Back to Journals » International Journal of General Medicine » Volume 15
Correlation of Maternal Prenatal Vitamin D Level with Postnatal Infant Growth in Length and Head Circumference: A Cohort Study on Vitamin D Status and Its Impact During Pregnancy and Childhood in Indonesia
Authors Noviandhari A ![]() , Faisal F
, Faisal F ![]() , Dhamayanti M
, Dhamayanti M ![]()
Received 9 August 2021
Accepted for publication 21 September 2022
Published 6 October 2022 Volume 2022:15 Pages 7631—7637
DOI https://doi.org/10.2147/IJGM.S333380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Anindita Noviandhari, Faisal Faisal, Meita Dhamayanti
Department of Child Health, Hasan Sadikin Hospital, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Anindita Noviandhari, Jl Durma 27, Bandung, West Java, 40264, Indonesia, Tel +62 8122029854, Fax +62 22 2035957, Email [email protected]; [email protected]
Objective: To determine the correlation of first trimester maternal 25-(OH)-D level with postnatal infant growth in Indonesia.
Materials and Methods: A cohort of 116 mother–infant pairs from Indonesia was prospectively studied. 25-(OH)-D level was measured in maternal serum at 10– 14 weeks of gestation and in umbilical cord blood shortly after birth. The newborns were observed longitudinally for 24 months. Length and head circumference were measured at birth and at ages 3, 6, 12, and 24 months. Spearman correlation and multiple linear regression analyses were performed.
Results: Mean 25-(OH)-D levels in the prenatal maternal serum and umbilical cord blood were 17.55 ± 7.33 ng/mL and 16.27 ± 6.14 ng/mL, respectively. Prenatal maternal 25-(OH)-D level weakly correlated with infant length (r = − 0.35) and head circumference (r = – 0.21) z-scores at age 3 months. Umbilical cord blood 25-(OH)-D level did not correlate with infant length or head circumference at any time point. Multiple linear regression showed an independent association between prenatal maternal 25-(OH)-D level and infant length z-score at age 3 months (p = 0.01, SE β = 0.02, and coefficient β = − 0.06).
Conclusion: First trimester maternal serum 25(OH)D level correlated with infant length and head circumference at age 3 months.
Keywords: umbilical cord blood, first trimester, infant, growth, pregnancy, vitamin D
Introduction
Vitamin D is a secosteroid prohormone with two active metabolites, calcidiol (25-(OH)-D) and calcitriol (1,25-OH2-D); each has roles in various metabolic processes.1 Several randomized clinical trials have shown the importance of vitamin D supplementation during the first 6 months of life in promoting growth in low birth weight babies.2 Vitamin D status during pregnancy and the first two years of life have a long-term effects on bone structure.3,4
Vitamin D deficiency during pregnancy has become a significant global health problem. Reported prevalence rates of vitamin D deficiency in pregnant women range from 20% to 90%.5,6 One study of 160 pregnant women in West Java reported a normal vitamin D level (>30 ng/mL) in only 3.5% of subjects in the first trimester of pregnancy; 21% were diagnosed with vitamin D insufficiency (25-(OH)-D level 25–29.6 ng/mL) and 75.5% with vitamin D deficiency (25-(OH)-D level <20 ng/mL).7,8 Vitamin D deficiency occurs in 40% to 50% of children worldwide. In Indonesia and Vietnam, the percentage of children with adequate 25-(OH)-D status is approximately 5% and 20%, respectively.9
Vitamin D deficiency has detrimental skeletal and extraskeletal consequences, especially in children. Up to 50% of children in countries with different economic status that receive a sufficient amount of sunshine across Africa, Asia, Europe, and North America are predicted to be vitamin D deficient.6 The American Academy of Pediatrics and Institute of Medicine both define vitamin D deficiency and insufficiency in children as 25-(OH)-D levels of ≤15 ng/mL and ≤20 ng/mL, respectively. The Endocrine Society Task Force on Vitamin D defines deficiency in children as 25-(OH)-D level ≤20 ng/mL, which is the same definition for adults.10,11
Although previous studies of the association of maternal vitamin D level during pregnancy with intrauterine or postnatal child growth are abundant, their findings are inconsistent and their recommendations vary.12–20 Moreover, few studies have examined vitamin D status in tropical countries.13 This study aimed to analyze the correlation of prenatal maternal vitamin D level in the first trimester with postnatal infant growth in Indonesian mothers and infants.
Materials and Methods
This study was part of a more extensive prospective cohort study conducted in Sukabumi city and Waled district, West Java, Indonesia from July 2016 to April 2018. The study was approved by the Research Ethics Committee of Universitas Padjadjaran.
The study subjects were women in early pregnancy with gestational age 10 to 14 weeks. All were singleton pregnancies. Women with associated comorbidities such as diabetes mellitus or pre-eclampsia were excluded. Midwives at primary health centers informed prospective participants of the study and then referred them to Al Mulk Hospital Sukabumi or Waled District Hospital to obtain more comprehensive information. Mothers who agreed to participate provided written informed consent. The subjects were observed during pregnancy until the time of labor. 25-(OH)-D level was measured in maternal serum at 10–14 weeks of gestation and in umbilical cord blood shortly after birth. The newborns were observed longitudinally for 24 months. Length and head circumference were measured at birth and at age 3, 6, 12, and 24 months.
25-(OH)-D blood level was measured using the enzyme-linked fluorescent assay technique with the VIDAS® 25 OH Vitamin D TOTAL (Biomerieux, Marcy-l’Étoile, France), an automated system that combines enzyme immunoassay and final fluorescence detection. This technique can measure 25-(OH)-D over a wide range of levels and correlates well with liquid chromatography-tandem mass spectroscopy results, the gold standard method of vitamin D level measurement.21 Anthropometric measurements were performed by trained staff according to World Health Organization standards.22 Growth measurements were converted to z scores using the World Health Organization Anthro Calculator.23
Categorical data are presented as numbers with percentage. Continuous data are presented as means with standard deviation. Maternal and umbilical cord blood 25-(OH)-D levels were compared between various patient characteristic groups using the Mann–Whitney U-test or Kruskal–Wallis test as appropriate. Spearman’s rank correlation was used to determine the correlations between maternal and umbilical cord blood 25-(OH)-D levels and z scores of infant length and head circumference. The correlation of other covariates with length and head circumference z scores was analyzed using multiple linear regression. Statistical analyses were conducted using SPSS software version 20 (IBM Corp., Armonk, NY, USA). P < 0.05 was considered significant.
Results
One hundred forty-two pregnant women in public health centers across Sukabumi and Waled district were eligible for study inclusion. After exclusions, including one newborn with anencephaly, 116 mother–infant pairs were analyzed. Mother and infant characteristics, maternal serum and umbilical cord blood 25-(OH)-D levels are shown in Table 1. Maternal serum and umbilical cord blood 25-(OH)-D levels did not differ between subjects when grouped according to various characteristics, except for maternal educational level.
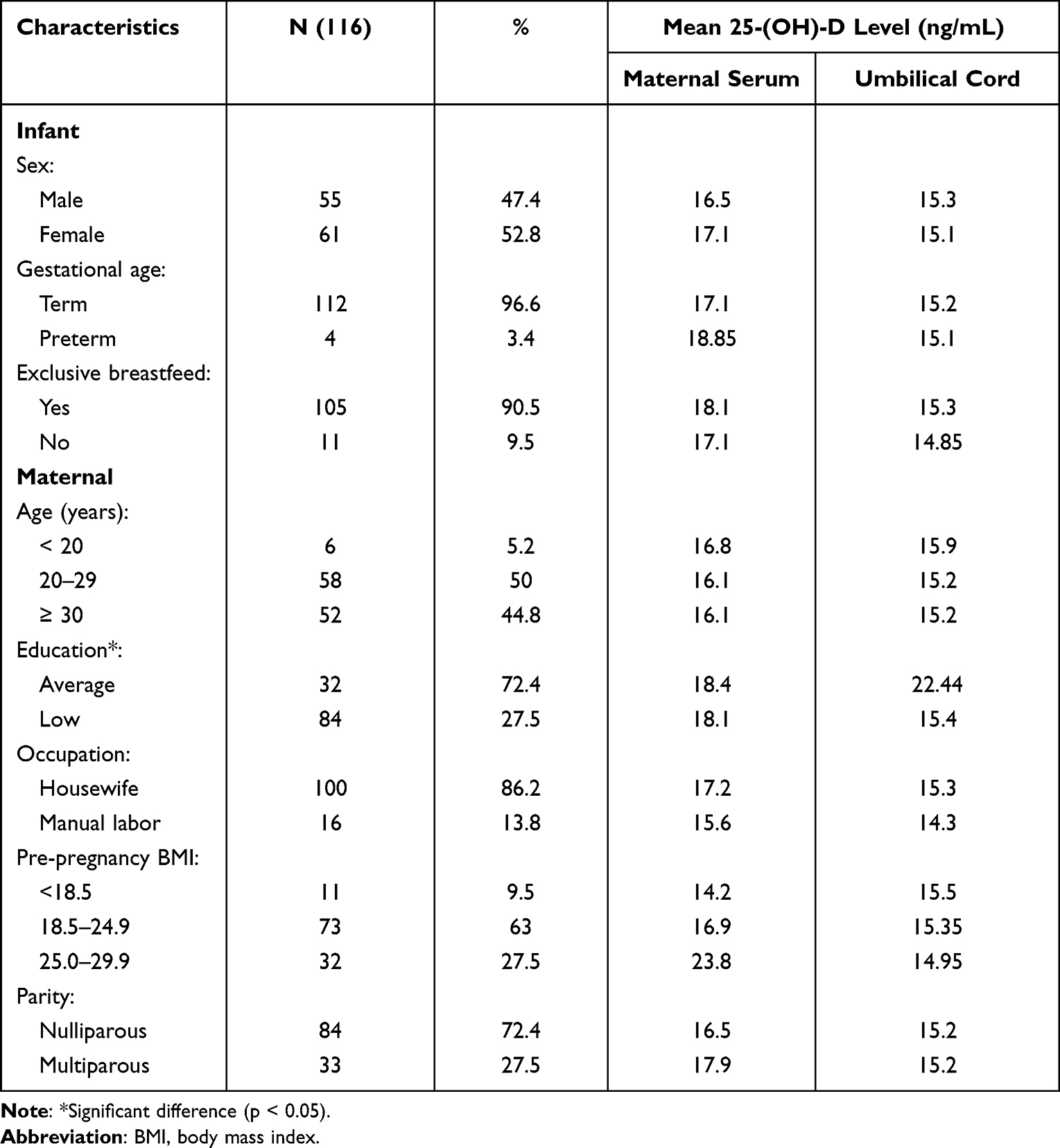 |
Table 1 Characteristics of Mother, Infant and Mean 25-(OH)-D Level |
Distribution of patients grouped according to 25-(OH)-D level status (insufficiency, deficiency, normal) in maternal serum and umbilical cord blood is shown in Figure 1. Overall, the normal status of vitamin D (25-(OH)-D ≥20 ng/mL) about 22%, meanwhile the mean 25-(OH)-D levels in maternal and umbilical cord blood were 17.55 ± 7.33 ng/mL and 16.27 ± 6.14 ng/mL, respectively.
 |
Figure 1 Distribution of patients grouped according to 25-(OH)-D status in prenatal maternal serum and umbilical cord blood. |
Infant length and head circumference z scores at birth and ages 3, 6, 12, and 24 months are depicted in Table 2. Correlation of prenatal maternal serum and umbilical cord blood 25-(OH)-D levels with infant length and head circumference z scores over time is shown in Table 3.
 |
Table 2 Infant Length and Head Circumference z Scores Over Time |
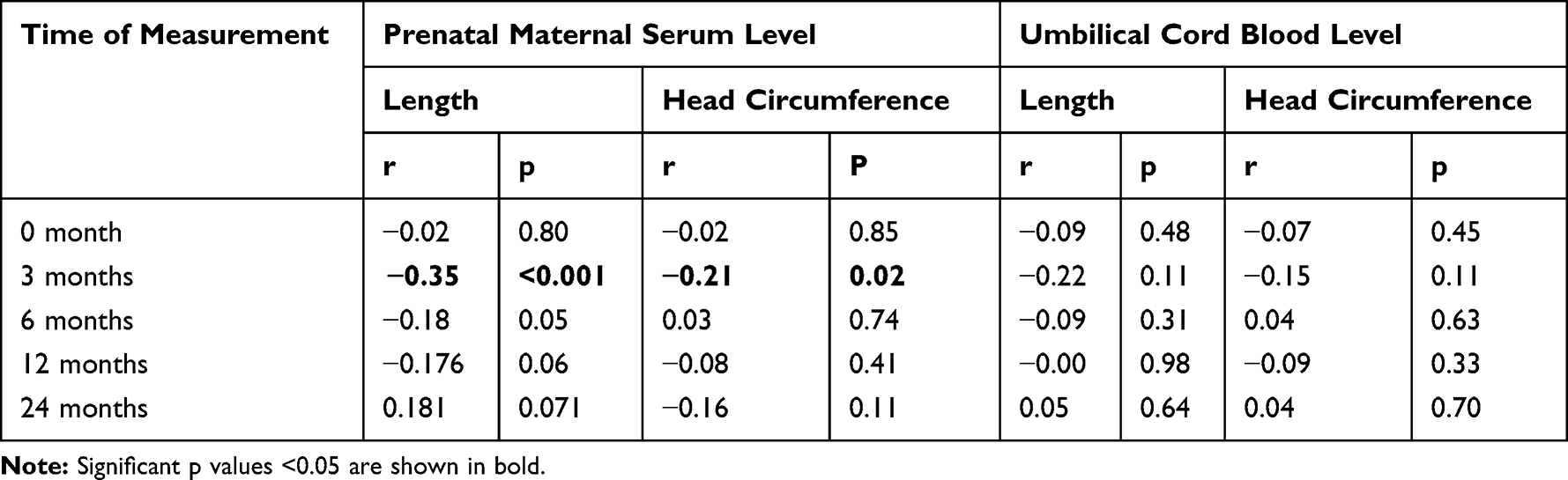 |
Table 3 Spearman Correlation Analysis of Prenatal Maternal Serum and Umbilical Cord Blood 25-(OH)-D Level with Infant Length and Head Circumference z Scores |
Prenatal maternal serum 25-(OH)-D level significantly correlated with both length and head circumference z scores at age 3 months. In contrast, umbilical cord blood level did not significantly correlate with either at any time point. Multiple regression analysis of factors associated with infant length and head circumference z scores at age 3 months is shown in Table 4. Prenatal maternal 25-(OH)-D level was independently associated with infant length z score (p = 0.01).
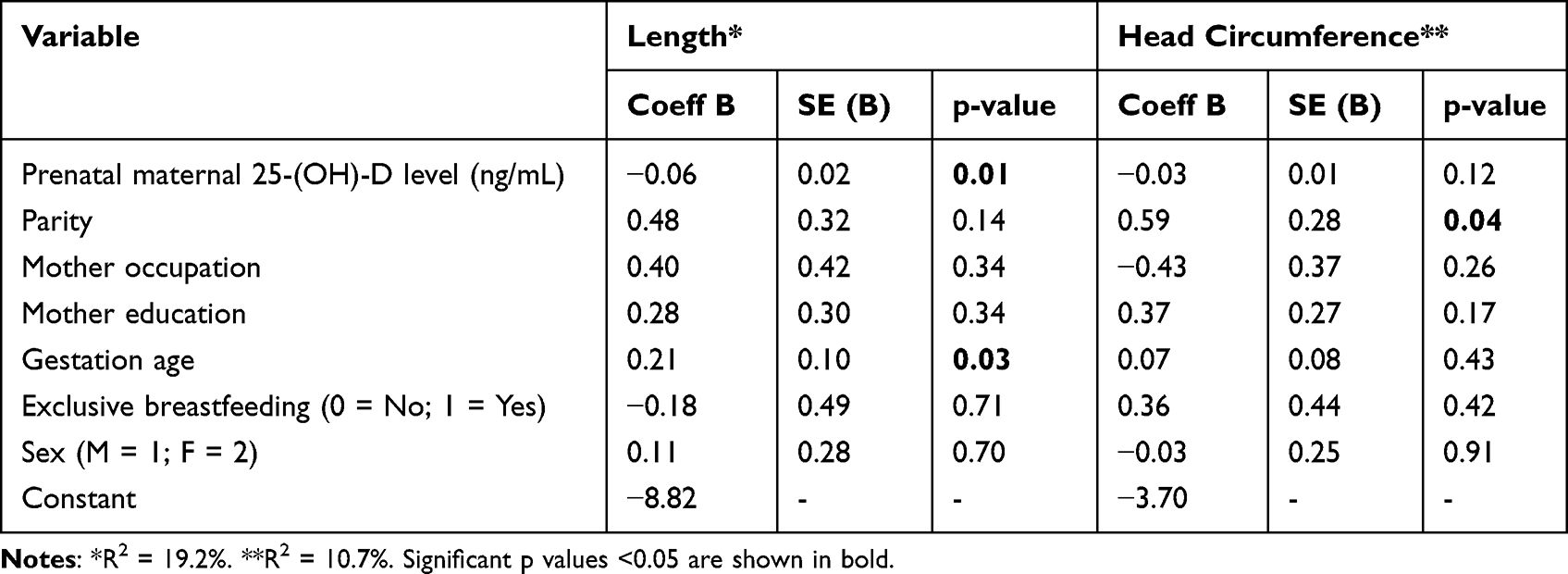 |
Table 4 Multiple Regression Analysis of Factors Associated with Infant Length and Head Circumference at Age 3 Months |
Discussion
Approximately one billion people around the world have vitamin D insufficiency or deficiency despite residing in countries with year-round exposure to sunshine.11 In this study of 25-(OH)-D level measured in pregnant women at 10 to 14 weeks of gestational age and in the umbilical cord at the time of birth, the level was insufficient or deficient at both time points. Totally about 78% pregnant women had hypovitaminosis, which is higher than the study in Brazil.24 Low vitamin D level in pregnancy is associated with lower birth weight and increased risk of small for gestational age.12,16,19,24 Low maternal vitamin D level is also associated with poor intrauterine fetal growth.16 Vitamin D deficiency may result in reduced linear growth and skeletal development. A recent study in West Java, Indonesia, reported that maternal serum vitamin D level was significantly associated with fetal biparietal diameter (β = 0.172, p = 0.028) and abdominal circumference (β = 0.819, p = 0.001).25 The impact of maternal vitamin D status on infant growth may continue beyond birth.16,18,20
To our knowledge, this is the first study in Indonesia to examine the association of prenatal maternal and umbilical cord vitamin D levels with infant measurements in the first 2 years of life. Other cohort studies in Singapore,13 Vietnam,14 and Sri Lanka15 found no correlation between maternal vitamin D deficiency and anthropometric measurements at birth and postnatal growth in the first two years of life. In a recent systematic review,20 infant weight was not correlated with maternal or umbilical cord blood vitamin D levels. Studies conducted in a multi-ethnic Asian population and an Australian population have reported similar findings.13,18
Previous studies have shown that maternal vitamin D level is significantly associated with infant linear growth at age 9 months and that a low level may increase the risk of stunted growth by four times12,26 Meanwhile, our study demonstrated an inverse correlation between prenatal maternal 25-(OH)-D level and infant length at age 3 months. This conforms to similar studies, which have shown an inverse association of maternal 25-(OH)-D level and infant length at age 6 months.14,16 By age 12 months, infant vitamin D levels increase, which may result in a growth spurt in length.12 On the other hand, the vitamin D level in pregnancy and obstetric results was associated with maternal polymorphisms in VDR. Hence, the VDR polymorphism may be a protective or risk factor for adverse events, according to the genetic profile of the woman.27 Our head circumference findings were similar to those of several other studies conducted in subtropical or tropical countries that demonstrated no correlation with umbilical cord blood vitamin D level.13,18–20
This study had several limitations. Confounding may have occurred because of interrelations among growth, eating patterns, comorbidities, and macro- and micro-nutritional intake. Since genetic variation may influence serum concentration of vitamin D, future longitudinal prospective and bigger studies are warranted.
Conclusion
Maternal serum 25-(OH)-D level in the first trimester of pregnancy had a significant inverse correlation with infant length and head circumference measured at age 3 months. Future studies should examine other infant growth parameters, such as muscle mass and adiposity, and consider more comprehensive maternal data regarding socioeconomic status, daily food intake, and nutrition.
Data Sharing Statement
The datasets from this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Ethics Research Committee of Universitas Padjadjaran (No. 133/UN6.KEP/EC/2018) and performed in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent.
Acknowledgments
We would like to thank the staff of Waled Hospital, Al Mulk Hospital Sukabumi, and Sukabumi Health Office and Primary Healthcare Centers for their contributions. We also thank Lani Gumilang, Bunga Mars, Putri Anisa, and Devi Yuli Agustini for their efforts as field researchers and Hadyana Sukandar for his statistical expertise.
Author Contributions
All authors made a significant contribution to the study, whether in conception, study design, execution, data acquisition, analysis, or interpretation. The authors also took part in drafting, revising, and critically reviewing the article and approved the final version for publication by this journal. The authors agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant-in-aid from Universitas Padjadjaran (No. 2476 /UN6.C/LT/2018).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Gil A, Plaza-Diaz J, Mesa MD, Vitamin D. Classic and novel actions. Ann Nutr Metab. 2018;72(2):87–95. doi:10.1159/000486536
2. Kumar GT, Sachdev HS, Chellani H, et al. Effect of weekly vitamin D supplements on mortality, morbidity, and growth of low birthweight term infants in India up to age 6 months: randomised controlled trial. Br Med J. 2011;342:d2975. doi:10.1136/bmj.d2975
3. Cooper C, Javaid K, Westlake S, Harvey N, Dennison E. The influence of vitamin D on bone health across the life cycle. J Nutr. 2005;135(11):2728S–2734S. doi:10.1093/jn/135.11.2728S
4. Javaid MK, Crozier SR, Harvey NC, et al.; The Princess Anne Hospital Study Group. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years- a longitudinal study. Lancet. 2006;367(367):36–43. doi:10.1016/S0140-6736(06)67922-1
5. Morales E, Guxens M, Llop S, et al. Circulating 25-hydroxyvitamin D3 in pregnancy and infant neuropsychological development. Pediatrics. 2012;130(4):e913–e920. doi:10.1542/peds.2011-3289
6. Al-Wassia H, Abo-Ouf N. Prevalence of vitamin D deficiency in mother–infant pairs in a tertiary hospital in the west coast of Saudi Arabia. J Clin Neonatol. 2016;5(4):243. doi:10.4103/2249-4847.194164
7. Judistiani RTD, Gumilang L, Nirmala SA, et al. Association of Colecalciferol, Ferritin, and anemia among pregnant women: result from cohort study on vitamin d status and its impact during pregnancy and childhood in Indonesia. Anemia. 2018;2018:2047981. doi:10.1155/2018/2047981
8. Dhamayanti M, Noviandhari A, Supriadi S, Judistiani RT, Setiabudiawan B. Association of maternal vitamin D deficiency and infants’ neurodevelopmental status: a cohort study on vitamin D and its impact during pregnancy and childhood in Indonesia. J Paediatr Child Health. 2020;56(1):16–21. doi:10.1111/jpc.14481
9. Poh BK, Rojroongwasinkul N, Nguyen BK, et al. 25-hydroxy-vitamin D demography and the risk of vitamin D insufficiency in the South East Asian Nutrition Surveys (SEANUTS). Asia Pac J Clin Nutr. 2016;25(3):538–548. doi:10.6133/apjcn.092015.02
10. Munns CF, Shaw N, Kiely M, et al. Global consensus recommendations on prevention and management of nutritional rickets. J Clin Endocrinol Metabol. 2016;101(2):394–415. doi:10.1210/jc.2015-2175
11. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metabol. 2011;96(7):1911–1930. doi:10.1210/jc.2011-0385
12. Leffelaar ER, Vrijkotte TG, van Eijsden M. Maternal early pregnancy vitamin D status in relation to fetal and neonatal growth: results of the multi-ethnic Amsterdam Born Children and their Development cohort. Br J Nutr. 2010;104(1):108–117. doi:10.1017/S000711451000022X
13. Ong YL, Quah PL, Tint MT, et al. The association of maternal vitamin D status with infant birth outcomes, postnatal growth and adiposity in the first 2 years of life in a multi-ethnic Asian population: the Growing Up in Singapore Towards healthy Outcomes (GUSTO) cohort study. Br J Nutr. 2016;116(4):621–631. doi:10.1017/S0007114516000623
14. Hanieh S, Ha TT, Simpson JA, et al. Maternal vitamin D status and infant outcomes in rural Vietnam: a prospective cohort study. PLoS One. 2014;9(6):e99005. doi:10.1371/journal.pone.0099005
15. Anusha K, Hettiaratchi UPK, Liyanage G, Gunasekera DPS. Vitamin D status of pregnant mothers and its effect on anthropometric measures in the offspring: a preliminary study. Sri Lanka J Child Health. 2018;47(3):210. doi:10.4038/sljch.v47i3.8540
16. Eckhardt CL, Gernand AD, Roth DE, Bodnar LM. Maternal vitamin D status and infant anthropometry in a US multi-centre cohort study. Ann Hum Biol. 2015;42(3):215–222. doi:10.3109/03014460.2014.954616
17. Gale CR, Robinson SM, Harvey NC, et al. Maternal vitamin D status during pregnancy and child outcomes. Eur J Clin Nutr. 2008;62(1):68–77. doi:10.1038/sj.ejcn.1602680
18. Gould JF, Anderson AJ, Yelland LN, et al. Association of cord blood vitamin D with early childhood growth and neurodevelopment. J Paediatr Child Health. 2017;53(1):75–83. doi:10.1111/jpc.13308
19. Aghajafari F, Nagulesapillai T, Ronksley PE, Tough SC, O’Beirne M, Rabi DM. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: systematic review and meta-analysis of observational studies. BMJ. 2013;346:f1169. doi:10.1136/bmj.f1169
20. Santamaria C, Bi WG, Leduc L, et al. Prenatal vitamin D status and offspring’s growth, adiposity and metabolic health: a systematic review and meta-analysis. Br J Nutr. 2018;119(3):310–319. doi:10.1017/S0007114517003646
21. Moreau E, Bacher S, Mery S, et al. Performance characteristics of the VIDAS(R) 25-OH Vitamin D Total assay - comparison with four immunoassays and two liquid chromatography-tandem mass spectrometry methods in a multicentric study. Clin Chem Lab Med. 2016;54(1):45–53. doi:10.1515/cclm-2014-1249
22. World Health Organization. The WHO Child Growth Standards. Geneva: World Health Organization; 2012.
23. World Health Organization. WHO Anthro, Version 3.2.2 [Computer Program]. Geneva: World Health Organization; 2011.
24. Pereira-Santos M, Carvalho GQ, Dos Santos DB, Oliveira AM. Influence of vitamin D serum concentration, prenatal care and social determinants on birth weight: a northeastern Brazilian cohort study. Br J Nutr. 2019;122(3):284–292. doi:10.1017/S0007114519001004
25. Judistiani RTD, Madjid TH, Irianti S, et al. Association of first trimester maternal vitamin D, ferritin and hemoglobin level with third trimester fetal biometry: result from cohort study on vitamin D status and its impact during pregnancy and childhood in Indonesia. BMC Pregnancy Childbirth. 2019;19(1):112. doi:10.1186/s12884-019-2263-1
26. Toko EN, Sumba OP, Daud II, et al. Maternal vitamin D status and adverse birth outcomes in children from rural Western Kenya. Nutrients. 2016;8(12):794. doi:10.3390/nu8120794
27. Pereira-Santos M, Carvalho GQ, Louro ID, Dos Santos DB, Oliveira AM. Polymorphism in the vitamin D receptor gene is associated with maternal vitamin D concentration and neonatal outcomes: a Brazilian cohort study. Am J Hum Biol. 2019;31(4):e23250. doi:10.1002/ajhb.23250
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.