Back to Journals » Infection and Drug Resistance » Volume 16
Correlation of Coagulation Dysfunction with Infection and Hypercapnia in Acute Exacerbation of COPD Patients
Authors Zheng LL, Wang S, Li ZG, Han L, Zhu CD, Li CY, Zhang XX, Deng X
Received 18 May 2023
Accepted for publication 2 August 2023
Published 18 August 2023 Volume 2023:16 Pages 5387—5394
DOI https://doi.org/10.2147/IDR.S421925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Li-Li Zheng,1 Sheng Wang,1 Ze-Geng Li,2 Lei Han,2 Chun-Dong Zhu,1 Chun-Ying Li,1 Xing-Xing Zhang,1 Xue Deng1
1Department of Respiratory Medicine of Geriatrics Center, The First Affiliated Hospital of Anhui University of Traditional Chinese Medicine, Hefei, 230000, People’s Republic of China; 2Anhui University of Traditional Chinese Medicine, Hefei, 230000, People’s Republic of China
Correspondence: Sheng Wang, Department of Respiratory Medicine, Geriatrics Center, The First Affiliated Hospital of Anhui University of Traditional Chinese Medicine, 117 Meishan Road, Shushan District, Hefei, 230000, People’s Republic of China, Tel +86 13855182043, Email [email protected]
Background: This study aims to explore the factors influencing the coagulation function of patients with chronic obstructive pulmonary disease (COPD) and its effects on thrombosis.
Methods: A total of 155 COPD patients, including 118 patients with acute exacerbation of COPD (AECOPD) and 37 patients with stable COPD (SCOPD), were enrolled in this study. Meanwhile, 50 patients with gastrointestinal polyps found during physical examination and treated with surgery in the same period were enrolled as the control group. The basic data, routine blood tests, C-reactive protein (CRP), procalcitonin (PCT), and coagulation indexes of the three groups were collected, as well as arterial blood gas indexes of AECOPD patients.
Results: The differences in erythrocyte count and hemoglobin among groups were not statistically significant. Compared with the SCOPD group and control group, white blood cell (WBC), neutrophil percentage, PCT, CRP, prothrombin time (PT), and fibrinogen (FIB) in the AECOPD group increased significantly, while the international normalized ratio (INR) decreased (P < 0.05). The differences in activated partial thromboplastin time (APTT) and D-dimer among groups were not statistically significant (P > 0.05). Thrombin time (TT) in the AECOPD group was shorter than that of the control group, and PT was longer than that of the SCOPD group (P < 0.05). Five patients with AECOPD and one patient with SCOPD had venous thrombosis.
Conclusion: The abnormal coagulation function in AECOPD patients is related to the degree of infection and hypercapnia, which may be a risk factor for thrombosis.
Keywords: acute exacerbation of chronic obstructive pulmonary disease, AECOPD, abnormal coagulation function, infection, thrombosis
Background
Chronic obstructive pulmonary disease (COPD) is a common, preventable, and treatable chronic airway disease that is characterized by persistent airflow restriction and corresponding respiratory symptoms; its pathological changes are mainly airway and/or alveolar abnormalities, which are usually related to significant exposure to harmful particles or gases, genetic susceptibility, abnormal inflammatory response, abnormal lung development, and other host factors participating in pathogenesis.1,2 Academician Chen Wang et al3 reveal that, at present, the overall prevalence of COPD among people aged 20 and over in China is 8.6%, of which the prevalence among people aged 40 and over is 13.7%; it is estimated that nearly 100 million people in China have COPD. COPD patients suffer 0.5–3.5 times more each year from acute exacerbation, and the average hospitalization cost per person is up to 12,000 yuan, which has seriously increased the economic burden of patients and society. The early inflammatory response of COPD is confined to the trachea and lungs, but in the course of the disease, hypoxia and chronic inflammation affect the whole body. When respiratory failure occurs in patients with acute exacerbation of COPD (AECOPD), circulatory and coagulation dysfunction often occurs, which is considered to be the cause of thrombotic events.4 Furthermore, abnormal coagulation and thrombosis may accelerate the progress of COPD, resulting in prolonged hospitalization, high hospitalization costs, poor prognosis, and even increased mortality.
Coagulation dysfunction and its role in COPD have been explored for many years. More and more evidence show that a hypercoagulable state exists in COPD, involving changes in a variety of coagulation factors.5 However, the pathogenesis of coagulation dysfunction caused by COPD remains unclear. Its main pathological manifestation, though, is local hypoxia in the lung, induced by inflammatory mediators acting on vasoactive receptors in the lung parenchyma, thereby resulting in repeated damage and repair of the airway wall, thickening and narrowing of the lumen, destruction of lung parenchyma, and thickening of the pulmonary vascular wall.6,7 Inflammatory mediators aggravate the airway inflammatory response, leading to pulmonary vascular injury and thereby making the function of endothelial cells of pulmonary arterioles abnormal. This results in the release of a large number of inflammatory and coagulation mediators, thus activating the coagulation mechanism, finally leading to abnormal platelet and coagulation functions and a sudden increase in the level of D-dimer (D-D) in the blood.8,9 Smoking is an important risk factor for thrombotic diseases. Toxic substances in cigarettes, such as nicotine and tar, can damage vascular endothelium and cause vascular endothelial dysfunction, thus promoting thrombosis.10 Additionally, smoking can damage lung tissue, resulting in the secretion of macrophages, participate in the inflammatory response, and activate the coagulation system. Therefore, the risk of thrombotic disease in people who have been exposed to cigarette smoke for a long time is higher than that of the general population.11 Studies reveal that when COPD patients have hypercapnia, they develop coagulation dysfunction. Activation of the coagulation system is a common phenomenon in inflammatory diseases. The degree of activation of the coagulation system increases during exacerbation of COPD.12 Studies reveal that abnormal coagulation function is seriously high in severe infection and that the main reason for its formation is the imbalance between the formation and clearance of intravascular fibrin.13,14 However, the risk factors for coagulation dysfunction in COPD patients are not clear. Obviously, discovering the causes of coagulation dysfunction in AECOPD is helpful in taking early intervention measures to improve the prognosis of patients. In this study, COPD patients hospitalized in the Department of Geriatric Respiratory Medicine of our hospital from January 2020 to December 2021 were enrolled as research subjects to explore the influencing factors of coagulation status and its impact on thrombosis in patients with COPD for the sake of devising timely and effective intervention methods to reduce the occurrence of pulmonary embolism secondary to COPD.15
Methods
Subjects
A total of 155 consecutive COPD patients hospitalized in our department from January 2020 to December 2021, along with 50 age-matched patients with gastrointestinal polyps found in physical examinations conducted during the same period, were fully enrolled as research subjects. All COPD patients met the Guidelines for the Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease (2013 Revision) formulated by the respiratory branch of the Chinese Medical Association and had previously been clinically diagnosed with COPD. The other inclusion criteria included patients who did not receive anticoagulation treatment in recent three months; patients who had no history of drug allergy and drug contraindications; and patients who knew about the study and could cooperate. The exclusion criteria were as follows: patients with tumors; patients suffering from pulmonary tuberculosis, bronchiectasis, asthma, or other lung diseases; patients suffering from diabetes, blood system diseases, and other diseases; patients with infections at other sites; patients with autoimmune diseases; and patients with liver and kidney dysfunction. This study was discussed and approved by the ethics committee of our hospital, and signed informed consent was given by all patients.
Data Acquisition
Using the method of retrospective investigation, the data of the cases that met the above conditions in the electronic medical record system were retrieved, and each case was recorded in detail, including the general information of the patient (course of disease, inpatient number, name, gender, and age); venous thrombosis of the lower limbs; blood examination results, including the first routine blood test results after admission (white blood cell [WBC] count, red blood cell count, hemoglobin, and neutrophil percentage [N%]), coagulation function indicators (prothrombin time [PT], activated partial thromboplastin time [APTT], international standardized ratio [INR], fibrinogen [FIB], thrombin time [TT], and D-D), and blood inflammation indicators (C-reactive protein and procalcitonin). In AECOPD patients, the blood gas analysis results of the latest blood samples were noted.
Statistical Analysis
Data were statistically analyzed using SPSS 26.0 software. Normally distributed data were expressed as a mean ± standard deviation ( ) and compared among multiple groups using one-way analysis of variance. For data with homogeneity of variance, pairwise comparison was conducted using the least significant difference (LSD) test, and data with heterogeneity of variance was compared using Dunnett’s T3 test. Non-normally distributed measurement data were expressed as the median, compared among multiple groups using the Kruskal–Wallis rank sum test, and pairwise comparison was conducted using the Bonferroni test. Count data were expressed as percentages (%) and compared between two groups using the Chi-square test. Correlation analysis was conducted using Spearman correlation analysis. P < 0.05 was considered statistically significant.
) and compared among multiple groups using one-way analysis of variance. For data with homogeneity of variance, pairwise comparison was conducted using the least significant difference (LSD) test, and data with heterogeneity of variance was compared using Dunnett’s T3 test. Non-normally distributed measurement data were expressed as the median, compared among multiple groups using the Kruskal–Wallis rank sum test, and pairwise comparison was conducted using the Bonferroni test. Count data were expressed as percentages (%) and compared between two groups using the Chi-square test. Correlation analysis was conducted using Spearman correlation analysis. P < 0.05 was considered statistically significant.
Results
Comparison of Demographic Baseline Data
A total of 205 subjects were included in this study. There were 118 cases in the AECOPD group, 37 cases in the stable COPD (SCOPD) group, and 50 cases in the healthy control group. Of the 118 AECOPD patients, 101 patients were male (85.6%), 17 patients were female (14.4%), the average age was 78.53 ± 7.82 years old, and venous thrombosis was found in five patients by B-ultrasound. Of the 37 patients with SCOPD, 33 patients were male (89.2%), 4 patients were female (10.8%), the average age was 78.22 ± 5.21 years old, and lower limb venous thrombosis was found in one patient by B-ultrasound. Of the 50 patients in the control group, 42 patients were male (84%), 8 patients were female (16%), and the average age was 76.86 ± 3.82 years old. There were no significant differences in age or gender between the AECOPD group, the SCOPD group, and the control group (Table 1).
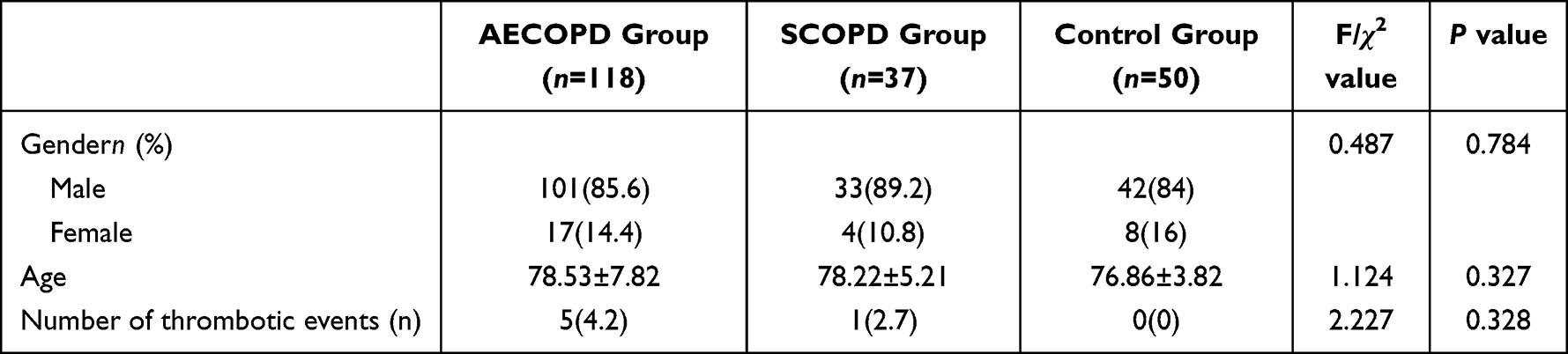 |
Table 1 Baseline Data of Patients in Three Groups |
Comparison of Routine Blood Test, PCT, and CRP
The differences in erythrocyte count and hemoglobin levels among groups were not statistically significant (P > 0.05). The differences in WBC, N%, PCT, and CRP among the three groups were all statistically significant (P < 0.05). WBC, N%, PCT, and CRP were significantly higher in the AECOPD group than in the SCOPD group and the control group, where the differences were statistically significant (P < 0.05, Table 2). In this study, blood gas analysis data of AECOPD patients were collected and retrieved. The results revealed that some patients had abnormal blood gas and acidosis. Among them, 21 cases (17.8%) had arterial blood pH lower than 7.35, and 61 cases (51.69%) had arterial blood CO2 partial pressure (PaCO2) higher than 50 mmHg.
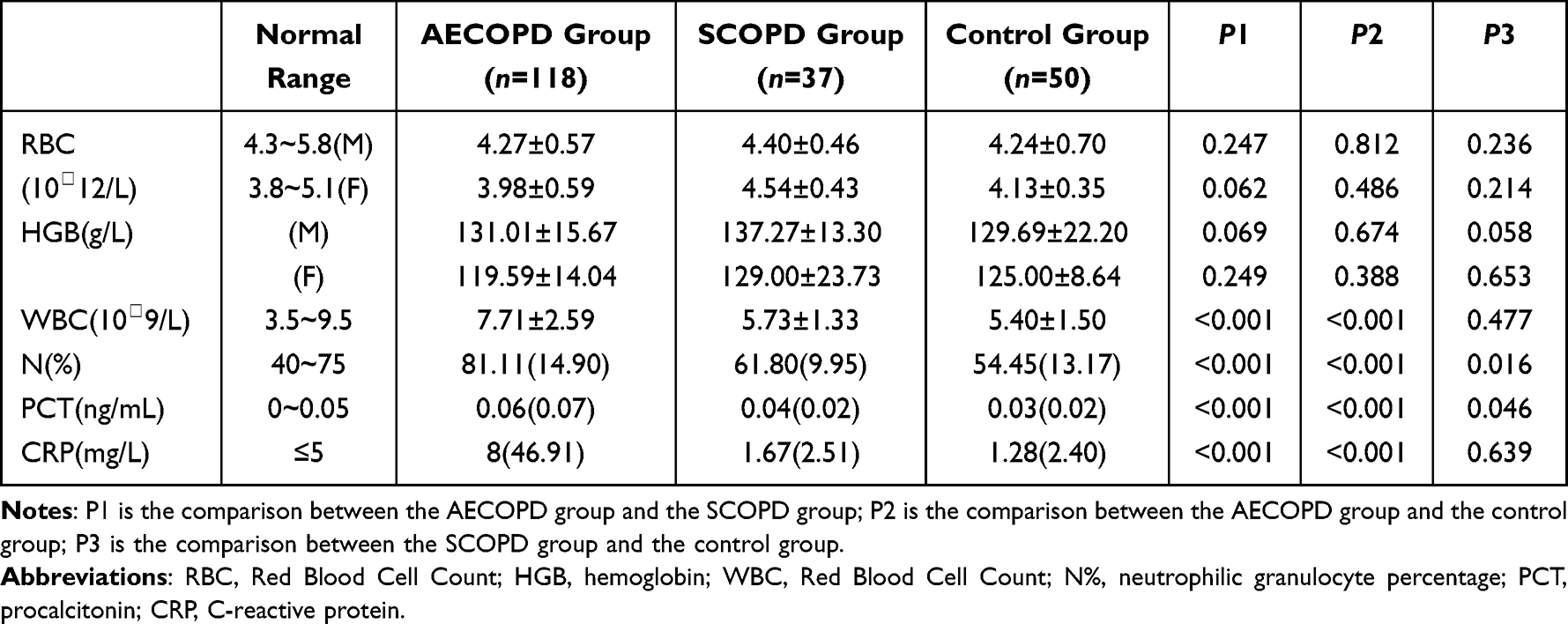 |
Table 2 Comparison of Routine Blood Test, PCT and CRP Indexes of Three Groups of Patients |
Comparison of Coagulation Indicators
There were no significant differences in APTT and D-D levels among the AECOPD group, the SCOPD group, and the control group (P > 0.05). The differences in TT, PT, FIB, and INR among the three groups were all statistically significant (P < 0.05). Compared with the SCOPD group and the control group, the FIB index in the AECOPD group was significantly higher, while the INR value was significantly lower, the differences being statistically significant (P < 0.05). PT in the AECOPD group was significantly longer than that of the SCOPD group, and TT in the AECOPD group was significantly shorter than that of the control group, the differences being statistically significant (P < 0.05, Table 3).
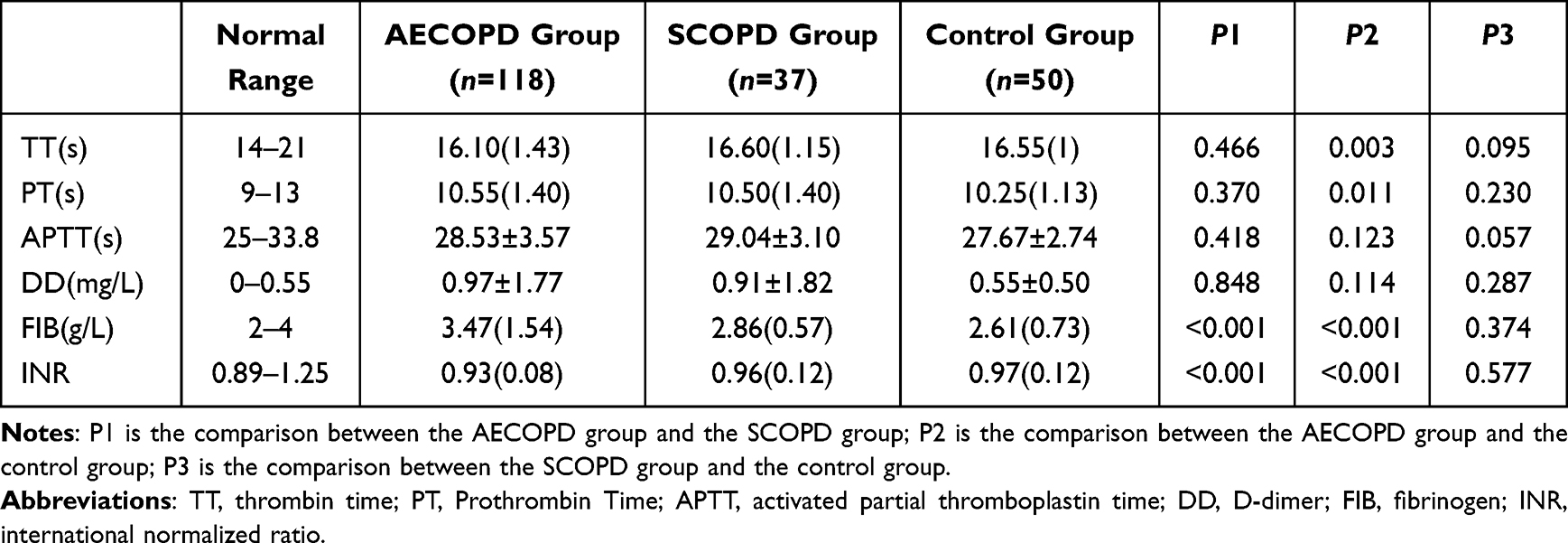 |
Table 3 Comparison of Coagulation Indexes of Three Groups of Patients |
Factors Affecting Coagulation State
The correlation analysis results for each factor and the coagulation indexes in AECOPD patients are shown in Figure 1. D-D, PT, and FIB levels were positively correlated with PCT, and INR was negatively correlated with PCT. The differences in PT (rs = 0.185, P < 0.001), FIB (rs = 0.358, P < 0.001), D-D (rs = 0.307, P < 0.001), and INR (rs = −0.277, P < 0.001) were statistically significant. D-D, PT, and FIB levels were significantly positively correlated with CRP levels, the correlation coefficients being PT (rs = 0.377), FIB (rs = 0.704), and D-D (rs = 0.361). INR was negatively correlated with CRP (rs = −0.553). In patients with abnormal blood gas analysis indicators, PT was negatively correlated with pH (rs = −0.184) and positively correlated with PaCO2 (rs = 0.199), suggesting that the abnormal coagulation state is related to hypercapnia and acidosis (Figure 1).
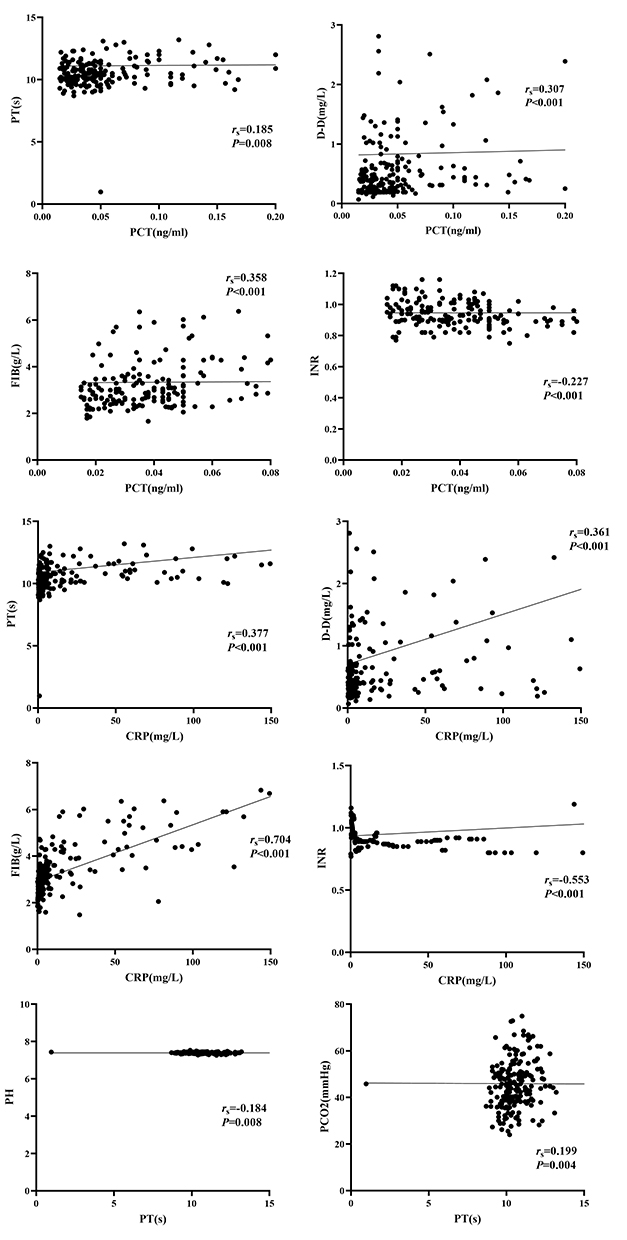 |
Figure 1 Correlation between coagulation indexes and inflammatory markers in AECOPD patients. |
Discussion
Coagulation dysfunction is common in COPD patients. PT, APTT, TT, and FIB are common indicators for clinical testing of coagulation function, which can directly reflect the levels of endogenous and exogenous coagulation factors.16,17 In this study, compared to the SCOPD group and the control group, FIB levels in the AECOPD group were significantly higher, while INR values were significantly lower. Compared to the SCOPD group, PT in the AECOPD group was significantly longer. Compared to the control group, TT in the AECOPD group decreased significantly, but the value was still within the normal range. The decrease of TT has no special clinical significance. Although there was no significant difference in D-D among the three groups, the average D-D levels in the AECOPD group were higher than the normal range; in combination with the prolongation of APTT and PT coagulation indexes, it is certainly a possibility that the coagulation time may be prolonged after the consumption of coagulation factors. These results suggest that abnormal coagulation function in AECOPD patients is a complex process.11 The present study reveals that the abnormal expression of coagulation indexes in COPD patients has a certain correlation with infection and hypercapnia, which may be involved in the formation of venous thrombosis of the lower limbs.
Respiratory infection is the most common predisposing factor for AECOPD. In the past, AECOPD was mainly considered to be related to bacterial infection, as about 30% of patients had obvious evidence of respiratory virus infection in the early stage of onset.18,19 When there is infection in the human body, the proper immune defense function is activated, and various inflammatory factors are released protectively to stimulate the vascular endothelial system and disorder the endothelial function; the coagulation pathway is also activated, leading to coagulation dysfunction.14,20,21 In this study, the N% in the AECOPD group was significantly higher than that of the SCOPD group, suggesting that AECOPD patients had bacterial infection (Table 2). PCT is the precursor of calcitonin and is mainly secreted by thyroid C cells. The level of PCT in peripheral blood of healthy people is very low, generally lower than 0.05ng/mL. When the body is infected by bacteria, fungi, parasites or affected by organ failure, PCT level is increased in the blood, which may be related to a large number of cytokines and endotoxins produced for the pathogen infection and they can inhibit PCT degradation. As an acute reaction protein, concentration of CRP is low in healthy people. When infection occurs in the body, under the stimulation of tumor necrosis factor-α (INF-α), interleukin (IL) −6 and other cytokines, its synthesis in the liver is increased, and its secretion into the blood is increased. CRP has been reported as an inflammatory cytokine to assist in the diagnosis of bacterial infections. Furthermore, we can find that, in addition to the neutrophil count and percentage, the increases of CRP and PCT were important inflammatory indexes apart from abnormal coagulation function, as the levels of CRP and PCT in the AECOPD group were significantly higher than those in SCOPD group. Closely monitoring the dynamic changes of these indicators plays an important role in understanding changes in the patients’ condition.
Coagulation dysfunction is common in AECOPD patients. In this study, compared to the SCOPD group, PT in the AECOPD group was significantly prolonged, and FIB in the AECOPD group was significantly increased (Table 3). As one of the molecular markers of hypercoagulability and hyperfibrinolysis in the body, D-D is a specific degradation product of cross-linked fibrin, which can better reflect the production of thrombin and the activity of fibrinolysin.22 Hypercoagulability is a significant feature of inflammatory lesions in COPD patients.21,23,24 In this study, the average level of D-D in the AECOPD patients was higher than that of the SCOPD group and the control group, suggesting that COPD patients have hypercoagulability and that, especially in AECOPD patients, the risk of microthrombosis is higher. Meanwhile, in this study, we found that 61 patients (51.69%) had hypercapnia with arterial carbon dioxide concentration exceeding 50mmHg, and 21 patients (17.8%) had acidosis. This study reveals that certain coagulation function indexes are positively correlated with PCT and CRP levels, as well as arterial blood carbon dioxide concentration. INR was significantly and negatively correlated with PCT and CRP. These results suggest that coagulation dysfunction is correlated with infection and hypercapnia.25 Among the subjects, five AECOPD patients and one SCOPD patient had deep venous thrombosis of the lower limbs, and it can reasonably be inferred that coagulation dysfunction is associated with infection, hypercapnia, and acid-base disturbance in COPD patients, coagulation dysfunction may be an important risk factor for thrombosis.
However, this study also has certain limitations. Firstly, the subjects had been smoking for different periods, and some AECOPD patients had received anti-infective treatment outside the hospital of different degrees and at different times prior to admission. These differences may directly affect the inflammatory indexes, the corresponding coagulation results, and blood gas analysis indexes. Secondly, after admission, patients were treated with oxygen therapy of different concentrations. Some patients were treated with non-invasive auxiliary ventilation. To some extent, all of these factors affected the partial pressure of carbon dioxide, and the partial pressure of oxygen could not be accurately assessed. Therefore, it is impossible to analyze the correlation between hypoxia and coagulation dysfunction. Thirdly, this was a retrospective study, and the sample size was small. Moreover, the number of patients in the control group, the SCOPD group, and the AECOPD group was different, which affected the accuracy of the experimental results. The patients in the control group were polyp patients in our hospital and were therefore not entirely healthy people. Large sample and multicenter studies are needed to confirm the relationship between coagulation dysfunction with infection and hypercapnia in COPD patients. There are still many other potential factors in COPD patients with venous thrombosis that clinical workers urgently need to explore.26
Conclusion
In summary, the present study confirms that COPD patients suffered from hypercoagulability and that, especially in AECOPD patients, coagulation dysfunction was particularly high. There are many factors that cause hypercoagulability in COPD patients; more common among these is that inflammation is associated with hypercapnia, which may be an important factor for thrombosis. Besides understanding the causes of abnormal coagulation function in COPD patients, alongside routine anti-infection treatment attention should also be paid to anticoagulation, which may improve the prethrombotic or microthrombotic status of patients, as it has a certain clinical value for alleviating the clinical symptoms and improving the prognosis.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of the First Affiliated Hospital of Anhui University of Traditional Chinese Medicine. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
This study was funded by the National Regional Innovation Joint Fund (U20A20398).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Group of Chronic obstructive pulmonary Disease. Respiratory Branch of Chinese medical association, working committee of chronic obstructive pulmonary disease, respiratory branch of Chinese medical association. Guidelines for diagnosis and treatment of chronic obstructive pulmonary disease (Revised 2021). Chin J Tuberc Respir Dis. 2021;44(03):170–205.
2. Hogea S-P, Tudorache E, Petronela Fildan A, et al. Risk factors of chronic obstructive pulmonary disease exacerbations. Clin Respir J. 2020;14(3):183–197. doi:10.1111/crj.13129
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health[CPH]study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
4. Pang H, Wang L, Liu J, et al. The prevalence and risk factors of venous thromboembolism in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease. Clin Respir J. 2018;12(11):2573–2580. doi:10.1111/crj.12959
5. Rahaghi FN, Pistenmaa CL. Hypercoagulation in COPD: the clot thickens. ERJ Open Res. 2021;7(4):00534–2021. doi: 10.1183/23120541.00534–2021.
6. Maschirow L, Khalaf K, Al-Aubaidy HA, et al. Inflammation, coagulation, endothelial dysfunction and oxidative stress in prediabetes-Biomarkers as a possible tool for early disease detection for rural screening. Clin Biochem. 2015;48(9):581–585. doi:10.1016/j.clinbiochem.2015.02.015
7. Liu J, Jiang N, Liu T, et al. Clinical effect of simvastatin combined with exercise training in the treatment of stationary chronic obstructive pulmonary disease complicated with metabolic syndrome. Pak J Pharm Sci. 2020;33(1(Special):437–440.
8. Liang G, Bowen JP. Development of trypsin-like serine protease inhibitors as therapeutic agents: opportunities, challenges, and their unique structure-based rationales. Curr Top Med Chem. 2016;16(13):1506–1529. doi:10.2174/1568026615666150915121447
9. Balaguer C, Peralta A, Rios A, et al. Effects of simvastatin in chronic obstructive pulmonary disease: results of a pilot, randomized, placebo-controlled clinical trial. Contemp Clin Trials Commun. 2016;2016:291–296.
10. Ji H, Xu LS, Gong WD, et al. 老年缺血性脑卒中患者康复治疗效果的影响因素 [Factors influencing rehabilitation effect in elderly patients with ischemic stroke]. Chin J Gerontol. 2020;40(11):2270–2273. Chinese.
11. Tang N, Li D, Wang X, et al. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844–847. doi:10.1111/jth.14768
12. Husebø GR, Gabazza EC, D’Alessandro Gabazza C, et al. Coagulation markers as predictors for clinical events in COPD. Respirology. 2021;26:342–351. doi:10.1111/resp.13971
13. Liang YQ. 血栓弹力图在儿童脓毒性休克凝血功能障碍中的应用 [Application of thromboelastogram in children with coagulopathy due to septic shock]. Chin J Mod Drug Appl. 2019;13(19):16–17. Chinese.
14. Lordan R, Tsoupras A, Zabetakis I. Platelet activation and prothrombotic mediators at the nexus of inflammation and atherosclerosis: potential role of antiplatelet agents. Blood Rev. 2021;45:100694. doi:10.1016/j.blre.2020.100694
15. Wu WB, Chen CZ, Yang DL, Qin JM, Feng JM. D-二聚体、B型钠尿肽与血气在慢性阻塞性肺疾病继发肺栓塞的预测价值 [Predictive value of D-dimer, B-type natriuretic peptide and blood gas in patients with pulmonary embolism secondary to chronic obstructive pulmonary disease]. Chin J Lung Disea. 2019;12(6):743–746. Chinese.
16. Liu M, Hu R, Jiang X, et al. Coagulation dysfunction in patients with AECOPD and its relation to infection and hypercapnia. J Clin Lab Anal. 2021;35:e23733. doi:10.1002/jcla.23733
17. Zhang YH, Jiang H, Liu F. 低分子肝素治疗老年慢性阻塞性肺疾病急性加重期患者的效果观察 [Effect of low molecular weight heparin on elderly patients with acute exacerbation of chronic obstructive pulmonary disease]. J Nanjing Med Univ. 2019;4(3):293–296. Chinese.
18. Zhu J, Pang J, Ji P, et al. Coagulation dysfunction is associated with severity of COVID-19: a meta-analysis. J Med Virol. 2021;93(2):962–972. doi:10.1002/jmv.26336
19. Perera PN, Armstrong EP, Sherrill DL, Skrepnek GH. Acute exacerbations of COPD in the United States: inpatient burden and predictors of costs and mortality COPD. Int J Chron Obstruct Pulmon Dis. 2012;9(2):131–141. doi:10.3109/15412555.2011.650239
20. Albayati MA, Grover SP, Saha P, et al. Postsurgical inflammation as a causative mechanism of venous thromboembolism. Semin Thromb Hemost. 2015;41:615–620. doi:10.1055/s-0035-1556726
21. Ashitani J, Mukae H, Arimura Y, et al. Elevated plasma procoagulant and fibrinolytic markers in patients with chronic obstructive pulmonary disease. Intern Med. 2002;41:181–185. doi:10.2169/internalmedicine.41.181
22. Shi MX, Zhang W, Liu L, et al. D-二聚体测定在慢性阻塞性肺疾病的疗效评价及预后意义的研究进展 [Research progress on the efficacy evaluation and prognostic significance of D-dimer determination in chronic obstructive pulmonary disease]. XianDai Sheng Wu Yi Xue Jin Zhan. 2017;17(29):5797–5800. Chinese.
23. Alessandri C, Basili S, Violi F, et al. Hypercoagulability state in patients with chronic obstructive pulmonary disease. chronic obstructive bronchitis and hemostasis group, Thromb. Hemost. 1994;72:343–346.
24. Aibar AMA, Laborda EK, Conget LF, et al. Hypercoagulability state and endothelial injury in stable chronic obstructive pulmonary disease patients. Anales del Sistema Sanitario De Navarra. 2010;33(1):43–50.
25. Lu XF. 老年慢性阻塞性肺疾病急性加重期合并呼吸衰竭患者凝血功能指标的变化 [Changes of coagulation function in elderly patients with acute exacerbation of chronic obstructive pulmonary disease complicated with respiratory failure]. Shi Yong Lin Chuang Yao Xue Za Zhi. 2016;20(03):169–170. Chinese.
26. Aleva F, Voets L, Simons S, et al. Prevalence and localization of pulmonary embolism in unexplained acute exacerbations of COPD: A systematic review and meta-analysis. Chest. 2017;151(3):544–554. doi:10.1016/j.chest.2016.07.034
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.