Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Correlation Between Knowledge and Self-Efficacy with Family Skills in Exercising Range of Motion for Post-Stroke
Authors Sari CWM ![]() , Nofrel V, Lukman M
, Nofrel V, Lukman M
Received 26 September 2022
Accepted for publication 10 January 2023
Published 10 February 2023 Volume 2023:16 Pages 377—384
DOI https://doi.org/10.2147/JMDH.S387686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Citra Windani Mambang Sari,1 Vier Nofrel,2 Mamat Lukman1
1Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Nursing Department, Health Ministry Polytechnic of Padang, Padang, West Sumatera, Indonesia
Correspondence: Citra Windani Mambang Sari, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang Km 21, Jatinangor, Bandung, West Java, 45363, Indonesia, Tel/Fax +6222-7796647; +62 81318641100, Email [email protected]
Introduction: Stroke is the third largest cause of death after heart disease and cancer. Post-stroke patients who have disabilities will lose independence and become dependent on others. The role of the family is significant in helping patients meet psychological, social and spiritual needs. In addition, the family plays a role in recovery and optimizing the client’s motor skills. A family member is the primary support system of direct service providers in every situation. This study aimed to examine the relationship between knowledge, self-efficacy and family skills in doing a range of motion exercises post-stroke.
Methods: Correlational research method with a Cross-Sectional Study approach with post-stroke client family research samples was taken in total sampling with 55 respondents. Analysis using bivariate analysis with Spearman’s-rho correlation test.
Results: The results showed that family knowledge was above average with a Median value of 15.00 (IQR = 2), family self-efficacy was above average with a Mean value of 51.47 (SD = 11.67), and family skills were above average with a mean value of 7.73 (SD = 2.70).
Discussion: The results of bivariate analysis stated that there was a relationship between family knowledge and family skills in doing a range of motion exercises with p-value = 0.00 (r = 0.613), and there was a relationship between family self-efficacy and family skills in doing a range of motion exercises with p-value = 0.00 (r = 0.497). This research has implications for community nurses to provide interventions and enhance visite to family members with post-stroke.
Keywords: knowledge, range of motion, self-efficacy, skills, stroke
Background
Stroke is a cause of serious disability for adults.1 In 2010, stroke was in the second position of most diseases (new cases), while in 2011, stroke was in the first position of most diseases (new patients), with a total of 228 cases. The results of the National Basic Health Research in 2018 stated that the prevalence of stroke in Indonesia based on the diagnosis of health workers in people aged ≥ 15 years was 10.9 / mile, an increase compared to 2013, which was 7 / mile.2 This prevalence rate increases with increasing life expectancy.
Based on data collected by the Indonesian Stroke Foundation, the most significant number of strokes in Indonesia ranks first in Asia. The number of deaths caused by stroke ranks second at the age above 60 years and fifth at the age of 15–59 years.3 In Indonesia, it is estimated that every year 500,000 people suffer a stroke, about 2.5% or 125,000 people die, and the rest have minor or severe disabilities. In general, it can be said that the incidence of stroke is 200 / per 100,000 population.3
The disability rate due to stroke is generally higher than the death rate; globally, 15 million people have a stroke each year, one-third die and the rest experience permanent disability.4 Data from the Indonesian Hospital Association (PERSI) shows that the level of disability due to stroke reaches 65%.5 Data from 1 hospital in Indonesia stated that stroke patients’ severe neurological deficits on admission (OR 5.31, 95% CI 1.60–17.60) were significantly associated with SAP.6 After a stroke, 80% of patients experience acute paresis of the upper extremity and only approximately one-third achieve full functional recovery.7 From previous research, early measures of upper extremity active and passive range of motion could predict recovery of upper extremity function and describe the trajectory for people with stroke.7,8 Based on research from the hospital, there are suboptimal services due to limited physiotherapy facilities and resources.9 In the hospital, physiotherapy is carried out by officers during working hours; then, the staff teaches the family to be able to do it. However, when the patient has returned home, the Range of Motion (ROM) exercise is not carried out by the patient’s family due to the lack of knowledge and family self-efficacy.9 It was regarding the concepts and techniques for doing ROM exercises, even though they must be done as early as possible and as often as possible. Not all families can perform ROM exercises on patients after they go home. Many families think that post-stroke clients should only sleep for rest, and ROM exercises are only done when there is a visit by a health worker or when the client is taken to undergo physiotherapy at the hospital.10 This is because the family lacks knowledge and has low self-efficacy, which impacts the family’s abilities and skills in doing ROM exercises.9,10
Family plays a vital role in the recovery process and in optimizing the motor skills of post-stroke clients.10 The family is the primary support system for direct service providers to every condition (health-sickness) of family members. The ability of families to care for patients is related to health behaviour theory, where all activities or activities of a person refer to three things: knowledge, attitudes and actions.10 Integrative review report that knowledge about recognizing and preventing stroke was poor.11 Previous research about skills for caregivers reports that caregivers have the essential skills to care for post-stroke patients at home needed urgently.12,13 With sufficient knowledge, the family will understand and be able to provide adequate care according to the patient’s needs. In addition, families need to know the consequences of stroke and the possible complications that will occur. Optimal recovery for sufferers is also challenging if the family does not know what to do to improve the condition of the disease and what treatment should be given to sufferers.3 In treating sick family members, the family must also have high self-efficacy. Self-efficacy refers to an individual’s belief that he can do a task, achieve a goal or overcome an obstacle.14 Self-efficacy and solid motivational support from the family can positively impact patients who have had a stroke in their attitudes and actions.
Some interventions that can be done in stroke patients other than medication or drug therapy are physiotherapy/exercises such as; weight training, balance training, resistance training, hydrotherapy, and Range of Motion (ROM) training. One form of stimulation or rehabilitation program often used is Range of Motion (ROM) exercises. ROM is a recommended physical exercise program for stroke patients.7,8,15 ROM exercises can be done actively or passively by involving the role of the family.7,8 It is hoped that, in this case, the family will have good knowledge, self-efficacy and skills about ROM and the implementation of ROM exercises in post-stroke clients in the community. This study aims to analyze the relationship between knowledge, self-efficacy and family skills in doing Range of Motion (ROM) exercises for post-stroke clients treated at home.
Methods
In this study, the method used is a type of Correlational research with a Cross-Sectional. The population comprises family members caring for post-stroke clients who undergo outpatient care at the Bandung Public Health Center, with 55 respondents using total sampling.
The data was collected at the respondent’s house by visiting the respondent’s home accompanied by a local health care. First, data was collected by providing a family demographic questionnaire, client demographics, knowledge questionnaires and self-efficacy questionnaires. Then the family was asked to complete a questionnaire according to the existing questions. After filling out the knowledge questionnaire, the family was asked to do a range of motion often done for post-stroke clients, and the PI observed the family and filled out a checklist sheet. Observation of family skills in carrying out a range of motion on respondents is carried out at home because home is a safe and comfortable place, and families are used to doing this.
The data collection tools used in this study were demographic data instruments for family members who care for post-stroke clients and general information about clients, knowledge assessment instruments, self-efficacy assessment instruments and family skill assessment instruments in performing Range of Motion (ROM) exercises. Family knowledge instrument on a range of motion exercises uses a knowledge questionnaire developed by researchers based on the seventh report of the joint national committee on prevention, detection, evaluation and treatment of high blood pressure guideline (JNC 7) and Jacobson’s Progressive Muscular Relaxation which identifies family knowledge about a range of motion exercises. The number of questions as many as 20 questions using the answer options “true” or “false”. The self-efficacy instrument used in this study was developed by researchers based on the seventh report of the joint national committee on prevention, detection, evaluation and treatment of high blood pressure guidelines (JNC 7), which had been used by Mularcik and Jacobson’s Progressive Muscular Relaxation. This instrument identifies how much confidence the family members who provide care have in performing a range of motion exercises on post-stroke clients at home. There are 16 statements in this questionnaire, where the assessment of statements uses a Likert scale with a range of 1 to 5. Answers 1 = not at all sure, 2 = not sure, 3 = not sure, 4 = sure, and 5 = very sure. The higher the score, the better the respondents’ self-efficacy level. The instrument for family skills in performing a range of motion exercises uses a checklist through observation adopted by researchers based on the range of motion exercise guide to identifying family skills in performing a range of motion exercises. There are 13 items in the checklist using the “true” or “false” answer options. Three instruments have been tested for validity and reliability using Pearson and Cronbach Alpha.
The results of the analysis of the knowledge variable are not normally distributed, so to see the relationship between knowledge and family skills in performing the Range of Motion, Spearman Rho analysis is used. Pearson analysis is used to analyse the relationship between self-efficacy and family skills in performing Range of Motion because the data is normally distributed.
Permission was obtained from the Research Ethics Commission of the Universitas Padjadjaran, with ethics No. 1526/UN6.KEP/EC/2019, in compliance with the Declaration of Helsinki. The community nurses introduced the PI to the patient and families who would be potential subjects of the study. All respondents received verbal and written explanations, and a consent form was given to respondents. Signed informed consent to participate was obtained for all participants. In this study, there were respondents under 18 years old, and PI had a permit from their parents. The PI assured the respondents that their participation was voluntary and that they could leave the research. All information was maintained confidentially, and the results were presented in aggregate for academic purposes only. Additionally, there was no risk associated with the completion of the questionnaires.
Results
Table 1 shows that the relationship between respondents and clients is mostly clients’ partners, as many as 29 respondents (52.7%). This shows that most respondents are partners (husband/wife) of clients who accompany and provide care to respondents at home. In the age category, most respondents were 46–65 years old, with as many as 28 respondents (50.9%). This shows that most of the respondents are in the elderly stage. In the gender category, most of the respondents were female, with as many as 44 respondents (80.0%). In the type of work status, most of the respondents did not work or were housewives, with as many as 36 respondents (65.5%). In the category of education level, most of the respondents with high school education were 23 respondents (41.8%). This shows that most respondents have a relatively high educational background.
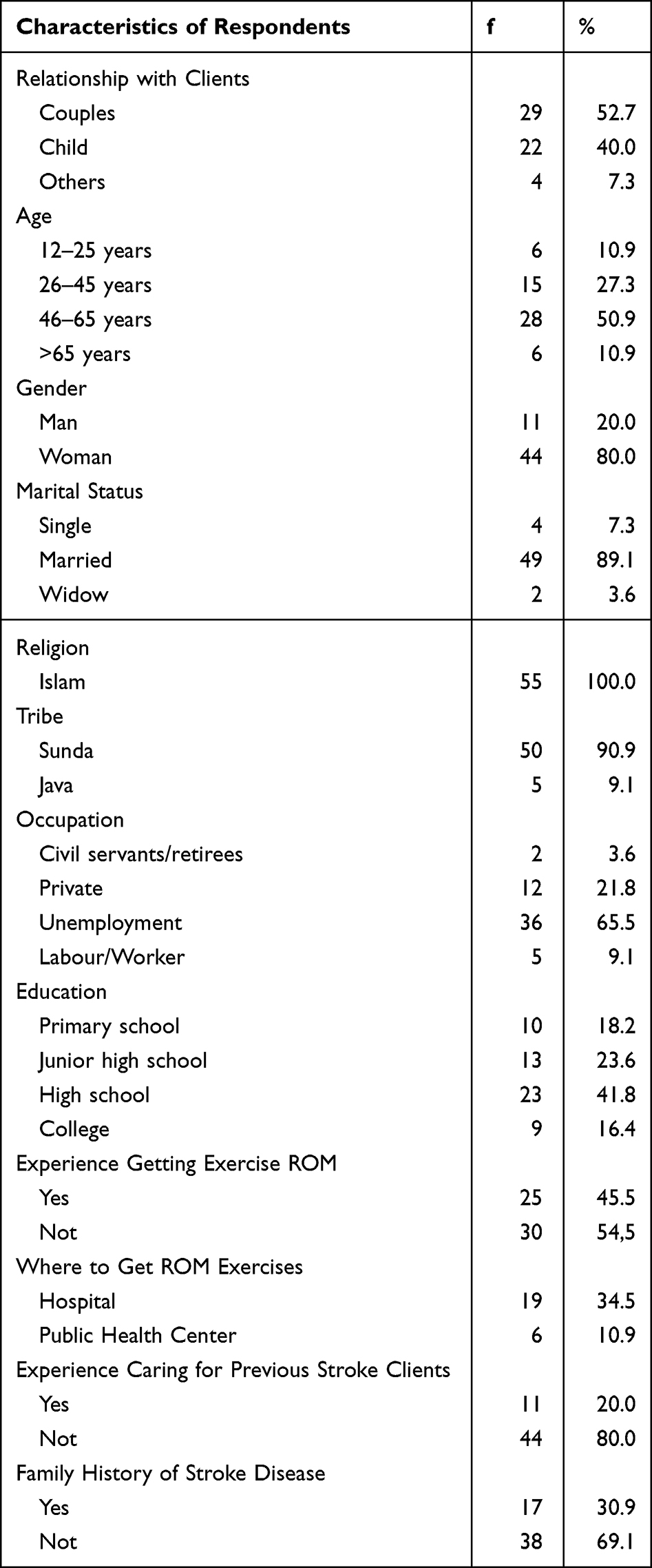 |
Table 1 Average Knowledge, Self-Efficacy and Family Skills About Range of Motion Exercises |
Table 2 shows that the respondent’s knowledge in the Median is 15.00 (IQR = 2), where from the 20 questions/statements, the minimum family score is six, and the maximum score is 18. Meanwhile, for the respondent’s self-efficacy, the mean value was 51.47 (SD = 11.67), were from the 16 questions/statements, the minimum score for the family was 19, and the maximum score was 78. Then for skills in doing a range of motion exercises, the mean value is 7.73 (SD = 2.70), where of the 13 items assessed/observed, the minimum score for the family is one, and the maximum score is 13. Finally, Table 3 shows that the results of the non-parametric analysis carried out using Spearman’s rho test show a significantly strong relationship between the variable family knowledge about a range of motion and family skills in doing range of motion exercises.
 |
Table 2 The Relationship Between Knowledge and Respondents’ Skills in Conducting Range of Motion Exercises |
 |
Table 3 The Relationship of Self-Efficacy with Respondents’ Skills in Conducting Range of Motion Exercises |
Table 4 shows that the Pearson test analysis results show a significant relationship between family self-efficacy variables in conducting a range of motion and family skills in doing a range of motion exercises. There is a relationship between the family self-efficacy variable and the family skills variable, with a strong correlation between family self-efficacy variables and family skills variables, including a moderate correlation (r = 0.497).
 |
Table 4 The Relationship of Self-Efficacy with Respondents’ Skills in Conducting Range of Motion Exercises |
Discussion
There was a significantly strong relationship between the variable family knowledge about a range of motion and family skills in doing a range of motion exercises. From the results of the analysis that has been carried out, it is known that most of the respondents have a good knowledge of the range of motion with a mean value of 14.69 (median = 15.00). This is because most of the respondents have a relatively high educational background, whereas most of the respondents with a high school education background are 23 respondents (41.8%). Having a relatively high educational background gives respondents a better knowledge and understanding of something.
Besides educational background, age is also a factor that influences the respondent’s knowledge. This study showed that most respondents were 46–65 years (50.9%). Increasing age has an effect on increasing maturity and maturity in thinking, which will affect one’s knowledge. According to a previous study, several factors influence personal knowledge, including age and higher education.16
Apart from age and educational background, another thing that affects the respondents’ knowledge is the experience of obtaining information. In this study, it is known that almost half of the respondents have experience getting information and training about a range of motion, as many as 25 respondents (45.5%). Experience getting information and range of motion exercises owned by respondents will increase respondent knowledge about a range of motion exercises. According to Forehand, based on Bloom’s Knowledge Taxonomy, knowledge results from knowing and occurs after the individual senses through the five senses of a particular object. This shows that the information and experience that individuals get on something will significantly affect their level of personal knowledge and skills in doing something.17
From the results of the analysis that has been carried out, it is known that most respondents have high self-efficacy in doing a range of motion exercises with a mean value of 51.47 (median = 51.00). Most respondents are 46–65 years (50.9%). Increasing age affects the increase in maturity or maturity in reasoning about the benefits of doing something. According to Sousa et al, a positive relationship exists between increasing age and increasing a person’s self-efficacy.18
Besides the age factor, the thing that also affects the respondent’s self-efficacy is the experience of getting information. In this study, it is known that almost half of the respondents have experience getting information and training about a range of motion, as many as 25 respondents (45.5%). The experience of getting information and exercising the range of motion possessed by the respondent increases the respondent’s confidence in doing a range of motion exercise. Shah et al stated that a person’s experience positively influences one’s self-efficacy.19 A person’s knowledge also affects a person’s self-efficacy. This study found that most respondents had good knowledge about a range of motion exercises.
Table 3 shows that most respondents have good skills in doing a range of motion exercises with a mean value of 7.73 (Median = 8.00). This is because almost half of the respondents have received information and experience in doing a range of motion exercises, as many as 25 respondents (45.5%). Skills are the capacities needed to carry out several tasks, including developing training results and gaining experience. With experience in the range of motion exercises that respondents own, it can improve respondents’ skills in doing a range of motion exercises for post-stroke clients treated at home. Skills are the application of knowledge so that a person’s skill level is related to the level of knowledge.
Based on the results of Spearman’s rho test, it can be seen that there is a significant relationship between the level of family knowledge and the level of family skills in doing a range of motion exercises. The results showed that the p-value obtained was 0.00, which means that there is a significant relationship between the level of family knowledge and family skills in doing a range of motion exercises for post-stroke clients in the Public Health Center work area in Bandung City.
The results showed that most respondents had good knowledge about a range of motion exercises. From the results of the analysis of knowledge that has been done, the mean value is 14.69 (median = 15.00). This is supported by several factors, including the relatively high educational background of 23 respondents (41.8%) who graduated from high school. Older age also affects knowledge, where most of the respondents are in the age range of 46–65 years (50.9%). Increasing age affects increasing maturity or maturity in thinking rationally. In addition to educational background and age factors, another thing that affects knowledge is experience, where as many as 25 respondents (45.5%) have had the experience of getting information about Range of Motion exercises.
The knowledge that the respondent has positively influenced the respondent’s skills in doing a range of motion (ROM) exercises for post-stroke clients treated at home. The results of this study indicate that families with good knowledge of a range of motion exercises have good skills in performing a range of motion exercises for post-stroke clients.
This is supported by research by Ja, which states that there is a relationship between knowledge of ROM and family guidance in implementing ROM in stroke patients.13 Meanwhile, research states that there is a relationship between the family knowledge level and the family’s ability to treat stroke patients at the Hospital.20,21 Another research conducted by Agonwardi stated that family knowledge significantly affected family skills in doing ROM exercises for family members with stroke.22
Drysdale & Mcbeath stated that individuals’ knowledge could help achieve goals, anticipate events experienced and respond to changing needs.23 In families with health problems where there are family members with stroke, family knowledge is an essential factor in how the family can provide optimal care for family members with stroke, especially in doing range of motion exercises to increase the client’s physical activity ability.
Based on the results of Spearman’s rho test, it can be seen that there is a significant relationship between family self-efficacy and the level of family skills. The results showed that the p-value obtained was 0.00, which means a significant relationship exists between the level of family knowledge and family skills in doing a range of motion exercises for post-stroke clients in the Public Health Centre work area.
The results showed that most respondents had good self-efficacy about range of motion exercises. From the results of the analysis of self-efficacy that has been carried out, the mean value is 51.47 (median = 51.00). This is supported by several factors, including older age which affects self-efficacy, where most respondents are 46–65 years (50.9%). According to Sousa, a positive relationship exists between increasing age and self-efficacy.18 The experiences obtained by respondents also positively influenced the respondent’s self-efficacy, where as many as 25 respondents (45.5%) had the experience of getting information about Range of Motion exercises.
The respondent’s self-efficacy positively influences the respondent’s skills in doing a range of motion (ROM) exercises on post-stroke clients treated at home. This study’s results indicate that families with good self-efficacy in doing a range of motion exercises have good skills for post-stroke exercises. This research is also in accordance with the results of research which reported that self-efficacy is very closely related to rehabilitation motivation.24
This is supported by research conducted by Ismatika at the Hospital, which states that there is a relationship between family self-efficacy and treatment behaviour in post-stroke patients.25 Bandura states self-efficacy is a person’s belief about their ability to produce the desired action and influence life.26 Self-efficacy will determine how a person feels, thinks and motivates himself to behave. Baron & Byrne suggest that self-efficacy assesses a person’s ability or competence to perform a task, achieve a goal and produce something.14 Self-efficacy owned by the family provides an overview of the family’s abilities and skills in providing care for post-stroke clients at home, especially in doing a range of motion exercises.27
Skills are the capacities needed to carry out several tasks, including developing training results and gaining experience. Skills can indicate the specific action performed or the nature by which the skill is performed. Many activities are considered a skill, consisting of several skills, and the degree of mastery achieved by a person describes the skill level. This occurs because it is a commonly accepted habit to state that one or more extended movement patterns or behaviours can be called skills.
Thus, it can be concluded that to achieve a good skill, it is necessary to pay attention to the following: First, a person’s factor, the willingness and seriousness of the person in the form of great motivation to master the skills being taught. Second, the learning process refers to how learning conditions are adjusted to a person’s potential and environment, significantly affecting skill mastery. Third, situational factors refer to the exercises or practices’ methods and techniques.
Based on the above explanation, family knowledge and self-efficacy positively affect family skills in carrying out a range of motion exercises for family members with post-stroke treatment at home. Previous studies support that a relationship exists between knowledge, self-efficacy and skills.28,29
Conclusion
The results of bivariate analysis stated that there was a relationship between family knowledge and family skills in doing a range of motion exercises with p-value = 0.00 (r = 0.613), and there was a relationship between family self-efficacy and family skills in doing a range of motion exercises with p-value = 0.00 (r = 0.497). This can have implications for community nurses to provide interventions with health education and practicing range of motion so they can continue to accompany families in caring for family members with post-stroke.
Acknowledgment
The authors want to thank all respondents and the Bandung public health office.
Disclosure
The authors report no conflicts of interest in this work.
References
1. CDC. Stroke. Available from: https://www.cdc.gov/stroke/.
2. Basic Health Research. Research and Development Agency for Health Ministry of Health of Indonesia. Jakarta: Basic Health Research; 2018.
3. Yayasan Stroke Indonesia. Tahun 2020 penderita stroke meningkat 2 kali; 2012. Acessed from: http://www.yastroki.com/.
4. National Stroke Foundation. National stroke audit: rehabilitation services report 2012. Melbourne, Australia: National Stroke Foundation; 2012. Accessed from: http://strokefoundation.com.au/prevent-stroke/.
5. Ministry of Health of the Republic of Indonesia. Data and Information on Indonesia’s Health Profile in 2018. Jakarta: Ministry of Health of the Republic of Indonesia; 2018.
6. Sari IM, Soertidewi L, Yokota C, Kikuno M, Koga M, Toyoda K. Comparison of characteristics of stroke-associated pneumonia in stroke care units in Indonesia and Japan. J Stroke Cerebrovasc Dis. 2017;26(2):280–285. doi:10.1016/j.jstrokecerebrovasdis.2016.09.018
7. Beebe JA, Lang CE. Active range of motion predicts upper extremity function 3 months after stroke. Stroke. 2009;40(5):1772–1779. doi:10.1161/STROKEAHA.108.536763
8. Hosseini ZS, Peyrovi H, Gohari M. The effect of early passive range of motion exercise on motor function of people with stroke: a randomized controlled trial. J Caring Sci. 2019;8(1):39. doi:10.15171/jcs.2019.006
9. Muhrodji P, Wicaksono HD, Satiti S, Trisnantoro L, Setyopranoto I, Vidyanti AN. Roles and problems of stroke caregivers: a qualitative study in Yogyakarta, Indonesia. F1000Research. 2021;10:380. doi:10.12688/f1000research.52135.1
10. Sunaryo S, Ulfiana E, Yasmara D. Health education about ROM increases family motivation in carrying out range of motion (ROM) in stroke infarct patients at Soetomo Hospital, Surabaya. J Crit Med Surg Nurs. 2015;3(2):28–32. doi:10.20473/cmsnj.v3i2.12290
11. Jones SP, Jenkinson AJ, Leathley MJ, Watkins CL. Stroke knowledge and awareness: an integrative review of the evidence. Age Ageing. 2010;39(1):11–22. doi:10.1093/ageing/afp196
12. Pitthayapong S, Thiangtam W, Powwattana A, Leelacharas S, Waters CM. A community based program for family caregivers for post stroke survivors in Thailand. Asian Nurs Res. 2017;11(2):150–157. doi:10.1016/j.anr.2017.05.009
13. Kim IJ. Sources of anxiety and burden of family caregivers of stroke patients: the role of self-efficacy and knowledge about care. Korean J Adult Nurs. 2012;24(1):1. doi:10.7475/kjan.2012.24.1.1
14. Baron & Bryne. Self-efficacy; 2000. Available from: http://www.treepjkr.multiply.com.
15. Srinayanti Y, Widianti W, Andriani D, Firdaus FA, Setiawan H. Range of motion exercise to improve muscle strength among stroke patients: a literature review. Int J Nurs Health Services. 2021;4(3):332–343. doi:10.35654/ijnhs.v4i3.464
16. Tan CE, Hi MY, Azmi NS, Ishak NK, Aziz AF, Abdul Aziz AF. Caregiving self-efficacy and knowledge regarding patient positioning among Malaysian caregivers of stroke patients. Cureus. 2020;12(3). doi:10.7759/cureus.7390
17. Forehand M. Bloom’s taxonomy. Emerg Perspect Learn Teach Technol. 2010;41(4):47–56.
18. Sousa JE, Costa MA, Abizaid A, et al. Four-year angiographic and intravascular ultrasound follow-up of patients treated with sirolimus-eluting stents. Circulation. 2005;111(18):2326–2329. doi:10.1161/01.CIR.0000164271.01172.1A
19. Shah NS, Wright A, Bai GH, et al. Worldwide emergence of extensively drug-resistant tuberculosis. Emerg Infect Dis. 2007;13(3):380. doi:10.3201/eid1303.061400
20. Simandalahi T. Analysis of the relationship between the level of knowledge and family attitudes with the family’s ability to care for post-stroke patients. J Health Medika Saintika. 2018;9(1):41–48.
21. Bauronga A, Ake J, Lumi M. The relationship between ROM knowledge and family guidance carrying out ROM exercise in stroke patients at the hospital. GMIM Bethesda Tomohon. Online J Sariputra Indonesia Univ. 2018;5(2):1–6.
22. Agonwardi A, Budi H. The effect of range of motion (ROM) exercise health education on family skills to perform ROM in stroke patients. J Endurance. 2016;1(1):47–54. doi:10.22216/jen.v1i1.1030
23. Drysdade M, Mcbeath M. Self-concept and tacit knowledge: differences between cooperative and non-cooperative education student. Asia Pacific J Cooperat Educ. 2012;13(3):169–180.
24. Kurniawati ND, Rihi PD, Wahyuni ED. Relationship of family and self efficacy support to the rehabilitation motivation of stroke patients. Eur Asian J BioSci. 2020;14(1):245.
25. Ismatika I, Soleha U. The relationship between self-efficacy and post-stroke patient self-care behavior at Islamic Hospital Surabaya. Sci J Health. 2017;10(2):139–148. doi:10.33086/jhs.v0i2.140
26. Bandura A. Guide for constructing self efficacy scales. Self efficacy beliefs of A dolescent; 2006:307–337. Available from: http://www.des.emory.edu/mfp/014Baduraguide.
27. Luthfa I. The role of the family in caring for the elderly after stroke. Family role to care for post stroke elderly. Unissula Nurs Conf. 2018;1(1). doi:10.26532/v1i1.2888.g2102
28. Sari CW, Yamin A, Santoso MB. Community-Based Education Program on knowledge and self-efficacy of type 2 diabetes mellitus’ patients in Bandung. Indonesian Contemporary Nursing Journal. 2017 30:38–44. Accessed from: http://journal.unhas.ac.id/index.php/icon/article/view/3583
29. Sari CW, Witdiawati W, Purnama D, Kurniawan T, Santoso MB. Effect of Integrated Care Programs on SelfEfficacy and SelfManagement Behaviors among Diabetic in a Primary Health Care in Indonesia. Sari CW, Witdiawati W, Purnama D, Kurniawan T, Santoso MB. Effect of Integrated Care Programs on SelfEfficacy and SelfManagement Behaviors among Diabetic in a Primary Health Care in Indonesia. Mal J Med Health Sci. 2022;18(SUPP3): 157161.;18(SUPP3): 157161.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Among Middle-Aged and Elderly Population Towards Ultrasound Screening for Strokes
Wang W, Peng Y, Tang K, Zheng Z, He L, Yang S
Journal of Multidisciplinary Healthcare 2024, 17:147-157
Published Date: 9 January 2024
Effect of Simulation-Based Education of Adult BLS-CPR on Nursing Students’ Skills and Knowledge Acquisition
Bdiri Gabbouj S, Zedini C, Naija W
Advances in Medical Education and Practice 2025, 16:663-673
Published Date: 22 April 2025
Enhancing Public Knowledge of Risk Factors and Warning Signs for Stroke and Heart Attack Through Home-Based Community Health Worker Interventions: A Cluster Randomized Trial
Muhihi A, Njelekela MA, Anaeli A, Mruma HA, Sunguya B, Kakoko D, Kessy AT, Mpembeni R, Urassa DP
International Journal of General Medicine 2025, 18:7591-7604
Published Date: 16 December 2025
Caregivers’ Knowledge, Attitudes, and Practices Regarding Risk Factors and Management of Post-Stroke Delirium Among Stroke Patients: A Cross-Sectional Study
Zhao L, Xu Y, Zhang Y, Gong Q, Bao J
International Journal of General Medicine 2026, 19:559169
Published Date: 14 January 2026