Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Correlation Between the Frailty of Elderly Patients on Regular Haemodialysis and the Quality of Life of Their Family Caregivers: A Cross-Sectional Evaluation
Authors Zhu Z, Li P, Chai D, Luan W
Received 2 August 2022
Accepted for publication 14 September 2022
Published 12 October 2022 Volume 2022:15 Pages 2321—2330
DOI https://doi.org/10.2147/JMDH.S384699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Zhu Zhu,1 Ping Li,2 Dongxue Chai,2 Wei Luan3
1Department of VIP Clinic, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, 200127, People’s Republic of China; 2Department of Hemodialysis Center, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, 200127, People’s Republic of China; 3Department of VIP Medical Office, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, 200127, People’s Republic of China
Correspondence: Wei Luan, Renji Hospital, Shanghai Jiao Tong University School of Medicine, No. 160 of Pujian Road, Pudong District, Shanghai, 200127, People’s Republic of China, Tel/Fax +86 21 6838 3088, Email [email protected]
Objective: To investigate the correlation between the frailty status of elderly patients on regular haemodialysis and the quality of life of their family caregivers.
Methods: 90 elderly patients with regular haemodialysis and 90 family caregivers of the respective patients were selected from January 2020 to April 2021. The influencing factors of the caregivers’ quality of life and correlation between patient debility and caregiver quality of life were analyzed by general information questionnaire, Tilburg debility index scale, self-care ability scale, family caregiver-related quality-of-life scale and social support scale.
Results: The quality of life of the family caregivers of elderly patients on regular haemodialysis is at the medium level (4.50 ± 2.96). Multiple linear stepwise regression analysis shows that the ability of patients to take care of themselves, the degree of patients’ weaknesses, whether they care for non-dialysis patients, the time to care for patients, social support and the type of current residence have significant impacts on the quality of life of the caregivers (p < 0.001). Variance analysis showed that the fitting degree of linear regression equation is relatively high, and the regression equation is significant (F = 9.195, p < 0.001, R = 0.595, R2 = 0.315). The quality of life of caregivers is positively correlated with the ability of the patients to take care of themselves, the length of care, social support and type of current residence (p < 0.05). The degree of weakness in patients is negatively correlated with taking care of non-regular dialysis patients (p < 0.05).
Conclusion: The ability of patients to take care of themselves, the degree of weakness of the patients, social support and the type of current residence are the influencing factors of the burden on the family caregivers of maintenance haemodialysis patients.
Keywords: maintenance haemodialysis, elderly patients, caregiver, quality of life
Introduction
Chronic kidney disease (CKD) is a common public health problem worldwide, with 8% to 16% of adults suffering from CKD.1,2 End-stage renal disease (ESRD) is the outcome of most primary and secondary kidney diseases.2–4 To prolong the lifespan and improve the patients’ quality of life, experts recommend renal replacement therapy, which is dominated by maintenance haemodialysis (MHD).5,6 Although MHD can extend patients’ life to a certain extent, ESRD has an irreversible disease progression and long-term treatment. Long-term haemodialysis will cause many complications, and its high cost will impose a huge economic burden on patients and their families and severely reduce the patients’ quality of life.
For haemodialysis patients, curing the disease is no longer the goal of treatment. Therefore, as it is particularly important to improve the quality of life of haemodialysis patients, long-term care and nursing are needed for patients with MHD. Since China is at an early stage of social and economic development, there is no established and solid social medical security system that corresponds to China’s current national conditions, and there are still some limitations in the community medical system. Chinese society is gradually becoming an aging society, and the proportion of elderly patients in haemodialysis cases is approximately 60%.5 Moreover, family members need to bear the main responsibility for care and nursing. In addition to haemodialysis every week, patients are nursed by their family members at home, which is a relatively economical and viable option. However, long-term burdensome daily care has a tremendous impact on the caregivers’ mind and body, which will cause psychosocial issues, such as depression, anxiety, fear and maladaptation. This will reduce the quality of life of caregivers, thereby affecting the quality of their care for the patients.7,8 Therefore, paying attention to caregivers’ quality of life and helping them to maintain healthy physiological and psychological states and good social adaptability can promote the recovery of patients, improve the quality of life of family caregivers and reduce the need for medical treatment.9 However, there are limited studies on the quality of life of family caregivers of elderly MHD patients.
The aim of this study is to investigate the correlation and influencing factors between the physical frailty of elderly MHD patients and their family caregivers’ quality of life and provide a reference basis for improving the family caregivers’ quality of life.
Objects and Methods
Research Objects
This study is a cross-sectional study that adopts the convenient sampling method. Ninety pairs of MHD patients who met the inclusion criteria and their main caregivers (180 persons in total) were selected as the study objects among the patients who were treated in the blood purification centre of our hospital and their main caregivers from January 2020 to April 2021.
The inclusion criteria for patients are as follows: ① ESRD patients treated with haemodialysis two to three times per week; ② Patients who have been treated with haemodialysis for at least 3 months; ③ Patients aged 60 and above who can verbally express themselves; and ④ Informed consent and voluntary participation. The inclusion criteria for caregivers are as follows: ① A family caregiver (spouse, child, parent, etc.) appointed by the patient who undertakes the primary day-to-day care; ② Aged 18 and above with clear verbal expression and normal communication skills; ③ Having taken care of the patient for at least 3 months; and ④ Informed consent and voluntary participation.
The exclusion criteria for patients are as follows: ① Patients with a malignant tumour disease or an expected life cycle of less than half a year; ② No independent behavioural ability; and ③ Communication difficulties. The exclusion criteria for caregivers are as follows: ① Employed caregivers; and ② No independent language expression ability. This study is approved by the Ethics Committee of the hospital. All patients and their families were informed about this study and provided informed consent.
Methods
Research Tools
The Mandarin Chinese language versions of the instruments were developed using independent forward–backward translations. The translations were checked for accuracy by native-speaker researchers.
General Information
The questionnaires focus on general information, including age, gender, family situation, how long they have been treated with haemodialysis, how medical expenses are paid and monthly expenses. General information about the caregivers includes their age, gender, marital status, religious belief, relationship with the patient, time spent caring and family income.
Tilburg Frailty Indicator (TFI)
This scale is a standard self-report questionnaire that was developed by Gobbens10 and his team in the Netherlands. The scale consists of the following two parts: Part A concerns the determinants of frailty syndrome, whereas Part B includes 15 questions about the presence of the major components of frailty, including 8 items on physical frailty, 4 items on psychological frailty and 3 items on social frailty.11 The total score ranges from 0 to 15, and frailty syndrome is recognised as being 5 points and above. The higher the score, the higher the degree of frailty of the study objects. The Cronbach’s α coefficient of the scale is 0.73.11
Activity of Daily Living
The Barthel Index rating scale was compiled by Mahoney and Barthel in the mid-1950s, with a Cronbach’s α coefficient of 0.916.12 The scale consists of the following 10 items: grooming, bathing, feeding, toilet use, dressing, bowels, bladder, stairs, transfer and mobility, and each item corresponds to three options (full dependency, need for help and full independency), with a total score of 100 points. The scoring standard is as follows: 100 points, where the subject can take care of themselves without help; 60 points and above, where the subject is mildly dysfunctional and able to complete some daily activities independently with some help; 41 to 59 points, where the subject is moderately dysfunctional and requires a lot of help in daily living activities; and 40 points and lower, where the subject is severely dysfunctional and unable to complete most daily activities without help. The lower the total score, the greater the dependence of patients.
Carer Quality of Life (CarerQoL) Scale
The adopted CarerQoL scale has been translated into Mandarin Chinese by Zhang et al with a validity of 0.821.13 The scale includes CarerQol-7D to assess the burden of caregivers and CarerQol-VAS to assess the general quality of life of caregivers. There are the following seven dimensions to the CarerQol-7D: relational problems, mental health, problems combining daily activities with caring, financial problems, physical health, fulfilment and support. The first five are problem dimensions, whereas the last two are positive dimensions, and each comes with three options of “no” (2 points), “some” (1 point) and “a lot” (0 points). The higher the score, the better the quality of life. CarerQol-VAS assesses the current degree of happiness of caregivers through a visual analogue scale that has 11 graduations, with “0” indicating not at all happy and “10” indicating very happy. The Cronbach’s α coefficient of this scale is 0.861.14
Social Support Re-Evaluated Scale
This scale was created by Xu, with a Cronbach’s α coefficient of 0.825–0.896.15 The scale comprises the following 10 items in three dimensions: objective support (3 items), subjective support (4 items) and degree of utilisation of social support (3 items), with a total score of 12 to 64 points. A total score of 22 points and lower indicates a low level of social support, a total score of 23 to 44 points indicates a moderate level of social support and a total score of more than 45 points indicates a high level of social support. The higher the score, the higher the level of social support.16
Questionnaire Distribution and Collection
Trained investigators investigated patients and caregivers who met the inclusion criteria. The questionnaires were filled out anonymously and collected on-site. In this study, 180 questionnaires were distributed, and all were collected, with an effective collection rate of 100%.
Statistical Method
In this study, SPSS 22.0 software was used to sort and analyse the data. Descriptive statistics were used to analyse the general data of patients continuously treated with haemodialysis and their caregivers, and the measurement data were described by “mean ± standard deviation”. The t-test and analysis of variance were adopted to analyse the differences in the quality-of-life score of family caregivers. The Pearson correlation analysis was used to study the correlation between patients’ frailty and their family caregivers’ quality of life, and the multiple linear stepwise regression analysis was adopted to analyse the factors influencing caregivers’ quality of life. With a bilateral significance level of α = 0.05, the difference was statistically significant when p < 0.05.
Results
General Information
Information about the patients: A total of 90 patients were selected in this study, including 52 males (57.8%) and 38 females (42.2%), which is consistent with existing study results.17,18 Their ages ranged from 60 to 89 years old (98.9%), and only one patient was over 90 years old (1.1%). More than half of the patients had an abnormal body mass index (BMI) (46, 51.1%) and serum albumin (52, 57.8%), and 32 patients had abnormal hemoglobin values (35.5%), which indicates that nearly half of the patients had anaemia and debilitating symptoms. All patients were continuously treated with haemodialysis for more than 3 months, and the longest time was more than 61 months, which indicates that patients with renal failure require long-term haemodialysis due to the long course of the disease. Moreover, 66 patients (73.3%) had been treated for more than 25 months. The income of most patients was less than RMB 400 per month (63.3%), which indicates that most elderly patients have a low financial status. Patients that pay using critical illness medical insurance account for 86.7% of the total number, self-payers for 1.1%, and patients that use other payment methods account for 12.2%, which suggests that medical insurance has a wide coverage. The proportion of patients with primary diseases that are dominated by hypertension is 53.3%. Table 1 shows the results.
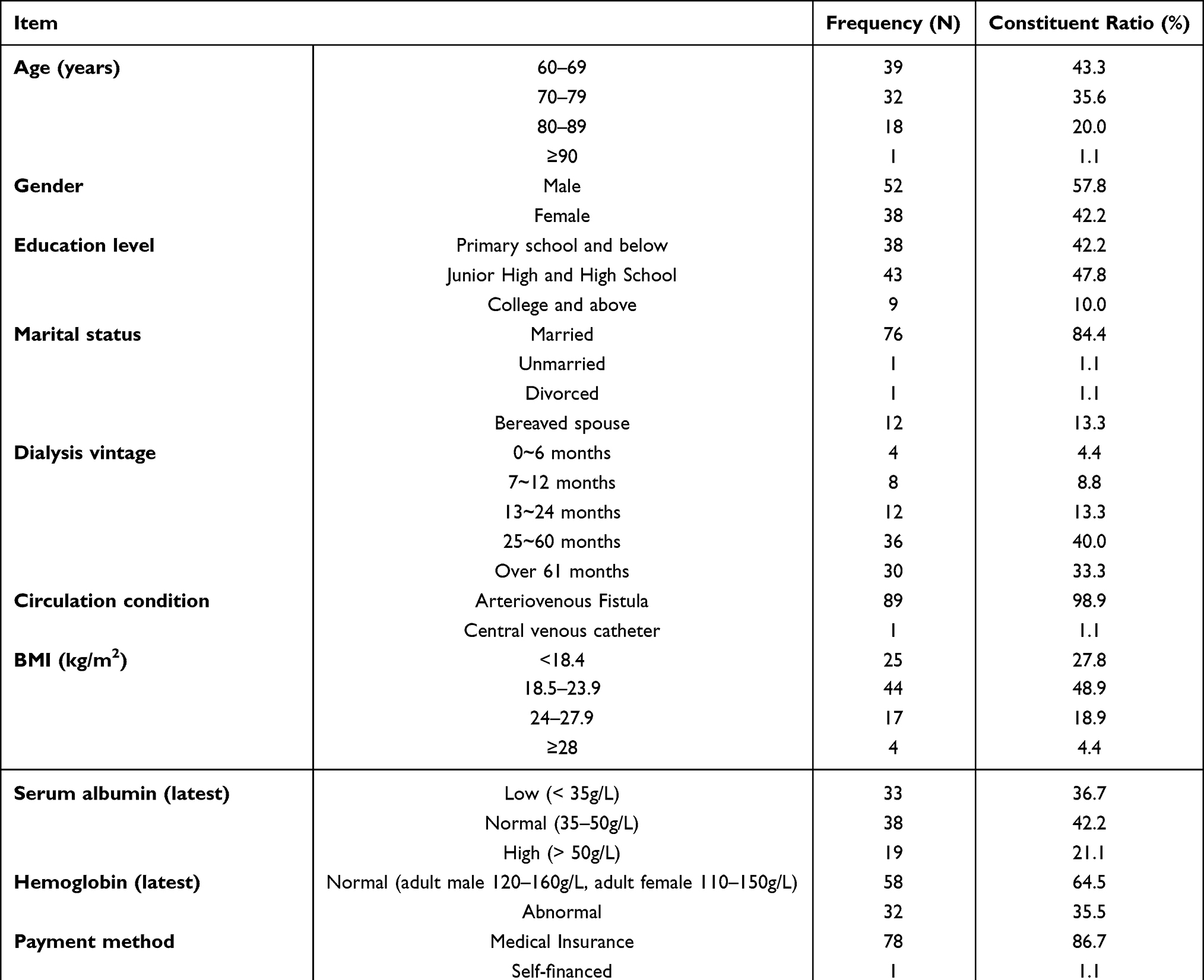 |
Table 1 General Information of Older Patients |
Information about the caregivers: A total of 90 caregivers were selected in this study, including 45 males (50%) and 45 females (50%), and their age was mainly 61 years and above (65.5%). This shows that the elderly is mostly taken care of by other elderly. Most of the caregivers are patients’ spouses, children or children’s spouses (94.4%), and 74.4% of caregivers live with their patients. So far, 67.8% of caregivers have cared for their patient for more than 25 months, and 76.7% of them are retirees. Moreover, 61.1% of them have a monthly income of less than RMB 4000, which indicates that most caregivers have a low financial income and heavy financial burden, which is consistent with Saban’s study results.19 Table 2 shows the results.
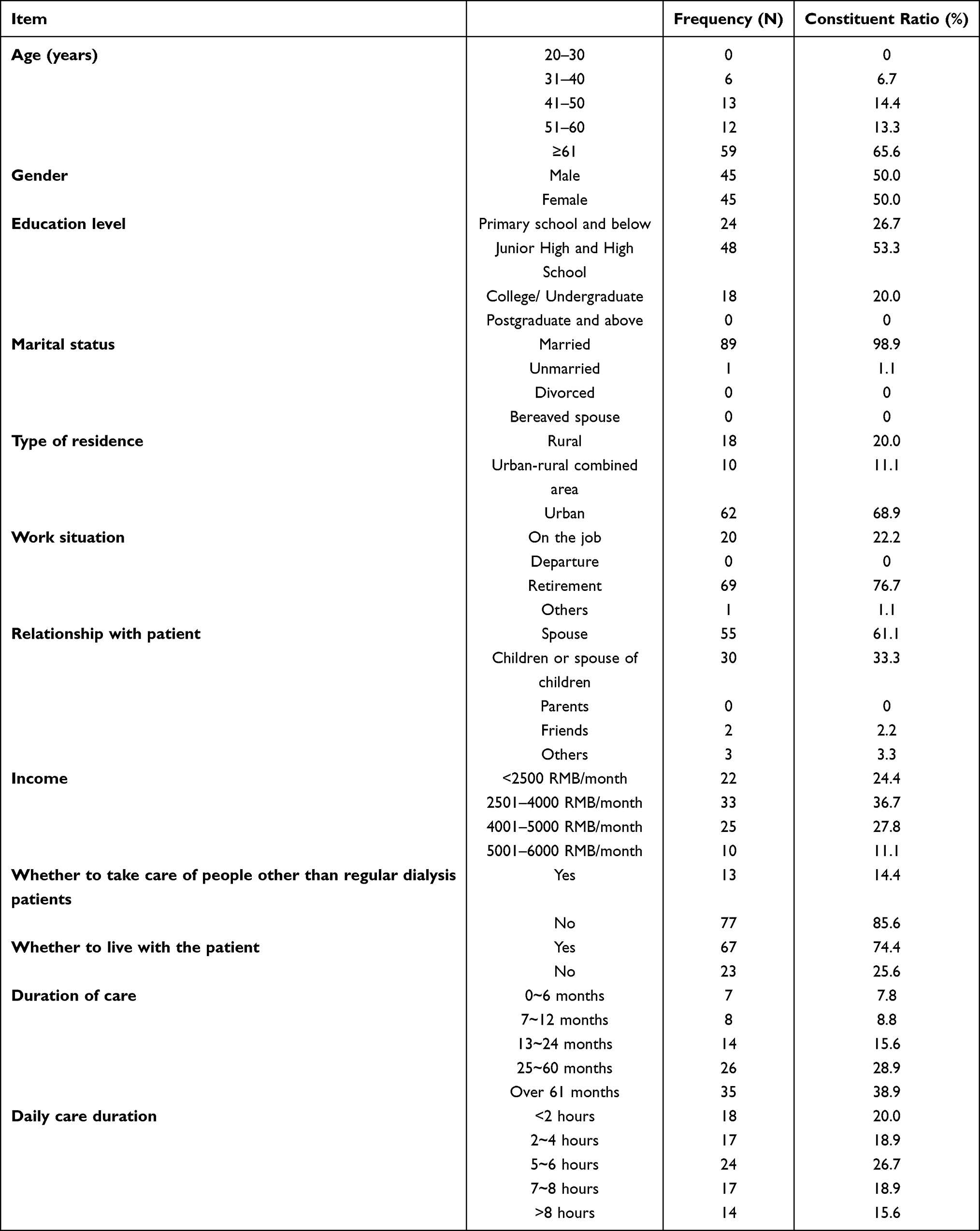 |
Table 2 General Information of Patients’ Caregivers |
Self-Care Ability and Frailty of Elderly Patients
In this study, as shown in Table 3, the patients’ self-care ability score was 45.94 ± 20.92 points, which is at the moderately dysfunctional level and indicates that the patients need considerable help to complete daily activities. The TFI score was 7.27 ± 3.16 points, which indicates that overall, the level of frailty is moderate.
 |
Table 3 The Ability of Older Patients to Take Care of Themselves and Their Degree of Frailty |
Quality of Life and Social Support of Caregivers
As shown in Table 4, the quality-of-life score of the family caregivers was 4.50 ± 2.96 points, which is at the moderate level. The QoL-VAS score was 6.41 ± 1.68 points, which is at the above-average level. The social support score was 32.52 ± 6.65 points, which is at the moderate level.
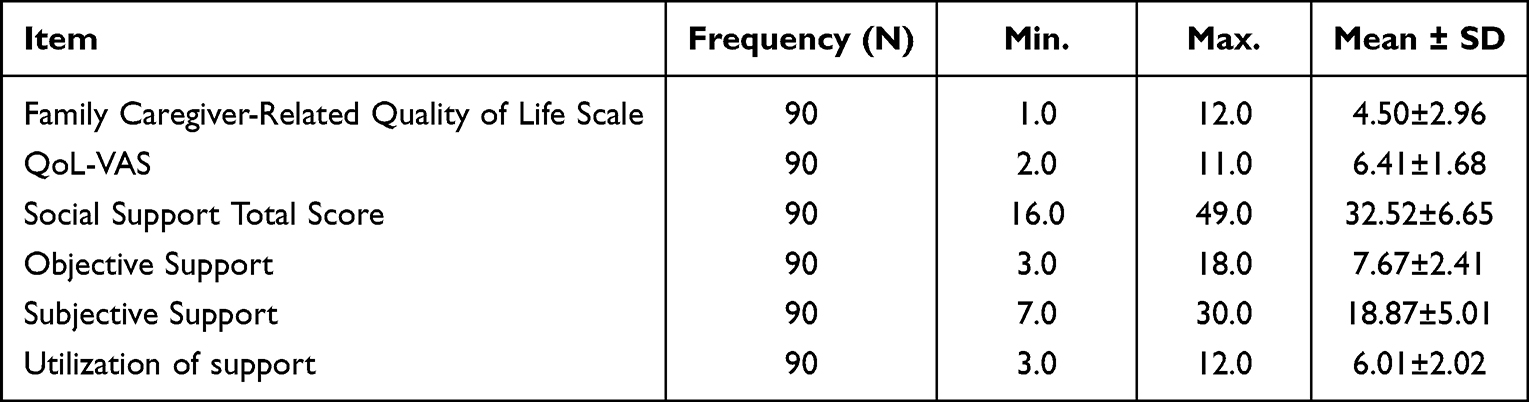 |
Table 4 Caregiver Quality of Life and Social Support |
Correlation Between Patients’ Physical Frailty and the Quality of Life of Their Family Caregivers
According to the analysis results in Table 5, there is a weak positive correlation between the physical frailty of patients and the quality of life of their family caregivers (r = 0.247, p < 0.019).
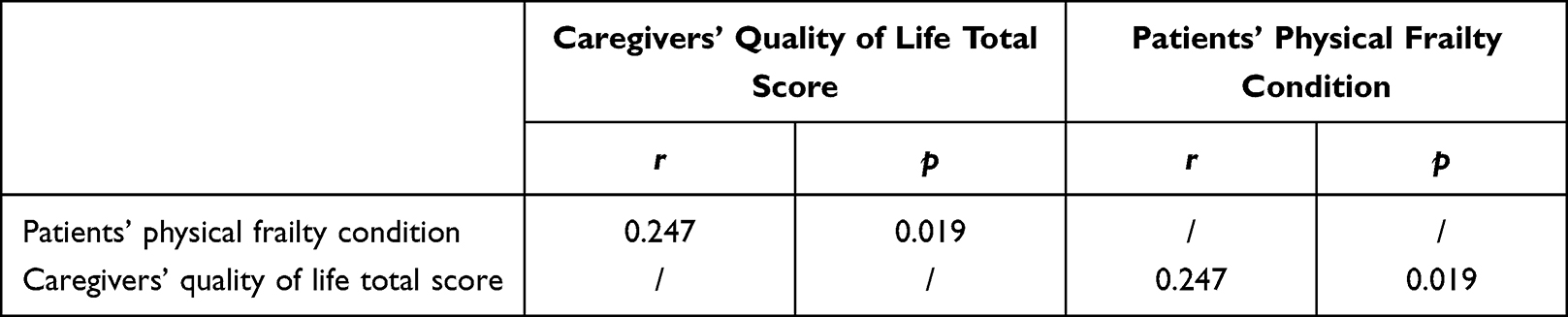 |
Table 5 Correlation Between Patients’ Physical Frailty and Their Family Caregivers’ Quality of Life |
Multiple Linear Regression Analysis of Factors Influencing the Quality of Life of Patients’ Family Caregivers
A multiple linear regression analysis was carried out using the quality of life of the primary caregivers of MHD patients as the dependent variable and the relevant factors with statistical significance in a single-factor analysis as the independent variables. The study results show that the patients’ self-care ability and degree of frailty and the caregivers’ time spent caring and social support have a significant influence. The stepwise regression equation is as follows: Y = 3.375+0.106X1-0.138X2-2.037X3+1.757X4+1.120X5+1.079X6. The quality of life of the family caregivers is positively correlated with the self-care ability of patients, the time spent caring for the patients, social support received and the type of current place of residence and is negatively correlated with the degree of frailty of patients and whether the family caregivers provide for other people in addition to the patients with regular haemodialysis treatment.
The result of the analysis of variance in Table 6 shows that the linear regression equation has a high degree of fit, and the regression equation is statistically significant (F = 9.195, p < 0.001), which indicates that the dependent variable of the regression equation is relatively highly explanatory of the independent variable. This explains 31.5% of the variation (R = 0.595, R2 = 0.354, R2 = 0.315 after adjustment) in the caring behaviour of caregivers.
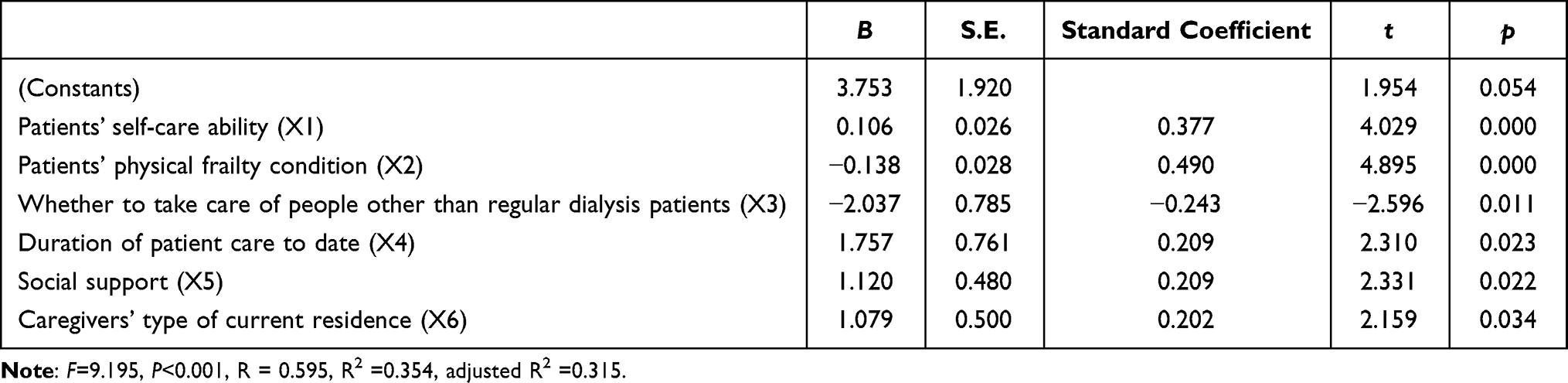 |
Table 6 A Multifactorial Analysis of Factors Affecting Caregivers’ Quality of Life |
Discussion
ESRD is an important disease that is gradually becoming more prevalent worldwide. It has a considerable impact on patients’ functional status and QOL. The accumulation of uremic toxins can cause uremic symptoms, such as dry skin and sleeping difficulties, thus affecting the daily life of patients.20 HD, the most common treatment option for ESRD, clears large amounts of uremic toxins and promises to improve the patient’s quality of life. However, haemodialysis itself causes significant changes in patients’ lifestyles and may reduce their quality of life. This may be due to haemodialysis-related complications, such as muscle cramps, pruritus, anorexia and access issues.21
General Information of Patients and Family Caregivers
This study found that elderly patients are mostly taken care of by other elderly. Most of the caregivers are patients’ spouses and children, which is consistent with the study results by Zhang Xu and Zhang et al22,23 In addition, most of the caregivers in this study did not receive higher education. Due to their limited level of education, the caregivers themselves did not have the necessary knowledge and skills to care for patients being treated with haemodialysis. Therefore, they need proper guidance, which could reduce their burden to a certain extent.19,24,25
Current Situation and Related Factors Influencing the Quality of Life of Family Caregivers
The results of this study showed that the CarerQol-7D score for the family caregivers was 4.50 ± 2.96 points, the QoL-VAS score was 6.41 ± 1.68 points and SSRS was 32.52 ± 6.65 points, which are all at a moderate level. There is a weak positive correlation between the physical frailty of elderly haemodialysis patients and the quality of life of their family caregivers. The higher the degree of physical frailty of the patients, the poorer the quality of life of the caregivers. According to the study results, the self-care ability of patients, the degree of frailty of patients, whether the family caregivers provide for other people in addition to the patients with regular haemodialysis treatment, the time spent caring for the patients, social support received, the current place of residence and the quality of life of the caregivers can be used to predict the quality of life of the family caregivers. The poorer the self-care ability of patients, the higher the degree of frailty patients. If, in addition to the patients with regular haemodialysis treatment, the caregivers also need to take care of other people, the burden on caregivers will increase, and their quality of life will be affected.26 Moreover, the social support that the family caregivers receive also has a large impact on their quality of life. When a stressful event occurs, social support may provide a certain buffering effect for the organism, thereby maintaining the health of the organism. The more social support the caregivers receive, the more social support they will subjectively feel. Social support improves the health and well-being of family caregivers by meeting their needs for intimacy, belonging and security, thereby reducing their level of burden.27
Improving the Quality of Life of Family Caregivers is Conducive to Improving the Quality of Care for Elderly MHD Patients
The quality of life reflects the individual’s state of health. The study shows that caring for patients reduces the caregivers’ quality of life. According to the results of this study, the quality of life of family caregivers of elderly patients with regular haemodialysis treatment is average and influenced by many factors. Domestic studies investigated the primary caregivers of haemodialysis patients and found that they face a heavy burden of care and high psychological pressure. These conclusions suggest that caregivers’ moods and behaviour can have an important impact on the progress and prognosis of haemodialysis patients. Therefore, we should pay more attention to caregivers,28,29 and medical institutions and government departments should provide them with substantial support.
The following methods can be adopted to improve the quality of life of caregivers: ① Increasing the social support to caregivers, relieving their pressure to care, improving their ability to care and other means can improve the quality of life of caregivers, thereby improving their quality of care for patients; ② The state and society can improve the medical insurance system, promote the integration of medical care and home-based care and appropriately reduce caregivers’ pressure and time spent on caring for the patients;30 and ③ Caregivers can be provided with emotional support, such as guidance by volunteers trained in psychology, to alleviate their depression and anxiety and relieve the pressure. In addition, professional care service centres can be established to organise social activities for caregivers to help them to communicate with each other better.31
The limitations of this study are as follows: ① It has a small sample size, and there are certain limitations to the possible conditions studied; ② It is primarily a cross-sectional study. Therefore, the causal relationship between the variables needs to be further investigated and confirmed, and the research data need to be continuously enriched to obtain more objective research results. In future work, these shortcomings should be improved.
Conclusion
Influenced by the medical environment and culture in China, most haemodialysis patients rely on their family members for care. The higher the degree of physical frailty of patients, the poorer the quality of life of the caregivers. Long-term haemodialysis treatment has a great impact on the patients’ physical and mental health, and their primary caregivers bear great pressure and burden. Therefore, there is a need to increase social support for caregivers, alleviate their pressure to care and improve their ability to care, which will improve caregivers’ quality of life, thereby finally achieving the goal of improving the quality of care for patients.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Renji Hospital, Shanghai Jiaotong University School of Medicine (RA-2020-298). Written informed consent was obtained from all participants in this study.
Funding
Shanghai Hospital Association Hospital Management Research Fund Project (X2020083); Special topic no. of clinical research in health industry of Shanghai Health Commission (202150032); Project number of liberal arts youth talent cultivation plan of Shanghai Jiaotong University (2022QN030).
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Webster AC, Nagler EV, Morton RL, et al. Chronic kidney disease. Lancet. 2017;389(10075):1238–1252. doi:10.1016/S0140-6736(16)32064-5
2. Yao X. Epidemiological Investigation of Patients with End-Stage Renal Disease in Zhejiang Province and Construction of Death Risk Prediction Model. Zhejiang: Zhejiang University; 2015.
3. He XF, Xu P, Lu AL. Study on the impact of social support on the quality of life and hope level of long-term hemodialysis patients. Chin J Geriatr Care. 2018;16(1):139–141. doi:10.3969/j.issn.1672-2671.2018.01.063
4. Hao YH, Jiang YF. Symptom experiences among maintenance hemodialysis patients: a cross-sectional study. Chin J Nurs. 2016;51(3):299–303. doi:10.3761/j.issn.0254-1769.2016.03.008
5. Zhou M. Analysis of psychological problems and nursing countermeasures of elderly hemodialysis patients. Chin Foreign Medl Res. 2011;22:99–100.
6. Qin HY, Jia P, Liu H. Nursing strategies for patients with chronic renal failure undergoing maintenance hemodialysis treatment by arteriovenous fistula. Iran J Public Health. 2016;45(10):1270–1275.
7. Li TT, Fan R, Lv GL. Analysis on the current situation and influencing factors of the burden of family caregivers of maintenance hemodialysis patients. Chin J Blood Purif. 2017;16(3):179–182. doi:10.3969/j.issn.1671-4091.2017.03.009
8. Frambes D, Given B, Lehto R, et al. Informal caregivers of cancer patients: review of interventions, care activities, and outcomes. West J Nurs Res. 2018;40(7):1069–1097. doi:10.1177/0193945917699364
9. Wu H, Wen XX, Li Y, et al. Analysis of the current situation and influencing factors of disease uncertainty in the main caregivers of elderly maintenance hemodialysis patients. J Qilu Nurs. 2020;26(01):5–9. doi:10.3969/j.issn.1006-7256.2020.01.002
10. Gobbens RJJ, Van assen MLA, Luijkx KG, et al. The Tilburg frailty indicator psychometric properties. J Am Med Dir Assoc. 2010;11(5):344–355. doi:10.1016/j.jamda.2009.11.003
11. Mlynarska A, Mlynarski R, Uchmanowicz I, Marcisz C, Golba KS. The relationship between frailty syndrome and concerns about an implantable cardioverter defibrillator. J Am Med Dir Assoc. 2021;22(3):551–558.e1. doi:10.1016/j.jamda.2020.08.012
12. Xue DX, Li J. Application of rehabilitation nursing based on Barthel index rating scale of general practice concept in hemiplegia patients aged >60 years after cerebral infarction. Clin Res. 2022;30(01):164–167.
13. Zhang YH. Study on the Quality of Life and Care Experience of Family Caregivers with Diabetes Foot. Tianjin Medical University; 2016.
14. Clarijs ME, Oemrawsingh A, Bröker MEE, Verhoef C, Lingsma H, Koppert LB. Quality of life of caregivers of breast cancer patients: a cross-sectional evaluation. Health Qual Life Outcomes. 2022;20(1):29. doi:10.1186/s12955-022-01930-0
15. Xu XF, Tian CQ, Yu Q, Huang HL, Tao MF. Self-management behavior, hope and social support in patients undergoing maintenance Hemodialysis. J Wannan Medl Coll. 2022;41(4).1
16. Voormolen DC, van Exel J, Brouwer W, et al. Actifcare Consortium. A validation study of the CarerQol instrument in informal caregivers of people with dementia from eight European countries. Qual Life Res. 2021;30(2):577–588. doi:10.1007/s11136-020-02657-5
17. Lowney AC, Myles HT, Bristowe K, et al. Understanding what influences the health-related quality of life of hemodialysis patients: a collaborative study in England and Ireland. J Pain Symptom Manage. 2015;50(6):778–785. doi:10.1016/j.jpainsymman.2015.07.010
18. Zhang XQ. Investigation of Symptom Burden and Analysis of Influencing Factors in Maintenance Hemodialysis Patients. Zhejiang University of traditional Chinese medicine; 2016.
19. Saban KL, Griffin JM, Urban A, et al. Perceived health, caregiver burden, and quality of life in women partners providing care to Veterans with traumatic brain injury. J Rehabil Res Dev. 2016;53(6):681–692. doi:10.1682/JRRD.2015.07.0143
20. Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease–a systematic review and meta-analysis. PLoS One. 2016;11(7):e0158765. doi:10.1371/journal.pone.0158765
21. Hasan LM, Shaheen DAH, El Kannishy GAH, Sayed-Ahmed NAH, Abd El Wahab AM. Is health-related quality of life associated with adequacy of hemodialysis in chronic kidney disease patients? BMC Nephrol. 2021;22(1):334. doi:10.1186/s12882-021-02539-z
22. Zhang X, Ren WH, Pan YH. Study on the impact of family empowerment program on the main caregivers of first-episode stroke patients. Chin J Nurs. 2018;53(2):133–138. doi:10.3761/j.issn.0254-1769.2018.02.001
23. Zhang JF, Li ZJ, Wang FY, et al. Study on the impact of family visit on the care burden and positive experience of caregivers of stroke patients. Chin J Nurs. 2017;52(7):830–834. doi:10.3761/j.issn.0254-1769.2017.07.013
24. Wang M, Xu H, Zhou HY. Relationship between sleep quality, care burden and psychological elasticity of caregivers of stroke patients with hemiplegia. J Nurs Sci. 2017;32(9):56–59. doi:10.3870/j.issn.1001-4152.2017.09.056
25. Feng YT. Analysis of Influencing Factors and Potential Categories of Mental Health Status of Caregivers of Lymphoma Patients. Zhengzhou University; 2016.
26. Baji P, Brouwer WBF, van Exel J, et al. Validation of the Hungarian version of the CarerQol instrument in informal caregivers: results from a cross-sectional survey among the general population in Hungary. Qual Life Res. 2021;30(2):629–641. doi:10.1007/s11136-020-02662-8
27. Liu X. Study on the Relationship Between Family Caregiver Burden, Coping Style and Social Support of Elderly Hemodialysis Patients. Jilin University; 2017.
28. Luo SX, Jiang QL, Zhang Y, et al. Study on the correlation between care behavior and care load of main caregivers of hemodialysis patients. Chin Nurs Res. 2012;26(20):1848–1850. doi:10.3969/j.issn.1009-6493.2012.20.012
29. Ji J, Zhao WH, Wei T, et al. A qualitative study on the feelings of direct caregivers of elderly hemodialysis patients. J Nurs Train. 2014;29(23):2146–2148.
30. Ying JP, Zhou JY, Cai GL, et al. Analysis of quality of life and its influencing factors in elderly hemodialysis patients. Nurs Rehabilitation J. 2020;19(04):20–24. doi:10.3969/j.issn.1671-9875.2020.04.005
31. Gao DQ, Dan Y, Zhang L, et al. Research progress of caregivers’ feelings and intervention of hemodialysis patients. Nurs Pract Res. 2016;13(22):22–24. doi:10.3969/j.issn.1672-9676.2016.22.008
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Does Intradialytic Group Exercise Programme Influence Patient-Reported Outcomes, Laboratory Parameters, and Anthropometric Parameters in Maintenance Hemodialysis Patients? A Single-Group Repeated-Measures Trial
Zhou L, Shi D, Zhang L, Wang Q, Chen L, Chen H
Patient Preference and Adherence 2023, 17:491-501
Published Date: 21 February 2023
The Influencing Factors of Frailty and Quality of Life in Elderly Patients After Spinal Surgery
Gong Z, Su F, Kang X, Zhong Y, Xie Y
Clinical Interventions in Aging 2024, 19:769-778
Published Date: 9 May 2024
A Systematic Review of Quality of Life in Patients with Short Bowel Syndrome and Their Caregivers
Chen Y, Yan M, Chen H, Sheng Y, Wang Z, Wu B
Patient Preference and Adherence 2024, 18:1217-1230
Published Date: 13 June 2024
Caregiver Burden in Bladder Cancer Patients with Urinary Diversion Post-Radical Cystectomy and the Need for Comprehensive Nursing Education: A Narrative Literature
Zhang T, Qi X
Journal of Multidisciplinary Healthcare 2024, 17:3825-3834
Published Date: 7 August 2024