Back to Journals » International Journal of General Medicine » Volume 17
Correlation of Prognostic Nutritional Index and Systemic Immune-Inflammation Index with the Recurrence and Prognosis in Oral Squamous Cell Carcinoma with the Stage of III/IV
Received 9 January 2024
Accepted for publication 8 May 2024
Published 20 May 2024 Volume 2024:17 Pages 2289—2297
DOI https://doi.org/10.2147/IJGM.S458666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Manjun Ye,* Lixia Zhang*
Department of Oral Surgery, Daqing Oilfield General Hospital, Daqing, Heilongjiang, 163000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Manjun Ye, Department of Oral Surgery, Daqing Oilfield General Hospital, No. 9 Zhongkang Street, Ertu District, Daqing, Heilongjiang, 163000, People’s Republic of China, Email [email protected]
Introduction: This study aimed to explore the correlation of systemic immune-inflammation index (SII) and prognostic nutritional index (PNI) with the recurrence and prognosis in patients with advanced oral squamous cell carcinoma (OSCC).
Methods: A total of 298 OSCC patients with the stage of III/IV were finally included in the study. SII = neutrophil count (109/L) × platelet count (109/L)/lymphocyte count (109/L). PNI = serum albumin (g/L) + 5 × total lymphocyte count (109/L).
Results: High preoperative SII and low preoperative PNI were independent risk factors for tumor recurrence in OSCC patients of the stage of III/IV. The area under the curves (AUC) for SII was 0.69 (0.63 to 0.76), for PNI was 0.72 (0.67 to 0.78), and for joint model was 0.81 (0.76 to 0.85). Patients with low level of joint model had significantly higher overall survival rate for 5 years follow-up than those with high level.
Discussion: Both preoperative SII and PNI are valuable independent tumor recurrence prediction index in patients with advanced OSCC. Meanwhile, the combination of preoperative SII and PNI is also valuable on OSCC recurrence and prognosis prediction.
Keywords: oral squamous cell carcinoma, prognostic nutritional index, systemic immune-inflammation index, recurrence, prognosis
Introduction
Oral squamous cell carcinoma (OSCC) is aggressive. Studies have shown that the incidence and mortality of OSCC in rural and urban China are on the rise.1 The prognosis of patients with OSCC is affected by many factors. Although the level of diagnosis and treatment of oral cancer has been improved worldwide, the prognosis of OSCC patients has not been significantly improved. Tumor recurrence is still the main cause of death in patients. Patients with recurrence have lower 5-year overall survival rate than patients without recurrence.2 How to accurately implement individualized treatment and scientifically evaluate the prognosis of patients with advanced OSCC has important clinical significance.
The impact of malnutrition on disease prognosis is manifested in multiple ways.3 First, the occurrence of malnutrition leads to the decline of the function of various organs of the body and the imbalance of components leads to the decline of the functions of various systems. Second, malnutrition can lead to a compromised immune system. Prognostic nutritional index (PNI) is a widely used index based on total lymphocyte counts and serum albumin (ALB) levels.4
Preoperative systemic inflammatory response participates in tumor development and consequently to overall survival.5 Systemic immune-inflammation index (SII) is a powerful prognostic indicator in several malignancies.6
The purpose of this work is to explore the correlation between PNI and SII and OSCC recurrence and prognosis, and the value of PNI and SII and their combined detection on OSCC recurrence and prognosis prediction.
Methods
Patients
The data of 380 OSCC patients was collected. Inclusion criteria: (1) Patients with primary oral tumor and diagnosed as squamous cell carcinoma by pathological examination; (2) Patients with age over 18 years old; (3) Patients received systematic treatment in our hospital; (4) Patients with complete clinical, pathological, and follow-up data; (5) Patients with clinical stage III~IV. Exclusion criteria: (1) Patients with serious underlying diseases; (2) Patients with a history of other malignant tumors; (3) Patients with active infection or inflammatory disease within 4 weeks before surgery; (4) Patients lost to follow-up. 298 patients were finally included in this study. The study was approved by XXX, and all the participants signed the informed written consent.
Recurrence is defined as in situ (local) recurrence of malignancy of the same histological origin in the in situ or neck or in situ + neck or distant area at least 4 weeks after the first standard surgical treatment. Recurrence was diagnosed through physical examination, magnetic resonance imaging (MRI), computed tomography (CT), and pathological examination. Distant metastases were diagnosed through medical history, clinical signs, positron emission tomography (PET), and CT.
TNM staging criteria for OSCC patients: based on the 2017 AJCC/UICC oral cancer TNM staging criteria combined with previous clinical and pathological data.
Treatment and Follow-Up
According to the Oral Cancer Diagnosis and Treatment Guidelines and our treatment experience, OSCC patients received surgery treatment, preoperative induction chemotherapy + surgery, surgery + postoperative radiotherapy and chemotherapy, and preoperative induction chemotherapy + surgery + postoperative radiotherapy and chemotherapy. The basis for the patient to receive preoperative induction chemotherapy are: (1) The tumor grows rapidly; (2) The pain is obvious; (3) Invasion of multiple anatomical structures makes resection more difficult. Patients treated with TP (cisplatin + docetaxel) regimen will be transferred to the radiotherapy department of our hospital to receive concurrent chemoradiotherapy. Surgical options include extended local excision of the primary tumor, extended primary tumor excision + neck lymphadenectomy, extended primary tumor excision + neck lymphadenectomy + free flap reconstruction.
The follow-up time of this study began on the first day after the operation of the patients. The follow-up methods were telephone and online appointments, and the patients were followed up in outpatient clinics, and the results of physical examination and auxiliary examination were recorded. The follow-up was continued for at least 5 years.
Nutritional Assessment
Prognostic nutritional index (PNI) was calculated by the following equation: serum albumin (g/L) + 5 × total lymphocyte count (109/L).
Immune Inflammation Assessment
Systemic immune inflammation index (SII) was calculated by the following equation: neutrophil count (109/L) × platelet count (109/L)/lymphocyte count (109/L)
Statistical Analyses
Analysis was performed by the SPSS software. The plot was made using GraphPad Prism 8.3.0. The data were shown as mean ± standard deviation (SD) or n (percentage). The comparisons of data between the two groups were done by unpaired t test with Welch’s correction, Fisher’s exact test, or Chi-square test. The correlation between PNI and SII was analyzed by the Pearson correlation analysis. Receiver operating characteristic (ROC) curves were plotted to evaluate the specificity, sensitivity, and differences by assessing area under the curves (AUC) of PNI and SII. The optimal cutoff value was calculated with the Youden index. Logit (Joint model) = 0.006 * SII - 0.067 * PNI. p values <0.05 were considered statistically significant.
Results
Clinicopathological Factors for Tumor Recurrence
There were 126 patients with tumor recurrence and 172 patients without recurrence. The overall recurrence rate was 42.3%, including 77 patients (61.1%) with primary tumor recurrence, 23 (18.3%) with cervical lymph node metastasis, 14 (11.1%) with both primary tumor recurrence and cervical lymph node metastasis, and 12 (9.5%) with distant metastasis.
The baseline characteristics of patients with tumor recurrence and with non-tumor recurrence were shown in Table 1. Age, gender, M classification, invasion depth, preoperative chemotherapy, postoperative radio-chemotherapy, and tumor location showed no significant difference between the two groups. The proportion of advanced T-stages (p = 0.009) and N-stages (p = 0.001) in patients with tumor recurrence were significantly higher than in those with non-tumor recurrence. Patients with tumor recurrence had significantly higher preoperative SII than those with non-tumor recurrence (p < 0.001), while the preoperative PNI was significantly lower (p < 0.001).
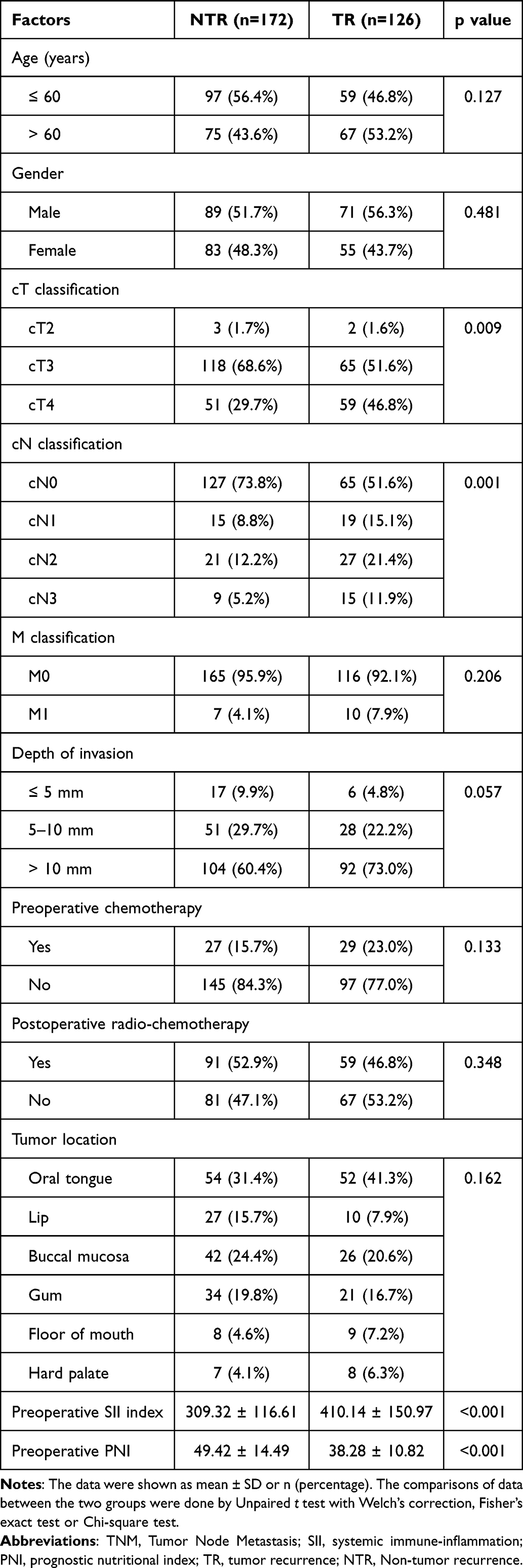 |
Table 1 Univariate Analysis of Clinicopathological Factors for Tumor Recurrence in Patients with Oral Squamous Cell Carcinoma of the Stage of III/IV |
Risk Factors for Tumor Recurrence
In 126 patients with tumor recurrence, the preoperative SII were significantly higher than in 172 patients without recurrence (p < 0.001) (Figure 1A). The preoperative PNI in patients with tumor recurrence were significantly lower than in patients without recurrence (p < 0.001) (Figure 1B).
 |
Figure 1 Comparisons of preoperative systemic immune-inflammation (SII) index (A) and prognostic nutritional index (PNI, B) between tumor recurrence (TR, n = 126) and non-tumor recurrence (NTR, n = 172) in patients with oral squamous cell carcinoma of the stage of III/IV. Notes: The plot was made using GraphPad Prism 8.3.0. ***p < 0.001 from Unpaired t test with Welch’s correction. |
Predictive Performance of PNI and SII for Tumor Recurrence
Pearson correlation analysis showed that PNI had a negative correlation with SII in patients with OSCC of the stage of III/IV (Figure 2).
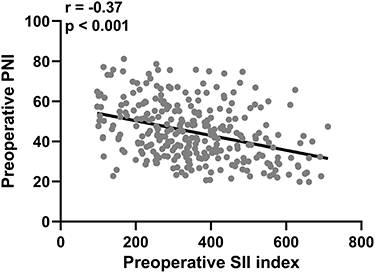 |
Figure 2 Pearson correlation analysis of preoperative systemic immune-inflammation (SII) index and prognostic nutritional index (PNI) in patients with oral squamous cell carcinoma of the stage of III/IV (n = 298). Notes: The plot was made using GraphPad Prism 8.3.0. |
The ROC and AUC were used to compare the predictive abilities of PNI, SII, and their joint for tumor recurrence (Figure 3 and Table 2). The AUC for SII was 0.69 (0.63 to 0.76), for PNI was 0.72 (0.67 to 0.78), and for joint model was 0.81 (0.76 to 0.85). The joint test model had higher AUC than single detection.
 |
Table 2 Predictive Values in ROC Analysis |
 |
Figure 3 ROC analysis of predictive values of preoperative systemic immune-inflammation (SII) index, prognostic nutritional index (PNI) and their joint test model for tumor recurrence in patients with oral squamous cell carcinoma of the stage of III/IV. Note: The plot was made using GraphPad Prism 8.3.0. |
Predictive Performance of the Combination of PNI and SII for Overall Survival
Overall survival curves for 5 years follow-up was shown in Figure 4. Patients with low level of joint model had significantly higher overall survival rate for 5 years follow-up than those with high level (p = 0.006).
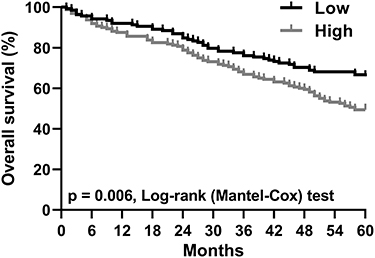 |
Figure 4 According to the cut off in ROC analysis of the joint test model of preoperative SII and PNI, 298 cases of patients with oral squamous cell carcinoma of the stage of III/IV were divided into high (> −0.94, n = 160) and low (< −0.94, n = 138) level. Notes: Overall survival curves during 5 years follow-up were plot. The plot was made using GraphPad Prism 8.3.0. |
Discussion
The clinical outcome of OSCC patients after surgery can be predicted by TNM staging; however, there are significant differences in prognosis among patients at the same TNM stage. Therefore, TNM staging is far from the best indicator in clinical prognosis evaluation.7
Host immune dysregulation, systemic or local excessive inflammation can promote tumor growth, metastasis, and treatment resistance.8 The number and function of tumor-infiltrating lymphocytes are significantly correlated with tumor onset and progression and clinical response to immunotherapy. Previous studies have shown that immune cells can exhibit both tumor-promoting and anti-tumor abilities according to their differentiation status.9 Tumor-infiltrating lymphocytes is composed of two complementary cellular components with different immune mechanisms, among which neutrophils can secrete a variety of cytokines and participate in non-specific inflammatory reactions, while lymphocytes respond to immune regulation, and the ratio of the two can stably reflect the inflammatory state of the body.10 Hematological indicators such as SII are considered as independent factors in the prognostic of many malignant tumors.11–14 High SII values have association with less favorable disease-free survival (DFS) and overall survival (OS) after curative resection in OSCC patients.15 In univariate analysis, high SII were significantly associated with worse disease-specific survival (DSS), and progression-free survival (PFS) of patients with OSCC.16 Another study demonstrated that SII is significantly associated with a poorer OS in univariate analysis but not a significant independent predictor in the multivariate analysis.17
Patients with OSCC of the stage of III/IV were analyzed. In patients with tumor recurrence, the preoperative SII index were significantly higher than in those with no tumor recurrence. This result indicated that the inflammation levels were higher preoperatively in patients with recurrence. The ROC curve was used to determine the predictive value of preoperative SII in OSCC recurrence, using the recurrence or non-recurrence of patients as the dependent variable during the observation period, and the SII value at the highest Youden index as the cut-off value. In this study, the preoperative SII cut-off value was 418.4.
PNI can reflect the immune and nutritional status of cancer patients.18 PNI is an effective prognostic factor in patients with various tumors.19–21 It was used to evaluate the preoperative surgical risk and postoperative complications of patients with tumors.
In advanced OSCC, the risk of malnutrition is increased by dysphagia and odynophagia.22 During the therapy, the changes in PNI are caused by influenced nutritional status and inflammation response. The clinical significance of PNI for OSCC has been elucidated.23 Compared with other inflammation-based biomarkers, PNI is not susceptible to infection, medication, and comorbidity, and is more reproducible and available.24 Thus, PNI is a reliable biomarker to reflect the condition of host antitumor immunity. A low PNI was noted to exhibit a significant association with shorter OS and DFS in patients with OSCC.25 Multivariate analysis identified PNI as an independent prognostic factor for OSCC patients and PNI offered an independent prognostic biomarker in OSCC patients undergoing radical surgery.26
In patients with OSCC of the stage of III/IV, the preoperative PNI were also analyzed. The preoperative PNI was significantly lower in those with tumor recurrence than in those with no tumor recurrence. This result indicated that the nutritional status was worse preoperatively in patients with recurrence. Multivariate analysis between patients with recurrence and patients without recurrence showed that low preoperative PNI was an independent risk factor for postoperative recurrence in OSCC patients. The ROC curve was employed to determine the predictive value of preoperative PNI in OSCC recurrence and the preoperative PNI cut-off value was 47.6.
In this study, we also analyzed the correlation between preoperative PNI and preoperative SII in 298 patients with OSCC of the stage of III/IV. The significant negative correlation between the two indexes suggested that high levels of inflammation are associated with poor nutritional status in stage III–IV OSCC patients. We built a SII and PNI joint model for the prediction of tumor recurrence in OSCC patients. Logit (Joint model) = 0.006 * SII - 0.067 * PNI. ROC analysis of predictive values of the joint test model indicated that this joint model significantly improves the sensitivity or specificity and area under the curve of a single index.
According to the cut off in ROC analysis of the joint test model of preoperative SII and PNI, 298 cases of patients with OSCC of the stage of III/IV were divided into high (> −0.94, n = 160) and low (< −0.94, n = 138) level. Patients with low level of joint model had significantly higher overall survival rate for 5 years follow-up than those with high level. The combined detection of preoperative SII and PNI also had significant value for the long-term prognosis of OSCC patients.
Patients’ immune system exerts a profound impact on the tumor microenvironment of human cancers, whereas the comprehensive investigation of cytokine profiles in tumor-infiltrating T-cells remains lacking. However, in specific tumor contexts (such as Kaposi’s sarcoma, Hodgkin’s disease, bronchial carcinoma, and cervical carcinoma), these T-cells predominantly express interleukins (ILs) 4 and 5, while exhibiting minimal interferon production. Notably, IL-4 and IL-5 are cytokines typically associated with T-helper type 2 (Th2) immune responses, whereas interferon is primarily linked to Th1 responses.27 Our current study therefore provides such an instance where high inflammation is associated with poor nutritional status in late stage OSCC patients. Moreover, the comprehensive analysis of cytokine and chemokine expression profiles within the tumor microenvironment holds greater relevance than focusing solely on the specific immune cell composition,28 hence it will be interesting to explore in the future the association of cytokine profiles, and perhaps the number of leukocytes, with the development of OSCC among different stages of patients.
This study also comes with limitations. First, the patients included were all of Chinese ethnicity, and a more diversified sample pool should be included to further validate the results. Second, this was a single-centered study, therefore to expand the scope and validity of the current data, a multi-centered study should be considered in the future.
Conclusions
In conclusion, both preoperative SII and PNI are valuable independent tumor recurrence prediction index in patients with advanced OSCC. Meanwhile, the combination of preoperative SII and PNI is also valuable on OSCC recurrence and prognosis prediction.
Data Sharing Statement
Data will be made available on request from the corresponding author Manjun Ye.
Statement of Ethics
The study was approved by the ethics committee of Daqing General Hospital, the study was performed in strict accordance with the Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects.
Informed Consent
All participants signed appropriate consent for participating this study.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Guo QY, Wang H, Wang Y. LncRNA H19 polymorphisms associated with the risk of OSCC in Chinese population. Eur Rev Med Pharmacol Sci. 2017;21(17):3770–3774.
2. Hosni A, Huang SH, Chiu K, et al. Predictors of early recurrence prior to planned postoperative radiation therapy for oral cavity squamous cell carcinoma and outcomes following salvage intensified radiation therapy. Int J Radiat Oncol Biol Phys. 2019;103(2):363–373. doi:10.1016/j.ijrobp.2018.09.013
3. Norman K, Pichard C, Lochs H, Pirlich M. Prognostic impact of disease-related malnutrition. Clin Nutr. 2008;27(1):5–15. doi:10.1016/j.clnu.2007.10.007
4. Mirili C, Yilmaz A, Demirkan S, Bilici M, Basol Tekin S. Clinical significance of prognostic nutritional index (PNI) in malignant melanoma. Int J Clin Oncol. 2019;24(10):1301–1310. doi:10.1007/s10147-019-01461-7
5. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
6. Tian BW, Yang YF, Yang CC, et al. Systemic immune-inflammation index predicts prognosis of cancer immunotherapy: systemic review and meta-analysis. Immunotherapy. 2022;14(18):1481–1496. doi:10.2217/imt-2022-0133
7. Gao J, Wang Y, Li F, et al. Prognostic nutritional index and neutrophil-to-lymphocyte ratio are respectively associated with prognosis of gastric cancer with liver metastasis undergoing and without hepatectomy. Biomed Res Int. 2019;2019:4213623. doi:10.1155/2019/4213623
8. Wong L, Bozhilov K, Hernandez B, et al. Underlying liver disease and advanced stage liver cancer are associated with elevated neutrophil-lymphocyte ratio. Clin Mol Hepatol. 2019;25(3):305–316. doi:10.3350/cmh.2019.0004
9. Schilling C, Stoeckli SJ, Vigili MG, et al. Surgical consensus guidelines on sentinel node biopsy (SNB) in patients with oral cancer. Head Neck. 2019;41(8):2655–2664. doi:10.1002/hed.25739
10. Yang J, Wan SQ, Huang L, et al. Analysis of hospitalization costs and length of stay for oral cancer patients undergoing surgery: evidence from Hunan, China. Oral Oncol. 2021;119:105363. doi:10.1016/j.oraloncology.2021.105363
11. Chrom P, Stec R, Bodnar L, Szczylik C. Incorporating Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in place of neutrophil count and platelet count improves prognostic accuracy of the international metastatic renal cell carcinoma database consortium model. Cancer Res Treat. 2018;50(1):103–110. doi:10.4143/crt.2017.033
12. Bazzi WM, Tin AL, Sjoberg DD, Bernstein M, Russo P. The prognostic utility of preoperative neutrophil-to-lymphocyte ratio in localized clear cell renal cell carcinoma. Can J Urol. 2016;23(1):8151–8154.
13. Yao C, Liu X, Tang Z. Prognostic role of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio for hospital mortality in patients with AECOPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2285–2290. doi:10.2147/COPD.S141760
14. Hung SP, Chen PR, Ho TY, et al. Prognostic significance of the preoperative systemic immune-inflammation index in patients with oral cavity squamous cell carcinoma treated with curative surgery and adjuvant therapy. Cancer Med. 2021;10(2):649–658. doi:10.1002/cam4.3650
15. Diao P, Wu Y, Li J, et al. Preoperative systemic immune-inflammation index predicts prognosis of patients with oral squamous cell carcinoma after curative resection. J Transl Med. 2018;16(1):365. doi:10.1186/s12967-018-1742-x
16. Cho U, Sung YE, Kim MS, Lee YS. Prognostic role of systemic inflammatory markers in patients undergoing surgical resection for oral squamous cell carcinoma. Biomedicines. 2022;10(6):1268. doi:10.3390/biomedicines10061268
17. Ruiz-Ranz M, Lequerica-Fernandez P, Rodriguez-Santamarta T, et al. Prognostic implications of preoperative systemic inflammatory markers in oral squamous cell carcinoma, and correlations with the local immune tumor microenvironment. Front Immunol. 2022;13:941351. doi:10.3389/fimmu.2022.941351
18. Li Z, Zhang D, Mo C, Zhu P, Fan X, Tang T. The prognostic significance of prognostic nutritional index in gastrointestinal stromal tumors: a systematic review and meta-analysis. Medicine. 2022;101(47):e32067. doi:10.1097/MD.0000000000032067
19. Demirelli B, Babacan NA, Ercelep O, et al. Modified glasgow prognostic score, prognostic nutritional index and ECOG performance score predicts survival better than sarcopenia, cachexia and some inflammatory indices in metastatic gastric cancer. Nutr Cancer. 2021;73(2):230–238. doi:10.1080/01635581.2020.1749290
20. Okadome K, Baba Y, Yagi T, et al. Prognostic nutritional index, tumor-infiltrating lymphocytes, and prognosis in patients with esophageal cancer. Ann Surg. 2020;271(4):693–700. doi:10.1097/SLA.0000000000002985
21. Wang Z, Wang Y, Zhang X, Zhang T. Pretreatment prognostic nutritional index as a prognostic factor in lung cancer: review and meta-analysis. Clin Chim Acta. 2018;486:303–310. doi:10.1016/j.cca.2018.08.030
22. Kono T, Sakamoto K, Shinden S, Ogawa K. Pre-therapeutic nutritional assessment for predicting severe adverse events in patients with head and neck cancer treated by radiotherapy. Clin Nutr. 2017;36(6):1681–1685. doi:10.1016/j.clnu.2016.10.021
23. Yoshida R, Gohara S, Sakata J, et al. Onodera’s prognostic nutritional index correlates with tumor immune environment and survival in patients with oral squamous cell carcinoma undergoing chemoradiotherapy. Transl Oncol. 2020;13(12):100850. doi:10.1016/j.tranon.2020.100850
24. Bruixola G, Caballero J, Papaccio F, et al. Prognostic nutritional index as an independent prognostic factor in locoregionally advanced squamous cell head and neck cancer. ESMO Open. 2018;3(6):e000425. doi:10.1136/esmoopen-2018-000425
25. Fang KH, Chang SW, Lee YC, et al. Preoperative prognostic nutritional index predicts prognosis of patients with oral cavity cancer. Oral Dis. 2022;28(7):1816–1830. doi:10.1111/odi.13840
26. Watabe Y, Aoki K, Ichikawa H, et al. A preoperative prognostic nutritional index is a prognostic indicator in oral squamous cell carcinoma patients undergoing radical surgery. Int J Oral Maxillofac Surg. 2021;50(11):1413–1421. doi:10.1016/j.ijom.2021.01.009
27. Singh N, Baby D, Rajguru JP, Patil PB, Thakkannavar SS, Pujari VB. Inflammation and cancer. Ann Afr Med. 2019;18(3):121–126. doi:10.4103/aam.aam_56_18
28. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. doi:10.1016/j.cell.2010.01.025
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Factors of Adrenocortical Carcinoma: Experience from a Regional Medical Center in Eastern China
Li P, Su X, Zhang X, Sun L, Zhang G
International Journal of General Medicine 2023, 16:453-465
Published Date: 3 February 2023
Nomogram Based on Preoperative Fibrinogen and Systemic Immune-Inflammation Index Predicting Recurrence and Prognosis of Patients with Borrmann Type III Advanced Gastric Cancer
Wang H, Yin X, Ma K, Wang Y, Fang T, Zhang Y, Xue Y
Journal of Inflammation Research 2023, 16:1059-1075
Published Date: 12 March 2023
Analysis of Pathogenic Bacteria Distribution and Related Factors in Recurrent Acute Cholangitis
Li K, Hu X, Lu Q, Zhang H, Zhou J, Tian S, Zhou F
Infection and Drug Resistance 2023, 16:4729-4740
Published Date: 20 July 2023
Prognostic Nutritional Index (PNI) as a Predictor in Patients with Metabolic Syndrome and Heart Failure
Zhang X, Zhang J, Liu F, Li W, Zhang T, Fang B, Zhang Z, Xie Q, Yang Y, Li X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2503-2514
Published Date: 18 August 2023
NUP62CL as an Immunological and Prognostic Biomarker of Oral Squamous Cell Carcinoma
Yu X, Xu L, Zhou Y, Zhou X, Yang L, Zhou Y
Journal of Inflammation Research 2023, 16:3799-3809
Published Date: 29 August 2023