Back to Journals » Journal of Pain Research » Volume 16
Correlation Between Pain Intensity and Quality of Recovery After Video-Assisted Thoracic Surgery for Lung Cancer Resection
Authors Yoon SH ![]() , Bae J
, Bae J ![]() , Yoon S
, Yoon S ![]() , Na KJ, Lee HJ
, Na KJ, Lee HJ ![]()
Received 18 June 2023
Accepted for publication 25 September 2023
Published 2 October 2023 Volume 2023:16 Pages 3343—3352
DOI https://doi.org/10.2147/JPR.S426570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amitabh Gulati
Soo-Hyuk Yoon,1,* Jinyoung Bae,2,* Susie Yoon,1,3 Kwon Joong Na,4,5 Ho-Jin Lee1,3
1Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul, Republic of Korea; 2Department of Anesthesiology and Pain Medicine, Ajou University School of Medicine, Suwon, Republic of Korea; 3Department of Anesthesiology and Pain Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea; 4Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul, Republic of Korea; 5Department of Thoracic and Cardiovascular Surgery, Seoul National University College of Medicine, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Ho-Jin Lee, Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul, 03080, Republic of Korea, Tel +82-2-2072-0039, Fax +82-2-747-8363, Email [email protected]
Purpose: The Quality of Recovery-15 (QoR-15) questionnaire provides a multifaceted assessment of postoperative recovery, and the resulting score is recommended as an endpoint in clinical studies focused on postoperative pain. We aimed to investigate the correlation between the QoR-15 score and postoperative pain intensity in surgical patients.
Patients and Methods: Adult patients who underwent video-assisted thoracoscopic surgery (VATS) for lung cancer resection and were enrolled in a prospective registry or in a previous prospective study were included in this study. Baseline and perioperative data, including the results of assessment using the Korean version of the QoR-15 (QoR-15K) questionnaire at 48 hours postoperatively, were collected from the database. Correlations between the QoR-15K total score, questionnaire dimensions, and postoperative pain intensity at 48 hours postoperatively were determined using the Spearman correlation coefficient (ρ).
Results: We analyzed a total of 137 eligible patients. Significant negative correlations were noted between the QoR-15K total score and pain intensity at rest (ρ = − 0.45, 95% confidence interval [CI]: − 0.57 − − 0.31, P < 0.001) and during coughing (ρ = − 0.55, 95% CI: − 0.65 − − 0.42, P < 0.001) at 48 hours postoperatively. The pain dimension and pain intensity at 48 hours postoperatively showed significant correlations with physical comfort, emotional state, and physical independence dimensions. Multivariable logistic regression revealed a significant negative association between the pain score at 24 hours postoperatively and good or excellent postoperative recovery.
Conclusion: The results support the impact of postoperative pain on the overall postoperative quality of recovery in patients who underwent VATS for lung cancer resection. Moreover, the QoR-15K score may be considered as a primary endpoint in clinical studies on postoperative pain control.
Keywords: pain, postoperative, patient-reported outcome measures, perioperative care, perioperative medicine, thoracic surgery, video-assisted
Introduction
Improving postoperative recovery is a major goal for perioperative clinicians. Postoperative recovery has been traditionally evaluated based on physiological parameters, postoperative morbidity, length of hospital stay, and mortality. However, these indicators are not similar to those indicating postoperative recovery from the patients’ perspective.1 Further, with the advances in perioperative management, recognizing the substantial effects of new treatments with these conventional indicators is becoming difficult.2
Several assessment tools have been developed to quantitatively evaluate postoperative recovery, considering its multi-dimensional aspects.3 Among them, the Quality of Recovery-15 (QoR-15) questionnaire, a short form of the QoR-40, can be used for a comprehensive assessment of postoperative recovery,4 and its resulting scores have been recommended as endpoints in clinical studies focused on patient comfort and pain.5 Recently, it has been recommended as a standard outcome measure for evaluating postoperative recovery in clinical studies of surgical patients.6,7 Against this backdrop, recently, the Korean version of the QoR-15 (QoR-15K) questionnaire was validated to assess the quality of recovery in Korean surgical patients.2
Postoperative pain is one of the physiological parameters that reflect postoperative recovery, and two among the 15 items of the QoR-15 questionnaire are directly associated with it.4 Postoperative pain not only causes physical distress in surgical patients, but also affects various factors related to postoperative recovery.8,9 Severe postoperative pain can significantly impair the achievement of “DrEaMing” (drinking, eating, and mobilizing) after surgery, which is one of the major goals of perioperative management.10,11 In addition, analgesic methods can affect postoperative recovery through their side effects.8 Further, severe acute postoperative pain can result in chronic postoperative pain, which can impair the long-term quality of life in surgical patients.12 Therefore, postoperative pain management is a crucial component in the enhanced recovery after surgery program, which has recently become the standard for perioperative medicine.13
Only few studies have examined the relationship between postoperative pain and the quality of postoperative recovery. To the best of our knowledge, only one study has reported a significant negative correlation between postoperative pain intensity and quality of postoperative recovery, evaluated using the QoR questionnaire in the early postoperative period.14 Since the quality of postoperative recovery has been considered an important endpoint in postoperative pain management,15 we aimed to investigate their correlation in patients who underwent video-assisted thoracoscopic surgery (VATS) for lung cancer resection. In addition, we also aimed to investigate the correlation between postoperative pain intensity and other dimensions of the QoR-15K questionnaire, except the pain dimension.
Materials and Methods
Study Design and Population
The present study was approved by the institutional review board (IRB) of Seoul National University Hospital, Seoul, Korea (No. 2209-077-1358) and executed in compliance with the Declaration of Helsinki. The need for informed consent was waived in this study due to its retrospective design that involved using prospectively collected anonymized registry data or previously collected prospective anonymized data on VATS for lung cancer resection.16 The prospective registry used in this study was approved by the IRB of Seoul National University Hospital, Seoul, Korea (No. 2205-059-1322) and consecutive adult patients undergoing VATS for lung cancer resection have been enrolled in this registry since June 2022. The previous randomized controlled trial (RCT) targeted patients who were scheduled for elective VATS for lung cancer resection, and patient recruitment took place from July 2020 to August 2021.16 Under the monitoring of our institution’s Institutional Review Board (IRB), we have complied with all relevant data protection and privacy regulations throughout the duration of this study.
Adult patients (≥ 19 years of age) who underwent VATS for lung cancer resection and enrolled in either the aforementioned registry from June 2022 to August 2022 or the aforementioned RCT16 were included in the present study. Patients who underwent surgery in areas other than the lungs at the same surgical time, in who unplanned conversion to thoracotomy was performed, or who were not followed-up at 48 hours postoperatively were excluded. Considering a previous study,2 the Spearman correlation coefficient between postoperative pain intensity and the total score of the QoR-15K questionnaire performed 48 hours postoperatively was assumed to be 0.4. In the planning stage of the study, a sample size of 61 was considered as sufficient to achieve 90% power to detect this level of correlation between the variables, with a two-sided alpha of 0.05. By August 2022, a total of 95 patients who underwent VATS for lung cancer resection were enrolled in the registry, and we judged that the number of patients included in this study should exceed 61, assuming a dropout rate of 30%. However, during the data analysis phase, we decided to include patients from our previous RCT,16 who had undergone the same surgery, to conduct additional analyses on significant predictors of postoperative recovery evaluated with the QoR-15K questionnaire 48 hours postoperatively. The revised protocol was re-approved by our hospital’s IRB.
Perioperative Management
For all patients registered in the prospective registry data, anesthesia induction was performed with the use of propofol, fentanyl, and rocuronium, while sevoflurane was used for anesthesia maintenance. A continuous infusion of remifentanil was administered selectively according to the attending anesthesiologists. All patients included in the RCT data received total intravenous anesthesia with a target-controlled infusion of propofol and remifentanil.16 During anesthesia induction, 5 mg of dexamethasone and 0.075 mg of palonosetron were administered intravenously to prevent postoperative nausea and vomiting (PONV) unless contraindicated.
At the end of the surgery, 30 mg of ketorolac or 1 g of acetaminophen, and 50 μg of fentanyl was administered intravenously, and a fentanyl-based intravenous patient-controlled analgesia (IV-PCA) was initiated to the patient. The IV-PCA consisted of fentanyl (20 μg/mL) at a bolus of 1 mL with a lockout interval of 10 minutes and no continuous infusion.17 Sugammadex was used for the reversal of neuromuscular blockade. After extubation, patients were transferred to the post-anesthesia care unit, where 50 μg of fentanyl was administered intravenously as a rescue analgesic. In the patients enrolled in the RCT, those belonging to the nefopam group received a total of 80 mg of nefopam administered during 24 hours perioperatively.16
Ward ambulation and oral intake were permitted after 6 hours postoperatively, and a tramadol/acetaminophen combination tablet (tramadol 75 mg/acetaminophen 650 mg every 12 hours or tramadol 37.5 mg/acetaminophen 325 mg every 6 hours) was routinely administered from the time of resumption of oral intake. During postoperative fasting in the ward, 1 g acetaminophen or 50 mg tramadol was administered intravenously as a rescue analgesic. After oral intake was resumed, 200 mg ibuprofen was administered orally as a first-line rescue analgesic and 5 mg oxycodone as a second-line rescue analgesic. Rescue analgesics were administered according to the attending surgeons’ decision.
Data Collection
Demographic, comorbidity, and perioperative data were collected from the registry or RCT database. The QoR-15K questionnaire administration was conducted by research nurses on the day before surgery and 48 hours postoperatively. The score of each dimension of the questionnaire was calculated as the sum of the scores of the following items in parentheses: physical comfort (1st, 2nd, 3rd, 4th, and 13th items), physical independence (5th and 8th items), psychological support (6th and 7th items), emotional state (9th, 10th, 14th and 15th items), and pain (11th and 12th items).4 In addition, postoperative pain intensity measured by an 11-point numeric rating scale at rest and during coughing at 24 and 48 hours postoperatively, IV-PCA fentanyl consumption during the first 24 hours and 24–48 hours postoperatively, the occurrence of PONV during the first 24 hours and 24–48 hours postoperatively, and administration of rescue analgesics during the first 24 hours and 24–48 hours postoperatively were investigated by the research nurses. Data regarding the occurrence of postoperative complications, graded according to the Clavien–Dindo classification,18 during hospitalization and the length of hospital stay were also collected.
Statistical Analysis
Descriptive statistical analysis was performed to reveal the demographic and perioperative characteristics. Categorical data are expressed as numbers (percentages) and continuous data as mean (standard deviation) or median (interquartile range [IQR]) values, according to the normality evaluated by the Shapiro–Wilk test. The Hodges–Lehmann method was used to estimate the median differences and their 95% confidence interval (CI) between the pre and postoperative QoR-15K scores. The primary outcome was the correlation between the QoR-15K total score and postoperative pain score at 48 hours postoperatively. The secondary outcomes were the correlations between the scores in each dimension of the QoR-15K and postoperative pain score at 48 hours postoperatively. The Spearman correlation coefficient (ρ) was used to estimate the correlations between the QoR-15K total or dimension’s score and postoperative pain score at 48 hours postoperatively. Additionally, we conducted a multivariable binary logistic regression analysis with backward stepwise elimination to assess good or excellent postoperative recovery at 48 hours after surgery. Good or excellent postoperative recovery was defined as a QoR-15K total score of 122 or higher, assessed at 48 hours postoperatively.19 The analyses included the following variables: female (versus male), age ≥ 65 years, American Society of Anesthesiologists physical status 3 (versus 1 or 2), body mass index ≥ 25 kg/m2, current smoker, preoperative QoR-15K < 136, total intravenous anesthesia (versus sevoflurane anesthesia), duration of anesthesia ≥ 3 hours, pain score during coughing at 24 hours postoperatively, and PONV during the first 24 hours postoperatively. We arbitrarily defined a poor preoperative state evaluated by the preoperative QoR-15K as a score of less than 136. Considering that movement-evoked pain has a greater impact on postoperative functional recovery than pain at rest,20 we included the pain score during coughing as a variable instead of the pain score at rest. Variables with a p-value < 0.2 in the univariable logistic regression analyses were included in the multivariable analyses.
P values less than 0.05 were considered statistically significant, and analyses were conducted using R software version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Among 94 patients enrolled in the prospective registry from June to August 2022, 69 patients met the inclusion criteria. The remaining 25 patients were excluded as they were discharged before 48 hours postoperatively (n = 16), not present even after several visits for follow-up assessment (n = 5), or underwent thoracotomy (n = 3) or VATS lobectomy with en-bloc chest wall resection (n = 1). Among 90 patients registered in the previous RCT data, a total of 68 patients completed the QoR-15K questionnaire at 48 hours postoperatively and were included in the study. Therefore, a total of 137 patients were included in this study for analyses. Demographics and perioperative characteristics are presented in Table 1. Table 2 presents the postoperative outcomes related to postoperative recovery. There were 11 patients for whom IV-PCA was discontinued due to opioid-related side effects (n = 9) or patient’s refusal (n = 2) within 24 hours postoperatively, and in an additional 12 patients, IV-PCA was discontinued for 24–48 hours postoperatively. In addition, one patient underwent emergency re-operation during the hospitalization period due to postoperative bleeding, and one patient died during the hospitalization period due to postoperative acute respiratory distress syndrome. Six patients had unplanned readmission within 30 days postoperatively (wound problem, n = 4; unknown fever, n = 1; and voiding problem, n = 1).
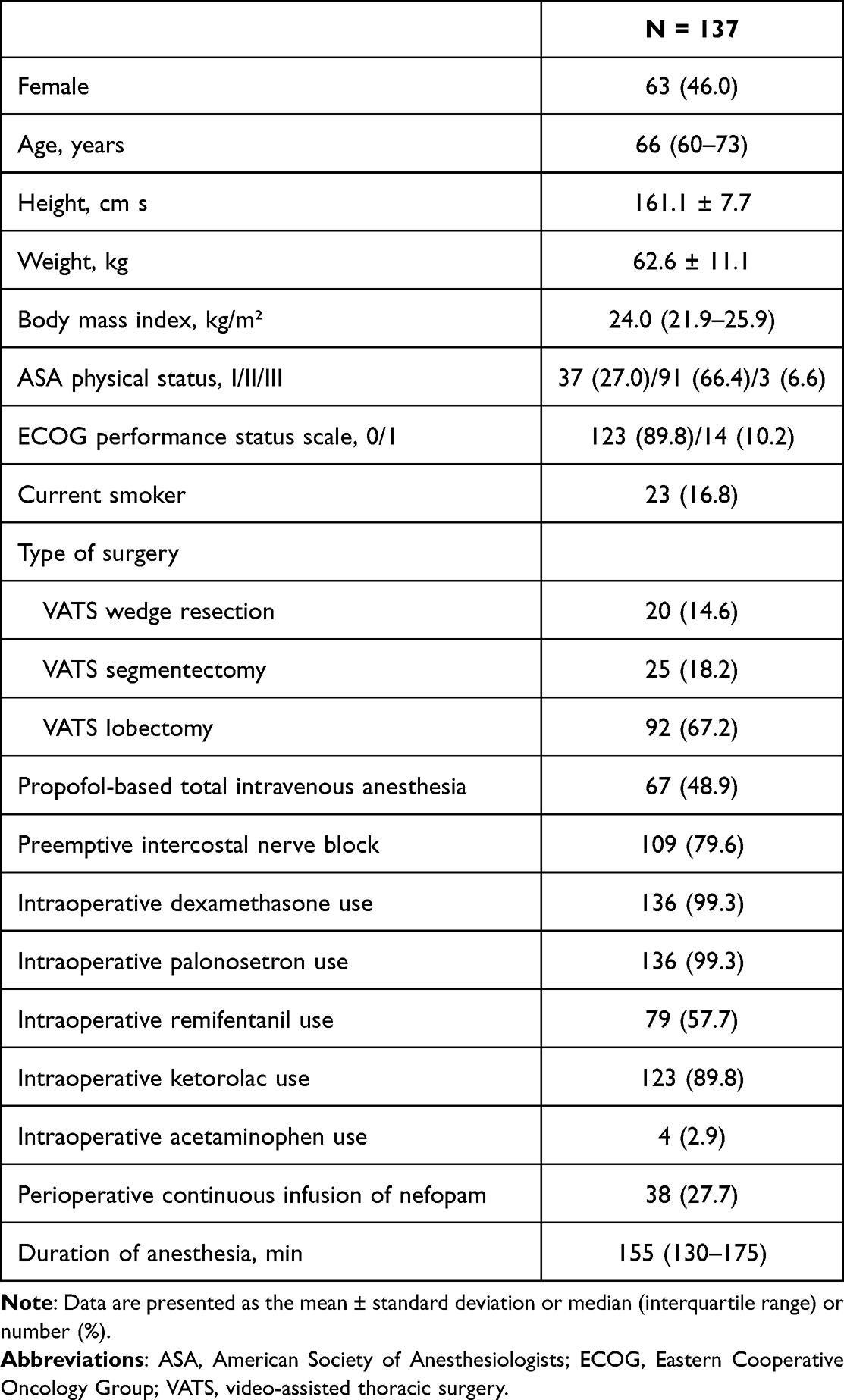 |
Table 1 Patient Demographics and Clinical Characteristics |
 |
Table 2 Postoperative Outcomes Related to Postoperative Recovery |
Changes in the QoR-15K total score and in each item before and 48 hours after surgery are summarized in Table 3. The median total QoR-15K score decreased from 148 (IQR: 142–150) before surgery to 123 (IQR: 108–135) at 48 hours postoperatively (median difference: −23, 95% CI: −26 – −20, P < 0.001; Table 3). Among all items of the postoperative QoR-15K questionnaire, the 11th item (moderate pain) showed the lowest median score and highest median difference between pre- and postoperative scores (median difference: 5, 95% CI: −5 – −4). Changes in the dimensions of the QoR-15K score before and 48 hours after surgery are summarized in Table 4.
 |
Table 3 Changes in the Korean Version of the Quality of Recovery-15 (QoR-15K) Questionnaire Scores Before and 48 Hours After Surgery |
 |
Table 4 Changes in the Dimensions of the Korean Version of Quality of Recovery-15 (QoR-15K) Before and 48 Hours After Surgery |
The inter-dimension correlations of the postoperative QoR-15K score and postoperative pain severity at 48 hours postoperatively are presented in Table 5. The QoR-15K score showed significant negative correlations with pain intensity at rest (ρ = −0.45, 95% CI: −0.57 – −0.31, P < 0.001) and during coughing at 48 hours postoperatively (ρ = −0.55, 95% CI: −0.65 – −0.42, P < 0.001). The pain dimension of the QoR-15K showed a significant correlation with the emotional state, physical comfort, and physical independence dimensions of the QoR-15K as well as pain intensity at rest and during coughing at 48 hours postoperatively.
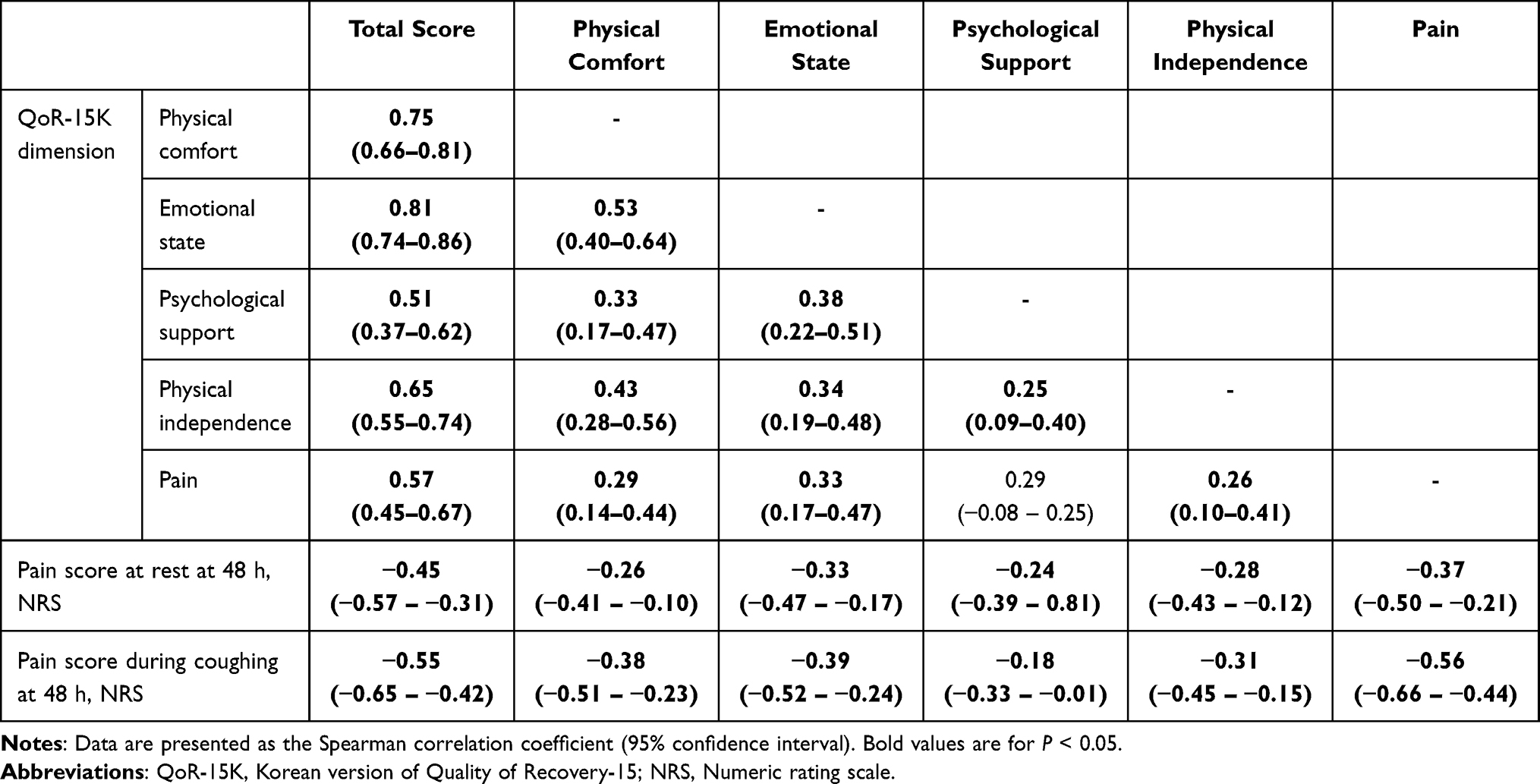 |
Table 5 Inter-Dimension Correlations of Postoperative Pain Intensity and Postoperative QoR-15K Scores |
Table 6 presents the results of the multivariable logistic regression analyses of good or excellent postoperative recovery at 48 hours postoperatively. Multivariable logistic regression analyses revealed that a preoperative QoR-15K score lower than 136 (OR [odds ratio]: 0.28, 95% CI: 0.09–0.83, P = 0.022), pain score during coughing at 24 hours postoperatively (OR: 0.82, 95% CI: 0.69–0.96, P = 0.016), and PONV during the first 24 hours postoperatively (OR: 0.35, 95% CI: 0.16–0.73, P = 0.005) were negatively associated with a good or excellent postoperative recovery.
 |
Table 6 Logistic Regression Analyses for Good or Excellent Postoperative Recovery at 48 Hours Postoperatively |
Discussion
In the present study, a significant negative correlation was found between pain intensity and quality of postoperative recovery, evaluated using the QoR-15K questionnaire at 48 hours postoperatively in patients who underwent VATS for lung cancer resection. The pain dimension of the QoR-15K assessment and postoperative pain score showed significant negative correlations with the other dimensions of the QoR-15K assessment, except for the psychological support dimension, which suggested that postoperative pain affected various aspects of postoperative recovery. Among all items of the QoR-15K questionnaire, the item with the lowest median score at 48 hours postoperatively was the 11th item (moderate pain). In addition, the pain score during coughing at 24 hours postoperatively showed a significant association with poor postoperative recovery, along with PONV and a low preoperative QoR-15K score. Therefore, in these patients, postoperative pain management appeared to be the most important perioperative component in improving postoperative recovery.
The major goal of postoperative pain management is not to eliminate pain, but to improve postoperative recovery by providing physical comfort that will not interfere with postoperative rehabilitation, such as ambulation. From this point of view, the quality of postoperative recovery would be more appropriate than pain intensity as the primary outcome in clinical studies on postoperative pain intervention. The assessment of the postoperative quality of recovery can evaluate not only the effect of analgesic interventions on postoperative pain intensity but also the overall improvement in postoperative recovery, including improvements in physical and psychosocial functions. Therefore, recently, several studies that used quality of postoperative recovery, rather than pain intensity, as the primary outcome have been reported.22–28 As the importance of using patient-reported outcome assessments such as the QoR-15 questionnaire in surgical patients is emphasized,29,30 the number of clinical studies on postoperative pain using the QoR-15 score as the primary endpoint is increasing.31
Postoperative recovery evaluated using the QoR questionnaire can provide more meaningful clinical information than that obtained using pain intensity scoring. In recent studies regarding the effect of regional analgesia on quality of recovery after breast cancer surgery, despite no significant group difference in pain scores at 24 hours postoperatively, the intervention group showed a higher QoR-15 score than that of the control group at 24 hours postoperatively.23,25 The following points may explain the results. First, the pain-related items of the QoR-15 questionnaire assess the condition over the past 24 hours, not the pain intensity at a specific time point. In the present study, the QoR-15K score showed a significant correlation with postoperative pain intensity, but it was only of a mild to moderate degree. Second, the decrease in opioid-induced side effects due to a decrease in postoperative opioid consumption over the previous 24 hours would have contributed to improvement in the overall quality of recovery. Last, the decrease in pain intensity over the previous 24 hours might have affected other dimensions as well as the pain dimension in the QoR-15 questionnaire assessment. In the present study, both the pain dimension of the QoR-15K questionnaire and pain score showed significant correlations with the emotional state, physical comfort, and physical independence dimensions of the QoR-15K questionnaire. Similarly, in a study regarding the effect of regional analgesia on quality of recovery after thoracic surgery, the significant decrease in pain scores up to eight hours postoperatively correlated with a significant difference in postoperative recovery at 48 hours postoperatively.24 This result can suggest that pain control during the immediate postoperative period is important for overall postoperative recovery during hospitalization.
Despite their significant correlation, the significance degree of correlation between pain intensity and QoR-15K score was moderate. This result might be because the quality of postoperative recovery was influenced by various factors, including postoperative pain. More specifically, in the present study, the emotional dimension of the QoR-15K questionnaire showed a strong correlation with the total score and pain dimension of the QoR-15K questionnaire, which was similar to the result of a previous study.32 In addition, in the present study, despite administration of dual prophylaxis for PONV in most patients, PONV occurred in a significant number of patients, which would have affected the QoR-15K total score, as well as the physical comfort dimension. Therefore, in clinical studies regarding the effect of pain intervention on postoperative recovery in a sample of modest size, control of these confounding variables should be considered.
Caution should be employed when interpreting the results of this study for the following reasons. First, this study has limited generalizability due to its retrospective design, which included a small number of patients who underwent a single type of surgery at a single institution. Differences in perioperative management depending on the type of surgery or institution may affect the primary outcome. Additionally, the degree of pain can vary depending on the type of surgery; therefore, the contribution of postoperative pain to overall postoperative recovery may also differ. Second, no gold standard for evaluating the quality of postoperative recovery exists. In the previous study on the validity of the QoR-15K questionnaire, the correlation between the QoR-15K score and QoR visual analog scale score was of a moderate to strong degree (r = 0.61; 95% CI, 0.51–0.69; P < 0.0001).2 However, the QoR-15 questionnaire assessment was the first patient-reported outcome measurement in surgical patients, the validity of which was verified according to a strict statistical process.6 Third, we routinely conducted the QoR-15K questionnaire only at 48 hours postoperatively due to the lack of personnel to conduct more assessments. Changes in the QoR-15 score over time after surgery may provide more valuable information on postoperative recovery.28 Lastly, we have not investigated the quality of postoperative recovery after discharge. The association between acute and chronic postoperative pain is well known,33 but so far, the impact of acute postoperative pain on the overall quality of postoperative recovery after discharge has not been reported. Especially in thoracic surgery, chronic postoperative pain occurs relatively frequently, and this can impair the long-term quality of life after surgery. Therefore, further research is needed regarding the impact of acute pain on the quality of both early and long-term recovery after surgery.
Conclusion
In conclusion, the QoR-15K score at 48 hours postoperatively showed a significant negative correlation with pain intensity at 48 hours postoperatively in patients who underwent VATS for lung cancer resection. In addition, both pain intensity and the pain dimension of the QoR-15K questionnaire showed significant correlations with other dimensions of the QoR-15K questionnaire in these patients. These results further demonstrate the impact of postoperative pain on overall postoperative recovery in patients who underwent VATS for lung cancer resection. Considering the significant correlation between the postoperative pain intensity and QoR-15K score, the QoR-15K score may be regarded as a primary endpoint in clinical studies on postoperative pain control. However, our study had several limitations that hinder the generalization of our conclusions, and further research will be needed on this subject, with a more diverse range of surgeries and a larger patient population.
Acknowledgments
We have obtained the permission from Anesthesiology, which owns the copyright of the original version of the QoR-15. The authors thank Editage for the English language editing.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rajabiyazdi F, Alam R, Pal A, et al. Understanding the meaning of recovery to patients undergoing abdominal surgery. JAMA Surg. 2021;156(8):758–765. doi:10.1001/jamasurg.2021.1557
2. Yoon S, Joo H, Oh YM, Lee J, Bahk JH, Lee HJ. Validation and clinical utility of the Korean version of the quality of recovery-15 with enhanced recovery after surgery: a prospective observational cohort study. Br J Anaesth. 2020;125(4):614–621. doi:10.1016/j.bja.2020.06.040
3. Abola RE, Bennett-Guerrero E, Kent ML, et al. American Society for enhanced recovery and perioperative quality initiative joint consensus statement on patient-reported outcomes in an enhanced recovery pathway. Anesth Analg. 2018;126(6):1874–1882. doi:10.1213/ANE.0000000000002758
4. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
5. Myles PS, Boney O, Botti M, et al. Systematic review and consensus definitions for the Standardised Endpoints in Perioperative Medicine (StEP) initiative: patient comfort. Br J Anaesth. 2018;120(4):705–711. doi:10.1016/j.bja.2017.12.037
6. Kleif J, Waage J, Christensen KB, Gögenur I. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anaesth. 2018;120(1):28–36. doi:10.1016/j.bja.2017.11.013
7. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
8. Wu CL, Richman JM. Postoperative pain and quality of recovery. Curr Opin Anaesthesiol. 2004;17(5):455–460. doi:10.1097/00001503-200410000-00017
9. Van Boekel RLM, Warlé MC, Nielen RGC, et al. Relationship between postoperative pain and overall 30-day complications in a broad surgical population: an observational study. Ann Surg. 2019;269(5):856–865. doi:10.1097/SLA.0000000000002583
10. Oliver CM, Warnakulasuriya S, McGuckin D, et al. Delivery of drinking, eating and mobilising (DrEaMing) and its association with length of hospital stay after major noncardiac surgery: observational cohort study. Br J Anaesth. 2022;129(1):114–126. doi:10.1016/j.bja.2022.03.021
11. Rivas E, Cohen B, Pu X, et al. Pain and opioid consumption and mobilization after surgery: post hoc analysis of two randomized trials. Anesthesiology. 2022;136(1):115–126. doi:10.1097/ALN.0000000000004037
12. Yoon S, Hong WP, Joo H, et al. Long-term incidence of chronic postsurgical pain after thoracic surgery for lung cancer: a 10-year single-center retrospective study. Reg Anesth Pain Med. 2020;45(5):331–336. doi:10.1136/rapm-2020-101292
13. Kehlet H. Postoperative pain, analgesia, and recovery-bedfellows that cannot be ignored. Pain. 2018;159(suppl 1):S11–S16. doi:10.1097/j.pain.0000000000001243
14. Wu CL, Rowlingson AJ, Partin AW, et al. Correlation of postoperative pain to quality of recovery in the immediate postoperative period. Reg Anesth Pain Med. 2005;30(6):516–522. doi:10.1016/j.rapm.2005.07.190
15. Hill J, Ashken T, West S, et al. Core outcome set for peripheral regional anesthesia research: a systematic review and Delphi study. Reg Anesth Pain Med. 2022;47(11):691–697. doi:10.1136/rapm-2022-103751
16. Yoon S, Lee HB, Na KJ, Park S, Bahk J, Lee HJ. Effect of continuous infusion of intravenous nefopam on postoperative opioid consumption after video-assisted thoracic surgery: a double-blind randomized controlled trial. Pain Phys. 2022;25(6):491–500.
17. Jung H, Lee KH, Jeong Y, et al. Effect of fentanyl-based intravenous patient-controlled analgesia with and without basal infusion on postoperative opioid consumption and opioid-related side effects: a retrospective cohort study. J Pain Res. 2020;13:3095–3106. doi:10.2147/JPR.S281041
18. Clavien PA, Barkun J, De Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
19. Kleif J, Gögenur I. Severity classification of the quality of recovery-15 score-An observational study. J Surg Res. 2018;225:101–107. doi:10.1016/j.jss.2017.12.040
20. Srikandarajah S, Gilron I. Systematic review of movement-evoked pain versus pain at rest in postsurgical clinical trials and meta-analyses: a fundamental distinction requiring standardized measurement. Pain. 2011;152(8):1734–1739. doi:10.1016/j.pain.2011.02.008
21. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118:1332–1340.
22. Abdallah FW, Patel V, Madjdpour C, Cil T, Brull R. Quality of recovery scores in deep serratus anterior plane block vs. sham block in ambulatory breast cancer surgery: a randomised controlled trial. Anaesthesia. 2021;76(9):1190–1197. doi:10.1111/anae.15373
23. Yao Y, Li H, He Q, Chen T, Wang Y, Zheng X. Efficacy of ultrasound-guided erector spinae plane block on postoperative quality of recovery and analgesia after modified radical mastectomy: randomized controlled trial. Reg Anesth Pain Med. 2020;45(1):5–9. doi:10.1136/rapm-2019-100983
24. Yao Y, Fu S, Dai S, et al. Impact of ultrasound-guided erector spinae plane block on postoperative quality of recovery in video-assisted thoracic surgery: a prospective, randomized, controlled trial. J Clin Anesth. 2020;63:109783. doi:10.1016/j.jclinane.2020.109783
25. Yao Y, Li J, Hu H, Xu T, Chen Y. Ultrasound-guided serratus plane block enhances pain relief and quality of recovery after breast cancer surgery: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(6):436–441. doi:10.1097/EJA.0000000000001004
26. Kim DH, Oh YJ, Lee JG, Ha D, Chang YJ, Kwak HJ. Efficacy of ultrasound-guided serratus plane block on postoperative quality of recovery and analgesia after video-assisted thoracic surgery: a randomized, triple-blind, placebo-controlled study. Anesth Analg. 2018;126(4):1353–1361. doi:10.1213/ANE.0000000000002779
27. Yao Y, Jiang J, Lin W, Yu Y, Guo Y, Zheng X. Efficacy of systemic lidocaine on postoperative quality of recovery and analgesia after video-assisted thoracic surgery: a randomized controlled trial. J Clin Anesth. 2021;71:110223. doi:10.1016/j.jclinane.2021.110223
28. Yoon HK, Joo S, Yoon S, Seo JH, Kim WH, Lee HJ. Randomized controlled trial of the effect of general anesthetics on postoperative recovery after minimally invasive nephrectomy. Korean J Anesthesiol. 2023. doi:10.4097/kja.23083
29. Medbery RL, Fernandez FG, Khullar OV. ERAS and patient reported outcomes in thoracic surgery: a review of current data. J Thorac Dis. 2019;11(suppl 7):S976–S986. doi:10.21037/jtd.2019.04.08
30. Kingsley C, Patel S. Patient-reported outcome measures and patient-reported experience measures. BJA Educ. 2017;17(4):137–144. doi:10.1093/bjaed/mkw060
31. Léger M, Campfort M, Cayla C, Lasocki S, Rineau E. Postoperative quality of recovery measurements as endpoints in comparative anaesthesia studies: a systematic review. Br J Anaesth. 2021;126(6):e210–e212. doi:10.1016/j.bja.2021.03.008
32. Gümüs K. The effects of preoperative and postoperative anxiety on the quality of recovery in patients undergoing abdominal surgery. J Perianesth Nurs. 2021;36(2):174–178. doi:10.1016/j.jopan.2020.08.016
33. Kim BR, Yoon SH, Lee HJ. Practical strategies for the prevention and management of chronic postsurgical pain. Korean J Pain. 2023;36(2):149–162. doi:10.3344/kjp.23080
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dexmedetomidine and Dexamethasone as Adjuvants to the Local Anesthetic Mixture in Rhomboid Intercostal and Sub-Serratus Block for Video-Assisted Thoracoscopic Surgery: A Randomized, Double-Blind, Controlled Trial
Liu QF, Shi CN, Tong JH, Li KP, Yang JJ, Ji MH, Liu QR
Drug Design, Development and Therapy 2024, 18:4485-4496
Published Date: 7 October 2024
Predictive Clinical Factors of Pain-Related Quality of Recovery Following Elective Gastrointestinal and Hepato-Pancreato-Biliary Surgery: An Observational Study in Norway
Bergestuen L, Hagen M, Kisa S
Journal of Pain Research 2025, 18:47-59
Published Date: 8 January 2025
Effect of Thoracic Paravertebral Block on Postoperative Pulmonary Complications After Video-Assisted Thoracoscopic Surgery: A Dual-Center Randomized Clinical Trial
Zhu J, Wei B, Wu L, Li H, Zhang Y, Lu J, Su S, Xi C, Liu W, Wang G
Therapeutics and Clinical Risk Management 2025, 21:691-703
Published Date: 15 May 2025
Quadratus Lumborum Block for Pain Management After Colorectal Surgery: Systematic Review and Meta-Analysis of Analgesic and Opioid-Sparing Effects
Han C, Wang Y, Tan H
Journal of Pain Research 2025, 18:5827-5841
Published Date: 3 November 2025
Perioperative Ketamine Exposure and Postoperative Atrial Fibrillation/Flutter Risk After Video-Assisted Thoracoscopic Surgery: A Multi-Institutional Study
Hung KC, Yu TS, Lai YC, Yu CH, Wu JY, Tsai WW, Chen IW
Drug Design, Development and Therapy 2025, 19:11173-11185
Published Date: 16 December 2025