P, Matera MG, Ritondo BL, et al. Efficacy and cardiovascular safety profile of dual bronchodilation therapy in chronic obstructive pulmonary disease: a bidimensional comparative analysis across fixed-dose combinations. Pulm Pharmacol Ther. 2019;2019:101841. doi:10.1016/j.pupt.2019.101841
17. Liu GG, Hu SL, Wu JH. China Guidelines for Pharmacoeconomic Evaluations.
18. National Bureau of Statistics. Average life expectancy of population; 2015. Available from: http://www.stats.gov.cn/.
19. Bai CX, Tang Y, Xin JB, et al. The efficacy and safety of tiotropium/olodaterol fixed-dose combination in patients with chronic obstructive pulmonary disease: a pooled subgroup analysis of Tonado 1+2. Chin J Tuberc Respir Dis. 2019;42(11):838–844.
20. Wedzicha JA, Buhl R, Singh D, et al. Tiotropium/Olodaterol Decreases Exacerbation Rates Compared with Tiotropium in a Range of Patients with COPD: pooled Analysis of the Tonado /DYNAGITO Trials. Adv Ther. 2020;37(10):4266–4279. doi:10.1007/s12325-020-01438-3
21. Ferguson GT, Fležar M, Korn S, et al. Efficacy of Tiotropium + Olodaterol in Patients with Chronic Obstructive Pulmonary Disease by Initial Disease Severity and Treatment Intensity: a Post Hoc Analysis. Adv Ther. 2015;32(6):523–536. doi:10.1007/s12325-015-0218-0
22. Wilson MR, Patel JG, Coleman A, et al. Cost-effectiveness analysis of umeclidinium/vilanterol for the management of patients with moderate to very severe COPD using an economic model. Int J Chron Obstruct Pulmon Dis. 2017;12:997–1008. doi:10.2147/COPD.S124420
23. Spencer M, Briggs AH, Grossman RF, et al. Development of an economic model to assess the cost effectiveness of treatment interventions for chronic obstructive pulmonary disease. Pharmacoeconomics. 2005;23(6):619–637. doi:10.2165/00019053-200523060-00008
24. Wise RA, Anzueto A, Cotton D, et al. Tiotropium Respimat inhaler and the risk of death in COPD. N Engl J Med. 2013;369(16):1491–1501. doi:10.1056/NEJMoa1303342
25. Selya-Hammer C, Gonzalez-Rojas Guix N, Baldwin M, et al. Development of an enhanced health-economic model and cost-effectiveness analysis of tiotropium + olodaterol Respimat fixed-dose combination for chronic obstructive pulmonary disease patients in Italy. Ther Adv Respir Dis. 2016;10(5):391–401. doi:10.1177/1753465816657272
26. Starkie HJ, Briggs AH, Chambers MG, et al. Predicting EQ-5D Values Using the SGRQ. Value Health. 2011;14(2):354–360. doi:10.1016/j.jval.2010.09.011
27. Zhou X, Wang Z, Song Y, et al. Periodontal health and quality of life in patients with chronic obstructive pulmonary disease. Respir Med. 2011;105(1):67–73. doi:10.1016/j.rmed.2010.06.017
28. Rutten-van Mölken MP, Hoogendoorn M. Holistic preferences for 1-year health profiles describing fluctuations in health: the case of chronic obstructive pulmonary disease. Pharmacoeconomics. 2009;27(6):465–477. doi:10.2165/00019053-200927060-00003
29. Sichuan Provincial Medical Security Bureau. Sichuan Provincial Centralized Procurement and Price Supervision Platform for Medicines and Instruments; 2023. Available from: https://www.scyxzbcg.cn/std/login.html.
30. Liu J, He X, Wu J. Economic Evaluation of Triple Therapy with Budesonide/Glycopyrrolate/ Formoterol Fumarate for the Treatment of Moderate to Very Severe Chronic Obstructive Pulmonary Disease in China Using a Semi-Markov Model. Appl Health Econ Health Policy. 2022;20(5):743–755. doi:10.1007/s40258-022-00732-1
31. Chen X, Wang N, Chen Y, et al. Costs of chronic obstructive pulmonary disease in urban areas of China: a cross-sectional study in four cities. Int J Chron Obstruct Pulmon Dis. 2016;11:2625–2632. doi:10.2147/COPD.S118523
32. Cai D, Shi S, Jiang S, et al. Estimation of the cost-effective threshold of a quality-adjusted life year in China based on the value of statistical life. Eur J Health Econ. 2022;23(4):607–615. doi:10.1007/s10198-021-01384-z
33. Capel M, Mareque M, Álvarez CJ, et al. Cost-Effectiveness of Fixed-Dose Combinations Therapies for Chronic Obstructive Pulmonary Disease Treatment. Clin Drug Investig. 2018;38(7):611–620. doi:10.1007/s40261-018-0646-0
34. Tebboth A, Ternouth A, N G-R. UK-specific cost-effectiveness of tiotropium + olodaterol fixed-dose combination versus other LAMA + LABA combinations in patients with COPD. Clinicoecon Outcomes Res. 2016;8:667–674. doi:10.2147/CEOR.S116546
35. van Boven J, Kocks J, Postma MJ. Cost-effectiveness and budget impact of the fixed-dose dual bronchodilator combination tiotropium–olodaterol for patients with COPD in the Netherlands. Int J Chron Obstruct Pulmon Dis. 2016;11:2191–2201. doi:10.2147/COPD.S114738
36. Selya-Hammer C, Gonzalez-Rojas Guix N, Baldwin M, et al. Development of an enhanced health-economic model and cost-effectiveness analysis of tiotropium + olodaterol Respimat fixed-dose combination for chronic obstructive pulmonary disease patients in Italy. Ther Adv Respir Dis. 2016;10:391–401.
37. Chen R, Gao Y, Wang H, et al. Association Between Adherence to Maintenance Medication in Patients with COPD and Acute Exacerbation Occurrence and Cost in China: a Retrospective Cohort Database Study. Int J Chron Obstruct Pulmon Dis. 2020;15:963–971. doi:10.2147/COPD.S234349
38. Wang ML, Avashia BH. Interpreting periodic lung function tests in individuals: the relationship between 1- to 5-year and long-term FEV1 changes. Chest. 2006;130(2):493–499. doi:10.1016/S0012-3692(15)51866-7
39. Scanlon PD, Connett JE, Waller LA, et al. Smoking Cessation and Lung Function in Mild-toModerate Chronic Obstructive Pulmonary Disease. The Lung Health Study. Am J Respir Crit Care Med. 2000;161(2Pt1):381–390. doi:10.1164/ajrccm.161.2.9901044
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.