Back to Journals » International Journal of General Medicine » Volume 16
Correlation Between Lipoprotein-Related Phospholipase A2 and Metabolic Syndrome
Authors Wang KY ![]() , Chen YC, Chen JY, Loke SS
, Chen YC, Chen JY, Loke SS ![]() , Yeh WC, Li WC
, Yeh WC, Li WC
Received 27 August 2023
Accepted for publication 15 December 2023
Published 22 December 2023 Volume 2023:16 Pages 6041—6049
DOI https://doi.org/10.2147/IJGM.S437397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Kai-Yu Wang,1 Yi-Chuan Chen,1,2 Jau-Yuan Chen,1,2 Song-Seng Loke,3 Wei-Chung Yeh,4 Wen-Cheng Li1,2,5
1Department of Family Medicine, Chang-Gung Memorial Hospital at Linkou, Taoyuan, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Department of Family Medicine, Chang-Gung Memorial Hospital at Kaohsiung, Kaohsiung, Taiwan; 4Department of Family Medicine, Chang-Gung Memorial Hospital at Keelung, Keelung, Taiwan; 5Department of Health Management, Xiamen Chang-Gung Hospital, Xiamen, People’s Republic of China
Correspondence: Wen-Cheng Li, Email [email protected]
Background: Lipoprotein-associated phospholipase A2 (Lp-PLA2) has been recognized as a valuable biomarker for identifying the risk of cardiovascular diseases and inflammation. Furthermore, there is strong evidence to suggest that metabolic syndrome is closely associated with chronic inflammation. Accordingly, the present study endeavors to examine the potential correlation between metabolic syndrome and the levels of Lp-PLA2.
Methods: To explore the relationship between Lp-PLA2 levels and metabolic syndrome, and to establish the predictive cut-off value of Lp-PLA2, a retrospective analysis was conducted using medical data from a sample of 3549 Chinese adults (comprising 2182 men and 1367 women) aged between 18 and 50 years, who had undergone health check-ups. In addition, the study also sought to investigate any potential differences in Lp-PLA2 levels based on sex and age.
Results: The analysis of the data indicated that participants had a mean age of 44.2 years, a mean Lp-PLA2 level of 589 IU/L, and a metabolic syndrome prevalence of 22%. Lp-PLA2 levels were significantly different between males and females, and a significant correlation was observed between Lp-PLA2 levels and clinical and metabolic characteristics, including BMI, cholesterol, and triglycerides. Interestingly, Lp-PLA2 demonstrated potential as an indicator of metabolic syndrome, particularly in females, despite other biomarkers, such as TG/HDL-C and WHR, exhibiting better area under the curve.
Conclusion: Our findings suggest that Lp-PLA2 may serve as a useful biomarker for identifying individuals at risk of developing metabolic syndrome, particularly in females. Further research is needed to explore the potential of Lp-PLA2 as a diagnostic and therapeutic target for metabolic syndrome.
Keywords: Lp-PLA2, lipoprotein, metabolic syndrome, cardiovascular risk, and lipid profile
Introduction
Lp-PLA2 was first discussed in the 1980s, and the study focused on whether the activity of Lp-PLA2 influences the peroxidation and degradation of low-density lipoprotein (LDL).1 The scientists then discovered that Lp-PLA2 played a crucial role in cardiovascular disease. According to Brilakis et al, study, it indicated that the mean Lp-PLA2 levels are related to LDL, high-density lipoprotein (HDL), total cholesterol, fibrinogen, and creatinine, and also correlated with coronary artery disease (CAD) with major adverse events. Lp-PLA2 was seen as another independent marker of CAD apart from C-reactive protein (CRP).2
Lp-PLA2 has two major functions on humans. Firstly, it has an antioxidant function. Lp-PLA2 is secreted by macrophages, mast cells, and T cells in the inner layer of the blood vessel wall, and it exists with LDL in the blood. When the body is under oxidative stress to induce LDL partial oxidization, Lp-PLA2 can hydrolyze its oxidative part. Secondly, its inflammation-activating effect is well established. Macrophages, mast cells, and T cells will secret more Lp-PLA2 under oxidative stress since larger spaces between endothelial cells make them migrate to the tunica intima. Besides, the macrophage in the intima will engulf oxidized LDL and turn into foam cells, which stimulates plaque growth and elevates the likelihood of a cardiovascular event.3 In short, Lp-PLA2 has a distinct correlation with the inflammation state.
Metabolic syndrome also has a known relationship with inflammation. With the prevalence of modern lifestyles and unhealthy eating habits, metabolic syndrome has become a major public health concern. In addition to cardiovascular disease and diabetes, metabolic syndrome is also fingered in the occurrence of chronic organ diseases, such as polycystic ovary and nonalcoholic fatty liver disease. Furthermore, individuals with metabolic syndrome typically experience metabolic overload, leading to heightened production of reactive oxygen species and inflammatory cytokines, ultimately subjecting the body to oxidative stress.4 This also induces adipocyte hypertrophy and macrophage accumulation to ameliorate the inflammatory state by increasing the level of insulin resistance.5
Therefore, in this study, we hope to explore the feasibility of Lp-PLA2 as a predictor of metabolic syndrome by analyzing the correlation between metabolic syndrome risk factors and Lp-PLA2 in the physical examination population. Also, we will estimate the cut-off value of Lp-PLA2 in high-risk metabolic syndrome populations (the presence of ≥3 risk factors for metabolic syndrome) to provide efficacious health management and alleviate the harm and deterioration in patients with metabolic syndrome.
Method
We retrospectively collected the medical records of Chinese adults (aged between 18 and 55 years) who underwent health examinations between 2018 and 2019 at the Xiamen Chang Gung Hospital. Subjects were excluded if they were affected by any of the following exclusion criteria: (1) with pregnancy (2) who were not fasting for more than 12 hours (3) who had medication for hypertension and /or hyperlipidemia control (4) who had chronic thyroid disease, thyroidectomy or chronic liver disease; and (5) whose data were incomplete.
A total of 2182 men and 1367 women were included in the analysis. After all the subjects provided informed consent, they were subjected to anthropometric and biochemical measurements for clinical data collection, which included body height, body weight, waist circumstance, blood pressure, fasting glucose, total cholesterol, triglyceride (TG), LDL, and HDL.
Laboratory Measurements
The clinical chemistry examination encompassed several measurements, including fasting blood glucose (FBG) assessed via Hexokinase enzyme assay using the Cobas Mira Chemistry System manufactured by Roche Diagnostic Systems, Montclair, NJ. Additional measurements were taken by an automatic biochemical analyzer (DxC 800, Beckman CoulterUniCel® DxC SYNCHRON®, Ireland) to assess total cholesterol, LDL, HDL, and TG. Furthermore, measurements were made to determine levels of Lp-PLA2, using a quantitative test through turbidimetric immunology (ABBOTT ARCHITECT c8000/c16000). Anthropometric measures were taken to determine body weight and height using calibrated scales and meters, respectively. The body mass index (BMI) was estimated utilizing the formula: body weight (kg)/ [height (m)]2. The waist circumference was measured between the lowest rib and the midpoint of the iliac crest. Blood pressure was measured after a 15-minute rest, and the subject was seated using an automated sphygmomanometer on the right arm. The mean arterial pressure was calculated using the formula: (2/3) × diastolic pressure + (1/3) × systolic pressure. Diabetes mellitus was defined as fasting glucose ≥ 7.0 mmol/L. Metabolic syndrome (MetS) was defined as subjects who exhibited three or more of the following criteria: (1) waist circumference ≥ 90 cm in men and ≥ 80 cm in women; (2) hypertriglyceridemia: TG ≥ 1.7 mmol/L (3) low HDL level < 1.03 mmol/L in men and < 1.29 mmol/L in women; (4) blood pressure ≥ 130/85 mmHg; and (5) fasting glucose ≥ 5.6 mmol/L.6
Statistical Analysis
At the outset of our data collection, we utilized Quantile-Quantile plots (Q-Q plots) for a visual assessment of the quantitative variable’s conformity to a normal distribution. The distinctive bell-shaped curve associated with a normal distribution became apparent in our analysis. Consequently, given the confirmation of a normal distribution in the dataset, we opted for the mean and standard deviation as our preferred measures of central tendency. This choice was motivated by their sensitivity to extreme values, aligning well with the characteristics of our data.
Prior research examined the connection between LDL and Lp-PLA2 levels in individuals with type 2 diabetes and found that the standardized regression coefficient of LDL was 0.11. To achieve a type I error of 1% and a power of 99%, a minimum sample size of 1966 was necessary based on the effect size observed.3
We conducted a comparison of basic characteristics between male and female subjects, including continuous and categorical variables, using an independent sample t-test and chi-square test, respectively. Additionally, we analyzed the relationship between Lp-PLA2 levels and comorbidities such as hypertension, diabetes, MetS, and lipid profile, using an independent sample t-test and stratifying by sex. Pairwise comparisons were conducted using the Bonferroni adjustment if the overall test was significant. Subsequently, the study compared Lp-PLA2 levels using a logistic regression model, adjusting for age and age plus BMI subgroups. Lastly, ROC curves for TG/HDL-C, Waist-to-height ratio (WHtR), and Lp-PLA2 were done for the cut-off point value and prediction power evaluation. All tests were two-tailed, and a significance level of p < 0.05 was set. The data analyses were conducted using SPSS 25 (IBM SPSS Inc., Chicago, IL, USA).
Result
A total of 3549 participants were included in the final analysis. 2182 of these participants were male. Their average age was 44.2 years. The average Lp-PLA2 level was 589 IU/L. Approximately 4.5% of the subjects were diagnosed with diabetes, and 22% already manifested MetS. Table 1 lists the basic characteristics, including cardiometabolic risk factors. The mean Lp-PLA2 level in men and women were 621.45 ± 158.56 IU/L and 537.92 ± 141.33 IU/L respectively. A significant difference of Lp-PLA2 was noted with a p-value < 0.05 among men and women respectively, similar to other factors listed in Table 1.
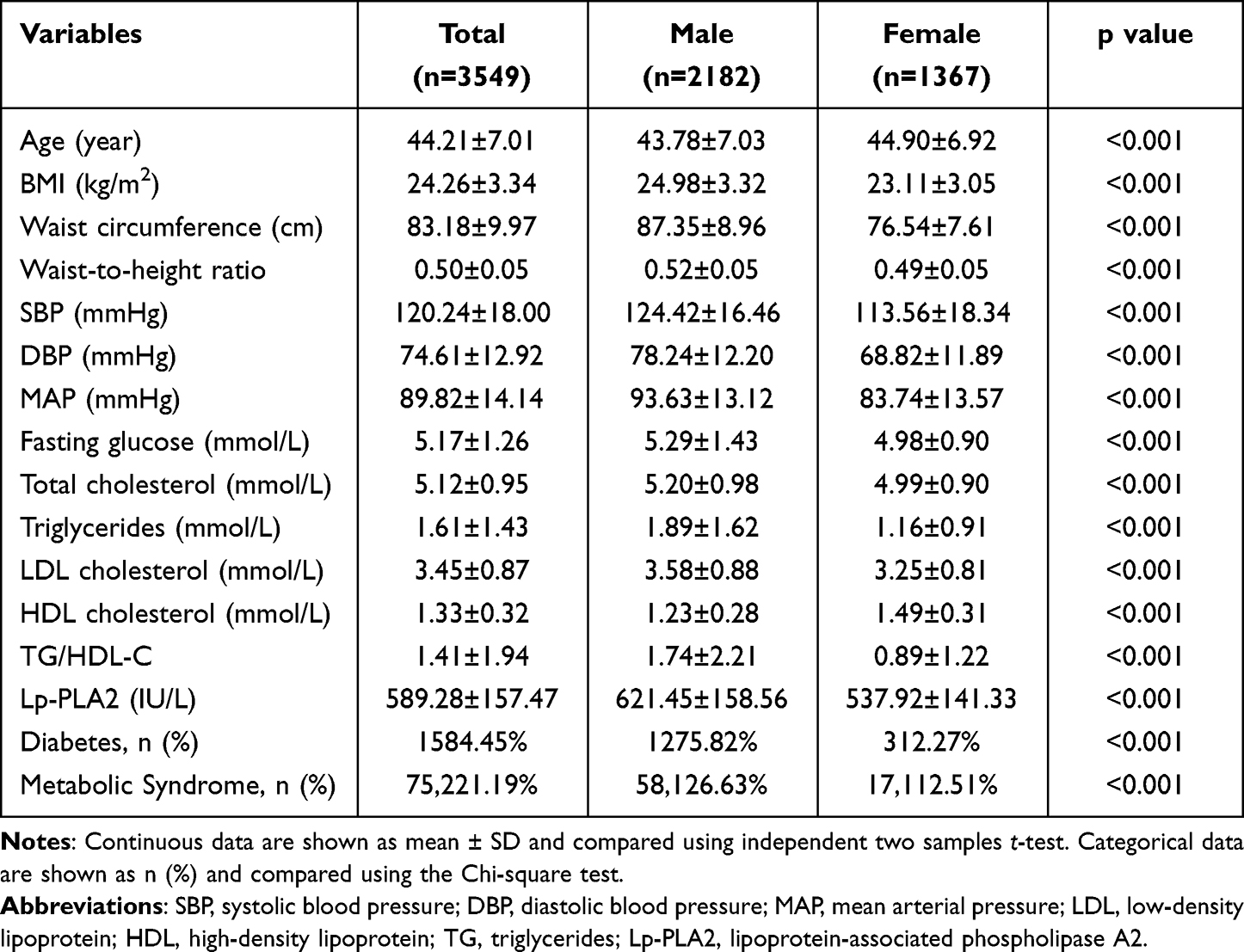 |
Table 1 Basic Characteristics of the Study Subjects |
Table 2 presents the findings regarding the associations between the Lp-PLA2 level (a continuous variable) and clinical/metabolic characteristics, stratified by gender. The results revealed that in both men and women, BMI, waist circumference, waist-to-height ratio, total cholesterol, triglycerides, HDL, LDL, and TG/HDL-C were significantly associated with Lp-PLA2 levels (p < 0.05). Furthermore, in men, SBP, DBP, and MAP demonstrated significant correlations with Lp-PLA2 (p < 0.05), while in women, fasting glucose presented a significant correlation with Lp-PLA2 (p < 0.05).
 |
Table 2 Pearson’s Correlation Coefficients Between Lp-PLA2 Levels and Cardiometabolic Risk Factors in Men and Women |
To examine whether there existed an association between particular characteristics and Lp-PLA2 levels, we stratified our sample into tertiles and conducted Pearson’s correlation analysis (as shown in Table 3). The findings indicate a statistically significant linear trend across all characteristics within the ordinal subgroups that were based on Lp-PLA2 levels (P < 0.05). Specifically, the prevalence of MetS among women demonstrated a rising trend as Lp-PLA2 levels increased, with rates of 9.78%, 10.55%, and 17.26% in the first, second, and third tertiles, respectively (P < 0.05).
 |
Table 3 Clinical and Metabolic Characteristics According to Lp-PLA2 Status |
To further confirm this observation, we conducted regression analyses (as presented in Table 4), with age and BMI as covariates. The results indicated that only in the female group did Lp-PLA2 exhibit a significant p-value (p < 0.05) after adjusting for age and BMI, reinforcing its potential as an indicator of MetS in this subgroup.
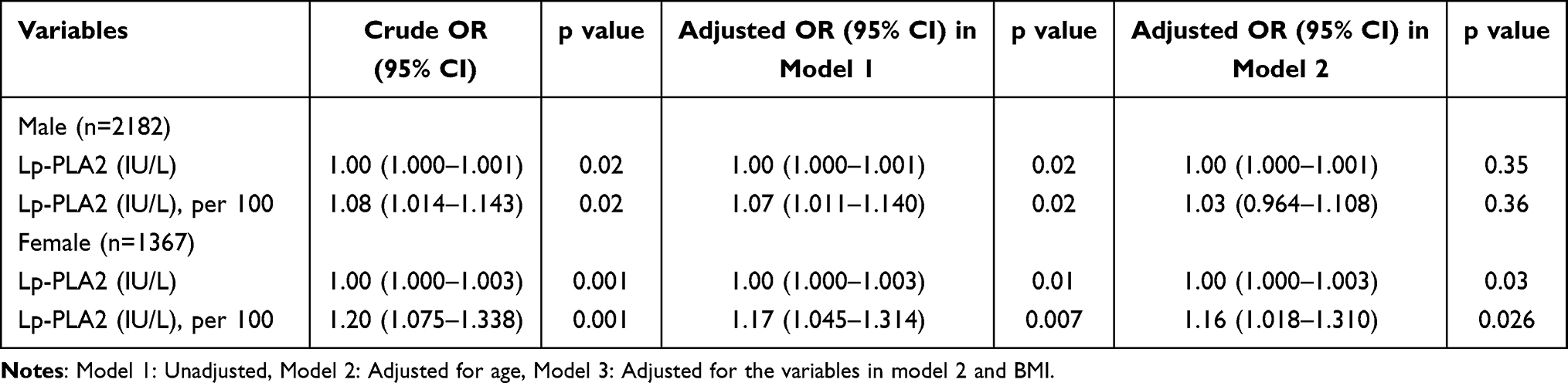 |
Table 4 Logistic Regression Analysis of Lp-PLA2 Level and Metabolic Syndrome |
Table 5 and Figure 1 present the ROC curves for three biomarkers: TG/HDL-C, waist-to-height ratio (WHtR), and Lp-PLA2, stratified by gender. In males, the results demonstrated that TG/HDL-C had a C-value of 0.86 (95% CI: 0.84–0.88), WHtR had a C value of 0.84 (95% CI: 0.82–0.86), and Lp-PLA2 had a C value of 0.53 (95% CI: 0.50–0.56). In females, the results indicated that TG/HDL-C had a C value of 0.93 (95% CI: 0.91–0.95), WHtR had a C value of 0.87 (95% CI: 0.84–0.89), and Lp-PLA2 had a C value of 0.59 (95% CI: 0.54–0.64). These findings suggest that although TG/HDL-C and WHR demonstrated better area under the curve, Lp-PLA2 may still have the potential to serve as an indicator of MetS, particularly among females.
 |
Table 5 Cut-off Value and Prediction Power for TG/HDL-C, Waist-to-Height Ratio (WHtR), and Lipoprotein-Associated Phospholipase A2 (Lp-PLA2) |
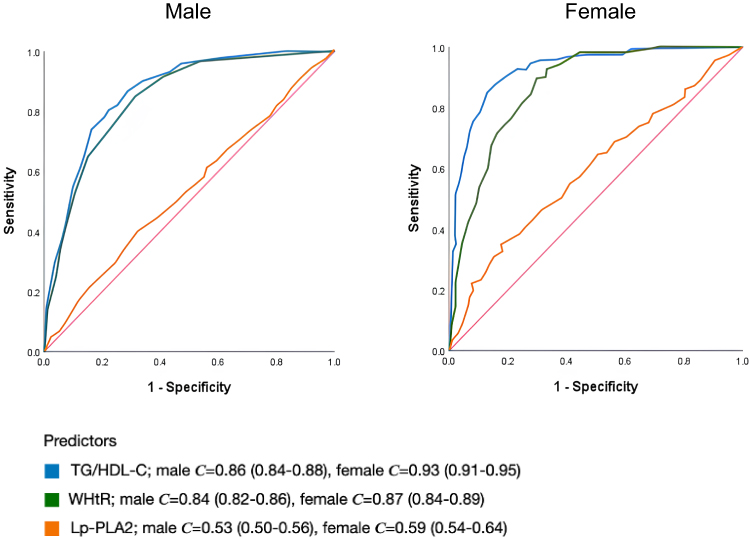 |
Figure 1 ROC curves assessing diagnostic performance of TG/HDL-C, WHtR, and Lp-PLA2 Stratified by Gender. ROC curves illustrate the discriminatory ability of TG/HDL-C, WHtR, and Lp-PLA2 for predicting Mets, with gender-specific analysis. In males, TG/HDL-C (C = 0.86, 95% CI: 0.84–0.88) and WHtR (C = 0.84, 95% CI: 0.82–0.86) showed strong performance, while Lp-PLA2 had lower discrimination (C = 0.53, 95% CI: 0.50–0.56). Among females, TG/HDL-C excelled (C = 0.93, 95% CI: 0.91–0.95), surpassing WHtR (C = 0.87, 95% CI: 0.84–0.89). Lp-PLA2 exhibited weaker discrimination (C = 0.59, 95% CI: 0.54–0.64). These findings highlight gender-specific variations in biomarker efficacy for Mets diagnosis, emphasizing the need for gender-specific analyses. |
Discussion
In this cross-sectional study, we aimed to investigate the association between Lp-PLA2 and MetS in a Chinese population. The study included a sample of 2182 men and 1367 women. Our findings indicate a significant correlation between Lp-PLA2 levels and risk factors for MetS, including BMI, WHtR, total cholesterol, LDL, and HDL, particularly in the female cohort. Additionally, after adjusting for age and BMI, we observed a significant association between Lp-PLA2 levels and MetS in females, with a cut-off value of 626.5. These results suggest that Lp-PLA2 could potentially serve as a biomarker for identifying and preventing MetS in females. The findings of this study are of great significance to healthcare professionals and policymakers, as they provide valuable insights for developing targeted prevention and treatment strategies for MetS.
Our study aimed to investigate the potential of Lp-PLA2 level as a biomarker of MetS across different age groups. For the concern of clinical practice and hormone alternation, we categorized the participants by age for screening the possible MetS disease. In our findings, total cholesterol and LDL were significantly related to Lp-PLA2 and exhibited a trend as Lp-PLA2 increased regardless of age. This result revealed the theory that LP-PLA2 coexists with LDL in the blood and the LDL level is strongly correlated with total cholesterol.5 Moreover, in Jabor et al research, there was also a strong correlation between Lp-PLA2 and LDL within acute coronary syndrome patients or the LDL level after 12 weeks of recovery. The result implied that LDL may be the major determinant of Lp-PLA2 in serum,6 and it had similar findings to this study.
Aside from total cholesterol and LDL level, other lipid profiles had a significant relationship to Lp-PLA2, including TG and HDL-C. The mechanism may be TG, HDL-C, and Lp-PLA2 production in the human body originating from adipose tissue.7 This pathway also contributed to atorvastatin intervention within coronary heart disease patients with a reduction of the Lp-PLA2 mass by 26%.8 In our study, TG to HDL ratio was an item of variables in the analyses, and the results all had a significant correlation to Lp-PLA2. According to other related research, a high TG/HDL ratio was related to coronary disease,9 insulin resistance,10 and atherosclerosis.11 Besides, Krawczyk et al had a similar finding as our study that a high TG/HDL ratio had the potential to be the prediction of MetS.12
Furthermore, a significant linear trend was observed between waist circumference, one of the diagnostic criteria, and the Lp-PLA2 level in our study, which aligns with the findings of da Silva et al that revealed a positive correlation between waist circumference and Lp-PLA2 level among adolescents, reflecting the activity of Lp-PLA2.13 Similarly, a study conducted among adults showed a significant association between central obesity, represented by higher waist circumference, and Lp-PLA2 levels.14 Hence, the correlation between waist circumference and Lp-PLA2 level may be applicable to all age groups. Additionally, our study found that WHtR had a significant association with Lp-PLA2 by gender. WHtR has been identified as a predictor of coronary heart disease by Hsieh and Yoshinaga15 and as an obesity-related indicator for hypertension and MetS in Rodrigues et al’s study,16 indirectly supporting the association between Lp-PLA2 and MetS.
Additionally, we analyzed the potential of Lp-PLA2 level as a biomarker of MetS across different genders, considering the scarcity of studies that have examined the association between MetS and Lp-PLA2 levels. A recent investigation sought to address this knowledge gap by recruiting 60 participants with diabetes mellitus and assessing the impact of obesity, lipid profiles, and blood pressure on Lp-PLA2 levels. The findings demonstrated a significant correlation between these factors and Lp-PLA2 levels. Moreover, subgroup analyses revealed a sex-specific difference in the relationship between these variables and Lp-PLA2 levels. Specifically, body fat and mean arterial pressure were found to be more strongly associated with Lp-PLA2 levels in males, while low-density lipoprotein cholesterol and triglycerides were more strongly associated with Lp-PLA2 levels in females.3 This observation is consistent with the findings presented in Table 2 of our study, and suggests that Lp-PLA2 could serve as a potential predictor of MetS in the Asian population.
Besides, regarding the link between Lp-PLA2 and diabetes, Nelson et al presented compelling pathways, indicating that Lp-PLA2 could potentially contribute significantly to the onset of insulin resistance, consequently elevating the risk of type 2 diabetes. One proposed mechanism revolves around the inflammatory activity associated with Lp-PLA2’s hydrolysis of oxidized phospholipids. This process is hypothesized to induce insulin resistance, a key precursor to diabetes. Elevated Lp-PLA2 levels are considered not only as potential markers of heightened adipose tissue inflammation but also as contributors to metabolic processes that underlie insulin resistance and pancreatic β-cell failure.17
In addition, Gonçalves et al’s study delves into the molecular intricacies of Lp-PLA2, elucidating its heightened presence in symptomatic plaques and its associations with proinflammatory cytokines.18 Simultaneously, English et al’s cross-sectional investigation further elucidates the correlations existing between Lp-PLA2, platelet-activating factor (PAF), and conventional cardiovascular risk factors.19 Crucially, the correlation between Lp-PLA2 and PAF, TNF-gamma, and IL-6 signifies a potential role in activating pro-inflammatory cascades. This interplay underscores the complex nexus between Lp-PLA2, insulin resistance, and inflammation, urging further exploration for its implications in metabolic syndrome and cardiovascular health.
Moreover, the function and activity of Lp-PLA2 are influenced by estrogen. Estrogen functions as 17β-estradiol (E2) in the human body, which can promote the healing of endothelial cells, and also lower the inflammation state by reducing the cytokines produced by monocytes and macrophages.20 The role of estrogen in influencing the hepatic lipid profile and preventing the development of nonalcoholic fatty liver disease/steatohepatitis (NAFLD/NASH) is of significant interest. Estrogen has been shown to induce hepatic production of very low-density lipoprotein (VLDL), which plays a crucial role in lipid assembly and secretion. Consequently, men and postmenopausal women, who have lower levels of estrogen, may have an increased risk of developing NAFLD/NASH due to their impaired hepatic lipid assembly and secretion.21 This suggests that sex differences play a significant role in the lipid profile and MetS, with estrogen levels being a key determinant of the lipid profile and the development of NAFLD/NASH.
In summary, it can be inferred that reduced levels of estrogen in males make them more susceptible to central obesity. Additionally, numerous studies have established a significant association between body mass index (BMI), waist circumference, and MetS as above mentioned. After accounting for these two variables, the predictive ability of Lp-PLA2 is eliminated. In contrast, premenopausal women have a lower accumulation of central adiposity due to estrogenic support when compared to males. Therefore, we collected participants between 18 to 55 years and discussed the Lp-PLA2 by gender in our study, and the result showed a relatively strong relationship between MetS among female participants. The ROC curve analysis revealed that Lp-PLA2 had higher prediction power in females than in males, and the cut-off point of Lp-PLA2 was 626.5 in the female group in our study. These results demonstrated that gender is an important factor to consider when using Lp-PLA2 as a biomarker for MetS.
The present study boasts a significant advantage with respect to its large sample size (n = 3549), which enabled the analysis and estimation of MetS. However, it is important to acknowledge the limitations of our investigation. Firstly, the study design adopted a cross-sectional approach, thus precluding the establishment of causality. Secondly, the sample population was drawn from individuals participating in routine health examinations, which may have resulted in selection biases, as these individuals are more likely to prioritize their health. As such, there is a possibility of underestimating the prevalence of certain characteristics such as blood pressure and lipid profile if this group is taken to be representative of the entire population. Thirdly, we employed a questionnaire to collect personal data, which may have unintentionally overlooked some medical history due to individual cognitive biases. Additionally, we did not factor in socio-economic-related variables such as education, income, and lifestyle, which are important determinants of MetS. Finally, the present study only measured Lp-PLA2 mass, rather than Lp-PLA2 activity, due to the limited availability of laboratory determinations. Nonetheless, previous research has demonstrated a correlation between Lp-PLA2 activity and MetS.22 Additional investigations are warranted to elucidate the association among carotid sonography, Lp-PLA2 levels, and MetS.
Conclusion
Our research establishes a significant association between Lp-PLA2 and various metabolic risk factors, underscoring its potential as an independent risk factor for metabolic syndrome, especially in females. The implications of our findings point towards Lp-PLA2 as a promising biomarker for identifying individuals at risk of developing metabolic syndrome, with a particular emphasis on its relevance in the female population. Moving forward, further investigation is imperative to unveil the full diagnostic and therapeutic potential of Lp-PLA2 in addressing metabolic syndrome.
Abbreviations
BMI, body mass index; CAD, coronary artery disease; CRP, C-reactive protein; DBP, diastolic blood pressure; FBG, fasting blood glucose; HDL, high-density lipoprotein; Lp-PLA2, lipoprotein-associated phospholipase A2; LDL, low-density lipoprotein; MAP, mean arterial pressure; MetS, metabolic syndrome; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; SBP, systolic blood pressure; TG, triglyceride; VLDL, very low-density lipoprotein; WHtR, waist-to-height ratio.
Data Sharing Statement
Raw data were generated at Chang-Gung Memorial Hospital. Derived data supporting the findings of this study are available from the corresponding author on request.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from Institutional Review Board of Chang-Gung Memorial Hospital (XMCGIRB2022015) and was conducted in accordance with the guidelines laid down in the Declaration of Helsinki in 2013. The Institutional Review Board of Chang Gung Memorial Hospital approved this study and waived the need of consent to participate because of this study’s retrospective, non-interventional design, and because patient data confidentiality and privacy were maintained.
Acknowledgments
We thank the staff in the Health Management Center of Chang Gung Hospital for data collection assistance.
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Steinbrecher UP, Parthasarathy S, Leake DS, Witztum JL, Steinberg D. Modification of low density lipoprotein by endothelial cells involves lipid peroxidation and degradation of low density lipoprotein phospholipids. Proc Natl Acad Sci. 1984;81(12):3883–3887.
2. Brilakis ES, McConnell JP, Lennon RJ, Elesber AA, Meyer JG, Berger PB. Association of lipoprotein-associated phospholipase A2 levels with coronary artery disease risk factors, angiographic coronary artery disease, and major adverse events at follow-up. Eur Heart J. 2004;26(2):137–144. doi:10.1093/eurheartj/ehi010
3. Kurniawan LB, Rampo H, Soraya GV, et al. Effect of obesity, glucose control, lipid profiles, and blood pressure on Lp-PLA2 levels in type 2 diabetes mellitus patients. Obesity Med. 2021;22:100318. doi:10.1016/j.obmed.2021.100318
4. Jakubiak GK, Osadnik K, Lejawa M, et al. “Obesity and insulin resistance” is the component of the metabolic syndrome most strongly associated with oxidative stress. Antioxidants. 2021;11(1):79. doi:10.3390/antiox11010079
5. Monteiro R, Azevedo I. Chronic inflammation in obesity and the metabolic syndrome. Mediators Inflammation. 2010;2010:1–10. doi:10.1155/2010/289645
6. International diabetes federation: the IDF consensus worldwide definition of the metabolic syndrome. Available from: https://www.idf.org/e-library/consensus-statements/60-idfconsensus-worldwide-definitionof-the-metabolic-syndrome.html.
7. Jackisch L, Kumsaiyai W, Moore JD, et al. Differential expression of Lp-PLA2 in obesity and type 2 diabetes and the influence of lipids. Diabetologia. 2018;61(5):1155–1166. doi:10.1007/s00125-018-4558-6
8. Schaefer EJ, McNamara J, Asztalos BF, et al. Effects of atorvastatin versus other statins on fasting and postprandial C-reactive protein and lipoprotein-associated phospholipase A2 in patients with coronary heart disease versus control subjects. Am J Cardiol. 2005;95(9):1025–1032. doi:10.1016/j.amjcard.2005.01.023
9. PLd L, Favarato D, Junior JRF, Lemos P, Chagas ACP. High ratio of triglycerides to HDL-cholesterol predicts extensive coronary disease. Clinics. 2008;63(4):427–432. doi:10.1590/S1807-59322008000400003
10. Ren X, Chen Z, Zheng S, et al. Association between Triglyceride to HDL-C Ratio (TG/HDL-C) and insulin resistance in Chinese patients with newly diagnosed type 2 diabetes mellitus. PLoS One. 2016;11(4):e0154345. doi:10.1371/journal.pone.0154345
11. Scicali R, Giral P, D’Erasmo L, et al. High TG to HDL ratio plays a significant role on atherosclerosis extension in prediabetes and newly diagnosed type 2 diabetes subjects. Diabetes Metab Res Rev. 2021;37(2):e3367. doi:10.1002/dmrr.3367
12. Krawczyk M, Rumińska M, Witkowska- Sędek E, Majcher A, Pyrżak B. Usefulness of the Triglycerides to High-Density Lipoprotein Cholesterol ratio (TG/HDL-C) in prediction of metabolic syndrome in Polish obese children and adolescents. Acta Biochim Pol. 2018;65(4):605–611. doi:10.18388/abp.2018_2649
13. da Silva IT, Timm ADS, Damasceno NR, et al. Influence of obesity and cardiometabolic makers on lipoprotein-associated phospholipase A2 (Lp-PLA2) activity in adolescents: the healthy young cross-sectional study. Lipids Health Dis. 2013;12(1):19. doi:10.1186/1476-511X-12-19
14. Chen Y, Li W, Chen Y, et al. The correlation between lipoprotein associated phospholipase A2 and central overweight status. Int J Immunopathol Pharmacol. 2021;35:205873842110485. doi:10.1177/20587384211048562
15. Hsieh SD, Yoshinaga H. Abdominal fat distribution and coronary heart disease risk factors in men-waist/height ratio as a simple and useful predictor. Int J Obes Relat Metab Disord. 1995;19(8):585–589.
16. Rodrigues SL, Baldo MP, Mill JG. Association of waist-stature ratio with hypertension and metabolic syndrome: population-based study. Arq Bras Cardiol. 2010;95(2):186–191. doi:10.1590/S0066-782X2010005000073
17. Nelson TL, Biggs ML, Kizer JR, et al. Lipoprotein-associated phospholipase A2(LP-PLA2) and future risk of type 2 diabetes: results from the cardiovascular health study. J Clin Endocrinol Metab. 2012;97(5):1695–1701. doi:10.1210/jc.2011-3026
18. Gonçalves I, Edsfeldt A, Ko NY, et al. Evidence supporting a key role of LP-PLA2-generated lysophosphatidylcholine in human atherosclerotic plaque inflammation. Arterioscler Thromb Vasc Biol. 2012;32(6):1505–1512. doi:10.1161/ATVBAHA.112.249854
19. English CJ, Lohning AE, Mayr HL, Jones M, Reidlinger DP. Interrelationships among platelet‐activating factor and lipoprotein‐associated phospholipase A2 activity and traditional cardiovascular risk factors. Biofactors. 2023;49(2):457–471. doi:10.1002/biof.1928
20. Trenti A, Tedesco S, Boscaro C, Trevisi L, Bolego C, Cignarella A. Estrogen, angiogenesis, immunity and cell metabolism: solving the puzzle. IJMS. 2018;19(3):859. doi:10.3390/ijms19030859
21. Yang M, Liu Q, Huang T, et al. Dysfunction of estrogen-related receptor alpha-dependent hepatic VLDL secretion contributes to sex disparity in NAFLD/NASH development. Theranostics. 2020;10(24):10874–10891. doi:10.7150/thno.47037
22. Acevedo M, Varleta P, Kramer V, et al. Comparison of lipoprotein-associated phospholipase A2 and high sensitive C-reactive protein as determinants of metabolic syndrome in subjects without coronary heart disease: in search of the best predictor. Int J Endocrinol. 2015;2015:1–7. doi:10.1155/2015/934681
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.