")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Cost and Cost-Effectiveness of Treating Childhood Cancer at Jimma Medical Center
Authors Genemo I , Chala TK , Hordofa DF , Sinkie SO
Received 15 November 2022
Accepted for publication 31 May 2023
Published 7 June 2023 Volume 2023:15 Pages 433—442
DOI https://doi.org/10.2147/CEOR.S395170
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Idiris Genemo,1 Temesgen Kabeta Chala,1 Diriba Fufa Hordofa,2 Shimeles Ololo Sinkie1
1Department of Health Policy and Management, Jimma University, Jimma, Oromia, Ethiopia; 2Department of Pediatric Oncology Unit, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Idiris Genemo, P.O.B. 378, Jimma, Ethiopia, Tel +251911052719, Fax +214-047-111-44-84, Email [email protected]
Background: More than 70% of childhood cancer patients die in Sub-Saharan African countries due to a lack of access. Additionally establishing a childhood cancer treatment service is perceived as expensive by the decision-makers of LMICs. However, there is a paucity of evidence on the actual cost and cost-effectiveness of this service in LMICs including Ethiopia. This study provides context-relevant evidence to consider childhood cancer treatment in the healthcare priority settings in Ethiopia and other LMICs.
Methods: Newly admitted case files of children for the year 2020/21 were reviewed. The cost was analyzed from the provider’s perspective. The effectiveness was calculated using DALY averted based on the 5 years of survival rates, which is estimated from the 1-year survival rate of Kaplan–Meier output. The do-nothing was our comparator, and we assumed no cost (zero cost) will be incurred for the comparator. To account for sensitivity analyses, we varied the discount rate, 5-year survival rate, and life expectancy.
Results: During the study period, 101 children were treated in the unit. The total annual and unit cost to give treatment to childhood cancer patients was estimated at $279,648 and $2769, respectively. The highest per-patient annual unit cost of treatment was Hodgkin’s lymphoma ($6252), while Retinoblastoma ($1520) was the least. The cost per DALY averted was $193, which is significantly less than Ethiopia’s GDP per capita ($936.3). The results remained very cost-effective in sensitivity analyses.
Conclusion: Childhood cancer treatment is very cost-effective in Ethiopia as per WHO-CHOICE thresholds even in a conservative adjustment of assumptions. Therefore, to enhance and improve children’s health, childhood cancer should get a better concern in health priority.
Keywords: unit cost, cost-effectiveness, childhood cancer, Ethiopia
Introduction
In the global priority to control non-communicable, adult cancer has received the highest focus.1 Additionally, there is a false perception that chronic diseases such as cancer are a disease of adults only and that it does not affect children.2 However, the truth is any part of the population and any portion of the body can be affected by cancer.3
Every year approximately 160,000 new cases and 90,000 children die due to cancer.4 When measuring the global burden of childhood cancer using disability-adjusted life years (DALYs), its actual number and death are low, but the burden of the disease is higher than any other disease in children and cancer in adults.5
Globally 11.5 million DALYs were contributed by childhood cancer, and more than 80% of the disease burden affected LMICs in 2017.6 Additionally, due to inaccessibility and not being able to pay for the care more than 70% of childhood cancer patients die of this disease in LMICs.7 In Ethiopia, childhood cancer frequency is rising at an alarming state.8 As stated by Tikur Anbessa Specialized Hospital clinical record, there were nearly 6000 incidents of childhood cancer per year in Ethiopia.9
The perception of establishing childhood cancer treatment is very expensive is among the major reason that hinders LMICs from considering this treatment scheme a national health priority.6,10 The policymakers in LMICs often also face difficulty in the allocation of resources due to the absence of credible information on the cost-effectiveness of different healthcare interventions.10
Furthermore, most of the previous studies in LMICs on cost and cost-effectiveness analysis of childhood cancer treatment have a limitation on their costing methodology and omission of key cost inputs which significantly underestimates total cost.6 The other gap of most research in LMICs is that they use top-down and gross costing approaches to conduct cost analysis studies.11
Most importantly, to our knowledge in Ethiopia, no study has demonstrated the establishment of a pediatric oncology service to be a reasonable use of insufficient resources with competing healthcare demands. To address this gap, we undertake a cost and cost-effectiveness analysis of a pediatric cancer treatment unit in Jimma Medical Centre (JMC). Besides, in this study, we tried to include all cost inputs for the analysis to avoid underestimation of total costs, we also conducted the costing analysis by using mixed methods of bottom-up micro-costing and top-down approaches to reach reliable and precise cost estimation.11 Therefore, to determine the total cost of treating childhood cancer in Jimma Medical Centre and to find whether treating childhood cancer in the center is cost-effective or not.
Methods
Study Area and Period
The study was conducted at Jimma Medical Centre (JMC) which is the only teaching and referral hospital in southwest Ethiopia with an 800-bed capacity and a catchment population of over 15 million.12 It gives services to about 15,000 inpatients, 11,000 emergency cases, and 4500 deliveries per year.13
The establishment of cancer treatment centers in five teaching referral hospitals was one national cancer control and treatment strategy.14 One of these five hospitals is Jimma Medical Center Pediatric Oncology Unit (JMCPOU).4 In this unit, there are 22 beds with one oncologist, four residents, and 14 nurses.
Study Population
All children with cancer who were admitted to JMCPOU were the source population, and among these, all patients in the year 2020/21 fiscal year (July 8, 2020, to July 7, 2021, ie, the 2013 Ethiopian Fiscal Year) were included for this study. The cost analysis of this study was conducted from the provider’s perspective.
The Study Comparator, Thresholds, and Discount Rate
In the treatment unit, there is no other option to treat cancer in children, therefore we chose no treatment (do nothing) as our comparator to the childhood cancer treatment unit of JMC. Currently, the types of treatment available in JMCPOU are chemotherapy and surgery.
The cost-effectiveness of treatment is interpreted based on the WHO-CHOICE thresholds.15 We used a 3% discount rate for the effectiveness of the treatment unit based on the WHO-CHOICE recommendation.
Data Collection and Analysis Procedures
Costs
A mixed methodology of bottom-up micro-costing and top-down gross costing approaches was employed to arrive at a reliable and precise cost estimate. After the classification of costs into recurrent costs and capital costs, a detailed conceptual tool was formulated.
All costs were adjusted for the average annual exchange rate of 2020 ($1:00 USD = 39.4 ETB), for conversion from Ethiopian currency (ETB) into USD to make an easier international comparison.16
Unit Cost Determination for Each Type of Cancer
To determine unit costs for each type of childhood cancer patient, two different methods were used. The first is to determine the unit cost of personnel, overhead, building, and equipment, we calculated the annual cost for each type of cost. Then, we allocated it to each type of cancer based on the annual proportion of each type of patient stay in the hospital. The second method is to determine the costs of drugs, diagnostics, and the operating room. For this, we collected the utilization of each patient from their respective case files then, we aggregated each type of cancer.
Recurrent Costs
Personnel Costs
To determine unit personnel costs, we identified all medical hospital staff involved in the treatment of childhood cancer patients, including pediatric oncologists, pediatric surgeons, residents, nurses, and pharmacists.
To calculate full-time equivalent medical staff costs using this approach, each medical staff’s yearly salaries including fringe benefits were collected. We calculated the staff cost of the non-dedicated medical staff their annual salaries were allocated to the proportion of their time dedicated to the unit.
Chemotherapy and Supportive Care Medications Cost
To allocate the cost of the drug to each type of cancer individual patient utilization was obtained from the pharmacy registry of the oncology treatment unit. This data was started to be collected electronically in the treatment unit for half of the study year using Microsoft Excel.
In this registry, all types of medications prescribed were recorded and whether they had been given to patients or ordered to be bought from outside was recorded. If the drug was not available in the pharmacy there was an NGO that would buy the drugs. And, to avoid the underestimation of the drug costs, we obtained the data on those drugs bought by this NGO from its finance office. The data were available only for six months in our study period. However, because we aimed to determine the annual cost, we multiplied the six-month data by two and the annual cost of drugs was obtained. Unit prices were obtained from the hospital pharmacy department.
Operating Room (OR) Cost
The OR costs associated with pediatric cancer patients were determined by identifying which type of procedure those patients had undergone surgery. Then, the unit cost was obtained from the Liaison office of the hospital.
Diagnostic Cost
It includes laboratory tests, radiology, and pathology. The quantity of each type of diagnostic test was collected from each patient’s case file. The collected data were aggregated for each type of cancer patient. The diagnosis test unit costs were obtained from the hospital’s main laboratory office of finance.
Overhead Costs
The overhead costs for the treatment unit include administrative personnel, water, electricity, supplies, consumables for a test, transport for blood products, information technology, building, and equipment maintenance. We used a markup method, to obtain the overhead cost of the pediatric oncology unit by assuming the total direct costs of treatment units are the same proportion as the total direct cost of the hospital.
Capital Costs
Equipment Cost and Building Cost
The furniture and other equipment that is specifically used by the centers such as beds, shelves, computers, and refrigerators were identified. The annual value of the building and each piece of equipment were determined by using the annualization method. The replacement value of the equipment was determined by obtaining the market prices of each item at the time of data collection.
To obtain the replacement value of building costs, we obtained the unit cost of constructing a one-meter square of a similar building. Then, to obtain the total current cost of the building, we multiply this cost by the total m2 of the childhood cancer treatment unit occupied.
Thirty years of useful life years were used for building 16, and each piece of equipment’s useful life years was obtained from the WHO-CHOICE project.17 The interest rate was obtained from local banks.
For the annual cost of equipment/building costs, we determined the annuity function which was calculated based on each equipment/building life year and interest rate. Annuity functions were obtained from the Drummonds.18 Finally, the annualized value of each piece of equipment and building was determined.
Outcomes
The effectiveness of the pediatric oncology unit was determined by collecting data on incidence cases of pediatric cancer patients within the study timeframe from the JMCPOU. During treatment, children suffer from a diminished quality of life; for this, we account for the Global Burden of Disease disability weight.19 In addition, because the average length of therapy varies based on the type of cancer, we used the median years “on therapy”, to obtain the length of disability.
The age of each patient at the time of diagnosis was collected to obtain the median age at the time of diagnosis. We derived potential life lost at the time of death using the Ethiopian population’s life expectancy.20
The other information that was collected was the date of patients who died within one year after the treatment, those who lost to follow-up, and their respective last contact before the loss to follow-up. With this information, we estimated the one-year survival rate of patients using Kaplan–Meier survival analysis. Then, the 5-year overall survival rate was estimated using a study in Chennai, India21.
We used this study to estimate our 5-year survival rate because there are no other studies. LMICs that can be related to our study that analyses the 5-year survival rate of all types of cancer. The Chennai, India study reveals that the average 5-year survival of all types of cancer patients is 62% of the 1-year overall survival of pediatric cancer patients.21 Therefore, we estimate the 5-year survival rate for our study using this same proportion of 62% 1-year survival rate. All of the above important parameters are listed in Table 1.
 |
Table 1 Variables and Sources Included in the Cost-Effectiveness Model |
To calculate the DALY of pediatric patients if they had not gotten treatment (without intervention), we assumed they will die within one month after they have been diagnosed with cancer in parallel to previous literature.24,25 However, we conducted this in sensitivity analysis by varying the patients who will die within months and one year. Finally, the difference between the two DALY scenarios is considered as DALY averted by the JMC pediatric oncology unit.
Sensitivity Analysis
In the Sensitivity analysis, the cost parameters we varied to include increasing medical personnel costs by 20%, this is because it is believed certain staff such as doctors are overburdened and work many more hours per week than the contract’s working hours. The other cost parameter is the overhead cost, this is because the markup method assumes a linear relationship between direct and indirect costs but children with cancer need special care, so they might use more overhead costs. Therefore, we increased the overhead cost by 20%.
The outcome parameters that were varied in sensitivity analysis include varying all parameter discount rates between extremes of 6% and 0%, the estimated value of five years survival rate, and the life expectancy of childhood cancer survivors. Additionally, to account for long-term morbidity, we applied the GBD disability weight for non-Hodgkin’s lymphoma (0.06) across the life course of all types of cancer survivors.
Data Quality Management
Tools were adopted from the literature and modified based on a study of interest.10,11,24 The collected data were analyzed using SPSS to estimate the one-year survival rate and Microsoft Excel 2019 for other forms of analysis.
Results
Distribution of the Types of Cancer and Their Costs
During the study period, 101 children with clinically suspected childhood cancer were registered in (JMCPOU) and started treatments. Among these patients, 55 patients were men (Table 2).
 |
Table 2 Distribution of the Types of Cancer and Their Costs in Different Genders |
Among the patients included in the study, more than one-third (42) patients were acute lymphoblastic leukemia (ALL), and 13 patients were Wilms tumor (WT). These two types of cancers account for more than half of all patients during the study period.
The annual cost to provide treatment to a new pediatric cancer unit in JMC, Jimma, Ethiopia; was estimated to be $279,648 for the year 2020/21. The highest total cost of all types of cancer was incurred for ALL, and it has a large composition and accounted for more than one-third of overall total costs. The least total cost incurred among major types of cancer treated in the center is RMS patients (Table 2).
On the other hand, among the major cost categories of the pediatric unit, the annual medical personnel cost was the largest single component accounting for 39% of all costs (Table 3), while the least-cost component of the total cost is the operating room cost of 0.1%.
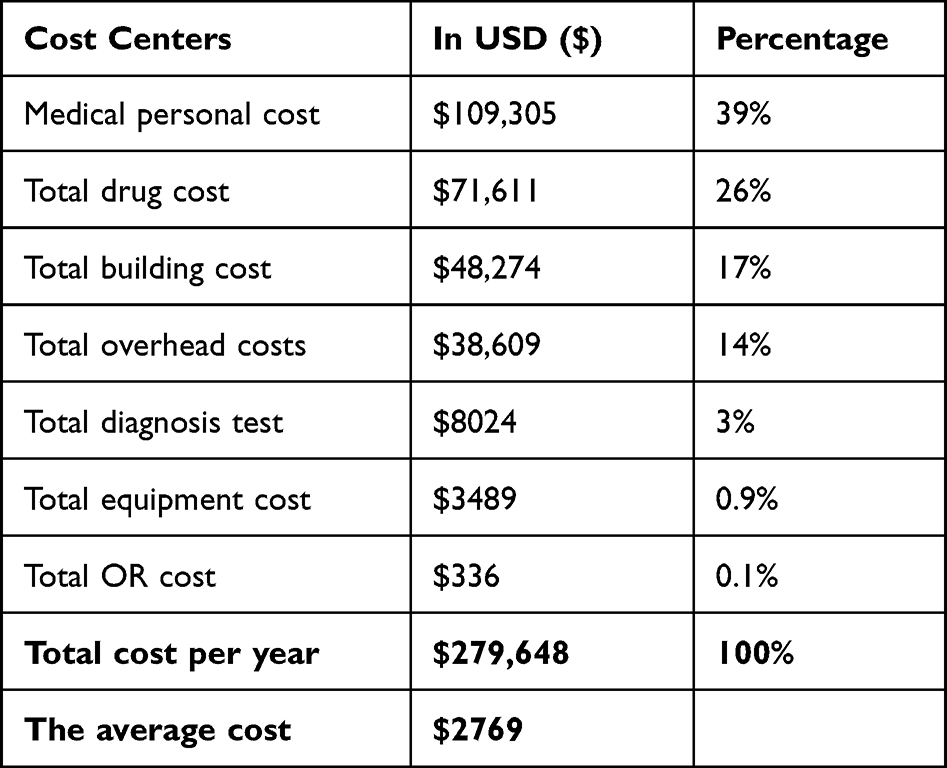 |
Table 3 The Annual Total Cost of Major Cost Categories in the JMC Pediatric Oncology Unit |
The Unit Cost of Treating Childhood Cancer
Based on the data from the JMCPOU, the unit cost per newly diagnosed childhood cancer patient was $2769 (Table 3). Of all types of cancer treated in JMCPOU, the two major types of lymphomas namely Hodgkin’s lymphoma and non-Hodgkin’s lymphoma accounted for the highest average cost to treat one patient per year (Figure 1).
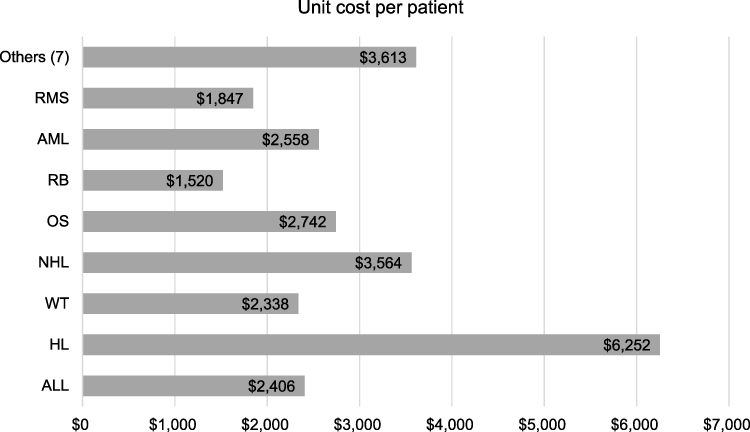 |
Figure 1 The treatment unit cost per patient for each type of cancer. |
For the two leukemia (ALL and AML), the unit cost per patient is about equal. The three least average costs per patient are accounted for among the major types of cancer treated in the JMCPOU Wilms tumor, Rhabdomyosarcoma, and Retinoblastoma. Other types of cancer consisting about seven types of cancer, if we distribute the average cost per patient for this type of cancer, it accounts for about $516 which is less than half of all other types of cancer. Total and average per-patient costs by category are detailed in Annex II.
On the other hand, among cost categories, the cost of personnel is also a significant cost driver for all types of cancer except for ALL, and OS where drug cost is significantly higher than other cost categories. OR and equipment unit cost is the least among all types of childhood cancer. All types of annual average cost categories for each type of cancer are detailed in Annex II.
The Cost-Effectiveness of the JMC Pediatric Oncology Unit
The 5-year survival rate was determined using a 1-year survival rate that was calculated using Kaplan–Meier survival analysis on SPSS. The output of the Kaplan–Meier one-year survival rate was about 75% (Figure 2). Using the Chennai, India21 proportion ratio and we estimated the 5-year survival rate which we get 47.6% of the 5-year survival rate.
 |
Figure 2 One-year survival curve of childhood cancer patients in Jimma Medical Center pediatric oncology unit. |
The parameters used to determine the cost-effectiveness of treating pediatric cancer patients in JMC are listed in Table 1. Using those parameters defined in the base cases (no early mortality and no excess morbidity; 3% discounting). The cost per life saved for a 5-year survival rate was $5236. The cost per DALY averted in the base case was $193, which is significantly less than Ethiopia’s per capita income ($936.3), thus meeting WHO-CHOICE criteria for being considered very cost-effective. These results were sustained after adjusting for 0% discounting levels ($90). When 6% discounting was tested, operating the cancer unit remained cost-effective ($324).
Sensitivity Analysis Results
In sensitivity analyses that allowed for deviation from the base cases, however, the resultant costs always remained very cost-effective (ie, below the threshold of 1 time the GDP per capita) (Table 4).
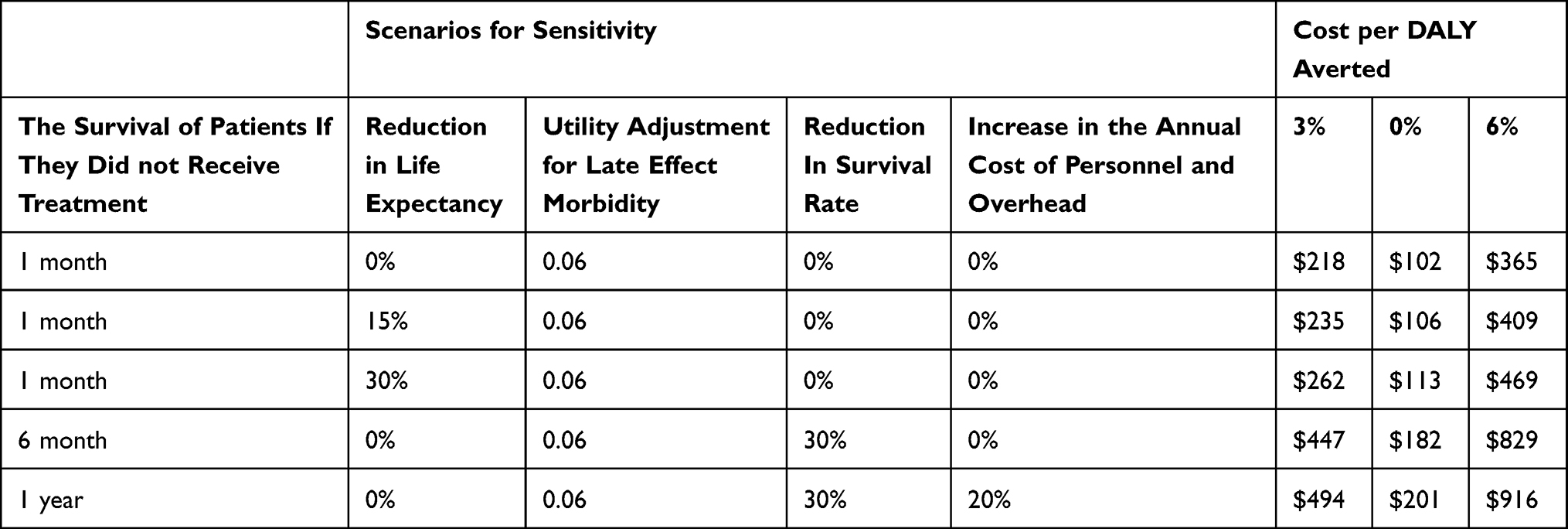 |
Table 4 One-Way and Multiway Sensitivity Analysis |
Discussion
This study is to the best of our knowledge, one of the very few economic evaluations in Sub-Saharan African countries, and no published study analyzes the cost or cost-effectiveness of a childhood cancer treatment unit in Ethiopia. In this study, we tried to find how much is the average cost per year to give care to children with cancer. In addition, we try to answer whether the JMCPOU is cost-effective or not based on the WHO-CHOICE threshold.
Accordingly, this study demonstrates that the program achieved 47.6% of the 5-year survival rate at 2769 USD cost per patient, and $193 cost per DALY was averted. The study of current analysis indicates that treating childhood cancers in Ethiopia, within highly conservative adjustment of assumptions, remains very cost-effective according to WHO-CHOICE thresholds.
When comparing the current study with similar previous studies, the average cost per childhood cancer patient in JMCPOU for newly diagnosed cancer was generally a bit higher than in other studies reported in Zimbabwe.25 On the other hand, it is significantly lower than other studies reported in LMICs (that range from the highest in Kenya)25 and El Salvador 21 to the medium in Ghana.10
Our study result shows that the annual cost of treating pediatric cancer patients is $279,648, which is relatively lower than other study results referred to above except for the Nigerian cases.25 The total cost of pediatric cancer also varies significantly in studies of different countries ranging from the annual total cost of $229,000 in Nigeria to $4 million in Kenya and $5.2 million in El Salvador. The observed variations can originate due to our study did not include indirect costs borne by the families, and instead, our cost analysis is restricted to the provider perspective.
The annual average cost of treating pediatric patients with HL is by far larger ($6252) than WT patients ($2338). This result is consistent with the study conducted in two South African hospitals26 related to HL patients. A study conducted in Rwanda, however, is not the case where the range or average costs between the two types of cancer are very close to each other. The methodological difference in our studies could cause such differences in results. Among the differences in our study, the health personnel, overhead, and capital costs are allocated to this type of cancer based on their stay in the hospital.
On the other hand, in our study, the JMCPOU achieved a 76.76% of 1-year survival rate. This result is relatively higher than other related studies conducted in LMIC ranging from 12.5% to 62%.10,24,25 The stated difference could be due to the assumptions involved in these studies that considered those lost to follow-up as dead. However, in our estimation of 1-year analysis, we used the Kaplan–Meier estimation of the survival rate.
This study also showed that, when conducting sensitivity analysis by changing the survival rate of patients, the cost-effectiveness of the treatment unit was below the threshold. However, the cost per DALY averted at different discount rates almost doubled. This shows that among different parameters and assumptions used to measure and determine the effectiveness of the treatment unit; the 5-year survival rate of patients has a significant effect on the cost-effectiveness of the treatment center.
The inability to fully consider all cost inputs, such as the cost of blood, are among the limitations of this study. The other limitation is that the hospital unit cost charged for services such as operating theatres (OR), and diagnostic test costs are assumed to include the amortization costs of equipment and personal costs.
The other study limitations worth noting are; first, many annual average costs were derived from the hospital’s relevant departments at the time of data collection which may not properly account for fluctuations in service users and inflation rate. Second, when it is compared to the other studies conducted in LMICs, our study that the one-year survival rate is extremely high and this could be due to improper follow-up of patients who stop receiving care or are lost to follow-up but included in the estimation of the one-year survival rate. Thirdly, several assumptions were necessary including the ratio of 5-year to 1-year survival and the markup method assumption to determine the overhead cost. Moreover, the cost-effectiveness among each type of cancer could differ; however, we assume the total cost-effectiveness will represent the individual cost-effectiveness. While the validity of the assumptions is not known, our overall results did not change in sensitivity analyses.
Conclusion
This study demonstrates that an investment of less than $2769 per patient can save children’s lives and safeguard families from the suffering and sorrow of losing a child to cancer. Additionally, the treatment of childhood cancer in a resource-limited setting represents a highly cost-effective intervention by international standards. Therefore, the finding of this study can be used as a piece of evidence to inform policy-makers to strengthen childhood cancer outcomes in Ethiopia and other sub-Saharan African countries.
Ethical Consideration
Ethical clearance was secured by Jimma University Institutional Review Board (IRB). Thereafter, permission was sought from the Head of the Oncology unit, to use the dataset about the study participants for research purposes only. The authors declare that the procedures were followed according to the regulations to the Helsinki Declaration of the World Medical Association.
Acknowledgments
We would like to thank JMCPOU and its healthcare professionals for providing all the necessary information about the staff composition and their time and dedication to the center. We acknowledge the cooperating Jimma Medical Center administrative staff for giving cost information. We would also like to extend our thanks to Jimma University, the Institute of Health, School of Post Graduate Director for providing financial support to carry out this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors have no conflicts of interest to disclose except Dr Diriba Fufa who is a Head of the pediatric oncology unit at Jimma Medical Centre, and also a Chair, at Jimma University, Health Institute Staff Council.
References
1. Denburg AE, Laher N, Mutyaba I, et al. The cost effectiveness of treating Burkitt lymphoma in Uganda. Cancer. 2019. doi:10.1002/cncr.32006
2. Endalamaw A, Assimamaw NT, Ayele TA, et al. Prevalence of childhood Cancer among children attending referral hospitals of outpatient departments in Ethiopia. BMC Cancer. 2021;21(1):1–10. doi:10.1186/s12885-020-07763-8
3. World Health Organization (WHO). Childhood cancer. 2021; Available from: https://www.who.int/news-room/fact-sheets/detail/cancer-in-children#. Accessed
4. Wąż P, Bielińska-Wąż D, Nandy A. The challenge of childhood cancer in developing countries. J Math Chem. 2014;52(1):132–140. doi:10.1007/s10910-013-0249-1
5. Force LM, Abdollahpour I, Advani SM, et al. The global burden of childhood and adolescent cancer in 2017: an analysis of the Global Burden of Disease Study 2017. Lancet Oncol. 2019;20(9):1211–1225. doi:10.1016/S1470-2045(19)30339-0
6. Fung A, Horton S, Zabih V, Denburg A, Gupta S. Cost and cost-effectiveness of childhood cancer treatment in low-income and middle-income countries: a systematic review. BMJ Glob Health. 2019;4(5):1–13. doi:10.1136/bmjgh-2019-001825
7. Alemu A. Patterns of solid childhood neoplasms in Jimma University Medical Center, Southwest Ethiopia - A histopathologic approach; 2017.
8. Yifru S, Muluye D. Childhood cancer in Gondar University Hospital, Northwest Ethiopia. BMC Res Notes. 2015;8:1–5. doi:10.1186/s13104-015-1440-1
9. Aziza Shad A; Llc MLC partner Phillips and cohen. Pediatric oncology in Ethiopia: an Inctr-USA And Georgetown University Hospital twinning Initiative with Tikur Anbessa Specialized Hospital - Cancer Control. Cancer Control Cancer Care in Emerging Health Systems. Available from: http://www.cancercontrol.info/cc2013/challinor/.
10. Renner L. Evidence from Ghana indicates that childhood cancer treatment in Sub- Saharan Africa is very cost effective: a report from the childhood cancer 2030 network abstract. J Global Oncol. 2021. doi:10.1200/JGO.17.00243
11. Hendriks ME, Kundu P, Boers AC, et al. Step-by-step guideline for disease-specific costing studies in low- and middle-income countries: a mixed methodology Marleen. Glob Health Action. 2014;9716. doi:10.3402/gha.v7.23573
12. Melkamu E, Yetwale A. Attitude of nurses and midwives towards collaborative care with physicians in Jimma University Medical Center, Jimma, South West Ethiopia. Hum Resour Health. 2020;18(1):1–8. doi:10.1186/s12960-020-00531-6
13. Melaku T, Gashaw M, Chelkeba L, et al. Evaluation of adult outpatient antibiotics use at Jimma Medical Center (With defined daily doses for usage metrics). Infect Drug Resist. 2021;14:1649–1658. doi:10.2147/IDR.S293080
14. Memirie ST, Habtemariam MK, Asefa M. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Global Oncol. 2018;(4):1–11. doi:10.1200/JGO.17.00175
15. Donald S. Shepard Dominic Hodgkin YEA. Manual WHO GUUIODE hospital cost analysis for manager.pdf; 2000.
16. Org.uk ERate. US dollar to Ethiopian birr spot exchange rates for 2020. Available from: https://www.exchangerates.org.uk/USD-ETB-spot-exchange-rates-history-2020.html.
17. WHO-CHOICE. Econometric estimation of WHO-CHOICE country-specific costs for inpatient and outpatient health service delivery. Available from: https://www.who.int/teams/health-systems-governance-and-financing/economic-analysis/costing-and-technical-efficiency/quantities-and-unit-prices-(cost-inputs)/econometric-estimation-of-who-choice-country-specific-costs-for-inpatient-and-outpatient-health-service-delivery.
18. Drummond MF, Sculpher MJ, Caxton K, Stoddart GL, George WT. Methods for the Economic Evaluation of Health Care Programmes.
19. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL, Asia S. Global Burden of Disease and Risk Factors Editors and Pacific the Caribbean. Oxford University Press; 2006.
20. Lustig N, Gonzalez E. Investigating in health for economic development; 2004.
21. Swaminathan R, Rama R, Shanta V. Childhood cancers in Chennai, India, 1990 – 2001: incidence and survival. Int J Cancer. 2008;26(11):2607–2611. doi:10.1002/ijc.23428
22. Ivinson AJ. Macroeconomics and health: investing in health for economic development: World Health Organization. Nat Med. 2002;8(6):551–552. doi:10.1038/nm0602-551b
23. World Bank. GDP per capita (current US$) - Ethiopia | data. Available from: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=ET.
24. Fuentes-alabi S, Bhakta N, Vasquez RF, Gupta S, Horton SE. The cost and cost-effectiveness of childhood cancer treatment in El Salvador, Central America: a report from the childhood cancer 2030 network. Cancer. 2018;124(2):391–397. doi:10.1002/cncr.31022
25. Githang’a J, Brown B, Chitsike I, et al. The cost-effectiveness of treating childhood cancer in 4 centers across sub-Saharan Africa. Cancer. 2021;127(5):787–793. doi:10.1002/cncr.33280
26. Freedman J, Goldberg L. Incidence of retinoblastoma in the Bantu of South Africa. Br J Ophthalmol. 1976;60(9):965–966.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.