Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Correlation Between Improvements in Melasma Quality of Life (MELASQoL-INA) and Modified Melasma Area and Severity Index (mMASI) Following Triple Combination Therapy
Authors Darmawan I, Indriatmi W, Rihatmadja R, Sitohang IBS ![]()
Received 7 July 2025
Accepted for publication 16 November 2025
Published 20 February 2026 Volume 2026:19 552194
DOI https://doi.org/10.2147/CCID.S552194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Irene Darmawan, Wresti Indriatmi, Rahadi Rihatmadja, Irma Bernadette S Sitohang
Department of Dermatology and Venereology Faculty of Medicine Universitas Indonesia - Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Correspondence: Irma Bernadette S Sitohang, Department of Dermatology and Venereology Faculty of Medicine Universitas Indonesia – Dr. Cipto Mangunkusumo Hospital, 71 Diponegoro Street, Jakarta Pusat, Jakarta, 10430, Indonesia, Tel +62818130761, Email [email protected]
Purpose: Melasma is a facial pigmentary disorder that commonly causes psychosocial distress. Quality of life (QoL) is not routinely assessed in daily practice; therefore, its improvement in relation with the reduction of melasma severity remains unclear, especially among people of color. This study aimed to determine whether clinical improvement after triple combination cream (fluocinolone acetonide 0.01%, hydroquinone 4%, and tretinoin 0.05%) correlated with improved QoL.
Patients and Methods: Participants with melasma were enrolled in a one-group pretest–posttest study and treated with triple combination cream for 12 weeks. The Melasma Quality of Life Scale (MELASQoL-INA, a validated questionnaire adapted into the Indonesian language) and the modified Melasma Area and Severity Index (mMASI) assessments were carried out at baseline visit and at weeks 4, 8, and 12 to evaluate QoL and clinical severity.
Results: Thirty female participants aged 30– 60 years, with Fitzpatrick skin type IV or V and without other facial skin conditions, completed the study. The most negatively affected QoL domains were emotional well-being (appearance concerns, embarrassment, and frustration) and social life (desire to interact with other people). Significant improvements were observed in both mMASI (median reduction from 4.45 to 1.80; p < 0.001) and MELASQoL-INA scores (median reduction from 37 to 17; p < 0.001) after 12 weeks of treatment. Although no correlation was observed between mMASI and MELASQoL-INA scores at week 12 (r = 0.029, p = 0.879), a weak positive correlation was found between their respective changes after treatment (r = 0.397, p = 0.03).
Conclusion: Clinical improvement in melasma severity following triple combination therapy is modestly associated with improved QoL. However, QoL impairment does not always correspond linearly with disease severity, highlighting the importance of integrating subjective QoL outcomes alongside clinical evaluations in the management of melasma.
Keywords: melasma, MELASQoL-INA, mMASI, quality of life, treatment
Introduction
Melasma is a common pigmentary disorder that predominantly affects individuals with Fitzpatrick skin types IV–V.1 Its predilection for the face and tendency to recur can significantly affect physical appearance.2 Beyond physical appearance, melasma imposes a substantial psychosocial burden, often contributing to emotional distress and a reduced quality of life (QoL). To assess this impact, the Melasma Quality of Life Scale (MELASQoL) was developed and subsequently adapted into several languages, including the Indonesian version (MELASQoL-INA).3,4
One factor that may contribute to reduced QoL in patients with melasma is disease severity, which can be objectively assessed using the Melasma Area and Severity Index (MASI) or the modified MASI (mMASI). While these tools are valuable for grading disease extent and guiding therapy, their relationship with patient-perceived QoL remains unclear. Previous studies have reported inconsistent correlations between melasma severity and QoL scores, likely due to differences in study design, population characteristics, and scoring tools used.5–8
Many studies have evaluated either clinical severity or QoL in isolation, rather than examining how both parameters evolve in response to treatment. To our knowledge, no previous study in the Indonesian population with Fitzpatrick skin types IV–V has prospectively evaluated the correlation between improvements in melasma severity and QoL using standardized tools such as mMASI and MELASQoL-INA. This represents a key gap in the literature, especially since QoL is rarely assessed in routine clinical practice, where therapeutic decisions are often based solely on visible skin improvement.
Several treatment options are available for melasma. The first line modalities include sun protection and topical brightening agents.9 Among these, topical hydroquinone and triple combination therapy containing hydroquinone are considered the current gold-standard treatments.10 This study aims to determine whether clinical improvement after triple combination cream therapy (fluocinolone acetonide 0.01%, hydroquinone 4%, and tretinoin 0.05%) correlates with improved QoL. Through this study, we aim to emphasize the value of combining clinical assessments with patient-reported QoL outcomes to promote a more holistic and patient-centered approach to melasma management.
Materials and Methods
This was a one group pretest–posttest study. The study protocol was reviewed and approved by the Ethics Committee of the Faculty of Medicine, Universitas Indonesia. Written informed consent was obtained from all participants before enrollment. The study was registered on ClinicalTrials.gov under the identifier NCT06516419. All research procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Study Participants
The study was conducted at our institution, a tertiary referral hospital serving the Greater Jakarta area, from February to May 2024. Participants were recruited through consecutive sampling from patients attending the Cosmetic Dermatology Division of the Dermatology and Venereology Outpatient Department. The sample size was calculated based on correlation analysis, resulting in an estimated requirement of 30 participants. Statistical parameters were set at α = 0.05 with 80% power, and an assumed correlation coefficient of 0.5, given the lack of prior studies evaluating the correlation between improvements in MELASQoL-INA and mMASI scores:

Eligible participants were women aged 30–60 years with Fitzpatrick skin type IV or V and a clinical diagnosis of melasma. Exclusion criteria included pregnancy or lactation, use of hormonal contraception within the past 6 weeks, application of topical brightening agents within the past 2 weeks, use of photosensitizing agents within the past 4 weeks, systemic therapy for melasma within the past 4 weeks, or a history of deep peeling procedures within the last 6 months. Participants with concurrent pigmentary disorders that could interfere with the assessment of melasma were also excluded.
Intervention
Participants received a fixed-dose triple combination cream containing fluocinolone acetonide 0.01%, hydroquinone 4%, and tretinoin 0.05%, applied once nightly for 12 weeks. All participants were also provided with SPF 45 sunscreen and a standardized facial cleanser for daily use. Compliance was monitored by weighing the cream tubes at each follow-up visit.
Evaluation
All clinical evaluations were conducted by the same investigator. Melasma severity was assessed using the mMASI score at baseline and at weeks 4, 8, and 12. The mMASI score was calculated as follows:
mMASI score = 0.3A(f)D(f) + 0.3A(lm)D(lm) + 0.3A(rm)D(rm) + 0.1A(c)D(c)
Where A represents the area of involvement and D represents the darkness of pigmentation. Subscripts denote facial regions: f = forehead, lm = left malar, rm = right malar, and c = chin. The area of involvement was scored as follows: 0 = absent, 1 = ≤10%, 2 = 10–29%, 3 = 30–49%, 4 = 50–69%, 5 = 70–89%, and 6 = 90–100%. The total score ranged from 0 to 24, with higher values indicating greater severity.
Quality of life was assessed using the MELASQoL-INA questionnaire at baseline and at weeks 4, 8, and 12. The questionnaire consists of 10 items, each scored from 1 (not bothered at all) to 7 (bothered all the time), with higher scores indicating poorer QoL. Completion of the MELASQoL-INA was supervised by the investigator, and participants were encouraged to seek clarification if any item was unclear.
Data Analysis
Data were analyzed using IBM SPSS Statistics for Windows, version 25.0. Differences in mMASI and MELASQoL-INA scores between pre- and post-therapy were assessed using the Wilcoxon signed-rank test. The Spearman correlation coefficient was employed to evaluate the relationship between mMASI and MELASQoL-INA scores, as well as between their respective changes (ΔmMASI and ΔMELASQoL-INA) following 12 weeks of therapy.
Results
The study was conducted at our institution, between February and May 2024. A total of 30 participants were recruited. Their mean age was 50.9 ± 4.8 years. Most participants were married (73.3%), had attained higher education (60%), and were employed (73.3%). The median age of melasma onset was 40 years (range: 30–55), and the median disease duration was 84 months (range: 1–360). A history of prior melasma treatment, including topical and procedural therapies, was reported in 53.3% of the participants. Routine sunscreen use, however, was documented in only 40% of the participants. The malar region was the most frequently affected site, and the mixed type of melasma was the most prevalent. Detailed clinical characteristics are presented in Table 1.
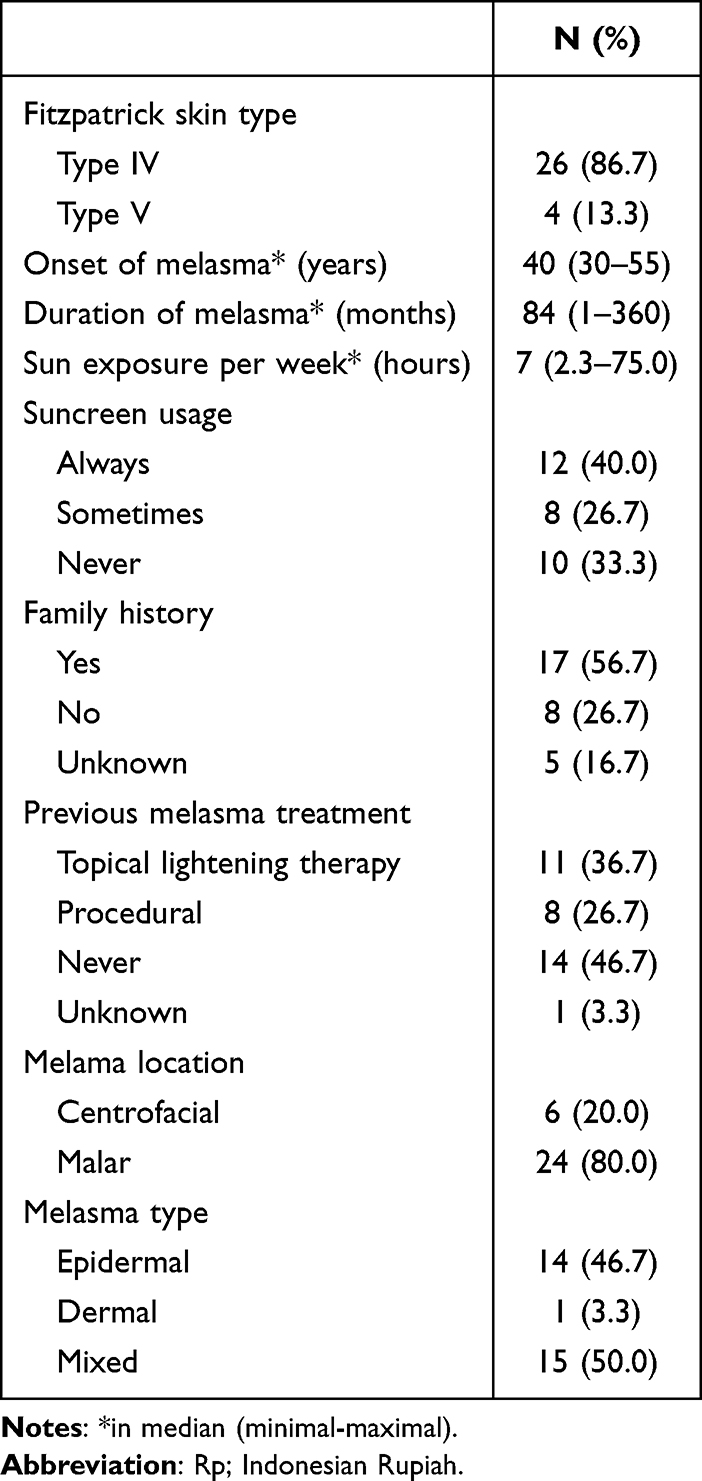 |
Table 1 Clinical Characteristics of Study Population (N=30) |
Quality of Life Assessment
Baseline QoL scores are presented in Table 2. The MELASQoL-INA questionnaire assesses three domains: emotional well-being, social life, and recreation/leisure.8 In this study, the emotional well-being domain (Q1–Q4: skin appearance, embarrassment, frustration, and depression) was the most negatively affected. The social life domain (Q5–Q7, Q10) and recreation/leisure domain (Q8–Q9) were also impaired, though to a lesser extent. Following therapy, the emotional well-being domain demonstrated the most pronounced improvement, as shown in Table 3.
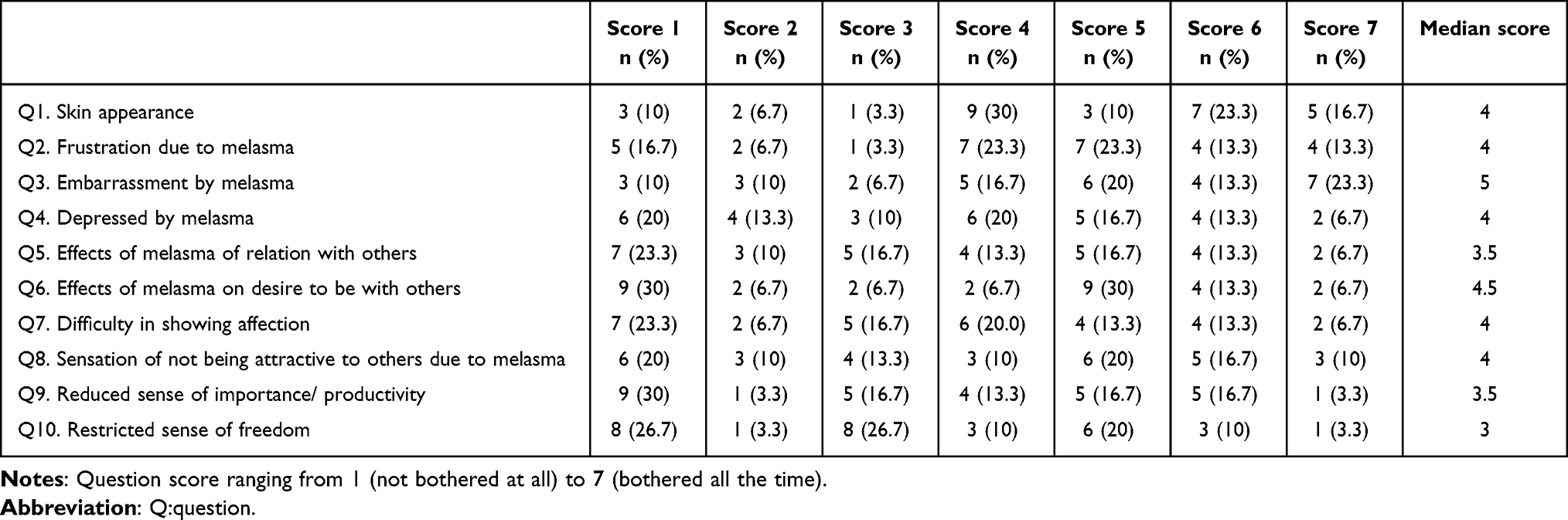 |
Table 2 Baseline Melasma Quality of Life Scale (MELASQOL-INA) Score of Melasma Patients (N=30) |
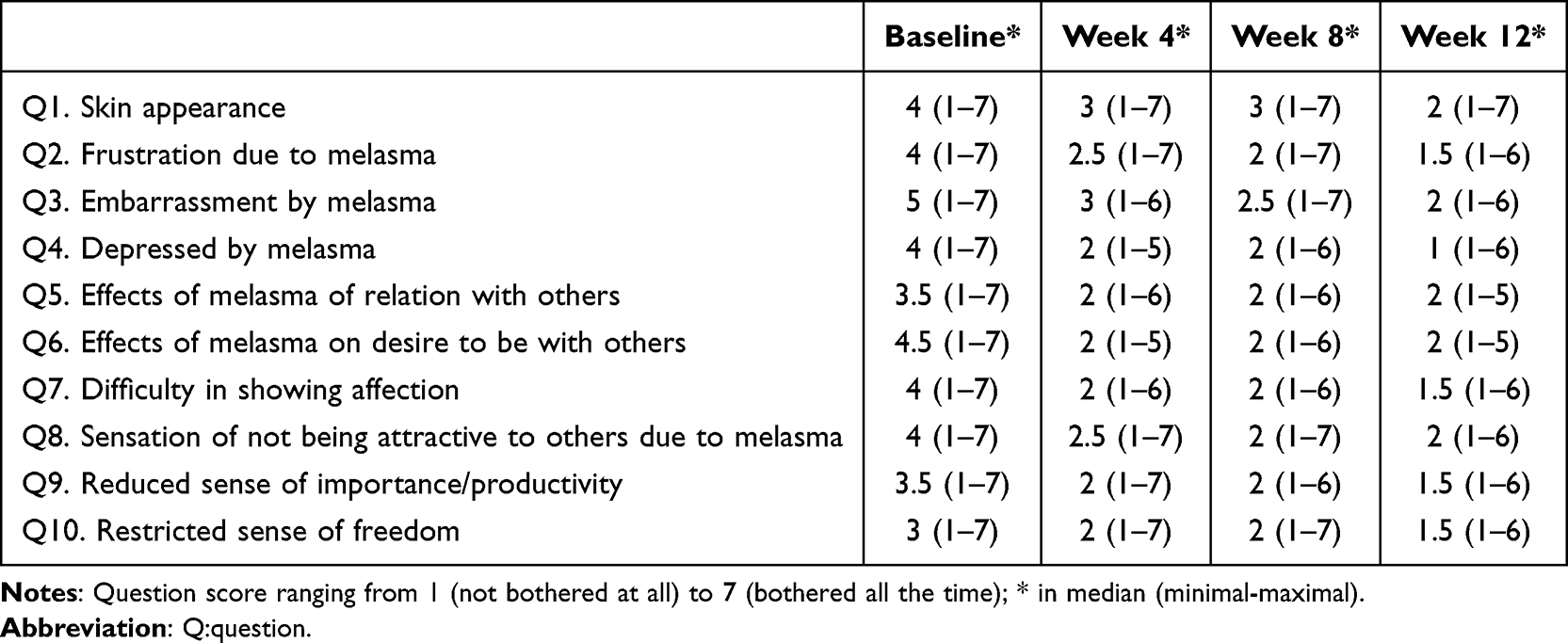 |
Table 3 Improvement of Melasma Quality of Life Scale (MELASQoL-INA) Score After Triple Combinations Cream Therapy |
mMASI and MELASQoL-INA Scores Before and After Therapy
At baseline, the median mMASI score was 4.45 (range: 1.3–13.9), and the median MELASQoL-INA score was 37 (range: 10–70). Improvements in both mMASI and MELASQoL-INA scores following treatment are illustrated in Figures 1 and 2. Significant reductions were observed in both scores after 12 weeks of therapy (p < 0.001). By week 12, the median mMASI score had decreased to 1.80 (range: 0.60–6.30), and the median MELASQoL-INA score had decreased to 17 (range: 10–59). The median reduction in mMASI was 2.55, while the median reduction in MELASQoL-INA was 15.5.
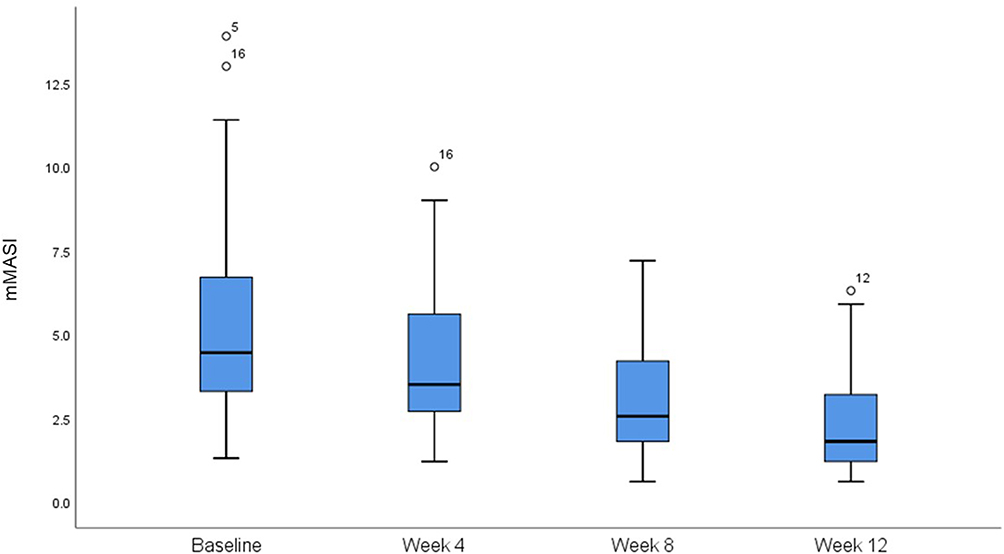 |
Figure 1 The improvement of modified melasma area and severity index (mMASI) score after triple combination therapy. |
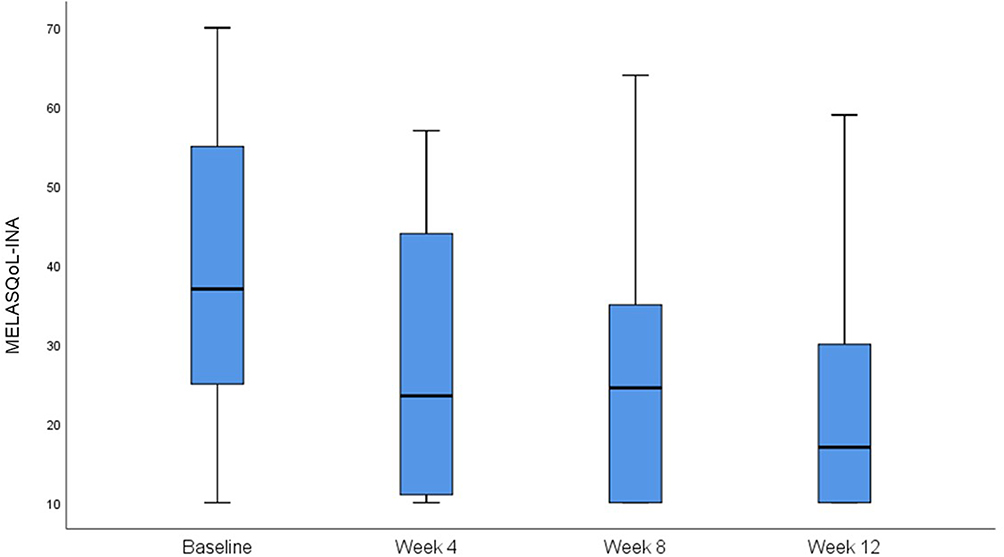 |
Figure 2 The improvement of melasma quality of life scale (MELASQoL-INA) score after triple combination therapy. |
MELASQoL-INA scores were categorized into mild (10–39), moderate (40–54), and severe (55–70) impairment levels.11 At baseline, 56.67% of the participants were classified as having mild impairment, 16.67% as moderate, and 26.67% as severe. By week 12, the distribution had shifted, with 86.67% classified as mild, 10% as moderate, and only 3.3% as severe. The median mMASI score at week 12 was 1.95 (range: 0.60–6.30) in the mild group and 1.20 (range: 1.20–1.80) in the moderate group. The single participant who remained in the severe group had a week 12 mMASI score of 2.80.
Correlation Between mMASI and MELASQoL-INA Scores
No significant correlation was observed between mMASI and MELASQoL-INA scores at week 12 (r = 0.029; p = 0.879). However, a weak positive correlation was found between changes in mMASI and MELASQoL-INA scores (ΔmMASI and ΔMELASQoL-INA), with a correlation coefficient of r = 0.397 (p = 0.03), as illustrated in Figure 3.
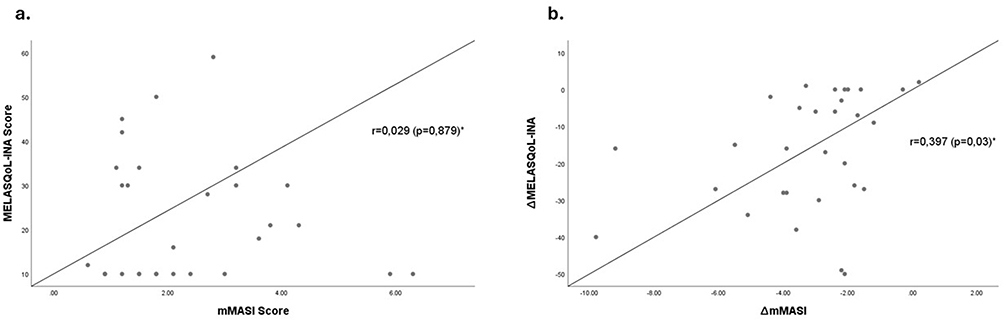 |
Figure 3 (a) Scatter plot showed no correlation between melasma quality of life scale (MELASQoL-INA) score and modified melasma area and severity index (mMASI) score. (b) There was a weak correlation between ∆MELASQoL-INA score and ∆mMASI score after 12 weeks of triple combination therapy. *Spearman correlation analysis. Abbreviations: ∆, delta; r, correlation coefficient. |
Safety
No serious adverse events occurred during the study. The most common side effects during the first 4 weeks of treatment included burning (43.3%), pruritus (53.3%), dry skin (53.3%), and local erythema (50%). By week 12, the frequency of these adverse events had decreased: burning was reported by 20% of the participants, pruritus by 3.3%, dry skin by 20%, and local erythema by 36.7%. Burning sensations were transient and most often occurred after facial cleansing. Importantly, no case of skin atrophy were observed. All participants completed the 12-week course of therapy.
Discussion
This study evaluated the QoL in individuals with melasma who had Fitzpatrick skin types IV or V, the most common skin types in the Indonesian population.12 At baseline, 50% of the participants reported being bothered (score of 5–7) by their appearance (Q1) and frustrated (Q2), 56.6% felt embarrassed (Q3), and 36.7% reported depression (Q4). These findings indicate that melasma affects the emotional well-being domain (Q1–Q4) more profoundly than the social life and recreation/leisure domains. This pattern aligns with previous studies conducted in Brazil, India, and Australia, suggesting that the emotional impact of melasma is substantial across different countries and cultural contexts.11,13,14
In the social life domain, the desire to be with others (Q6) was the most affected, with 50% of the participants reporting scores of 5–7. Similar findings have been reported in Brazil and Australia.13,15 In the recreation and leisure domain, 46.7% of the participants scored 5–7 on feeling unattractive to others (Q8). Previous studies have shown that melasma negatively affects self-perception of attractiveness and reduces the desire to socialize. However, its impact on productivity, desire to show attention to others (Q9), and sense of freedom (Q10) appears to be less pronounced. Similar findings were reported in India.11
The median baseline MELASQoL-INA score in this study was 37 (range: 10–70), consistent with findings from Indonesia, India, and Brazil.5,6,14 However, this score was lower than the values reported in Australia, Singapore, and France.15–17 These differences may reflect variations in the perceived impact of melasma across skin types. In individuals with darker skin, melasma may be less visually contrasting against the surrounding normal facial skin, resulting in a less pronounced effect on QoL. Additionally, several other factors have been identified as influencing QoL in patients with melasma, including age, education level, income, history of melasma treatment, disease duration, history of psychiatric disorders, and clinical severity of melasma.18
This study included participants aged 30–60 years. Misery et al17 (France) reported higher MELASQoL scores among individuals older than 45 years, whereas Balkrishnan et al3 (United States) found higher scores in the younger participants aged 20–30 years. In contrast, Harumi et al16 (Singapore) observed no significant association between MELASQoL scores and demographic variables such as age. These conflicting findings highlight the lack of consistent evidence regarding the influence of age on QoL in patients with melasma.
In Brazil, lower education and income levels were associated with higher MELASQoL scores.19 It was proposed that a limited understanding of the disease may increase anxiety.20 In our study, 60% of the participants had a high level of education (at least completion of high school). Most studies, with the exception of Kothari et al,21 have found that MELASQoL scores increase with longer disease duration. Prolonged duration has also been linked to more severe melasma and a history of previous treatments.20 In our study, factors such as older age, longer disease duration, and multiple prior treatments may have contributed to the relatively high MELASQoL-INA scores observed.
After 12 weeks of therapy, gradual improvement was observed in both mMASI and MELASQoL-INA scores, indicating that reductions in melasma severity were accompanied by improvements in QoL. Similarly, Cestari et al13 (Brazil) reported significant improvement in melasma severity, evaluated using the original MASI, and in MELASQoL scores after 8 weeks of triple combination cream therapy. Arellano et al22 also documented improvements in MASI and MELASQoL after 8 weeks of daily triple combination cream therapy, with sustained benefits up to 6 months when transitioned to a maintenance regimen (twice weekly) or gradually tapered.
This study found that melasma severity did not have a linear relationship with QoL. At week 12, some participants with mild MELASQoL-INA scores demonstrated relatively high mMASI values (0.60–6.30), while others with moderate impairment in QoL reported lower mMASI scores (1.20–1.80). This finding is consistent with our correlation analysis, which showed no significant association between mMASI and MELASQoL-INA scores after therapy. Together, these results suggest that clinical severity alone may not fully capture the psychosocial burden experienced by patients with melasma.
Several other studies have also reported no significant correlation between melasma severity and QoL, including those by Jusuf et al5 (Indonesia), Freitag et al14 (France), Harumi et al16 (Singapore), and Sarkar et al23 (India). In contrast, two studies reported significant correlations: Abou-Taleb et al24 (Egypt) found a weak correlation (r = 0.38), while Tursina et al25 (Indonesia) reported a moderate correlation (r = 0.512). The Egyptian study, by Abou-Taleb et al24 included younger participants (≥18 years), a wider range of Fitzpatrick skin types (III–V), a predominantly unemployed population (86%), and a higher baseline mean mMASI score (9.82), although MELASQoL scores were not reported. The Indonesian study by Tursina et al25 included younger participants (≥18 years) and higher mMASI scores (moderate–severe). In that study, participants with mild melasma often did not perceive the condition as bothersome, whereas those with severe melasma commonly reported embarrassment and reduced self-confidence.25
These inconsistent findings across studies support the understanding that clinical severity is not the sole factor influencing patients’ perception of melasma. Clinicians often rely primarily on physical examination to assess treatment outcomes, which may lead to discrepancies between objective clinical evaluations and patients’ lived experiences.3 For instance, clinicians may judge melasma as mild, while the patient may feel considerable psychosocial distress, or conversely, a severe clinical presentation may be reported by the patient as only mildly bothersome. In this study, the participant with the highest week-12 mMASI score (6.30) reported only mild impairment in QoL, whereas others with lower mMASI scores described moderate QoL disturbance. Because QoL assessment is inherently subjective, it can be shaped by factors such as age, personality traits, occupation, and social interactions.19 This variability likely explains the absence of a strong correlation between mMASI and MELASQoL-INA scores in this study.
Nonetheless, a weak positive correlation was observed between improvements in mMASI and MELASQoL-INA scores following 12 weeks of triple combination cream therapy (r = 0.397; p = 0.03). This suggests that greater clinical improvement in melasma severity was modestly associated with greater perceived improvement in QoL. Visible reductions in melasma may thus contribute positively to patients’ emotional well-being, social interactions, and recreational activities, although the relationship is not strongly linear.
The findings of this study support the clinical use of both mMASI and MELASQoL-INA as practical tools for assessing treatment outcomes in melasma. mMASI is a straightforward and cost-effective clinical tool, but consistent and accurate scoring requires training and experience, particularly in busy outpatient settings where time is limited. MELASQoL-INA is recommended for routine clinical use, as it is a brief, simple, and validated tool for the Indonesian population. With only 10 items, it can be self-administered during waiting periods, enhancing efficiency in clinical practice. Importantly, both tools are low-cost, non-invasive, and widely accessible, making them suitable for use in various healthcare settings across Indonesia and other resource-limited environments. Assessing the psychosocial impact of melasma is essential for developing holistic and individualized treatment strategies. Notably, discrepancies between clinical improvement and patient-reported outcomes should prompt clinicians to consider adjusting treatment approaches, including the potential integration of psychological interventions.
Limitations
The primary limitation of this study is its single-center design, which may not adequately capture the diversity of perspectives, socioeconomic backgrounds, and QoL experiences across the broader Indonesian population. Although data on potentially influential factors such as age, duration of melasma, and socioeconomic status were collected, these variables were not included in the analysis, as the primary objective was to examine the direct correlation between better improvements in melasma severity and QoL. As a result, the reported correlation is unadjusted and should be interpreted in the context of this specific aim.
Future Perspectives
Future studies incorporating multivariable analyses and multicenter recruitment are warranted to further explore the complex interactions between clinical severity, psychosocial factors, and QoL in patients with melasma. Qualitative studies that explore patient perspectives on the psychosocial burden of melasma may provide deeper insights beyond questionnaire-based assessments. Given the substantial impact of melasma on QoL, further research should also explore the role of psychological interventions in improving patient-reported outcomes and advancing a more patient-centered approach to care.
Conclusion
This study demonstrated a positive correlation between improvements in melasma severity, measured using the mMASI, and improvements in QoL, assessed using the MELASQoL-INA, following 12 weeks of triple combination therapy. The findings underscore that clinical improvement in melasma is associated with enhanced patient-reported outcomes. However, significant QoL impairment may persist even in cases of mild clinical severity, highlighting the importance of incorporating psychosocial assessment into routine management. These results support the integration of QoL measures into holistic and individualized treatment strategies for melasma.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The raw data will be available and remain accessible for up to 5 years following the publication date.
Acknowledgments
Authors are grateful to Dr. Cipto Mangunkusumo Hospital to provide facilities for this research dan Universitas Indonesia for the funding under grant number PKS – 170/UN.2.INV/HKP.05/2024. The authors extend their appreciation to Frylie Fremiati MD for assisting this research data collection.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Sarkar R, Arora P, Garg V, Sonthalia S, Gokhale N. Melasma update. Indian Dermatol Online J. 2014;5(4):426. doi:10.4103/2229-5178.142484
2. Handel AC, Miot LDB, Miot HA. Melasma: a clinical and epidemiological review. An Bras Dermatol. 2014;89(5):771–9. doi:10.1590/abd1806-4841.20143063
3. Balkrishnan R, McMichael AJ, Camacho FT, et al. Development and validation of a health-related quality of life instrument for women with melasma. Br J Dermatol. 2003;149(3):572–577. doi:10.1046/j.1365-2133.2003.05419.x
4. Aditya R. Validity and reliability of melasma quality of life scale questionnaire in Bahasa Indonesia for female patients. J Gen Proced Dermatology Venereol Indones. 2020;4(2):58–65.
5. Jusuf NK, Putra IB, Mahdalena M. Is there a correlation between severity of melasma and quality of life? Open Access Maced J Med Sci. 2019;7(16):2615–2618. doi:10.3889/oamjms.2019.407
6. Sarkar R, Garg S, Dominguez A, Balkrishnan R, Jain RK, Pandya A. Development and validation of a Hindi language health-related quality of life questionnaire for melasma in Indian patients. Indian J Dermatol Venereol Leprol. 2016;82(1):16–22. doi:10.4103/0378-6323.168937
7. Dogramaci AC, Havlucu DY, Inandi T, Balkrishnan R. Validation of a melasma quality of life questionnaire for the Turkish language: the MelasQoL-TR study. J DermatolTreat. 2009;20(2):95–99. doi:10.1080/09546630802287553
8. Maranzatto C, Miot H, Miot L, Meneguin S. Psychometrican analysis and dimensional structure of the Brazilian version of melasma quality of life scale (MELASQoL-BP). An Bras Dermatol. 2016;91(4):422–428. doi:10.1590/abd1806-4841.20165014
9. Grimes PE, Ijaz S, Nashawati R, Kwak D. New oral and topical approaches for the treatment of melasma. Int J Womens Dermatology. 2019;5(1):30–36. doi:10.1016/j.ijwd.2018.09.004
10. Sarma N, Chakraborty S, Poojary SA, et al. Evidence-based review, grade of recommendation, and suggested treatment recommendations for melasma. Indian Dermatol Online J. 2017;8(6):406–442. doi:10.4103/idoj.IDOJ_187_17
11. Dodmani P, Deshmukh A. Assessment of quality of life of melasma patients as per melasma quality of life scale (MELASQoL). Pigment Int. 2020;7(2):75. doi:10.4103/Pigmentinternational.Pigmentinternational_46_19
12. Du Y, Du Z, Doraiswamy C, et al. Facial skin characteristics and concerns in Indonesia: a cross-sectional observational study. Ski Res Technol. 2022;28(5):719–728. doi:10.1111/srt.13189
13. Cestari TF, Hexsel D, Viegas ML, et al. Validation of a melasma quality of life questionnaire for Brazilian Portuguese language: the MelasQoL-BP study and improvement of QoL of melasma patients after triple combination therapy. Br J Dermatol. 2006;156(Suppl 1):13–20. doi:10.1111/j.1365-2133.2006.07591.x
14. Freitag FM, Cestari TF, Leopoldo LR, Paludo P, Boza JC. Effect of melasma on quality of life in a sample of women living in southern Brazil. J Eur Acad Dermatol Venereol. 2008;22(6):655–662. doi:10.1111/j.1468-3083.2007.02472.x
15. Anderson L, Rodrigues M. Quality of life in a cohort of melasma patients in Australia. Australas J Dermatol. 2019;60(2):160–162. doi:10.1111/ajd.12969
16. Harumi O, Goh CL. The effect of melasma on the quality of life in a sample of women living in Singapore. J Clin Aesthet Dermatol. 2016;9(1):21–24.
17. Misery L, Schmitt AM, Boussetta S, Rahhali N, Taieb C. Melasma: measure of the impact on quality of life using the French version of MELASQOL after cross-cultural adaptation. Acta Derm Venereol. 2010;90(3):331–332. doi:10.2340/00015555-0837
18. Zhu Y, Zeng X, Ying J, Cai Y, Qiu Y, Xiang W. Evaluating the quality of life among melasma patients using the MELASQoL scale: a systematic review and meta-analysis. PLoS One. 2022;17(1):e0262833. doi:10.1371/journal.pone.0262833
19. Pollo CF, Miot LDB, Meneguin S, Miot HA. Factors associated with quality of life in facial melasma: a cross-sectional study. Int J Cosmet Sci. 2018;40(3):313–316. doi:10.1111/ics.12464
20. Dominguez AR, Balkrishnan R, Ellzey AR, Pandya AG. Melasma in Latina patients: cross-cultural adaptation and validation of a quality-of-life questionnaire in Spanish language. J Am Acad Dermatol. 2006;55(1):59–66. doi:10.1016/j.jaad.2006.01.049
21. Kothari P, Sharma YK, Patvekar MA, Gupta A. Correlating impairment of quality of life and severity of melasma: a cross-sectional study of 141 patients. Indian J Dermatol. 2018;63(4):292–296. doi:10.4103/ijd.IJD_10_17
22. Arellano I, Cestari T, Ocampo-Candiani J, et al. Preventing melasma recurrence: prescribing a maintenance regimen with an effective triple combination cream based on long-standing clinical severity. J Eur Acad Dermatol Venereol. 2012;26(5):611–618. doi:10.1111/j.1468-3083.2011.04135.x
23. Sarkar R, Ghunawat S, Narang I, Verma S, Garg V, Dua R. Role of broad ‐ spectrum sunscreen alone in the improvement of melasma area severity index (MASI) and melasma quality of life index in melasma. J Cosmet Dermatol. 2019;18(4):1066–1073. doi:10.1111/jocd.12911
24. Abou-Taleb DAE, Ibrahim AK, Youssef EMK, Moubasher AEA. Reliability, validity, and sensitivity to change overtime of the modified melasma area and severity index score. Dermatol Surg. 2017;43(2):210–217. doi:10.1097/DSS.0000000000000974
25. Tursina D, Hajar S, Inggriyani CG. Hubungan derajat keparahan melasma dengan kualitas hidup pada pasien melasma di praktek swasta dokter spesialis kulit dan kelamin Kota Banda Aceh [The association between melasma severity and quality of life of melasma patients in private practice of dermato-venereologists in Banda Aceh]. J Ilm Mhs Medisia. 2017;2:18–23.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Postural Orthostatic Tachycardia Syndrome: Diagnosis and Management Guide for Nurses
Seeley MC, Lau DH, Gallagher C
Nursing: Research and Reviews 2023, 13:41-49
Published Date: 14 November 2023
Understanding Chronic Obstructive Pulmonary Disease Management and Treatment Patterns in General Medicine: Results From the ASTER Study in Italy
Genga G, Alecci U, Vighini M, Stabile C, Cinquepalmi D, Grassi B, Pistelli R
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3135-3145
Published Date: 4 September 2025
Current Trends and Future Insights on Rosacea Treatment: A Bibliometric Analysis
Wang D, Zhang J, Wang B, Gao J, Zhang G
Clinical, Cosmetic and Investigational Dermatology 2025, 18:3397-3412
Published Date: 13 December 2025
Clinical Features, Mechanisms, and Management of Anxiety in Youth with Tic Disorders: A Narrative Review
Zhang S, Han F, Chen J, Shen X, Li Y
Neuropsychiatric Disease and Treatment 2026, 22:582875
Published Date: 3 March 2026