Back to Journals » Journal of Inflammation Research » Volume 19
Correlation Between Subepithelial Fibrosis and Vitamin D Deficiency in Chronic Rhinosinusitis with Nasal Polyps: Insights from Histological and Transcriptomic Analyses
Authors Chi M, Wang K, Bi M, Yang Z, Xing Y ![]() , Fan Y
, Fan Y
Received 9 October 2025
Accepted for publication 24 January 2026
Published 5 February 2026 Volume 2026:19 570759
DOI https://doi.org/10.2147/JIR.S570759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tara Strutt
Mengshi Chi,1,* Kanghua Wang,1,* Mingmin Bi,1 Zheng Yang,2 Yuhan Xing,3 Yunping Fan1
1Department of Otorhinolaryngology, The Seventh Affiliated Hospital of Sun Yat-Sen University, Shenzhen, 518107, People’s Republic of China; 2Department of Pathology, The Seventh Affiliated Hospital of Sun Yat-Sen University, Shenzhen, 518107, People’s Republic of China; 3School of Public Health (Shenzhen), Sun Yat-sen University, Shenzhen, 518107, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunping Fan, Department of Otorhinolaryngology, The Seventh Affiliated Hospital of Sun Yat-Sen University, No. 628, Zhenyuan Road, Guangming (New) District, Shenzhen, Guangdong, 518107, People’s Republic of China, Tel +0755-81206892, Email [email protected]; [email protected] Yuhan Xing, School of Public Health (Shenzhen), Sun Yat- Sen University, No. 66 Gongchang Road, Guangming District, Shenzhen, 518107, People’s Republic of China, Email [email protected]
Purpose: To investigate the correlation between serum vitamin D status and clinical, histological, and gene expression profiles in patients with chronic rhinosinusitis with nasal polyps (CRSwNP).
Patients and Methods: This observational study enrolled patients with CRSwNP from November 2019 to September 2021, and diagnoses were confirmed according to the 2020 European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS 2020). Clinical features, histopathological characteristics, and gene expression profiles were analyzed across groups with serum vitamin D deficiency status. Histopathological evaluations and mRNA sequencing were performed on a subset of nasal polyp specimens.
Results: Among 101 patients with CRSwNP, a comprehensive analysis revealed no significant correlation between vitamin D deficiency and most clinical parameters or treatment prognosis, except for a notable age difference among groups with serum vitamin D-deficiency, insufficiency, and sufficiency. Histologically, a higher prevalence of subepithelial fibrosis was observed in the vitamin D-deficient group. Moreover, transcriptomic analysis demonstrated significant differences in expression profiles among the groups, with upregulated genes in the deficient group enriched in extracellular matrix components and downregulated genes related to axoneme assembly and cilium movement.
Conclusion: Our findings suggest a connection between vitamin D deficiency and subepithelial fibrosis in nasal polyps, pointing to a possible involvement of vitamin D status in fibrosis-related pathological processes in CRSwNP.
Keywords: chronic rhinosinusitis, nasal polyps, vitamin D deficiency, tissue fibrosis, transcriptomic profiles
Introduction
Chronic rhinosinusitis (CRS) represents an inflammatory disorder affecting 8–14% of the global population.1,2 CRS is commonly classified into two phenotypes: CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP) based on polyp presence. The increasing interest in CRSwNP research is attributed to its complex pathogenesis, significant symptom burden, and challenging management.3,4 In Western countries, CRSwNP predominantly exhibits a Type 2 (T2) inflammation pattern.5 In contrast, patients from China demonstrate a mixed Type 1 (T1) and Type 3 (T3) inflammatory profile,6 underscoring the heterogeneity in inflammatory mechanisms and downstream tissue remodeling processes across different populations.
Vitamin D, a steroid hormone, undergoes an initial hepatic hydroxylation to form the circulating metabolite 25-hydroxyvitamin D (25(OH)D), which is subsequently converted into its active form, 1,25-dihydroxyvitamin D (1,25(OH)2D), primarily through renal hydroxylation. Serum 25(OH)D status is influenced by environmental and regional factors, for example, sunlight exposure, season, and latitude. Vitamin D is recognized for its immunomodulatory properties,7–9 including the differentiation of Th17 cells,10 proliferation of activated B cells, and generation of plasma cells.11 Recent investigations have also highlighted vitamin D’s role in modulating neutrophilic and eosinophilic inflammation.9,12 Although the precise role of vitamin D in CRSwNP pathogenesis is still being elucidated, accumulating evidence points towards a significant involvement in its pathophysiology.
Furthermore, serum levels of 25(OH)D may serve as a potential independent predictor for chronic diseases, with accumulating evidence linking vitamin D deficiency to CRSwNP.13 However, a key unresolved question is whether vitamin D influences the structural pathology of CRSwNP, particularly tissue remodeling and fibrosis. Previous in vitro work suggests that vitamin D can inhibit fibroblast proliferation and suppress matrix metalloproteinase expression, indicating potential effects on tissue remodeling in CRSwNP.14 However, the in vivo relationship and functional significance of vitamin D with respect to the pathological structural characteristics of nasal polyps are still unclear.
This study compared clinical and histological features among CRSwNP patients stratified by serum vitamin D status (deficient, insufficient, and sufficient). Additionally, we investigate gene expression profiles between CRSwNP patients with and without serum vitamin D deficiency. Collectively, our research aims to delineate vitamin D–associated characteristics of CRSwNP and to explore molecular pathways potentially involved in fibrosis-related structural remodeling of nasal polyps.
Materials and Methods
Cohort
This was a single-center, retrospective study. We enrolled consecutive patients admitted to the Department of Otorhinolaryngology, Seventh Affiliated Hospital of Sun Yat-sen University, between November 2019 and September 2021. During the study period, 126 patients with CRSwNP were initially screened. A study flowchart illustrating the patient selection process is presented in Figure 1. Eligible participants were individuals aged 16 years or older who were scheduled to undergo bilateral endoscopic sinus surgery (ESS) for CRSwNP. The diagnosis for CRSwNP was independently confirmed by two senior physicians according to the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS 2020) criteria.15 Patients were excluded if they met any of the following criteria: (1) incomplete clinical records, including missing tissue samples, baseline blood counts, nasal endoscopy videos, or computed tomography (CT) images; (2) use of topical intranasal corticosteroids within four weeks or systemic corticosteroids within twelve weeks prior to the initial blood draw; (3) presence of co-existing conditions such as fungal rhinosinusitis, cystic fibrosis, gastrooesophageal reflux, or sinonasal malignancy; or (4) missing post-operative follow-up data at the 12 month time point. Twenty-five patients were excluded, including 16 who were lost to follow-up and 9 with unavailable or poor-quality H&E whole-slide images. Ultimately, 101 patients were included in the final analysis. Based on serum vitamin D levels, patients were classified into three groups: vitamin D–deficient (n = 34), insufficient (n = 48), and sufficient (n = 19). A standardized data collection form was used to extract the following information: anonymised patient ID, gender, smoking status, comorbidities (asthma, allergic rhinitis), history of previous Endoscopic Sinus Surgery (ESS), and peripheral blood eosinophil count. Disease severity was assessed using the pre-operative Lund–Kennedy endoscopic score (LKS) and the Lund–Mackay CT score (LMS). Comorbid asthma was diagnosed based on the Global Initiative for Asthma (GINA 2010) guidelines,16 and allergic rhinitis was defined according to the Allergic Rhinitis and its Impact on Asthma (ARIA) criteria.17 To ensure reliability, the LKS was calculated independently by two blinded investigators, and the results were averaged. The LMS was determined by consensus between a radiologist and a rhinologist, with a third senior reviewer consulted to resolve any discrepancies.18
 |
Figure 1 Flow Diagram of Patient Screening and Enrollment. In this study, we enrolled 101 patients with chronic rhinosinusitis with nasal polyps (CRSwNP). Based on serum vitamin D levels, patients were classified into three groups: vitamin D-deficient (n = 34), vitamin D-insufficient (n = 48), and vitamin D-sufficient (n = 19). |
This study was reviewed and approved by the Ethics Committee of Seventh Affiliated Hospital of Sun Yat-sen University (KY-2024-238-01). Written informed consent was obtained from all participants prior to their inclusion in the study.
Clinical Assessment and Patient’s Follow-up
The symptom severity and treatment outcome were assessed in the cohort. The total nasal symptom score (TNSS) was calculated as the sum of scores for four individual symptoms, including nasal congestion, anterior rhinorrhea, postnasal drip, and loss of smell. These nasal symptoms were assessed using a scale of 0 = None, 1 = Mild, 2 = Moderate, or 3 = Severe. The TNSS used in our study was the instantaneous TNSS (iTNSS). The iTNSS score was calculated based on the severity of symptoms reported by the patient at the time of the clinic visit/data collection, reflecting the instantaneous status of the disease. Disease control was assessed according to the EPOS 2020 criteria,15 with status classified as controlled, partly controlled, or uncontrolled. Two experienced otolaryngologists, blinded to patients’ clinical and laboratory data, performed the classification independently. Discrepancies were resolved by consensus, and a third senior otolaryngologist was consulted if necessary.
Histopathologic Evaluation
Nasal polyp specimens were collected from all participants undergoing endoscopic sinus surgery. Consistent with prior studies,19–21 a comprehensive histopathological assessment was performed to evaluate various tissue features. All histological evaluations were performed by two independent researchers who were blinded to the patients’ clinical data, including serum vitamin D status and other clinical parameters. The assessment included evaluation and scoring of features such as basement membrane thickening, squamous metaplasia, subepithelial fibrosis, and goblet and gland cell densities. Additionally, mucosal ulceration, subepithelial edema, epithelial hyperplasia, Charcot-Leyden crystal (CLC) formation, and eosinophil aggregates were evaluated. The classification of basement membrane thickening was determined by thickness measurements and categorized as mild, moderate, or severe. Squamous metaplasia was quantified based on the proportion of metaplastic cells and categorized as none (no squamous cell metaplasia), mild (<50% squamous cell metaplasia), moderate (50–75% squamous cell metaplasia), or severe (>75% squamous cell metaplasia). Subepithelial fibrosis was classified as absent, present (mild; <50% of the field affected), or extensive (moderate to severe; ≥50% of the field affected). For the primary statistical analysis, fibrosis was analyzed using three groups—absent, mild (present), and extensive (combining moderate and severe)—to ensure sufficient statistical power and to highlight clinically significant pathological changes. At 400x magnification, counts were performed for goblet cells, total inflammatory cells, eosinophils, neutrophils, and gland cells. The severity of subepithelial edema was categorized into none, mild (focal edema, <10%), moderate (10–50%), and severe (diffuse edema >50% or polypoid changes). Both mucosal ulceration and epithelial hyperplasia, as well as CLC formation and eosinophil aggregates, were identified as either present or absent. Eosinophil aggregates were specifically defined as one or more clusters of over 20 eosinophils per high power field within the lamina propria. For each nasal polyp specimen, counts were performed on three tissue blocks. In each block, five non-overlapping subepithelial fields were randomly selected for counting at 400× high-power field (HPF) using an ocular grid, and the mean number of cells per HPF was calculated for each cell type. All histological quantification was independently performed by two pathologists blinded to the clinical data and patients’ vitamin D status. Inter-rater reliability was assessed on a random subset of 20% of slides using the intraclass correlation coefficient (ICC), which indicated excellent agreement (ICC = 0.85). Any remaining discrepancies were resolved by joint review.
Bulk RNA Sequencing for Nasal Polyps
Total RNA was extracted utilizing the TRIzol Reagent (Invitrogen, CA, USA) in accordance with the manufacturer’s protocol. RNA purity and quantification were assessed using the NanoDrop 2000 spectrophotometer (Thermo Scientific, USA), and RNA integrity was verified using the Agilent 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA). Subsequently, RNA-seq library construction was performed using the VAHST Universal V6 RNA-seq Library Prep Kit, following the manufacturer’s instructions. Transcriptome sequencing and subsequent analysis were carried out by OE Biotech Co., Ltd. (Shanghai, China). Sequencing was conducted on an Illumina NovaSeq 6000 platform, generating 150 bp paired end reads. Initial processing of raw reads in fastq format involved quality control using fastp, where low-quality reads were filtered out to produce clean reads. These clean reads were then aligned to the reference genome using HISAT2. Gene expression levels were quantified in terms of FPKM (Fragments Per Kilobase of transcript per Million mapped reads), and the read counts for each gene were determined using HTSeq-count.
Measurement of Serum 25-Hydroxyvitamin D Level
Prior to surgery, serum levels of 25-hydroxyvitamin D (25-(OH)D) were measured in all participants using an enzyme-linked immunosorbent assay (ELISA) provided by ALPCO Immunoassays (Salem, New Hampshire, USA). Based on the established guidelines, Vitamin D levels were categorized as follows: deficient (< 20 ng/mL), insufficient (20-< 30 ng/mL), and normal (≥ 30 ng/mL).22 Patients were stratified into three vitamin D status groups (deficient, insufficient, and sufficient) for clinical and histological comparisons; however, for transcriptomic analysis, the insufficient and sufficient groups were consolidated into a single “non-deficient” reference group to enhance statistical power.
Statistical Analysis
Clinical and demographic data are presented as means with standard deviations (SD) or medians with interquartile ranges (IQR), as appropriate. The normality of data distribution was evaluated using the Shapiro–Wilk test. Univariate comparisons of normally distributed variables were conducted using t-tests, whereas the Mann–Whitney U-test was applied to non-normally distributed variables. Categorical variables were analyzed using Chi-square tests or Fisher’s exact tests when appropriate. Because the proportional odds assumption was violated (test of parallel lines, P < 0.05), multinomial logistic regression is used to estimate category-specific associations between vitamin D deficiency and fibrosis severity. Fibrosis status (absent, present, or extensive) was included as the outcome variable, with “absent fibrosis” as the reference category. Vitamin D deficiency (yes/no) was included as the main predictor, and age (continuous) was adjusted for as a covariate. Results are reported as adjusted multinomial odds ratios (AOR) with 95% confidence intervals. All statistical analyses were performed using R software (Version 4.3.1). A two-sided P < 0.05 was considered statistically significant.
Transcriptomic data analysis was conducted using R software (Version 4.3.1). Differential expression was assessed using the DESeq2 R package. Principal component analysis (PCA) was utilized to confirm the biological replicates’ consistency. Genes were considered significantly differentially expressed if they met the criteria of a padjust value less than 0.05 and an absolute fold change greater than 1.5. Cluster analysis of these differentially expressed genes (DEGs) was executed using the Pheatmap R package. Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analyses of the DEGs were performed to identify significantly enriched terms, using the Clusterprofiler R package.
Results
General Characteristics of the Cohort
A total of 101 patients diagnosed with CRSwNP were included in the study. The cohort predominantly consisted of males (73.3%), with a mean age of 39.9 years. Among these patients, thirty-four (33.7%) had comorbid allergic rhinitis, and three (3.0%) had asthma. A subset of eight patients (7.9%) had undergone two or more sinus surgeries. Additionally, seven individuals (6.9%) were identified as current smokers. The subsequent research workflow was illustrated in Figure 2.
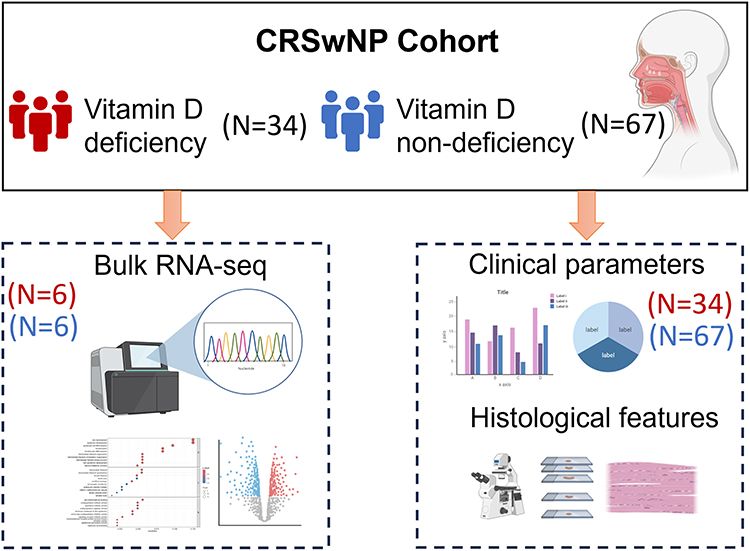 |
Figure 2 Workflow of study. The figure provides a visual summary of the methodology and analytical approach applied in the study. Initial analyses were performed on clinical parameters and histological features across the vitamin D-deficient (n = 34) and non-deficient groups (n = 67). Subsequently, from each cohort, six samples were carefully chosen for bulk RNA sequencing. This was followed by a comprehensive analysis of the transcriptomic expression profiles. |
Clinical Features of Patients by Serum 25(OH)D Status
To evaluate the clinical implications of vitamin D status, patients were categorized into deficient, insufficient, and sufficient groups based on their serum 25(OH)D concentrations, with baseline characteristics presented in Table 1. The age of patients in the vitamin D-deficient group was significantly lower than that in the non-deficient group (P = 0.017). Furthermore, the Total Nasal Symptom Score (TNSS) was higher in the deficient group compared to the non-deficient group, although this difference approached but did not reach statistical significance (P = 0.107). No significant differences were observed between the groups in terms of gender, the presence of comorbid allergic rhinitis, comorbid asthma, history of prior sinus surgery, smoking history, and preoperative LMS. Additionally, eosinophil counts in peripheral blood and tissue, as well as tissue neutrophil counts, did not differ significantly across the groups. Similarly, there were no significant differences in disease control status among the groups.
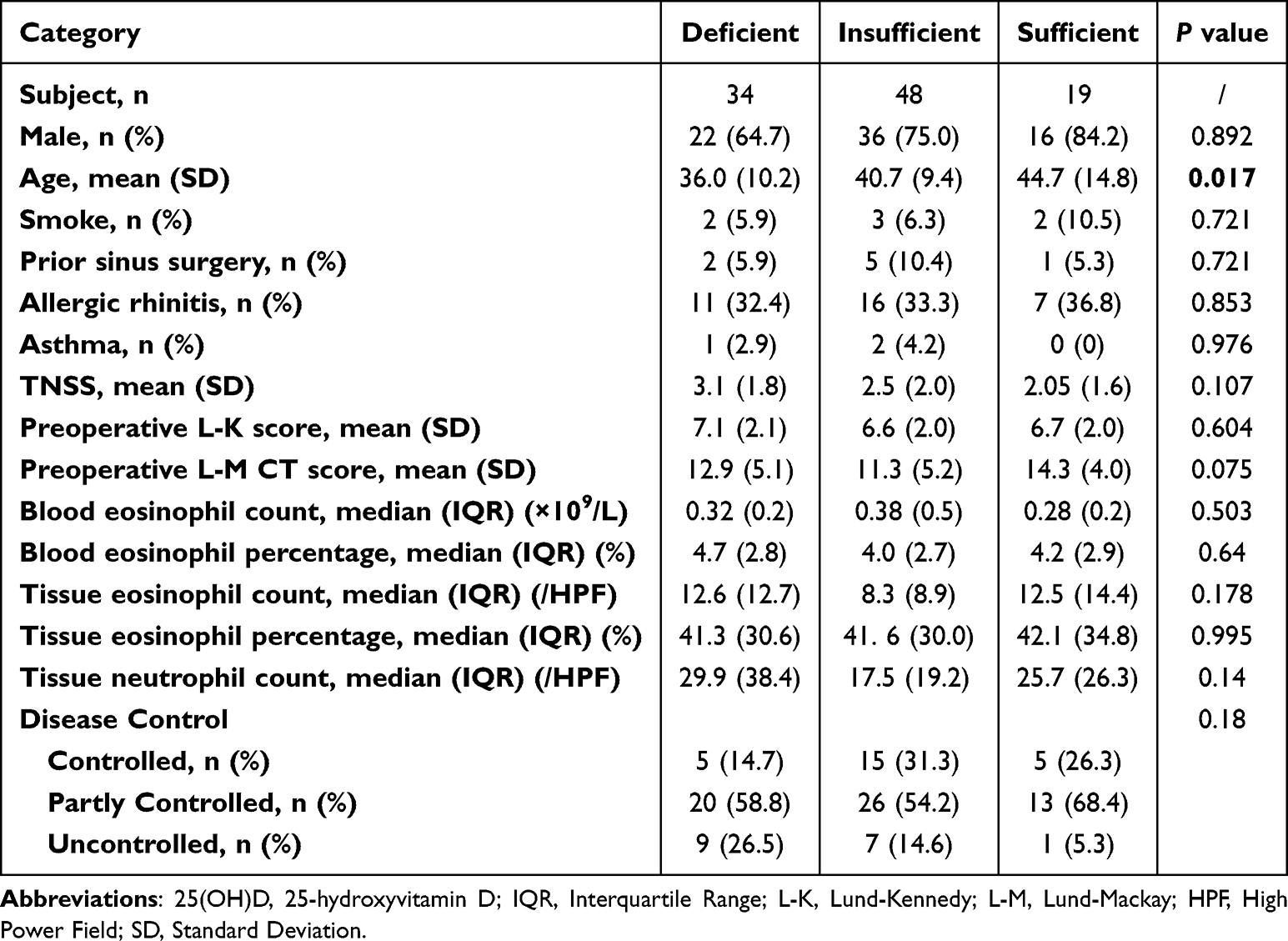 |
Table 1 Clinical Characteristics of Patients Stratified by Serum 25(OH)D Status |
Comparison of Histological Features Among CRSwNP Patients Stratified by Serum Vitamin D Status
To further characterize the pathohistological features of nasal polyp tissues in relation to vitamin D status, we performed a comprehensive comparative analysis of tissue structural characteristics among patients stratified into deficient, insufficient, and sufficient vitamin D groups. Subepithelial fibrosis differed significantly among the three vitamin D status groups (P = 0.008). Patients with vitamin D non-deficiency predominantly exhibited present (mild) fibrosis, whereas those with vitamin D-deficiency levels showed a higher proportion of extensive (moderate to severe) fibrosis. Representative histological images illustrating these differences are presented in Figure 3. Additionally, an increased thickness of the basement membrane was observed in the nasal polyps of in vitamin D sufficient and insufficient groups compared to the deficient group, although this variation did not reach statistical significance. Other histopathological features did not differ significantly across the three vitamin D status groups. Detailed results are provided in Table 2. After adjustment for potential confounders, including age, sex, season of blood sampling, smoking status, comorbid allergic rhinitis, comorbid asthma, and history of prior endoscopic sinus surgery, we initially fitted a multivariable ordinal logistic regression model with fibrosis grade as the outcome. However, the proportional odds assumption was violated (test of parallel lines, P < 0.05). Therefore, a multinomial logistic regression model was adopted as the final analytical approach, with “absent fibrosis” as the reference category. In the fully adjusted multinomial model, vitamin D deficiency was significantly associated with increased odds of mild (present) subepithelial fibrosis compared with absent fibrosis (adjusted OR 28.75, 95% CI 2.22–372.29, P = 0.010). In contrast, no statistically significant association was observed between vitamin D deficiency and extensive fibrosis. Other covariates, including age, sex, season of blood sampling, smoking status, comorbid allergic rhinitis, comorbid asthma, and prior endoscopic sinus surgery, were not significantly associated with fibrosis severity in either comparison. Complete model coefficients are presented in Table S1. Sensitivity and subgroup analyses were further performed to assess the robustness of the association between vitamin D deficiency and subepithelial fibrosis severity. Specifically, sensitivity analyses excluding participants aged <18 years (Table S2) and subgroup analyses restricted to non-smoking patients (Table S3) yielded results consistent with the primary analysis. In addition, exploratory analyses were conducted to evaluate the association between subepithelial fibrosis and disease outcomes (Table S4), as well as correlations between serum vitamin D levels and inflammatory biomarkers (Table S5); however, no statistically significant associations were observed in these analyses.
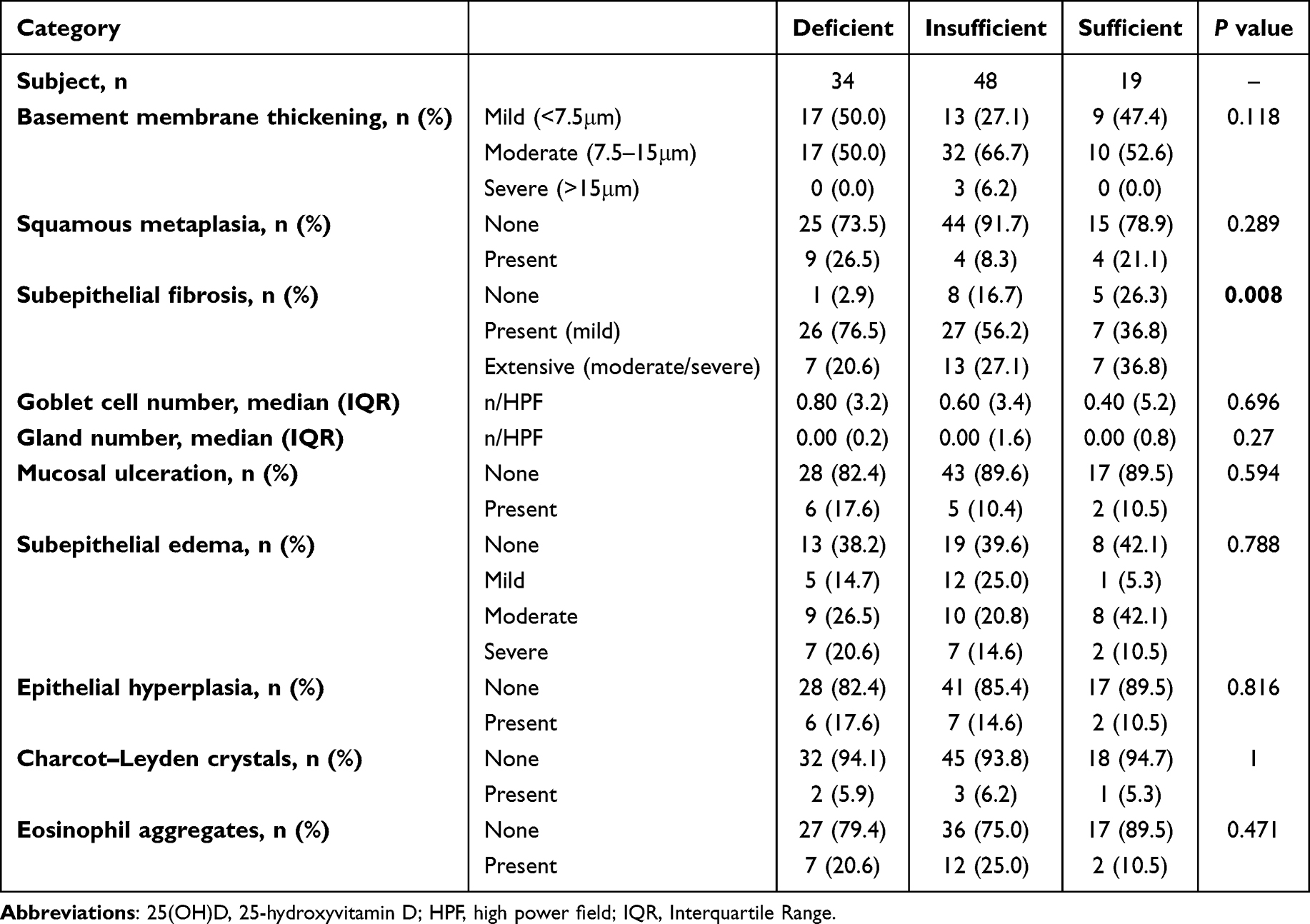 |
Table 2 Histopathological Features of Nasal Polyps Stratified by Serum 25(OH)D Status |
 |
Figure 3 Representative histological images of subepithelial fibrosis in the vitamin D-deficient and non-vitamin D-deficient groups (H&E staining, 200×). The images from left to right show mild, moderate, and severe subepithelial fibrosis, respectively. Subepithelial fibrosis was classified as absent, present (mild; <50% of the field affected), or extensive (moderate to severe; ≥50% of the field affected). Moderate to severe fibrosis characterized by significant basement membrane thickening are predominantly observed in the vitamin D-deficient group. |
Gene Expression Profile Between Vitamin D Deficiency Group and Vitamin D Non-Deficiency Group
To explore the intrinsic transcriptomic differences between groups with and without vitamin D deficiency, we selected six samples from each group for comprehensive Bulk RNA sequencing (RNA-seq) analysis. Using Principal Component Analysis (PCA) and heatmap visualization, we discerned significant distinctions between the vitamin D-deficient and non-deficient groups (Figure 4a and b). Compared to the non-deficient group, the deficient group exhibited upregulation of 100 genes and downregulation of 68 genes (Figure 4c). Notably, in the vitamin D-deficient group, there was a significant upregulation of genes encoding collagen and fibrillin, specifically COL11A1, COL26A1, COL8A1, FBN1, COL1A2, and COL3A1. This upregulation correlates with enhanced tissue fibrosis in the vitamin D-deficient group relative to the non-deficient group. The genes that were significantly upregulated and downregulated are catalogued in Tables 3 and 4, respectively.
 |
Table 3 The Significantly up-Regulated Genes in the Vitamin D Deficient Group Compared to Non-Deficient Group |
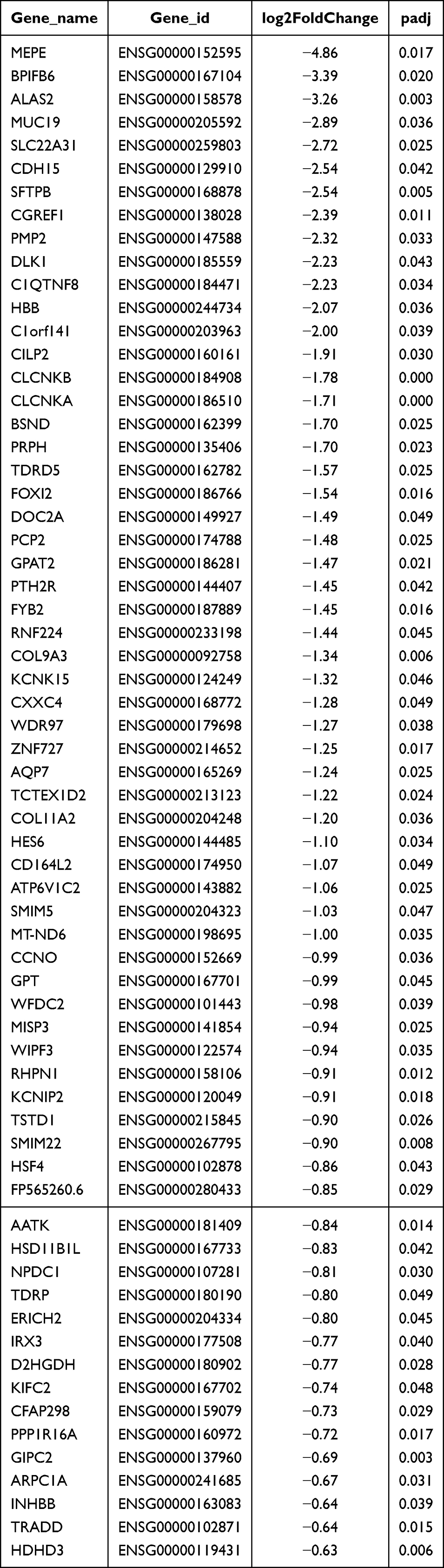 |
Table 4 The Down-Regulated Genes in the Vitamin D Deficient Group Compared to Non-Deficient Group |
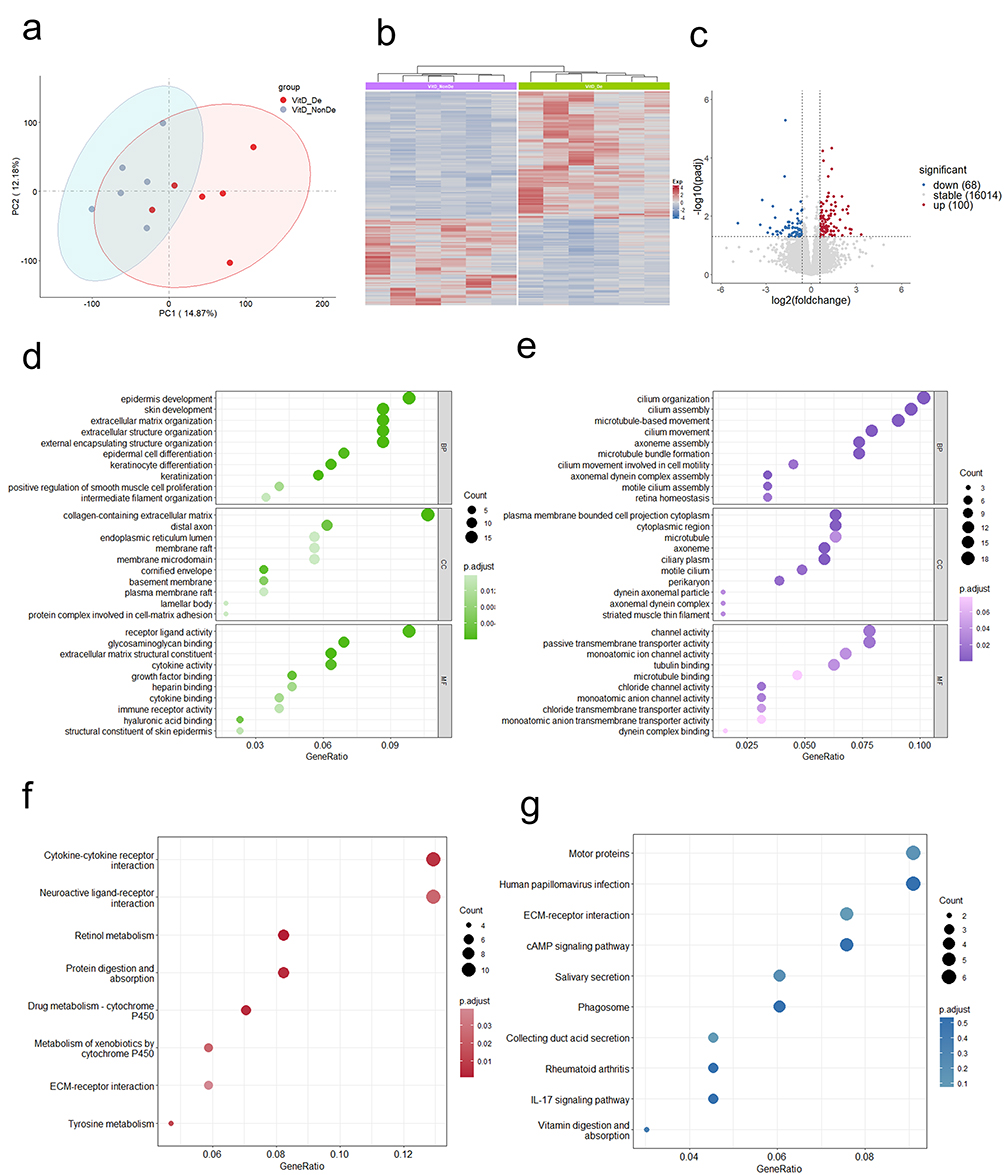 |
Figure 4 Transcriptomic analysis between vitamin D-deficient group and vitamin D non-deficient group. (a) Principal Component Analysis (PCA) of the samples from both groups, illustrating the distribution of variance. (b) Heatmap displaying the gene expression profiles of the vitamin D non-deficient and deficient groups, based on differentially expressed genes. (c) Volcano plot depicting the landscape of differentially expressed genes, with statistical significance plotted against fold-change values. (d) Gene Ontology (GO) enrichment analysis of significantly up-regulated genes. (e) GO enrichment analysis of significantly down-regulated genes. (f) Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis for significantly up-regulated genes. (g) KEGG analysis for significantly down-regulated gene. |
Furthermore, we conducted pathway enrichment analysis on the differentially expressed genes. In the Gene Ontology (GO) analysis for Biological Processes (BP), the upregulated genes in the vitamin D deficient group were significantly enriched in processes related to the extracellular matrix structure and organization. For the Cellular Component (CC) category, these genes predominantly related to the collagen-containing extracellular matrix. In terms of Molecular Function (MF), the focus was on the structural constituents of the extracellular matrix (Figure 4d). Conversely, the significantly downregulated genes were primarily involved in pathways associated with axoneme assembly, microtubule bundle formation, and cilium movement, among other relevant GO pathways (Figure 4e). Detailed results of these significant GO enrichment pathways are provided in Table S6 and S7.
Additionally, the Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analysis revealed that ECM-receptor interaction was a prominent pathway enriched with upregulated genes in the vitamin D deficient group (Figure 4f). The analysis of pathways enriched with downregulated genes highlighted the vitamin digestion and absorption pathway (Figure 4g). Comprehensive details on the KEGG enrichment pathways are documented in Table S8 and S9. This extensive analysis underscores the molecular alterations induced by vitamin D deficiency and highlights potential targets for further investigation and therapeutic intervention.
Discussion
Our integrated histopathological and transcriptomic analysis demonstrates that vitamin D deficiency in CRSwNP is more strongly correlated with subepithelial fibrosis than with inflammatory infiltration. Histological analysis revealed that vitamin D-deficient patients had a significantly higher incidence of subepithelial fibrosis. Meanwhile, transcriptomic profiling indicated altered expression of genes enriched in extracellular matrix organization pathways, which was consistent with the observed structural changes. Together, these findings indicate that vitamin D deficiency correlates preferentially with tissue remodeling rather than inflammatory burden in nasal polyps. This positions subepithelial fibrosis as a previously underappreciated pathological hallmark of vitamin D-deficient CRSwNP. Building on previous reports that vitamin D exerts important immunomodulatory effects and is implicated in the pathophysiology of nasal polyps,23–25 our study provides the first systematic evidence linking low vitamin D status specifically to a fibrosis-predominant disease phenotype.
Histopathological analysis identified subepithelial fibrosis as the most prominent feature associated with vitamin D deficiency, whereas epithelial injury and inflammatory cell infiltration did not differ significantly between groups. Changes in histopathological structures are often closely associated with pathogenesis and inflammatory characteristics.20,26–28 Consistently, transcriptomic profiling revealed differential expression of genes involved in extracellular matrix (ECM) organization, collagen synthesis, and fibroblast growth factor–related pathways. This concordance between structural and molecular findings supports the notion that vitamin D deficiency is preferentially associated with tissue remodeling rather than inflammatory burden, in line with previous reports linking low vitamin D levels to enhanced fibrosis in CRSwNP.14,29 This pattern suggests that vitamin D deficiency may be linked to altered stromal cell behavior and fibrogenic signaling thresholds without necessarily altering inflammatory cell recruitment, thereby uncoupling tissue remodeling from overt inflammation.
Clinically, while previous studies have reported more severe disease manifestations in vitamin D-deficient CRSwNP patients,30,31 our findings suggest that the impact of vitamin D status on symptom severity and postoperative outcomes may be limited at the clinical level in our cohort. Notably, despite comparable clinical presentations between groups, pronounced differences were observed at the histological and transcriptomic levels, supporting the concept that tissue remodeling may precede overt clinical deterioration. The observed age difference between groups likely reflects baseline cohort characteristics rather than an independent association with vitamin D status and was accounted for in subsequent analyses.
Despite similar clinical presentations across vitamin D status groups, our comprehensive histological and transcriptomic analyses revealed a distinct ECM-enriched molecular signature exclusively in vitamin D-deficient nasal polyps, consistent with enhanced fibrotic remodeling. This suggests that vitamin D deficiency may be linked to early structural changes even without evident clinical deterioration. This profibrotic phenotype arises within the characteristic immunological context of East Asian CRSwNP, where inflammation typically exhibits a mixed Th1/Th17 pattern rather than the Th2-dominant profile observed in Western populations. In this context, vitamin D deficiency may predominantly affect tissue remodeling pathways rather than classical inflammatory responses. Although causality cannot be inferred from our observational data, existing evidence provides a plausible mechanism. The vitamin D active metabolite, 1,25(OH)2D, modulates TGF-β/SMAD2/3 signaling, thereby limiting myofibroblast differentiation and excessive ECM deposition;32–34 thus, Vitamin D deficiency may blunt these antifibrotic effects, fostering a profibrotic microenvironment. Beyond its role in fibroblast regulation, vitamin D contributes to the maintenance of epithelial barrier integrity, promotes tissue repair,36 and inhibits epithelial–mesenchymal transition.37 Respiratory epithelial cells are also capable of locally converting inactive vitamin D into its active form, enabling site-specific regulation of host defense mechanisms.38 In parallel, vitamin D signaling has been shown to suppress TLR4/NF-κB–mediated inflammatory responses in respiratory epithelial cells and to enhance glucocorticoid-mediated anti-inflammatory effects.39 Furthermore, clinical evidence suggests that variations in vitamin D receptor signaling are associated with glucocorticoid responsiveness in airway diseases.35 Collectively, these mechanisms offer a biologically plausible explanation for the structural changes observed in vitamin D-deficient CRSwNP, even when there is no significant clinical deterioration.
This study has several strengths. First, we integrated structured histopathological assessment with transcriptomic profiling, enabling a robust evaluation of tissue remodeling and its molecular correlates. Second, by focusing on subepithelial fibrosis rather than inflammatory cell infiltration alone, we addressed a clinically relevant but underexplored aspect of CRSwNP pathophysiology. Third, our analysis was conducted in an East Asian CRSwNP cohort, providing insights into the role of vitamin D within a non–Th2-dominant inflammatory context.
Despite these strengths, several limitations warrant acknowledgment. First, the sample size was relatively modest, and our findings have not yet been validated in a larger, independent external cohort. The wide confidence intervals observed for the association between vitamin D deficiency and mild fibrosis likely reflect the limited number of cases within specific histological strata; thus, these results should be interpreted with caution. Future studies with larger multi-center cohorts are needed to validate our findings and enhance their generalizability. Second, the scale of the transcriptomic sequencing was constrained, necessitating further validation in larger cohorts to confirm the molecular signatures identified. Subsequent studies with deeper transcriptomic profiling or single-cell sequencing could further refine the ECM-enriched molecular signature identified herein. Third, as a retrospective clinical study, it lacks direct experimental evidence (eg, in vitro or in vivo models) to establish a definitive causal link and elucidate the precise immunomodulatory mechanisms through which vitamin D deficiency drives tissue fibrosis in nasal polyps. Furthermore, the absence of patient-reported outcome measures, such as the 22-item Sinonasal Outcome Test (SNOT-22), limits our ability to assess the long-term clinical burden and health-related quality of life. Additionally, key physiological determinants of serum vitamin D levels, including body mass index (BMI) and sunlight exposure, were not systematically recorded, which may have introduced residual confounding or affected the precision of our estimates. Regarding lifestyle factors, although sensitivity analyses excluding smokers yielded consistent results, cigarette smoking remains a potential confounder. Due to the inherent limitations of retrospective data, we lacked a refined stratification of smoking exposure (eg, pack-years), highlighting the need for prospective studies with more precise, longitudinal assessments. Finally, the findings may be subject to regional bias, highlighting the need for multi-center, cross-geographical comparative research to confirm the universality of our conclusions.
Conclusion
In conclusion, vitamin D deficiency was associated with specific histological features, particularly subepithelial fibrosis, in patients with CRSwNP. Transcriptomic analysis further revealed distinct gene expression profiles in the vitamin D–deficient group, with enrichment of extracellular matrix–related pathways. Our findings support a potential link between vitamin D status and fibrotic tissue remodeling in CRSwNP, suggesting that vitamin D deficiency may characterize a subset of patients with a more pronounced fibrotic phenotype. Further mechanistic studies using in vitro and animal models are warranted to elucidate the direct role of vitamin D in regulating fibroblast activity and extracellular matrix deposition. Prospective clinical studies are also needed to determine whether modulation of vitamin D status could influence disease course or postoperative outcomes in CRSwNP.
Data Sharing Statement
The datasets are available from the corresponding author upon reasonable request. The accession number of raw sequencing data from nasal polyp samples in this study is GSA (Genome Sequence Archive) HRA007203.
Acknowledgments
We extend our gratitude to the Otorhinolaryngology team at the Seventh Affiliated Hospital of Sun Yat-sen University for their invaluable assistance. We also thank the Pathology Department of the same institution for providing essential technical support.
Author Contributions
Mengshi Chi: Conceptualization, data collection, data curation, formal analysis, investigation, methodology, writing – original draft. Kanghua Wang: Data curation, validation, visualization, writing – review & editing. Mingmin Bi: Data collection, data curation, validation, writing – review & editing. Zheng Yang: Investigation, methodology, quality control, writing – review & editing. Yuhan Xing: Conceptualization, supervision, writing – review & editing. Yunping Fan: Conceptualization, funding acquisition, resources, supervision, writing – review & editing. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. All authors have agreed on the journal to which the article will be submitted. Mengshi Chi and Kanghua Wang contributed equally to this work as co-first authors. Yuhan Xing and Yunping Fan contributed equally to this work as co-corresponding authors.
Funding
This study was funded by the Sanming Project of Medicine in Shenzhen (grant number SZSM202111005) and the National Key R&D Program of China (Grant No. 2023 YFC2410200).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Shi JB, Fu QL, Zhang H, et al. Epidemiology of chronic rhinosinusitis: results from a cross-sectional survey in seven Chinese cities. Allergy. 2015;70:533–16. doi:10.1111/all.12577
2. Sedaghat AR, Kuan EC, Scadding GK. Epidemiology of chronic rhinosinusitis: prevalence and risk factors. J Allergy Clin Immunol Pract. 2022;10:1395–1403. doi:10.1016/j.jaip.2022.01.016
3. Takabayashi T, R.p S. Formation of nasal polyps: The roles of innate type 2 inflammation and deposition of fibrin. J Allergy Clin Immunol. 2020;145:740–750. doi:10.1016/j.jaci.2020.01.027
4. Kato A, Schleimer RP, Bleier BS. Mechanisms and pathogenesis of chronic rhinosinusitis. J Allergy Clin Immunol. 2022;149:1491–1503. doi:10.1016/j.jaci.2022.02.016
5. Bachert C, Zhang N, Hellings PW, et al. Endotype-driven care pathways in patients with chronic rhinosinusitis. J Allergy Clin Immunol. 2018;141:1543–1551. doi:10.1016/j.jaci.2018.03.004
6. Wang X, Zhang N, Bo M, et al. Diversity of T H cytokine profiles in patients with chronic rhinosinusitis: a multicenter study in Europe, Asia, and Oceania. J Allergy Clin Immunol. 2016;138:1344–1353. doi:10.1016/j.jaci.2016.05.041
7. Malaguarnera L. Vitamin D and microbiota: two sides of the same coin in the immunomodulatory aspects. Int Immunopharmacol. 2020;79:106112. doi:10.1016/j.intimp.2019.106112
8. Hamza FN, Daher S, Fakhoury HMA, et al. Immunomodulatory properties of vitamin D in the intestinal and respiratory systems. Nutrients. 2023;15:1696. doi:10.3390/nu15071696
9. Xiao Q, Wang H, Song J, et al. Impaired local Vitamin D3 metabolism contributes to IL-36g overproduction in epithelial cells in chronic rhinosinusitis with nasal polyps. Rhinology. 2024;62:236–249. doi:10.4193/RhinRhin23.123
10. Fakhoury HMA, Kvietys PR, AlKattan W, et al. Vitamin D and intestinal homeostasis: Barrier, microbiota, and immune modulation. J Steroid Biochem Mol Biol. 2020;200:105663. doi:10.1016/j.jsbmb.2020.105663
11. Chen S, Sims GP, Chen XX, et al. Modulatory effects of 1,25-dihydroxyvitamin D3 on human B cell differentiation. J Immunol. 2007;179:1634–1647. doi:10.4049/jimmunol.179.3.1634
12. Huang W, Zhang Y, Li Y, et al. Vitamin D impedes eosinophil chemotaxis via inhibiting glycolysis-induced CCL26 expression in eosinophilic chronic rhinosinusitis with nasal polyps. Cell Commun Signal. 2025;23:104. doi:10.1186/s12964-025-02078-2
13. Bavi F, Movahed R, Salehi M, et al. Chronic rhinosinusitis with polyposis and serum vitamin D levels. Acta Otorhinolaryngol Ital. 2019;39:336–340. doi:10.14639/0392-100X-2439
14. Sansoni ER, Sautter NB, Mace JC, et al. Vitamin D3 as a novel regulator of basic fibroblast growth factor in chronic rhinosinusitis with nasal polyposis. Int Forum Allergy Rhinol. 2015;5:191–196. doi:10.1002/alr.21474
15. Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58:1–464. doi:10.4193/Rhin20.401
16. Brożek JL, Bousquet J, Baena-Cagnani CE, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126:466–476. doi:10.1016/j.jaci.2010.06.047
17. Brożek JL, Bousquet J, Agache I, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140:950–958. doi:10.1016/j.jaci.2017.03.050
18. Psaltis AJ, Li G, Vaezeafshar R, et al. Modification of the Lund-Kennedy endoscopic scoring system improves its reliability and correlation with patient-reported outcome measures. Laryngoscope. 2014;124:2216–2223. doi:10.1002/lary.24654
19. Snidvongs K, Lam M, Sacks R, et al. Structured histopathology profiling of chronic rhinosinusitis in routine practice. Int Forum Allergy Rhinol. 2012;2:376–385. doi:10.1002/alr.21032
20. Xu X, Seet JE, Yap QV, et al. Latent class analysis of structured histopathology in prognosticating surgical outcomes of chronic rhinosinusitis with nasal polyps in Singapore. Rhinology. 2023;61:358–367. doi:10.4193/Rhin22.455
21. Cui Y, Wang K, Shi J, et al. Endotyping difficult-to-treat chronic rhinosinusitis with nasal polyps by structured histopathology. Int Arch Allergy Immunol. 2023;184:1036–1046. doi:10.1159/000530864
22. Lee EJ, Hwang CS, Kim K-S. Lack of correlation between serum 25(OH)D level and endoscopy-based chronic rhinosinusitis in Korean adults. Rhinol J. 2018;57:139–146.
23. Pantazidou G, Papaioannou I, Skoulakis C, et al. Vitamin D levels in chronic rhinosinusitis in patients with or without nasal polyposis: a systematic review. Cureus. 2023;15:e46275. doi:10.7759/cureus.46275
24. Shrestha P, Deepak R, Bhalla AS, et al. Vitamin D and interleukins in chronic rhinosinusitis with polyposis. Indian J Otolaryngol. 2022;74:4756–4760. doi:10.1007/s12070-022-03085-2
25. Thakur P, Potluri P. Association of serum vitamin D with Chronic RhinoSinusitis in adults residing at high altitudes. Eur Arch Otorhinolaryngol. 2021;278:1067–1074. doi:10.1007/s00405-020-06368-y
26. Baird AM, Masliah J, Filip P, et al. Histopathologic features of biologic therapy nonresponders in chronic rhinosinusitis with nasal polyposis. Int Forum Allergy Rhinol. 2023;14:939–949.
27. Brown HJ, Tajudeen BA, Kuhar HN, et al. Defining the allergic endotype of chronic rhinosinusitis by structured histopathology and clinical variables. J Allergy Clin Immunol Pract. 2021;9(10):3797–3804. doi:10.1016/j.jaip.2021.06.013
28. Brescia G, Alessandrini L, Giacomelli L, et al. A classification of chronic rhinosinusitis with nasal polyps based on structured histopathology. Histopathology. 2020;76:296–307. doi:10.1111/his.13969
29. Wang L, Tai C, Chien C, et al. Vitamin D decreases the secretion of matrix metalloproteinase-2 and matrix metalloproteinase-9 in fibroblasts derived from Taiwanese patients with chronic rhinosinusitis with nasal polyposis. Kaohsiung J Med Sci. 2015;31:235–240. doi:10.1016/j.kjms.2015.02.001
30. Mostafa BE, Taha MS, Abdel Hamid T, et al. Evaluation of vitamin D levels in allergic fungal sinusitis, chronic rhinosinusitis, and chronic rhinosinusitis with polyposis. Int Forum Allergy Rhinol. 2016;6:185–190. doi:10.1002/alr.21585
31. Zand V, Baradaranfar M, Vaziribozorg S, et al. Correlation of serum vitamin D levels with chronic rhinosinusitis disease severity. Iran J Otorhinolaryngol. 2019;32:35–41.
32. Lee SA, Yang HW, Um JY, et al. Vitamin D attenuates myofibroblast differentiation and extracellular matrix accumulation in nasal polyp-derived fibroblasts through smad2/3 signaling pathway. Sci Rep. 2017;7(1):7299. doi:10.1038/s41598-017-07561-6
33. Meng XM, Nikolic-Paterson DJ, Lan HY. TGF-β: the master regulator of fibrosis. Nat Rev Nephrol. 2016;12(6):325–338. doi:10.1038/nrneph.2016.48
34. Ramirez AM, Wongtrakool C, Welch T, et al. Vitamin D inhibition of pro-fibrotic effects of transforming growth factor beta1 in lung fibroblasts and epithelial cells. J Steroid Biochem Mol Biol. 2009;118(3):142–150. doi:10.1016/j.jsbmb.2009.11.004
35. Mohamed NA, Abdel-Rehim AS. Influence of vitamin D receptor gene FokI and ApaI polymorphisms on glucocorticoid response in patients with asthma. Int Forum Allergy Rh. 2019;10(4):556–563. doi:10.1002/alr.22511
36. Liao S, Huang Y, Zhang J, et al. Vitamin D promotes epithelial tissue repair and host defense responses against influenza H1N1 virus and Staphylococcus aureus infections. Respir Res. 2023;24:175. doi:10.1186/s12931-023-02477-4
37. Xiong XR, Tian XL, Huo RJ, et al. 1α, 25-dihydroxyvitamin D3 inhibits transforming growth factor β1-induced epithelial-mesenchymal transition via β-catenin pathway. Chin Med J-Peking. 2020;133(11):1298–1303. doi:10.1097/CM9.0000000000000830
38. Hansdottir S, Monick MM, Hinde SL, et al. Respiratory epithelial cells convert inactive vitamin D to its active form: potential effects on host defense. J Immunol. 2008;181(10):7090–7099. doi:10.4049/jimmunol.181.10.7090
39. Wang L, Zhao Y, Yao S, et al. Vitamin D improves the effect of glucocorticoids on attenuating lipopolysaccharide-induced IL-6 production via TLR4/NF-κB pathway in human respiratory epithelial cells. Int Arch Allergy Immunol. 2022;183(9):1017–1028. doi:10.1159/000524855
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.